
Abstract
BACKGROUND
The Problem
As of December 2002, 19.2 million women were living with HIV/ AIDS, nearly double the 1997 figure of 12.2 million infected women (UNAIDS 2002; UNAIDS 1998). The majority of infected women are of child-bearing age with the bulk of new infections occurring among adults under the age of 25 (UNAIDS 2001). It is increasingly recognized that gender inequality, in all its forms, it largely responsible for the rapid spread of HIV/AIDS throughout the world (UNIFEM 2001). The factors that increase women's vulnerability to HIV infection can be categorized into two main areas; physiological factors, and social, economic and political factors. In terms of sexual transmission of the virus, heterosexual women's increased physiological vulnerability to HIV is due to the sensitive nature of the mucosal lining of the vagina and cervix, its large surface area and the large concentrations of HIV virus present in infected male semen (as compared to female secretions). These factors combine to make unprotected heterosexual intercourse the leading source of HIV infection for women worldwide. Undiagnosed or asymptomatic sexually transmitted infections, which are common among women, also increase the chances of HIV infection. In addition to this physiological vulnerability, sociocultural factors interplay to create a reality that places women at increased risk. Gender inequity, economic vulnerability and cultural practices and norms that favor male sexuality and power create an environment where women have little choice and power to negotiate safer sexual practices. These factors intertwine in women's lives to not only increase their susceptibility to HIV infection but also to create barriers to effective care and support.
The aim of this systematic review is to assess the effectiveness of peer-based interventions to improve the health and well-being of women with HIV. A secondary objective is to assess whether peer-based interventions decrease health inequalities between advantaged and disadvantaged groups.
The Intervention
Interventions that involve contact with an individual or group of peers (paid or voluntary) offering support, education or counselling that is intended to influence one of the health related outcomes.
Types of Interventions: One-on- one counselling and a peer group: is defined as a counselor/social worker giving one-on-one advice to the participant, and the participates involved in discussion groups with their following peers. Example, one-on-one counselling where psycho-educational content is the focus, one on one counselling might also address issues related to sexual abuse, ability to disclosure HIV status and drug use. Peer-led support groups: is defined as a peer who also is a female that is HIV positive and is leading the peer group with HIV positive females. Example, a peer mentor leader who is also an HIV positive female, is assigned a group of HIV-positive women. Professional-led support groups: is defined as a health professional who is leading a peer group with HIV positive females. Example, a healthcare worker, community care worker, nurse or doctor who leading the discussion group with women who are HIV positive Peer-based discussion groups: is defined as HIV-positive female participants partaking in a discussion with other HIV positive status. Example, a structured psychosocial support group intervention, tailored to meet the specific needs of pregnant women.
How the Intervention Might Work
Peer-based interventions have the potential to enhance health equity for women with HIV/AIDS by improving accessibility, acceptability and affordability of counselling and support (i.e. emotional, instrumental or informational) and may facilitate access to other treatment services. These interventions may help reduce feelings of isolation and stigma by providing social support (Sartore 2013). Moreover, in areas of the world where HIV is delaying progress towards gender equity, these types of interventions may be essential in imparting skills of self-efficacy and confidence among women and encouraging community advocacy and mobilization around issues of HIV/AIDS. See our logic model (Figure 1).
