
Abstract
BACKGROUND
The problem, condition or issue
Violence against children includes all forms of violence under 18 years old, whether perpetrated by parents or other caregivers, peers, romantic partners, or strangers (World Health Organization [WHO, 2018]). As defined by The United Nations Children's Fund (UNICEF), violence is, “all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse” (UNICEF, 2017). It includes maltreatment, bullying, youth violence, intimate partner violence, sexual violence and emotional or psychological violence (detailed definition given in Appendix 1).
More than one billion children—half the children in the world—are victims of violence every year (Hillis et al., 2016). Global Burden of Disease estimates that 91.4% of deaths due to interpersonal violence occur in low- and middle-income countries (LMICs) and the rate of collective violence being 10 times higher in LMICs than high-income countries (HICs) (Mercy et al., 2017).
Violence, exploitation and abuse against children occur in the homes, families, schools, care and justice systems, workplaces and communities across all contexts, including as a result of conflict and natural disasters (UNICEF, 2011). Children are especially vulnerable to abuse, exploitation and trafficking (collective violence) during emergencies and armed conflicts. Children in different setting are exposed to various forms of violence including sexual abuse, armed violence, trafficking, child labour, gender-based violence, gang violence, peer-violence, corporal punishments, cyber bullying, female genital mutilation, violence in war/conflict affected region and child marriage (UNICEF, 2010).
A few striking features of childhood violence have drawn substantial international attention in recent years. First, violence exposure starts early in childhood through experience of corporal punishment as early as age. Second, much of the violence experienced by children is at the hands of adults who are typically to be found within a circle of trust and caregiving—parents, teachers, neighbours and authority figures. Third, there is also a striking rise in peer violence as children grow older and violence spills into peer relationships including through bullying [offline and online], dating and intimate partner violence, as well as gang violence (Know Violence in Childhood, 2017).
Evidence suggests that certain risk factors for violence may manifest differently across gender and age groups. WHO estimates that the highest child homicide rates occur in adolescents, especially boys, aged 15–17 years and among children 0–4 years old (WHO, 2004). A 2011 review estimated the global lifetime prevalence of childhood sexual abuse to be about 18% for girls compared with 8% for boys (Stoltenborgh, Van Ijzendoorn, Euser, and Bakermans-Kranenburg, 2011). Girls all over the world are victims of child marriage, forced pregnancy, female genital mutilation, trafficking and child labour. The situation is alarming in LMICs because of higher rates of violence against girls as compared to HICs (WHO, 2013). In schools and other education settings boys seem to be more at risk than girls for harsh physical punishment and abuse. As per Global School-based Student Health Survey (GSHS) reports of physical violence among students aged 13–15 are relatively common and are more in boys than girls (GSHS, 2013). Children in war-affected regions of the world are vulnerable and easy targets for coercion. In 2016, the United Nations (UN) verified over 20,000 incidents of child violation in regions of armed-conflict (UN, 2017).
Figure 1 describes the classification of violence as stated in World report on Violence and Health (WHO, 2002). According to the report, violence is categorised into self-directed violence, interpersonal violence and collective violence based on victim-perpetrator relationship. Interpersonal violence includes family, intimate partner and community violence whereas collective violence encompasses larger group of people such as social, political and economic violence (Krug, Dahlberg, Mercy, Zwi & Lozano, 2002). The focus of present Evidence and Gap map (EGM) is only on interpersonal and collective violence against children. This map excludes self-directed violence and neglect as this is the scope of an on-going EGM on child abuse and neglect in LMICs (Sinha, Radhika, Jha & John, 2018). Structural violence is also beyond the scope of this map as the factors leading to and interventions to reduce/prevent such form of violence are far more complex than explanations would imply.
