
Abstract

Background
1.1 DESCRIPTION OF THE PROBLEM
Although many maternal deaths are preventable, health of mothers has been a much neglected issue especially in low income countries (Cook 2004; DFID 2011a). In the recent past, more than 350,000 women have died each year from preventable complications related to pregnancy and childbirth (Ki-Moon 2010). Almost all (99%) maternal deaths continue to occur in poorly resourced countries, with 225 deaths per 100,000 livebirths occurring in low to middle income countries (LMICs) compared with 18 deaths per 100,000 livebirths in high income countries in 2011 (Lozano 2011).
Achieving Millennium Development Goal 5 (MDG5) - to reduce maternal mortality by 75% between 1990 and 2015 - will require an annual decline in mortality of 5.5% (Wilmoth 2010). Although methods for estimating maternal deaths are acknowledged to be weak (Wilmoth 2010), all recent estimates show maternal deaths to be declining. There has been a one-third drop from 409,100 maternal deaths in 1990 to 273,500 deaths in 2011 (Lozano 2011). This current rate of decline clearly will not be sufficient to meet the overall MDG5 target by 2015 – a mere three years away.
A maternal death is defined as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration, the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes (WHO 1993). A maternal near-miss case is where a woman nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of the termination of the pregnancy (Say 2009). Common life-threatening complications include severe postpartum haemorrhage, severe pre-eclampsia, eclampsia, sepsis/severe systemic infection, and ruptured uterus (WHO 2011a).
The main causes of maternal death are haemorrhage, infection, obstructed labour and complications of unsafe abortion (Khan 2006). Many of these causes have a link with nutrition, and may even reach back to before the woman's own birth (Rush 2000). For example, severe anaemia is linked to deaths from complications such as postpartum haemorrhage and short stature of mothers may lead to obstructed labour.
In many low income countries, diets are often based on cereals or legumes, with little variety, few animal products and a restricted range of fruits and vegetables (Ladipo 2000). Over 40% of the world's pregnant women have anaemia, with 90% living in Africa or Asia (Sanghvi 2010). Women with anaemia typically have deficiencies of many other nutrients such as iodine, vitamin A, and zinc that can lead to greater morbidity and mortality for both mother and child (Black 2008, Shankar 2009, van den Broek 2003).
1.2 DESCRIPTION OF THE INTERVENTION
Many life-threatening or serious events/morbidities in pregnant women may be amenable to nutrition interventions (Christian 2002). Ideally many of these interventions would have a preventive focus e.g. iron supplementation, food fortification or dietary diversification to decrease the incidence of anaemia in women before they become pregnant.
Nutrition is the business of both the health and agriculture sectors, and consequently has not always been high on the list of development priorities (DFID 2011b). Relevant interventions range from large national programs to local programs or interventions targeted at particular groups of women. These interventions can be classified as:
Nutrition specific interventions and programs which include fortification, supplementation (food or nutrients) and behaviour change communications interventions aimed at improving nutrition practices and use of nutrition services. Examples include multiple micronutrient, iron/folate or vitamin A supplementation, iron fortification, dietary diversification, protein or energy supplements and nutrition education interventions.
Nutrition sensitive interventions and programs which include programs that address some of the underlying determinants of nutrition (e.g. poverty, food insecurity, poor health, gender inequity, etc). Such programs include agriculture programs, social safety net programs, health programs, and education programs.
Some of potentially effective solutions such as supplementation may seem straightforward to implement, but the reality of achieving health gains is very complex. There are many access, contextual, behavioural and system barriers to implementation of nutritional programs for women of reproductive age. One fundamental cause of pregnant women and other women of reproductive age being undernourished is poverty which leads to a limited ability to purchase and consume sufficient and/or suitable food. Discrimination against women and girls which restricts their access to food (Gittlesohn 1997) and health care, lack of quality antenatal care, and cultural and social beliefs and practices such as ‘eating down’ to avoid giving birth to a large baby, may also contribute to undernourishment (Nag 1994).
1.3 HOW THE INTERVENTION MIGHT WORK
Nutrition interventions or other interventions aimed at improving women's nutritional status may work directly to improve maternal survival by preventing or treating disease, infections or nutritional deficiencies; by improving immune status; or by improving healthcare seeking behaviour including the use of quality antenatal, intrapartum and postnatal care. Early nutritional interventions may influence growth of young women and girls and thus reduce the incidence of obstructed labour, specifically when due to cephalopelvic disproportion. Improved nutrition may lessen fatigue and also improve women's emotional wellbeing.
