
Abstract
Linked Article
1. Background
1.1 DESCRIPTION OF THE CONDITION
The care farming approach has been used in attempt to provide health and social support to a range of people. As such, the intervention does not target any specific conditions. The number of care farms has been growing, particularly in Europe with an estimated 1000 care farms in the Netherlands (Elings et al., 2011) and over 200 in the UK (Care-Farming, 2014), 900 in France, 300 in Belgium, 160 in Germany, 675 in Italy and 100 in Ireland (Di Lacovo and O'Connor, 2009).
In the UK, approximately 30% of service users in care farms are offenders referred from probation services. These offenders often have mental and physical health problems (Elings, 2012a, Elings, 2007, Brooker et al., 2009); drug addiction and substance misuse problems (Abracen et al., 2000); socioeconomic deprivation (Farrington, 1990), have witnessed domestic violence (Caputo et al., 1999); have a family history of criminal violence (Farrington and West, 1990); and have experienced harsh or neglectful parenting (Pederson et al., 2012). Care farms may provide an environment where offenders can be provided with opportunities and are able to build their self-esteem and hope for the future, this may in term not only improve their mental health but also increase their chances of maintaining a crime-free life.
Care farms also provide services to young people many of whom have severe conduct problems, ADHD, autistic disorders or have been excluded from school (Elings, 2012b). Evidence suggests that the numbers of young children who have conduct disorders are increasing (Robins et al., 1999, Mcewan, 2014) and a large proportion of youth who show problem behaviour at a young age go on to develop antisocial personality disorders as an adult (Rutter et al., 1997) or can experience social exclusion(Hassiotis and Hall, 2008). Conduct disorders can also increase the risk of psychoactive substance use disorders, bipolar disorder and smoking in the long-run(Biederman et al., 2008). As with offenders, many young people with conduct disorders may have had limited contact with nature or responsibility of caring for other living creatures or plants. The care farm provides this interaction which may well increase self-esteem and provide a sense of purpose for these young people. This could have direct benefits to quality of life and longer-term impacts on social and educational opportunities.
Elderly people, including those with dementia, and those with physical or learning disabilities also utilize care farms (Elings et al., 2011). Being able to be physically active in nature may help to improve both the physical and mental well-being of these groups. Levels of depression and anxiety are often higher among these groups than the general populations (Pederson et al., 2011), and findings suggest that depression can cause worse health scores when combined with chronic conditions such as arteritis, asthma or diabetes (Moussavi et al., 2007). The literature on green care indicates that people often find solace when they have contact with nature, particularly when they are engaged in activities such as farming or gardening (Sempik et al., 2010). Studies have also shown that connectedness to nature has a positive effect on people's mental, physical, and psychological well-being, and spiritual beliefs (Bragg, 2013b, Sempik et al., 2010). As a result, care farms may be beneficial for a wide range of service users.
1.2 DESCRIPTION OF THE INTERVENTION
Care farming (also called social farming) has been defined as the use of commercial farms and agricultural landscapes as a base for promoting mental and physical health through normal farming activity (Hassink et al., 2007, Hassink, 2003, Hine, 2008). A care farm utilises the whole or part of a farm to provide health, social or educational care services for different groups of people, providing a supervised, structured programme of farming-related activities rather than occasional one-off visits (Care-Farming, 2014).
Care farming is a truly complex intervention. Farms differ in the type of farming activities (e.g. horticulture and livestock farming), other activities (e.g. gardening, conservation, and woodwork) and level of support provided (e.g. health promotion, counselling, skills qualifications). There is also a wide range of clients using care farms. These include those with dementia, depression, learning disabilities, substance misuse and behavioural issues, as well as offenders. Given this complexity, the main defining feature of a care farm is the involvement in farm activities for a therapeutic purpose. It is also important to highlight the farming component of the intervention, this helps to distinguish care farms from horticultural- or animal-based therapy projects. Care farms function as a social enterprise where income gained by agricultural production is used to finance the care farm (Elings et al., 2011).
A diverse range of activities can be offered to clients at a care farm. Activities selected are primarily determined by the particular needs of the client and the type of farm. For example, at one care farm in Worcester, UK, clients such as those with substance misuse problems and offenders will attend the farm twice a week for approximately 25 sessions. The first session is focused on skills training and cognitive development; following sessions are work -based, including activities such as growing vegetables, harvesting, and retailing produce and working with the farmer to manage a large herd of beef cattle (Willowdene and RITE Social Enterprises, 2013). Another care farm in West Yorkshire has clients that include young people, those with learning disabilities and offenders. These clients take part in gardening, conservation work, bee keeping and fish farming (The ABLE Project, 2013). These are just two examples of UK care farms, and other farms will have other activities depending on the nature of the farm and the clients. Apart from engaging in different activities, some care farms offer clients the opportunity to interact with other professional caregivers to receive counselling or support to develop a healthier lifestyle. A recent survey of care farms in England found that on average, 34 participants attended a care farm per week however, this varied largely from a single participant to a maximum of 300 participants. The length and duration of the care farm intervention is determined by the need of the client and this varied from 1 to 3 times a week, continued on average for 30 weeks(Bragg, 2014a).
In addition, the intervention can vary depending on the setting where it is delivered. For example, in the Netherlands an agriculturally productive farm will offer some form of care or health promotion to their clients, where as in Germany care farms are frequently connected to a healthcare institution rather than being solely based on agricultural production (Haubenhofer et al., 2010). German care farms often function on a large scale, as government subsidies are only provided to farms with more than 300 clients (Haubenhofer et al., 2010).
