
Abstract

Background
The problem, condition or issue
Micronutrient malnutrition (MMN) is widely prevalent and significantly associated with the global burden of poverty and disease. In 2000, the World Health Report identified deficiencies in iron, vitamin A, iodine, and zinc as being the most significant risk factors for poor health outcomes globally (WHO, 2000). Together, over one third of the world's population are deficient in these key vitamins and minerals (WHO, 2000). The groups most vulnerable to MMN include pregnant and lactating women and young children (Black, 2001; Black et al., 2008). The WHO states that globally, 190 million preschool children and 19.1 million pregnant women are vitamin A deficient (WHO, 2009), approximately 100 million women of reproductive age (WRA) suffer from iodine deficiency (Leslie, 1991), and 1.62 billion people are anaemic (B Benoist, 2008), though these estimates reflect a relatively large degree of uncertainty. The majority of these individuals live in low-and middle-income countries (LMICs) where resources are scarce, diets are not diversified, and health care systems are often not equipped for proper management. The consequences of micronutrient deficiencies by themselves, or in association with overt malnutrition, may relate to both intermediate and long term outcomes. For example: iron-deficiency anemia is a common consequence of low iron; iodine deficiency can cause stillbirth, miscarriage, and a range of cognitive deficits in neonates; visual impairments and blindness can result from vitamin A deficiency; and congenital anomalies, including neural tube defects (NTDs) are strongly linked to low folic acid intake in pregnancy. While MMN itself has lasting physiological consequences, it also puts an individual at a greater risk for contracting infectious diseases, increasing the severity disease, and experiencing mortality from common infections such as diarrhea, malaria, pneumonia, and measles (Bhutta, 2008). Both maternal and child deaths are a common consequence of MMN. However, adverse outcomes extend beyond health parameters. Economic and social development is hindered as a result of secondary consequences such as lower work productivity and mental and cognitive decline of those who suffer from MMN (Grantham-McGregor et al., 2007; Hoddinott, 2012; Horton, 2008). Additionally, public health costs are great, inducing a significant burden on both caregivers and health care systems. As such, the international community has become increasingly aware of the importance of dealing with the MMN epidemic.
The intervention
Large-scale food fortification (LSFF) refers to the process whereby one or more essential micronutrients are deliberately added to a staple food or condiment during processing in order to improve its nutritional quality. Otherwise referred to as mass fortification, it is a nutrition-specific intervention that is typically initiated, mandated, and regulated by governments for the purpose of correcting or avoiding micronutrient deficiencies in populations that are at increased risk. Basic commodities, such as flour, oil, salt, sugars, and condiments, are typically chosen as the vehicle for LSFF due to their widespread and regular consumption. Fortificants are defined as the source of micronutrient, while micronutrient premixes refer to that which is blended with the fortificant in order to more feasibly introduce the mixture into the food vehicle. Numerous factors must be taken into consideration throughout planning, including the concentration of the fortificant – such that it is both efficacious and safe, – it's absorptive properties, stability, and how it will affect the sensory qualities of the food vehicle chosen. LSFF is currently promoted as a cost-effective strategy for reducing physiological and clinical outcomes associated with micronutrient deficiencies, particularly when food is processed centrally and existing technologies and distribution networks can be taken advantage of. This is in contrast to targeted fortification practices that capitalize on specific food vehicles for a particular subset of the population (e.g. infant formula) or home fortification, whereby soluble or crushable tablets, micronutrient powders or micronutrient-rich spreads are added to foods at the level of the household. Supplementation, usually in the form of pills, capsules and syrups, is another public health intervention aimed at reducing micronutrient deficiencies. Although it has the advantage of supplying an optimal amount of micronutrient per dose, major barriers to the success of this strategy include poor compliance and a lack of supplies, especially in LMICs. To date, the mandatory iodization of salt is the most widely utilized mass fortification measure on a global scale. Reports from UNICEF indicate that in 2013, 75 percent of households globally consumed iodized salt (UNICEF, 2015). Other common examples include vitamin A fortification of sugar and cooking oil, vitamin D-fortified milk, and iron-fortified flour. While food fortification has a long history of use in industrialized countries, some LSFF programmes have only recently gained momentum in LMICs.
How the intervention might work
The purpose of LSFF is to prevent or reverse micronutrient deficiencies by increasing the nutritional content of staple foods that are widely and regularly consumed by the population at risk of micronutrient deficiency. Primary studies conducted in ideal settings suggest that food fortification is likely to be a biologically efficacious strategy: fortificants available in fortified foods have the potential to be absorbed and bioconverted to the active forms necessary to produce the desired health effects in humans (Abrams et al., 2003; Ballot, MacPhail, Bothwell, Gillooly, & Mayet, 1989; Mannar & Gallego, 2002; Muhilal, Permeisih, Idjradinata, Muherdiyantiningsih, & Karyadi, 1988; Solon et al., 2000; Solon et al., 1996; Thuy et al., 2003). However, in real-world settings, outcomes will depend upon a host of programmatic and contextual factors that will influence the successful implementation of a LSFF program.