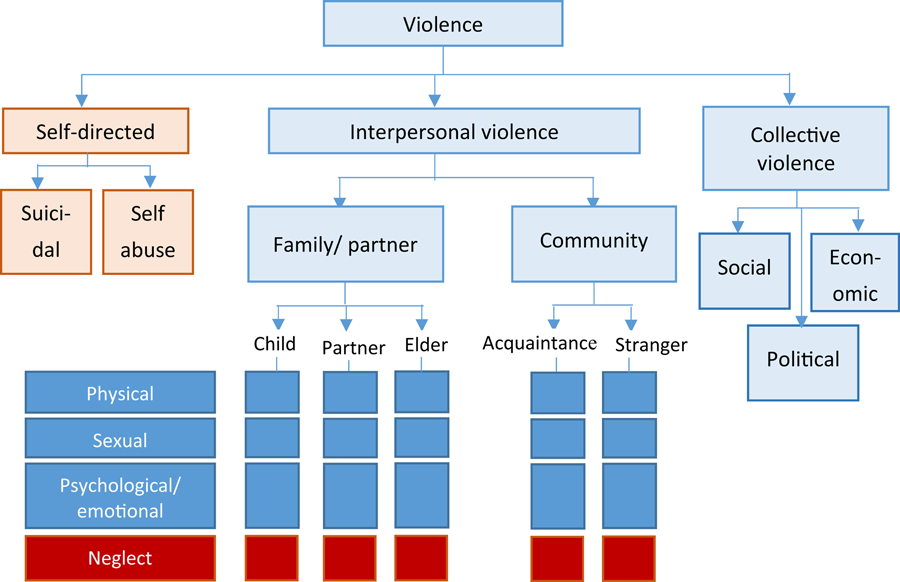
Typology of violence (Source: WHO, 2002), and areas (in blue) covered by the present Evidence and Gap map (EGM) [Color figure can be viewed at wileyonlinelibrary.com]
Violence experienced by children is of concern because of the serious intergenerational impacts on the future wellbeing of children. Experience of violence during childhood increases the risk of becoming victims or perpetrators of violence during adulthood (WHO, 2007). Violence can negatively affect physical, mental, sexual, and reproductive health, and may increase the risk of acquiring human immunodeficiency virus (HIV) in some settings (WHO, 2017). Violence against children is associated with poor education outcomes, economic insecurity including food insecurity, parental unemployment, inadequate housing and other basic necessities for children and families in LMICs (Peterman, Neijhoft, Cook, & Palmero, 2017). The global costs related to physical, psychological and sexual violence have been estimated to be between 3% and 8% of global GDP (Pereznieto, Montes, Langston, & Routier, 2014).
Although experiencing violence in childhood impacts lifelong health and well-being, it is often preventable (World Health Organization, 2018). As part of the post-2015 sustainable development goals (SDG) agenda, the UN issued a global call-to-action: to eliminate violence against children (United Nations Development Programme [UNDP, 2017]). In recognition of this, a specific target [SDG 16.2] was included in the 2030 Agenda for Sustainable Development giving renewed impetus towards the realisation of the right of every child to live free from fear, neglect, abuse and exploitation. Several other SDG targets address specific forms of violence such as eliminating violence against women and girls in public and private spheres [SDG 5.2], eliminating harm towards children such as child marriage and female genital mutilation [target 5.3], promotion of nonviolent educational environment [SDG 4.7] and the eradication of child labour, including the recruitment and use of child soldiers [target 8.7]. The year 2019 also marks the 30th anniversary of the adoption of the UN Convention on the Rights of the Child (CRC), which provides an important opportunity to gain a better understanding of the nature, extent and causes of violence against children.
Finally, the launch of the Global Partnership to End Violence against Children in 2016, serves as a global platform whose aim is “ending violence against children in every country, every community and every family” (End Violence Against Children, 2018). As part of the SDGs, the UN General Assembly has made a global commitment to ending all forms of violence against children. A technical package supporting seven evidence-based strategies to end violence against children—INSPIRE—developed by the WHO and nine other international agencies and initiatives, has been widely promoted and adopted as an essential tool in supporting national investments and actions towards realising this commitment (WHO-INSPIRE, 2016).
In response to above there is an increased need to invest in generating sound evidence on effective strategies to prevent or end violence against children, in order to strengthen the evidence to policy architecture in this area. There has been a substantial increase in recent years in pilot programmes testing violence prevention strategies, many of which have contributed to the strategies prioritised in the INSPIRE technical package. However, there are still many gaps in the evidence base from these programmes, including geographical gaps, thematic gaps and missing information that constrain the building of a concerted evidence-informed policy and investment agenda. EGMs can contribute by providing an overview of available quality studies, identifying gaps and thereby supporting the prioritisation of global evidence synthesis needs and primary data collection.
In order to move towards the ambitious targets laid out in the SDGs, it is likely that substantial improvements in resource allocation will be needed to promote interventions which are effective in improving outcomes in particular contexts. The purpose of this evidence and gap map is to assist policy-makers and practitioners in gaining access to evidence on the effectiveness intervention to reduce violence against children. This will also help to identify research gaps with little or no evidence synthesis and to provide a resource for informing policy and practice. The EGM does not replace other primary research or address specific methodological or other gaps, but lays out an assessment of evidence availability in order to guide further research investment.