The clients that utilize care farms also differ according to the setting of the intervention, for example in the Norway the clients tend to be primarily young children and psychiatric clients, where as in the United Kingdom, Belgium, the Netherlands and Italy a variety of different people use the intervention(Haubenhofer et al., 2010). Clients will engage in different activities on the farm depending on their needs and interests. For example, frail elderly clients may engage in activities that require less physical exertion such as potting plants or selling produce; young people and offenders may thrive on more physical tasks and also be involved in activities that can build their skills for future employment. The authors' initial scoping of the published and unpublished literature has not identified any details and comprehensive cross-sectional studies of care farming across Europe, the US or other high income country. If such cross-sectional studies are found during this review, this important background information will be added to the publication of the findings of the review.
While the number of care farms is growing across Europe and their services are increasingly commissioned by a range of public health and social sector organisations, commissioners face challenges in identifying evidence of their effectiveness. The complexities and multi-faceted nature of care farms means that this is not an intervention that lends itself easily to a randomised controlled study design. The observational evidence that is available is published in a wide range of journals across Europe and is not easily synthesised.
Care farming can be seen as one element within a wider discourse of ‘green care’. Green care has been defined by Sempik and Bragg (2013) as follows:
Green care utilises plants, animals and landscapes to create interventions to improve health and wellbeing; (i.e. it does not represent a casual encounter with nature) It also provides care and support to enable people to reach their true potential (i.e. although many of the approaches are termed ‘therapies’ or ‘therapeutic’, they are not necessarily directed at treating or curing conditions and diseases but, as in the case of people with learning difficulties, for example, they provide care, support, training and other opportunities to enable those individuals to develop. Such opportunities are often not available elsewhere.) (Sempik and Bragg, 2013)
An overview of green activities and their relationship with nature has been developed by Bragg (Bragg, 2014b) and distinguishes between merely experiencing the natural environment and interacting with natural elements. Care farming is seen as a subset within these broader green care approaches.
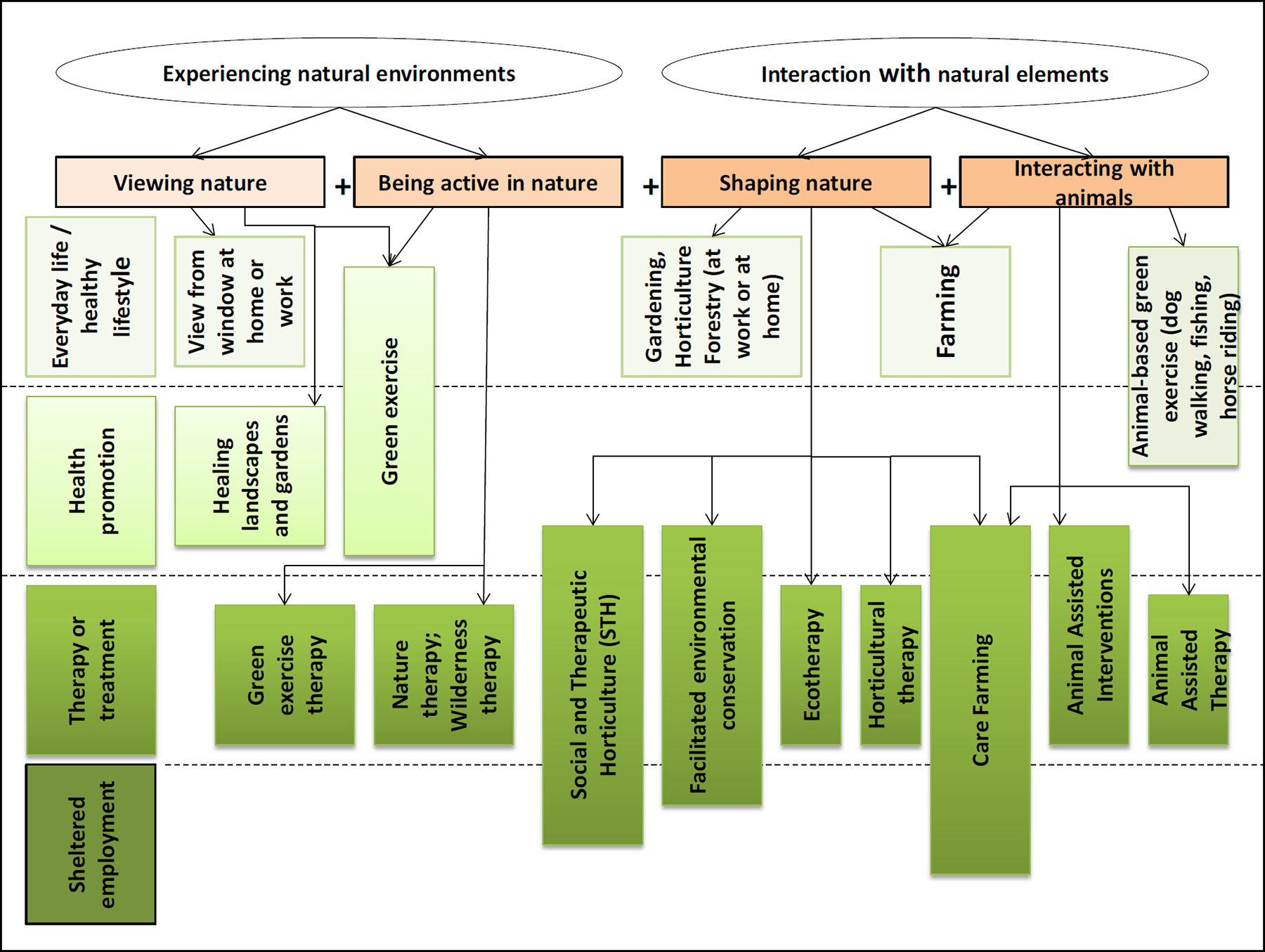
Care Farms within the Typology of Green Care
The evidence base for the effectiveness of care farming is relatively recent (within the last 10 years). Much research originates from The Netherlands and Norway. Berget, Ekeburg and Braastad (Berget et al., 2008) conducted one of the few RCTs focusing specifically on psychiatric patients and their interaction with animals in the farm setting. They found significant improvements in self-efficacy and coping ability at 6 months follow up. Kam and Siu 2010 (Kam and Siu, 2010) conducted a small RCT among 22 participants with psychiatric illness and found improvements in anxiety and depression following horticultural sessions on the farm. Pedersen et al. conducted a small RCT of 29 people with psychiatric illness and reported significant decreases in anxiety and depression ((Pederson et al., 2012). Several cross-sectional and qualitative studies have found that many participants benefit from the relationship with the farmer (and their family and other staff); being part of a social community; engaging in meaningful activities in a green environment; and for some, the possibility for work opportunities (Berget et al., 2007, Pederson et al., 2011, Pederson et al., 2012, Elings, 2012a, Elings, 2007). The fact that the farm provides an informal, non-care context which is close to the experience of everyday life, is also valued (Hassink et al., 2007; Hassink et al., 2009; Bragg, 2013a). Qualitative studies also point to improvements in mental well-being and improvements in social interactions (Hassink et al., 2011, Leck, 2013). Positive behavioural impacts such as reduced police contact and drug use have been noted amongst young participants (Hassink et al., 2009). Reductions in anxiety and depression have been observed in people with mental health issues (Pederson et al., 2012, Berget and Grepperud, 2011, Gonzalez et al., 2009, Bragg, 2013a) and those with psychiatric and addiction problems have also experienced improved social and work skills (Elings et al., 2011, Hassink et al., 2009, Bragg, 2013a, Berget et al., 2008, Berget et al., 2007, Leck, 2013). People with learning difficulties also appear to benefit, with increased life skills and improved social interaction (Leck, 2013). Improved dietary intake has also been noted in a small controlled before and after study comparing among people with dementia attending a care farm compared to those receiving day care (De Bruin et al., 2010).