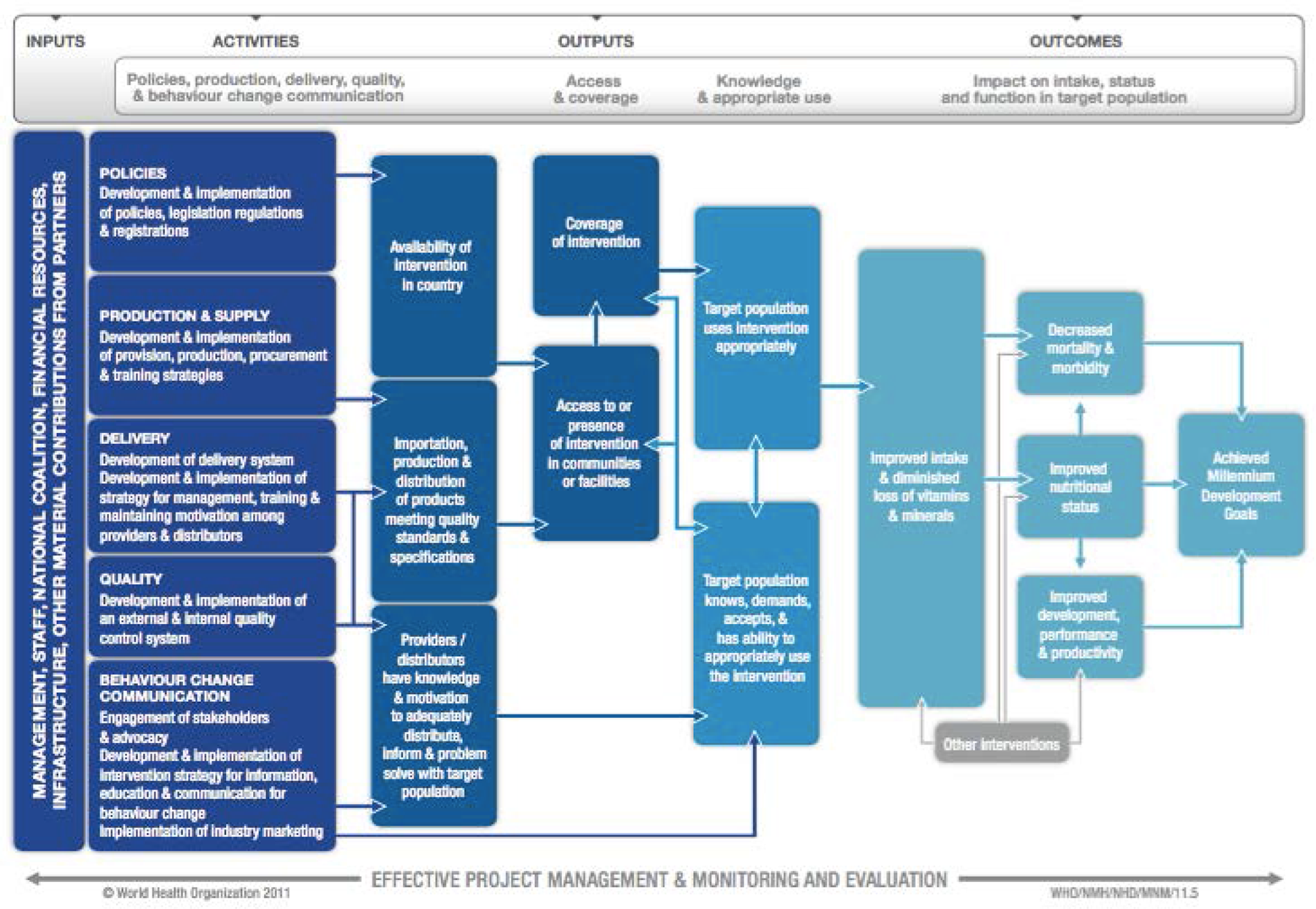
In 2009, the Department of Nutrition for Health and Development from the World Health Organization (WHO) and the International Micronutrient Malnutrition Prevention and Control Program from the US Centers for Disease Control and Prevention (CDC) established a working group to develop a standardized logic model for the purpose of implementing successful micronutrient interventions, including LSFF, in public health programs across various contexts (Figure 1) (WHO/CDC, 2011). Though it necessitates adaptation at the local, regional, and national level, this figure outlines the LSFF inputs and activities that should theoretically produce the desired health and nutritional benefits in a population. The following points explain in brief the critical components of a LSFF program.