Fetal, neonatal and infant survival and health is closely related to maternal nutrition: deficiencies in key micronutrients such as folate can lead to serious congenital birth defects, and intra-uterine growth retardation, which can result from poor maternal nutrition, can lead to low birth weight in newborns (Kramer 1987). Therefore, the prevention and reduction of maternal undernutrition is vital for ensuring fetal, neonatal and infant health and survival.
A long-term aim would be for all women to enter pregnancy in an adequately nourished state. Almost one third of adolescent girls in low-middle income countries are married and conceive within a year of marriage (WHO 2011b); in sub-Saharan Africa, nearly two-thirds of women have their first child before the age of 20 years (Bongaarts 1998). Clearly, intergenerational perspectives and activities are required to break the cycles of poverty and malnutrition and ensure that women are well nourished at all stages of life.
It is likely that single nutritional interventions will need to be supported by other strategies in order to be effective on a broad scale. However nutrition programs have not always been well integrated with maternal and child health (MCH) programs and “there is an emerging international consensus that the convergence of nutrition and MCH is essential” (Streatfield 2008, p.238). There are many impediments to the implementation of effective interventions, particularly in poor countries. Some important considerations are access to food (physical, social, economic and cultural access); workforce availability and retention and program transferability and sustainability; weak health systems; and policy barriers (Zehner 2009).
The effectiveness of nutritional interventions at improving nutritional and health status among females of reproductive age and pregnant and lactating women in LMICs depends on several overlapping factors ranging from cost of food and availability of a diversity of foods, to broader factors associated with social and political structures. Underlying chronic conditions can also affect a woman's ability to adequately absorb nutrients and diseases such as HIV/AIDS and malaria can also lead to serious nutritional deficiencies and severely compromised immune systems. Many interventions (household, community or facility based) have been used to address the poor nutritional status of women, including provision of food directly or improved access to the means to produce food or purchase food such as through voucher systems or cash transfers; macronutrient and micronutrient supplementation; nutritional advice and counselling; and preventing and treating diseases which adversely affect nutritional status. Successful interventions can not only improve a woman's nutritional status but can also decrease maternal morbidity and mortality. Ideally each woman would enter pregnancy in a well-nourished state but this may be largely dependent on the nutritional status of one's own mother and whether or not a woman has been adequately nourished throughout her whole life, including during the prenatal months. Evidence suggests that poor nutrition in the womb can lead to long-term, chronic health problems (Barker, 1997). An intergenerational perspective is therefore crucial.
There are many pathways to improving women's nutrition – and many barriers which hinder the ability of nutritional interventions to prevent maternal morbidity and mortality. These are outlined in the logic model/conceptual framework (Anderson 2011) shown in Figure 1.
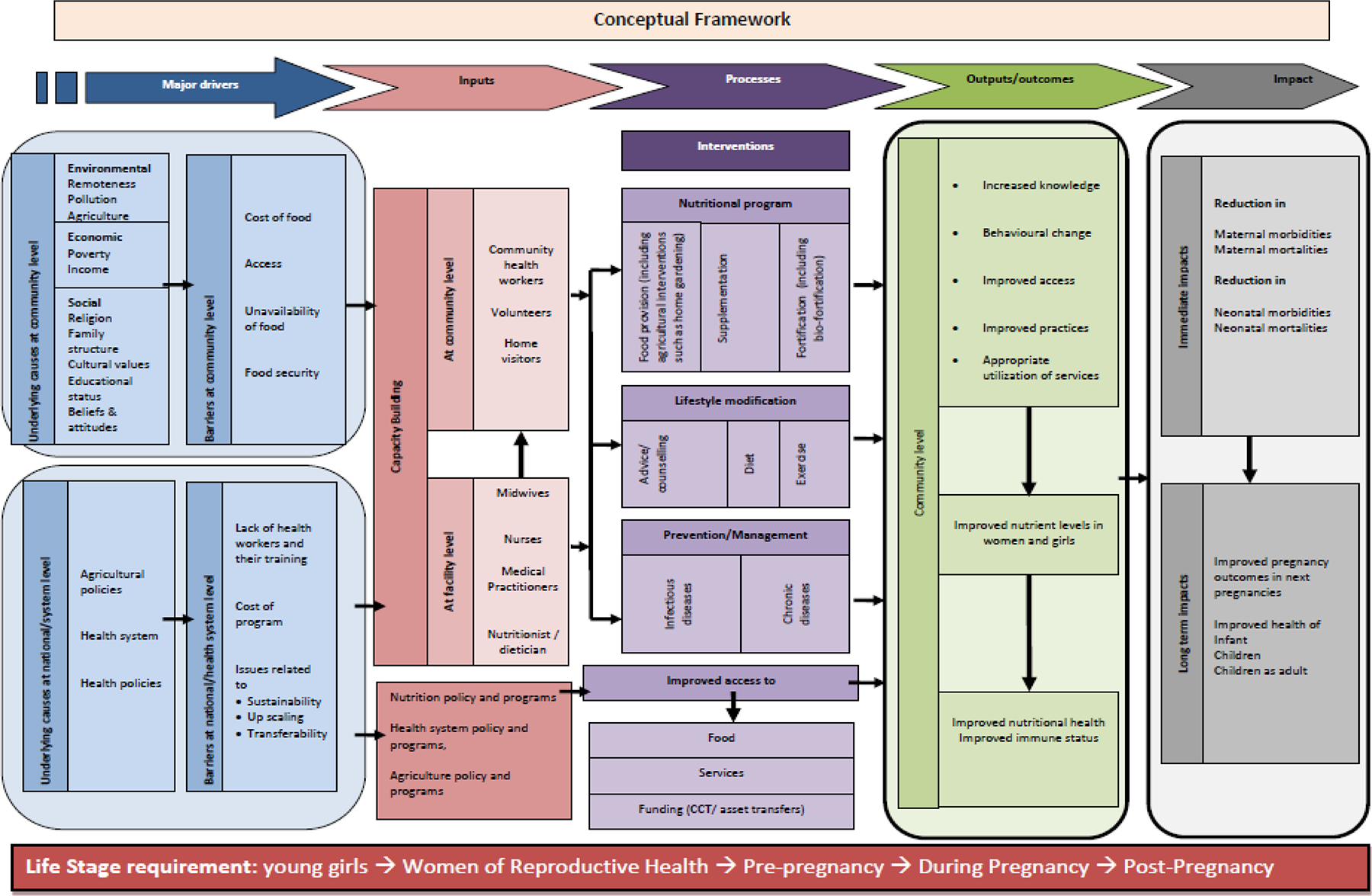