1.3 HOW THE INTERVENTIONS MIGHT WORK
Sempik, Hine and Wilcox (2010) have collated theoretical frameworks that may explain how care farms are beneficial to health, well-being and social functioning among different population groups. In particular, they identify the following dimensions which are all present within care farming and the theoretical explanations for the effectiveness of these dimensions: Looking at nature: Attention restoration theory (Kaplan and Kaplan, 1989) highlights how the view or experience of nature is inherently interesting or stimulating, requires no particular effort but plays an important role in recovery from mental fatigue. Similarly, the biophilia hypothesis put forward by (Wilson, 1984) emphasises our inherent connection to nature, and our need to be in nature to achieve individual meaning and personal fulfilment (Kellert and Wilson, 1993). Being active in nature: The evidence for the effectiveness of physical activity in improving mental and physical health is well established (Stathopolou et al., 2006). Care farms bring an added element of being active in nature. The increasing body of evidence on green exercise indicates synergistic benefits of physical activity in a natural environment to improve self-esteem, mood and reduced blood pressure (Hine et al., 2008b, Peacock et al., 2007, Pretty et al., 2005, Pretty et al., 2007). Shaping and nurturing nature: Care farms also offer clients the opportunity to nurture and shape nature, whether this is caring for animals, fish, bees or growing crops, vegetables or trees. Theories of reciprocity help explain why this element may be effective due to a need to see ourselves as part of a larger whole (Lebel, 2003). While the health effects of caring for farm animals is not well researched, there is more evidence of the therapeutic role of companion animals in improving well-being for those with psychiatric disorders, addiction problems and physical ailments (Friedmann and Thomas, 1995, Fine, 2006). Social interaction: Care farms also offer opportunities for social interaction, often through working with others as a team on the farm. The benefits of such social interaction for vulnerable client groups has been identified, particularly in terms of mental health (Sempik and Spurgeon, 2006) and plays a significant role in mental health recovery models (Cloninger, 2006). Being engaged in a worthwhile purpose: Care farms also include significant elements of daily routine and responsibility to ensure the productivity of the farm. The benefits of work, structure and responsibility have been associated with both mental and physical health (Boardman, 2003, Warr, 1987). Skills building: A feature of many care farms is that they provide an opportunity for clients to learn new practical skills relating to the farm work that they undertake. Some care farms take this a step further and offer qualifications. This type of skills building may well have both short-term benefits through enhancing confidence and self-esteem, as well as long term benefits through the creation of opportunities for future employment or voluntary work. This concept can be further explained through the experiential learning theory which highlights that “knowledge is created through the transformation of experiences”(Kolb et al., 2001).
In addition to these theories, Hassink et al. (2009) highlight that the sense of community is the most valued aspect of the care farm. Participants find that they develop friendships and feel that they belong to the larger community at the care farm. Hassink et al. (2011) also finds that the role of the farmer is an important aspect of the care farm. Farmers were perceived as a role model with a strong sense of identity, who were proud of their business. Especially for youth, the farmer and the family functioned as an important role model. In addition clients with mental illnesses appreciated that they were treated with respect and without prejudice and valued the farmer as an informal caregiver.