WHO/CDC logic model for micronutrient interventions in public health
Prior to implementation, the political climate should be molded such that there is both acceptance and advocacy from leaders. This will create an enabling environment that encourages participation from both the private and industrial sectors. Often, LSFF efforts are controlled through food laws and related practices, which help to specify the logistical elements of a program. These features, such as fortificant type, concentration, and food vehicle, are based upon the defined public health objectives and prevalence of micronutrient deficiencies, population-level dietary patterns, and usual micronutrient intakes (WHO & FAO, 2006). Feasibility is another critical arm of any food fortification program, and includes the availability of supplies, manufacturers, and distribution channels, as well as the costs required to both implement and sustain the intervention. For the continued availability of adequately fortified foods in a population, quality control and quality assurance mechanisms are critical. Additionally, appropriate marketing and education strategies are essential to communicate the benefits of fortification to consumers such that uptake is sustained. This is an especially important component in the case of voluntary fortification. The latter half of the pathway indicates intermediate outcomes, such as accessibility, awareness, and reach, that can significantly influence LSFF performance overall.
Though the pathway is portrayed as linear, multiple feedback loops exist throughout. The end result, whether positive or negative, will link back to the preceding portion(s) of the pathway such that adjustments can be made where appropriate to obtain maximal benefit. With each of these mechanisms in place, and with the appropriate cross-talk between them, it is thought that LSFF will have a sustained and beneficial impact among target populations.
Why it is important to do the review
Food fortification, as a strategy, has been used safely and effectively to prevent micronutrient deficiencies in HICs for more than a century. It is becoming an increasingly attractive investment in LMICs for several reasons, including rapid urbanization and increasing household purchasing power leading to a greater proportion of the population relying on centrally-processed foods. However, up to this point, evidence to document the true impact of LSFF in LMICs has been limited.
There have been a small number of systematic reviews of efficacy and effectiveness trials attempting to discern the effects of single and multiple micronutrient food fortification on infants and school children (Best et al., 2011; Eichler, Wieser, Ruthemann, & Brugger, 2012; Ramakrishnan, Goldenberg, & Allen, 2011). Two reviews (Best et al., 2011; Eichler et al., 2012; Ramakrishnan et al., 2011) focused on developing countries, while a third (Best et al., 2011) was not restricted by location. When the results are taken together, it was established that LSFF improved micronutrient status, reduced anemia prevalence, and increased linear growth. However, effects on other intermediate and functional outcomes varied depending on the study setting. Another recent review (Pachon, Spohrer, Mei, & Serdula, 2015) specifically examined the effectiveness of government-supported flour fortification programs on iron status and anemia in children and women of reproductive age. Evidence pertaining to children was, once again, inconclusive. Overall, gaps in this body of knowledge have impeded us from establishing the effects of fortification on childhood morbidity, mortality, and development.
A recent systematic review by Das et al. (Das, Salam, Kumar, & Bhutta, 2013) evaluated the impact of single, dual, or multiple micronutrient fortification of staples, condiments, or processed foods on both women and children's health globally. Results differed between children and women, though both showed improvement of serum micronutrient levels following fortification. Comparable to findings by others, zinc showed no effect on iron absorption of children, though did increase linear growth. Among women, fortification with calcium and vitamin D was shown to have a significant impact among the post-menopausal age group only. The use of folate significantly decreased the prevalence of congenital abnormalities and, similarly, salt iodization was able to reduce hypothyroidism among women. Again, evidence on morbidity and mortality outcomes in both women and children was lacking, and Das noted that evidence from the developing world was too scarce to comment on the effects of fortification in this setting.
Indeed, although numerous fortification strategies have been shown to be efficacious in many HICs (Das, Kumar, Salam, & Bhutta, 2013; Eichler et al., 2012; T Jiang, 2010), more rigorous and relevant evidence is required from LMICs. Existing reviews are limited to specific subsets of populations and are based on controlled trials only. The current evidence has yet to be coherently analyzed to assess the relevance of findings from programmatic settings or large-scale effectiveness evaluations in community settings. A more comprehensive review is required – one that takes into account both quantitative (effectiveness) and qualitative (analysis of programs/barriers/lessons) measures, especially in real-world programmatic settings.
This review will summarize evidence on the impact of LSFF programs for staple foods in LMICs. It will provide a comprehensive synthesis of LSFF effects on health and nutritional status in various contexts. Key recommendations will be succinctly summarized, and dissemination of findings for use in advocacy, policy, and programmatic decision-making will take place where possible.
Objectives
The review was commissioned by the Global Alliance for Improved Nutrition (GAIN), who specified that the micronutrients for inclusion in the review should include iron, iodine, folic acid, vitamin A, vitamin D, and calcium, either individually or within multiple micronutrient combinations. Typical staple foods include salt, wheat and corn flour, rice, milk, sugar, and soy sauce.