The factors that reduce program effectiveness are complex and relate to issues as diverse as distribution failures and lack of adherence (women are unwilling or unable to adhere in the short or longer term). This illustrates the importance of understanding the processes of implementation and the reasons for sustainability of improved outcomes, which may well differ between contexts.
1.4 WHY IT IS IMPORTANT TO DO THIS REVIEW
Every two minutes around the world there is a maternal death– and one woman dies every seven minutes from postpartum haemorrhage, the single most common cause of maternal mortality (Potts 2010). It is therefore important to synthesise the evidence about the effects of interventions to prevent maternal deaths and reduce maternal morbidities. In this review we will present the evidence about the potential of nutritional interventions or interventions to change nutritional status in women of reproductive age in making an impact on maternal mortality and morbidity.
Maternal mortality and morbidity are the main focus of the review. Maternal mortality and morbidity are also inextricably linked with stillbirth and neonatal deaths and there have been recent calls for health systems to deliver more effectively for both mothers and babies (Pattinson 2011). Pregnancy outcomes are important in their own right, and also as an indicator of maternal health due to problems in accurately measuring maternal mortality prevalence (maternal mortality is usually measured in terms of prevalence rates per 100,000 live births, requiring very large sample datasets for precise estimates) or self-reported morbidity. Pregnancy outcomes will therefore also be included in this review.
There are systematic reviews that examine maternal and child health impacts of some nutrition interventions such as iron supplementation (Fernández-Gaxiola 2011) and magnesium sulphate supplementation (Duley 2003), and agricultural interventions such as home gardens (Masset 2012). Our proposed review is the only one that we are aware of that encompasses such a wide scope in terms of target population and breadth of the various interventions.
This review will synthesise the evidence about which programs are likely to successfully influence maternal nutrition and therefore lead to improvements in maternal mortality and morbidity. It also aims to outline what is necessary to implement effective programs and interventions and will therefore aim to be highly relevant for both policy and practice.
2 Objective of the review
Main objective:
To assess the effects of nutrition interventions or programs or those directed at influencing maternal nutritional status (nutrition-sensitive interventions/programs) on maternal mortality and serious maternal morbidities.
Additional questions and objectives:
1. Do effects differ by program or contextual characteristics?
To assess whether effects differ by type of intervention/program, by regimen or by timing; To explore variation in effects according to settings and contexts, population characteristics, social, economic and political factors, how programs are delivered and who delivers them.
2. How does uptake influence effect of nutrition interventions and how can uptake rates be improved?
To explore why rates of adherence to nutrition interventions/programs vary and how these variations in uptake influence the effect of nutrition interventions/programs; To document barriers and enablers to uptake of nutrition interventions/programs and to explore how barriers can be reduced and how enabling strategies can be increased;
3. Which strategies are likely to increase implementation?
To assess the effect of strategies to deliver and implement nutrition interventions/programs in different contexts and to determine what is required to optimise up-scaling, transferability and sustainability of nutrition interventions/programs.