Given the range of client groups that utilise care farms, the mechanisms influencing effectiveness are likely to vary with the needs of the participant. For example, dissonance theory may offer further insights into why care farms might be particularly effective for offenders. Key elements of dissonance theory are the recognition that the interventions that are most successful in reducing recidivism are those that can be individualised, when there are opportunities for building human relationships, opportunities or hooks for change and opportunities to reflect on past experiences and behaviour (Farrall and Bowling, 1999, Weaver and McNeill, 2007), when the offender can develop their self-efficacy (Maruna, 2001, McCulloch, 2005, McNeill, 2006), social capital by learning and applying new skills, develop a new more positive identity, (Farrell, 2004, Giordano et al., 2002, Laub and Samson, 1993, Maruna, 2001, McNeill and Maruna, 2007) and being more hopeful by focusing on the possibilities rather than limitations. It may be that care farms offer opportunities in all these areas. In this review we will identify, particularly through qualitative studies, mechanisms that may explain the effects of care farms for other key population groups. In addition, we also would explore how these mechanisms would relate to existing theories and conceptual frameworks.
1.4 WHY IT IS IMPORTANT TO DO THIS REVIEW
Finding interventions that can improve the health and well-being of different population groups is an important public health goal. If successful interventions can be found they may have a role to play in reducing inequalities. Improving the lives of the most disadvantaged can have far-reaching societal benefits, for example through enhancing social cohesion, reducing use of health and social care service usage and reducing crime (Wilkinson and Pickett, 2009). Care farming is one intervention that can potentially offer these benefits to a wide range of people.
In recognition of this, commissioners and policy makers are beginning to turn to care farms as a potentially effective intervention. Farmers across Europe are increasingly looking for ways to diversify the use of their land, and care farming may be an increasingly attractive option. As such there is great potential for the increase in the use of care farms as an intervention to bring beneficial outcomes to a range of different population groups. However there is little evidence on effectiveness (in relation to context and client groups) that can guide decision making about resource allocation.
We have identified two previous reviews on care farms. Hine et al (2008a) documented the extent and range of care farming initiatives and summarised evidence for benefits to mental health. Elings (2012a) reviewed the literature on therapeutic benefits across a number of vulnerable client groups. These reviews have helped shape the current proposal but there is a need for a systematic review to capture the full range of both published and grey literature, and to synthesise the evidence in a way that can garner current knowledge on what aspects of care farming may work, when, and for whom.
From its early establishment in Scandinavia, the Care Farming movement is expanding across Europe. In parallel with this, there are a growing number of evaluations of care farms for particular client groups. Due to the diverse nature of the client groups and the geographical locations of care farms, this evidence is rarely brought together. This review aims to synthesise this evidence, drawing out key lessons for policy makers and practitioners on the effectiveness of care farms in improving health and well-being for a wide range of clients.
This systematic review is part of a feasibility and pilot study, funded by NIHR's Public Health Research Programme, which is the start of a planned programme of work to identify the cost-effectiveness of care farm in improving the quality of life of offenders and reducing recidivism (see: http://medhealth.leeds.ac.uk/info/561/research/1045/understanding_the_impacts_of_care_farms_on_health_and_wellbeing). Through this pilot project, human and financial resources are available to undertake this systematic review and to disseminate findings to key stakeholders including commissioners, academics and care farmers.
2 Objectives
The primary objective is to systematically review the available evidence of the effects of care farms on quality of life, health and social well-being on service users.
Where possible we will synthesise the evidence in order: To understand the size of the effect that care farms may have on the health, wellbeing or social outcomes of different population groups. To examine whether effects differ depending on the activities and characteristics of the farm/farmer, the duration of time participants spend at the farm, the number and diversity of the participants on the farm, and whether the farm is the only intervention. To understand the mechanisms of change for different population groups attending care farms using a range of study methodologies, including qualitative studies.
3 Methods
3.1 TYPES OF STUDIES
We do not expect to find many randomised controlled trials of the effectiveness of care farms. Due to the possible paucity of such evidence, we are keen to include observational and qualitative studies. These studies will also be valuable in identifying possible mechanisms of action to inform our logic model.
The study designs to be included in the review are: Randomised controlled trials (RCTs) with randomisation at individual or cluster level. Quasi randomised study designs and cluster quasi RCTs, where participants are allocated by some means other than randomisation (e.g. on case number, date of birth etc.). Interrupted Time Series that clearly define intervention points and record at least three outcome measurement points before and after (or before and during) the intervention. Non randomised observational studies that are prospective and have a control group, including: Cohort studies, which must occur over a reasonable timescale for effects to be detectable and attributable (at least 6 months) and accurately record drop-out figures/characteristics. Case control studies that report cases and controls from studies whose comparability on relevant baseline characteristics and potential confounders can be judged, and comprehensively report confounders. Controlled before and after studies, where data collection must be contemporaneous and groups comparable on baseline scores. Qualitative studies: All designs of qualitative study will be considered including phenomenology, ethnography, grounded theory, and case studies. Any of the following methods of analysis will be included: thematic analysis discourse/ conversation analysis, and narrative analysis. Since our aim is to understand the main mechanisms by which care farms influence quality of life we envisage that thematic analysis will be the most valuable, however other qualitative designs may also have much to offer.
In addition to the study designs mentioned above, we will consider including before and after studies that do not have a control group as we expect to find some studies utilizing this method. We will synthesise the results of single group pre-post designs separately from other study designs. The findings may provide useful information on the nature and context of care farms and the mechanisms that may support effectiveness. Single-subject designs will be excluded.
