
Abstract
BACKGROUND
The problem, condition or issue
Childhood trauma has been receiving increased attention and it is increasingly being recognized as a significant public health concern (Lang, Campbell, & Vanerploeg, 2015). Trauma exposure involves “actual or threatened death, serious injury, or sexual violence” that is either directly experienced or witnessed, or learning that any traumatic experiences have happened to a loved one, or having repeated exposure to details of traumatic events (APA, 2013, p. 271). Prevalence estimates of trauma experienced in childhood or adolescence vary by type of traumatic event (e.g., physical abuse, neglect, sexual abuse, witnessing violence, natural disasters) and how and when the traumatic experience is measured, but can range between 4% and 71% (Finkelhor et al., 2015; McLaughlin et al., 2013; Saunders & Adams, 2014). Exposure to traumatic events can disrupt brain development and can have immediate and lifelong adverse effects on social, emotional and physical wellbeing, including deficits executive functioning, developmental delays, behavioural health problems, difficulty regulating emotions and behaviour, academic performance and IQ, school behaviour problems, delinquency, substance abuse, and mental health and psychiatric disorders (Anda et al., 2006; Delaney-Black et al., 2002; DePrince et al., 2009; Flannery et el., 2004; Lang, Campbell, & Vanerploeg, 2015; Lansford et al., 2002). In a systematic review specifically examining school-related outcomes of traumatic event exposure, Perfect and colleagues (2016) identified 44 studies that examined cognitive functioning, 34 that examined academic functioning and 24 that examined social-emotional-behavioural functioning. Their findings suggest that youth who have experienced trauma are at significant risk for impairments across various cognitive functions, including IQ, memory, attention and language/verbal ability; poorer academic performance and school-related behaviours such as discipline, dropout and attendance; and higher rates of behavioural problems and internalizing symptoms.
Exposure to different types of trauma have been associated with varying types and complexity of adverse outcomes. Kira and colleagues’ (2012) study of African American and Iraqi refugee youth found that different types of trauma differentially impact different components of cognitive functioning, including perceptual reasoning, working memory, processing speed and verbal comprehension. In another study examining effects of different types of trauma, exposure to violence was found to be associated with depression, separation anxiety and conduct problems, whereas exposure to non-interpersonal traumatic events was associated with phobic anxiety (Briggs-Gowan et al., 2010). Moreover, there is some evidence that the effects of trauma are cumulative, thus youth who experience a greater number of traumatic events are more at risk for adverse outcomes and more complex symptoms through adulthood (Chartier et al., 2010; Cloitre et al.; Hodges et al., 2013). Duke and colleagues (2010) analyzed data from respondents to the 2007 Minnesota Student Survey (n = 136,549), and identified “a significant positive relationship between each adverse event and delinquent behaviors for girls and boys,” (p. e782). While exposure to traumatic or potentially traumatic experiences are associated with a range of short and long-term outcomes, there are multiple pathways through which trauma can impact various domains across the life course. Moreover, not all youth will experience the same traumatic events in the same way and not all youth will develop symptoms following a traumatic experience (Layne et al., 2009).
Given the growing research on trauma and increased knowledge about the prevalence, consequences and costs associated with trauma, there have been increased efforts at the local, state and federal levels to make systems “trauma-informed” (Lang, Campbell, & Vanerploeg, 2015). In an effort to examine the extent to which federal legislation has been proposed to advance trauma-informed practice, Purtle & Lewis (2017) conducted a policy mapping study of federal legislative proposals from 1973 to 2015 that explicitly mentioned trauma-informed practice. The authors identified 49 bills introduced, beginning in December 2009 with the Domestic Minor Sex Trafficking Deterrence and Victims Support Act, and observed a dramatic increase over time with 28 bills being introduced in 2015 alone. Altogether, the 49 bills contained 71 sections that included trauma-informed language, with the highest proportion of those specifically targeting youth in primary and secondary schools (16 sections, 22.5%). For example, the United States Congress established the National Child Traumatic Stress Network (NCTSN) in 2000 through a congressional initiative that is funded by the Substance Abuse and Mental Health Services Administration (SAMHSA). The NCTSN (n.d. a) is a growing network of providers, researchers, and families with a broad mission to improve care and access to services for traumatized children, their families, and communities. The NCTSN offers training, support, and resources aimed at treatment, intervention development, program evaluation, systems change, and the integration of trauma-informed and evidence-based practices in all child-serving systems. The Administration for Children and Families, Center for Medicare and Medicaid Services, the Department of Justice, and the Department of Education have also recognized the impact of child trauma on youth well-being and development and are launching initiatives and implementing policies designed to promote the use and expansion of trauma-informed systems and programs across child-serving organizations and agencies (Lang, Campbell and Vanderploeg, 2015; SAHMSA, 2014).