4. What are the effects of maternal nutrition interventions or programs on neonates, infants and children?
To assess effects on neonatal, infant and child survival in studies evaluating the effects of nutritional interventions or programs on maternal mortality.
In Table 1 we have expanded the objectives into study design, participants, interventions and outcomes to clarify the scope of the review.
OBJECTIVES EXPANDED TO SHOW STUDY DESIGN, PARTICIPANTS, INTERVENTIONS AND OUTCOMES
3 Methods
3.1 CRITERIA FOR INCLUDING STUDIES IN THE REVIEW [PICOS]
3.1.1 Participants
Girls and women of reproductive age (including pregnant and lactating women) from low and middle income countries (The World Bank Group 2011) and marginalised and/or disadvantaged girls and women of reproductive age from high income countries. Clusters of women from regions or villages will also be eligible. Health care providers or policy makers from the studies reporting information on implementation, up-scaling or sustainability of programs.
3.1.2 Interventions
To reflect the reality that “solutions to undernutrition must go beyond the provision of specific nutrients” (DFID 2011b), we have adapted the typology outlined in the ‘Scaling up nutrition’ report (DFID 2011b) which makes a distinction between specific nutrition interventions and those which are nutrition-sensitive:
Nutrition specific interventions and programs which include fortification, supplementation (food or nutrients) and behaviour change communications interventions aimed at improving nutrition practices and use of nutrition services;
Nutrition sensitive interventions and programs (which include programs that address some of the underlying determinants of nutrition (e.g. poverty, food insecurity, poor health, gender inequity, etc). Such programs include agriculture programs, social safety net programs, health programs, and education programs;
We will report the effects of the nutrition component separately wherever possible. We plan to contact study authors to request these data if not available in study publications. Comparators will be standard care or no program/intervention or delayed intervention, or different types of nutrition program or package. Interventions may occur during pregnancy and/or lactation, pre-pregnancy or inter-pregnancy.
3.1.3 Outcomes
3.1.3.1 Primary Outcomes
Maternal death (ideally reported as standardised definition (WHO 2009), but as reported by study investigators if not) Causes of maternal death (as reported by study investigators) Near-miss maternal cases (ideally reported as standardised definition (WHO 2011a - see Appendix), but as reported by study investigators if not) Severe maternal complications (adapted from WHO 2011a; or as reported by study investigators) Severe postpartum haemorrhage Severe pre-eclampsia Eclampsia Sepsis or severe systemic infection Ruptured uterus Severe complications of abortion Obstructed labour Critical interventions (WHO 2011a) - any of: Admission to intensive care unit Interventional radiology Laparotomy (includes hysterectomy, excludes caesarean section) Use of blood products
3.1.3.2 Secondary Outcomes
Perinatal death (stillbirth or early neonatal death) Stillbirth Neonatal death Infant death Complications of pregnancy: Miscarriage Insufficient gestational weight gain Excessive gestational weight gain Prolonged labour Postpartum haemorrhage Pre-eclampsia and/or gestational hypertension Anaemia Infection Postpartum depression Mode of birth (caesarean, spontaneous vaginal, assisted vaginal) Congenital anomalies Neonatal morbidity: Intrauterine growth restriction (as defined by study investigators) Small for gestational age (as defined by study investigators) Preterm birth (< 37 weeks) Low birthweight (< 2500 g) Admission to neonatal intensive care Maternal emotional health (distress, anxiety, depression)
Intermediate outcomes
Adherence and uptake of interventions and programs Women's knowledge, attitudes and behaviour, such as breastfeeding Accessing health care system including antenatal care Referral to health practitioners Type and level of referral to health practitioners Nutritional status, including serum indicators such as serum iron, haemoglobin, zinc, retinol (vitamin A), and vitamins D and E Anthropometric measures such as mid upper arm circumference and BMI in nonpregnant women Dietary changes Immune status (e.g. CD4 counts) Rates of termination of pregnancy Use of contraception
Long-term outcomes
Postpartum maternal health Chronic diseases such as cardiovascular disease, obesity, diabetes Interpregnancy intervals Number of subsequent pregnancies Teenage pregnancies Infant and child growth (e.g. height-for-age, weight-for-age, weight-for-height) Child development and cognition
For qualitative synthesis
Reasons for adherence and uptake of interventions and programs Barriers and enablers related to implementation, up-scaling, transferability and sustainability of the interventions. Strategies used in implementation, up-scaling, transferability and sustainability of the interventions. Suggestions to optimise implementation, up-scaling, transferability and sustainability of the interventions.