3.2 TYPES OF PARTICIPANTS
Relevant studies of clients attending care farms of any age will be included in the review. The list below presents the likely population groups. We acknowledge, however, the possibility of identifying other relevant client groups during the execution of the review. Offenders serving community orders or similar sentences in the community rather than in prison; offenders ‘on-licence’ (i.e. recently leaving prison to re-enter the community). People with drug and alcohol problems People with mental health problems including anxiety, depression and psychiatric disorders Young people with challenging behaviour, particularly those excluded/ facing exclusion from school or those at risk of offending People with health problems particularly long term conditions, including dementia. People with learning difficulties People receiving palliative care
3.3 TYPES OF INTERVENTIONS
All care farms have some degree of ‘farming’ (crops, livestock, woodland etc.) and of ‘care’ (including health care, social rehabilitation, education or training), but the balance of these elements differs from care farm to care farm. Many care farms offer therapeutic contact with farm livestock or with crop plants, but some also provide specific therapies and interventions such as Animal Assisted Therapy (AAT) and Horticultural Therapy (HT).
The extent of the ‘caring’ element also differs from farm to farm. It may be that some clients particularly benefit from the noticeable absence of a ‘care’ or ‘institutional’ element and the presence of a working, commercial farm. Yet the situation at other care farms may be far more ‘care’ and ‘carer’ oriented with the farming element present primarily to produce benefits for clients rather than for agricultural production.
It is possible to consider a scale which has at one end a care farm with farming production as its primary focus and at the other a care farm with its main focus on provision of care services. Between these two extremes lies a potential myriad of different approaches (i.e. care farms with slightly different foci, depending on the needs of participants, motivations and goals of the project and the type of farming enterprise). Care farming is taken in this review to be an inclusive term, including all these different types of farm and their variation in motivation and type of application be that social, therapeutic or vocational.
The review will not include interventions that are purely categorised as ‘therapy’ whether in relation to animals or other natural elements; examples include pet therapy and donkey/equine therapy, where these activities are not part of a working farm. The review will also exclude petting farms and farms used for ‘one off’ educational activities. Interventions provided in hospital or in prisons will also be excluded.
Comparison conditions: An initial literature search found no trials and only a couple of small European studies which have used a comparator group. However, any studies identified during this systematic review that compare care farms to a suitable comparator will be included. Comparators will be specific to the population group studied, for example offenders serving their community order on a care farm could be compared to those serving their order by providing another community service such as cleaning public areas or for those with addiction problems, another drug rehabilitation programme.
3.4 LENGTH OF FOLLOW UP
The review will include any length of follow up of participants subsequent to their attendance at the care farm. Where possible, outcomes will be grouped as short term (under 6 months), medium term (up to 5 years) and long term (over 5 years).
3.5 TYPES OF OUTCOME MEASURES
Primary outcome: Quality of life as measured by a validated quality of life measure such as the EQ5D (Szende et al., 2014), SF36 (Ware et al., 2007.), CORE-OM (Gray and Mellor-Clark, 2007), WEMWBS (Tennant et al., 2007).
Secondary outcomes: While our primary outcome is quality of life, we will include any outcomes that use a recognised measure of health, wellbeing or behaviour, assessed using self-report or objective measures. This review will cover a broad range of secondary outcomes. We aim to use this review and evidence from our primary research to identify pathways to change for different population groups and develop a logic model to explain these relationships. Being too restrictive in the secondary outcomes for the review would limit our understanding of these potential mechanisms. The secondary outcomes will therefore include, but not be restricted to: Measures relevant to mechanisms known to be determinants of health: physical activity nutrition and diet Physiological measures: heart rate cortisol levels per cent body fat or BMI Behavioural measures: recidivism employment drug use alcohol smoking school exclusion social interaction and functioning self-esteem empowerment participation in society
To be included in the meta-analysis the primary outcome (quality of life) needs to be measured using a validated instrument.). We will include studies using self-reported, objectively measured or routinely collected data (e.g. police or school data). We will not exclude any outcome measure falling within the broad definition of health, well-being and social functioning. The outcomes studied will be recorded and will help in understanding the potentially wide range of benefits of care farms.
3.5.1 Electronic searches:
Health, education, environmental, criminal justice and social science databases will be searched to identify studies from a variety of disciplines. Care farms are seen as both a health and a social intervention, and so are likely to be reported in the literature relating to these disciplines. The selection of databases is extensive, offering a good international coverage of journals in attempt to identify relevant studies throughout the world. A single search strategy will be used to identify both quantitative and qualitative studies. We will not impose restrictions on publication format or language in the search strategy.
Electronic resources to be searched: Applied Social Services Index and Abstracts 1987+ (ASSIA) (ProQuest) CINAHL 1981+ (EbscoHost) The Campbell Library Embase Classic+Embase 1947+ (Ovid) ERIC 1966+ (ProQuest) FRANCIS 1972+ (EbscoHost) Global Health 1910+ (Ovid) GreenFILE 1910+ (EbscoHost) MEDLINE ® 1946+ (Ovid) MEDLINE ® In-Process and Other Non-Indexed Citations (Ovid) National Criminal Justice Reference Service Abstracts 1975+ (ProQuest) Criminal Justice Abstracts 1830+ (EbscoHost) PsycINFO 1806+ (Ovid) Social Services Abstracts 1979+ (ProQuest) Sociological Abstracts 1952+ (ProQuest) Web of Science. Science Citation Index Expanded (SCI-EXPANDED) –1900-present (Thomson Reuters) Web of Science. Social Sciences Citation Index (SSCI) –1900-present (Thomson Reuters) Social Care Online 1980+ (SCIE) Scopus 1995+ (Elsevier)
3.5.2 Unpublished literature searches
In order to further limit publication bias and improve the generalizability of results, we will search databases of grey literature (including conferences, dissertations and reports) and websites likely to contain unpublished reports of studies on care farms.
