
Abstract
Background
Almost two billion people who are deficient in vitamins and minerals are women and children in low- and middle-income countries (LMIC). These deficiencies are worsened during pregnancy due to increased energy and nutritional demands, causing adverse outcomes in mother and child. To reduce micronutrient deficiencies, several strategies have been implemented, including diet diversification, large-scale and targeted fortification, staple crop bio-fortification and micronutrient supplementation.
Objectives
To evaluate and summarize the available evidence on the effects of micronutrient supplementation during pregnancy in LMIC on maternal, fetal, child health and child development outcomes. This review will assess the impact of single micronutrient supplementation (calcium, vitamin A, iron, vitamin D, iodine, zinc, vitamin B12), iron-folic acid (IFA) supplementation, multiple micronutrient (MMN) supplementation, and lipid-based nutrient supplementation (LNS) during pregnancy.
Search Methods
We searched papers published from 1995 to 31 October 2019 (related programmes and good quality studies pre-1995 were limited) in CAB Abstracts, CINAHL, Cochrane Central Register of Controlled Trials, Embase, International Initiative for Impact Evaluations, LILACS, Medline, POPLINE, Web of Science, WHOLIS, ProQuest Dissertations & Theses Global, R4D, WHO International Clinical Trials Registry Platform. Non-indexed grey literature searches were conducted using Google, Google Scholar, and web pages of key international nutrition agencies.
Selection Criteria
We included randomized controlled trials (individual and cluster-randomized) and quasi-experimental studies that evaluated micronutrient supplementation in healthy, pregnant women of any age and parity living in a LMIC. LMIC were defined by the World Bank Group at the time of the search for this review. While the aim was to include healthy pregnant women, it is likely that these populations had one or more micronutrient deficiencies at baseline; women were not excluded on this basis.
Data Collection and Analysis
Two authors independently assessed studies for inclusion and risk of bias, and conducted data extraction. Data were matched to check for accuracy. Quality of evidence was assessed using the GRADE approach.
Main Results
A total of 314 papers across 72 studies (451,723 women) were eligible for inclusion, of which 64 studies (439,649 women) contributed to meta-analyses. Seven studies assessed iron-folic acid (IFA) supplementation versus folic acid; 34 studies assessed MMN vs. IFA; 4 studies assessed LNS vs. MMN; 13 evaluated iron; 13 assessed zinc; 9 evaluated vitamin A; 11 assessed vitamin D; and 6 assessed calcium. Several studies were eligible for inclusion in multiple types of supplementation. IFA compared to folic acid showed a large and significant (48%) reduction in the risk of maternal anaemia (average risk ratio (RR) 0.52, 95% CI 0.41 to 0.66; studies = 5; participants = 15,540; moderate-quality evidence). As well, IFA supplementation demonstrated a smaller but significant, 12% reduction in risk of low birthweight (LBW) babies (average RR 0.88, 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; high-quality evidence). MMN supplementation was defined as any supplement that contained at least 3 micronutrients. Post-hoc analyses were conducted, where possible, comparing the differences in effect of MMN with 4+ components and MMN with 3 or 4 components. When compared to iron with or without FA, MMN supplementation reduced the risk of LBW by 15% (average RR 0.85, 95% CI 0.77 to 0.93; studies = 28; participants = 79,972); this effect was greater in MMN with >4 micronutrients (average RR 0.79, 95% CI 0.71 to 0.88; studies = 19; participants = 68,138 versus average RR 1.01, 95% CI 0.92 to 1.11; studies = 9; participants = 11,834). There was a small and significant reduction in the risk of stillbirths (average RR 0.91; 95% CI 0.86 to 0.98; studies = 22; participants = 96,772) and a small and significant effect on the risk of small-for-gestational age (SGA) (average RR 0.93; 95% CI 0.88 to 0.98; studies = 19; participants = 52,965). For stillbirths and SGA, the effects were greater among those provided MMN with 4+ micronutrients. Children whose mothers had been supplemented with MMN, compared to IFA, demonstrated a 16% reduced risk of diarrhea (average RR 0.84; 95% CI 0.76 to 0.92; studies = 4; participants = 3,142). LNS supplementation, compared to MMN, made no difference to any outcome; however, the evidence is limited. Iron supplementation, when compared to no iron or placebo, showed a large and significant effect on maternal anaemia, a reduction of 47% (average RR 0.53, 95% CI 0.43 to 0.65; studies = 6; participants = 15,737; moderate-quality evidence) and a small and significant effect on LBW (average RR 0.88, 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; high-quality evidence). Zinc and vitamin A supplementation, each both compared to placebo, had no impact on any outcome examined with the exception of potentially improving serum/plasma zinc (mean difference (MD) 0.43 umol/L; 95% CI −0.04 to 0.89; studies = 5; participants = 1,202) and serum/plasma retinol (MD 0.13 umol/L; 95% CI −0.03 to 0.30; studies = 6; participants = 1,654), respectively. When compared to placebo, vitamin D supplementation may have reduced the risk of preterm births (average RR 0.64; 95% CI 0.40 to 1.04; studies = 7; participants = 1,262), though the upper CI just crosses the line of no effect. Similarly, calcium supplementation versus placebo may have improved rates of pre-eclampsia/eclampsia (average RR 0.45; 95% CI 0.19 to 1.06; studies = 4; participants = 9,616), though the upper CI just crosses 1.
Authors' Conclusions
The findings suggest that MMN and vitamin supplementation improve maternal and child health outcomes, including maternal anaemia, LBW, preterm birth, SGA, stillbirths, micronutrient deficiencies, and morbidities, including pre-eclampsia/eclampsia and diarrhea among children. MMN supplementation demonstrated a beneficial impact on the most number of outcomes. In addition, MMN with >4 micronutrients appeared to be more impactful than MMN with only 3 or 4 micronutrients included in the tablet. Very few studies conducted longitudinal analysis on longer-term health outcomes for the child, such as anthropometric measures and developmental outcomes; this may be an important area for future research. This review may provide some basis to guide continual discourse around replacing IFA supplementation with MMN along with the use of single micronutrient supplementation programs for specific outcomes.
Linked Article
PLAIN LANGUAGE SUMMARY
Micronutrient and vitamin supplementation during pregnancy improves some maternal and child health outcomes
Micronutrients and vitamins are important for the body's normal functioning, growth and development, but many women and children get too few from their diets.
What is this review about?
Micronutrient deficiencies, the lack of essential vitamins and minerals, are especially a concern during pregnancy, when energy and nutrient demands are greater for both mother and foetus, and can lead to adverse health and development outcomes for the mother and child, such as being born too soon or too small.
A cost-effective strategy that has been implemented worldwide is to provide micronutrient and vitamin supplementation during pregnancy to achieve better health outcomes in the mother and child. There are different types of supplementation, including provision of a single micronutrient/vitamin (e.g. vitamin D), two micronutrients/vitamins (e.g. iron-folic acid supplementation), or several micronutrients/vitamins, which can be in the form of tablets, powders, or fat-based products.
Multiple micronutrient supplementation will help women and children who have more than one type of deficiency. However, it is understood that some micronutrients and vitamins can compete for absorption in the body and, as such, intake of several micronutrients at the same time may not be as effective as one would hope.
It is important to evaluate the various types of supplementation in pregnancy and their effects on maternal and child health outcomes to determine the best strategy for reducing poor outcomes.
What is the aim of this review?
This Campbell systematic review evaluates the various types of supplementation in pregnancy and their effects on maternal and child health outcomes to determine the best strategy for reducing poor outcomes.
What studies are included?
We searched for papers published between 1995 and 31 October 2019 in a variety of relevant databases and within grey literature. This systematic review included 314 papers across 72 studies (involving 451,723 women), of which 64 studies (involving 439,649 women) contributed to meta-analysis.
The included studies used the following comparisons: iron-folic acid supplementation versus folic-acid only; multiple-micronutrient supplementation versus iron-folic acid or iron alone; lipid nutrient-based supplementation versus multiple micronutrients; and iron, zinc, vitamin A, vitamin D or calcium supplementations, each compared to placebo.
What are the main findings of the review?
Across all comparisons, micronutrient and vitamin supplementation had little to no effect on the number of deaths among mothers and infants. Overall, women who received multiple micronutrient supplementation had fewer babies that were born early (<37 weeks of gestation), fewer babies born too small (<2500 g) and fewer babies who were smaller in size than normal for their gestational age, compared to women who received iron-folic acid supplementation. Iron or iron-folic acid supplementation was very good at improving maternal anaemia.
Mothers who received calcium supplementation may have had a decreased risk of pre-eclampsia and eclampsia during pregnancy, and mothers who received vitamin D compared to mothers who received placebo may have had fewer babies that were born early (<37 weeks of gestation).
Women supplemented with vitamin A compared to mothers given placebo had higher amounts of serum/plasma retinol, while zinc supplementation had no effect on all maternal and child outcomes reported.
Lipid nutrient-based supplementation showed little to no effect compared to multiple micronutrients; however, there were very few studies included and further research should be conducted.
What do the findings of this review mean?
The findings of this review support the use of micronutrient and vitamin supplementation during pregnancy to improve certain maternal and child health outcomes, which is especially important for populations living in low- and middle-income settings. Supplementation with multiple micronutrients was particularly good at improving several outcomes.
Further research should be done to establish the effects of supplementation on pregnant adolescents, who may have specific needs. Also, more data is needed to understand supplementation effects on long-term health and development outcomes for mother and child.
How up-to-date is this review?
The review authors searched for studies published up to October 2019.
BACKGROUND
Description of the condition
Close to two billion people today are deficient in key vitamins and minerals; of these individuals, the vast majority are women and children residing in low- and middle-income countries (LMIC) (Black et al., 2013; Development Initiatives, 2018). Among women of reproductive age (WRA) in LMIC, micronutrient deficiencies result from diets that chronically lack diversity and thus do not provide sufficient amounts of essential vitamins and minerals to meet recommended daily allowances (FAO and WHO, 2004). In some cases, infections and/or chronic disease may contribute to micronutrient deficiencies by directly inhibiting nutrient absorption (Bailey et al., 2015).
Because of increased nutritional requirements throughout pregnancy, micronutrient deficiencies are often exacerbated during this time. Additionally, repeated pregnancies and short inter-pregnancy intervals have been shown to contribute to poor maternal micronutrient status (Darnton-Hill, & Mkparu, 2015). As such, multiple concurrent deficiencies (in two or more micronutrients) are common among pregnant women, especially in LMIC (Allen & Peerson, 2009; Black, 2003). Though population-level estimates are mostly lacking, the global prevalence of prenatal iron deficiency anaemia is estimated to be 19.2% (95% confidence interval (CI) 17.1%-21.5%), while vitamin A deficiency affects 15.3% (95% CI 6.0%-24.6%) of pregnant women (Black et al., 2013). Restricting to LMIC could produce slightly larger prevalence estimates.
Micronutrient deficiencies are associated with a host of adverse outcomes for both the mother and the baby. Anemia in pregnancy, typically caused by iron deficiency, increases the risk of maternal mortality, perinatal mortality, and low birthweight (Allen 2001; Christian, 2010; Haider et al., 2013). Low folate levels are unequivocally associated with neural tube defects (NTD) (De-Regil et al., 2015], and severe iodine deficiency affects fetal development, including increasing the risk of mental retardation and cretinism (Dunn, 1993). Low calcium intake during pregnancy is associated with the development of hypertension, and hypertension is one of the leading causes of maternal morbidity, mortality, fetal growth restriction and preterm birth (Bucher et al., 1996; Ortega et al., 1999; Hofmeyr, 2018). Similarly, low vitamin D levels throughout gestation can lead to pre-eclampsia and, subsequently, increase the risk of preterm birth, small-for-gestational age (SGA), and perinatal mortality (De-Regil et al., 2016; Dror, 2011; MacKay et al., 2001). The effects of maternal zinc deficiency are not well understood, but it has been suggested that zinc supplementation during pregnancy can result in the reduction of preterm birth (Ota et al., 2015). Maternal malnutrition has also been shown to manifest through intergenerational effects, impacting the short-term and long-term outcomes of offspring, including growth, neurodevelopment and cognition, and cardiometabolic, pulmonary, and immune function (Gernand et al., 2016). Poor maternal nutrition reduces a newborn's chance to achieve proper growth and development in the short-term and, together, these early life inputs can establish the trajectory for chronic and other diseases later in life. Evidence has indicated that poor fetal and infant growth can lead to stunting in adulthood, chronic diseases relating to nutrition, lower educational attainment, reduced income, and even decreased birthweight in the next generation (Victora et al., 2008), highlighting the immense health and social consequences of maternal malnutrition.
Description of the intervention
Several strategies exist for reducing micronutrient malnutrition among women. These include diet diversification, large-scale and targeted fortification, bio-fortification of staple crops, and micronutrient supplementation with tablets or powders (Bhutta et al., 2008). This review will encompass micronutrient supplementation interventions during pregnancy.
Generally, micronutrient supplementation is used as a short term, preventive strategy that is targeted towards specific at-risk population groups (Bailey et al., 2015). As such, supplementation has been recommended as part of routine antenatal care to overcome the complications associated with micronutrient deficiencies during pregnancy.
Within the context of routine antenatal care for pregnant women, the World Health Organization (WHO) currently recomends daily iron-folic acid (IFA) supplementation with 30-60 mg of elemental iron and 400 ug of folic acid (WHO, 2016). In populations where anaemia prevalence is less than 20% or where side effects from daily supplementation are severe, weekly IFA supplementation with 120 mg of elemental iron and 2800 ug folic acid is recommended instead (WHO, 2016). The WHO has issued several context-specific recommendations as well: i) daily calcium supplementation (1.5-2.9 grams oral elemental calcium) in populations with low dietary intake of calcium; ii) daily (up to 10,000 IU) or weekly (up to 25,000 IU) vitamin A supplementation where vitamin A deficiency is a severe public health problem (WHO, 2016). Currently, zinc supplementation is recommended only where there is rigorous research to support its provision, and vitamin D supplementation is not recommended for pregnant women to improve maternal and perinatal outcomes (WHO, 2016).
To address the issue of multiple deficiencies, the United Nations Children's Fund (UNICEF), United Nations University (UNU), and the WHO developed a multiple micronutrient (MMN) tablet that provides the daily recommended intake of vitamin A, vitamin B1, vitamin B2, niacin, vitamin B6, vitamin B12, folic acid, vitamin C, vitamin D, vitamin E, copper, selenium, and iodine with 30 mg iron and 15 mg of zinc for pregnant women (UNICEF, WHO, and UNU, 1999). Other such tablets have been developed for supplementation studies on a case-by-case basis, typically providing at least three essential micronutrients.
More recently, the use of lipid-nutrient supplements (LNS) has been proposed to combat the adverse effects of maternal micronutrient deficiencies. Similar to MMN supplements, LNS contain a range of vitamins and minerals, but also provide energy, protein, and essential fatty acids. They are considered lipid-based because energy from LNS comes in the form of fats, such as vegetable fat, peanut/groundnut paste, milk powder and sugar (Arimond et al., 2015). Lipid-based products like Plumpy'nut were traditionally used for the treatment of severe acute malnutrition, but have since been adapted to contain a lower dose of energy such that daily supplementation with LNS products could be used as a preventive therapy for undernutrition (Arimond et al., 2015).
Supplementation with MMN is not recommended for pregnant women to improve maternal and perinatal outcomes, as more research is needed (WHO, 2016). The WHO has not yet issued any guidance for LNS (WHO, 2016).
How the intervention might work
Micronutrients, essential vitamins and minerals that are obtained from the diet, are critical for a host of metabolic activities that support tissue growth and functioning. As such, they are fundamental in enabling the healthy development of the fetus and promoting optimal pregnancy outcomes. Antenatal micronutrient supplementation interventions aim to increase circulating levels of vitamins and minerals in pregnant women in order to meet the recommended daily intakes, which are higher than normal due to increased physiological demands during pregnancy. Through tablets or other vehicles (e.g. syrup, drops, powder, or food matrices), the micronutrients are ingested and bioconverted to their active form in order to support maternal health and fetal development throughout gestation.
Through primary studies and meta-analysis of randomised controlled studies (RCTs), some antenatal micronutrient supplementation interventions have proven to be efficacious in improving congenital/birth outcomes, including lowering the risk of NTD, cretinism, premature rupture of membranes (PROM), low birthweight, and preterm birth (Bougma et al., 2013; De-Regil et al., 2015; De-Regil et al., 2016; Haider et al., 2013; Lassi et al., 2013; Ota et al., 2015; Rumbold et al., 2015; Zhou et al., 2013). The duration of exposure needed to produce clinically meaningful results may vary depending on the supplement. For example, it is recommended that folic acid supplementation begin as early as possible, and ideally prior to conception (WHO, 2016), while daily iron supplementation that begins mid-gestation has been effective at improving some outcomes (Peña-Rosas et al., 2015).