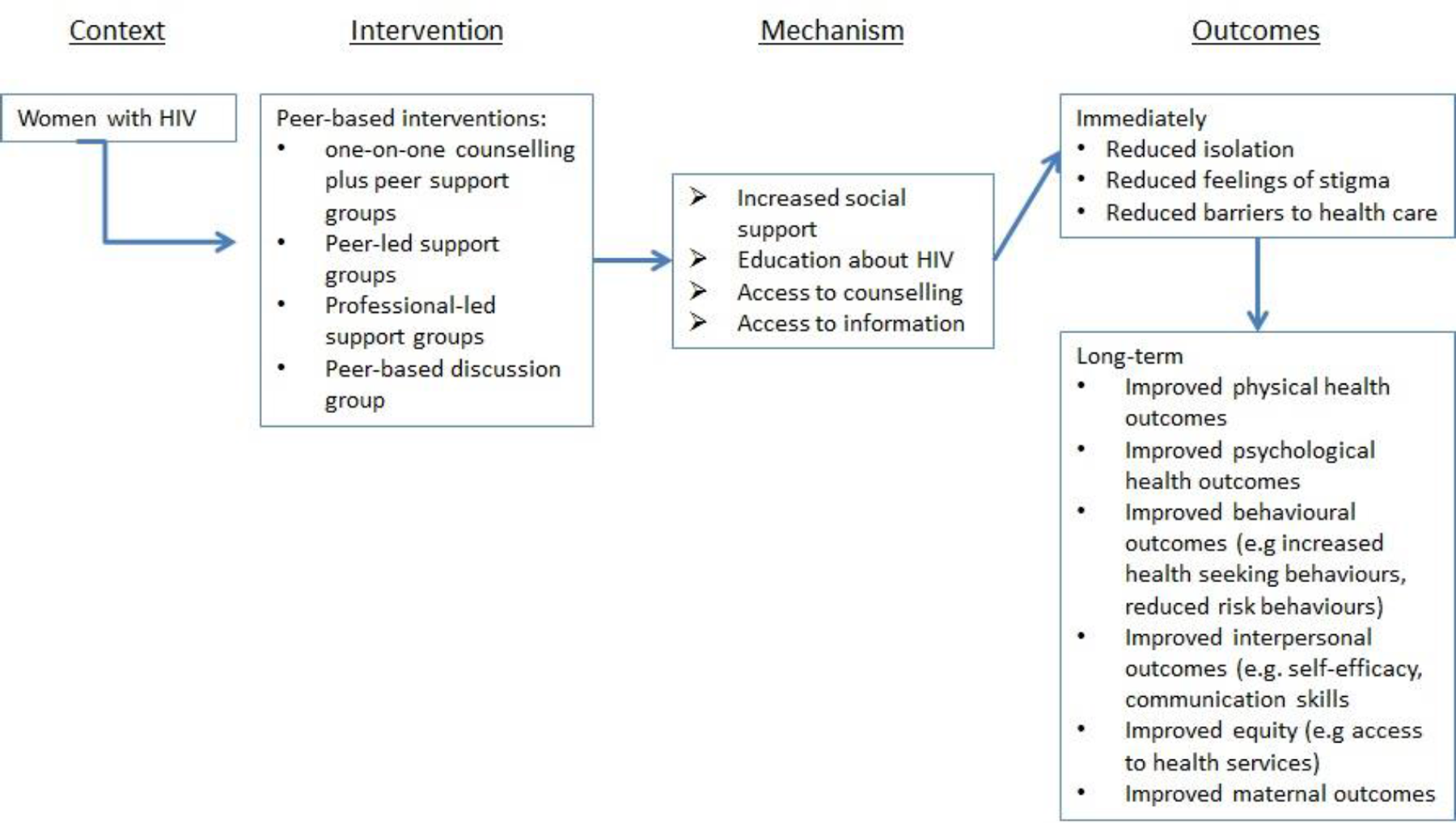
Logic model for peer-based interventions for HIV-positive women
Why it is Important to do the Review
HIV positive women have distinct need for support, education and counselling. Peer to peer interactions are one way to deliver a support framework. Women are often the central caregivers in the family and cope with unique stressors and responsibilities. They have lower economic status and fewer resources. These factors create barriers to treatment, care and support. The rise in HIV infections in women necessitates urgent investigation into their psychological and social support needs and the interventions that are designed to address them.
The contribution of this review
To the best of our knowledge, this is the first systematic review to assess how peer-based interventions reduce the morbidity and mortality in HIV-positive women. Previous reviews exist that examine the efficacy of various interventions for ‘at-risk’ women but no systematic reviews were located that examine this question for women already infected with HIV. The results of this review will inform researchers and policy makers if peer-based interventions are effective in reducing the health outcomes mentioned in this review. This review will help policy makers make decisions with the best possible evidence.
OBJECTIVES
To examine the literature and evidence surrounding peer-based interventions for HIV positive women to determine: The effectiveness of these strategies in improving the physical, mental and psychosocial health of women. Whether these strategies decrease health inequalities between advantaged and disadvantaged groups. We will use the PROGRESS acronym to identify characteristics that may contribute to disadvantage (see outcomes for further definition).
METHODOLOGY
Characteristics of studies relevant to the objectives of the review
Criteria for inclusion and exclusion of studies in the review
Interventions
Interventions that involve contact with an individual or group of peers (paid or voluntary) offering support, education or counselling that is intended to influence one of the outcomes listed below. Interventions led or facilitated by a professional (or non-peer) will be included providing the focus of the intervention is to provide peer-to-peer interaction and it can be determined that the professional maintains a secondary role. Information on the characteristics or roles of the intervention facilitators will be taken from the study publication if available or if necessary contact with the study authors will be made to clarify this information. For the purposes of this review a peer will be defined as: an individual who shares common characteristics with the ‘targeted’ group or individual allowing her to relate to, and empathize with, that individual on a level that a non-peer would not be able to do. Common characteristics required would vary in different contexts but should include: age, gender, sexual orientation, socioeconomic status, religion, ethnicity, place of residence, culture, education and value system. For the purposes of this review individuals do not have to be HIV positive in order to meet the definition of peer presented here. It is felt that in many cases women may share a multitude of risk factors and personal histories that will allow them to effectively relate to one another and be considered as ‘peers’ without having to share infection status. However, we will perform a sub-group analysis for those studies that used HIV-positive versus HIV-negative peer leaders.