Resources to be searched: HMIC Health Management and Information Consortium 1983+ (Ovid) ProQuest Dissertations & Theses A&I 1743+ (Proquest) Web of Science. Conference Proceedings Citation Index- Science (CPCI-S) –1990-present (Thomson Reuters) Web of Science. Conference Proceedings Citation Index- Social Science & Humanities (CPCI-SSH) –1990-present (Thomson Reuters) Databases of ongoing trials such as Current Controlled Trials (http://www.controlled-trials.com/). Websites: European Network for Rural Development http://enrd.ec.europa.eu/
Ministry of Justice https://www.justice.gov.uk/
Care Farming UK http://www.carefarminguk.org/
Social farming in Europe http://sofar.unipi.it/index_file/socialfarfming.htm
http://www.umb.no/greencare (no longer updated)
https://www.novapublishers.com/catalog/product_info.php?products_id=41368
http://www.regjeringen.no/nb/dep/lmd/dok/rapporter-og-planer/rapporter/2012/green-care-in-the-nordic-countries–a-re.html?id=712600 (Nordic report)
http://www.matmerk.no/inn-pa-tunet (Norwegian website for green care)
In addition to electronic and unpublished literature searches, we will attempt to identify further relevant studies by examining the reference lists of included studies and any relevant systematic reviews identified, and by tracking citations of key papers using Google Scholar and Web of Science Citation Indexes. We will make full use of our links into the networks across Europe to request care farmers and researchers to locate any evaluations that they have. Further relevant studies will be identified through citation tracking activities. We will hand-search the NJAS - Wageningen Journal of Life Sciences and the abstracts of Care Farm and Social Farm conferences held in the UK and Europe.
3.5.3 Search Terms
The searches will aim to identify studies of care farms or agricultural-related therapies and rehabilitation practices within a farm setting. The searches will not be limited to a particular study type or participant group. Scoping searches have indicated limited literature on ‘care farms’, and we have therefore supplemented the ‘care farm’ phrase searches with a broader search to identify agricultural-related therapeutic and rehabilitative interventions that occur in farm settings. Our
search strategy excludes references indexed as animal-only studies due to the high number of veterinary science studies of therapies for farm animals.
Where available, alerting systems will be set up in each of the databases to keep the reviewers aware of any studies published during the time frame of the review.
--------------------------------------------------------------------------------
Database: Ovid MEDLINE(R) <1946 to September Week 3 2014>
Search Strategy:
-------------------------------------------------------------------------------- (care adj3 (farm or farms or farming or ranch or ranches)).tw. (61) (rehab* adj3 (farm or farms or farming or ranch or ranches)).tw. (6) (“social farm*” or “therapeutic farm*”).tw. (2) or/1-3 [care/rehab farms or ranches] (69) (farm* or farms* or ranch or ranches or land).tw. (67798) (agricultur* adj2 (setting* or environment* or facility or facilities)).tw. (962) (aquacultur* or hydroponic* or “market garden*” or ”horticult* unit*” or “horticult* garden*” or (small adj3 holding*) or (nurser* adj1 garden*)).tw. (5981) Agriculture/ and *“Delivery of Health Care”/ (45) “green space*”.tw. (250) or/5-9 [farms] (73773) exp nature/ (605) (nature* adj1 (therap* or intervention* or rehabilitation)).tw. (94) (green adj2 (care or exercise)).tw. (48) ((Heal or healing or sensory) adj3 garden*).tw. (19) exp Horticultural Therapy/ (13) exp animal assisted therapy/ or exp equine-assisted therapy/ (209) “animal* assisted”.tw. (170) ((riding or equine) adj1 (therap* or intervention* or rehabilitation)).tw. (67) (horticultur* adj1 (treatment* or “vocation* program*” or therap* or intervention* or rehabilitation)).tw. (31) (forest adj (therap* or intervention*)).tw. (10) onotherap*.tw. (1) hippotherap*.tw. (72) ecotherap*.tw. (3) social horticultur*.tw. (0) or/11-22 [specific agric/gardening therapies] (1197) exp agriculture/ (60791) exp *Gardening/ (329) (garden* or horticultur*).tw. (7539) ((cart or carts) adj2 (drive or driving)).tw. (0) craft*.tw. (3063) woodwork*.tw. (318) (woodland* adj3 (restor* or manage*)).tw. (25) exp “Conservation of Natural Resources”/ (31678) conservation*.tw. (49857) (paddock* adj2 maintenance).tw. (0) farm mechanics.tw. (0) ((bird* or nature) adj3 watch*).tw. (43) (apiar* or beekeep* or “bee keep*” or ”bee yard*” or beehive*).tw. (666) or/26-38 [Agriculture, Gardening, Countryside activities] (140923) rehabilitation/ or “activities of daily living”/ or animal assisted therapy/ or equine-assisted therapy/ or art therapy/ or bibliotherapy/ or dance therapy/ or early ambulation/ or exercise therapy/ or motion therapy, continuous passive/ or muscle stretching exercises/ or plyometric exercise/ or resistance training/ or occupational therapy/ or recreation therapy/ or rehabilitation, vocational/ (116891) rehabilitation centers/ (6945) rh.fs. (169525) correctional.tw. (2082) (therapy or therapies).tw. (1281666) th.fs. (1466805) or/40-45 [Rehabilitation or Therapy] (2633349) 39 and 46 [Agric/Garden/Countryside Rehab or Therapy] (4893) 25 or 47 [All Agric related therapies or rehab] (6043) 10 and 48 [Farms and Agric related therapies or rehab] (382) 4 or 49 [Care Farms or Agric therapy/rehab at farm setting] (440) exp Horticultural Therapy/ or “re-entry garden*”.tw. [feedback from campbell, with less emphasis on farm or Agri setting] (13) 4 or 49 or 51 [Care Farms or Agric therapy/rehab at farm setting] (453) exp Veterinary Medicine/ or exp Animal Experimentation/ (27933) exp animals/ not (exp animals/ and exp humans/) (4013594) 53 or 54 [Items to remove] (4029420) 52 not 55 (285)
3.6 DATA EXTRACTION AND MANAGEMENT
We will store all the references identified by the search in EndNote software. We will record (in an Excel spreadsheet) all websites searched, the date of searches, and the details of any reports found or further contacts made.