Why it is important to do this review
There are several existing systematic reviews that examine the impact of single and multiple micronutrient supplementation interventions in pregnancy (Appendix 1), many of which incorporate data from studies conducted in low- and middle-income settings. However, significant heterogeneity in results has been reported (e.g., for antenatal iron supplementation); this has not yet been explained by subgroup analysis. In addition, inconclusive results for several micronutrient supplementation interventions (e.g., folic acid supplementation for maternal health and pregnancy outcomes, calcium supplementation (other than for preventing or treating hypertensive disorders) for pregnancy and infant outcomes, and zinc supplementation for improving pregnancy and birth outcomes) were found, warranting further investigation. Many of the systematic reviews listed (Appendix 1) are several years old, underscoring the need to update the evidence in order to capture newly completed study data. There is the hope that with more power to detect differences, some unanswered questions will be resolved. For example, previous evidence suggests that male infants are at a greater risk for morbidity and mortality relative to their female counterparts, especially in the perinatal, neonatal and early infancy stages (Stevenson et al., 2000; Waldron, 1998; Zhao et al., 2017). As well, sex-specific differences in infant mortality following MMN supplementation were noted in a study by Smith and colleagues (Smith et al., 2017). Thus, additional exploration is required to confirm the sex-specific differences in morbidity and mortality amongst infants. Additionally, concerns have been raised regarding the safety of iron supplementation in women with high haemoglobin concentrations, and the potentially negative long-term consequences that unabsorbed iron may have on child morbidity (Mwangi et al., 2017; Paganini et al., 2016).
In addition to the limitations of existing systematic reviews of RCTs, the effectiveness of antenatal micronutrient supplementation interventions in a real world setting has not been well established. We aim to understand which antenatal supplementation interventions are effective to improve key maternal and child health, nutrition, and mortality outcomes in LMIC. We will include data from large programme evaluations as well as smaller studies. Additionally, we will include adolescent women as a pre-specified subgroup, which will help to elucidate strategies that can mitigate the risks associated with adolescent pregnancy in LMIC (Bhutta et al., 2017). Lastly, we hope to answer some of the remaining questions outlined above, including potential infant sex-specific differences and safety concerns following supplementation in pregnancy. Taken together, these results will inform the evidence on which to base policy and programming relating to micronutrient supplementation in pregnancy for women in LMIC. In addition, this review will point to any gaps in the existing evidence.
OBJECTIVES
This review will summarize the available evidence on antenatal micronutrient supplementation interventions in LMIC. For each intervention, results will be summarized separately.
Specific objectives: What is the impact of single micronutrient supplementation (calcium, vitamin A, vitamin D, iodine, zinc, vitamin B12) during pregnancy on maternal, birth, child health and development outcomes at longest follow-up? What is the impact of iron folic acid supplementation during pregnancy on maternal, birth, child health and development outcomes? What is the impact of multiple micronutrient supplementation during pregnancy on maternal, birth, child health and development outcomes? What is the impact of lipid-based nutrient supplementation during pregnancy on maternal, birth, child health and development outcomes?
METHODS
Criteria for considering studies for this review
Types of studies
We included the following study designs: Randomized controlled studies (RCTs), where participants were randomly assigned, individually or in clusters, to intervention and comparison groups. Cross-over designs were eligible for inclusion. Quasi-experimental designs, which include: Natural experiments: studies where non-random assignment is determined by factors that are out of the control of the investigator. One common type includes allocation based on exogenous geographical variation. Controlled before-after studies (CBA), in which measures were taken of an experimental group and a comparable control group both before and after the intervention. We also required that appropriate methods were used to control for confounding, such as statistical matching (e.g., propensity score matching, or covariate matching) or regression adjustment (e.g., difference-in-differences, instrumental variables). Regression discontinuity designs; here, allocation to intervention/control is based upon a cut-off score. Interrupted time series (ITS) studies, in which outcomes were measured in the intervention group at least three time points before the intervention and after the intervention.
Reviews were excluded.
Types of participants
Participants were healthy (i.e. non-diseased) pregnant women of any age and parity living in LMIC. LMIC will be defined by the World Bank Group at the time of the search for this review. Though our aim was to include healthy pregnant women, the prevalence of micronutrient deficiencies is high in these settings, indicating that women are likely to have one or more micronutrient deficiencies at baseline; women were not excluded on this basis. Studies that include only a subset of eligible participants were retained as eligible, but were only included in analysis where data had been disaggregated appropriately for use.
Types of interventions
The following interventions targeting pregnant women were included, and were analysed separately: Single micronutrient supplementation (calcium, vitamin D, iodine, folic acid, iron, vitamin A, zinc, vitamin B12) compared to placebo (Supplementation may take the form of tablets, drops, syrup or powder) Iron folic acid supplementation compared to folic acid alone or placebo Vitamin D and calcium supplementation compared to placebo MMN compared to iron folic acid supplementation or placebo: For MMN, studies that use fewer than 3 micronutrients in its composition were excluded (Haider & Bhutta, 2017; Kawai et al., 2011) LNS compared to MMN or placebo
For logistical reasons, we did not include every vitamin and mineral. Interventions were chosen based on relevance (i.e., most prevalent nutritional deficiencies) and data availability when considering the LMIC context.
There were no restrictions regarding: i) the duration of exposure to the intervention, ii) the provider of the intervention, iii) the frequency of the intervention (e.g. daily or intermittent supplementation), or iv) the food vehicle utilized for LNS interventions. We included studies where co-interventions (e.g. education) were provided for both the intervention and the comparison groups.
Types of outcome measures
To be included within this review, studies measured at least one of the following primary and/or secondary outcomes. We looked at maternal, fetal, neonatal and child health and nutrition outcomes that will help to inform related policy and practice. For simplifying, we grouped all secondary outcomes of interest by these domains. Unless otherwise specified, all outcomes listed were dichotomized (yes/no). We used mean and standard deviation (SD) to report all continuous outcomes (maternal biochemical status, newborn anthropometry, newborn/child biochemical status). Outcome definitions can be found in brackets below. International Units (IU) were used for all maternal outcomes whereas z-scores were used for child outcomes, because z-scores are adjusted for age.
Primary outcomes
Maternal Mortality (death while pregnant or within 42 days of pregnancy termination) Anemia/iron deficiency anaemia in third trimester of pregnancy [WHO, 2011] Non-anemic: > or equal to 110 g/L Anemic: <110 g/L low birthweight (<2500 g) perinatal mortality (stillbirths and deaths <or equal to 7 days)
Secondary outcomes
Maternal Outcomes
Morbidity from study enrolment up to 3 months post-partum: Pre-eclampsia/eclampsia Gestational hypertension Antepartum haemorrhage Postpartum haemorrhage Premature rupture of membranes Placental abruption Infections during pregnancy Bone mineral density Night blindness Need for blood transfusion
Biochemical status at endline: Micronutrient deficiencies Vitamin A (serum/plasma retinol) (continuous) Iron (serum/plasma ferritin, plasma TfR, TIBC) (continuous) Serum/plasma/red blood cell folate (continuous) Serum/plasma zinc (continuous) Serum/plasma alkaline phosphatase (continuous) Serum/plasma copper (continuous) Serum/plasma vitamin D (25-hydroxyvitamin D) (continuous) Thyroglobulin concentration (continuous)
Fetal Outcomes
Mortality: Miscarriage (loss of pregnancy before 28 weeks gestation) Stillbirth (death at or beyond 28 weeks of gestation)
Morbidity: Congenital anomalies
Newborn Outcomes
Mortality: Neonatal mortality (deaths between 0 and 28 days)
Morbidity: Preterm birth (<37 weeks gestation) Small-for-gestational age (defined by study authors) Macrosomia (birthweight >4000 g)
Anthropometry measured from birth up to 14 days: Birth weight (z-scores) (continuous) Birth length (z-scores) (continuous) Head circumference (z-scores) (continuous)
Child Outcomes
Mortality: Infant mortality (deaths between 0 and 12 months) Under-five mortality (deaths between 0 and 59 months)
Morbidity: Stunting (-2 z-score or lower) at longest follow up Wasting (-2 z-score or lower) at longest follow up Underweight (-2 z-score or lower) at longest follow up Bone mineral density (continuous) Development outcomes (as defined by study authors) Infection
Biochemical status at endline: Micronutrient deficiencies Vitamin A (serum/plasma retinol) (continuous) Iron (serum/plasma ferritin, plasma TfR) (continuous) Serum/plasma/red blood cell folate (continuous) Serum/plasma zinc (continuous) Serum/plasma vitamin D (25-hydroxyvitamin D) (continuous) Anaemia Hemoglobin concentration (continuous) Iron deficiency anaemia
Other Outcomes
Relevant long-term outcomes during adolescence or adulthood, as specified by study authors. For example: Anthropometrics (stunting, wasting, underweight) in children >59 months Cognitive and motor development as assessed by study investigators at longest follow up (e.g. Bayley Mental Development Index, Bayley Psychomotor Development Index, Stanford-Binet test) Educational attainment (completion of primary or secondary school) Mode of delivery (vaginal, instrumental vaginal, caesarean)
Adverse outcomes: any reported throughout intervention period (e.g. urinary tract infections, kidney stones, hyperthyroidism, allergic reactions, etc.), including short-term adverse outcomes (e.g. vomiting, abdominal pain, constipation, diarrhoea, unpleasant tastes).
Duration of follow-up
There was no minimum duration of follow up.
Types of settings
Other than the LMIC inclusion criteria, there were no restrictions regarding study setting.
Any post hoc changes to eligibility criteria or outcomes studied were aligned with the review objectives and were clearly stated with reasons justified.
Search methods for identification of studies
The search strategy was guided by our PICO model (Table 1), but was restricted by outcome in order to retain a broader search. The search was conducted using indexing terms, including medical subject headings (MeSH), keywords, and free text words. Details of the search strategy can be found in Appendix 2. To capture the most relevant evidence, we included articles published from 1995 to the end of June 2018 (related programmes and good quality studies before 1995 were very limited). There were no language or publication restrictions. Manual searches were conducted within reference lists of review articles and included studies, and experts were contacted to obtain any additional relevant maternal that may have been missed. The search process, including month/year of search, was documented to ensure that replication is possible.
PICO table used for formulating our search strategy
Electronic searches
The search was run in the following databases, selected based on their applicability to the subject material: CAB Abstracts CINAHL Cochrane Central Register of Controlled Trials (CENTRAL) Embase International Initiative for Impact Evaluations (3ie) LILACS (Latin American and Caribbean health sciences literature) Medline POPLINE Web of Science WHOLIS (WHO library database)
Searching other resources
Unpublished Studies
ProQuest Dissertations & Theses Global R4D (Research for Development) material from UK government's Department for International Development WHO International Clinical Trials Registry Platform (ICTRP)
Grey Literature
Non-indexed, grey literature searches was conducted to locate relevant programme evaluations and any additional studies. We searched Google, Google Scholar, and web pages of key international nutrition agencies (listed below) using key words based on PICO methodology. We used advanced search options, where possible. Google results were screened online until no relevant result appeared in 3 consecutive pages. Canadian Agency for Drugs and Technologies in Health (CADTH) tool for searching health-related grey literature (http://www.cadth.ca/resources/finding-evidence/grey-matters) Centers for Disease Control and Prevention (CDC) Emergency Nutrition Network (ENN Global Alliance for Improved Nutrition (GAIN) Hellen Keller International International Food Policy and Research Institute (IFPRI) IZiNCG Nutrition International (NI) Sight and Life Foundation UNICEF World Food Programme (WFP)
Data collection and analysis
Description of methods used in primary research
The vast majority of included studies were randomised or cluster-randomised controlled studies that followed our inclusion/exclusion criteria, as listed above. For example, in a study published by Christian and colleagues (Christian et al., 2003), pregnant Nepalese women were cluster-randomised to 1 of 5 groups: i) daily supplements of vitamin A (control), ii) daily supplements of vitamin A + folic acid, iii) daily supplements of vitamin A + folic acid + iron, iv) daily supplements of vitamin A + folic acid + iron + zinc, or v) daily multiple micronutrient supplements (including vitamin A) from early pregnancy to 72 hours postpartum. Outcomes assessed included infant anthropometrics (birth weight, length, and head circumference), and low birthweight (<2500 grams).
Criteria for determination of independent findings
In order to take into account potential sources of dependency, we grouped studies in terms of their location, population, the programme that is being evaluated (if applicable), and intervention type to ensure that there is no double counting of evidence when synthesizing results across studies. Where there were multiple papers that described the same study, these papers were combined and coded as a single study.
For studies that include multiple intervention arms, we selected one pair (intervention and control) that satisfied the inclusion criteria of the review and excluded the rest. If >2 intervention groups met the eligibility criteria, then these groups were combined into a single pair-wise comparison group and data was disaggregated into corresponding subgroups, or these arms were separated into different forest plots to ensure that there was no double counting of participants. Where multiple effect sizes from the same study and intervention-control comparison were eligible, we chose to include the estimate with the larger sample size, though this occurred rarely.
Selection of studies
Two independent reviewers performed title and abstract screening using specified inclusion/exclusion criteria. Where not enough information could be gleaned from the title alone, then abstracts were screened in order to determine eligibility for full text screening. All full texts were then screened in duplicate, with application of the same inclusion/exclusion criteria. A third reviewer resolved any disagreements. Both title/abstract and full text screening were done using Covidence, a web-based software platform for systematic reviews. We assessed inter-reviewer reliability/agreement by checking the number of conflicts in the Resolve Conflicts page following each stage of screening.
Examples of included studies
Mridha MK, Matias SL, Chaparro CM, et al. (2016) Lipid-based nutrient supplements for pregnant women reduce newborn stunting in a cluster-randomised controlled effectiveness study in Bangladesh. Am J Clin Nutr; 103(1):236-49. Roberfroid D, Huybregts L, Lamou H et al. (2008). Effects of maternal multiple micronutrient supplementation on fetal growth: a double-blind, randomised controlled study in rural Burkina Faso. Am J Clin Nutr; 88:1330-40.
Examples of excluded studies
Harvey LJ, Dainty JR, Hollands WJ, et al. (2007) Effect of high-dose iron supplements on fractional zinc absorption and status in pregnant women. Am J of Clin Nutr; 85:131-6. Ineligible population (high-income setting) Boran P, Tokuc G, Vagas E, et al. (2006) Impact of zinc supplementation in children with acute diarrhoea in Turkey. Arch Dis Child; 91(4):296-99. Ineligible population (children 6 months to 5 years of age)
Data extraction and management
For all included studies, we extracted data into a standardized data abstraction form that was comprised of a general study information sheet and a quantitative outcomes sheet. The data abstraction form was piloted before it was finalized. While all arms of a study were described in the tables of included studies, data was extracted and reported on only for those arms that met review criteria. All data abstraction was performed in duplicate. Coders were trained in systematic review methods, and data abstraction was cross-checked with primary study data for accuracy by the team lead.
Each general study information sheet contained the following: General study information: authors, publication year, language of study, study design Study setting: World Bank region, country, World Bank income level, city/town, urban/urban slum/rural/mixed setting, duration of data collection, date of data collection Study population: sample size recruited, sample size analysed, male/female/mixed (%), age range of participants, mean/median age of participants, description of participants (i.e. inclusion/exclusion criteria applied to recruitment) Intervention characteristics: type of intervention, food vehicle utilized (where applicable), duration of intervention, level of delivery, unit of randomisation (where applicable), dose of micronutrient(s) provided, frequency of provision (i.e. daily, weekly, etc.), duration of follow up, attrition rate Programmatic indicators (based on the WHO/CDC logic model (De-Regil et al., 2014)): policies, production, delivery strategies, quality control, behaviour change communication strategies, access and coverage, knowledge and appropriate use Funding source of programme (where applicable) Quality assessment (see section below: critical appraisal of studies
Each quantitative outcome sheet contained the following: Subgroup (if applicable) Subgroup sample size Outcome type (based on outcomes listed above) Outcome units Outcomes: Outcome measure treatment group Outcome measure comparison group Standard deviation Effect size: Effect measure (specify type); unadjusted and adjusted 95% confidence interval (CI) P-value of effect measure Standard error (SE) or standard deviation (SD) or t-statistic
Assessment of risk of bias in included studies
We critically appraised individual studies using the Cochrane Effective Practice and Organisation of Care (EPOC) guidelines for randomised studies, non-randomised studies, controlled before-after studies, and interrupted time series (ITS) studies. EPOC guidelines include the following standardized criteria for assessing bias of randomised, non-randomised, and controlled before-after studies [Cochrane Effective Practice and Organisation of Care (EPOC), 2017]: Random sequence generation Allocation concealment Baseline outcome measurements similar Baseline characteristics similar Incomplete outcome data Knowledge of the allocated interventions adequately prevented during study Protection against contamination Selective outcome reporting Other risks of bias (e.g. bias in measurement: validity and reliability of the measures used)
For ITS studies, the following criteria was considered [Cochrane Effective Practice and Organisation of Care (EPOC), 2017]: Intervention independent of other changes Shape of intervention effect pre-specified Intervention unlikely to affect data collection Knowledge of the allocated interventions adequately prevented during study Incomplete outcome data Selective outcome reporting Other risks of bias (e.g. bias in measurement: validity and reliability of the measures used)
For EPOC rating schemes for randomised studies, non-randomised studies, and controlled before-after studies please see Table 2 and for interrupted time series studies, see Table 3.