Participants
Studies targeting HIV positive women in any setting (i.e. clinic, home, community, church) are eligible for inclusion. Studies targeting women ‘at-risk’ of HIV infection, but who are not currently infected, will be excluded. In order to address the second objective of this review we will aim to identify studies that include women from various demographic groups.
Outcomes
Studies reporting at least one of the following outcomes were included: Physical health outcomes: vertical HIV transmission (from mother to child), t-cell count, opportunistic infections, mortality, morbidity, progression to AIDS, pain. Psychological health outcomes: depression, self-esteem, confidence, well-being, quality of life, as assessed by standard scales such as the SF36. Behavioral outcomes: health seeking behaviors, adherence to treatment regimes, risk behaviors (i.e. unprotected sex, multiple partners, drug use), contraceptive decisions. Interpersonal outcomes: negotiation skills, self-efficacy, knowledge, attitudes. Equity outcomes: decreased inequalities in access to services, treatment and/or support, increased access for women identified as ‘disadvantaged’ across one or more of the PROGRESS factors. Maternal-related outcomes: coping, mother/child adjustment, disclosure to children, maternal self care practices and improvement in child health. Adverse effects caused by peer-based interventions
To assess effects of peer-based interventions on health inequalities, the effects of peer-based interventions across PROGRESS will be examined, if these are reported by the study authors. PROGRESS is an acronym used to identify characteristics which may contribute to disadvantage, including: Place of residence, Race/ethnicity/culture/language, Occupation, Gender/sex, Religion, Education, Socioeconomic status, and Social capital/resources (Evans 2003, O'Neill 2014).
Research methods/designs
We will include randomised controlled trials (RCTs), controlled before-after CBA (studies), and interrupted time series (ITS) studies. Those studies that do not include a control or comparison group will be excluded. Studies that include a control group that are qualitative in nature will also be included (see data analysis section for more detail).
Search strategy for finding eligible studies
The following search strategy will be used to search the following databases: MEDLINE, CINAHL, PSYCINFO, EMBASE, CENTRAL, AMED, Sociological Abstracts. Minor terminology changes will be made to suit the various databases. Search Strategy: exp hiv infections/ (hiv or aids).tw. acquired immun$ deficiency syndrome.tw. or/1-3 Female/ (wom#n or mother$).tw,sh. 5 or 6 4 and 7 peer group/ or social support/ (peer adj2 (support or education or counsel$ or lead$ or led or group)).tw. (social support or social group$ or support group$).tw. (peer based intervention$ or peer-based intervention$).tw. or/9-12 4 and 8 13 and 14 We will search relevant conferences for potentially eligible abstracts. Key stakeholders and contacts working in the field of HIV/AIDS will be contacted, including staff of government, non-government and academic organizations to identify community-based research or grey literature sources. The following organizations will be contacted: The Canadian International Development Agency (CIDA), Care Canada, Raks Thai Foundation (CARE Thailand), The International Development Research Council (IDRC, Canada), The Department for International Development (United Kingdom), World Health Organization, World Bank, Swedish Development Agency, International AIDS Alliance (India, Mozambique, Ukraine, Zambia, Washington offices), Global Network of People Living with HIV/AIDS (PLWHA), International Community of Women Living with HIV/AIDS, Population Council, United States Agency for International Development (USAID), ActionAID (United Kingdom), Prisoner's HIV/AIDS Support Action Network (PASAN, Canada), The Rockefeller Foundation.
Data extraction and study coding procedures
Data will be extracted independently in duplicate. The data abstraction forms will be based on the EPOC data collection forms, and modified to fit this review. Data will be extracted on: study design, description of the intervention, context of intervention (i.e. health facility, church-based, community, non-governmental organization, etc.), details about group leader (i.e. demographics, training, serostatus, professional etc.), details about participants (including number in each group, baseline health information), length of intervention and follow-up, definition of peer used, health outcomes, PROGRESS characteristics and data analysis. Consensus will be reached by discussion, when necessary. We will carefully describe the interventions given to both ‘experimental’ and ‘control‘ groups.
Risk of bias
The EPOC quality checklists for randomized controlled trials (RCTs), interrupted time series(ITS), controlled clinical trials (CCT), and controlled before-after studies (CBAs) will be used (EPOC 2002). These checklists account for study design, randomization method, appropriate selection of outcomes and statistical methods, confounding factors, method of data collection, and characteristics of control groups.