3.1.4 Study Types
Studies of various designs addressing the effects of the nutrition interventions on maternal, fetal and neonatal outcomes of interest as well as studies evaluating implementation of these interventions will be considered for inclusion, along with qualitative studies that address reasons for adherence or lack of uptake of these interventions.
3.1.4.1 Quantitative studies
Randomised controlled trials (including cluster trials), other controlled trials, or observational cohort studies without controls, interrupted time series, case-control and cross-sectional studies will be included in synthesis of effects.
3.1.4.2 Qualitative studies
Qualitative studies (reporting surveys or interviews) will be included where they report on primary evidence and address behaviours such as adherence, or report information on barriers and enablers, and/or factors affecting scaling up or sustainability of programs. Relevant qualitative information will also be collected from studies providing quantitative data.
We will not use any methodology inclusion criteria to screen qualitative evidence; all studies reporting evidence will be included in this analysis. We will, however, critically appraise this evidence using explicit criteria (see Methods below).
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.2.1 Electronic searches
We will search the following ‘mainstream’ or specialist databases as they cover most of the main nutrition and maternal health journals and the general health and medical journals which publish in this area: MEDLINE, EMBASE, The Campbell Library, The Cochrane Library, The Reproductive Health Library, Maternal and Infant Care, Web of Science, CAB Abstracts, Scopus, Popline, SCIRUS, Electronic Theses and Dissertations (ETD).
We will use the cited references feature in Web of Science and Scopus.
We will also search the following regional databases: #x2028;○ African Index Medicus, LILACS, CBM, Australasian Medical Index, IndMED, KoreaMed, IMSEAR, WPRIM.
A search strategy for MEDLINE is attached (see Appendix). This strategy will be adapted for the other databases listed above.
As some of the relevant literature is published in the form of monographs and reports or in journals which may not be indexed in databases, we will search or scan the following specialist and NGO sources: WHO Regional Index Medicus for the Eastern Mediterranean region (EMRO) eLENA HINARI WHO Global Health Library World Bank DFID ELDIS OpenGrey Partnership for Maternal, Newborn and Child Health Global Strategy for Women's and Children's Health Healthy Newborn Network International Food Policy Research Institute (US) Micronutrient Institute Global Alliance for Improved Nutrition Concern International, Valid International/Valid Nutrition, Helen Keller International, Action Against Hunger, Save the Children
We will also search Google and Google Scholar using terms such as “Millennium Development Goal 5”, “MDG5”, “maternal mortality and nutrition”, “safe motherhood”, “essential nutrition actions” and we will also use the cited references feature in Google Scholar.
Search dates will be from 1990 to present.
3.2.2 Other Searches
We will scan 2011 and 2012 issues of journals likely to publish relevant studies, including Food Nutrition Bulletin and Maternal Child Nutrition.
We will search reference lists of potentially eligible studies and systematic reviews addressing our interventions of interest. We will contact key authors publishing in the area of maternal nutrition.
No language or publication status restrictions will be applied. We will attempt to obtain translations where possible if the review team is unable to translate particular papers.
3.3 DATA COLLECTION AND ANALYSIS
3.3.1 Selection of studies
Potential study eligibility will be independently assessed through a two-level process. At least two review authors will apply the predefined screening criteria (see Appendices 1 and 2). Any studies considered obviously irrelevant from screening the titles and/or abstracts will be excluded at the first level. Any uncertainties at the first level screening will be re-assessed on the basis of full text in the second level of screening.
We will also contact the primary authors of the study for any insufficient or unclear information if required. Any disagreement will be solved by discussion. If needed, a third review author will be consulted for any unsolved disagreement, and a consensus will be sought. Reasons for exclusion of studies will be documented.
3.3.2 Data extraction and management
Data from the included studies will be independently coded and extracted by at least two review authors using the predefined data extraction forms (see appendices 3, 4 and 5). If there are two or more papers describing the same study, they will be combined and coded as a single study. A third review author will be consulted in the event of any disagreements, and consensus will be sought. We will attempt to contact authors of the original reports to obtain further details if required.
We will extract frequency for the binary outcomes, and mean with standard deviation for the continuous outcomes. The adjusted effect sizes will be also collected for observational studies if possible. The pre-post change effect sizes will be extracted for the interrupted time series and before-and-after studies. For qualitative findings, we plan to extract all themes or qualitative information identified in the primary studies and relevant to the research questions. Extraction of qualitative data will be driven by a theoretical framework of behaviour change and motivation (Michie 2011).