The promotion and provision of trauma-informed approaches in school settings is growing at a rapid rate across the United States. At least 17 states have been identified in which trauma-informed approaches have been implemented at the school, district, and even state-wide levels (Overstreet & Chafouleas, 2016). This rapid increase in the growth of trauma-informed approaches in schools has been fuelled by a number of local, state, and federal initiatives and increasing support by education related organizations. For example, there are explicit provisions for trauma-informed practices in the Every Student Succeeds Act (ESSA, 2015), the legislation that replaced No Child Left Behind, including training of school personnel in understanding when and how to refer students affected by trauma, and grant programs that provide funding to support services that are based on trauma-informed practices that are evidence-based (section 4108). The promotion of trauma-informed schools is also supported by the National Education Association and state-level agencies have been spearheading efforts to develop guidelines and implement change within and across school systems.
The intervention
Trauma-informed approaches are being promoted and used across child serving systems and constitute a relatively new approach to trauma care for children and youth being served within the child welfare, juvenile justice, mental health and education systems. While trauma-specific interventions, such as Trauma-Focused CBT, are well known and widely used to treat trauma-related symptoms and disorders in both adults and children, trauma-informed approaches to care are distinct from trauma-specific interventions. However, what is essential to a “trauma-informed approach” has not always been clearly operationalized, and the approach and variations of the approach have been referred to in varying ways, e.g. “trauma-informed care,” “trauma-sensitive,” “trauma-informed system” (Hanson & Lang, 2016). To date, there is no consensus on the use of these terms, which makes efforts to both implement and study trauma-informed approaches to care challenging.
While there is much confusion, overlap and misuse of the various terminologies in this rather nascent area of practice and research, we are drawing from SAMHSA and the NCTSN to define trauma-informed approaches for the purpose of this review. SAMHSA (2014) defines trauma-afformed approaches (which the agency uses interchangeably with “trauma-informed care”) as incorporating “key trauma principles into the organizational culture” of the program, agency, or system (p. 9). A trauma-informed approach is thus more akin to a multi-tiered framework such as School-Wide Positive Behavioral Supports (SWPBIS; Chafouleas et al., 2016), and is based on incorporating four key assumptions and six key principles, generalizable to any setting, that are infused across all levels of an organization rather than implementing a prescribed set of practices or interventions (SAMHSA, 2014; see Figure 1).
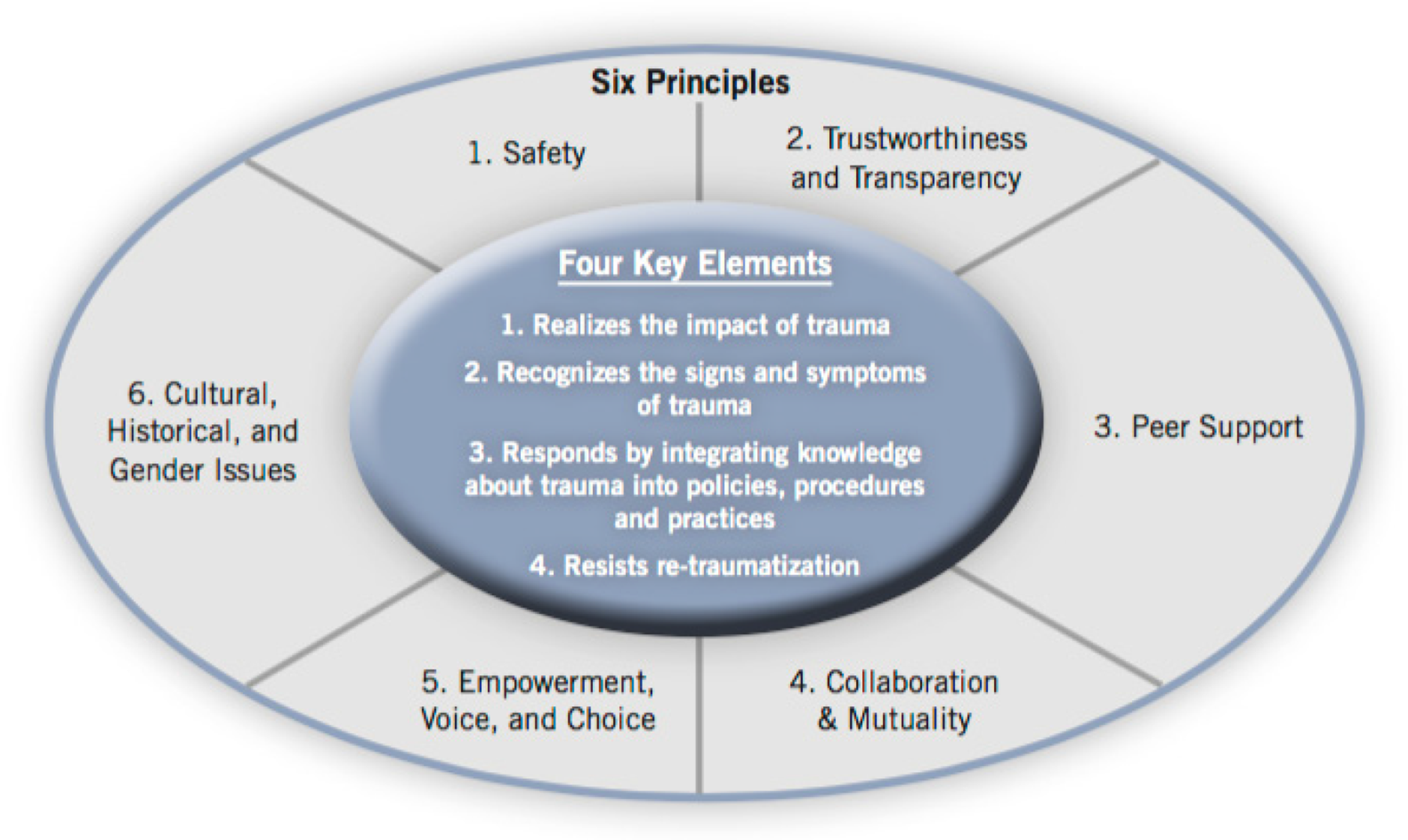
SAMHSA's trauma-informed approach (Lang et al., 2015)
A trauma-informed program, organization, or system is one that (SAMHSA, 2014, p. 9): Realizes the widespread impact of trauma an understands potential paths for recovery Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system. Responds by fully integrating knowledge about trauma into policies, procedures, and practices Seeks to actively resist re-traumatization of both persons served and staff
The six key principles of a trauma-informed approach include safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice and choice; and cultural, historical and gender issues (SAMHSA, 2014).