EPOC criteria for assessing risk of bias in randomised trials, non-randomised trials, and controlled before-after studies
EPOC criteria for assessing risk of bias in interrupted time series studies
In addition, the Cochrane risk of bias (ROB) tool (Higgins & Green, 2011) was used for randomised studies, including cluster-randomised studies and step-wedge designs. The ROB tool used the following criteria for assessment of bias. Of note, we assessed performance and detection bias separately. Selection bias: random sequence generation and allocation concealment Performance bias: blinding of participants and personnel Detection bias: blinding of outcome assessment Attrition bias: incomplete outcome data Reporting bias: selective reporting Other sources of bias
All risk of bias assessments were performed in duplicate and supportive evidence for all ROB judgements was documented. A third reviewer resolved any disagreements. An overall score was not provided.
Measures of treatment effect
We converted data for each outcome into the same format (e.g. means and standard deviations for continuous data), including appropriate conversion of scales such that an increase/decrease always indicated improvement or deterioration of an indicator. In the case that included studies had data that were reported in a not 'usable' way (i.e., data cannot be pooled with other data), we retained the study as eligible but restricted it from further analysis.
We analyzed dichotomous and continuous outcomes separately. For dichotomous outcomes, results were presented as summary risk ratios (RRs) with 95% CIs, whenever possible, in order to compare risk of the outcome between intervention and control groups. When including incidence data, we combined risk ratios (events per child) and rate ratios (events per child year) because of their similar interpretation and scale. We presented continuous outcome data as either a mean difference (MD), if outcomes were measured on the same scale, or a standardized mean difference (SMD), if outcomes were measured on different scales, with 95% CIs. Both change from baseline scores and final measurements (for RCTs only) were eligible, and were pooled where there is meta-analysis with MD (i.e., scales are the same and measurements are in the same unit) Higgins & Green, 2011. We carefully considered reporting of the appropriate means and standard deviations (either of final measurements or of changes from baseline) if both change and final values were used in one meta-analysis. We did not combine final values and change scores as SMDs because the standard deviation in this case reflected differences in measurement reliability. Where it was necessary to combine measures of treatment effects with SMDs (for example, in the case of child development outcomes), we used change scores as opposed to endline values, but only where authors had appropriately reported the SD of the change score.
Unit of analysis issues
All interventions and, within those interventions, outcomes were meta-analysed separately. We also meta-analysed RCTs and quasi-experimental studies separately.
Special attention was given to cluster-randomised studies; this was to ensure that clustering was appropriately accounted for within the analysis of the primary study, such that study precision was not over or under-estimated within our analysis. If necessary, we adjusted effect estimates of cluster-randomised studies using the mean cluster size (M) and the intra-cluster correlation coefficient (ICC), which quantified the extent to which data from the same cluster were correlated [design effect = 1 + (M-1) ICC]. The design effect was then used to adjust the study data such that a study was reduced to its effective sample size. We did not make any adjustments if authors appropriately adjusted for cluster design already.
Randomized and non-randomised studies with contemporaneous comparison groups were analysed separately, but were pooled if differences in findings were not statistically significant. We analyzed and reported findings from controlled before-after and ITS study designs separately.
Dealing with missing data
Where data was incomplete or in a form that could not be converted with the information available, we contacted the corresponding author for clarification or to obtain missing data. If authors have accounted for missing data (i.e. multiple imputations), we used the adjusted data within our analysis.
Assessment of heterogeneity
Statistical heterogeneity was assessed using Tau2, I2 and significance of the Chi-square test; we also assessed heterogeneity visually using forest plots. Based on prior theory and clinical knowledge, we expected clinical and methodological heterogeneity in effect sizes in this literature. Therefore, we attempted to explain any observed statistical heterogeneity using subgroup analysis (see below).
Assessment of reporting biases
If the number of studies was sufficient (>10), funnel plots were used to visually assess publication bias. This kind of bias is unlikely if data forms a symmetric inverted funnel shape around the mean effect estimate. In addition, we performed Egger's test to determine funnel plot asymmetry.
Data synthesis
Statistical analysis was carried out using Review Manager 5.3 and Stata. We followed intention to treat (ITT) analysis for RCTs. We reconstructed the data to create an ITT analysis where authors reported a per protocol analysis.
Random effects meta-analysis was used to account for any expected heterogeneity in interventions, comparisons, outcomes, or settings within the studies included in a given synthesis. Where meta-analysis was deemed inappropriate due to substantial methodological or statistical heterogeneity between studies, we summarized the findings of the included studies in narrative or table form.
The generic inverse-variance approach was used for both dichotomous and continuous outcomes, such that the study weights were adjusted according to the variance of the effect estimate (i.e. the larger studies with smaller standard error were given more weight than smaller studies with larger standard error). For random effects analyses, the DerSimonian and Laird method was applied to incorporate a measure of variation (Tau2) among intervention effects from different studies.
We used raw summary estimates to construct meta-analyses from RCTs and adjusted estimates to construct meta-analyses from observational studies. We interpreted overall effect estimates that had an associated p-value <0.05 as statistically significant, but also commented on those effects where the upper or lower confidence interval has just crossed the line of no effect. In the case of the latter, where the confidence intervals fell between the line of no effect and 0.06, the effect estimates were interpreted with caution as possibly significant (i.e. may have or may have not had an effect). Where confidence intervals were >0.06, effect estimates were interpreted as not significant.
We also reported non-significant findings. Where possible, interaction tests were used to determine if there was a relevant difference in effect across sub-groups. We based the conclusion that an intervention was effective in one subgroup but not another on a direct test of the mean difference between two groups (i.e., with meta-regression).
We used the GRADE tool to assess the body of evidence for selected outcomes for which a meta-analysis was conducted. We chose the following outcomes: maternal mortality, maternal anaemia, low birthweight, and perinatal mortality.We summarized this assessment in a 'Summary of Findings' table, created by the GRADEpro software. We rated the quality of the body of evidence for each selected outcome as high, moderate or low, or very low. Randomized studies were initially rated as high quality evidence but they were downgraded according to the five criteria listed below. Quasi-experimental studies initially were rated as low quality evidence, but they could be upgraded if they did not have any serious methodological limitations. They could also be downgraded further.
There were five criteria that downgraded evidence (Atkins & GRADE, 2004): Risk of bias in individual studies Indirectness of evidence Unexplained heterogeneity or inconsistency of results Imprecision of results High probably of publication bias
There were three criteria that upgraded the evidence for quasi-experimental studies with no serious methodological limitations. (Atkins & GRADE, 2004): Large magnitude of effect Presence of a dose response relationships Effect of plausible residual confounding
Quality ratings, as determined by GRADE, are found in Table 4.
Quality of evidence, as determined by GRADE criteria
Subgroup analysis and investigation of heterogeneity
Heterogeneity was assessed based on clinical knowledge and theory and investigation of statistical criteria such as Tau2, I2 and significance of the Chi-sqaure test.
Depending on data availability (> or equal to three studies per subgroup of interest), we conducted sub-group analyses on the primary outcomes for the following variables: Age (10-14 years, 15-19 years, 20-29 years, 30-39 years, 40+) Geographical region (based on WHO regions) Sex of infant Baseline nutritional status Anemic versus non-anemic Undernutrition versus normal nutrition, based on body mass index (BMI; BMI <18.5) Low stature versus normal stature Duration of intervention Women recruited prior to conception versus first trimester versus second trimester versus third trimester of pregnancy Frequency of intervention Daily versus intermittent IFA supplementation Dose of intervention 30 mg versus 60 mg elemental iron for IFA, MMN, or LNS supplementation UNIMMAP versus adapted UNIMMAP versus non-UNIMMAP formulations for MMN supplementation (UNICEF, WHO, and UNU, 1999) MMN supplements that contained a similar number and type of vitamins and minerals as the UNIMMAP formulation were categorized as 'adapted UNIMMAP' (+/−2 micronutrients, when compared to the standard UNIMMAP formulation) Supplements with the same composition as UNIMMAP but different doses of vitamins and minerals were categorized as 'adapted UNIMMAP'
Variables were selected a priori, based on evidence to support their potential to impact the intervention effect. We carefully interpreted results from subgroup analyses. We also used meta-regression techniques to assess how characteristics of studies (explanatory variables) may influence the size of the effect estimate (outcome variable). Potential variables may include the setting, dosing frequency, dosing form, compound, duration, route, sex of infant, SES status, or nutritional status.
Any subgroup analysis that was conducted post hoc was exploratory in nature and was stated as such.
Sensitivity analysis
Sensitivity analyses were conducted to determine whether the removal of studies with high risk of bias or the removal of non-randomised studies significantly impacted findings. We defined studies as having a high risk of bias if one or more domains have been judged as 'high risk' or two or more domains have been judged as 'unclear risk'.
Treatment of qualitative research
We did not include qualitative research.
RESULTS
Description of studies
Results of the search
We identified of 27,987 records from our database search and 670 records through hand-searching and searching grey literature (Figure 3). Following title and abstract screening, full text screening was completed for 1,678 papers (1,246 from the database search and 432 from the grey literature and hand-search combined). Of these, a total of 72 studies, with 314 associated papers, were identified for inclusion based on our pre-defined inclusion and exclusion criteria. Eight studies were included in the review but did not contribute data to the meta-analyses for various reasons: data was in a form that could not be pooled with other studies, no reported outcomes of interest, or insufficient number of studies to pool for meta-analysis; at minimum, 3 studies were required to conduct a meta-analysis for a given outcome (Diogenes et al., 2013; Duggan et al., 2014; Gowachirapant et al., 2017; Hambidge et al., 2019; Jarjou et al., 2006; Korkmaz et al., 2014; Prawirohartono et al., 2011; Taherian et al., 2002).
Included studies
We identified a total of 72 studies (number of included papers = 314), involving 451,723 women as eligible for inclusion in this review (Figure 3). Eight trials were included in the review, but did not contribute data to the meta-analyses (Diogenes et al., 2013; Duggan et al., 2014; Gowachirapant et al., 2017; Hambidge et al., 2019; Jarjou et al., 2006; Korkmaz et al., 2014; Prawirohartono et al., 2011; Taherian et al., 2002). Of these, Gowachirapant et al. (2017) was the only study that examined iodine supplementation versus placebo and Hambidge et al. (2019) was the only study that reported the effects of LNS versus placebo. Diogenes et al. (2013) and Taherian et al. (2002) were excluded from meta-analyses because they were the only two studies that fit our eligibility criteria and evaluated the impact of calcium plus vitamin D versus placebo supplementation. Jarjou et al. (2006) examined calcium supplementation versus placebo (for which we have conducted meta-analyses); however, this study reported outcomes that could not be pooled with other studies. Similarly, Korkmaz et al. (2014) was excluded from the iron versus placebo comparison and Prawirohartono et al. (2011) was excluded from the vitamin A versus placebo comparison and the zinc versus placebo comparison due to no common outcomes of interest. Duggan et al. (2014) was the only study that reported effects of vitamin B12 supplementation compared to placebo.
Twelve studies were conducted in the East Asia Pacific region (Dijkhuizen et al., 2001; Gowachirapant et al., 2017; Hanieh et al., 2013; Huy et al., 2009; Liu et al., 2013; Muslimatun et al., 2001; Prawirohartono et al., 2011; Supplementation with Multiple Micronutrients Intervention Trial (SUMMIT) Study Group, 2008; Sunawang et al., 2009; Tanumihardjo, 2002; Zeng et al., 2008; Zhao et al., 2015). Of these, 2 were excluded from analysis (Gowachirapant et al., 2017; Prawirohartono et al., 2011). Countries represented include: China (Liu et al., 2013; Zeng et al., 2008; Zhao et al., 2015), Indonesia (Dijkhuizen et al., 2001; Muslimatun et al., 2001; Prawirohartono et al., 2011; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tanumihardjo, 2002), Vietnam (Hanieh et al., 2013; Huy et al., 2009), and Thailand (Gowachirapant et al., 2017).
Only 1 study was conducted in Europe & Central Asia, in Turkey (Korkmaz et al., 2014).
Seven studies were conducted in Latin America & the Caribbean (Belizán et al., 1997; Castillo-Durán et al., 2001; Caulfield et al.,1999; Diogenes et al., 2013; López-Jaramillo et al., 1997; Merialdi et al., 2004; Ramakrishnan et al., 2003). Of these, 1 was excluded from analysis (Diogenes et al., 2013). Countries represented include: Argentina (Belizán et al., 1997), Chile (Castillo-Durán et al., 2001), Peru (Caulfield et al., 1999; Merialdi et al., 2004), Brazil (Diogenes et al., 2013), Ecuador (López-Jaramillo et al., 1997) and Mexico (Ramakrishnan et al., 2003).
Thirteen studies were conducted in the Middle-East and North Africa region (Aminisani et al., 2009; Asemi et al., 2013; Asemi et al., 2016; Falahi, 2010; Mohammad-Alizadeh-Charandabi et al., 2015; Naghshineh & Sheikhaliyan, 2016; Ouladsahebmadarek et al., 2011; Sabet et al., 2012; Sorouri et al., 2016; Taherian et al., 2002; Vaziri et al., 2016; Ziaei et al., 2007, 2008). Of these, 1 was excluded from analysis (Taherian et al., 2002). All 13 studies were conducted in Iran.
Nineteen studies were conducted in South Asia (Ahmad et al., 2016; Bhutta et al., 2009; Choudhury et al., 2012; Christian et al., 2003; Duggan et al., 2014; Hafeez et al., 2005a, b; Hossain et al., 2012; Khan et al., 2016; Kumar et al., 2009; Osendarp et al., 2000; Osrin et al., 2005; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Sablok et al., 2015; Sahu et al., 2009; Tofail et al., 2008; West et al., 1999; West et al., 2011; West et al., 2014). Approximately half of the studies (n=8) were conducted in Bangladesh (Ahmad et al., 2016; Choudhury et al., 2012; Osendarp et al., 2000; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Tofail et al., 2008; West et al., 2011; West et al., 2014). Four studies were conducted in India (Duggan et al., 2014; Kumar et al., 2009; Sablok et al., 2015; Sahu et al., 2009), 3 in Nepal (Christian et al., 2003; Osrin et al., 2005; West et al., 1999), and 4 in Pakistan (Bhutta et al., 2009; Hafeez et al.,2005a,b; Hossain et al., 2012; Khan et al., 2016).
Eighteen studies were conducted in Sub-Saharan Africa (Ashorn et al., 2015; Cox et al., 2005; Dewey, 2009; Darling et al., 2017; Etheredge et al., 2015; Fawzi et al., 2007; Friis et al., 2004; Huybregts et al., 2009; Jarjou et al., 2006; Kæstel et al., 2005; Kirkwood et al., 2010; Menendez et al., 1995; Moore et al., 2012; Preziosi et al., 1997; Roberfroid et al., 2008; Saaka et al., 2009; Semba et al., 2001; Zagré et al., 2007). Of these, Jarjou et al., 2006 was the only study excluded from analysis. Countries represented include Burkina Faso (Huybregts et al., 2009; Roberfroid et al., 2008), The Gambia (Jarjou et al., 2006; Menendez et al., 1995; Moore et al., 2012), Ghana (Cox et al., 2005; Dewey, 2009; Kirkwood et al., 2010; Saaka et al., 2009), Guinea-Bissau (Kæstel et al., 2005), Malawi (Ashorn et al., 2015; Semba et al., 2001), Niger (Preziosi et al., 1997; Zagré et al., 2007), Tanzania (Darling et al., 2017; Etheredge et al., 2015; Fawzi et al., 2007) and Zimbabwe (Friis et al., 2004).
Two studies, Villar et al. (2006) and Hambidge et al. (2019) were multi-country studies. Villar et al. (2006) was conducted in India, Peru, South Africa and Vietnam; Hambidge et al. (2019) was conducted in Democratic Republic of Congo, Guatemala, India and Pakistan.
A total of 439,649 women participated in the remaining 64 studies (Ahmad et al., 2016; Aminisani et al., 2009; Asemi et al., 2013; Asemi et al., 2016; Ashorn et al., 2015; Belizán et al., 1997; Bhutta et al., 2009; Castillo-Durán et al., 2001; Caulfield et al., 1999; Choudhury et al., 2012; Christian et al., 2003; Cox et al., 2005; Mohammad-Alizadeh-Charandabi et al., 2015; Dewey, 2009; Dijkhuizen et al., 2001; Etheredge et al., 2015; Falahi, 2010; Fawzi et al., 2007; Friis et al., 2004; Hafeez et al., 2005a, 2005b; Hanieh et al., 2013; Hossain et al., 2012; Huy et al., 2009; Huybregts et al., 2009; Kæstel et al., 2005; Khan et al., 2016; Kirkwood et al., 2010; Kumar et alk., 2009; Liu et al., 2013; López-Jaramillo et al., 1997; Menendez et al., 1995; Merialdi et al., 2004; Moore et al., 2012; Muslimatun et al., 2001; Naghshineh & Sheikhaliyan, 2016; Osendarp et al., 2000; Osrin et al., 2005; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Ramakrishnan et al., 2003; Roberfroid et al., 2008; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Semba et al., 2001; Sorouri et al., 2016; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tanumihardjo, 2002; Tofail et al., 2008; Vaziri et al., 2016; Villar et al., 2006; West et al., 1999; West et al., 2011; West et al., 2014; Zagré et al., 2007; Zeng et al., 2008; Zhao et al., 2015; Ziaei et al., 2007, 2008).
