
Abstract
1 Background
1.1 DESCRIPTION OF THE CONDITION
Accidents at work are estimated to kill more than 300,000 workers worldwide every year (Concha-Barrientos, Nelson, Fingerhut, Driscoll, & Leigh, 2005). In the European Union, the number of fatalities amounts to nearly 5,000 cases annually, and accidents at work cause many more cases of disability each year (Eurostat, 2004b). Aside from the human cost, workplace accidents also represent a significant economic burden to society (Eurostat, 2004a). Although the risks of accidents at work have been reduced over the last 20-30 years, the number of accidents remains unacceptably high and continues to receive much attention from a wide spectrum of policy and decision-makers.
In this review, an ‘accident at work’ is understood as an accident which causes physical harm (injury) to people at work; that injury may be minor, major or fatal. We use the term ‘accident’ for the causal event(s) leading to the harmful exposure of an individual, whereas we reserve the term ‘injury’ for physical harm as the consequence(s) of such an event. In the health and safety field it is important to distinguish ‘accidental injuries’ from chronic injuries related to long term exposures, as the aetiologies are different. We found the European Commission definition of a work accident the most exhaustive and clear (European Commission 1999). In this review an accident at work is thus defined as “a discrete, sudden and unexpected occurrence in the course of work which leads to physical harm (injury)”. This includes cases of acute poisoning and wilful acts of other persons, but excludes deliberate self-inflicted injuries and accidents on the way to and from work (commuting accidents). The phrase “in the course of work” is taken to mean whilst engaged in an occupational activity, or during the time spent at work and includes road traffic accidents occurring in the course of work.
However, we exclude accidents where the resulting injury is mental harm alone. Occupational diseases, such as occupational dermatitis and repetitive strain injuries, are not included in this review, because they have longer exposure periods, are not discrete, sudden and unexpected, and thus fall outside the definition of an accident. However, harmful exposures, such as acute poisoning and chemical burns are included, as the exposure period is short, and the event is usually discrete, sudden and unexpected, and thus accidental. It should be emphasized, that in this review the term ‘accidental’ does not mean unpredictable or unpreventable, even the specific event can be unforeseen by the victim. Most accidental injuries and their precipitating events are predictable and preventable (Davis & Pless, 2001).
The safety science literature has identified a number of measures influencing risk, safety behaviour and accidents at work (Haddon, 1968; Guldenmund, 2010b; Zohar, 2010; Kjellén, 2000; Tuncel, Lotlikar, Salem, & Daraiseh, 2006; Heinrich, 1931; Rivara & Thompson, 2000b; Spangenberg, 2010). The development in the research field has improved the predictive power of theories and conceptual models over the last four decades, and these have informed authorities, companies and employees in developing more reliable and efficient measures for the prevention of accidents at work (Hale, 2006).
In the last 10-15 years, the multidimensional characteristics of risk to workers, and not least the understanding of how to prevent accidents at work, have been widely emphasized in the safety science literature (Reason, 1997; Kjellén, 2000; Shannon, Robson, & Sale, 2001; Robson, Shannon, Goldenhar, & Hale, 2001; Guastello, 1993; Lund & Aarø, 2004). This development is referred to as the “third age of safety” (Hale & Hovden, 1998). Where accidents previously were seen from a technical, legal or human factors perspective, in recent years cultural and organisational factors have become important additional perspectives included in accident prevention programs at work (Spangenberg, 2010; Mearns, Whitaker, & Flin, 2003; Parker, Lawrie, & Hudson, 2006; Grote, 2007), and so represent a key perspective to understand the complex and multifaceted approaches to reduce harm to workers (Rasmussen, 1997; Spangenberg, Mikkelsen, Kines, Dyreborg, & Baarts, 2002). Six categories of approach can be identified: Multifaceted approaches: safety interventions for the prevention of accidents at work are characterised as a complex process which usually integrates a number of components. Research has emphasised the importance of integrating these various components in order to achieve a high level of safety at work (Guastello, 1993; DeJoy, 2005). Attitudinal approaches: the focus here is on the modification of knowledge and attitudes and its consequences for behaviour and accidents (Lund & Aarø, 2004). Behavioural approaches: the principles of the behaviour based approach are known worldwide by practitioners and are supported by organisational and psychological theory (Scott Geller, 2011; Saari, 1998; Krause & Russel, 1994). Safety Climate approaches: these include, for example, leader-based safety interventions which impact on safety climate and have consequences for behaviour and safety at work (Kines, Andersen, Mikkelsen, Dyreborg, & Zohar, 2010; Zohar & Luria, 2003). Since the seminal safety climate article by Zohar in 1980 (Zohar, 1980), a number of safety climate studies have emerged (Dedobbeleer & Béland, 1991; Flin, Mearns, O'Connor, & Bryden, 2000; Glendon & Litherland, 2001; Zohar, 2002; Zohar & Luria, 2003). This type of intervention seems to be supported by a consistent theoretical framework, relating to organizational sense making processes (Weick, 1993; Zohar & Luria, 2004; Weick, 1995), social interactions (Morgeson & Hofmann, 1999), social exchange and climate theory (Christian, Bradley, Wallace, & Burke, 2009; Nahrgang, Morgeson, & Hofmann, 2007; Mearns, Hope, Ford, & Tetrick, 2010; Zohar, 2003; Zohar & Luria, 2004). Structural approaches: these include, for example, the use of occupational health and safety management systems (OHSMS's), either initiated internally by the company or externally by legal bodies or other stakeholders (Heinrich, 1931; Haddon, 1968; Lingard & Holmes 2001, Robson et al, 2007). Safety culture approaches: these represents a central approach to safety intervention in theory and practice (Nielsen, 2014; Guldenmund, 2000; Guldenmund, 2010b; Hale, 2010)
1.2 DESCRIPTION OF THE INTERVENTION
In this review we focus on primary safety interventions, defined as any attempt deliberately applied to promote safety and decrease the frequency or severity of accidental injuries at work (Robson et al., 2001), that affect risks and safety at work and which can have consequences for the occurrence of accidents causing injury to people at work. Such accidents may subsequently have consequences in terms of disability, work absence and other personal and economic costs.
As safety interventions are rarely based on one component alone, it is expected that some of the safety interventions for the studies included in this review will consist of more than one type of intervention component, such as safety training, a safety campaign, goal setting, safety feedback or machine safeguarding. It is recognised in the field that there is a certain lag phase (latency period) in the implementation of safety interventions, and that this is dependent on the type of safety intervention and the context (Robson et al. 2007). For example the introduction of a new provision or safety legislation will have a longer lag phase compared to the introduction of a new safeguard on a machine. This will be taken into consideration when effects of interventions are evaluated. A safety intervention may consist of one or more components, and can run for a shorter or longer period of time, or involve a permanent change, such as new regulations or orders.
A safety intervention can be initiated at work, e.g., by the employer or the employees, or initiated externally by public authorities, social partners or other stakeholders, but the intervention attempts to improve safety and prevent accidents at work. Interventions aimed at the prevention of accidents at work can operate at different levels, namely at the micro-, meso- or macro-level, i.e., individual, group or organisational, or the broader societal-industry level, respectively (Landeweerd, Urlings, De Jong, Nijhuis, & Bouter, 1990; Hofmann, Jacobs, & Landy, 1995; Lund and Aarø, 2004; Spangenberg, 2010; Haslam et al., 2005; Dyreborg, 2011).
This review adopts an inclusive approach to the meaning of a safety intervention, and recognises the various theoretical approaches and distinctions made in the scientific literature and in practice in this field. It is not expected that studies evaluating safety interventions in general are explicit about how the intervention might work, but on the basis of the information we will seek to classify the types of interventions. Lund and Aarø (2004) have suggested that safety interventions for prevention of accidents at work might work by applying three main types of measures: attitude modification, behaviour modifications and structural modifications. Additionally, a fourth type, safety climate modifications, is suggested by a large body of research (Christian et al., 2009; Spangenberg, 2010; Nahrgang et al., 2007; Zohar & Luria, 2003; Zohar, 2002). In practice, these types of measures can involve a number of different components to form integrated safety interventions.
In this review we define a safety intervention component as an independently operating entity in the intervention, which can stand-alone. This means, for example, that the instruction to the use of a specific item of fall protection equipment is not a component in itself, but is part of the component ‘introduction of fall protection equipment’, since the introduction to the use of the equipment would be meaningless without this equipment. However, in the case where a general introduction or campaign about fall risks at a workplace is given to raise awareness among workers besides the introduction of fall protection equipment, it will be classified as two separate components, as both components can be stand-alone interventions.
Below is listed the main types of components of safety interventions directed at the individual or the group/organisational level, respectively.
Attitude modification: This may be achieved by means of information and persuasive messages in campaigns, leaflets, booklets, films, posters, direct mail, guidelines, or by teaching or various counselling approaches.
Behaviour modification: This may be achieved by means of training, incentives, goal setting, feedback, or individual coaching etc.