Conceptual framework of the EGM
Violence prevention is a complex field, involving a variety of strategies addressing different risk factors that are enmeshed in familial and social relationships, determined often by power inequalities as well as learned social behaviours and norms. In order to build on advances in the field of violence prevention, this EGM draws on the same framework developed by WHO and partners in recent years. The INSPIRE framework has been identified as the basis for the intervention-outcome framework for the present EGM (WHO-INSPIRE, 2016). 1 The INSPIRE framework supports the SDGs aiming to reduce significantly all forms of violence and related death rates everywhere. The seven INSPIRE strategies are supported by and contribute to activities aimed at achieving several SDG goals that target risk factors for violence against children, including those that address poverty, health, gender equality, education, safe environments and justice, and are therefore important to include in programming to prevent violence against all children (WHO-INSPIRE, 2016).
The INSPIRE technical package presents strategies based on the best available evidence to help countries and communities intensify their focus on the prevention programmes and services with the greatest potential to reduce violence against children, applicable to their contexts. The ambition of INSPIRE is to provide a unifying approach to the field of violence prevention. 2 The use of the INSPIRE framework to guide the design of the EGM will help purposively update the field of knowledge supporting INSPIRE and point to specific gaps and priorities that will need attention.
Figure 2 shows how this EGM builds on the seven strategies of the INSPIRE framework to develop intervention and outcome categories.
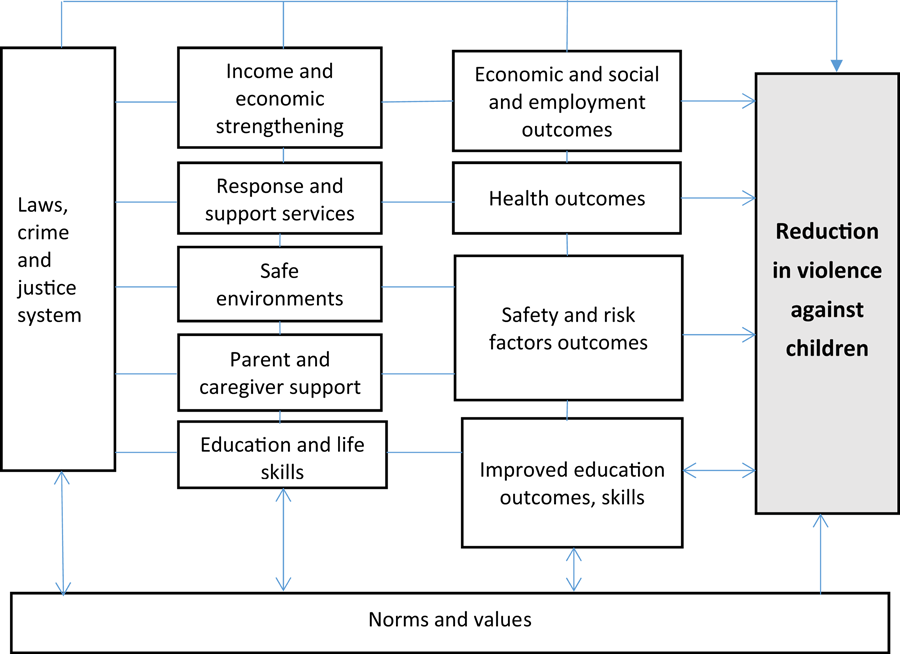
Conceptual framework for intervention and outcomes to reduce violence among children (Source: Authors' own design) [Color figure can be viewed at wileyonlinelibrary.com]
The scope of this EGM is to capture all the effectiveness studies on reducing interpersonal violence and collective violence against children in LMICs. In so doing, the EGM will contribute to broadening the included interventions and outcomes in the INSPIRE framework to better reflect the state of evidence on violence against children, and independently provide an updated overview of knowledge and evidence gaps for the field.
The intended users are policymakers and funding organisations which are working to reduce interpersonal violence against children. The present EGM will provide an overview of all available evidence on the key outcome domains and interventions aimed at reducing violence against children in LMICs using an intervention-outcome framework. It will identify areas in which there are existing bodies of synthesised knowledge to inform policy, and those areas in which there is little or no evidence synthesis.