Most of the outcomes were defined in the same way across different studies. The exception to this was in Christian et al., (2003) and Liu et al., 2013, where perinatal mortality was defined as stillbirths (from 28 weeks of gestation to delivery) and early neonatal death from birth to 6 days after delivery; this is compared to all other studies that defined perinatal mortality as stillbirths plus early neonatal deaths from birth to 7 days after delivery. For iron deficiency (measured by serum ferritin levels), Zhao et al., 2015 defined iron deficiency as a serum ferritin of <15ug/L, while the remaining studies (Falahi, 2010; Liu et al., 2013; Preziosi et al., 1997) reported it as a serum ferritin of <12ug/L. Lastly, Villar 2006 combined pre-eclampsia and eclampsia cases; the other studies only considered pre-eclampsia cases.
All studies reported sources of funding except: Asemi et al., 2013; Caulfield et al.,1999; Dijkhuizen et al., 2001; Falahi, 2010; Huy et al., 2009; Huybregts et al., 2009; Jarjou et al., 2006; Korkmaz et al., 2014; López-Jaramillo et al., 1997; Menendez et al., 1995; Merialdi et al., 2004; Mohammad-Alizadeh-Charandabi et al., 2015; Muslimatun et al., 2001; Osendarp et al., 2000; Ouladsahebmadarek et al., 2011; Preziosi et al.,1997; Saaka et al., 2009; Sablok et al., 2015; Tanumihardjo, 2002; Villar et al., 2006; Ziaei et al., 2007, 2008.
Forty-two studies included a statement of disclosure regarding potential conflicts of interest related to the study (Ahmad et al., 2016; Asemi 2016; Belizán et al., 1997; Castillo-Durán et al., 2001; Christian et al., 2003; Dijkhuizen et al., 2001; Diogenes et al., 2013; Duggan et al., 2014; Etheredge et al., 2015; Fawzi et al., 2007; Friis et al., 2004; Gowachirapant et al., 2017; Hambidge et al., 2019; Hanieh et al., 2013; Hossain et al., 2012; Jarjou et al., 2006; Kæstel et al., 2005; Khan et al., 2016; Kirkwood et al., 2010; Korkmaz et al., 2014; Liu et al., 2013; Mohammad-Alizadeh-Charandabi et al., 2015; Moore et al., 2012; Ramakrishnan et al., 2003; Roberfroid et al., 2008; Roth et al., 2013; Hafeez et al., 2005a, 2005b; (AViDD); Roth et al., 2018 (MDIG); Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Sorouri et al., 2016; SUMMIT Study Group, 2008; Tofail et al., 2008; Vaziri et al., 2016; West et al., 2011; Zhao et al., 2015; Ashorn et al., 2015; Dewey, 2009; Osrin et al., 2005; West et al., 2014; Zeng et al., 2008).
Of these, 37 studies (Ahmad et al., 2016; Asemi et al., 2016; Belizán et al.,1997; Castillo-Durán et al., 2001; Christian et al., 2003; Dijkhuizen et al., 2001; Diogenes et al., 2013; Duggan et al., 2014; Etheredge et al., 2015; Fawzi et al., 2007; Friis et al., 2004; Gowachirapant et al., 2017; Hafeez et al., 2005a, 2005b; Hambidge et al., 2019; Hanieh et al., 2013; Hossain et al., 2012; Jarjou et al., 2006; Kæstel et al., 2005; Khan et al., 2016; Kirkwood et al., 2010; Korkmaz et al., 2014; Liu et al., 2013; Mohammad-Alizadeh-Charandabi et al., 2015; Moore et al., 2012; Ramakrishnan et al., 2003; Roberfroid et al., 2008; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Sorouri et al., 2016; SUMMIT Study Group, 2008; Tofail et al., 2008; Vaziri et al., 2016; West et al., 2011; Zhao et al., 2015) declared no conflict of interest amongst all authors. The five remaining studies (Ashorn et al., 2015; Dewey, 2009; Osrin et al., 2005; West et al., 2014; Zeng et al., 2008) indicated that one or several of the study's authors had a conflict of interest.
The remaining 30 studies (Aminisani et al., 2009; Asemi et al., 2013; Bhutta et al., 2009; Caulfield et al., 1999; Choudhury et al., 2012; Cox et al., 2005; Darling et al., 2017; Falahi, 2010; Huy et al., 2009; Huybregts et al., 2009; Kumar et al., 2009; López-Jaramillo et al., 1997; Menendez et al., 1995; Merialdi et al., 2004; Muslimatun et al., 2001; Naghshineh & Sheikhaliyan, 2016; Osendarp et al., 2000; Ouladsahebmadarek et al., 2011; Prawirohartono et al., 2011; Preziosi et al., 1997; Saaka et al., 2009; Semba et al., 2001; Sunawang et al., 2009; Taherian et al., 2002; Tanumihardjo, 2002; Villar et al., 2006; West et al., 1999; Zagré et al., 2007; Ziaei et al., 2007, 2008) did not provide any statement of disclosure, and thus we could not comment on any potential conflicts of interest.
Participants
The 64 studies included in the data analyses involved 439,649 women at varying gestational ages at baseline, ranging from early pregnancy (<20 weeks of gestation) to <37 weeks of gestation. Most participants were enrolled in the studies at <or equal to 20 weeks of gestation. Included participants were healthy and without anaemia (i.e. were not recruited based on anemia status), any chronic or systemic medical condition (e.g. cardiac disease, tuberculosis, human immuno-deficiency virus (HIV)), or heightened risk of pregnancy complication (e.g. history of pre-eclampsia/eclampsia). Two studies (Ashorn et al., 2015; Friis et al., 2004) included a subgroup of pregnant women who were HIV-positive; however, the data for these subgroups were not included in this review. Across all studies, baseline characteristics of participants in the intervention and control groups were comparable, except for the following studies: Christian et al (2003); Friis et al. (2004); Ramakrishnan et al. (2003); Roberfroid et al. (2008); Zagré et al. (2007). In Christian et al., (2003), the control group included more participants who represented a specific ethnic background and owned land compared to the intervention group. In Friis et al. (2004), there were more primigravidae participants in the placebo/control group than in the intervention group. In Ramakrishnan et al. (2003), the intervention group had a higher proportion of single mothers and participants with lower mean BMI than in the control group. In Roberfroid et al. 2008, the serum hemoglobin (Hb) level of participants in the intervention group was lower than in the control group, and maternal BMI was lower in the control group than in the intervention group. Finally, in Zagré et al. (2007) the placebo group included more participants who were less educated and living in poverty than in the intervention group; as well, there were more households and preventive measures against malaria amongst participants in the intervention group.
Intervention
All supplements were given orally and in the form of tablets (except for lipid-based supplements). Supplements were given to pregnant women throughout the remainder of their pregnancy from the time of enrolment.
IFA Supplementation versus Folic Acid Supplementation
Seven studies assessed IFA supplementation compared to folic acid supplementation or placebo (Christian et al., 2003; Etheredge et al., 2015; Liu et al., 2013; Menendez et al., 1995; Zeng et al., 2008; Zhao et al., 2015; Ziaei et al., 2007). Of these, 5 were included in the iron versus placebo comparison, with folic acid supplementation provided as a co-intervention (Christian et al., 2003; Etheredge et al., 2015; Liu et al., 2013; Menendez et al., 1995; Ziaei et al., 2007). Three studies had multiple intervention arms and were included in other comparisons: Christian et al., 2003; Liu et al., 2013; Zeng et al., 2008. Studies provided 30 mg to 60 mg of iron, with the majority providing 60 mg of iron, and 400-500 ug of folic acid in their supplements.
MMN supplementation versus IFA supplementation or placebo
Thirty-four studies assessed MMN versus IFA supplementation (Aminisani et al., 2009; Asemi et al., 2016; Ashorn et al., 2015; Bhutta et al., 2009; Caulfield et al., 1999; Choudhury et al., 2012; Christian et al. ,2003; Dewey, 2009; Dijkhuizen et al., 2001; Fawzi et al., 2007; Friis et al., 2004; Hafeez et al., 2005a, 2005b; Hanieh et al., 2013; Huy et al., 2009; Kæstel et al., 2005; Liu et al., 2013; Merialdi et al., 2004; Moore et al., 2012; Muslimatun et al., 2001; Osrin et al., 2005; Ramakrishnan et al., 2003; Roberfroid et al., 2008; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tofail et al., 2008; Villar et al., 2006; West et al., 2014; Zagré et al., 2007; Zeng et al., 2008).
For this review, MMN was defined as the provision of at least 3 micronutrients (e.g. iron, folic acid and vitamin A). Trials could be considered MMN even in situations where iron with or without folic acid was provided in a separate supplement. Thus, it is possible that these studies could be included in other comparisons as well. For example, where a study investigates the effects of vitamin A versus placebo supplementation, but all women are provided IFA as the standard of care, then data from this study would be included in the vitamin A versus placebo and MMN vs. IFA comparisons. There were twelve of these types of studies (Aminisani et al., 2009; Caulfield et al., 1999; Dijkhuizen et al., 2001; Hafeez et al., 2005a, 2005b; Merialdi et al., 2004; Muslimatun et al., 2001; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016; and Villar et al., 2006) that were included in other comparisons; mainly zinc versus placebo and vitamin A versus placebo. Asemi et al. (2016) evaluated calcium with vitamin D supplementation versus placebo (plus IFA), and was included in the MMN versus IFA comparison; however, this study was not included in any other comparison given the insufficient number of studies to undertake meta-analyses for calcium with vitamin D supplementation. Five studies had multiple intervention arms and were included in other comparisons: Ashorn et al., 2015; Christian et al., 2003; Dewey, 2009; Liu et al., 2013; Moore et al., 2012; Zeng et al., 2008.
The composition of MMN supplement varied across all studies. Eleven studies used the UNIMMAP formulation, developed by UNICEF, WHO and United Nations University (Bhutta et al., 2009; Huy et al., 2009; Kæstel et al., 2005; Liu et al., 2013; Osrin et al., 2005; Roberfroid et al., 2008; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tofail et al., 2008; Zagré et al., 2007; Zeng et al., 2008). Another 3 studies used an adapted UNIMMAP formulation which contained the exact same combination of vitamins and minerals, but in different dosages (Hanieh et al., 2013; Moore et al., 2012; West et al., 2014). The remaining 20 studies used non-UNIMMAP formulations for their MMN supplements (Aminisani et al., 2009; Asemi et al., 2016; Ashorn et al., 2015; Caulfield et al., 1999; Choudhury et al., 2012; Christian et al., 2003; Dewey, 2009; Dijkhuizen et al., 2001; Fawzi et al., 2007; Friis et al., 2004; Hafeez et al., 2005a, 2005b; Merialdi et al., 2004; Muslimatun et al., 2001; Ramakrishnan et al., 2003; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016 and Villar et al., 2006).
The dose of iron in the MMN supplement differed across all studies. The studies that used UNIMMAP all contained 30 mg of elemental iron (Bhutta et al., 2009; Huy et al., 2009; Kæstel et al., 2005; Liu et al., 2013; Osrin et al., 2005; Roberfroid et al., 2008; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tofail et al., 2008; Zagré et al., 2007; Zeng et al., 2008). Of the studies that used an adapted UNIMMAP formulation, 2 studies used 60 mg of iron (Hanieh et al., 2013; Moore et al., 2012) and 1 study used 27 mg of iron (West et al., 2014). Of the studies that used a non-UNIMMAP formulation for the MMN supplement, 7 studies included 60 mg of iron in their formulation (Caulfield et al., 1999; Choudhury et al., 2012; Christian et al., 2003; Fawzi et al., 2007; Merialdi et al., 2004; Muslimatun et al., 2001; Ramakrishnan et al., 2003). Seven other studies used dosages of iron <60 mg, ranging from 20 mg to 40 mg (Aminisani et al., 2009; Ashorn et al., 2015; Dewey et al., 2009; Dijkhuizen et al., 2001; Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016), while 2 studies used 66 mg of iron (Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG). Two studies (Friis et al., 2004; Hafeez et al., 2005a, 2005b) did not indicate the dose of iron in the MMN supplement.
Lipid-based nutrient supplementation versus MMN supplementation or placebo (control)
Four studies assessed LNS supplementation versus MMN supplementation or placebo (Ashorn et al., 2015; Dewey et al., 2009; Huybregts et al., 2009; Moore et al., 2012). Ashorn et al. (2015) and Dewey, 2009 utilized the same formulation for the LNS supplement, presented in a powder form: 20 g sachets containing 2.6 g protein, 10 g fat, 4.59 g linoleic acid, 0.59 g linolenic acid. These were given alongside a non-UNIMMAP formulation of multiple micronutrients. Huybregts et al. (2009) also provided a powder that contained 1.56 MJ of energy: carbohydrates 15.9 g, protein 14.7 g, fat 27.6 g, MUFA 12.1 g, PUFA 7.3 g, Omega-3 fatty acids 0.4 g, omega-6 fatty acids 7.0 g), 9.1 g total dietary fibre; this was given alongside a UNIMMAP MMN supplement. Moore et al. (2012) provided LNS that contained energy (746 kcal), protein (20.8 g), lipids (52.6 g), alongside a non-UNIMMAP MMN supplement.
Vitamin A versus placebo
Nine studies assessed vitamin A supplementation versus placebo (Cox et al., 2005; Darling et al., 2017; Kirkwood et al., 2010; Muslimatun et al., 2001; Prawirohartono et al., 2011; Semba et al., 2001; Tanumihardjo, 2002; West et al., 1999; West et al., 2011). Of these, 1 study was excluded from analysis (Prawirohartono et al., 2011). Studies provided vitamin A in doses ranging from 10,000 IU of retinol weekly to 70,000 IU of retinol weekly, with the majority of studies providing 17,000-25,000 IU of retinol weekly.
Zinc versus placebo
Thirteen studies assessed zinc supplementation versus placebo (Ahmad et al., 2016; Aminisani et al., 2009; Castillo-Durán et al., 2001; Caulfield et al., 1999; Christian et al., 2003; Darling et al., 2017; Dijkhuizen et al., 2001; Hafeez et al., 2005a, 2005b; Merialdi et al., 2004; Osendarp et al., 2000; Prawirohartono et al., 2011; Saaka et al., 2009; Sorouri et al., 2016). Of these, 1 was excluded from analysis (Prawirohartono et al., 2011). Studies provided zinc in doses ranging from 15 mg to 50 mg of zinc sulphate daily. The majority of studies provided 20 to 30 mg of zinc daily.
Iron versus placebo
Thirteen studies assessed iron supplementation versus placebo (Christian et al., 2003; Etheredge et al., 2015; Falahi et al., 2010; Korkmaz et al., 2014; Liu et al., 2013; Menendez et al., 1995; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Tanumihardjo, 2002; Zeng et al., 2008; Zhao et al., 2015; Ziaei et al., 2007, 2008). Of these, 1 was excluded from analysis (Korkmaz et al., 2014). Studies provided iron in doses ranging from 30 mg to 100 mg. The majority of studies provided 50 or 60 mg of iron; one study (Ouladsahebmadarek et al., 2011) provided 30 mg of iron and Preziosi et al., 1997 provided 100 mg.
Vitamin D versus placebo
Eleven studies assessed vitamin D supplementation versus placebo (Asemi et al., 2013; Hossain et al., 2012; Khan et al., 2016; Mohammad-Alizadeh-Charandabi et al., 2015; Naghshineh & Sheikhaliyan, 2016; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Vaziri et al., 2016). Studies provided doses of vitamin D ranging from 2800 IU to 75,000 IU of vitamin D weekly. The majority of studies provided vitamin D in doses ranging from 10,000 to 25,000 IU per week.
Calcium versus placebo
Five studies assessed calcium supplementation versus placebo (Belizán et al., 1997; Jarjou et al., 2006; Kumar et al., 2009; López-Jaramillo et al., 1997; Villar et al., 2006). Of these, 1 study was excluded from being pooled with other studies in meta-analysis (Jarjou et al., 2006). Studies provided calcium supplementation in doses ranging from 500 mg daily to 2000 mg of calcium daily.
Excluded studies
We excluded 1,364 studies from this review. Of these, 434 studies were excluded based on an ineligible intervention; 466 were of the wrong study design; 353 involved the wrong population (e.g. high-income country or child population); 75 reported ineligible outcomes; 17 involved the wrong comparison; 5 were abstracts; and 14 studies were inaccessible. Please see the Characteristics of excluded studies for the excluded studies found through our grey literature and hand-searches, and their respective reasons for exclusion (n = 295). For the remaining excluded studies (n = 1069) found through the various database searches and their respective reasons for exclusion, please refer to Tables 5–16.
Characteristics Table of Excluded Studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Characteristics table of excluded studies (Database Searches)
Risk of bias in included studies
The risk of bias of the included studies was overall low with at least 50% of the judgements at low risk for three domains (random sequence generation, allocation concealment, and incomplete outcome data. For the remaining four domains, at least 75% of the judgements were assessed as low risk. The domain with the highest risk of bias was incomplete outcome data (attrition bias). See Figures 1 and 2, and the Characteristics of included studies tables for further details on the risk of bias for each included study.