Climate/culture modifications: Climate, culture or social norms may be changed through leadership-based interventions, goal-setting, feedback, introduction or modification of safety management approaches, or by the influence of sectorial- or societal-level changes and modification of values or norms related to safety at work.
Structural modification: Contextual factors are changed through legislation, regulation, enforcement and economical or other incentive systems. This also refers to changes in the organization of safety management systems, the physical environment, engineering, i.e., modification of equipment and products, and implementation of rules and regulation, workers' rights and interests etc.
If other types of safety interventions are found in the included studies, they will be added to the classification scheme (see detailed classification in section 12.3).
The review excludes secondary and tertiary interventions, such as on-site injury treatment, rehabilitation and return to work programs. Public safety campaigns directed at the general population and community-based safety interventions are also excluded from the review, as they are not primarily implemented at workplaces.
1.3 HOW THE INTERVENTION MIGHT WORK
Even though the working environment, the nature of work, and the workforce vary from one industry to another, we assume that the different types of safety interventions work in similar ways across various settings, although the effect may be modified by contextual factors, such as whether the industry is static or dynamic (Sadayappan & Moaued, 2011; Cooper, 2007). Work settings that experience transient workforces, such as in construction work, can be a barrier to the implementation of safety interventions as steps taken are easely lost when staff disappear and new ones come in. Also peer pressures resulting from the social dynamics within a group could be weaker in dynamic settings with unstable workgroups, thus making safety interventions more difficult to maintain, for example, in improvement to the safety climate in construction work (Dedobbeleer & Béland, 1991; Kines et al., 2010).
In the following we describe how the four main types of safety interventions might work with references to the most relevant theory in the field.
Attitude modification: The underlying assumption of this type of measures is that attitudes can be modified by the provision of information and knowledge to the relevant persons, and that this in turn can influence behaviour. The theoretical or conceptual support of such approaches is the KAP (Knowledge-Attitudes-Practices) model (Lund and Aarø, 2004). According to this model, safety-related behaviour is determined by an individual's knowledge and attitudes. Within this perspective safety information, e.g., provided by pamphlets, safety campaigns, or safety courses, can change peoples' behaviours, through providing them with the right information or knowledge about the hazards at the workplace, and the consequences these can have on their health.
In particular, social psychology research has provided theoretical knowledge on the relationship between attitudes and human behaviour (Hofmann & Tetrick 2003). This attitude behaviour relationship has provided the basis for a number of practical approaches for the prevention of accidents and injuries at work, where knowledge and information related to risk and safety at work has been disseminated or taught to workers with the intention to modify their attitudes and promote safer behaviour (Burke et al. 2006).
To our knowledge Wicker's (1969) review is the first to review research on the relationship between attitudes and behaviour. He concluded that attitudes probably do not predict behaviour. Since this review, social psychology researchers have sought to develop models that increase the predictive power of attitudes. The main approach within the psychology research area has been to build more complex models of the relationship between attitudes and behaviour, by inclusion of a number of additional components assumed to affect behaviour (Armitage & Conner 2001). The two most known models are the Theories of Reasoned Action (TRA) (Ajzen & Fishbein 1980; Fishbein & Ajzen 1975) and Theory of Planned Behaviour (TPB) (Ajzen 2012). The assumption is that behavioural intention is the best predictor of behaviour. Behavioural intention is regarded as a product, not only of attitudes, but also of social influences (including social norms) and self-efficacy (or perceived behavioural control).
Behaviour modifications are based on an environmental approach. Where the attitude modification approaches mainly explains behaviour in terms of internal mental states and cognitive processes (knowledge-attitudes-behaviour), behaviour modification approaches represent an external focus that explains behaviour in terms of environmental consequences (Luthans & kreitner 1985).
The theoretical framework for the behaviour modification programs is based on behaviourism, specifically operant (learned) conditioning that can be traced back to B.F. Skinner (1969), who contributed with the distinction between learned and unlearned behaviour. Skinner suggested that humans choose various responses to receive a particular consequence. This contingency is framed as the Antecedent-Behaviour-Consequence (A-B-C) model, where both antecedents and consequences are responsible for affecting the behaviour of an individual. Where antecedents serve to define or signal the behaviour, then the consequences of behaviour serve in influencing and reinforcing the behaviour more directly and also encourage the occurrence of behaviour (Krause et al. 1999). Skinners theoretical framework has been expanded by inclusion of the mediating role of cognition, and the term organisational behaviour modification has been suggested for this approach (Luthans & kreitner 1985). Another important expansion of the Skinnerian approach is the social learning theory (Bandura 1971). These theoretical frameworks have informed safety intervention research and practice. Some commonly used components in behaviour-based safety interventions are safety training, goal-setting and feedback, observation and feedback, verbal feedback, data analysis, and problem solving (McAfee & Winn 1989, Krause 1999). A number of behaviour based safety studies have been conducted since the 1970's (Tuncel et al. 2006), which includes a number of various models and components (Cooper 2007; Laitinen & Ruohomäki 1996).
Structural modifications are approaches comprised of a number of models and components related to changes in the physical, organisational or regulatory environment. A common feature of the structural approaches is that environmental factors are changed, often over longer time and more profound. One type of structural modification is the engineering control, e.g., introduction of machine safeguards, walkways, elimination of hazardous substances or materials, and other changes in the physical environment, that directly influences individuals' safety without necessarily affecting their behaviour. Another type of structural change is social control, e.g., changes in laws and regulations that provide coercive power or incentives for people or organisations to change behaviour.
Engineering control approaches are based on the hierarchy of controls (Lingard & Holmes 2001) stating that the most effective preventive measures are taken by eliminating the risk at the source. The most common models used are based on a simple linear model, where a chain of multiple events culminate in an injury. The safety prevention is then directed at removing one or more elements involved in this chain of events, to prevent the occurrence of the injury. One such model is Heinrichs ‘Domino theory’ (Heinrich, 1931), which has had a tremendous effect on practical safety interventions, and still is much in use. A further development of these models are the complex linear models, such as ‘Haddons Matrix’ (Haddon 1968) and the Swiss cheese model (Reason 1997).
Another type of structural modification is social control, which is related to legislation, enforcement and legal sanctions of rules and regulations to achieve behaviour on a non-voluntary basis, or marketing, which is a voluntary exchange, e.g., insurance related benefits for low risk companies. Regulation may serve as a potentially powerful institutional force to promote the adoption of occupational health and safety policies and practices (Chambers et al. 2013). The basic idea is that such instruments provide an incentive for companies or people at work to stick to certain (legal) standards, either because of the risk of penalties in case of noncompliance, or because a benefit can be achieved in exchange for an appropriate behaviour (Rothschild 2000).
Safety climate and culture modifications: Safety culture has long been a subject of interest for safety science, and particularly so following the Chernobyl nuclear meltdown in 1986. However, the theoretical framework for safety culture is generally underdeveloped and the link to research on organizational culture has been weak or even non-existent (Choudhry et al. 2007; Guldenmund 2000). There is, for instance, no widely accepted definition of an organization's safety culture or any consensus on how to change a safety culture to improve safety. Therefore, the concept of safety culture is vague and not easily translated into safety prevention efforts, which may explain why there is a noticeable lack of (safety) culture change intervention studies in the safety literature (DeJoy 2005; Hale et al. 2010; Nielsen 2014). The most elaborated theory of safety culture is based on Edgar Schein's Theory of organizational culture (Schein 2004), where the essence of culture is its core of basic assumptions that manifest as values and in turn defines behavioral norms, e.g., norms that influence safety behavior. The basic assumptions and values are taken for granted and maintained by members of a group, and will be taught to new members as the correct way of thinking and feeling in relation to specific aspects, such as safety. Following this, safety culture might be defined as those aspects of the organizational culture which will impact on attitudes and behavior related to increasing or decreasing safety or risk (Guldenmund, 2010a).
A related concept of culture is climate, which describes the shared perceptions of organizational policies, practices, and procedures, both formal and informal (Reichers & Schneider 1990). Safety climate is supported by a wide range of consistent theoretical frameworks, relating to organizational sense making processes (Weick, 1993; Zohar & Luria, 2004; Weick, 1995), social interactions (Morgeson & Hofmann, 1999), social exchange and climate theory (Christian, Bradley, Wallace, & Burke, 2009; Nahrgang, Morgeson, & Hofmann, 2007; Mearns, Hope, Ford, & Tetrick, 2010; Zohar, 2003; Zohar & Luria, 2004).