The EGM will include studies of effectiveness of violence prevention strategies such as experimental and nonexperimental evaluations and systematic reviews. It does not aim to synthesise key messages from the available evidence but will only map the availability of quality evidence on childhood violence prevention based on the INSPIRE framework. As the EGM is focused on documenting availability of evidence, coverage of the breadth of strategies in the INSPIRE framework will be feasible and also strategic as identified above.
The scope of the EGM is defined by a framework of intervention and outcomes presented in two dimensions: the rows lists seven interventions and its subcategories, and seven outcome domains as columns. Each cell shows studies which contain evidence on that combination of intervention and outcome. Included studies are coded for additional characteristics as filters, such as population subgroup, context, country, region and type of violence, nature of violence and conflict-affected regions.
Existing EGMs and/or relevant systematic reviews
The child welfare mega map (UNICEF Research Brief, 2018) was a basis for developing the present EGM. The mega map identified gaps in the area of violence against children in LMICs. The present EGM is an outcome of the findings of mega map which found, the evidence for protecting children from violence and exploitation is low in LMICs, nonetheless it is a priority area for policy and practice (UNICEF Research Brief, 2018).
There are four additional related ongoing maps. There is a map on child maltreatment and neglect which is restricted to HICs (Kornør, John, Brynhildur, Biedilæ, & Albers, 2017). A second map for LMICs focuses on child neglect (Sinha, Radhika, Jha, & John, 2018), whereas we will focus on child violence (we elaborate on this distinction below). The third map registered by Albers et al. (2019) is about institutional responses to child maltreatment, not focussing on any specific region. The fourth evidence and gap map is an unpublished work undertaken by Institute for Security Studies in partnership with the University of Johannesburg and Wits University to address violence against women and children in South Africa. There is no existing EGM for violence against children in LMICs on a global scale.
OBJECTIVES
The objective of this EGM is to provide an overview of the existing evidence base and gaps in evidence aimed at reducing violence against children in LMICs using an intervention-outcome framework.
Consistent with this, the EGM will Identify existing gaps in evidence to better inform future investment in research. Identify clusters of primary studies that offer opportunities for evidence synthesis. Identify, appraise and summarise existing evidence from systematic reviews of the effect of intervention to reduce violence against children.
Defining evidence and gap maps
EGMs are evidence collections that map out existing and ongoing systematic reviews or primary studies in a sector or subsector. The EGMs are presented in two dimensions the rows list interventions and the column list outcome domains. Each cell shows studies which contain evidence on that combination of intervention and outcomes.
EGM framework
The EGM framework will inform the inclusion and exclusion criteria of the EGM. Here, we describe the population, intervention, comparison, outcomes (indicators) and study designs for the map (Table 1).
Intervention categories, subcategories and examples
Intervention categories, subcategories and examples
The primary population of interest for this map is children and adolescents from LMICs. LMICs are defined by World Bank as low-income economies—those with a Gross National Income (GNI) <$995; lower middle-income economies—those with a GNI per capita between $996 and $3,895; and upper middle-income economies—those with a GNI per capita between $3,896 and $12,055 (The World Bank, 2018). As defined in the INSPIRE handbook, “Child” means any person aged under 18 years (WHO-INSPIRE, 2018). Following the guideline, children irrespective of their sex in the age group of ≤18 years will be included in the EGM. The age group is classified based on the WHO age criteria stated as follows: infanthood (<3 years of age), childhood (3–10 years), adolescence (10–18 years) (WHO-GAA, 2017).
Population subgroup of interest includes girls, orphans and vulnerable children, children with disabilities, children belonging to ethnic minorities, child sex workers, child brides, isolated children/street children, children with HIV/acquired immunodeficiency syndrome (AIDS), migrants and children affected by conflict and humanitarian crises, including refugees and child soldiers.
Intervention
This EGM is focused on effectiveness studies of interventions where the primary aim is the reduction of violence against children. The intervention-outcome framework is based on the INSPIRE framework which identifies seven evidence-based strategies to prevent violence against children viz. implementation and enforcement of laws; norms and values; safe environments; parent and caregiver support; income and economic strengthening; response and support services; and education and life skills (WHO-INSPIRE, 2016). The intervention categories are based on the seven strategies of INSPIRE, however, the subcategories are based on pilot coding of key 30 studies, expert advice and discussion within the team and advisory members The deviation from the INSPIRE strategies for the first category viz. implementation and enforcement of laws, which was kept as laws, crime and justice in the present map. This deviation was based on the pilot coding of studies. For an EGM it is best practice to have fewer subcategories so that complex interventions can be coded correctly and avoid unnecessary overlap between subcategories.