Study flow diagram
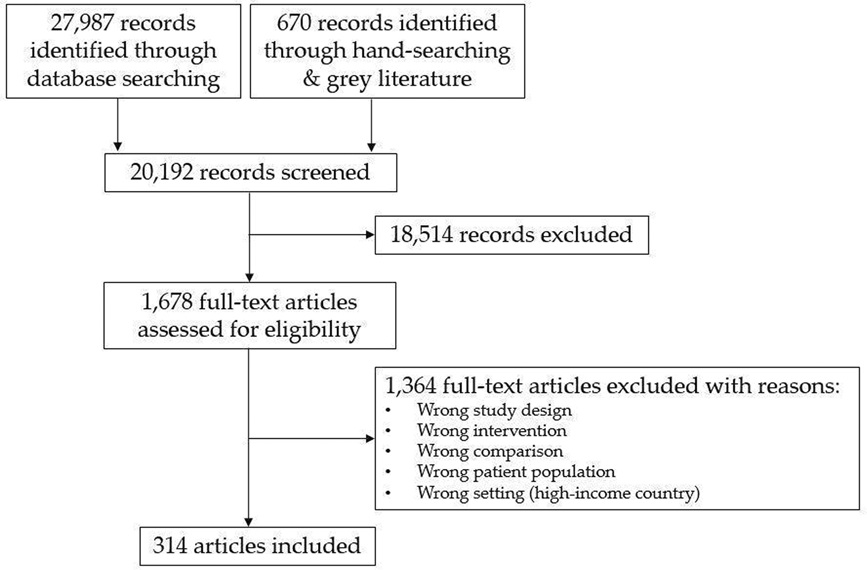
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
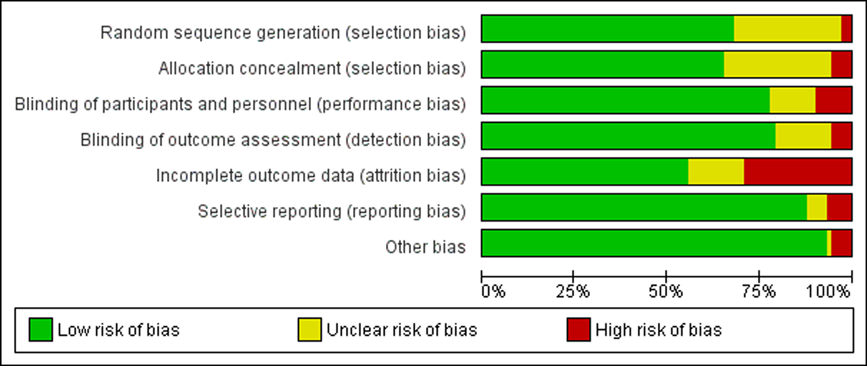
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study
Allocation (selection bias)
Randomisation Sequence Generation
The included studies were of variable risk of bias in terms of randomisation of participants. Of the 73 included studies, 21 did not mention or describe the method used to generate a randomisation sequence in sufficient detail to permit judgement (Ahmad et al., 2016; Aminisani et al., 2009; Castillo-Durán et al., 2001; Caulfield et al.,1999; Choudhury et al., 2012; Dijkhuizen et al., 2001; Falahi 2010; Kumar et al., 2009; Menendez et al., 1995; Muslimatun et al., 2001; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Sabet et al., 2012; Sahu et al., 2009; Semba et al., 2001; Sunawang et al., 2009; Taherian et al., 2002; Tanumihardjo et al., 2002; Tofail et al., 2008; Vaziri et al., 2016; Zagré et al., 2007). Two studies were assessed as high risk related to randomisation (Huy et al., 2009; Mohammad-Alizadeh-Charandabi et al., 2015). The remaining studies adequately reported randomisation procedures for assigning participants to the intervention and control groups.
Allocation Concealement
The included studies were of variable risk of bias in terms of allocation concealment. Of the included studies, 19 studies did not mention or describe the method used to allocate concealment in sufficient detail to permit judgement Ahmad et al., 2016; Asemi et al., 2016; Christian et al., 2003; Falahi 2010; Hossain et al., 2012; Kæstel et al., 2005; López-Jaramillo et al., 1997; Muslimatun et al., 2001; Naghshineh & Sheikhaliyan, 2016; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Sabet et al., 2012; Sahu et al., 2009; Sunawang et al., 2009; Taherian et al., 2002; Tanumihardjo et al., 2002; Tofail et al., 2008; Vaziri et al., 2016; Zagré et al., 2007). Four studies were assessed as high risk for allocation concealment (Huy et al., 2009; Huybregts et al., 2009; Menendez et al., 1995; Sablok et al., 2015). The remaining studies had adequate allocation concealment of participants to the intervention and control groups.
Blinding (performance bias and detection bias)
For several included studies, it was unclear whether participants and personnel were appropriately blinded to the treatment allocation (Choudhury et al., 2012; Hossain et al., 2012; Kæstel et al., 2005; Moore et al., 2012; Muslimatun et al., 2001; Ouladsahebmadarek et al., 2011; Sahu et al., 2009; Sunawang et al., 2009; Taherian et al., 2002). Seven studies were assessed as high risk in terms of blinding (Diogenes et al., 2013; Hambidge et al., 2019; Huy et al., 2009; Huybregts et al., 2009; Menendez et al., 1995; Preziosi et al., 1997; Sablok et al., 2015).
In terms of blinding of outcome assessors, eleven studies did not clearly describe the method used to blind outcome assessors to permit judgement (Choudhury et al., 2012; Hambidge et al., 2019; Hossain et al., 2012; Kæstel et al., 2005; Muslimatun et al., 2001; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Sabet et al., 2012; Sahu et al., 2009; Sunawang et al., 2009; et al., Taherian 2002). Four studies did not adequately blind outcome assessors, and were thus assessed as high risk (Diogenes et al., 2013; Huy et al., 2009; Huybregts et al., 2009; Sablok et al., 2015).
Incomplete outcome data (attrition bias)
Loss to follow up was >20% in 21 studies (Ahmad et al., 2016; Castillo-Durán et al., 2001; Caulfield et al., 1999; Darling et al., 2017; Dijkhuizen et al., 2001; Diogenes et al., 2013; Duggan et al., 2014; Friis et al., 2004; Hambidge et al., 2019; Huy et al., 2009; Moore et al., 2012; Muslimatun et al., 2001; Osendarp et al., 2000; Osrin et al., 2005; Ouladsahebmadarek et al., 2011; Prawirohartono et al., 2011; Ramakrishnan et al., 2003; Sahu et al., 2009; Semba et al., 2001; Tofail et al., 2008; Zhao et al., 2015). Thus, these studies were assessed as high-risk for incomplete outcome data. Zagré et al. (2007) reported an attrition less than 20%; however, the proportion of women who dropped out was significantly higher in the MMN group versus the IFA group. Thus, this study was assessed as unclear risk. Other studies that were deemed unclear risk were: Falahi 2010; Gowachirapant et al., 2017; Huybregts et al., 2009; Kæstel et al., 2005; Kirkwood et al., 2010; Korkmaz et al., 2014; Preziosi et al., 1997; Sablok et al., 2015; Taherian et al., 2002; West et al., 1999).
Selective reporting (reporting bias)
In the majority of the included studies, there was no indication of selective reporting. However, in four studies, incidence of selective reporting was unclear (Asemi et al., 2013; Kirkwood et al., 2010; Prawirohartono et al., 2011; Sablok et al., 2015). In five additional studies, the risk of selective reporting was assessed as high, as authors did not report all of the outcomes described in the methods (Caulfield et al., 1999; Hambidge et al., 2019; Hanieh et al., 2013; Semba et al., 2001; Zhao et al., 2015).
Other potential sources of bias
In the majority of the included studies we did not identify other possible sources of bias. Sablok 2015 was assessed as unclear risk given that the intervention and control groups were significantly different in size. Four studies were assessed as high risk for other sources of bias (Gowachirapant et al., 2017; Kirkwood et al., 2010; Prawirohartono et al., 2011; West et al., 2011). In Gowachirapant et al. (2017), authors indicated that their iodine concentration measurements were not accurately conducted and that participants may have been mis-classified. They also stated that iodine nutrition may have influenced participants' behaviours to consume more iodine rich foods. In Kirkwood et al. (2010), the authors revealed that women were switched into different treatment arms if they migrated to a different cluster area. Prawirohartono et al. (2011) began in 1994; however, results of the original study were not published with reasons not provided. The results presented here pertain to follow-up studies conducted in 2011 and 2013. Lastly, authors of West et al. (2011) indicated that the vitamin A supplementation outcomes may have been biased by women receiving vitamin A to treat for night blindness.
Effects of interventions
Comparison I: IFA versus Folic Acid
Seven studies contributed to this comparison (Christian et al., 2003; Etheredge et al., 2015; Liu et al., 2013; Menendez et al., 1995; Zeng et al., 2008; Zhao et al., 2015; Ziaei et al., 2007). Of these, 2 studies were conducted in sub-Saharan Africa (Etheredge et al., 2015; Menendez et al., 1995), 3 in East Asia Pacific, specifically in China (Liu et al., 2013; Zeng et al., 2008; et al., Zhao 2015), 1 in Nepal, South Asia (Christian et al., 2003) and 1 in Iran, Middle East & North Africa (Ziaei et al., 2007). Three studies utilized a similar formulation of IFA supplement; the equivalent of 60 mg elemental iron and 400 ug folic acid (Christian et al., 2003; Zeng et al., 2008; Zhao et al., 2015). Liu et al. 2013 used 30 mg of iron and 400 ug of folic acid, while Etheredge et al. (2015) and Menendez et al. (1995) utilized 60 mg of iron and 5 mg of folic acid, and Ziaei 2007 used 50 mg of iron and 1 mg of folic acid. In one study, women received 1000 ug vitamin A daily with their supplements (Christian et al., 2003), and in another study, women received iron and folic acid in separate capsules (Zhao et al., 2015). For all studies, participants began supplementation at enrolment and continued until delivery. Liu et al. (2013) began supplementation at the women's first prenatal visit until delivery. Etheredge 2015 stated that enrolment was at or before 27 weeks of gestation; while Zhao et al. (2015) stated enrolment began at the first prenatal visit, and Ziaei et al. (2007) stated that women were in their early stage of the second trimester at enrolment. Enrolment was undefined and unclear in 3 studies Christian et al., 2003; Menendez et al., 1995; Zeng et al., 2008.
Primary Outcomes
When comparing IFA to folic acid supplementation, maternal anaemia was reduced by 48% (average risk ratio (RR) 0.52, 95% confidence interval (CI) 0.41 to 0.66; studies = 5; participants = 15,540; random effects; Tau2 = 0.07; I2 = 88%; moderate quality evidence; Analysis 1.1). IFA supplementation also reduced low birthweight (average RR 0.88, 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; random-effects; Tau2 = 0.00%; I2 =0%; high quality evidence; Analysis 1.2); however, IFA probably did not reduce perinatal mortality (average RR 0.88, 95% CI 0.71 to 1.08; studies = 4; participants = 17,464; random-effects; Tau2 = 0.00; I2 = 0%; moderate quality evidence; Analysis 1.3) when compared to supplementation with folic acid alone.
Secondary Outcomes
When compared to folic acid alone, IFA supplementation increased maternal hemoglobin concentration (average mean difference (MD) 6.95 g/L; 95% CI 2.80 to 11.1; studies = 7; participants = 16,089; random-effects; Tau2 = 29.46; I2 = 98%; Analysis 1.4). Likewise, IFA supplementation increased maternal serum/plasma ferritin (average MD 15.87 ug/L; 95% CI 2.96 to 28.79; studies = 5; participants = 3,894; random-effects; Tau2 = 194.91; I2 = 100%; Analysis 1.5), though there was no difference in maternal serum/plasma transferrin receptor (average MD -0.16; 95% CI -0.96 to 0.65; studies = 3; participants = 2,431; random-effects; Tau2 = 0.46; I2 = 99%; Analysis 1.6). Additionally, there was no difference in neonatal mortality (average RR 0.85; 95% CI 0.55 to 1.31; studies = 3; participants = 15,794; Tau2 = 0.07; I2 = 47%; Analysis 1.7), preterm births (average RR 0.96 95% CI 0.64 to 1.44; studies = 5; participants = 17,637; random-effects; Tau2 = 0.18; I2 = 96%; Analysis 1.8), SGA (average RR 1.03; 95% CI 0.87 to 1.23; studies = 4; participants = 6,549; random-effects; Tau2 = 0.02; I2 = 69%; Analysis 1.9), or infant mortality (average RR 1.10; 95% CI 0.84 to 1.45; studies = 3; participants = 14,748; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 1.10) when comparing IFA and folic acid supplementation.
Subgroup Analysis
Due to insufficient data (this review required > or equal to 3 studies per subgroup of interest), subgroup analyses of the primary outcomes were not conducted based on maternal age, geographical region, sex of infant, baseline nutritional status in mothers (anemic vs. non-anemic; undernutrition vs. normal nutrition based on body mass index: BMI <18.5; low stature vs. normal stature), duration of intervention, time of recruitment (preconception vs. first trimester vs. second trimester vs. third trimester of pregnancy), daily vs. intermittent IFA supplementation and dose of intervention.
Comparison II: MMN versus IFA
Thirty-four studies contributed data to this comparison (Aminisani et al., 2009; Asemi et al., 2016; Ashorn et al., 2015; Bhutta et al., 2009; Caulfield et al., 1999; Choudhury et al., 2012; Christian et al., 2003; Dewey et al., 2009; Dijkhuizen et al., 2001; Fawzi et al., 2007; Friis et al., 2004; Hafeez et al., 2005a, 2005b; Hanieh et al., 2013; Huy et al., 2009; Kæstel et al., 2005; Liu et al., 2013; Merialdi et al., 2004; Moore et al., 2012; Muslimatun et al., 2001; Osrin et al., 2005; Ramakrishnan et al., 2003; Roberfroid et al., 2008; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tofail et al., 2008; Villar et al., 2006; West et al., 2014; Zagré et al., 2007; Zeng et al., 2008). Of these, 10 studies were conducted in sub-Saharan Africa; 2 conducted in Ghana (Dewey et al., 2009; Saaka et al., 2009); 2 in Malawi (Ashorn et al. (2015); Semba et al. (2001); 1 each in Burkina Faso (Roberfroid et al., 2008); Gambia (Moore et al., 2012); Guinea-Bissau (Kæstel et al., 2005); Tanzania (Fawzi et al., 2007); Zimbabwe (Friis et al., (2004); and Niger (Zagré et al., 2007). Eight studies were conducted in the East Asia & Pacific region; 4 were conducted in Indonesia (Dijkhuizen et al., 2001; Muslimatun et al., 2001; SUMMIT Study Group, 2008; Sunawang et al., 2009), 2 in Vietnam Hanieh et al., 2013; Huy et al., 2009) and 2 in China (Liu et al., 2013; Zeng et al., 2008). Nine studies were conducted in the South Asia region; of which 5 were conducted in Bangaldesh (Choudhury et al., 2012; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Tofail et al., 2008; West et al., 2014), 2 in Nepal (Christian et al., 2003; Osrin et al., 2005), 2 in Pakistan (Bhutta et al., 2009; Hafeez et al., 2005a, b). Three studies were conducted in Latin America & the Caribbean: 2 in Peru (Caulfield et al., 1999; Merialdi et al., 2004) and 1 in Mexico (Ramakrishnan et al., 2003). Three studies were conducted in the Middle East & North Africa; all in Iran (Aminisani et al., 2009; Asemi et al., 2016; Sorouri et al., 2016). One study, Villar et al. (2006), was a multi-country study, conducted in India, Peru, South Africa and Vietnam.
Eleven studies used the UNIMMAP formulation, developed by UNICEF, WHO and United Nations University (Bhutta et al., 2009; Huy et al., 2009; Kæstel et al., 2005; Liu et al., 2013; Osrin et al., 2005; Roberfroid et al., 2008; SUMMIT Study Group, 2008; Sunawang et al., 2009; Tofail et al., 2008; Zagré et al., 2007; Zeng et al., 2008). The UNIMMAP formulation consists of 800 RE of vitamin A, 200 IU vitamin D, 10 mg of vitamin E, 70 mg of vitamin C, 1.4 mg of thiamin, 1.4 mg of riboflavin, 18 mg of niacin, 1.9 mg of pyridoxine, 2.6 mg of cobalamin, 400 ug of folic acid, 30 mg of iron, 15 mg of zinc, 2 mg of copper, 65 mg of selenium and 150 ug of iodine. Three studies used an adapted UNIMMAP formulation which contained the exact same combination of vitamins and minerals, but in different dosages (Hanieh et al., 2013; Moore et al., 2012; West et al., 2014). Hanieh et al. (2013) used 60 mg of iron and 1500 ug of folic acid; Moore et al. (2012) used a formulation that doubled the volume of every component of the UNIMMAP formulation, along with 60 mg of iron and 400 ug of folic acid. West 2014 changed the volumes of vitamin A (770 retinol equivalents), vitamin E (15 mg), vitamin C (85 mg), folic acid (600 ug), iron (27 mg), zinc (12 mg), copper (1 mg), selenium (60 ug and iodine (220 ug).