The NCTSN (n.d. b) adapts the model outlined by SAMHSA to a context specific to youth and families, and describes their model as a “trauma-informed child- and family-service system,” in which:
all parties involved recognize and respond to the impact of traumatic stress on those who have contact with the system, including children, caregivers, and service providers. Programs and agencies within such a system infuse and sustain trauma awareness, knowledge, and skills into their organizational cultures, practices, and policies. They act in collaboration with all those who are involved with the child, using the best available science, to facilitate and support the recovery and resiliency of the child and family.
In essence, a trauma-informed approach is not a standalone intervention that can be delivered in isolation, but rather a framework to guide systems. A trauma-informed approach can include trauma-specific interventions, but trauma-specific interventions alone are not seen as sufficient for achieving optimal outcomes or to influence service systems (SAMHSA, 2014). Hanson & Lang (2016) identify three core domains essential to trauma informed care that they derived from analysing definitions and components across several organizations and authors, including SAMHSA and NTCSN: (a) workforce/professional development, (b) organizational changes, and (c) practice changes.
Examples of trauma-informed approaches implemented in schools
As described above, trauma-informed approaches are complex interventions and involve a number of components at various levels, thus providing some examples of such programs can be helpful in elucidating this complexity. One example of a trauma-informed approach is the Healthy Environments and Response to Trauma in Schools (HEARTS) program that was implemented in elementary schools (K-8th grade) in the San Francisco Unified School District. HEARTS is a whole-school program developed by the University of California, San Francisco to promote school success for students who have been impacted by trauma (Dorado et al., 2016). This whole-school approach used the response to intervention three tier framework of universal, selected and targeted interventions and included supports at the system, adult (teacher/staff) and student levels at each tier. Activities involved changes in school policies and school-wide practices; training, professional development and consultation for all school staff around trauma-sensitive practices and stress, burnout and secondary trauma; and use of evidence-informed universal, secondary and targeted trauma-informed interventions.
Trauma-informed approaches are also used at the pre-school level. A multi-organization collaboration implemented a trauma-informed approach in head start programs in the Appalachian region of the US (Shamblin, Graham, & Bianco, 2016). This comprehensive, 3 tier model involved the use of trained consultants in the classroom to provide three tiers of services. The first tier was universal consultation, intended to build teacher capacity to deliver an evidence-based social-emotional curriculum (Second Steps or Incredible Years) to children and help teachers understand trauma-informed principles through training and mentoring of teachers. The second tier involved targeted consultation of teachers to develop behaviour plans and specific strategies to address challenging behaviours of individual children in the classroom which take into account the child's trauma experience. The third tier included the provision of intensive services wherein the consultant provided on-site mental health assessment and treatment to children and their families. For children who had experienced trauma, the consultant provided Trauma-Focused Cognitive Behaviour Therapy and/or Parent-Child Interaction Therapy. Additionally, the collaboration provided workforce development training to preschool teacher and other child service providers at various times during the year.
While schools may be implementing trauma-informed approaches, it is unclear to what extent or how much variation there is in what schools are implementing, how much emphasis they are putting on various components (e.g., workforce development versus organizational change versus practice changes) and whether schools may implement trauma-informed approaches differently based on the characteristics of their students, neighbourhood, country or other contextual factors.