Safety climate has been a widely researched approach to accident prevention since the term was introduced by Zohar (1980). Although there is no general consensus on a definition of safety climate, and the literature has been plagued by conceptual ambiguity (Zohar 2010), meta-analyses have identified some common ground and reveal that safety climate is a robust predictor of safety performance (Nahrgang et al. 2007). The assumption underlying this approach is that the safety climate of an organization/group, which can be understood as a socially constructed phenomenon as it emerges as a group-level property through shared cognitions and social consensus, informs workers on how they are expected to act under different circumstances. Thus, the safety climate reflects the shared priority of safety in an organization/group compared to other competing goals such as productivity or quality. It has been suggested, that safety climate can be understood as a surface manifestation (espoused values) of the deeper cultural levels (Guldenmund 2000; Guldenmund 2010b; Schein 2004). Furthermore, the culture and climate approaches have brought focus on the role of leaders and leadership in creating general organizational change and the prevention of accidents at work. These approaches are often centered on the commitment to and priority of safety demonstrated by supervisors and top management (Hofmann & Tetrick 2003; Zohar 2002).
1.4 WHY IT IS IMPORTANT TO DO THIS REVIEW
Accidents at work are prevalent in society, but there are several gaps in our knowledge on the efficiency of various safety prevention components designed to be used by policy makers and practitioners to prevent accidents at work.
Despite earlier attempts to summarize the evidence, the effectiveness of strategies for preventing accidents at work remains unclear. One limitation is that previous reviews have restricted their focus to one type of injury, for example, eye injuries, or one type of prevention measure (Tuncel et al., 2006; Robson et al., 2005; Robson et al., 2007; Cameron & Duff, 2007), one type of event, e.g. falls (Hsiao & Simeonov, 2001; Rivara & Thompson, 2000a), or on one industry, e.g. agriculture or construction industry (Lisa & Risto, 2000; Lehtola et al., 2008; Rautiainen et al., 2008). Specificity of focus can decrease the likelihood of misclassification and may therefore be useful when addressing very narrow review questions. On the other hand this would also severely restrict the number of studies eligible for review. Also, too specific a focus produces results that are ultimately not useful in broadly addressing the types of safety interventions that aim to prevent injuries at work, i.e., identify a ‘best’ approach to safety intervention in a particular context. For this reason this review will consider all work settings and the contextual factors reported, and also consider the relevant follow-up times, as the latency period for when to expect an effect will differ depending on the type of safety intervention. The current evidence may be summarised as follows:
Multifaceted approaches: A review of accident prevention programs by Lund and Aarø (2004) concludes that the greatest effect is obtained in a combination of attitudinal, behavioural and structural approaches (multi-faceted interventions). Even though the review is comprehensive, and provides a very useful categorization and modelling of the level and type of intervention, the study did not establish summarized effect sizes for the various prevention measures. Moreover, the study also included non-occupational accidents such as those occurring during leisure time, in traffic and at homes. The review also suggested that it might not be possible to influence an organisation's safety culture directly, and this has also been supported by other studies (Richter & Koch, 2004; G. Grote, 2007). A review by Guastello (1993) compared reductions in accidents for ten types of workplace safety interventions, and showed that individual approaches had smaller effect sizes compared to more comprehensive (multi-faceted) programs. However, the review did not assess the statistical significance for effect sizes; thorough and systematic assessment of the methodological quality of the included studies was lacking; and finally, an appropriate conceptual categorization of the workplace safety programs was missing. A recent update of a Cochrane systematic review (van der Molen et al., 2008) assessed the effectiveness of preventing injuries in the construction industry (van der Molen et al., 2013). Of the 17 studies included in the review, 12 were Interrupted Time Series studies (ITS) and one was a controlled before-and-after (CBA) study. The authors reported limited evidence for the effectiveness of a multifaceted safety campaign (Spangenberg et al., 2002) and a multifaceted drug program (Wickizer, Kopjar, Franklin, & Joesch, 2004) in preventing injuries, and no evidence was found that legislation is effective in preventing nonfatal or fatal injuries in the construction industry (Lipscomb, Li, & Dement, 2003). The methodology of this review has been criticised recently for a lack of sensitivity to context and a lack of flexibility in using the Effective Practice of Organisation of Care (EPOC), which makes it difficult to address challenges faced by workplace interventions (Lipscomb, Pompeii, Myers, Schoenfisch, & Dement, 2009). In order to avoid such criticism in the present review we have taken some important methodological steps: firstly, we do not restrict the review to the construction industry; secondly, we implement various methods for the control of ITS designs; thirdly, we distinguish between various types of safety interventions by classifying them theoretically and conceptually; fourthly, we consider the contextual factors reported; and finally, we consider the relevant follow-up times, as the latency period for when to expect an effect will differ depending on the type of safety intervention.
Attitudinal approaches: Modification of knowledge and attitudes and its consequences for behaviour and accidents has been researched in various settings outside and inside the workplace. Attitudes seem to be related to behaviour and accidents, even though the evidence is not clear (Williamson, Feyer, Cairns, & Biancotti, 1997; Lund and Aarø, 2004; Guastello, 1993; Rundmo, 2000).
Behavioural approaches: Behaviour-based interventions have shown a consistent positive effect on the reduction of the reporting of accidents at work (Krause, Seymour, & Sloat, 1999; Tuncel et al., 2006; Zohar & Luria, 2003; Cooper, 2007; Stajkovic & Luthans, 2001). A systematic review and meta-analysis have been carried out on behavioural safety interventions in 2006 (Tuncel et al.). The study shows evidence for the effect of behavioural safety interventions. However, the review excluded training interventions, such as those addressing the antecedents of behaviour.
Safety Climate approaches: Three recent meta-analytic studies revealed that safety climate offers robust prediction of safety related outcomes across industries and countries (Beus, Payne, Bergman, & Arthur, Jr., 2010; Nahrgang et al., 2007; Christian et al., 2009), and thus demonstrate the strength of an inverse relationship between safety climate and safety outcome, such as work accidents (Zohar, 2010; Zohar, 2002). A fourth recent meta-analytic study showed that a supportive workplace environment was consistent in explaining safety outcomes and other variables across industries (Nahrgang et al. 2011).
Structural approaches: A review covering literature until July 2004 (Robson et al. 2005; Robson et al. 2007) concluded that the body of evidence was insufficient to make recommendations either in favour or against Occupational Health and Safety Management Systems (OHSMS's). The present review will update this evidence by including the last eight years and by a broader scope of literature search. Another type of structural approach is the implementation of legislation and enforcement of rules and regulations to improve safety at work and decrease accidental injuries. A recent review covering literature until January 2013 concluded that there is evidence that labour inspections decrease occupational diseases and/or accidental injuries in the long term, but not in the short term (Mischke et al, 2013). The review thus included both the effect on either health and safety hazards or rates of occupational diseases and injuries. The quality of the evidence was considered low. The review excluded studies on the effect of voluntary consultations. The present review will only consider effects on accidental injuries, but will include the effects of voluntary consultations such as soft regulations, occupational health service systems and safety audits.
Safety culture approaches: Reviews of safety culture interventions have mainly been conducted as qualitative assessments and primarily based on a theoretical evaluation of the effectiveness (Gadd & Collins, 2002; Vaughan, 1996; McDonald, Corrigan, Daly, & Cromie, 2000; Farrington-Darby, Pickup, & Wilson, 2005; Guldenmund, 2000), and in some cases include organizational aspects (Guldenmund, 2010a; Hale, Guldenmund, van Loenhout, & Oh, 2010; Weick, 1987; Parker et al., 2006; Hale & Hovden, 1998). As safety culture represents a central approach to safety intervention in theory and practice, it is important to evaluate the existing knowledge, and assess the effect of safety culture on behaviour and accidents at work, if the quality of the available studies allows for such an evaluation.
Even though a number of reviews and evaluations of safety interventions have been conducted, reviews of workplace safety interventions using systematic approaches are limited in number, not up to date, and not comprehensive, particularly in systematic reviews that include programs covering different levels and types of components. This review aims to evaluate the effects of the main types of safety interventions for preventing injuries at work and to synthesize best practices that are widely applicable.
This systematic review will summarize the most recent scientific evidence on the effectiveness of the main types of safety interventions and their components in preventing accidents at work; the process will be based on the conceptual model of Lund and Aarø (2004). A main type of safety intervention could be, for example, attitude/knowledge modification at the individual level or structural modification at the organizational level (Figure 1). The review aims to fill the gap in the extant knowledge on safety interventions at work by evaluating the effects of the main types of interventions for preventing injuries at work and to synthesize best practices that are widely applicable. The review will not be confined by language, geographical location of the study, age or gender. It will only consider accidents at work; it will not include those which occur in the home, or during leisure activity, or which involve third parties such as hospital patients or pedestrians passing a construction site.