Table 1 lists the intervention categories and subcategories. Examples of programme names are given in brackets. These are listed to aid with search and coding. They will not appear in the subcategory label in the map. The included interventions cover all main strategies to reduce violence against children outcomes operating across different contexts and relations where risks exist—from the individual level to families, communities, institutions and societies. The subcategories of interventions are largely based on INSPIRE guidelines, definitions for which are given as Appendix 1.
The intervention categories included in our map are: Law, crime and justice system Norms and values Safe environment Parent, child and caregiver support Income and economic strengthening Response and support services Education and life skills.
The outcomes domains and subdomains will be the main categories and subcategories across the interventions in our map. The included studies should have a component of ending or reducing violence against children as a primary outcome. The seven main outcome categories are listed in the Table 2 given below:
Outcome domains and subdomains
Outcome domains and subdomains
Types of study designs
Systematic reviews and impact evaluation or studies of effectiveness will be included for the EGM. Systematic reviews collating data on the effectiveness of interventions to prevent violence against children, child marriages and child labour will be included in the EGM. Systematic reviews containing one or more studies from LMICs will be included. Among primary studies, the best evidence is provided by randomised controlled trials (RCT), but for the present map, non-RCTs will be used as a supplement to the available evidence in a particular area. Impact evaluation studies using quantitative data to evaluate the effectiveness of the intervention will be included based on the primary outcome of interest in the study viz. violence against children which includes direct violence inflicted on children, child marriages and child labour.
The dearth of RCTs is anticipated because in some cases or when addressing some issues related to violence, RCTs could be unethical. For non-RCTs, a pretest of the outcome measure and relevant demographic characteristics, and/or statistical control of such characteristics will be present as a criteria for inclusion of pre–post test studies with or without comparison group. The study designs which will be included in the EGM are as follows: systematic reviews and impact evaluations done as—RCTs, quasi-experimental studies, analytical observational (cohort studies), Modelling with empirically grounded parameters (instrumental variables), controlled before-after studies and interrupted time-series. Relevant on-going studies will be included.
Treatment of qualitative research
We do not plan to include qualitative research in the EGM.
Types of settings
All types of settings, where interventions for violence against children were implemented, will be included in the EGM. On the basis of the framework, the settings may be: school, home, centre or facility, community and so on.
Status of studies
Relevant ongoing studies will be included in the EGM.
The detailed eligibility criteria is given in Appendix 3.
Search strategy and status of studies
The search will be as comprehensive as possible, using (but not limited to) relevant bibliographic databases, web-based search engines, websites of specialist organisations, bibliographies of relevant reviews, and targeted calls for evidence using professional networks or public calls for submission of articles.
Additionally, citation searches of included studies in Google Scholar, Scopus and Web of science will be performed. Reference lists of the included reviews will be reviewed (Appendix 2).
Databases
Systematic review databases 3ie Systematic Review Database Campbell Collaboration Cochrane Collaboration for Environmental Evidence EPPI Centre Evaluation Database of Education Research PROSPERO Research for Development Swedish Agency FOR Health Technology Assessment and Assessment of Social Services Epistomonikos Academic databases Applied Social Sciences Index and Abstracts (ASSIA) CABI's Global Health Caribbean Child Development Centre Online Publication Database CINAHL EBSCO EBSCOhost (Caribbean Search) Econlit Eldis Embase Emerald insight ERIC Google Scholar International Bibliography of Social Sciences (IBSS) IDEAS-Repec Popline JGATE JOLIS JSTOR MEDLINE PsycINFO PubMed RedALyC (La Red de Revistas Científicas de América Latina, el Caribe, España y Portugal) SafetyLit SciELO SCOPUS Social Science Research Network (SSRN) Sociological abstracts (ProQuest) The National Bureau of Economic Research (NBER) Web of Science WHO's Global Health Library International Organisations (Bilateral and multilateral) DFID (including Research for Development (R4D) ILO IOM Save the Children UN Women UNDP UNFPA Evaluation Database UNHCR UNICEF UNICRI UNODOC USAID WHO/PAHO Grey Literature search/websites Abdul Latif Jameel Poverty Action Lab (J-PAL) Action against Hunger Action Aid http ADOLEC African Development Bank Africa-Wide Africaportal.org African journals online (AJOLS) Anulib Association for the Development of Africa British Library for Development Studies CAF Development Bank of Latin America CARE CEPAL/ECLAC—Economic Commission