The remaining 20 studies used non-UNIMMAP formulations for their MMN supplements (Aminisani et al., 2009; Asemi et al., 2016; Ashorn et al., 2015; Caulfield et al., 1999; Choudhury et al., 2012; Christian et al., 2003; Dewey et al., 2009; Dijkhuizen et al., 2001; Fawzi et al., 2007; Friis et al., 2004; Hafeez et al., 2005; Merialdi et al., 2004; Muslimatun et al., 2001; Ramakrishnan et al., 2003; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016; and Villar et al., 2006). Of this list, Aminisani et al., 2009; Caulfield et al., 1999; Dijkhuizen et al., 2001; Villar et al., 2006; Hafeez et al., 2005; Merialdi et al., 2004; Muslimatun et al., 2001; Roth et al., 2013 (AViDD); Saaka et al., 2009; Semba et al., 2001; Sorouri et al., 2016 used MMN formulations that included iron, folic acid and 1 other micronutrient, typically zinc or vitamin A. Choudhury et al. (2012) and Roth et al. (2018) (MDIG) utilized MMN supplements that contained 4 components; Choudhury et al. (2012) used iron 60 mg, 400 ug of folic acid, 30 mg of vitamin C and 5 mg of zinc, and Roth et al. (2018) (MDIG) used iron 66 mg, folic acid 350 ug, calcium 500 mg and vitamin D (dosages differed across different arms). The remaining studies (Ashorn et al., 2015; Dewey et al., 2009; Fawzi et al., 2007; Friis et al., 2004; and Ramakrishnan et al., 2003) used formulations that had many micronutrient and vitamin components that differed from UNIMMAP. For example, some used the UNIMMAP formulation with the addition of pantothenic acid, vitamin K, and manganese (Ashorn et al., 2015; Dewey et al., 2009). The other studies removed some of the UNIMMAP components and added others into their study formulations (Fawzi et al., 2007; Friis et al., 2004; and Ramakrishnan et al., 2003).
In addition to any pre-specified, per-protocol subgroup analyses, an exploratory post-hoc analysis based on the number of micronutrients and vitamins comprised in each supplement (supplements containing 3 or 4 micronutrients versus supplements containing >4 micronutrients) was conducted for all outcomes. Post-hoc analyses were conducted for the following outcomes: maternal anaemia, maternal iron-deficiency anaemia, low birthweight, perinatal mortality, maternal serum/plasma hemoglobin concentration, maternal serum/plasma ferritin concentration, maternal iron deficiency, maternal serum/plasma transferrin receptor concentration, maternal serum/plasma retinol concentration, maternal serum/plasma zinc concentration, maternal serum/plasma folate concentration, maternal serum/plasma vitamin B12 concentration, stillbirths, congenital anomalies, preterm births, SGA, mode of delivery - Caesarean section, neonatal mortality, development outcomes: general intelligence, verbal comprehension and language, and motor function, child diarrhea, child serum/plasma hemoglobin concentration, child serum/plasma ferritin concentration, child serum/plasma retinol concentration, and child serum/plasma zinc concentration.
Primary Outcomes
Compared to iron with or without folic acid supplementation, MMN supplementation made no difference to maternal mortality (average RR 1.04, 95% CI 0.71 to 1.51; studies = 6; participants = 75,051; random-effects; Tau2 = 0.00; I2 = 0%; moderate quality evidence; Analysis 2.1) and had no effect on maternal anaemia (average RR 1.02; 95% CI 0.95 to 1.10; studies = 16; participants = 23,356; random-effects; Tau2 = 0.01; I2 = 57%; high quality evidence; Analysis 2.2). A post-hoc analysis comparing studies with MMN containing >4 micronutrients to those with MMN containing 3 or 4 micronutrients showed no difference in the effects on maternal anaemia.
Maternal iron deficiency anaemia was not improved, though the certainty of evidence was very low (average RR 1.12; 95% CI 0.62 to 2.02; studies = 4; participants = 1,595; random-effects; Tau2 = 0.24; I2 = 73%; very low quality evidence; Analysis 2.3). Post-hoc analysis comparing studies based on supplement composition showed no difference in effect.
MMN supplementation had a large effect on low birthweight, reducing the risk by 15% (average RR 0.85; 95% CI 0.77 to 0.93; studies = 28; participants = 79,972; random-effects; Tau2 = 0.03; I2 = 70%; high quality evidence; Analysis 2.4). However, post-hoc analysis comparing the subgroups of studies whose MMN formulation contained >4 micronutrients to those whose formulation contained <or equal to 4 micronutrients, revealed that the former subgroup demonstrated a greater reduction in risk of low birthweight (average RR 0.79, 95% CI 0.71 to 0.88; studies = 19; participants = 68,138; random-effects; Tau2 = 0.03; I2 = 74%; Analysis 2.3.1 versus average RR 1.01, 95% CI 0.92 to 1.11; studies = 9; participants = 11,834; random-effects; Tau2 =0.00; I2 = 1%; Analysis 2.3.2). There was a significant difference between subgroups (test for subgroup differences: Chi2 = 11.51; P = 0.0007).
Compared to IFA, MMN did not demonstrate any important effect on perinatal mortality (average RR 1.00; 95% CI 0.90 to 1.11; studies = 16; participants = 92,769; random-effects; Tau2 = 0.01; I2 = 43%; high quality evidence; Analysis 2.5). Post hoc-analysis showed no difference in perinatal mortality between studies with MMN containing >4 micronutrients (average RR 0.97; 95% CI 0.88 to 1.07; studies = 14; participants = 90,959; random effects; Tau2 = 0.01; I2 = 33%; Analysis 2.5.1) compared to MMN with <or equal to 4 micronutrients (average RR 1.79; 95% CI 0.56 to 5.76; studies = 2; participants = 1,810; random effects; Tau2 = 0.38; I2 = 25%; Analysis 2.5.2). The test for sub-group differences was non-significant (test for subgroup differences: Chi2 = 1.06, P = 0.30).
Secondary Outcomes
Compared to iron with or without folic acid supplementation, MMN supplementation made no difference to maternal hemoglobin (average MD -0.34 g/L, 95% CI -1.53 to 0.86; studies = 16; participants = 26,312; random-effects; Tau2 = 4.61; I2 = 92%; Analysis 2.6) and ferritin concentrations (average MD -2.37 ug/L, 95% CI -7.84 to 3.10; studies = 11; participants = 5,149; random-effects; Tau2 = 79.82; I2 = 100%; Analysis 2.7). Similarly, MMN supplementation had no effect on maternal iron deficiency (average RR 1.39; 95% CI 0.88 to 2.20; studies = 3; participants = 1,182; random-effects; Tau2 = 0.14; I2 = 86%; Analysis 2.8). Post-hoc analyses for maternal hemoglobin and ferritin concentrations, and maternal iron deficiency all showed no differences in the effects between studies that provided supplements with >4 micronutrients and studies whose formulations contained 3 or 4 micronutrients. MMN supplementation may have slightly improved maternal serum transferrin receptor concentration, although the confidence interval of the pooled estimate just crossed the line of no effect (average MD 0.12 mg/L; 95% CI -0.03 to 0.27; studies = 7, participants = 2,550; random-effects; Tau2 = 0.02; I2 = 79%; Analysis 2.9).
Similarly, MMN supplementation slightly improved maternal serum retinol concentration (average MD 0.11 umol/L; 95% CI 0.05 to 0.17; studies = 7; participants = 3,111; random-effects; Tau2 = 0.00; I2 = 60%; Analysis 2.10), maternal serum zinc concentration (average MD 0.40 umol/L; 95% CI 0.18 to 0.62; studies = 5; participants = 3028; random-effects; Tau2 = 0.07; I2 = 49%, Analysis 2.11), and maternal serum vitamin B12 concentration (average MD 14.77 pmol/L; 95% CI 5.13 to 24.42; studies = 3; participants = 962; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.12), but had no effect on maternal serum folate concentration (average MD -1.66 nmol/L; 95% CI -4.75 to 1.08; studies = 5; participants = 2,614; random-effects; Tau2 = 10.28; I2 = 79%; Analysis 2.13).
MMN supplementation probably did not improve the risk of miscarriage (average RR 0.99; 95% CI 0.94 to 1.04; studies = 13; participants = 88,971; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.14). However, MMN supplementation did reduce the risk of stillbirths (average RR 0.91; 95% CI 0.86 to 0.98; studies = 22; participants = 96,772; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.15) when compared to IFA. In a post-hoc analysis, no significant differences in stillbirths were observed between MMN formulation groups (test for subgroup differences: Chi2 = 0.05; P = 0.82).
MMN supplementation, compared to IFA, did not reduce congenital anomalies (average RR 0.73; 95% CI 0.41 to 1.29; studies =7; participants = 4,195; random-effects; I2 = 0%; Analysis 2.16), but may have slightly reduced births that were considered preterm, although the line of no effect just crosses one (average RR 0.96, 95% CI 0.91 to 1.01; studies = 29; participants = 99,855; random-effects; Tau2 = 0.00; I2 = 37%; Analysis 2.17). In post-hoc analysis, no significant differences were observed between studies that provided MMN comprised of of 3 or 4 micronutrients versus MMN comprised of >4 micronutrients (test for subgroup differences: Chi2 = 0.69; P = 0.41). MMN supplementation showed a small 7% improvement in the risk of babies considered SGA overall (average RR 0.93; 95% CI 0.88 to 0.98; studies = 19; participants = 52,965; random-effects; Tau2 = 0.00; I2 = 38%; Analysis 2.18). However, when comparing MMN supplement formulations, there were significant differences in SGA between groups (test for subgroup differences: Chi2 = 10.49; P = 0.001). Women who took MMN supplements comprised of >4 micronutrients showed greater reduction in risk of SGA when compared to women who took MMN with <or equal to 4 micronutrients (average RR 0.90; 95% CI 0.85 to 0.96; studies = 16; participants = 50,788; random-effects, Tau2 = 0.00; I2 = 33%; Analysis 2.19.1 compared to average RR 1.07; 95% CI 0.98 to 1.16; studies = 3; participants = 2,177; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.19).
MMN supplementation during pregnancy overall had no effect on reducing the risk of Caesarean section as a mode of delivery (average RR 1.00; 95% CI 0.94 to 1.07; studies = 11; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.19). Post-hoc analysis showed no significant difference between studies which provided MMN with 3 or 4 micronutrients (average RR 0.97; 95% CI 0.90 to 1.04; studies = 6; participants = 10,527; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.19.2) when compared to and studies that provided MMN with >4 micronutrients (average RR 1.13; 95% CI 0.99 to 1.29; studies = 5; participants = 13,217; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.19.1) (test for subgroup differences: Chi2 = 3.86, P = 0.05).
For outcomes pertaining to the child, MMN supplementation probably did not reduce the risk of neonatal mortality overall (average RR 0.98; 95% CI 0.90 to 1.06; studies = 17; participants = 82,293; random-effects; I2 = 14%; Analysis 2.20). No significant differences were observed between studies that used MMN supplements comprised of >4 micronutrients and studies using MMN supplements containing <or equal to 4 micronutrients (test for subgroup differences: Chi2 = 1.65, P = 0.20).
Compared to IFA, MMN supplementation during pregnancy probably had no effect on reducing infant mortality (average RR 0.99; 95% CI 0.92 to 1.08; studies = 10; participants = 55,595; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.21). In terms of nutritional indicators, MMN supplementation had no effect on the risk of child wasting (average RR 1.02; 95% CI 0.88 to 1.18; studies = 5; participants = 9,671; random-effects; Tau2 = 0.00; I2 = 7%; Analysis 2.22), stunting (average RR 0.99; 95% CI 0.92 to 1.07; studies = 7; participants = 11,264; random-effects; Tau2 = 0.00; I2 = 30%; Analysis 2.23), or underweight (average RR 0.95; 95% CI 0.84 to 1.07; studies = 4; participants = 931; random-effects; Tau2 = 0.01; I2 = 45%; Analysis 2.24).
There were four types of child developmental outcomes that were assessed in this comparison group: general intelligence, verbal comprehension and language, motor function, and executive function scores. Compared to IFA, MMN supplementation showed no effect on general intelligence (standard MD 0.00; 95% CI -0.06 to 0.07; studies = 8; participants = 12,172; Tau2 = 0.00; I2 = 36%; Analysis 2.25), and showed no effect on motor function (standard MD -0.02; 95% CI -0.17 to 0.13; studies = 7; participants = 12,057; random-effects, Tau2 = 0.03; I2 = 89%; Analysis 2.26). There was also no difference in effect of MMN supplementation compared to IFA on verbal comprehension and language (standard MD 0.02; 95% CI -0.13 to 0.16; studies = 4; participants = 10,781; random-effects, Tau2 = 0.02; I2 = 84%; Analysis 2.27). However, MMN supplementation compared to IFA did have a positive effect on executive function scores (standard MD 0.09; 95% CI 0.01 to 0.17; studies = 3; participants = 2,511; random-effects, Tau2 = 0.00; I2 = 0%; Analysis 2.28).
Compared to IFA, MMN supplementation during pregnancy reduced the occurrence of diarrhea in children (average RR 0.84; 95% CI 0.76 to 0.92; studies = 4; participants = 3142; random-effects; I2 = 0%; Analysis 2.29). Maternal MMN supplementation had no impact on child hemoglobin concentration (average MD 0.01 g/L; 95% CI -0.63 to 0.66; studies = 7; participants = 13,067; random-effects; Tau2 = 0.25; I2 = 61%; Analysis 2.30) or on ferritin levels (average MD 1.85 ug/L; 95% CI -0.81 to 4.50; studies = 4; participants = 1,443; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.32). MMN supplementation, when compared to IFA, demonstrated slight improvements in child serum retinol concentrations (average MD 0.06 umol/L; 95% CI 0.02 to 0.09; studies = 3; participants = 868; random-effects; Tau2 = 0.00; I2 = 69%; Analysis 2.31). MMN supplementation did not have any major impact on zinc concentrations in children (average MD 0.04 umol/L; 95% CI -0.21 to 0.30; studies = 3; participants = 944; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 2.33), nor on anaemia among children (average RR 0.83; 95% CI 0.54 to 1.27; studies = 3; participants = 1,458; random-effects; Tau2 = 0.13; I2 = 92%; Analysis 2.34).
Subgroup Analysis
Subgroup analyses were conducted for the MMN vs. IFA comparison for maternal mortality, maternal anaemia, perinatal mortality and low birthweight based on MMN formulation (UNIMMAP vs. adapted UNIMMAP vs. non-UNIMMAP formulations), geographical region, duration of intervention and dose of iron. Please see below for results under heading 'Subgroup Analysis I: MMN supplementation versus IFA'.
Comparison III: LNS versus MMN
Four randomized controlled trials that assessed LNS supplementation against MMN reported eligible outcomes (Ashorn et al., 2015; Dewey et al., 2009; Huybregts et al., 2009; Moore et al., 2012). Each study was conducted in Africa and in a rural setting, except Dewey et al. (2009) which was conducted in a peri-urban setting. In 2 studies, women were provided supplements throughout pregnancy only (Huybregts et al., 2009; Moore et al., 2012), while in Ashorn et al. (2015) and Dewey et al. (2009), supplementation was continued up to 6 months postpartum. LNS supplementation was daily, and came packaged within a 20 g foil sachet in 2 studies (Ashorn et al., 2015; Dewey et al., 2009). Moore et al. (2012) and Huybregts et al. (2009) provided participants with daily LNS in the form of a fatty spread. Daily MMN supplementation was provided in the form of tablets to the control groups across all studies, but with variable composition. Three studies utilized a non-UNIMMAP formulation (Dewey et al., 2009; Ashorn et al., 2015; Moore et al., 2012), while the fourth used UNIMMAP tablets. In Dewey et al. (2009) and Ashorn et al., 2015, the iron concentration in the MMN tablet was 20 mg while in Moore et al., 2012, it was 60 mg. Folic acid in the MMN tablets was 400 ug across all studies. Three studies provided participants with intermittent preventive treatment of malaria (Ashorn et al., 2015; Dewey et al., 2009; Huybregts et al., 2009).
Primary outcomes
Compared to MMN, LNS supplementation had no effect on the risk of LBW (average RR 0.92; 95% CI 0.75 to 1.13; studies = 4; participants = 2,727; random-effects; Tau2 = 0.0, I2= 0.0%; moderate quality evidence; Analysis 3.1) and made no difference to perinatal mortality (average RR 1.01; 95% CI 0.65 to 1.65; studies = 3; participants = 2,771; random-effects; Tau2 = 0.04, I2= 21%; low quality evidence; Analysis 3.2).
Secondary Outcomes
There was no difference in the risk of miscarriage between participants supplemented with LNS compared to those supplemented with MMN (average RR 1.12, 95% CI 0.69 to 1.80; studies = 3; participants = 2,865; random-effects; Tau2 = 0.0, I2= 0.0%; Analysis 3.3). Compared to MMN, LNS supplementation made no difference in the risk of stillbirths (average RR 0.47; 95% CI 0.12 to 1.81; studies = 3; participants = 2,481; random-effects; Tau2 = 0.0, I2= 0.0%; Analysis 3.4). Similarly, there were no effects of LNS on neonatal mortality (average RR 0.81; 95% CI 0.45 to 1.45; studies = 3; participants = 2,727; random-effects; Tau2 = 0.0, I2= 0.0%; Analysis 3.5) or on preterm birth (average RR 1.15; 95% CI 0.93 to 1.42; studies = 4; participants = 2,953; random-effects, Tau2 = 0.0, I2= 0.0%; Analysis 3.6). LNS supplementation did not reduce the risk of SGA infants (average RR 0.96; 95% CI 0.86 to 1.07; studies = 4; participants = 2,716; random-effects, Tau2 = 0.0, I2= 0.0%; Analysis 3.7).