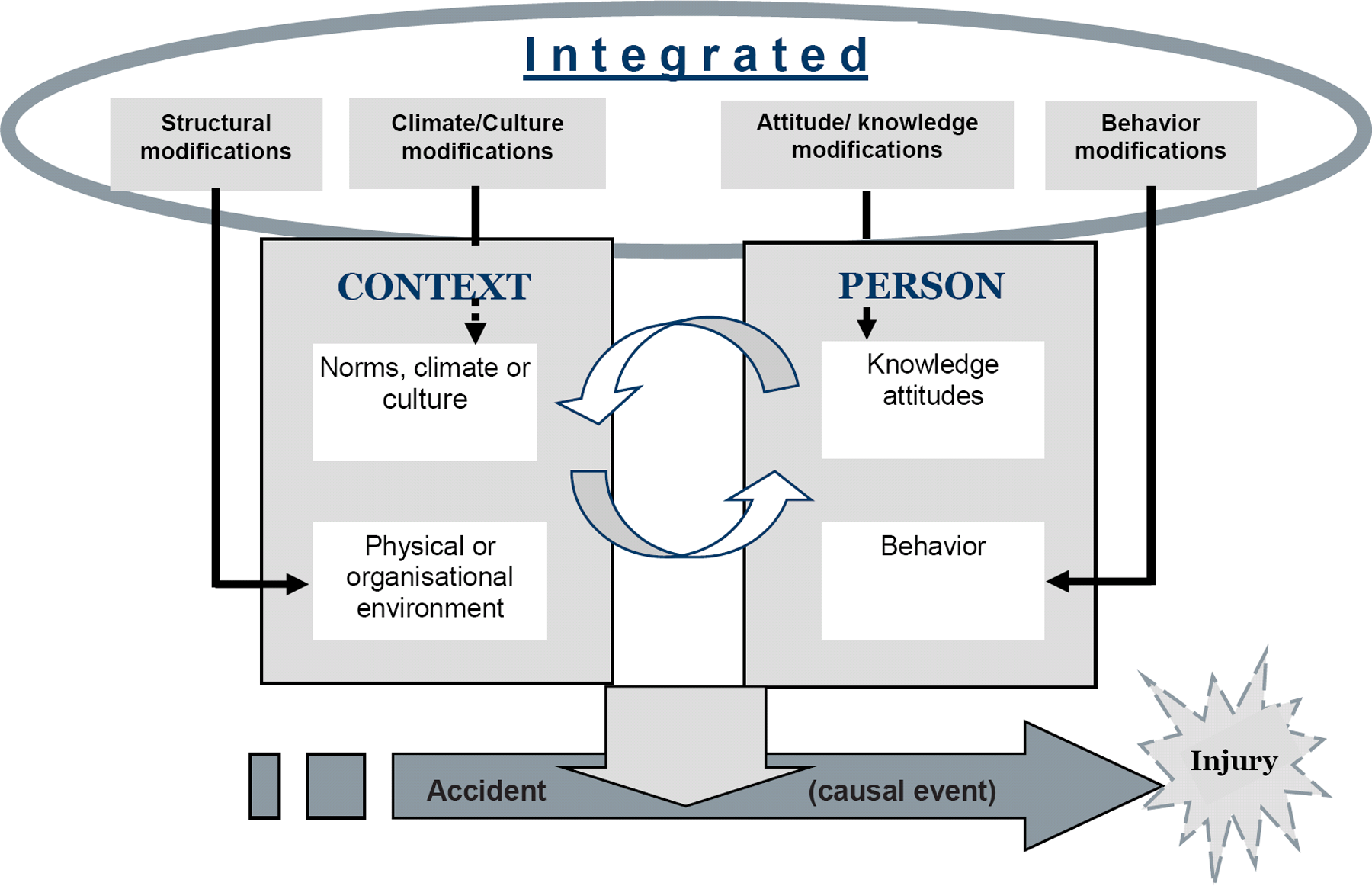
Possible pathways for preventing injuries at work
2 Objective of the review
The objective of this review is to assess the effectiveness of safety interventions in preventing accidents at work (SIPAW). The review aims: to compare safety interventions to no treatment, treatment as usual or alternative intervention. if possible, to examine which constituent components of safety intervention programs contribute most strongly to preventing accidents at work for a given setting or context.
3 Methods
3.1 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
A variety of research designs have been used to evaluate workplace safety interventions. Random allocation is not always feasible for all types of safety interventions in workplace settings because of a number of practical issues. Moreover, workplaces are often highly dynamic and complex social entities and accidents are rare events, thus not lending workplace safety interventions to be evaluated using highly controlled studies. For the same reason, observational studies are included in the review which allows for the assessment of longer term effects and opportunities to incorporate larger samples at times. Thus, for the purposes of this review we will be including a broader range of studies than is typically found in Campbell reviews. In addition, because safety interventions are often directed at the workplace level, this review will not only consider studies measuring effects at the level of the individual, but also consider studies measuring effects at the organizational level. We will, however, keep studies measuring effects at the individual level separate from studies measuring effects at the organizational level because they are asking different questions and are analysing data at two different levels.
3.1.1 Types of studies
In this review the following types of studies are eligible for inclusion: Randomised controlled trials (RCTs), including studies with cluster randomisation. Quasi randomised study designs (where participants are allocated by means such as alternate allocation, person's birth date, the date of the week or month, case number or alphabetical name order) Non randomised control study designs (quasi-experimental designs) such as controlled two group study designs, and study designs using observational data where statistical methods such as modelling of differences in differences are used. Nonrandomised controlled studies will be required to provide information on baseline comparability of the cohorts and use statistical tools to adjust for all baseline differences that are statistically significant before the intervention. Interrupted time series (ITS), which use observations at multiple time points before and after an intervention (the ‘interruption‘). In safety science studies the ITS design, in particular, is useful for the evaluation of the effect of legislative changes, changes in safety procedures, changes in the use of new types of machinery, etc. Single group study designs with before and after measures. As we suspect that there will be few RCTs and a limited number of non-randomised control study designs used in safety intervention studies, single group study designs are included to give a better sense of the most important components included in safety interventions for the prevention of accidents at work.
The comparison conditions will be either no intervention, treatment as usual or alternative intervention. This does not apply to before-after studies and Interrupted Times Series Studies (ITS), where there will likely be no comparison condition, or the comparison condition could be the general working population or another relevant comparison group. We will consider an ITS study to fall into one of three groups: ITS with internal control conditions, ITS with external control conditions, and ITS without control conditions.
The simple before-and-after study is a type of non-experimental design that is commonly used in safety science studies. Although it can suffer from serious threats to internal validity, it can provide preliminary evidence for intervention effectiveness, in particular when it is supplemented with complementary information (Robson et al., 2001). Simple before and after designs will not be included in any meta-analysis, but will be described and compared, and reported in a narrative analysis.
Given that the duration of interventions and the duration of follow-up will vary greatly depending on the safety intervention and the setting, we will include studies with any length of durations in this review. We will also include retrospective cohorts since these may be the only practical way of examining policy effects; retrospective cohorts are used to establish time series, especially for occupational cohorts.
Types of studies not eligible for inclusion: Studies measuring effects only after the intervention is applied. Single-subject designs or case studies Case-crossover studies, which are typically used to assess injury aetiology Cross-sectional and case control studies Laboratory studies
3.1.2 Types of participants
The population in the scope of this review is limited to people in the working population, either at the individual or at the organizational level. Accidents at work are thus limited to those actually engaging in the work, this include voluntary as well as unpaid employees. This also includes any subsets or special populations of participants, such as studies that select females or young employees at worksites for interventions. The review will not be confined by the geographical location of the study, nor by the age or gender of participants.
The review will only consider accidents at work, and will not consider those which occur in the home, or during leisure activity; similarly, road traffic accidents not related to work, and accidents involving third parties (such as hospital patients or pedestrians passing a construction site) are omitted.
3.1.3 Types of interventions
All types of safety interventions are of interest for this review. We assume that safety interventions can be classified into one of the following four categories:
Attitude modification: where the aim is to modify attitudes by means of information and persuasive messages in campaigns, leaflets, booklets, films, posters, direct mail, or various counselling approaches etc.
Behaviour modification: where the aim is to modify behaviour through approaches such as training, incentives, goal setting, feedback, and coaching.
Climate modifications: where the aim is to change climate, social norms and culture through leadership-based interventions, by the introduction or modification of safety management approaches, or by the influence of sectorial- or societal-level norms and expectations that impact organizational preferences and world views.
Structural modification: where the aim is to change contextual factors through legislation, regulation, enforcement, economic incentives and/or other types of modification that influence the organization of work safety, physical environment, engineering, modification of equipment and products.
Usually, more than one type of safety intervention is included in a safety intervention program (integrated approach). Each type of safety intervention described above may consist of one or more components (multifaceted). A conceptual model, based on Lund and Aarø (2004), is presented in figure 1, which indicates some possible pathways to prevent accidents. Behaviour of members of the organization and the organizational and physical environment provide the main risk factors for accidents at work. Attitudes and beliefs at the individual level, and social norms, climate and culture at the group or organizational level are process factors that may influence the presence of risk factors at work. Guidance on the classification of safety interventions are presented in appendix 12.3.
3.1.4 Types of outcomes
A series of primary and secondary outcomes of interest have been identified for inclusion in the review process. Both organization level outcomes and individual level outcomes are to be included. All sources of outcome data, including self-report, will be eligible.