How the intervention might work
One out of every four children attending school has been exposed to a traumatic event, which can impact school performance, impair learning, and cause physical and emotional distress (NCTSN, 2008). Moreover, the majority of youth who have experienced trauma do not receive services, and those who are exposed to a potentially traumatic event do not necessarily need an intervention (Layne et al., 2009). Due to the relatively high rates of youth exposed to traumatic events and the negative impacts of those traumatic experiences on academic achievement and life course outcomes, schools represent a natural system in which to help prevent and reduce the adverse effects of trauma and more effectively engage students in the learning process (Chafouleas, Johnson, Overstreet, & Santos, 2016). Trauma-informed schools adopt the trauma-informed approach to “create educational environments that are response to the needs of trauma-exposed youth through the implementation of effective practices and system-change strategies” (Overstreet & Chafouleas, 2015, p. 1). A trauma-informed approach in schools is designed to create a systematic model for schools to decrease the impact of trauma on students (Wiest-Stevenson & Lee, 2016) and more appropriately address academic, behavioral and socio-emotional problems by recognizing and responding to student behavior from a trauma-informed perspective. This is done through a multi-level approach intended to improve the school environment through implementing trauma-informed policies and procedures; increase the ability of school staff to recognize and more effectively respond to students through professional development; and prevent, mitigate and reduce trauma-associated symptoms through evidence-informed practices, leading to improved student academic, behavioral, and socio-emotional outcomes.
As described above, a trauma-informed approach involves strategies implemented at various levels in the school and includes workforce/professional development, organizational change, and practice change using evidence-informed practices (Hanson & Lang, 2016).
Workforce/Professional Development
The workforce and professional development component is intended to increase staff knowledge about the prevalence and effects of trauma and associated cognitive, behavioral and socio-emotional effects of trauma. In addition, PD is intended to increase staff's ability to recognize signs and symptoms of trauma and improve skills in appropriately responding to students exhibiting trauma symptoms so that staff can more effectively address student behavior and make appropriate referrals for more targeted services. For example, typical strategies school staff use when addressing disruptive behavior that focus on consequences for misbehavior can exacerbate problems with trauma victims and miss an opportunity to more effectively intervene. By being trained to use a trauma-informed lens, school staff can proactively prevent and deescalate problematic behaviors that would typically disrupt the classroom and student learning, improving the learning environment for the entire class, and positively impact students’ behavior, socioemotional and academic outcomes (Lang, Campbell, & Vanderploeg, 2015). Additionally, workforce development initiatives may also promote the recognition of and skills to cope with secondary stress and prevent burnout, which may occur in providers serving traumatized populations.
Organizational Environment and Practices
Schools may implement any of the following policies and procedures to realize organizational changes that maximize learning and reduce incidences of both traumatization and re-traumatization. Changes may include: modifying disciplinary practices, which contextualize the notion of “accountability” within an understanding of common reactions to trauma, minimize disruption in education, and model respectful relationships; establishing protocols for communication among caregivers, the school, and community agencies; modifications to the school's physical environment to promote safety; and, fostering partnerships with and linkages to community health and mental health resources (Cole et al., 2009).
Trauma-focused Practices
The practice change component to trauma-informed schools involves implementing screening and universal, selective and/or indicated intervention programs that incorporate knowledge about trauma and are evidence-informed. Schools may directly provide screening and intervention services in the school or collaborate with other providers to either implement programs and services in the school or refer students for screening and services in the community. Ideally, trauma-informed schools would provide screening and interventions at all levels either directly or indirectly; however, some schools may not have the resources to provide all levels of screening and intervention.
Why it is important to do the review
Although one could argue about the necessity or value of schools adopting a trauma-informed approach, trauma-informed approaches are being promoted and used across child serving systems, and the number of states and school districts adopting trauma-informed approaches in schools is growing rapidly (Overstreet & Chafouleas, 2016). While the intent of creating trauma-informed approaches in schools is a noble one, there is relatively little known about the benefits, costs, and how trauma-informed approaches are being defined and evaluated (Berliner & Kolko, 2016). Indeed, it is unclear whether schools adopting a trauma-informed approach (i.e., being a “trauma-informed school”) are effective in reducing trauma symptoms or affecting behavioural or academic outcomes, as the proponents of the movement propose. Adopting a trauma-informed approach in a complex system such as a school building or district is a time consuming and potentially costly endeavour and thus it is important to assess the effects of this approach to inform policy and practice. Also, from our cursory review of the literature, the description of the trauma-informed approaches being implemented in schools vary in terms of the types of strategies used in each of the three areas and the relative emphasis on the three areas (policy/procedures, professional development and practices), thus it is important to conduct a systematic inventory and description of the trauma-informed approaches implemented in schools to more fully understand how this approach is being utilized in schools, and whether variations in the components impact outcomes.
To date, we have not located any systematic reviews specifically examining effects of trauma-informed approaches in schools. We have identified reviews that have examined trauma-specific interventions for adolescents (e.g., Black, Woodworth, Tremblay & Carpenter, 2012; Cary & McMillen, 2012) and those that examine school-based interventions for specific trauma-related disorders, such as PTSD (e.g., Rolfsnes & Idsoe, 2011); however, these reviews are examining effects of trauma-specific interventions rather than trauma-informed approaches. By virtue of these studies’ primary research questions and inclusion criteria, the scope of these reviews were not designed to evaluate other domains of trauma-informed approaches (professional development and organizational changes) and thus cannot comprehensively inform decisions related to whether a trauma-informed approach is effective.