Subgroup Analysis
Due to insufficient data (this review required > or equal to three studies per subgroup of interest), subgroup analyses of the primary outcomes were not conducted based on maternal age, geographical region, sex of infant, baseline nutritional status in mothers (anemic vs. non-anemic; undernutrition vs. normal nutrition based on body mass index: BMI <18.5; low stature vs. normal stature), duration of intervention, time of recruitment (preconception vs. first trimester vs. second trimester vs. third trimester of pregnancy), daily vs. intermittent IFA supplementation and dose of intervention.
Comparison IV: Vitamin A versus Placebo
Nine studies evaluated vitamin A supplementation versus placebo (Cox et al., 2005; Darling et al., 2017; Kirkwood et al., 2010; Muslimatun et al., 2001; Semba et al., 2001; Tanumihardjo et al., 2002; Prawirohartono et al., 2011; West et al., 1999; West et al., 2011). Of these, 4 studies were conducted in sub-Saharan Africa, with 2 in Ghana and 1 each in Malawi and Tanzania (Cox 2005 et al.,; Darling et al., 2017; Kirkwood et al., 2010; Semba et al., 2001). Three studies were conducted in East Asia & Pacific, specifically in Indonesia (Muslimatun et al., 2001; Tanumihardjo et al., 2002; Prawirohartono et al., 2011), and 2 studies were conducted in Nepal and Bangladesh, South Asia (West et al., 1999; West et al., 2011). Four studies gave participants supplementation from enrolment to the end of pregnancy or delivery (Darling et al., 2017; Muslimatun et al., 2001; Semba et al., 2001; West et al., 1999). Cox et al. (2005) provided supplementation from enrolment until 6 weeks postpartum and in West et al. (2011), participants received supplements from enrolment to 12 weeks postpartum. One study did not explicitly state when the intervention ended (Kirkwood et al., 2010).
Of these 9 studies, one was excluded from meta-analysis because no common outcomes of interest were reported (Prawirohartono et al., 2011). For a narrative synthesis of this study, see below under 'Other studies and comparisons not included in meta-analysis'.
Eight studies were included in the meta-analysis of vitamin A supplementation versus placebo (Cox et al., 2005; Darling et al., 2017; Kirkwood et al., 2010; Muslimatun et al., 2001; Semba et al., 2001; Tanumihardjo et al., 2002; West et al., 1999; West et al., 2011).
Primary outcomes
Compared to placebo, vitamin A supplementation did not affect maternal mortality (average RR 0.90; 95% CI 0.68 to 1.18; studies = 3; participants = 124,002; random-effects; Tau2 = 0.02; I2 = 35%; low quality evidence; Analysis 4.1).
Secondary outcomes
Vitamin A supplementation, when compared to placebo, had no effect on maternal hemoglobin concentration (average MD 0.51 g/L; 95% CI -2.42 to 3.43; studies = 5; participants = 1,683; random-effects; Tau2 = 4.23; I2 = 41%; Analysis 4.2), but may have slightly improved maternal serum retinol (average MD 0.13 umol/L; 95% CI -0.03 to 0.30; studies = 6; participants = 1,654; random-effects; Tau2 = 0.04; I2 = 92%; Analysis 4.3), although the lower CI of the pooled estimate effect just crossed the line of no effect. Supplementation with vitamin A had effect on the risk of stillbirths (average RR 1.01; 95% CI 0.96 to 1.07; studies = 3; participants = 115,223; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 4.4).
Subgroup Analysis
Due to insufficient data (this review required > or equal to three studies per subgroup of interest), subgroup analyses of the primary outcomes were not conducted based on maternal age, geographical region, sex of infant, baseline nutritional status in mothers (anemic vs. non-anemic; undernutrition vs. normal nutrition based on body mass index: BMI <18.5; low stature vs. normal stature), duration of intervention, time of recruitment (preconception vs. first trimester vs. second trimester vs. third trimester of pregnancy), daily vs. intermittent IFA supplementation and dose of intervention.
Comparison V: Zinc versus Placebo
Thirteen studies evaluated prenatal zinc supplementation compared to placebo (Ahmad et al., 2016; Aminisani et al., 2009; Castillo-Durán et al., 2001; Caulfield et al., 1999; Christian et al., 2003; Darling et al., 2017; Dijkhuizen et al., 2001; Hafeez et al., 2005; Merialdi et al., 2004; Osendarp et al., 2000; Prawirohartono et al., 2011; Saaka et al., 2009; Sorouri et al., 2016). Of these, 3 were conducted in Latin America and the Caribbean; 2 in Peru (Caulfield et al., 1999; Merialdi et al., 2004) and 1 in Chile (Castillo-Durán et al., 2001). Two were conducted in the Middle East & North Africa; both conducted in Iran (Aminisani et al., 2009; Sorouri et al., 2016). Four were conducted in South Asia, with 2 in Bangladesh (Ahmad et al., 2016; et al., Osendarp et al., 2000); 1 in Pakistan (Hafeez et al., 2005) and 1 in Nepal (Christian et al., 2003).Two were conducted in East Asia and Pacific (Indonesia) Dijkhuizen et al., 2001; Prawirohartono et al., 2011, and two in sub-Saharan Africa, in Ghana and Tanzania (Saaka et al., 2009 and Darling et al., 2017, respectively).
Three studies provided supplementation to the participants from enrolment until past delivery; Caulfield et al. (1999) and Merialdi et al. (2004) provided supplementation until 1 month postpartum; Ahmad et al., 2016 provided it until 6 months postpartum. Eight studies provided supplementation until delivery (Aminisani et al., 2009; Christian et al., 2003; Darling et al., 2017; Dijkhuizen et al., 2001; Hafeez et al., 2005; Osendarp et al., 2000; Saaka et al., 2009 and Sorouri et al., 2016). One study did not indicate until when supplementation was given (Castillo-Durán et al., 2001).
One study was excluded from meta-analysis because no common outcomes of interest were reported in this study (Prawirohartono et al., 2011) and thus data could not be pooled with the other studies. For a narrative synthesis of this study, see below under 'Other studies and comparisons not included in meta-analysis'. Twelve studies contributed data to the various meta-analyses for this comparison (Ahmad et al., 2016; Aminisani et al., 2009; Castillo-Durán et al., 2001; Caulfield et al., 1999; Christian et al., 2003; Darling et al., 2017; Dijkhuizen et al., 2001; Hafeez et al., 2005; Merialdi et al., 2004; Osendarp et al., 2000; Saaka et al., 2009; Sorouri et al., 2016).
In addition to any pre-specified, per-protocol subgroup analyses, an exploratory post-hoc analysis based on whether studies provided strictly zinc supplements vs. studies that provided zinc supplements along with additional micronutrients (e.g. iron folic acid as prenatal standard of care. Post-hoc analyses were conducted for low birthweight, preterm births, small-for-gestational age and maternal serum/plasma zinc concentration.
Primary outcomes
When compared to placebo, zinc supplementation probably made no difference to the risk of low birthweight infants (average RR 1.08; 95% CI 0.94 to 1.25; studies = 10; participants = 4,633; random-effects; Tau2 = 0.01; I2 = 13%; moderate-quality evidence; Analysis 5.1). In a post-hoc analysis, there was no significant difference in the pooled effect estimates for low birthweight observed between studies that provided zinc supplements with additional micronutrients (mainly iron and folic acid, as prenatal standard of care) (average RR 1.02; 95% CI 0.80 to 1.31; studies = 8; participants = 4,176; random-effects; Tau2 = 0.03; I2 = 28%; Analysis 5.1.1) and studies that that provided only zinc supplements compared to placebo (average RR 1.15; 95% CI 0.92 to 1.44; studies = 2; participants = 457; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 5.1.2) (test for subgroup differences: Chi2 = 0.49, P = 0.48).
Secondary outcomes
When compared to placebo, zinc supplementation in pregnancy had no effect on the risk of pre-eclampsia/eclampsia (average RR 1.01; 95% CI 0.53 to 1.93; studies = 3; participants = 1,226; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 5.3), nor on the risk of preterm births (average RR 0.97; 95% CI 0.80 to 1.17; studies = 11; participants = 5,017; random-effects, Tau2 = 0.02; I2 = 22%; Analysis 5.4). In a post-hoc analysis, no difference was observed between studies that provided zinc supplements along with additional micronutrients (mainly iron folic acid supplementation as prenatal standard of care) and studies that provided only zinc supplementation compared to placebo.
Zinc supplementation compared to placebo also had no effect on reducing the risk of having an infant born SGA (average RR 1.05; 95% CI 0.97 to 1.13; studies = 3; participants = 2,174; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 5.5). No significant differences in effect were observed between studies that provided additional micronutrients (average RR 1.08; 95% CI 0.98 to 1.20; studies = 2; participants = 1,764; Analysis 5.5.1) and studies that gave strictly zinc (average RR 1.00; 95% CI 0.90 to 1.12; studies = 1; participants = 410; Analysis 5.5.2) (test for subgroup differences: Chi2 = 0.99, P = 0.32).
Zinc supplementation may have slightly improved maternal serum zinc concentration (average MD 0.43 umol/L; 95% CI -0.04 to 0.89; studies = 5; participants = 1,202; random-effects; Tau2 = 0.16; I2 = 79%; Analysis 5.6), although the lower confidence interval just crossed the line of no effect. Studies that provided strictly zinc supplements did not show significant differences in maternal serum zinc concentration (average MD 0.86 umol/L; 95% CI 0.67 to 1.05; studies = 2; participants = 485) compared to studies that provided additional micronutrients (average MD 0.01 umol/L; 95% CI -0.70 to 0.72; studies = 3; participants = 717) (test for subgroup differences: Chi2 = 5.18, P = 0.02).
Subgroup Analysis
Subgroup analyses were conducted for low birthweight based on geographical region. Please see below for results under heading 'Subgroup Analysis II: Zinc supplementation versus Placebo'.
Comparison VI: Iron versus Placebo
Thirteen studies assessed iron supplementation (Christian et al., 2003; Etheredge et al., 2015; Falahi 2010; Liu et al., 2013; Menendez et al., 1995; Ouladsahebmadarek et al., 2011; Preziosi et al., 1997; Tanumihardjo et al., 2002; Zeng et al., 2008; Zhao et al., 2015; Ziaei et al., 2007; Ziaei et al., 2008 and Korkmaz et al., 2014). Of these, 4 studies were conducted in the Middle East and North Africa, specifically in Iran (Falahi, 2010; Ouladsahebmadarek et al., 2011; Ziaei et al., 2007; Ziaei et al., 2008), while 3 studies were conducted in sub-Saharan Africa (Etheredge et al., 2015; Menendez et al., 1995; Preziosi et al., 1997), representing Tanzania, The Gambia and Niger, respectively. Four studies were conducted in East Asia and Pacific; 3 were in China and 1 was in Indonesia (Liu et al., 2013; Tanumihardjo et al., 2002; Zeng et al., 2008; Zhao et al., 2015). One study was conducted in Nepal, in the South Asia region (Christian et al., 2003).
One study was excluded from meta-analysis because no common outcomes of interest were reported (Korkmaz et al., 2014), and thus data could not be pooled with the other studies. For a narrative synthesis of this study, see below under 'Other studies and comparisons not included in meta-analysis'. Of these, 12 studies contributed data to this comparison (Christian et al., 2003; Etheredge et al., 2015; Falahi, 2010; Liu et al., 2013; Menendez et al., 1995; Ouladsahebmadarek et al. 2011; Preziosi et al., 1997; Tanumihardjo et al. 2002; Zeng et al., 2008; Zhao et al. 2015; Ziaei et al., 2007; Ziaei et al., 2008).
The majority of included studies utilized supplements containing 60 mg of elemental iron (Etheredge et al., 2015; Falahi, 2010; Menendez et al., 1995; Tanumihardjo et al. 2002; Zeng et al., 2008; Zhao et al. 2015). Two studies gave participants 50 mg of iron (Ziaei et al., 2007; Ziaei et al., 2008), 3 studies gave participants 30 mg of iron (Christian et al., 2003; Liu et al., 2013; Ouladsahebmadarek et al. 2011), and 1 study gave 100 mg of iron (Preziosi et al., 1997).
In Tanumihardjo 2002 participants received 8.4 umol of vitamin A daily and in Menendez et al. (1995) and Etheredge et al. (2015) participants received 5 mg of folic acid daily. All women received intermittent preventative treatment for malaria in Etheredge et al. (2015).
In terms of duration of the intervention, the majority of included studies gave supplementation from enrolment to delivery (Christian et al., 2003; Etheredge et al., 2015; Menendez et al., 1995; Preziosi et al., 1997; Zeng et al., 2008; Zhao et al. 2015; Ziaei et al., 2007). Liu et al. (2013) gave supplementation from the first prenatal visit to delivery, Ouladsahebmadarek et al. (2011) gave supplementation from 13 weeks of gestation until delivery, and Tanumihardjo et al. (2002) gave supplementation for 8 weeks following enrolment. One study (Ziaei et al., 2008) gave iron supplementation from enrolment to 6 weeks postpartum.
In addition to any pre-specified, per-protocol subgroup analyses, an exploratory post-hoc analysis based whether studies provided strictly iron supplementation compared to placebo vs. studies that provided iron supplements along with additional micronutrients (typically folic acid as prenatal standard of care). Post hoc analyses were conducted for maternal anaemia, maternal serum/plasma hemoglobin, maternal serum/plasma ferritin, and maternal iron deficiency.
Primary Outcomes
When compared to placebo, iron supplementation in pregnancy improved maternal anaemia (average RR 0.53; 95% CI 0.43, to 0.65; studies = 6; participants = 15,737; random-effects; Tau2 = 0.06; I2 = 84%; high quality evidence; Analysis 6.1). For maternal anaemia, we conducted a post-hoc analysis of studies that gave strictly iron supplements versus placebo compared to studies where iron supplementation was combined with other supplements (most commonly folic acid as prenatal standard of care or vitamin A). There were no significant difference between subgroups, though only one study contributed to the analysis of strictly iron versus placebo (Analysis 6.1.1 and 6.1.2) (test for subgroup differences: Chi2 = 0.44, P = 0.51).
When compared to placebo, iron supplementation demonstrated a moderate 12% reduction in the risk of low birthweight (average RR 0.88; 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; random-effects; Tau2 = 0.00; I2 = 0%; high quality evidence; Analysis 6.3) but no difference in perinatal mortality (average RR 0.88; 95% CI 0.71 to 1.08; studies =4; participants = 17,464; random-effects; Tau2 = 0.00; I2 = 0%; high quality evidence; Analysis 6.4).
Secondary outcomes
Iron supplementation, when compared to placebo, made no difference in reducing the risk of pre-eclampsia/eclampsia during pregnancy (average RR 1.55; 95% CI 0.91 to 2.63; studies = 3; participants = 2,773; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 6.5). However, it did improve maternal hemoglobin concentration (average MD 7.80 g/L; 95% CI 4.08 to 11.52; studies = 11; participants = 25,916; random-effects; Tau2 = 36.63; I2 = 99%; Analysis 6.6), and it improved maternal ferritin concentration (average MD 24.14 ug/L; 95% CI 10.83 to 37.45; studies = 9; participants = 5,045; random-effects; Tau2 = 370.94; I2 = 100%; Analysis 6.7).
There were no significant differences between subgroups for maternal hemoglobin concentration (test for subgroup differences: Chi2 = 0.03, P = 0.85; Analysis 6.6.1 and 6.6.2). However, post-hoc analysis showed that mothers who took strictly iron versus placebo had significantly lower serum ferritin (average MD of 7.09 ug/L; 95% CI 4.45 to 9.72; studies = 3; participants = 365; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 6.7.2) compared to mothers who took iron supplements plus additional micronutrients (average MD 32.87 ug/L; 95% CI 15.39 to 50.34; studies = 6; participants = 4,680; random-effects; Tau2 = 526.07; I2 = 100%; Analysis 6.7.1) (test for subgroup differences: Chi2 = 8.17, P = 0.004).
There was no impact of iron supplementation on maternal transferrin receptor concentration (average MD -0.16; 95% CI -0.96 to 0.65; studies = 3; participants = 2,431; random-effects; Tau2 = 0.46; I2 = 99%; Analysis 6.8); however, iron supplementation improved iron deficiency when compared to placebo (average RR 0.54; 95% CI 0.40 to 0.74; studies = 4; participants = 2,522; random-effects; Tau2 = 0.06; I2 = 82%; Analysis 6.9). In a post-hoc analysis, the effect was significantly larger in studies that strictly gave iron (average RR of 0.34; 95% CI 0.23 to 0.51; studies = 2; participants = 2,177; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 4.9.2) when compared to studies that gave other supplements along with iron (average RR 0.67; 95% CI 0.54 to 0.83; studies = 2; participants = 345; random-effects; Tau2 = 0.02; I2 = 78%; Analysis 4.9.1) (test for subgroup differences: Chi2 = 8.32, P = 0.004).
When compared to placebo, iron supplementation did not have an effect on neonatal mortality (average RR 0.85; 95% CI 0.55 to 1.31; studies = 3; participants = 15,524; random-effects; Tau2 = 0.07; I2 = 47%; Analysis 6.10), nor on the risk of preterm births (average RR 0.94; 95% CI 0.63 to 1.41; studies = 6; participants = 18,419; random-effects; Tau2 = 0.21; I2 = 96%; Analysis 6.11). Iron supplementation also did not improve the risk of having babies considered SGA (average RR 1.04; 95% CI 0.87 to 1.24; studies = 4; participants = 6,549; random-effects; Tau2 = 0.02; I2 = 71%; Analysis 6.12), nor did it improve the risk of infant mortality (average RR 1.10; 95% CI 0.84 to 1.45; studies = 3; participants = 14,748; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 6.13).