for Latin America and the Caribbean Child and Youth Finance International CIFF Clinton Foundation Concern Worldwide Division for Social Policy & Development Child Fund International Fórum Brasileiro de Segurança Pública CPC Learning Network EU CORDIS Gates Foundation GreyNet International Innovations for Poverty Action (IPA) Database International Center for Research on Women (ICRW) Inter-American Development Bank (IADB) International Food Policy Research Institute (IFPRI) International Rescue Committee (IRC) International Red Cross IPC-IG (Working papers) Joanna Briggs Institute Evidence-Based Practice Database LLC/Centre for Human Services LTSHM MedCarib Medecins Sans Frontières Oak Foundation One International Opengrey Organization of American States (OAS) Overseas Development Institute Project Concern Proquest Dissertations & Theses RAND Corporation Sexual Violence Research Initiative (SVRI) Social Care Online UN Economic and Social Council UNESCO UNICEF Innocenti Research Centre University Research Co. United Nations Population Fund Urban Youth Evidence Synthesis Valid International Working Group on Early Childhood Development World Bank Group (WBG) Within WBG: Spanish Impact Evaluation Fund (SIEF) Within WBG: Korean Trust Fund (KTF) World Food Programme World for World Organization World Vision.
All titles and abstracts, and then full text, will be double screened, with a third-party arbitrator or in the event of disagreement. The screening tool is given as Appendix 4. Automation will not be used.
Data extraction, coding and management
Coding will be done independently by two coders, with a third-party arbitrator or in the event of disagreement.
Quality appraisal
The quality of the included systematic reviews will be assessed using AMSTAR 2 (Shea et al., 2017) and done independently by two reviewers. We will quality rate the primary studies (individual studies) based on the quality assessment tool for individual studies as described below. The quality assessment of all systematic reviews will be done and it will be aimed to be completed for primary studies within the set deadlines.
Due to the extensive grey literature aimed to be searched, the authors anticipate low/medium quality studies, from LMICs, can be included in the EGM. Studies will not be excluded based on the quality assessment and a colour coding will show the studies with different quality ratings on the map.
The tool used to assess study quality is shown in Appendix 5. This tool includes six criteria that are appropriate for the assessment of quantitative impact evaluations. These are as follows:
Study design (potential confounders taken into account): Impact evaluations need either a well-designed control group (preferably based on random assignment) or an estimation technique which controls for confounding and the associated possibility of selection bias.
Power calculations: Small sample size can result in an under-powered study with a high risk of not detecting an effect from the intervention when there actually is one. The combination of under-powered studies and publication bias can put an upward bias on the assessment of the overall effect size from a body of literature. The problem of sample size is addressed by conducting power calculations before the study to determine the required sample size. We will not use this item in the overall assessment of the study. However coding mention of power calculations signals the importance of both conducting and reporting power calculations.
Attrition or losses to follow up: Can be a major source of bias in studies, especially if there is differential attrition between the treatment and comparison group (called the control group in the case of RCTs) so that the two may no longer be balanced in pre-intervention characteristics. The US Institute of Education Sciences What Works Clearing House (WWC) has developed standards for acceptable levels of attrition, in aggregate and the differential, which are applied here.
Clear definition of violence: for a study to be useful the study population must be clear, which means that the type and degree of violence should be clearly defined, preferably with reference to a widely-used international standard.
Description of intervention: If the intervention is not well described then the evidence may be misinterpreted to support an intervention not actually supported by study findings. For example, “case work” or “shelter” are very broad descriptions, so more detail of the intervention is required so as to know what is actually being evaluated. We rate as low if the description is just named with no description, medium if there is a short description, and high if there is a detailed description. We do not use this item in the overall assessment of the study.
Definition of outcomes: Outcomes should be clearly defined so that study findings can be properly interpreted. So far as possible, unless a subjection perception is required, that questions should rely on objective factors, and utilise data collection instruments which have been validated for the context in which they are being applied. We rate as high of there is clear definition of the outcome and how it is being measured, or reference to an existing tool. Medium rating is given is if there is a brief description, and low if the outcome is named but not adequately described.