OBJECTIVES
This purpose of this review is to identify, describe and synthesize the evidence of effects of trauma-informed approaches in schools to provide guidance for policymakers and educators and to identify important gaps in the evidence base.
Specifically, the research questions guiding this review include: What evidence is available to examine the effectiveness of trauma-informed practices in schools? What are the study, intervention, and participant characteristics of studies that have rigorously evaluated the effects of trauma-informed schools? What are the components of trauma-informed approaches being used in schools? What are the effects of trauma-informed schools on trauma symptoms, socio-emotional outcomes, behavior, and academic outcomes? Are there certain components of trauma-informed approaches that are more effective than others? What adverse outcomes are reported by authors?
METHODOLOGY
Criteria for including and excluding studies
Types of study designs
To be included in this review, studies must use one of the following research designs: randomized controlled trial (RCT) or quasi-experimental design (QED). To be included in the review, studies must use a comparison group using a wait list control, no treatment, treatment-as-usual and alternative treatment control group, therefore single group pre-post test studies will be excluded. We will exclude studies in which the comparison group may receive a different type of intervention that would meet criteria as a trauma-informed approach (defined below), but will include studies in which comparison groups receive an alternative treatment that does not meet that criteria (e.g., a comparison group receiving a standalone trauma intervention would be included). The type of comparison group used in each study will be coded and examined as a moderator. Given the nascent nature of research in this area, we anticipate lower-quality quasi-experimental and experimental studies. Although higher quality designs will provide higher quality evidence, we are interested in capturing the research that currently exists and describing the quality of that research to inform research development in this area. Therefore, we will not require that studies provide pre-test data or make statistical adjustments; however, we will code study design and analysis elements and if there are sufficient number of studies, we will use design and analysis elements to conduct sensitivity and moderator analyses.
Types of participants
We will include studies that are examining effects of the intervention in a school setting serving preK-12 (or equivalent grade levels in other countries) students. We anticipate that studies may report effects at the individual or school level. We will include studies that measure outcomes at any level and will code and synthesize outcomes accordingly.
Types of interventions
SAMHSA (2014) defines a trauma-informed approach as a program, organization, or system that realizes the impact of trauma, recognizes the symptoms of trauma, responds by integrating knowledge about trauma policies and practices, and seeks to reduce re-traumatization. Three key elements of a trauma-informed approach include workforce development, trauma-focused services, and organizational environment and practices (Hanson & Lang, 2016). SAMHSA distinguishes between a trauma-informed approach from trauma-specific interventions, the latter which are specific interventions designed to treat or otherwise address the impact/symptoms of trauma and facilitate healing. We intend to examine the effects of trauma-informed approaches implemented in school settings, often referred to as trauma-informed schools.
We anticipate that there will be wide variation in the implementation of the trauma-informed approach used in schools and variability in the principles and practices adopted by schools. We believe that identifying and describing this variation will be a significant contribution to the literature as currently “trauma-informed schools” is often discussed as if everyone agrees on what this means or that any effort to become a “trauma-informed school” will be equally meaningful and effective.
Therefore, we want to be able to discern between studies examining trauma-specific interventions and those that are attempting a more comprehensive trauma-informed approach while not being overly limiting. Thus, for the purposes of this review, the intervention will be considered a trauma-informed school approach if at least two of the following three components are present: Workforce/professional development- components of the program are designed to increase knowledge and awareness of school staff on the impact, signs and symptoms of trauma, including secondary traumatization. Professional development does not necessarily have to be provided to all school staff in a school, but there must be some staff development component as part of the program. Organizational change- may include school-wide policies and procedures and/or strategies or practices intended to create a trauma-informed environment integrating the key principles of the trauma-informed approach. Practice change and use of evidence informed trauma practices- the program must implement changes in practice behaviours across the school, including trauma-specific screening, prevention and/or intervention services.
While including interventions that may only provide evidence of implementing two of the three components, we will be coding each of the components and will be able to describe whether studies included all three components, and if not, which components were included. If there are sufficient studies and variation between studies on this variable, we will examine whether the trauma-informed approach included all three components or not as a moderator.
Types of outcome measures
Primary Outcomes. Studies must report at least one of the following student-level outcomes: Trauma symptoms/mental health outcomes (e.g., anxiety, depression, post-traumatic stress disorder) Academic performance (e.g., standardized achievement tests, measures of content mastery, reading, grades) Behavior (e.g., disciplinary referrals, aggression and other externalizing behaviors, time on task, compliance, attendance[ND1]) Socio-emotional (e.g., stress, engagement, social skills, self-esteem, emotion regulation, grit)
Measurement of above outcomes may be conducted using standardized or unstandardized instruments and may be self-, parent-, or teacher-reported or researcher administered measures. To be included in the meta-analysis, primary study authors must report enough information to calculate an effect size. If sufficient information to calculate an effect size is not provided, every effort will be made to contact primary study authors and request the necessary information.