Screening 1: Titles and Abstracts
Two reviewers (NW and ZR) will independently screen the titles and abstracts of articles and grey
literature retrieved to assess eligibility, as determined by the inclusion and exclusion criteria listed above.
Screening 2: Full text
For those studies that are selected as potentially eligible for inclusion, we will retrieve full copies, and all review authors will be involved in assessing whether studies meet the review's inclusion criteria; each full-text report will be assessed independently and in duplicate. We will keep records of all eligibility decisions and will store the eligibility assessment form (with brief details of study design, participants and interventions, along with the final eligibility decision) with each study report. AH will play an advisory role for studies with a criminal justice element.
Any disagreements will be discussed and resolved by consensus at each stage of the eligibility assessment. Persisting disagreements that cannot be resolved by discussing with a third reviewer will be addressed by contacting the study authors. If this is unsuccessful, the disagreement will be recorded in the review. Multiple reports from the same study will be coded separately before combining information across reports. We will use the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) chart to detail the process of study selection (Moher et al., 2009).
Information on study design, sample characteristics, intervention characteristics, and outcomes will be extracted from studies using a template based on the CPHG Data Extraction and Assessment Template (Higgins and Green, 2011) (see appendix 1). We will use a separate data extraction form for qualitative studies (see appendix 2). When extracting findings from qualitative papers, we will distinguish between findings which describe the understandings of the participants (first-order constructs) and the interpretations or conclusions of the study authors (second order constructs).
3.7 ASSESSMENT OF RISK OF BIAS IN INCLUDED STUDIES
The EPOC Risk of Bias tool will be used for all RCTs, non-randomised controlled trials, controlled before and after studies and Interrupted Time Series (Higgins and Green, 2011)(see back of appendix 1). The Effective Public Health Practice Project tool (EPHPP) will be used to appraise other quantitative studies (Armijo-Olivo et al., 2012) (Appendix 3). Studies with the majority of domains categorised as “no” or ”unclear” in the EPOC Risk of Bias tool will be coded very high risk of bias, similarly, studies categorized as weak in the EPHPP tool will be coded very high risk of bias. If it is possible to conduct a meta-analysis, any studies with a very high risk of bias will be excluded.
Qualitative studies will be assessed using an adapted version of the Consolidated Criteria for reporting Qualitative research (COREQ) tool (Tong et al., 2007a, Long and Godfrey, 2004)(Appendix 4). Three categories of reporting standard will be established for each item: clearly met; unsure and not met.
We will pilot the tools with a sub-set of identified studies to ensure a consistent approach to assessment within the team.
Two review authors will independently assess risk of bias for each study. We will resolve any disagreement by discussion or by involving an additional review team member. If there is insufficient information (i.e. more than half of the domains or assessment items are judged as unclear or not met) to be able to address risk of bias, we will contact the authors and if there is no response then we will assess it as “unclear”.
To further facilitate discussion about the strengths and weaknesses of the research design, studies will be graded overall, to summarise the ‘weight of evidence’ each study can contribute to the review's findings (Gough, 2007). The categories below will be used:
A = The trustworthiness of the results judged by the quality of the study within the accepted norms for undertaking the particular type of research design used in the study (methodological quality)
B = The appropriateness of the use of that study design for addressing the systematic review's research question (methodological relevance)
C = The appropriateness of focus of the research for answering the review question. (topic relevance)
D = Judgement of overall weight of evidence (WoE) based on the assessments made for each of the criteria A-C.s
The overall weight of evidence score will be included in the table reporting the studies selected for full text review. The weight of evidence score will only be used as a guide to the reader, and will not be used to quantitatively weight studies in the meta-analysis.
3.8 ASSESSMENT OF REPORTING BIAS
If reviewed papers appear only to report certain outcomes and may not be reporting outcomes with a negative effect, we will contact study authors to identify missing outcome data. If we are unable to gather this missing data and we believe it may be a major source of bias, we will conduct sensitivity analyses excluding these studies.
If sufficient studies were found funnel plots will be used to asses for publication bias. If there are at least ten studies in a meta-analysis, we will create contour-enhanced funnel plots to investigate relationships between effect size and standard error(Peters et al., 2008). If asymmetry is found we will explore possible reasons as asymmetry can be found due to methodological heterogeneity.