References will be managed using EndNote X4 (Thomson Reuters, USA 2010). We will use RevMan 5 (Nordic Cochrane Centre, Cochrane Collaboration 2011) to prepare our review and we plan to use SAS 9.3 (SAS Institute Inc, USA 2011) for any meta-regression analyses. We will use Microsoft Excel to conduct synthesis of qualitative information.
3.3.3 Assessment of risk of bias in included studies
Two review authors will independently assess quality of studies and risk of bias for each study. The quality of the quantitative studies and qualitative studies will be separately assessed using different approaches.
3.3.3.1 Quantitative controlled studies
We will use the criteria recommended by the Cochrane Effective Practice and Organization of Care Group 1 to assess risk of bias for controlled studies, including randomised controlled trials and non-randomised studies that have a well-defined control group; and the methods outlined by NICE (2009) for other study designs (case control and cohort studies). The risk of potential bias will be assessed as low, high or unclear for each component. We will resolve any disagreement by discussion or by involving a third assessor. The risk of different biases for RCTs and other comparative studies, as outlined in by EPOC, is as follows:
• Random sequence generation (checking for possible selection bias)
For each included study we will describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups. A risk of bias is low for any truly random process (e.g. random number table, computer random number generator), or high for any non-random process (e.g. odd or even date of birth; hospital or clinic record number; assignment based on self-selection by participant or programme planner).
• Allocation concealment (checking for possible selection bias)
For each included study we will describe the method used to conceal allocation to interventions prior to assignment and will assess whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment. The risk is low if the allocation methods, such as telephone or central randomisation, consecutively numbered sealed opaque envelopes were used; and high for any open random allocation, unsealed or non-opaque envelopes, alternation, or date of birth.
• Baseline outcome measurement (checking for confounding/group equivalence)
For each included study we will describe whether outcomes were measured prior to the intervention, and the extent to which important differences were present across study groups. The risk is low if performance or patient outcomes were measured prior to the intervention, and no important differences were present across study groups, or if imbalanced but appropriate adjusted analysis was performed (e.g. analysis of covariance); and high if important differences were present and not adjusted for in analysis, or if no baseline measurement was conducted.
• Baseline characteristics (checking for confounding/group equivalence)
For each included study we will describe whether baseline characteristics are reported, and the extent to which important differences were present across study groups. The risk is low if baseline characteristics are reported and similar across groups, or if imbalanced but appropriate adjusted analysis was performed; and high if there is no report of characteristics in text or tables or if there are differences between groups which are not accounted for in adjusted analysis.
• Blinding of participants and personnel (checking for possible performance bias)
For each included study we will describe the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We will assess blinding separately for different outcomes or classes of outcomes.
• Contamination (checking for possible performance bias)
For each included study we will describe the likelihood that the control group received the intervention. The risk is low if allocation was by community, institution or practice and it is unlikely that the control group was exposed to the intervention (e.g. control group is geographically separated); and high if allocation was to individual or patient, and it is likely that the control group was exposed to the intervention (e.g. this is particularly likely if the intervention consists solely of information or training).
• Blinding of outcome assessment (checking for possible detection bias)
For each included study we will describe the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. The risk is low for outcomes measured objectively, or, for self-reported or subjectively measured outcomes, if outcome assessors were blinded; and high if outcome assessors were not blinded for self-reported or subjectively measured outcomes. We will assess blinding separately for different outcomes or classes of outcomes.
• Losses to follow-up (checking for possible attrition bias)
For each included study which includes baseline measurement, we will describe the extent of differential attrition between groups, and whether attrition is likely to bias the assessment of outcomes. The risk is low if attrition is not differential between groups, or is shown to be uncorrelated with risk factors; and high if attrition differs by groups and no evidence is presented to indicate systematic attrition by particular exposure groups.
• Selective reporting (checking for reporting bias)
For each included study we will describe how we investigated the possibility of selective outcome reporting bias and what we found. Where it is clear that all of the study's pre-specified outcomes and all expected outcomes of interest to the review have been reported, a low risk of bias will be documented. In contrast, the risk of bias will be regarded as high where not all the study's pre-specified outcomes have been reported, or one or more reported primary outcomes were not pre-specified, or outcomes of interest are reported incompletely and so cannot be used fully, or study fails to include results of a key outcome that would have been expected to have been reported.
• Overall risk of bias
We will make explicit judgements about whether studies are at high risk of bias, according to the criteria given in the Cochrane Handbook (Higgins 2011). We will assess the likely magnitude and direction of the bias and whether we consider it is likely to impact on the findings. We will explore the impact of the level of bias through undertaking sensitivity analyses if needed.
3.3.3.2 Interrupted time series studies
Quality of the findings of interrupted time series will be assessed by two independent review authors using the methods recommended by EPOC (2009). We will solve any disagreement by discussion or by involving a third assessor. We will assess each of the following criteria as done, not clear or not done. “Not clear” will be subsequently coded as “not done” if no further information is obtained from the authors.