Secondary Outcomes.
We anticipate study authors will measure additional outcomes at different levels (individual, classroom, school) and will also report teacher outcomes and outcomes related to implementation (e.g., satisfaction, fidelity). We are also interested in reporting of adverse outcomes. For all outcomes that do not fit into one of the primary outcome categories as noted above, we will code the outcomes and categorize them post-hoc for descriptive purposes. If there are a sufficient number of studies reporting the same outcomes, we will extract effect size data and conduct a meta-analysis.
Duration of follow-up
We will include measurement points at post-test and all follow-up time points. We do not anticipate finding studies with long-term follow-up, but will code all time points for which sufficient data is available. We will synthesize studies that report similar follow-up time points (i.e., up to 3 months, 3-6 months, 6-12 months, > 12 months) if there are more than 2 studies that report sufficient data.
Types of settings
We will include studies of interventions conducted in a pre-school through 12th grade (or equivalent) school setting.
Other Criteria
We will not limit studies based on publication status, geographical location or language, although we may be limited in our ability to translate studies written in a language other than English. We will make every effort to translate non-English language reports and document those that we are unable to translate. We will search for studies that have been published in the last 10 years, as this is a relatively recent movement.
Procedures for applying inclusion criteria
One reviewer will conduct the initial search in all sources and will save the search results in an electronic format. At this stage, the reviewer will examine titles and abstracts and will discard results that are obviously ineligible (non-empirical report, book review, editorial, adult participants, prior to 2006 etc.). For those that are not obviously ineligible, the reviewer will retrieve the reports, save them in an electronic file, and document the bibliographic information, source, and date retrieved in a database. Two reviewers will then independently screen each of the reports for eligibility using a screening instrument (see Appendix A). The two reviewers will compare the coding and identify all discrepancies. The review team will discuss discrepancies and will resolve all discrepancies through consensus.
Search strategy
We propose to include all studies that meet the inclusion criteria outlined above. We will attempt to identify and retrieve both published and unpublished studies through a comprehensive search that includes multiple electronic databases, research registers, grey literature sources, and reference lists of reviews and relevant studies.
Electronic Databases
. Academic Search Complete . CBCA Education . Database of Research on International Education . Education Source . ERIC . MEDLINE . ProQuest Dissertations and Theses . PsycINFO . Social Science Citation Index . CINAHL
Research Registers and Websites
. Cochrane Collaboration Library . Database of Abstracts of Reviews of Effectiveness . National Technical Information Service . System for Information on Grey Literature . Evidence for Policy Practice Information and Coordinating Centre (EPPI-Centre)
Grey literature sources
. Social Science Research Network . Authors of prior studies will be contacted in an attempt to obtain unpublished studies, studies in process and published studies missed in the database search. . Conference abstracts and proceedings will be reviewed to identify potentially relevant studies. Conference searches will include: . The Society for Research on Educational Effectiveness (https://www.sree.org/pages/conferences/index.php) . American Educational Research Association Repository (http://www.aera.net/EventsMeetings/tabid/10063/Default.aspx.) . Society for Research on Child Development (SCRD) . Society for Research on Adolescence (SRA) . International Society for Traumatic Stress Studies (https://www.istss.org/) . Tampa Children's Mental Health Research and Policy Conference . Clearinghouses, research centers and disciplinary and government websites will be reviewed to identify potential sources of relevant studies: . The US Department of Education's web site contains reports of funded programs and initiatives: http://www2.ed.gov/about/offices/list/opepd/ppss/reports.html
. The Institution of Education Sciences, What Works Clearinghouse contains reports of intervention investigations: http://ies.ed.gov/funding/grantsearch/index.asp
. Trauma and Learning Policy Initiative: traumasensitiveschools.org . National Child Traumatic Stress Network: . American Public Health Association . Association for Psychological Science . American Psychological Association . International Society for Traumatic Stress Studies The reference lists from prior reviews and included studies will be reviewed for potential studies. We will also conduct forward citation searching using Google Scholar to search for studies citing included studies.
Search terms and keywords
We will use combinations of terms related to the intervention, population, study design, and setting to search the electronic databases. Database-specific strategies will be explored for each database, including the use of truncation and database-specific limiters and thesauri will be consulted to employ more precise search strategies within each database. Below are examples of the types of terms we anticipate using: Intervention/condition: trauma-informed OR trauma-sensitive OR “trauma services” OR trauma OR PTSD OR “post-traumatic stress disorder” AND Targeted population: “elementary school” OR “primary school” OR “high school” OR “secondary school” OR “middle school” OR kindergarten OR pre-kindergarten OR child* OR youth OR adolescent OR school Report type: evaluation OR intervention OR treatment OR outcome OR program OR trial OR experiment OR “control group” OR “controlled trial” OR quasi-experiment” OR random*
Data extraction and study coding procedures
For all studies that pass the eligibility screening process described above, two reviewers will independently code all eligible studies using a structured data extraction form (see Appendix B). The data extraction form includes items related to bibliographic information and source descriptors (e.g., report type, country); study methods (e.g., assignment to condition, outcomes reported); characteristics of intervention (e.g., description of components; role of evaluator, fidelity assessment); participant and setting characteristics (e.g., grade level, race/ethnicity of participants; type/location of schools); and outcome data needed to calculate effect sizes.