3.9 MEASUREMENT OF TREATMENT EFFECT
Binary Outcomes
For dichotomous outcomes such as recidivism, employment, smoking, and drug use we will calculate odds ratios (Higgins and Green, 2011). Odds ratios greater than 1 will represent a positive intervention effect.
Continuous Outcomes
For continuous outcomes such as heart rate or BMI we expect results to be measured in the same unit, for these outcomes we plan to use mean difference (MD). For the quality of life outcome we expect to find continuous data with the measurement made on a scale. We plan to use standardized mean differences (SMDs) with 95% CI for continuous outcomes that have used different instruments to measure the same outcome.
Synthesising binary and continuous data
If studies present both continuous and dichotomous results for the same outcome, then we will consult a statistician to determine whether it is appropriate to convert continuous data into dichotomous data. If deemed appropriate then these data will be transformed into a common effect size metric prior to synthesis. Where ordinal data is presented from shorter validated measurement scales, we will group and analyse as dichotomous outcomes for which we will calculate odds ratios (Higgins and Green, 2011).
3.10 DATA SYNTHESIS
3.10.1 Quantitative Studies that can be synthesised
While we do not expect to find studies with sufficient homogeneity to be able to pool their effects, if we do find studies that have measured the same outcome in similar populations we will conduct meta-analyses for each outcome separately. For example, we will conduct a meta-analysis for quality of life outcome using data from people with alcohol and drug addiction. Since we expect to find some between-study variance, random-effects model will be considered. We will not separate meta-analyses by study design, but sensitivity analyses will be conducted to measure the robustness of the results.
Both RCTs and CRCTs will be included in the analyses provided that standard errors for the CRCTs have been appropriately adjusted. If we identify CRCTs that did not account for potential clustering, then we will adjust the standard errors or sample sizes using the method described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2011). The adjustment method requires the intraclass correlation coefficient (ICC). If this is not available, we will use the ICCs from analogous cluster-randomized trials. If analogous studies are not available, we will use a series of plausible values and examine the effect using a sensitivity analysis.
While we do not expect to find studies that have used interrupted time series (ITS), if we do find such studies we will synthesise them separately using the method described in Ramsay et al. (2003)
3.10.2 Quantitative studies that cannot be synthesised
We believe that the majority of the studies we find will not record data that can be synthesised statistically. In this situation, the data will be synthesised narratively according to the ESRC guidance (Popay, 2006). The main steps of the narrative synthesis will involve articulating a theory of how the care farm might work as an intervention to improve health, wellbeing and /or social functioning. The data from each study will be included in a tabular form which will illustrate emerging patterns in reported impacts of care farms and study characteristics. A narrative description of all studies, regardless of study design, will be included in the final review to accompany this tabulation. This information will provide a definitive map of research of the impacts of care farms and help to point to how future research design could be improved within this field. The narrative synthesis will not use vote counting to summarize study findings.
3.10.3 Subgroup analysis
We are interested to know whether the effect of care farms differs depending on the activities and characteristics of the farm/farmer, the duration of time participants spend at the farm, the number and diversity of the participants on the farm, and whether the farm is the only intervention
Possible subgroups include: working with animals conservation work horticulture commercial farm or social enterprise staff skills/participant to staff ration
The exact list of relevant sub groups will be determined by the studies found during the review. Because the number of studies is likely to be small, we anticipate only being able to present findings in sub groups to inform our discussion of possible mechanisms of effectiveness for different groups and interventions. Any quantitative sub group analysis will require sufficient individual level data and adequate homogeneity across studies. If this is the case and we have over 10 studies we would consider meta regression to investigate how a categorical study characteristic is associated with the intervention effects in the meta-analysis (Higgins and Green, 2011).
3.10.4 Synthesis of qualitative research
We expect to identify many qualitative studies of the impacts of care farms on different client groups. We believe these studies will be valuable in helping to uncover impacts that might be missed by quantitative studies. We hope these studies will also provide valuable information on the theoretical underpinnings of care farm programmes, shed light on important confounding factors and pathways which may help explain the variance in predicted health, wellbeing and social impacts between population groups and interventions.
Qualitative studies are likely to vary in terms of the type of care farm intervention and the client group studied, as well as the methodological approach and quality. For these reasons we propose to conduct a thematic synthesis of the qualitative data in accordance with the method used by Murray et al. (2012). Findings from each study will be tabulated to provide a textual summary of the data of each of the key factors experienced by client groups when attending care farms. For each client group, these experiential factors will be grouped, simultaneously but separately, facilitating a thematic analysis and examination of emerging themes with respect to reported impacts, mediating factors, and pathways affecting health, well-being and social impacts. We will then map these finding to the evidence derived from the quantitative studies in order to produce one overall set of findings.
3.10.5 Sensitivity analysis
To measure the robustness of the results we will conduct sensitivity analyses. For example, sensitivity analyses will be conducted according to study design (i.e. excluding quasi and non-randomized controlled trials) and in relation to risk of bias (i.e. excluding studies with high risk of bias).
3.11 DECLARATIONS OF INTEREST
The authors undertaking this systematic review are also implementing an NIHR PHR funded feasibility study entitled: ‘Understanding the Impacts of Care Farms on Health and Well-being: A Pilot study to inform the design of a follow-on study to assess the cost-effectiveness of care farms in improving health and wellbeing and reducing re-offending’.
We plan to use the findings of this feasibility study to inform the design of a follow-on natural experiment of the effects of care farms on quality of life of offenders.