3.1.4.1 Primary outcomes
The primary outcomes of interest include: Incidence of accidental work injuries causing physical harm Number of lost working days due to injury events and cases of work disability Proxy measures of injury incidence, such as changes in safety behaviours and/or changes in injury risk factors (proximal risk factors)
We have included safety behaviour and relevant injury risk factors as primary outcomes, as they are considered proxies for accidents at work (Laitinen et al., 2003; Laitinen and Paivarinta, 2010). Outcomes of mental or psychological harm resulting from an accident will be excluded from the review.
3.1.4.2 Secondary outcomes
The secondary outcomes of interest include process factors viewed as distal risk factors for injury: Changes in knowledge and attitudes Changes in norms, climate and culture
Accidents at work are relatively rare events, from a statistical perspective, compared to measures of safety-related behaviour and workplace risk factors; the latter are often used in evaluation of safety interventions. We are particularly interested in identifying studies where both secondary and primary outcomes may be measured. Cases where we might identify that changes are seen in knowledge levels or safety climate, for example, as well as in injury rates would add significantly to the knowledge of work injury prevention efforts.
3.1.4.3 Outcome measures
The primary outcomes of safety interventions are typically measured as dichotomous (binary) data, as for each individual there are only two possible categorical responses, e.g., injury or no injury. Injury incidence is an injury rate. The rate may be expressed in a number of ways typically taking the form of number of injuries/population size in a given time period. Cases of work disability and number of lost working days can be expressed similarly. It is not uncommon for these rates to be calculated based on a denominator of person-time, such as hours of work. Prevalence rates (%) are acceptable given a stable work population over time. Changes in a relevant injury risk factors or safety behaviour might also be measured as a binary variable (exposed - yes or no, or safe/correct behaviour – yes or no).
Measures of knowledge, attitudes, climate and culture will usually be expressed continuously where data can take any value in a specified range, e.g., a safety climate scale. Measurement of safety attitudes as well as climate and culture in the context of safety intervention research are evolving constructs (Flin et al 2000; Seo et al 2004; Kines et al 2011). We expect to see them measured in a variety of ways depending on the context of the work and the specific research questions. Consequently, we are not restricting our assessments to any pre-specified scales or indices.
The exact duration of follow-up will be recorded for each study, where applicable. We will examine outcomes at the following time points: post-test (immediately after the intervention ends); short-term follow-up (up to and including six months after the intervention ends); medium-term follow-up (more than six months and up to and including 12 months post-intervention); and, long-term follow-up (more than 12 months post-intervention).
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.2.1 Electronic searches
Relevant studies will be identified through electronic searches of bibliographic databases, government policy databanks and internet search engines. We will include grey literature by, for example, searching the OSH ROM and Google. No language or date restrictions will be applied to the searches. PubMed 1966 - to present (includes MEDLINE) Embase 1980 - to present CINAHL 1981 – to present EI Compendex OSH ROM (we search in NIOSHTIC 1977-present, HSELINE 1977-present, CIS-DOC 1974-present) PsycINFO 1806 - present EconLit Business Source Elite Web of Science 1969-present Perosh Safetylit.org ProQuest (dissertations) or the interface
The websites of the following organisations will be searched for relevant documents: World Health Organisation (WHO) European Agency for Safety and Health (OSHA) European Agency for the Improvement of Living and Working Standards (Eurofond) International Labour Organisation (ILO) Organisation for Economic Co-operation and Development (OECD) National Institutes of Occupational Safety and Health Cochrane Library
3.2.2 Search terms
The search strategy that will be used for MEDLINE is reproduced below. It will be modified, where necessary, for the other databases listed. The full details of such modifications will be reported in the completed review. We have used trial filters that allow non-randomised studies and simple before and after studies to be included in this review. The filters are developed on the basis of “Cochrane's highly sensitive Search Strategy for identifying randomized trials in MEDLINE” (Higgins & Green, chapter 6, 2008). However, its ability to identify ITSs and CBAs is not so well known in terms of sensitivity and specificity (Fraser C & Thomson-O'Brien MA, 2000). The search strategy in this review, as a whole, is developed taking into account both sensitivity and specificity of searches (Verbeek et al., 2005), and also the resources allocated to this review project. #1 injur*[Title/Abstract] OR accident*[Title/Abstract] OR harm[Title/Abstract] OR harmful[Title/Abstract] OR fall[Title/Abstract] OR falls[Title/Abstract] OR falling[Title/Abstract] OR burn[Title/Abstract] OR burns[Title/Abstract] OR poison*[Title/Abstract] OR slip [Title/Abstract] OR slips[Title/Abstract] OR slippery[Title/Abstract] OR trip [Title/Abstract] OR trips [Title/Abstract] OR fatal*[Title/Abstract] OR wounds and injuries[MeSH Terms] #2 safety behaviour[Text Word]) OR safety behavior[Text Word]) OR risk behaviour[Text Word]) OR risk behavior[Text Word] #3 risk-taking [MeSH Terms] #4 #2 OR #3 #5 #1 OR #4 #6 accidental falls[MeSH Terms] OR injuries[MeSH Subheading] #7 occupational[Text Word] OR work[Text Word] OR workplace[MeSH Terms] OR workplace OR work place OR worksite OR work site #8 accidents, occupational[MeSH Terms] #9 #6 AND #7 #10 #5 AND #7 #11 #8 OR #9 OR #10 - OUTCOME #12 safety[MeSH Terms] OR safety management[MeSH Terms] OR prevention and control[MeSH Subheading] OR safet*[Text Word] OR prevent*[Text Word] OR control*[Text Word] OR risk[Title/Abstract] OR risks[Title/Abstract] OR risk[MeSH Terms] OR risk management[MeSH Terms] OR accident prevention[MeSH Terms] OR hazard[Text Word] OR hazards[Text Word] OR hazardous[Text Word] – INTERVENTION #13 #11 AND #12 – OUTCOME + INTERVENTION #14 randomized controlled trial[pt] OR randomized controlled trials[mh] OR random allocation[mh] OR double-blind method[mh] OR single-blind method[mh] OR clinical trial[pt] OR clinical trials[mh] OR “clinical trial”[tw] OR ((singl*[tw] OR doubl*[tw] OR trebl*[tw] OR tripl*[tw]) AND (mask*[tw] OR blind*[tw])) OR “latin square“[tw] OR placebos[mh] OR placebo*[tw] OR random*[tw] OR quasi*[tiab] OR research design[mh:noexp] OR comparative study[pt] OR evaluation studies[pt] OR follow-up studies[mh] OR prospective studies[mh] OR retrospective studies[MeSH Terms] OR interrupted time series[Text Word] OR group[Text Word] OR groups[Text Word]OR control[tw] OR controll*[tiab] OR prospectiv*[tw] OR retrospective*[Text Word] OR before-after OR pre-post OR pre-test OR post test OR volunteer*[tw]) NOT (animal[mh] NOT human[mh])) - STUDY DESIGN #15 #13 AND #14 – OUTCOME + INTERVENTION + STUDY DESIGN #16 #15 Limits: Review #17 #15 NOT #16 – OUTCOME + INTERVENTION + STUDY DESIGN, NOT REVIEWS
The retrieved reviews in the searches will be kept in a separate database for further search of relevant studies. This database will be screened for relevant reviews, and relevant studies will be selected from the reviews, following the procedure described in 3.3.1.
3.2.3 Searching other resources
Literature searching in the field of occupational injury cannot be limited to database searches, as much of the literature is not well-indexed. We will therefore use supplementary search methods to capture relevant literature in the field.
We will use the Google (www.google.com) search engine with selected terms from the above strategy to search the grey literature and to attempt to identify further unpublished studies. The first 100 hits of the Google search will be included. We will also examine the reference lists in any relevant review we identify. We will not conduct hand searches but will instead search the OSH ROM, which covers a wide range of publications, including grey literature.
Reference lists of included studies will be examined to identify further relevant studies.
Personal contacts with international experts will be made in attempt to identify any studies that have not been captured by other search procedures or which are unpublished.
3.3 DATA COLLECTION AND ANALYSIS
3.3.1 Selection of studies
Literature screening will be done at three levels (on the basis of title, abstract, and full text). At the first level, pairs of reviewers (JDY, KBF, ADZ, PKI, KNI and KRA) will independently read titles of reports and articles identified in the search to exclude reports that are clearly irrelevant. A report will only move on to the second screening level if the answer is yes or uncertain to the question of whether or not the study reports on accidents at work.
At the second screening level, reviewers in pairs (PKI, JDY, KNI, ADZ, NNH, KBF and KRA) will independently evaluate the report on the basis of the abstract. Uncertain reports from level one will be evaluated again on the basis of the abstract and only retained if they are about accidents at work. At the second level the eligibility inclusion criteria are extended, and a report will only move on to the third level of screening if the answer is yes or uncertain to the question of whether or not the study evaluates a safety intervention aimed at preventing accidents at work.