Two trained coders, Brandy Maynard and Anne Farina, will code all included studies. If greater than 20 studies are eligible for inclusion in the review, a third coder may be recruited to assist with coding. Maynard is a trained Campbell reviewer and has substantial experience coding intervention studies for systematic reviews. Farina is a doctoral student who also has experience coding intervention studies. Both coders have been involved in the development of the data extraction form and protocol. Moreover, coders will pilot test the code form together using diverse types of studies and will discuss any items that are unclear and ensure mutual understanding of all items. Following pilot testing of the form, two coders will independently code 100% of the included studies. Coders will compare coding and will identify and discuss discrepancies, which will be resolved through consensus. If consensus cannot be reached between the two coders, a third member of the review team will be consulted to resolve the discrepancy. Initial discrepancies will be recorded and inter-rater reliability will be reported.
Criteria for determination of independent findings
We are interested in four primary outcome constructs: trauma symptoms/mental health, academic performance, externalizing behaviors, and socio-emotional functioning. We anticipate that included studies will use multiple measures for each outcome, multiple reports of the same outcome measure, multiple follow-up time points, and possibly more than one counterfactual condition. These circumstances create statistical dependencies that violate assumptions of standard meta-analytic methods. In order to ensure independence of study-level effect sizes, we will include only one effect size estimate from each independent sample on each outcome construct.
For cases in which a study uses multiple measures (i.e., observation and a standardized instrument) of the same construct, we will code data for each measure and create a study level average across the measures. In cases of multiple reports on the same outcome (i.e., parent and child report), we will code data for each report and take an average of all reports. In cases where multiple points of follow-up are provided, we will code follow-up points to conduct a separate analysis for effect sizes comparing studies with similar points of follow-up. In the case of multiple counterfactual conditions, we will select the comparison condition that is most similar to those in the other included studies.
Risk of bias
Two review authors will independently assess risk of bias in all included studies using the Cochrane Collaboration's risk of bias tool (Higgins et al., 2011) for RCTs and the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) -NRSI (Sterne et al., 2014) for QED studies. We will follow procedures for each of the RoB tools to code risk of bias for each study. Following independent coding by two authors, coders will meet to identify any discrepancies, and all discrepancies will be resolved through consensus. If consensus cannot be reached between the two reviewers, a third member of the review team will be consulted.
Risk of bias in each domain will be reported within and across studies in the results section using narrative and graphs. We anticipate that most studies included in this review will be at high risk of bias; thus, we do not plan to restrict analyses based on risk of bias nor do we anticipate using risk of bias as a moderator variable. We plan to present all included studies and provide a narrative discussion of risk of bias to include discussion of the potential limitations of the review as well as implications of bias in the interpretation of the results in the Discussion section of the review.
Statistical procedures and conventions
We will conduct descriptive analyses on variables of interest from all included studies to provide information regarding: Study participants Settings where studies are situated Relevant intervention characteristics Risk of bias across RCT and QED studies on each domain
Following descriptive analysis, we will estimate effect sizes for each included study. We will calculate the magnitude of effect using the standardized mean difference effect size with Hedges’ g correction for continuous outcomes and odds ratios for outcomes presented as dichotomous variables. We anticipate that outcomes within a category will be measured using similar metrics and therefore, effect sizes within each category will only use either Hedges’ g or odds ratio metrics in the analysis. If, however, outcomes within one of the outcome categories are measured in different metrics, we will convert them to Hedges’ g using CMA software. For studies in which the unit of assignment (e.g., classroom, school) does not match the unit of analysis (e.g., student) and the primary study authors did not account for clustering in their analysis, we will follow recommendations in the Cochrane Handbook (Higgins et al., 2011, 16.3.4) to derive approximately correct analysis by reducing the size of each trial to its ‘effective sample size’ (Rao, 1992) by dividing the sample size for each group by the ‘design effect’ (1 + (M-1)ICC). We will apply this correction only to findings that are statistically significant as nonsignificant findings will remain nonsignificant without the correction (WWC manual).
Following the estimation of individual study level effects, we will conduct separate meta-analyses to pool studies for each outcome construct. Within each of these domains, included studies may use multiple measures and/or multiple reports (e.g., parent, teacher) of the same measure. These circumstances created statistical dependencies that violate assumptions of standard meta-analytic methods. In order to ensure independence of study-level effect sizes, the mean of different measures of the same construct per reporter (e.g., parent, child) will be taken to estimate a study-level average across the measures by reporter type (child reported measures will be pooled separately from parent reported measures). We will follow standard procedures in CMA version 3.0 to use the mean of the selected outcomes for studies with multiple measures of the same outcome construct. In cases where data for multiple points of follow-up are reported, we will code effect size data at each follow-up point to conduct a separate analysis for effect sizes comparing studies with similar points of follow-up.