The review has one main objective: To determine the impact of large-scale food fortification (LSFF) of staple foods with key micronutrients (iron, folic acid, iodine, vitamin A, calcium, vitamin D), individually or in combination thereof, on primary and secondary health outcomes in low- and middle-income countries (LMICs).
Methodology
Criteria for including and excluding studies
Types of study designs
Eligible study designs for estimating causal effects include:
Case-control studies Cross-sectional studies (including those using instrumental variable designs or statistical matching) Discontinuity designs (where eligibility is based on a threshold on an ordinal or continuous variable like a consumption expenditure or poverty index) Interrupted time series (ITS) designs Longitudinal cohort studies Natural experiments Serial cross sectional studies where before/after analyses are possible (including panel data studies with multiple observations on the same individuals/groups over time) Randomized controlled trials (RCTs)
In order to capture LSFF effectiveness (i.e. impact in a real-world setting), only national implementation programs or large-scale trials and observational studies will be considered for inclusion. For trials with multiple arms, only those that meet the eligibility criteria will be included. We will also include data from unpublished studies (including grey literature) to reduce the effects of publication bias.
Efficacy1 or proof-of-concept studies comparing micronutrient compounds, fortificant concentrations, or food vehicles, will be excluded.
Types of participants
Participants will include all residents of low- and middle-income countries (LMICs), as defined by the World Bank Group at the time of the search. While we are aiming to assess males and females of all ages, studies will not be excluded if participants are comprised of only one subset (e.g. children <5 years of age). Where data allows, the review will describe the intervention effect on population subgroups (e.g. urban versus rural populations) in order to consider whether there are issues of equity in access to fortified staple foods.
Studies reporting on populations in high-income countries will be excluded.
Types of interventions
Eligible interventions are large-scale food fortification (LSFF) programs – the mandatory or voluntary addition of essential micronutrients to widely consumed staple foods or condiments – for the purpose of improving health outcomes of populations. This review will focus specifically on LSFF with iron, vitamin A, iodine, folic acid, calcium, vitamin D, or multiple micronutrients. There are no restrictions regarding duration of exposure to the intervention, whom it is provided by, or the food vehicle that is utilized, pending it is considered a staple food in the context in which it has been implemented.
Excluded interventions provide targeted fortification, home fortification, or biofortification, or use food vehicles that are considered non-staple foods or condiments, including fortified blended foods and complementary foods.
Comparators may include no treatment (non-fortified foods), standard care (usual feeding practices), alternate treatment (e.g. diet supplementation), or wait-list. Author-defined comparison groups will be used for all analyses.
Types of outcome measures
The following is a non-exhaustive list of outcomes that are considered relevant to our review (see also Table 1). While functional outcomes are more relevant for stakeholders, biochemical outcomes are more often reported, as they are easier to measure. As such, we will include both types of outcomes. Primary outcomes are marked in asterisks.
Types of outcome categories
Biochemical outcomes:
Prevalence of micronutrient deficiency or change in micronutrient status, as measured by dietary intake or biomarkers of nutrient status:
*Serum retinol Serum folate Red blood cell (RBC) folate Serum ferritin Plasma retinol Plasma ferritin Haemoglobin concentration Urinary iodine concentration Serum vitamin D Serum phosphate Serum calcium Serum parathyroid hormone Serum zinc.
Studies assessing bioavailability will be excluded.
Functional health outcomes:
Deficiency diseases and nutrition disorders where the prevalence or rate is provided before and after LSFF. These include, but are not limited to:
Acute malnutrition (defined as weight for height) Stunting (defined as height for age) Underweight (defined as weight for age) *Anemia Hypo/hyperthyroidism *Goiter Night blindness and xerophthalmia Adverse pregnancy outcomes *Neural tube defects (NTDs) Neurological impairment Cognitive dysfunction Bone mass density Morbidity Mortality.
This review will also highlight any adverse effects of the intervention that have been reported on within included studies. Study eligibility will not be based on outcome reported. However, the quantitative analysis will be restricted to only those studies that report a relevant biochemical or functional outcome in one or more studies.
The selection process will be documented in detail, using a PRISMA flow chart. Any post-hoc decisions that are made regarding the eligibility of a study for inclusion will also be documented within the review. In the case that a study is excluded from the quantitative analysis based on outlier results, sensitivity analyses will be performed.
Duration of follow-up
There are no restrictions regarding duration of follow-up.
Types of settings
All low and middle-income settings are eligible.
Additional inclusion criteria
As a logistical decision based on time/resource constraints, the review will be limited to reports published in English. Studies that report in a language other than English will be excluded. This will be noted as a limitation within the review.