At the third screening level, studies will be evaluated on the basis of the full text by reviewers in pairs (KNI, KRA, HJL, FWG, JLU, MTÖ, KJM, DZO, PKI and JDY). Uncertain reports from level two will be evaluated again on the basis of the full text, and only retained if it is about the evaluation of a safety intervention at work. At the third level the eligibility inclusion criteria are extended to the following; the study meets the study design inclusion criteria (see section 1.3 and 11.3, Q20 Guidance box). Primary investigators will be contacted (if possible) to clarify study eligibility if necessary.
In the event of disagreements, a third reviewer and content specialist (KNI, KRA, HJL, FWG, JLU, MTÖ, KJM, DZO and PKI) will be consulted and consensus will be sought. Exclusion reasons for studies that otherwise might be expected to be eligible will be documented and presented in an appendix. The overall search and screening process will be illustrated in a flow-diagram (chapter 13). Kappa scores will be reported to check inter-rater reliability.
The inclusion coding questions for level 1, 2 and 3 screening will be piloted and adjusted if required (see Appendix 12.2).
3.3.2 Data extraction and management
Pairs of reviewers (HJL, FWG, JLU, MTÖ, KRA, KNI, DZO, OOL and PKI) will independently code and extract data from the included studies. A data extraction sheet will be piloted on several studies and revised as necessary.. Extracted data will be stored electronically. Disagreements will be resolved by consulting an independent reviewer with extensive content and methods expertise (HJL, DZO, OOL and JDY). Data and information will be extracted on: type of industry (NACE), type of work settings, the characteristics of participants (age, gender, other), types of intervention component included (by use of classification), fidelity of intervention, control conditions, research design, risk of bias and potential confounding factors, outcomes and results (see overview in appendix 12.4).
3.3.3 Assessment of risk of bias in included studies
We will assess the methodological quality of RCTs using the risk of bias model in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, 2008). The risk of bias model's point of departure is RCTs, and will therefore be adapted to accommodate confounding factors associated with non-randomised study designs included in this review. With non-randomised studies, we will pay particular attention to selection bias, baseline differences between groups, and the potential for selective outcome reporting (Higgins & Green, 2008, p. 395). If the details provided are insufficient for a judgement on risk of bias to be made, we will contact the study authors for further information.
Risk of bias assessment will be based on five dimensions (described below). The assessment questions with a rating of low risk, high risk, and uncertain risk of bias, will be piloted and modified (see risk of bias table in appendix 12). Pairs of review authors (HJL, JLU, MTO, KRA, OOL, PKI and JDY) will independently assess the risk of bias for each of the included studies. Disagreements will be resolved by a third reviewer with content and/or statistical expertise (KNI, HJL and JDY). We will report the risk of bias assessment for each study included. This assessment will also inform sensitivity analysis (see 3.4.2 Sensitivity analysis).
Risk of Bias dimensions:
Selection bias is understood as systematic baseline differences between groups (i.e. observable factors are not adequately accounted for) and can therefore compromise comparability between groups. Selection bias applies to all types of designs, including RCT, but the risk of selection bias is considered to be higher in non-randomised study (NRS) designs. For each study we will assess (i) whether possible differences between intervention and control groups were accounted for, and (ii) whether it was done appropriately.
Performance bias refers to systematic bias and confounding related to intervention fidelity and/or influence from components, other than the components related to the interventions and comparisons of interest, which may confound outcome results. The fidelity of the intervention and influence from contextual factors will be evaluated for all studies, e.g., whether the degree of implementation performance is measured and evaluated by the authors (Robson et al., 2001; Kristensen, 2005), and whether the possible influence of contextual factors have been accounted for.
Detection bias is concerned with systematic differences between groups in relation to how outcomes are determined, including blinding of outcome assessors. A particular concern in safety intervention evaluation is changes in reporting of accidents over time, as well as differences in reporting propensity between groups. For example, if an intervention raises the awareness of safety activities during the intervention period, this could increase the propensity of employees to report accidents. Another important detection bias is the regression-to-the-mean in cases representing unusually high rates of accidents in either the intervention or control units.
Attrition bias concerns the completeness of sample and follow-up data. This bias refers to systematic differences between drops outs and completers from a study. Safety intervention studies often require companies, groups or members of an organisation to change the way they usually work, and therefore put a burden on the participants, which can result in them dropping out, and hence change the characteristics of the intervention group. Restructuring and closing downs of units may also result in changing characteristics of the intervention groups, and if these characteristics are related to the outcome of interest, then the effect will be biased. For each study, we will also assess whether attrition bias has been evaluated and taken appropriately into account.
Reporting bias refers to both publication bias (see 3.3.8 Assessment of publication bias) and selective reporting of outcome data and results. There can be differences in reporting of severe and less severe accidents, and thus it is important to consider whether changes are real or due to differences in severity of accidents, when using non randomized control groups. If we suspect reporting bias, we plan to contact the study authors, asking them to provide missing outcome data. Where this is not possible, and the missing data are thought to introduce serious bias, we plan not to include the outcome data from the particular study.
We will examine for other potential sources of bias focussing on whether study authors have reported such potential sources or confounding factors, and how they have dealt with them.
There are some common confounding factors in safety intervention studies that we particularly will take into account in the assessment of the studies (Robson et al., 2001). History can be a confounding factor when other events than the intervention occur which could affect the outcome in focus of the study. Studies with longer follow-up times will have an increased risk of confounding related to history events, and history threats are particularly a risk in simple before and after studies. The process of deploying a measuring instrument may also have an effect on the outcome, such as the use of a baseline questionnaire raises awareness and changes attitudes or safety practices.
The “placebo effect”, known from clinical studies, is also relevant for safety interventions, if participants already have a definite view on the successfulness of the intervention component(s), and this may have an effect on the outcome independent of the effect of the intervention itself. Similarly, the “Hawthorne effect” refers to an effect of the involvement of researchers upon the outcome measures, independent of the effect of the components of the safety intervention. Finally, “maturation effect”, refers to cases where the apparent effect of a safety intervention could be influenced by the intervention group developing naturally during the study period, such as improved knowledge about and experience with hazards and safety precautions. There are a number of approaches available to deal with known confounding factors in safety interventions (Robson et al., 2001), and we will assess how authors have dealt with these confounding factors.
We will also consider the effects of any industrial sponsorship or funding on impartiality and outcomes as a possible source of bias.
3.3.4 Measures of the effect of safety interventions
The effects of safety interventions can be measured by using inherently dichotomous outcome data, such as having an accident or not having an accident. The effect measures are most likely injury rates. However, proxy outcome measures for accidental injuries, such as changes in safety behaviour and /or changes in more proximal risk factors are also accepted. The review will include the obvious relevant effect measures, such as rate (or risk) ratios (RR) or rate (or risk) differences (RD) that are used to compare injury rates among those exposed to the intervention and those who were not. These effect measures may compare the same population in different periods of time (before and after the intervention) or different populations (exposed vs not exposed). Odds ratio (OR) is another effect measure often used in this research field, which is the ratio of the probability of a particular event will occur to the probability that it will not occur. It is possible that investigators may report the odds of injury among populations who received an intervention compared to those who did not, as odds ratios (ORs). Time-to-event (survival data) measures are entirely appropriate and are often incorporated in incidence density measures using person-time in the rate denominator. Reported effect measures will be plotted as point estimates, or described in more explicit detail where appropriate.
Sometimes measures can be established from a scale, e.g., safety climate, which can take any value in a specified range, and thus provide inherently continuous data. Basically, two types of summary statistics are available for meta-analysis, of continuous data: the mean difference and the standardized mean difference for different scales (Higgins & Green, 2008). Continuous outcome data will be converted into standardized mean differences (SMDs) with 95% confidence intervals. If means and standard deviations were not available, we will use the methods suggested by Lipsey and Wilson (2001) to calculate SMDs from e.g. F-ratios, t-values, chi-squared values and correlation coefficients. Differences in sample size will be taken into account by using Hedges' (adjusted) ‘g’ (inverse variance weight). Also the direction of a scale or other type of measure will be adjusted for, e.g., multiply the mean values from one set of studies by ‘–1‘.
3.3.5 Unit of analysis issues
We will take into account the unit of analysis of the studies to determine whether individuals or groups were randomised (i.e. cluster randomised trials), whether individuals may have undergone multiple interventions simultaneously, whether results were reported at multiple time points, and whether there were multiple treatment groups. It is common in the safety science field that interventions are directed at the workplace or organizational level. Studies with organization level outcomes will be pooled separately from individual level outcomes.
Cluster randomization
In cluster randomisation statistical analysis errors can occur when the unit of allocation (e.g. workplace) is different from the unit of analysis (e.g. employees). In studies where the error of clustering is taken into account, effect estimates and their standard errors will used. If the clustering effect has not been controlled for, we will request individual participant data to calculate an estimate of the intra-cluster correlation coefficient (ICC). If that is not available, we will obtain external estimates of the ICC from similar studies, and enter these data into RevMan to analyse effect sizes and confidence intervals using the generic inverse variance method (Higgins & Green, 2011: Section 16.3.3).