Synthesis procedures and statistical analysis
Treatment effects will be calculated for randomized controlled trials (RCTs) and controlled before-after studies (CBAs) separately. For continuous outcomes, where baseline data is available from randomized controlled trials (RCTs) and controlled before-after studies (CBAs), pre-intervention and post-intervention means or proportions will be reported for both study and control groups and the absolute change from baseline will be calculated (mean difference (MD) change in study group values minus change in control group values), along with 95 per cent confidence intervals. When baseline data is not available, results will be expressed as the relative percentage change (a difference between post-intervention values in the study and control groups expressed as a percentage of post-intervention values in the control group). For dichotomous outcomes, the relative risk (RR) of the outcome compared to the control group will be calculated.
When possible, studies with cluster allocation (e.g., cluster-randomized trials, cluster-allocated controlled before and after studies, and interrupted time series) that have errors in the unit of analysis will be adjusted using the variance inflation factor, as described in the Cochrane Handbook, if the required data can be obtained from the study authors. If not available, we will obtain ICC from other similar studies with similar outcomes if the ICC is not published.
Subgroup analysis and investigation of heterogeneity
We plan to assess effects of peer-based interventions on health inequities by conducting subgroup analyses across PROGRESS categories. PROGRESS identifies eight categories across which differences in health might be considered health inequities: Place of residence (e.g. low- and middle-income country/high-income country), Religion, Occupation, Gender, Race/ethnicity/culture, Education, Socioeconomic status and Social capital/resources (Evans 2003, O'Neill 2014).
Heterogeneity will be assessed by statistical tests for heterogeneity (I2 and chi-squared) as well as visual inspection of the forest plots.
Sensitivity analysis
If possible, we will investigate whether characteristics of the intervention or population mediate the effect using process evaluation and sensitivity analysis.
Footnotes
SOURCES OF SUPPORT
DECLARATIONS OF INTEREST
The authors have no competing interests to declare.
REVIEW AUTHORS
| Name: | Jennifer Petkovic |
| Title: | |
| Affiliation: | Centre for Global Health, Bruyere Research Institute, University of Ottawa |
| Address: | 43 Bruyère Street, Annex E room 302 |
| City, State, Province or County: | Ottawa, On |
| Postal Code: | K1N 5C8 |
| Country: | Canada |
|
|
Peter Tugwell |
| Title: | |
| Affiliation: | Bruyere Research Institute, University of Ottawa |
| Address: | 43 Bruyere Street, Annex E room 302 |
| City, State, Province or County: | Ottawa, On |
| Postal Code: | K1N5C8 |
| Country: | Canada |
| Email: |
|
ROLES AND RESPONSIBILITIES
Content: Annette O'Connor, Marion Doull, Vivian Welch Systematic review methods: Vivian Welch, Jennifer Petkovic, Marion Doull, Peter Tugwell, Jessica Aweya Statistical analysis: George Wells Information retrieval: Manosila Yoganathan
PRELIMINARY TIMEFRAME
Training and pilot testing on the inclusion criteria: Fall 2016
Searches for eligible studies: Fall 2016
Screening the results from the literature search: Fall 2016
Training and pilot testing the study coding procedure: Fall 2016
Extraction of data from eligible research reports: Fall 2016
Statistical analysis: Winter 2017
Preparation of the final review report: Winter 2017
PLANS FOR UPDATING THE REVIEW
The review will be updated every two years. JP will be responsible for leading the updates.
AUTHORS' RESPONSIBILITIES
By completing this form, you accept responsibility for preparing, maintaining, and updating the review in accordance with Campbell Collaboration policy. The Coordinating Group will provide as much support as possible to assist with the preparation of the review.
A draft protocol must be submitted to the Coordinating Group within one year of title acceptance. If drafts are not submitted before the agreed deadlines, or if we are unable to contact you for an extended period, the Coordinating Group has the right to de-register the title or transfer the title to alternative authors. The Coordinating Group also has the right to de-register or transfer the title if it does not meet the standards of the Coordinating Group and/or the Campbell Collaboration.
You accept responsibility for maintaining the review in light of new evidence, comments and criticisms, and other developments, and updating the review every five years, when substantial new evidence becomes available, or, if requested, transferring responsibility for maintaining the review to others as agreed with the Coordinating Group.
The support of the Coordinating Group in preparing your review is conditional upon your agreement to publish the protocol, finished review, and subsequent updates in the Campbell Library. The Campbell Collaboration places no restrictions on publication of the findings of a Campbell systematic review in a more abbreviated form as a journal article either before or after the publication of the monograph version in Campbell Systematic Reviews. Some journals, however, have restrictions that preclude publication of findings that have been, or will be, reported elsewhere and authors considering publication in such a journal should be aware of possible conflict with publication of the monograph version in Campbell Systematic Reviews. Publication in a journal after publication or in press status in Campbell Systematic Reviews should acknowledge the Campbell version and include a citation to it. Note that systematic reviews published in Campbell Systematic Reviews and co-registered with the Cochrane Collaboration may have additional requirements or restrictions for co-publication. Review authors accept responsibility for meeting any co-publication requirements.