Examples of excluded studies
Zimmerman, M.B. et al. Comparison of the efficacy of wheat-based snacks fortified with ferrous sulfate, electrolytic iron, or hydrogen-reduced elemental iron: randomized, double-blind, controlled trial in Thai women. Am J Clin Nutr. 2005 Dec:82(6):1276-82.
Reason for exclusion: efficacy study comparing iron compounds.
Sari, M. et al. Effect of iron-fortified candies on the iron status of children aged 4–6 y in East Jakarta, Indonesia. Am J Clin Nutr. 2001 Jun:73(6):1034–9.
Reason for exclusion: candies are not considered a staple food.
Search strategy
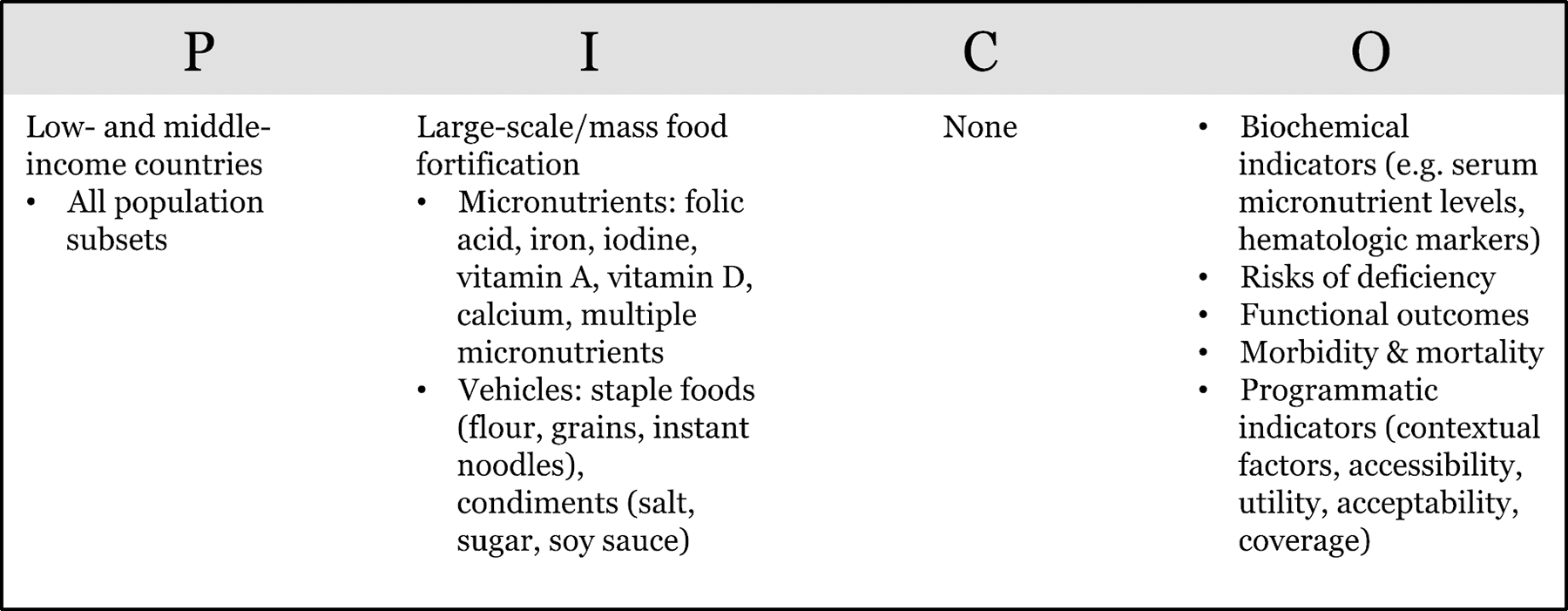
All appropriate, available electronic reference libraries of indexed medical journals and analytic reviews will be utilized. The search strategy will be run in a total of 15 databases, chosen based on their relevance to the subject material of the review, and guided by the PICO methodology (Table 2):
PICO table formulating the review search query
Medline Embase CAB Abstracts Cochrane Library Cumulative Index to Nursing and Allied Health Literature (CINAHL) Popline Jolis Catalogue Jolis Plus WHO regional databases (WHOLIS) System for Information on Grey Literature in Europe (SIGLE) LILACS database for Latin American and Caribbean Health Sciences Literature British Library for Development Studies (BLDS) IDEAS database for economics and finance research Google Google Scholar.
The search will be conducted using indexing terms, including medical subject (MeSH) headings and free text words. Guided by our PICO model (table 1), the search brackets fall into 5 categories: staple foods and condiments, key micronutrients, large-scale/mass food fortification, outcomes, and population. There will be no date restriction on published articles. The search process, including the month/year of search, will be documented for replicability. Details of the search strategy can be found in appendix 1. Manual searches will be conducted within the reference lists of review articles and included primary studies in order to identify any additional sources of information.