Multiple intervention groups and multiple interventions per individuals
Multiple intervention groups (with different individuals) within a study with one control group will be pooled if appropriate and compared to the one control group. Multiple control groups will only be pooled if appropriate, i.e., the multiple interventions and/or control groups does not include the same individuals. Also, if there is an overlap between multiple intervention groups, only one intervention group will be coded and compared to the control group to avoid overlapping samples. We will perform separate analyses if a treatment as usual or an alternative intervention comparison group includes one or more prevention program components.
3.3.6 Dealing with missing data and incomplete data
The level of missing data and the degree of attrition (dropouts) will be assessed for each of the included studies. In the case of missing data (e.g. Ns, means and standard deviations) the primary study authors will be contacted, if possible, and the missing data will be requested. Attrition rates and reasons for attrition will be recorded from the included studies; if information is not available authors will be contacted if possible. In the event that missing data cannot be provided, we will report and calculate the available data only; no imputation will be used
Information on intention to treat analysis (ITT) will also be recorded (see appendix risk of bias). In studies where ITT analysis was not used, the available data will be included in the meta-analysis if missing data can be assumed to be missing at random and/or will not affect results (Higgins & Green, 2008). Sensitivity analysis will be run to examine influences on the effects in these studies. Alternatively in cases where inadequate ITT analysis is used, and where missing data and dropouts are not judged to be missing at random, separate meta-analyses will be run.
3.3.7 Assessment of heterogeneity
Statistical heterogeneity in outcomes for studies included in the meta-analysis will be assessed visually (forest plots) along with the Chi-squared (Q) statistic and p-value, and the I-squared and τ-squared statistics (Higgins 2008). I2 computes approximately the proportion of variation due to heterogeneity rather than sampling error. Percentages over 75-80% may suggest heterogeneity concerns. However, as noted by Borenstein et al. (2009), an I2 of 90% or greater denotes “only that most of observed variation is real, but does not imply that the effects are dispersed over a wide range (they could fall in a narrow range, but be estimated precisely)”. Thus interpretation of I2 percentages will be applied with caution.
In case of heterogeneity, we will take the following steps: conduct a sensitivity analysis, in which methodologically weak trials are removed from the analyses and results compared for the primary outcomes; perform a visual inspection of the forest plots for evidence of inconsistency in results; and compare the results of fixed-effect and random-effects analyses
3.3.8 Assessment of publication bias
Meaningful funnel plots require an adequate number of studies with a diverse range of sample sizes (Hayashino et al., 2005; Glasziou et al., 2001). Funnel plots will be drawn and inspected if there are at least ten studies with appropriate data. We will assess funnel plot asymmetry visually, and use formal tests for funnel plot asymmetry. As the Cochrane Handbook currently states “….. it is not possible to make definitive recommendations on choice of tests for funnel plot asymmetry” (Higgins & Green, 2008, p. 10.17), we will consult the most recent version of the Handbook for advice when our data are ready for analyses. If asymmetry is detected in any tests or is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
3.4 DATA SYNTHESIS
A subset of studies from the review will be considered for more rigid meta-analyses and effect estimation, when appropriate criteria are met for the combining of data.
We will pool included studies depending on the availability of data and heterogeneity in relation to participants, interventions and outcomes. Due to the expected variation in types of safety prevention programs, and the combination of program components, we will use random effects models and will check for heterogeneity using the Q statistic and I2 with fixed effects to confirm this assumption. These expected variations will be explored in relation to influences on intervention effects where possible. Furthermore, we will only pool studies within each of the five main types of interventions, and only if content experts find this scientifically sound. RCTs and non-RCTs will be pooled separately, ITS studies will be analysed separately, and considered as supplementary data. Incongruent non-RCTs will also be pooled separately if necessary. Studies with a single group will be considered supplementary data and analysed separately from those with two-group designs.
Binary (dichotomous) outcomes will be analysed using relative risk ratio, odds ratio, risk difference. Time-to-event outcomes will be analysed using log hazard ratios. Confidence intervals of 95% for all individual study data will be calculated. For meta-analysis, the summarized intervention effect estimated across the relevant studies will be calculated as a weighted average of the intervention effects estimated in the individual studies (inverse-variance method and its variant the DerSimonian and Laird method (DerSimonian & Laird, 1986). The standard error of the summarized intervention effects is used to calculate the confidence intervals of 95% for the summarized intervention effect. For continuous outcome measures, the standardized mean difference is used as a summary ‘effect’, in cases where the studies all assess the same outcome, e.g., safety climate, but measure it in a variety of ways. If it is necessary to transform dichotomous effect sizes to SMD, we will use the methods suggested by Sáchez-Meca, Marín-Martínes, & Chacón-Moscoso (2003) which allow dichotomous and continuous data to be pooled together.
However, careful consideration will be made to evaluate if different measures of the same construct are conceptually congruent. If this is not the case, different measures for the one construct will be analysed separately.
If studies report multiple measures of the same construct at different points in time, separate meta- analysis will be conducted for the different measurement points. As mentioned previously, we will record the exact time points of follow–ups, and use this information to inform and document the choice of relevant and meaningful duration intervals for the analysis of outcomes.
Absolute versus relative effects will be analysed separately. Therefore, studies with control groups that are ‘no treatment’ or ‘wait list controls’ will be analysed separately from treatment as usual (TAU) and other interventions
Analysis will be conducted in the latest version of Revman and SAS.
3.4.1 Subgroup analysis, moderator analysis and investigation of heterogeneity
Subgroups analysis will be conducted where it is possible and relevant to explore possible influences on variation of treatment effect differences. Where possible, this will be explored in relation to the moderators listed in the table below.
3.4.2 Sensitivity analysis
Sensitivity analysis will be used to examine the rigour of conclusions in relation to the quality of data and approaches to analysis. Sensitivity analysis will be used to investigate possible study design influences on intervention effects. The influence of study quality will be examined by excluding low quality studies such as those not controlling for baseline differences, with high attrition, where ITT analysis was not carried out, and where there was no control for censoring effects.
3.4.3 Narrative analysis
To capture the main types of safety interventions and provide a sense of the research in the field of safety prevention, we plan to include a narrative analysis where appropriate. To make this presentation more transparent, we will report separately on studies that could not be combined in meta-analyses (before and after designs, for example), in a manner that will focus on intervention characteristics and contextual factors (Lehtola et al., 2008).
The narrative analysis will contribute to enhancing our understanding of safety prevention-programs and specific program components included in the review, and will inform the discussion section. The narrative will include a review of theoretical aspects of interventions, or the lack thereof, and reports of fidelity of interventions.
The approach taken will follow that of Best Evidence Synthesis as described by Petticrew & Roberts, 2006, and Slavin, 1995). This synthesis will thus be supplementary to the meta-analysis, and will focus in particular on those types of interventions not covered by the meta-analysis.
In this narrative analysis we will summarise information on whether the evaluation was conceptually framed around a theory (how it should work), and whether the fidelity of the intervention is known (why it works in practice) (Kristensen, 2005; Lipscomb et al., 2009). This is important in order to evaluate whether a lack of effect is due to a theory failure or an implementation failure, a distinction often neglected in systematic reviews.
Footnotes
5 Appendices
5.3 GUIDANCE FOR TYPES OF SAFETY INTERVENTIONS
1.1.0.: Attitude modification: attitudes are modified by means of information and persuasive messages in campaigns, leaflets, booklets, films, posters, direct mail, guidelines, or various counselling approaches etc. (Not specified) 1.1.1 Safety campaign, by use of various means (one way communication) 1.1.2 Counselling approaches (two way communication, including group discussions) 1.1.3 Teaching, education to increase knowledge and awareness (classroom, workplace etc. but not training (1.2.2) that is focusing on skills) 1.1.9 Other types of attitude modifications not listed above Excludes, e.g., skill training focused on behaviour change, coded under 1.2.2.