Independence of the intervention to other changes (checking secular changes) whether the intervention occurred independently to other changes over time.
Appropriateness of data analysis
if there were sufficient data points to enable reliable statistical inference and a formal test for trend was used (requires at least 3 points recorded pre and post-intervention, and either a repeated measures analysis being performed or ANOVA or multiple t-test being used and at least 30 observations per data point).
• Correlation between intervention and data collection (checking detection bias)
if the intervention itself was unlikely to affect data collection, e.g. sources and methods of data collection were identical before and after intervention.
• Blinding assessment of primary outcomes
if clearly described in the original paper that the primary outcome variables had been assessed blindly or they were objective, such as length of hospital stay, or biochemical indicators (such as iron, haemoglobin, zinc concentrations) as assessed by a standardised test.
• Completeness of dataset
if dataset covered more than 80% of the total number of participants or episodes of care in the study.
3.3.3.3 Qualitative studies (or qualitative data reported within quantitative studies)
Two review authors will independently use core criteria adapted from the Critical Appraisal Skills Programme (CASP) checklist for appraising qualitative studies or qualitative content within quantitative studies (www.casp-uk.net). Any disagreement will be resolved by discussion or by involving a third assessor. These criteria are as follows:
Is the aim of the research clearly stated?
Is there a clear link to relevant literature/theoretical framework?
Does the paper include a clear description of:
the context?
the sample selection?
methods for data collection and recording?
methods of analysis?
3.3.3.4 Reliability of outcome measurement
Outcome measurement is considered reliable if two or more raters had at least 90% agreement or kappa at 0.8 or more; also if the outcome variables were collected from an automatic system, such as length of hospital stay or values of biochemical indicators. It is however scored “not clear” if reliability was not reported for outcome measures that had been obtained by chart extraction or collected by an individual.
3.3.4 Measures of treatment effect
Risk ratios and mean difference with 95% confidence intervals will be computed for dichotomous and continuous outcomes, respectively. In the case that a continuous outcome is measured differently among trials, the standardised mean difference may be used to combine trial results. If the data are very sparse, the Peto odds ratio will be used for dichotomous, and Mann-Whitney test for continuous data. For non-randomised studies, we will use adjusted effect sizes or other methods to address potential confounding.
If an outcome is measured at multiple time points in a controlled study, we will usually take the measure at longest follow-up.
If an outcome is measured at multiple time points in an interrupted time series study, we will compute a summary of effect size for each outcome at each time point separately, taking potential auto-correlation into account.
3.3.5 Unit of analysis issues
We will include cluster-randomised trials in the analyses along with individually randomised trials. Their sample sizes will be adjusted by the methods described in the Cochrane Handbook (Higgins 2011) using an estimate of the intracluster correlation coefficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC.
If we identify both cluster-randomised trials and individually-randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
We will also acknowledge heterogeneity in the randomisation unit and perform a sensitivity analysis to investigate the effects of the randomisation unit. A statistician will be involved in this part of the analysis.
3.3.6 Dealing with missing data and incomplete data
For each included study, and for each outcome or class of outcomes, we will describe the completeness of data including attrition and exclusions from the analysis. We will state whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomized participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information is reported, or can be supplied by the trial authors, we will re-include missing data in the analyses which we undertake. The risk of bias will be regarded as low if there were no missing outcome data or missing outcome data were balanced across groups; and high for any numbers or reasons for missing data imbalanced across groups, “as treated” analysis done with substantial departure of intervention received from that assigned at randomisation.
3.4 DATA SYNTHESIS
3.4.1 Quantitative Synthesis
As the review will include both quantitative and qualitative data, we propose a mixed design and mixed methods systematic review. A mixed-methods model is an appropriate way to address several research questions in the same systematic review. The review aims not only to address whether the nutrition interventions are effective, but to also explore more qualitatively why effects of interventions vary by setting and of possible approaches to overcome the barriers and increase the enablers of their implementation. The qualitative component will help extend the review by reporting evidence from qualitative studies or qualitative component of quantitative studies to address important aspects other than effectiveness including implementations, up-scaling, transferability and sustainability of the nutrition interventions.
We will use the principles and methods of the Campbell and Cochrane Collaborations (Higgins 2011) integrated with evaluation of program impact, context (setting, population characteristics, feasibility, sustainability, scalability) and analysis of barriers and enablers.