Non-indexed grey literature searches will be conducted primarily in Google and Google Scholar. These may include program descriptions, government reports, conference abstracts, or workshop reports. Grey literature documents will be provided by the Global Alliance for Improved Nutrition (GAIN). We will also search other standard sources of grey literature such as SIGLE/OpenGrey. Additionally, key international nutrition agencies such as The Micronutrient Initiative, will be individually contacted for further information. We will also conduct snowballing of references, and hand-searching relevant journals and websites as appropriate.
Relevance decisions will be based on two rounds of screening: titles and abstracts, followed by full text. Two independent reviewers will screen both abstracts and full texts in order to identify studies adhering to the inclusion/exclusion criteria. Any disagreements on selection of studies will be resolved by a third, independent reviewer. Quality assessment will also be performed in duplicate for each study.
Description of methods used in primary research
Because of the inclusion criterion that states that studies must be evaluating nationally implemented fortification programs or large-scale trials only, many similar methodologies are found within the primary research covered by this review. Most abundant are ITS designs, which examine a specific health outcome in a population, or segment of a population, at multiple time points prior to and following the implementation of a food fortification program. To exemplify these methods, we describe details of eligible studies in the following section.
Hertrampf, E. and Cortes, F. National food-fortification program with folic acid in Chile. Food Nutr Bull. 2008 Jun:29(2 Suppl):S231-7.
In the year 2000, the Chilean Ministry of Health implemented a National program that mandated the fortification of all wheat flours with 2.2mg/100g folic acid in an attempt to combat neural tube defects (NTDs). This study utilized a hospital-based prospective time-series design to examine the prevalence of NTDs in all live and stillbirths during a pre-fortification (1999–2000) and post-fortification (2001–2002) period. This hospital-based surveillance system encompassed nine public hospitals in the city of Santiago, accounting for 60 percent of births in Santiago and 25 percent in all of Chile. A trained staff member was responsible for reviewing all birth documentation, registering and describing NTD. A clinical geneticist reviewed all diagnoses to confirm correct NTD type (anencephaly, spina bifida, or encephalocele). Total prevalence rates were then calculated as total number of NTD per 10,000 births for both time periods.
Using hospital-based surveillance is a common design when measuring NTD rates. Many other studies pertaining to LSFF use cross-sectional methods to capture data on other health outcomes, such as anemia. The following study is one such example:
El Hamdouchi, A. et al. Does flour fortification with electrolytic elemental iron improve the prevalence of iron deficiency anaemia among women in childbearing age and preschool children in Morocco? Mediterr J Nutr Metab. 2003(6):73–78.
This study examines the prevalence of iron-deficiency anemia (IDA) in two post-fortification periods (May 2006 and January 2008) following a wheat flour fortification program with iron in Morocco. The target population consisted of women aged 15–49 years and preschool children aged 2–5 years who were recruited at 38 health centres covering both rural and urban areas of the country. The centres were chosen based on their accessibility to patients, pre-existing maternal and child health activity, and proximity to a hospital laboratory. To measure serum hemoglobin (Hb), blood was collected from each participant and transported to the laboratory for analysis. Anemia was defined by WHO criteria for preschool children as a Hb level <11.0 g/dL [mild= 10–10.9 g/dL, moderate= 7–9.9 g/dL, severe <7 g/dL]. WHO criteria defined anemia among women of childbearing age as Hb <12.0 g/dL [mild= 10–10.9 g/dL, moderate= 7–9.9 g/dL, severe <7 g/dL]. Mean ± standard deviations were calculated for Hb, examined with unpaired t tests and deemed significant if p values <0.05. Study results were displayed as both mean Hb (g/dL) and prevalence of IDA (%), broken down into the varying categories, in order to give a clear picture of any changes that occurred between 2006 and 2008.
Of the methods used in primary research to estimate the causal effects of food fortification, cross-sectional and longitudinally based interrupted time series designs are common. Some additional methodologies include retrospective before and after designs using hospital administrative or surveillance data, repeated cross-sectional studies, and controlled or randomized controlled trials using large-scale cluster sampling methods.
Criteria for determination of independent findings
We do not anticipate non-independence of study measures to be problematic within our analyses. As most included studies will consist of before/after designs, estimates will be based on separate populations (e.g. hospital-based surveillance of NTD rates in live and stillbirths before and after LSFF implementation). If multi-arm studies are included, intervention groups will be combined or separated into different forest plots, and we will ensure that there is no double counting of participants. If an outcome is reported in several different metrics, we will perform unit conversions in order to pool the data. We do anticipate differences in the types of literature and we will ensure that any analysis will take possible sources of dependency into account by grouping papers into studies/programmes and ensuring that no double counting of evidence takes place when synthesizing across programmes.