Baseline balance: Baseline balance means that the treatment and comparison groups have the same average characteristics at baseline, not only for outcomes but also for other factors which may affect the impact of the programme such as a prior history of parental alcohol abuse. We rate low confidence on study findings if baseline balance is not reported for non-RCTs or it is reported and there is a significant difference of 10% or >10%, medium confidence if imbalance is between 5% and 10%, and high if an RCT or if imbalance is 5% or <5%.
Overall assessment: The overall assessment uses a weakest link in the chain principle so that the overall assessment is the lowest of assessment given to any of the relevant items. As mentioned above, not all items are used in this assessment. So the overall assessment is the lowest of the assessments for items 1, 4, 6 and 7.
Many difficult ethical dilemmas may arise when gathering information among children and adolescents. Given the obvious sensitive nature of research into violence against children, it is indeed challenging to conduct studies assessing violence against children. Despite experience, education, and good intentions, skilled professionals often find themselves questioning how to proceed with their activities with young people. Every person has a right to privacy, hence preserving the confidentiality of personal information is one of the fundamental principles governing the collection of data about individuals. In line with the above stated challenges, an ethical coding tool for measuring ethical standards of primary intervention/effects study was developed (Council for International Organisations of Medical Sciences, 2009; Population Council, 2005; Save the Children, 2004; WHO-Ethical and Safety Recommendations, 2007). The nine item tool has five critical and four noncritical items. The scoring is done as ‘Strong ethical standards’, ‘Moderate ethical standards’ and ‘weak ethical standards’. The complete tool with scoring is given in Appendix 6. No study will be disqualified based on adequacy of ethical standards. Findings of the ethical considerations will be presented in report.
ANALYSIS AND PRESENTATION
Unit of analyses
Each entry in the map will be a systematic review or a primary study of effectiveness. The final EGM will identify the number of studies covered by the map in each sector or subsector.
Presentation
In addition to the interventions and outcomes, the following filters will be coded: Population subgroups: The age group is classified based on the WHO age criteria stated as follows: infanthood (<3 years of age), childhood (3–10 years) and adolescence (10–18 years). Context: Very high prevalence settings • Pregnant women, orphans, juvenile offenders, children with disabilities, children belonging to ethnic minorities, child sex workers, child brides, isolated children/street children, children with HIV/AIDS, male, female, LGBTQ, father, mothers. Region: East Asia & Pacific, Europe & Central Asia, Latin America & Caribbean, Middle East & North Africa, North America, South Asia, Western Central Africa, Eastern Central Africa Country Economies: Low-income economies, Lower-middle-income economies, Upper-middle-income economies, High-income economies Type of violence: Interpersonal violence Family (intimate partner/community) Collective violence: Social/political/economic (riot, conflict) Nature of violence: Physical Sexual Emotional/psychological Polyvictimization. Conflict-affected regions: This will be defined based on Department for International Development (DFID) list of conflict affected regions updated as per current year (2018/2019).
The EGM report shall provide tabulations or graphs of the number of studies, with accompanying narrative description, by Intervention category and subcategory Outcome domain and subdomain Table of “aggregate map” of interventions and outcomes Region Year Study type Type of violence Population subgroups.
STAKEHOLDER ENGAGEMENT
An advisory group was formed at the inception stage of this EGM. Feedback from the group members was received and assimilated in the framework plan at the title registration stage. The stakeholders will be engaged at all stages of the EGM to review and comment on interventions, studies, outputs, map findings and provide advice on dissemination channels.
This map is commissioned by UNICEF Innocenti who will take the lead in introducing the map into relevant policy discussions. The advisory group members for this EGM includes experts from all the pillars of INSPIRE framework as social, economic, education, health and wellbeing and they have been involved in working towards Violence against children in their fields including use of INSPIRE. Through a joint effort by UNICEF Innocenti and the advisory group members we are positive that this work will contribute to greater alignment of global and national efforts and will form the basis for improving the evidence base on violence against children in low and middle income countries.