For interventional studies, we will conduct random-effects meta-analyses with an inverse variance weight when it is sensible to combine studies (clinical or statistical heterogeneity is not of high concern). The random-effects summary will be treated as the average range of possible treatment effects and we will discuss the clinical implications of treatment effects differing between trials. The results will be then presented as the average treatment effect with 95% confidence intervals, and the estimates of T2 and I2. If not appropriate to conduct meta-analyses and/or synthesise effect sizes, we plan to report review findings in tabular and narrative form.
We will report separate estimates of the intervention effects by study design. Findings of randomised studies will be presented separately for those of prospective cohort studies and of interrupted time series and cross-sectional studies.
Given the low incidence rates of the primary outcomes, we also plan to conduct power analysis, both of the individual studies and for the meta-analyses. If the meta-analysis could not be carried out, we plan to report forest plots together with an assessment of statistical power in the narrative review.
A cross-design synthesis will be considered only when sufficiently large number of studies included in the review might allow univariate and multivariate exploration of why differences in results might emerge from different study designs. In this situation, the assumptions underlying the comparison will be made explicit, and the possibility of design-related differences in effects will be critically examined.
If we obtain sufficient included studies and observe any variation in the covariates, a meta-regression using a random effects model will be carried out to identify any relation between the observed variables and the heterogeneity.
3.4.1.1 Assessment of heterogeneity
We will assess statistical heterogeneity in each meta-analysis using the T2, I2 and Chi2 statistics. We will regard heterogeneity as substantial if I2 is greater than 30% and either T2 is greater than zero, or there is a low P value (less than 0.10) in the Chi2 test for heterogeneity.
3.4.1.2 Investigation of Heterogeneity
The review aims to describe the effect of the intervention in different circumstances. The following moderators will be examined for their potential influence on the effect of the intervention on the primary outcomes: Participants Pregnant women versus lactating women versus pregnant or lactating women versus women of reproductive age who are not pregnant or lactating Settings (participants in low-income setting versus marginalised women from a high income setting) Nutritional status (undernourished versus not) Underlying diseases (with versus without) Risk of developing outcome (low versus high-risk) Area Level of urbanisation (rural versus urban area) Baseline maternal mortality rate (higher versus lower) Program characteristics Focus of the program (what does the program address? e.g. anaemia) Nature (stand-alone, embedded, integrated) Kinds of delivery Timing of the program (before pregnancy, during pregnancy, after pregnancy) Duration of the program Type of intervention (nutrition, non-nutrition); if nutrition, then type of nutrition supplement.
The primary outcomes will be used in subgroup analysis. For meta-analyses using methods other than inverse variance, we will assess differences between subgroups by inspection of the subgroups' confidence intervals (non-overlapping confidence intervals indicate a statistically significant difference in treatment effect between the subgroups) or we will apply interaction tests if possible.
3.4.1.3 Sensitivity Analysis
The potential effects of biases on the quality of the included trials will be assessed by sensitivity analysis. We will exclude the high-bias studies from the analysis to identify whether there are any substantive differences to the pooled result. The sensitivity analyses will be carried out to explore statistical heterogeneity and the effects of any assumptions made such as the value of the ICC used for cluster-randomized trials.
3.4.1.4 Assessment of Publication Bias
If there are 10 or more studies in a meta-analysis we will investigate reporting biases (such as publication bias) using funnel plots. We will assess funnel plot asymmetry visually, and use formal tests for funnel plot asymmetry. If asymmetry is detected in any of these tests or is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
3.4.2 Qualitative Synthesis
For qualitative data, we will use thematic analyses to synthesise qualitative findings through clear identification of prominent themes, and providing organised and structured ways of dealing with a large volume of literature under these themes.
4 Timeline
Submission of draft review: 15 August 2012
5 Acknowledgements
We would like to thank AUSAID for funding this review and for support provided by 3ie and IDCG.
Footnotes
8 Appendices
9 Contribution of Authors
All authors will contribute to applying methods, reviewing and editing content and interpreting results. Philippa Middleton has designed the search strategy and will conduct the searches. Zulfiqar Bhutta, Zohra Lassi, Tran Son Thach and Philippa Middleton will assess study eligibility, extract data, structure the results and produce review drafts. Tran Son Thach will provide statistical expertise, assisted by Philippa Middleton, Zulfiqar Bhutta and Zohra Lassi. Philippa Middleton, Tanya Bubner, Zulfiqar Bhutta, Zohra Lassi, Vicki Flenady and Caroline Crowther will provide expertise in qualitative methods and implementation strategies.
10 Declarations of Interest
All authors have published in the area of maternal nutrition. Professor Bhutta has conducted trials and other studies which may be considered for inclusion in this review. Professor Bhutta and Zohra Lassi are currently conducting or planning trials or studies which may be considered for inclusion in this review.