Details of study coding categories
Study data will be abstracted into a standardized data abstraction form that is comprised of a general study information sheet and a quantitative outcome sheet. All data abstraction will be done in duplicate.
Each general study information sheet will include the following:
General information (author, publication year, language of study, study design) Study setting (country, length of study, year(s) of data collection, urban/rural) Study population (total study population (N), number and description of participants) Intervention (date of LSFF implementation, mandatory/voluntary status, level of intervention (e.g. national or regional), micronutrient(s) of interest, fortificant compound, fortificant concentration, food vehicle chosen, duration of intervention, other micronutrient intervention(s) being utilized by participants) Additional notes Funding source for program/study Quality assessment (see section 3.6)
Some of these variables will be considered as potential moderators (see section 3.7).
Each quantitative outcomes sheet will contain the following information:
Subgroup Subgroup (N) Outcome category* Outcome definition Outcome units Outcomes (for intervention & comparison group): Outcome measure comparison group (or pre-fortification) Outcome measure treatment group post-fortification Standard deviation Effect: Effect measure (specify type) 95% confidence interval P-value of effect measure Standard error or t-statistic Additional notes
*Biochemical and functional outcomes will be further broken down into the following categories: anthropometry, micronutrient deficiency, biochemical status, developmental outcome, morbidity, and mortality.
Critical appraisal of studies
Individual studies will be critically appraised according to a set of criteria based on study type, using the Cochrane guidelines. All quality assessment will be done in duplicate to ensure reliability.
For ITS studies, the following standard criteria will be taken into consideration: i) independence of the intervention, ii) pre-specified shape of the intervention effect, iii) effect of the intervention on data collection, iv) knowledge of the intervention during the study, v) incomplete outcome data, vi) selective outcome reporting, and vii) other risks of bias. For RCTs (including cluster-RCTs), non-randomized controlled trials, and controlled before-after studies, the following criteria will be considered: i) adequate randomization, ii) allocation concealment, iii) similar baseline characteristics and outcome measures between intervention and control groups, iv) incomplete outcome data, v) blinded assessment, vi) study contamination, vii) selective outcome reporting, and viii) any other risks of bias will be considered. Assessment of adjustment for confounding and the potential for reverse causality will be included for quasi-experimental and observational study types. For uncontrolled before and after studies, careful consideration will be given to historic events/confounding variables and the quality of data collection before and after intervention implementation. These studies will be deemed high risk of bias. Loss to follow up of study participants will be assessed for all studies (>20% loss to follow up is considered a serious limitation). Where a study investigates multiple outcomes, risk of bias due to lack of blinding will be considered separately.
‘Low risk of bias’ studies will demonstrate clear measurement of and control for confounding, including selection bias, where intervention and comparison groups are described adequately and risks of spillovers or contamination are small, and where reporting biases and other sources of bias are unlikely. Studies with ‘medium risk of bias’ will be those where there are threats to validity of the attribution methodology, or there are risks of spillovers or contamination, arising from inadequate description of intervention or comparison groups or possibilities for interaction between groups. ‘High risk of bias studies’ are those where there is evidence of spillovers or contamination to comparison groups from the same communities, and reporting biases are evident. The body of evidence for each pooled outcome will then be assessed for quality using the Child Health Epidemiology Research Group (CHERG) grading system, an extension of the guidelines developed by the Cochrane Collaboration and the Working Group for Grading of Recommendations Assessment, Development and Evaluation (GRADE). CHERG incorporates three categories of criteria for quality assessment: (i) volume and consistency of evidence; (ii) effect size; (iii) strength of statistical evidence, as reflected by the p-value (Walker et al., 2010). Quality assessment information can be found within the study information sheet of the data abstraction form.
Statistical procedures and conventions
Outcome data that are not in the form of means and standard deviations for continuous outcomes and proportions or number of events for discrete outcomes will be converted to such, where possible. We will ensure that scales are consistently measured across studies, such that an increase or decrease across the scale will always indicates improvement or deterioration of an indicator. Where data are incomplete or in a form that is unable to be converted, the author will be contacted for clarification. In the event that access to additional data is not possible, the outcome will be excluded from further analysis.
Meta-analyses will be performed wherever participants, interventions, comparisons, and outcomes are sufficiently similar to ensure a meaningful answer (i.e. across similar PICOs). They will be performed separately per micronutrient (vitamin A, iron, iodine, folic acid, vitamin D, calcium, and multiple micronutrients) and outcome (where pre- and post-fortification outcomes are reported in >1 study). We will analyse randomised and non-randomised studies with contemporaneous comparison groups separately, pooling only where differences in findings are not statistically significant. We will report separately findings from studies without contemporaneous comparators (e.g. uncontrolled interrupted time series and uncontrolled pretest-posttest studies). Review Manager Software version 5.3 will be utilized. Approximately correct analysis of cluster-randomized trials, whereby standard errors will be calculated using information on effective sample size, will be used to correct for any unit of analysis errors, where the original study authors failed to do so. Study effect sizes will be appropriately weighted in pooled analysis to take into account inverse variance. Dichotomous and continuous outcomes will be analysed separately. For dichotomous outcomes, results will be presented as summary risk ratios (RR) or odds ratios (OR) with 95% confidence intervals (CI). Continuous data will be presented as standardised mean differences (SMD) between intervention and comparison groups.