1.2.0.: Behaviour modification: behaviour is modified through various approaches, such as training, incentives, goal setting, feedback, individual coaching etc. (Not specified) 1.2.1 Individual goal setting (implicit, assigned, participative or self-assigned) 1.2.2 Safety training, and other types of training in order to improve skills, proficiency, dexterity, and other types of accomplishments (e.g., skill training, not just attitudinal changes) 1.2.3 Incentives (economic, benchmarking, safety bonus and other individual level incentives) 1.2.4 Individual feedback or safety coaching (e.g., face-to-face, and self-feedback, such as completion of a checklist) 1.2.9 Other types of behaviour modifications not listed above
2.1 Climate modifications: climate, social norms and culture, may be changed through leadership-based interventions, introduction or modification of safety management approaches, or by the influence of sectorial- or societal-level changes and modification aimed at changes at the place of work. (Not specified). 2.1.1 Goal setting at group or organisational level (implicit, assigned, participative or self-assigned) 2.1.2 Safety-coaching – teams, departments etc. (mainly employee directed) 2.1.3 Safety-coaching, leaders (top-leaders, middle management and nearest leaders) 2.1.4 Competitions (benchmarking, safety bonus and other group or organizational level incentives) 2.1.5 Safety feedback to work groups, leaders and workplace in general (e.g., face-to-face, public feedback, briefing at toolbox meetings, self-feedback, such as completion of a checklist) 2.1.6 Safety feedback to stakeholders, or other persons or groups outside the workplace who can influence workplace safety, e.g., the owner or client of a construction project (Types include face-to-face, public feedback, briefing, meetings, or other types of safety performance measurements) 2.1.9 Other types of climate modifications, not listed above
2.2 Structural modification: contextual factors are changed through legislation, regulation, enforcement and economics. This also refers to changes in the organization of safety management systems, the physical environment, engineering, i.e., modification of equipment and products, and implementation of rules and regulation, workers' rights and interests etc. (Not specified). 2.2.1 Legislative changes and enforcement 2.2.2 Economic incentives 2.2.3 Soft regulation (e.g., CSR, agreements between social partners or industry groups, benchmarking between companies etc.) 2.2.4 Engineering controls, such as design, availability and maintenance of technology (e.g., modifications in physical environment, engineering, modification of equipment and products, such as safety guards on machines, availability of lifting devices and the like), includes also elimination of risk factors (such as asbestos). 2.2.5 Administrative controls, such as introduction or modification of safety policies (e.g., new lifting policies), Safety Management Systems (e.g., ISO/OHSAS or other safety standards or guidelines), including modifications of monitoring, feedback & learning systems (e.g., procedures for incident, accident, dangerous situation reporting, audit systems, audit inspections etc.) 2.2.6 Employee participation or involvement is the introduction or modification of an environment in which people have an impact on decisions and actions that affect their jobs and their safety in these jobs. This include worker participation in the planning and selection of tools, procedures and goals, or by improving rights to participation in company decisions and to participation in e.g., Health and Safety boards, advisory committees etc. 2.2.9 Other types of structural modifications, not listed above
3.1 Combination of components at the individual level.
3.2 Combination of components at the group or organisational level
3.3 Combination of components across levels (individual and group/organisational level)
5.4 DATA EXTRACTION OVERVIEW
Random assignment Quasi-random assignment Other (describe) (comparison group / if time series then jump to #10.
Individual Stratified/blocked Match pairs Cluster randomisation Other (describe) Not clear
Computer generate Random numbers table Coin or dice Other Description unclear Not reported
One More than one (state number and specify)
One More than one (specify & explain)
Were participant inclusion/exclusion criteria mentioned? No Yes (describe) Participant or group characteristics. What is the level of analysis (individual/group/workplace/unit level)? _____________________
No Yes (describe differences) Unclear
No Yes (describe differences) Unclear
No Yes (describe) Unclear
Give a short description of the safety intervention Classify the safety intervention by use of the classification in section 12.3
Not reported Total number of days Total number of weeks Total number of months Total number of years Not applicable
Not reported Describe activity, per hour Describe activity, per day Describe activity, per week Describe activity, per month Describe activity, per year Not applicable
None reported Description of methods: __________
Not mentioned Mentioned (specify & cite pg.#)
Yes (describe & cite pg#) No Can't tell
Treatment as usual (pg. # & describe) Alternative intervention (pg. # & describe) No intervention
state number: __
When was the first measurement after baseline (e.g., 12 weeks after baseline)? When was the last follow up data collected (e.g., 26 weeks after baseline)? Other
Yes (describe) No (specify differences) Can't tell
Yes (describe) No (specify differences) Can't tell
d. Yes, describe (describe) e. No (specify differences & pg. #) f. Can't tell
N's
Safety intervention group
Control group
TOTAL
Pg. # & NOTES
Completed baseline measures
Randomly assigned Or non-randomly allocated
Completed first measure after
baseline
Completed 1st follow-up (add rows as required for additional follow-ups)
* add columns for additional intervention and control/comparison groups.
SAFETY INTERVENTION
CONTROL Group
TOTAL
Pg. # & NOTES
Gender (e.g. % male)
Age (e.g. mean)
Branch (economic activity, NACE, level 1)
Occupation (ISCO 88, level 1)
Lone workers or not (yes or no)
Type of setting (code – see section 3.4.1)
Size of enterprise (use size bands in section 3.4.1)
Other characteristics
• Add columns for additional intervention and control/comparison groups.
Id no.:
Author:
Year:
Outcome
Outcome measurement
Reliability & Validity
Format
Direction
Source (specify)
Blinding (outcome assessors)
Pg. # & notes
(input from protocol)
(specify)
Specify
Describe measurement
Dichotomous
Event OR
Yes
Continuous
High score is
No
Positive
Can't tell
Negative
Can't tell
Id no.:
Author:
Year:
OUTCOME
TIME POINT (record exact time taken from baseline)
SOURCE
VALID Ns
N W/EVENT
% WITH EVENT
STATISTICS
Pg. # & NOTES
(specify)
specify
• 1st measure after baseline
Log hazard ratio
• 1st follow-up
Log rank ration
• 2nd follow-up
Risk ratio
• 3rd follow-up
OR
• 4th follow-up
Safety Int.
Safety Int.
Safety Int.
95% CI
• Other
DF
P- value
Mantel-Haenszel
Chi2
Other
Covariates (control variables)
Comparison
Comparison
Comparison
Id no.:
Author:
Year:
TIME POINT (record exact time taken from baseline)
SOURCE
VALID Ns
Means
SDs
STATISTICS
Pg. # & NOTES
OUTCOME
(specify)
Specify
• 1st measure after baseline
P
• 1st follow-up
t
• 2nd follow-up
Safety Int.
Safety Int.
Safety Int.
F
• 3rd follow-up
Df
• 4th follow-up
ES
• Other
Other
Covariates
Comparison
Comparison
Comparison
5.5 RISK OF BIAS TABLE
| Dimensions | Domains | Description | Reviewer author's decision |
|---|---|---|---|
| Selection Sample bias | Sequence generation | Describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups. |
Was the random sequence generation adequate? (In the case of cluster randomised studies with small numbers, was stratified or pair-matched randomisation used to generate cluster randomisation?) Yes No Unclear |
| Allocation concealment | Describe the method used to conceal the allocation sequence in sufficient detail to determine whether the intervention allocations could have been foreseen in advance of, or during, enrolment. |
Was allocation adequately concealed? (For cluster RCTs - were individuals recruited prior to cluster randomisation (if not, was the cluster adequately concealed prior to concealment)? Yes No Unclear |
|
| Equivalent groups | Describe baselines differences between intervention and comparison groups. |
Were baselines reported, checked and cases of imbalances adequately controlled for? Yes No Unclear |
|
| Performance bias | Intervention fidelity and/or exposure to other confounding factors | Describe measures taken to secure intervention fidelity and/or exposure to other factors besides the intervention and comparison that may confound the results (or that a control comparison received the intervention). |
Do the study reports deal with intervention fidelity, or account for other confounding factors? Yes No Unclear |
| Detection bias | Blinding of outcome assessors (Assessments for each main outcome or class of outcomes). | Describe if outcome assessors were blinded, or if outcome assessors had vested interests. |
Was knowledge of the allocated intervention adequately prevented during the study? Outcome assessors were not blinded but the review authors judge that the outcome was not likely to be influenced by lack of blinding. Yes No Unclear |
| Statistical analysis (Assessment for outcomes using time to event data) |
Censoring (also related to attrition bias — see below) Describes measures taken to account for censoring in time-to-event data. Cluster and unit of analysis issues. |
Censored data reported and adequately accounted for (i.e. censoring unlikely to introduce bias?) (For cluster RCTs, were appropriate methods used to account for clustering?) Yes No Unclear |
|
| Attrition bias | Incomplete outcome data (Assessments for each main outcome or class of outcomes). | Describe the completeness of the sample and follow data for each main outcome, including whether attrition and exclusions were reported /and reasons given), and if any re-inclusions in analyses performed by the review authors, including the use of ITT. |
Were incomplete outcome data adequately accounted for? (For cluster RCTs, were all clusters included in the outcome data and analysis?) Yes No Unclear |
| Reporting bias |
Selective reporting of outcome and results (Assessments for each main outcome or class of outcomes) . |
If possible check that pre-specified primary outcomes have been reported. |
Are reports of the study free of suggestion of selective outcome reporting? Yes No Unclear |
| Other sources of bias | Other potential sources of bias. | Describe whether study authors have reported additional concerns regarding other potential sources of bias, such as history, placebo effect, industrial sponsorship etc., and whether they were adequately accounted for. |
Was the study apparently free of other problems that could put it at high risk of bias? Yes No Unclear |
6 Contribution of authors
Who is responsible for the below areas? Please list their names: Content: JDY, PKI, HJL, KJM, MTÖ, FWG, KNI, KRA, JLU, DZO Systematic review methods: JLU, JDY, OOL, HJL, KRA, DZO Statistical analysis: OOL, HJL, KNI, DZO Information retrieval: JDY, ELB and PKI
7 Declarations of interest
None known.