The advisory group members for the EGM are as follows: Dr. Karen Devries, Associate Professor in Social Epidemiology, LSHTM Professor Lorraine Sherr, Head of Health Psychology Unit, Institute of Global Health, UCL Professor J. (Julia) Sloth-Nielsen, Professor, Department of Public Law and Jurisprudence, University of the Western Cape and Professor of Children's Rights in the Developing World, University of Leiden Shivit Bakrania, Knowledge Management Specialist, Research Facilitation and Knowledge Management unit, UNICEF Innocenti Centre Professor A.K. Shiva Kumar, Global Co-Chair, Know Violence in Childhood Professor Andrés Villaveces, Senior Scientist, Division of Violence Prevention, NCIPC, US Centers for Disease Control and Prevention, and Department of Epidemiology, University of North Carolina (UNC), Chapel Hill Dr. Amber Peterman, Consultant, UNICEF Innocenti Centre and Associate Adjunct Professor at UNC Chapel Hill Dr. Lucie Cluver, Professor of Child and Family Social Work, Centre for Evidence-Based Social Intervention in the Department of Social Policy and Intervention, Oxford University Professor Rebecka Lundgren, Deputy Director and Research Director, Institute for Reproductive Health, Georgetown University Dr. Charlene Coore Desai, Resident Advisor, USAID Applying Science to Strengthen and Improve Systems (ASSIST) Project, Jamaica Dr. Kerry Albright, Chief, Research facilitation and Knowledge management, UNICEF Innocenti Centre
ROLES AND RESPONSIBILITIES
Content:
Ramya Subrahmanian has an extensive experience in research, policy advocacy, training and teaching. She has experience in use of evidence across all of UNICEF's policy areas. In her previous capacity as Executive Director, Know Violence in Childhood, she oversaw the commissioning of over 45 new papers on violence prevention including systematic reviews on LMICs, as well as the publication of an updated annotated bibliography.
EGM methods:
Ashrita Saran and Howard White have previous experience in systematic review methodology, including searching, data collection, and theory-based synthesis, which means they are proficient in carrying out the various processes in an EGM, such as search, eligibility screening, quality assessment and coding. They have undertaken an overview of approaches to mapping in a range of organisations. Jill Adona is an experienced screener and coder who has previously worked on Campbell Collaboration research projects. Jill has attended training workshops on evidence synthesis provided by both 3ie and Campbell. Prachi Pundir has experience in systematic reviews and has previously worked on systematic reviews and meta-analysis with Public Health Evidence South Asia, Manipal and all authors are proficient in carrying out the various processes in an EGM, such as eligibility screening, quality assessment and coding.
Information retrieval:
Ashrita Saran, and Prachi Pundir have training in designing and implementing search strategies.
SOURCES OF SUPPORT
The funding for this research is supported by UNICEF Office of Research - Innocenti. The deliverable deadline for the EGM is August 31, 2019.
DECLARATIONS OF INTEREST
The authors declare there is no conflict of interest.
PRELIMINARY TIMEFRAME
Approximate date for submission of the EGM: July 31, 2019.
PLANS FOR UPDATING THE EGM
Once completed, the EGM will be updated yearly, provided we have availability of funds. The lead author and/or the corresponding authors will be responsible for updating the EGM.
Footnotes
In 2018, follow-up resources on INSPIRE technical package were published. “INSPIRE indicator guidance and results framework” (UNICEF-INSPIRE, ![]() ) and “INSPIRE handbook: action for implementing the seven strategies” were the two resources to improve the implementation and use of the guidelines (UNICEF, 2018; WHO, 2018). The “INSPIRE handbook” explains in detail how to choose and contextually implement interventions and “Indicator Guidance and Results Framework” is designed to help governments and agencies to monitor progress and track change over time when INSPIRE strategies are implemented.
) and “INSPIRE handbook: action for implementing the seven strategies” were the two resources to improve the implementation and use of the guidelines (UNICEF, 2018; WHO, 2018). The “INSPIRE handbook” explains in detail how to choose and contextually implement interventions and “Indicator Guidance and Results Framework” is designed to help governments and agencies to monitor progress and track change over time when INSPIRE strategies are implemented.
Violence is rooted in social, economic and cultural factors that impact communities, families, relationships and the children's experiences of their daily lives. The social ecological model (given on page 17 of INSPIRE guidelines document; WHO-INSPIRE, ![]() ) depicts this interplay of individual, relationship, community and societal factors. Individual-level factors include biological and personal history aspects such as sex, age, education, income, habits; Close-relationship level factors include parenting practices, family, separation, peers; Community-level factors include schools, workplaces and neighbourhoods and society-level risk factors include legal and social norms including health, economic, educational and social policies.
) depicts this interplay of individual, relationship, community and societal factors. Individual-level factors include biological and personal history aspects such as sex, age, education, income, habits; Close-relationship level factors include parenting practices, family, separation, peers; Community-level factors include schools, workplaces and neighbourhoods and society-level risk factors include legal and social norms including health, economic, educational and social policies.