To synthesize effects across studies, a weighted mean effect will be calculated by weighting each study level effect size by the inverse of its variance. Random effects statistical models will be used throughout unless a compelling case arises for fixed effect analysis. RCT and QED studies will be pooled to allow for greater statistical power unless there are statistically significant differences between the study design types.
Following the estimation of summary effects, we will conduct a test of homogeneity (Q-test) and the I2 statistic will also be used to describe the percentage of total variation across studies due to the heterogeneity rather than chance. We will also construct a forest plot displaying study-level mean effect sizes and 95% confidence intervals for the included studies to provide opportunity for visual analysis of the precision of the estimated effect sizes, detection of studies with extreme effects, and information regarding heterogeneity of studies.
Provided there are a sufficient number of studies, we will conduct moderator analysis to examine characteristics of the study methods, interventions, and student samples that may be associated with effect size. The approach to moderator analysis will be dependent upon the available data. If there are sufficient studies available, meta-regression will be used. If we do not have adequate statistical power for meta-regression, we will use the analog to the ANOVA to conduct moderator analysis using the following variables: 1) student grade level (elementary, middle, high school); 2) program variations (used all three trauma-informed components or only 2). Sensitivity analysis will be conducted to examine the potential effects of outliers and studies not reporting or controlling for group differences. If necessary, additional sensitivity analysis will be conducted if other issues arise that may impede our confidence in the estimated pooled effect size estimates. Moderator analysis will be conducted using Comprehensive Meta-Analysis 2.2 (CMA). We will also assess for publication bias using funnel plots and the Egger's test, both conducted in CMA v. 3.
If there is not a sufficient number of studies to conduct meta-analysis, we will present each of the included studies descriptively and identify deficiencies and gaps in the research base. When possible, we will calculate an effect size per each relevant outcome and provide the point estimate and confidence intervals.
Treatment of qualitative research
We do not plan to include qualitative research.
Footnotes
REVIEW AUTHORS
| Name: Brandy R. Maynard, Ph.D. | |
| Title: Assistant Professor | |
| Affiliation: Saint Louis University | |
| Address: Tegeler Hall, 3550 Lindell Boulevard | |
| City, State, Province or County: | St. Louis, MO |
| Postal Code: 63103 | |
| Country: USA | |
| Phone: 269-876-8903 | |
| Email: |
|
|
|
|
| Name: Anne Farina | |
| Title: Doctoral Student, Graduate Research Assistant | |
| Affiliation: Saint Louis University | |
| Address: Tegeler Hall, 3550 Lindell Boulevard | |
| City, State, Province or County: | St. Louis, MO |
| Postal Code: 63103 | |
| Country: USA | |
| Phone: | |
| Email: |
|
|
|
|
| Name: Nathaniel A. Dell, AM, LMSW | |
| Title: Team Lead, Research & Evaluation | |
| Affiliation: Places for People, Inc. | |
| Address: 4130 Lindell Boulevard | |
| City, State, Province or County: | St. Louis, MO |
| Postal Code: 63108 | |
| Country: USA | |
| Phone: | |
| Email: |
|
ROLES AND RESPONSIBILITIES
Please give a brief description of content and methodological expertise within the review team. It is recommended to have at least one person on the review team who has content expertise, at least one person who has methodological expertise and at least one person who has statistical expertise. It is also recommended to have one person with information retrieval expertise. Please note that this is the recommended optimal review team composition. Content: Brandy Maynard, Anne Farina, and Nathaniel Dell will be responsible for the substantive content related to trauma informed schools. Systematic review methods: Brandy Maynard has significant experience and expertise in systematic review methods and Anne has training and some experience in systematic review methods. Dell has experience with systematic review methods, and has lead and contributed to several published reviews. Maynard has completed and published multiple systematic reviews/research syntheses. Statistical analysis: Brandy Maynard will be responsible for statistical analysis. Maynard has been trained in meta-analytic techniques and has conducted several meta-analyses. Information retrieval: Maynard, Dell, and Farina are experienced in information retrieval. Maynard and Farina will also consult with the information retrieval specialist at Saint Louis University in the planning and execution of the search strategy.
FUNDING
We will be receiving funding form the Campbell ECG through a mini-grant to support the conduct of this review.
POTENTIAL CONFLICTS OF INTEREST
The review team declares no potential conflicts of interest.
PRELIMINARY TIMEFRAME
Note, if the protocol or review are not submitted within 6 months and 18 months of title registration, respectively, the review area is opened up for other authors. Date you plan to submit a draft review: May 2017
PLANS FOR UPDATING THE REVIEW
Maynard will be responsible for updating the review.