There are several characteristics of included studies that will be retained for examination as potential moderators of study outcomes. These include:
Study country Age and sex of participants Socioeconomic status Urban/rural residence Level of education Baseline micronutrient status Food vehicle utilized Fortificant type Concentration of fortificant Duration of intervention Mandatory or voluntary fortification Free distribution/market distribution of fortified food and level of implementation (e.g. national, regional, school-based) Multi-interventional exposure (e.g. diet supplementation along with food fortification).
Subgroup analyses will be performed according to age group for all outcomes. Age groupings will be determined by data that is available, but we would anticipate the following basic categories: children 6–59 months, children >5 years, adolescents 10–19 years, women of reproductive age (WRA) 15–49 years, men 15–49 years. Along with providing the overall population-level effect of LSFF, we will separate children, WRA, and men into multiple forest plots to visualize this effect of age and sex. Further subgroup analyses (e.g. by study design) will be conducted where possible in order to assess the potential of confounding by each additional moderator variable. For example, subgroup analysis by food vehicle (e.g. vitamin A fortification of oil versus sugar) may prove to determine important differences in effectiveness of a LSFF program. All subgroup analyses will include reporting of statistical tests of the mean difference between groups examined. Any moderator variables that are identified post hoc will be clearly noted as such within the report.
For the interpretation of results, overall effect estimates that have an associated p-value <0.05 will be deemed statistically significant. Non-significant findings will be interpreted and reported appropriately. To address heterogeneity among studies, a random effects model will be used, where the weighting of studies is more balanced. Additionally, between-study heterogeneity will be examined using the I-squared and Tau-squared statistics and a Chi-square test (where a p-value <0.1 is considered statistically significant), and through visual inspection of forest plots. Accuracy of numeric data (magnitude and direction of effects in reported studies compared to review) will be checked, and sensitivity analyses will be performed in order to determine the robustness of results, including according to study design and risk of bias assessment. Review conclusions will be based solely on findings from the quantitative synthesis of included studies.
Treatment of qualitative research
We do not plan to include qualitative research.
Footnotes
Review authors
|
|
Emily C. Keats |
| Title: | Research Associate |
| Affiliation: | The Centre for Global Child Health, the Hospital for Sick Children (SickKids) |
| Address: | 686 Bay Street, suite 11.9805 |
| City, State, Province or County: | Toronto, Ontario |
| Post code: | M5G 0A4 |
| Country: | Canada |
| Email: |
|
|
|
|
|
|
Zulfiqar A. Bhutta |
| Title: | Principal Investigator |
| Affiliation: | The Centre for Global Child Health, The Hospital for Sick Children (SickKids) |
| Address: | 686 Bay Street, suite 11.9805 |
| City, State, Province or County: | Toronto, ON |
| Post code: | M5G 0A4 |
| Country: | Canada |
| Email: |
|
|
|
Ayesha Siddiqua, Daina Als |
| Title: | Research Assistants |
| Affiliation: | The Centre for Global Child Health, The Hospital for Sick Children (SickKids) |
| Address: | 686 Bay Street, suite 11.9805 |
| City, State, Province or County: | Toronto, ON |
| Post code: | M5G 0A4 |
| Country: | Canada |
| Email: |
|
|
|
Jai Das |
| Title: | Assistant Professor |
| Affiliation: | The Centre for Excellence in Women and Child Health, Aga Khan University |
| City, State, Province or County: | Karachi |
| Post code: | |
| Country: | Pakistan |
| Email: |
|
Roles and responsibilities
Content: Zulfiqar A. Bhutta Systematic review methods: Emily C. Keats, Daina Als, Jai Das Statistical analysis: Emily C. Keats, Ayesha Siddiqua, Jai Das Information retrieval: All
Sources of support
This review is funded by the Global Alliance for Improved Nutrition (GAIN).
Declarations of interest
The Global Alliance for Improved Nutrition (GAIN) has a specific interest in large-scale food fortification programmes and activities. However, GAIN is not involved in the referee process for this review, which has been managed independently by the Campbell International Development Coordinating Group (IDCG).
Preliminary timeframe
January 2019
Plans for updating the review
Dr. Zulfiqar Bhutta would guarantee future updates of the review as contact author.