Subgroup Analysis
Subgroup analyses were conducted for maternal anaemia based on geographical region and dose of iron. Please see below for results under heading 'Subgroup Analysis III: Iron supplementation versus Placebo'.
Comparison VII: Vitamin D versus Placebo
Eleven studies contributed data to this comparison (Asemi et al., 2013; Hossain et al., 2012; Khan et al., 2016; Mohammad-Alizadeh-Charandabi et al., 2015; Naghshineh & Sheikhaliyan, 2016; Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG); Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Vaziri et al. 2016). Approximately half of the studies (n = 5) were conducted in the Middle East and North Africa region, specifically in Iran (Asemi et al., 2013; Mohammad-Alizadeh-Charandabi et al., 2015; Naghshineh & Sheikhaliyan, 2016; Sabet et al., 2012; Vaziri et al. 2016). The other half of the studies (n = 6) were conducted in the South Asia region; 2 were conducted in Bangladesh (Roth et al., 2013 (AViDD); Roth et al., 2018 (MDIG)), 2 in Pakistan (Hossain et al., 2012; Khan et al., 2016) and 2 in India (Sablok et al., 2015; Sahu et al., 2009). Six studies indicated that they gave participants supplementation from enrolment to delivery; enrolment was at various gestational ages, ranging from 12 weeks to 28 weeks of gestation (Hossain et al., 2012; Khan et al., 2016; Naghshineh & Sheikhaliyan, 2016; Roth et al., 2018 (MDIG); Sabet et al., 2012; Vaziri et al. 2016). Three studies were specific in their duration of intervention: Asemi et al. (2013) indicated that supplementation was given for nine weeks after enrolment; Mohammad-Alizadeh-Charandabi et al., 2015 stated supplementation was given for 60 days after enrolment and Roth et al., 2013 (AViDD) indicated that on average, women received supplementation for approximately 10 weeks after enrolment. Sablok et al. (2015) did not indicate the end of the supplementation period.
In addition to any pre-specified, per-protocol subgroup analyses, an exploratory post-hoc analysis based whether studies provided strictly vitamin D supplementation compared to placebo vs. studies that provided vitamin D along with additional micronutrients (typically iron and folic acid as prenatal standard of care). Post hoc analyses were conducted for preterm births, SGA, maternal serum/plasma vitamin D, and mode of delivery - caesarean section.
Primary outcomes
There were no primary outcomes that were measured by studies included in this comparison.
Secondary outcomes
Compared to placebo, vitamin D supplementation in pregnancy may have reduced the risk of preterm births (average RR 0.64; 95% CI 0.40 to 1.04; studies = 7; participants = 1,262; random-effects; Tau2 = 0.17; I2 = 45%; Analysis 7.1), although the upper limit of the CI just crosses 1. In a post-hoc analysis, mothers who took strictly vitamin D had a significantly reduced risk of preterm births (average RR 0.33; 95% CI 0.17 to 0.62; studies = 2; participants = 303; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 7.1.2) compared to mothers who took vitamin D plus additional micronutrients, typically iron-folic acid as the prenatal standard of care (average RR 0.94; 95% CI 0.64 to 1.36; studies = 5, participants = 959; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 7.1.1) (test for subgroup differences: Chi2 = 7.71, P = 0.006).
Vitamin D supplementation showed no effect on the risk of having SGA infants overall (average RR 0.93; 95% CI 0.57 to 1.53; studies = 3; participants = 851; random-effects; Tau2 = 0.12; I2 = 63%; Analysis 7.2). Post-hoc analysis indicated no significant differences in births considered SGA between studies that strictly gave vitamin D supplementation and studies that provided vitamin D plus additional micronutrients (test for subgroup differences: Chi2 = 5.32, P = 0.02).
Vitamin D supplementation, when compared with placebo, improved maternal serum vitamin D concentrations (average MD 44.70 nmol/L; 95% CI 21.94 to 67.45; studies = 9; participants = 1,092; random-effects, Tau2 = 1149.40; I2 = 99%; Analysis 7.3). No significant differences in maternal serum vitamin D concentration were noted when comparing studies that provided strictly vitamin D and studies that provided additional micronutrients (test for subgroup differences: Chi2 = 0.16, P = 0.69).
Vitamin D supplementation demonstrated no effect on maternal serum calcium concentrations (average MD -0.06 mg/dL; 95% CI -0.21 to 0.09; studies = 5; participants = 759; random-effects; Tau2 = 0.02; I2 = 84%; Analysis 7.4). Lastly, vitamin D supplementation, compared to placebo, had no effect on reducing the risk of caesarean section as a mode of delivery (average RR 1.05; 95% CI 0.94 to 1.18; studies = 5; participants = 1,063; random effects; Tau2 = 0.00; I2 = 0%; Analysis 7.5). Our post-hoc analysis revealed no significant differences between groups for caesarean sections (test for subgroup differences: Chi2 = 0.26, P = 0.61).
Subgroup Analysis
Due to insufficient data (this review required more than or equal to three studies per subgroup of interest), subgroup analyses of the primary outcomes were not conducted based on maternal age, geographical region, sex of infant, baseline nutritional status in mothers (anemic vs. non-anemic; undernutrition vs. normal nutrition based on body mass index: BMI <18.5; low stature vs. normal stature), duration of intervention, time of recruitment (preconception vs. first trimester vs. second trimester vs. third trimester of pregnancy), daily vs. intermittent IFA supplementation and dose of intervention.
Comparison VIII: Calcium vs. Placebo
Five studies assessed calcium supplementation versus placebo (Belizán et al.,1997; Jarjou et al., 2006; Kumar et al., 2009; López-Jaramillo et al., 1997; Villar et al., 2006). One study was excluded from meta-analysis because no common outcomes of interest were reported (Jarjou et al., 2006). For a narrative synthesis of this study, see below under 'Other studies and comparisons not included in meta-analysis' section. Thus, 4 studies contributed data to this comparison (Belizán et al., 1997; Kumar et al., 2009; López-Jaramillo et al., 1997; Villar et al., 2006). Two studies were conducted in Latin America and the Caribbean (Belizán et al., 1997; López-Jaramillo et al., 1997) and 1 study was conducted in South Asia (Kumar et al., (2009). Villar et al. (2006) is a multi-country study that was conducted in Peru, South Africa, Vietnam and India.
In addition to any pre-specified, per-protocol subgroup analyses, an exploratory post-hoc analysis based whether studies provided strictly calcium supplementation compared to placebo vs. studies that provided calcium along with additional micronutrients (typically iron and folic acid as prenatal standard of care). Post-hoc analyses were conducted for low birthweight, pre-eclampsia/eclampsia, stillbirths, preterm births, and mode of delivery - Caesarean section.
Primary Outcomes
Compared to placebo, calcium supplementation in pregnancy did not improve the risk of low birthweight infants (average RR 0.99; 95% CI 0.95 to 1.04; studies = 3; participants = 9,498; random-effects; Tau2 = 0.00; I2 = 0%; high quality evidence; Analysis 8.1). No significant difference in effect was noted between studies that provided strictly calcium and those that provided additional micronutrients (test for subgroup differences: Chi2 = 0.12, P = 0.73).
Secondary outcomes
Calcium supplementation, when compared to placebo, may have improved the risk of pre-eclampsia/eclampsia (average RR 0.45; 95% CI 0.19 to 1.06; studies = 4; participants = 9,616; random-effects; Tau2 = 0.52; I2 = 80%; Analysis 8.2), although the upper CI for the pooled effect estimate just crossed the line of no effect. In a post-hoc analysis, compared to studies that provided additional nutrients along with the calcium supplement (mainly iron and folic acid as prenatal standard of care), women who received strictly calcium had a much greater reduction in the risk of pre-eclampsia/eclampsia (average RR 0.30; 95% CI 0.17 to 0.52; studies = 3; participants = 1,304; random-effects, Tau2 = 0.00; I2 = 0%; Analysis 8.2.2 compared to average RR 0.92; 95% CI 0.75 to 1.13; study = 1; participants = 8,312; random-effects; Analysis 8.2.1), though only one study contributed to Analysis 8.2.1. Effects between subgroups were significantly different (test for subgroup differences: Chi2 = 14.17, P = 0.0002).
Calcium supplementation probably did not reduce the risk of stillbirths (average RR 0.87; 95% CI 0.70 to 1.07; studies = 4; participants = 10,287; random-effects; Tau2 = 0.00; I2 = 0%; Analysis 8.3). A post-hoc analysis revealed no significant difference in stillbirths when comparing mothers who took calcium plus additional nutrients (average RR 0.86; 95% CI 0.69 to 1.07; studies = 1; participants = 8,378; Analysis 8.2.1) and those who took strictly calcium (average RR 0.97; 95% CI 0.44 to 2.15; studies = 3; participants = 1,909; Analysis 8.2.2) (test for subgroup differences: Chi2 = 0.09, P = 0.77).
Calcium supplementation probably did not reduce the risk of preterm births (average RR 0.84; 95% CI 0.65 to 1.08; studies = 4; participants = 9,933; random-effects; Tau2 = 0.02; I2 = 40%; Analysis 8.4), and there was no significant difference in effect between sub-groups when conducting our post-hoc analysis (test for subgroup differences: Chi2 = 0.77, P = 0.38).
Lastly, calcium supplementation versus placebo had no effect on reducing the risk of Caesarean section as a mode of delivery (average RR 0.99, 95% CI 0.84 to 1.15; studies = 3; participants = 10,000; random-effects; Tau2 = 0.01; I2 = 26%; Analysis 8.5). In a post-hoc analysis, no significant differences in Caesarean sections were observed between studies that gave mothers strictly calcium and studies that provided additional nutrients alongside calcium (test for subgroup differences: Chi2 = 0.50, P = 0.48).
Subgroup Analyses
Due to insufficient data (this review required > or equal to three studies per subgroup of interest), subgroup analyses of the primary outcomes were not conducted based on maternal age, geographical region, sex of infant, baseline nutritional status in mothers (anemic vs. non-anemic; undernutrition vs. normal nutrition based on body mass index: BMI <18.5; low stature vs. normal stature), duration of intervention, time of recruitment (preconception vs. first trimester vs. second trimester vs. third trimester of pregnancy), daily vs. intermittent IFA supplementation and dose of intervention.
Subgroup Analysis I: MMN supplementation versus IFA
For studies comparing MMN supplementation versus IFA supplementation, we conducted subgroup analyses based on MMN formulation, duration of intervention, dose of iron in the intervention, and geographical region.
For maternal mortality, there were no significant differences between groups when comparing UNIMMAP plus adapted UNIMMAP to non-UNIMMAP formulations of supplements (P for subgroup differences = 0.87; Analysis 9.1). In addition, there were no significant differences based on geographical region (P for subgroup differences = 0.61; Analysis 9.2), duration of intervention (P for subgroup differences = 1.00; Analysis 9.3), or dose of iron (P for subgroup differences = 1.00; Analysis 9.4).
Similarly, for the outcome maternal anaemia, there were no significant differences between groups when considering supplement formulation (P for subgroup differences = 0.65; Analysis 9.5), geographical region (P for subgroup differences = 0.51; Analysis 9.6), or dose of iron (P for subgroup differences = 0.83; Analysis 9.7).
For perinatal mortality, we found no significant differences between groups when examining MMN formulation (P for subgroup differences = 0.88; Analysis 9.8), geographical region (P for subgroup differences = 0.68; Analysis 9.9), or dose of iron (P for subgroup differences = 0.68; Analysis 9.10).
No significant difference was observed between studies that used the UNIMMAP formulation (average RR 0.74; 95% CI 0.61 to 0.90; studies = 11), compared to studies that used adapted UNIMMAP (average RR 0.88; 95% CI 0.85 to 0.91; studies = 3) and non-UNIMMAP supplements (average RR 0.92; 95% CI 0.81 to 1.05; studies = 12; P for subgroup differences = 0.18; Analysis 9.11).
We observed a greater reduction in risk of low birthweight in women in studies conducted in Western Pacific (average RR 0.46; 95% CI 0.38 to 0.56; studies = 4), compared to studies conducted South Asia, Americas and Eastern Mediterranean regions (P for subgroup differences <0.00001; Analysis 9.12). Villar et al. (2006) was excluded from this subgroup analysis because it was a multi-country study and the data was not disaggregated by country.
No significant difference in the reduction of low birthweight risk was observed between studies that utilized <60 mg of iron in their MMN supplements (average RR 0.79; 95% CI 0.69 to 0.89; studies = 18) and studies that utilized 60 mg of iron in their supplements (average RR 0.96; 95% CI 0.83 to 1.12; studies = 7; P for subgroup differences = 0.05; Analysis 9.13). Villar et al. (2006) was excluded from this subgroup analysis because the dosage of iron was not indicated in the methods.
Subgroup Analysis II: Zinc supplementation versus Placebo
For studies comparing zinc supplementation versus placebo, we conducted a subgroup analysis for the outcome low birthweight based on geographical region. We found no significant differences by region (P for subgroup differences = 0.39; Analysis 11.2).
Subgroup Analysis II: Iron supplementation versus Placebo
For studies examining iron supplementation versus placebo, we conducted subgroup analysis for the outcome maternal anaemia based on geographical region and dose of iron in the intervention supplement. For both region (P for subgroup differences = 0.49; Analysis 10.1) and dose (P for subgroup differences = 0.69; Analysis 10.2), we found no significant differences by subgroup.
Descriptive Summary of Additional Studies (not included in meta-analyses):
Calcium plus vitamin D versus placebo supplementation
Diogenes et al. (2013) evaluated prenatal supplementation of calcium with vitamin D compared to placebo. Diogenes et al. (2013) was not included in any comparison for analysis in this review given that there was insufficient number of studies to conduct pooled analysis for calcium with vitamin D prenatal supplementation. The primary outcomes reported by Diogenes et al. (2013) were bone measurements in adolescent mothers at 5 and 20 weeks postpartum, including total bone mineral content (BMC) and total bone mineral density (BMD), and serum vitamin D concentration measured at baseline and postpartum. Serum vitamin D concentration levels in mothers who received prenatal supplementation were higher than those in mothers of the placebo group at 5 weeks and 20 weeks postpartum. In terms of bone measurements, the authors postulated that there may be an effect of increased calcium intake during pregnancy on reduced postpartum bone loss in adolescent mothers.
Taherian et al. (2002) also evaluated calcium plus vitamin D vs. placebo supplementation; however, it could not be pooled with the other two studies (Diogenes et al., 2013 and Asemi et al., 2016) given that they shared no common reported outcomes. The primary outcome was the prevalence of preeclampsia, whereby significant differences were observed in the frequency reduction of preeclampsia in women receiving only low-dose aspirin daily or only calcium-vitamin D supplements daily compared to placebo. No significant difference in the reduction of preeclampsia was observed between the aspirin and calcium-vitamin D groups.
Note: Asemi et al. (2016) was included in the MMN vs. IFA comparison; however could not be pooled with Diogenes et al. (2013) or Taherian et al. (2002) to form a comparison group for calcium plus vitamin D supplementation versus placebo.
Iodine versus placebo
Gowachirapant et al. (2017) was the sole study that evaluated this type of supplementation. Participants were provided iodine or placebo tablets; there was no indication of provision of iron folic acid or multiple micronutrient supplements as additional prenatal supplementation. Primary outcomes reported were developmental outcomes in children, specifically verbal and performance IQ scores on WPPSI-III and the global executive composite score from BRIEF-P in children aged 5 to 6 years. Secondary outcomes included child's auditory performance, weight and height, maternal urinary iodine concentration, maternal thryoid stimulating hormone (TSH) concentration, maternal total thyroxine (T4) concentration. There were no significant differences between the iodine and placebo groups in terms of any child development outcomes. Maternal urinary iodine concentration was higher in the iodine group compared to the placebo group during pregnancy, but not at 6 weeks postpartum. In terms of maternal TSH and T4 concentrations, there were no significant differences between the intervention and control groups reported in by the authors.
LNS vs. placebo
Hambidge et al. (2019) was the only study that reported the effects of LNS vs. placebo; there was no report of iron-folic acid or other multiple micronutrient given to both intervention arms and the control arm. The first intervention arm received the LNS supplement from the time of random assignment until delivery (Arm 1) while the second intervention arm received the LNS supplement during trimester 2 or 3 until delivery (Arm 2). Placebo group was Arm 3. The primary outcome of this study was newborn length-for-age z score (LAZ). Secondary outcomes included weight, head circumference (HC), BMI, and WAZ, HC-for-age (HCAZ) and BMI for age (BMIAZ) z scores, prevalence of low birthweight, small-for-gestational age and preterm infants. For all sites, there was no significant difference in LAZ between the two intervention arms (Arm 1 and Arm 2); however, small positive effects in LAZ were observed in Arm 1 compared to Arm 3 for the sites in Guatemala, Pakistan, India and Democratic Republic of Congo. Similar effects were noticed comparing Arms 2 and 3 for combined sites and Pakistan. Effect sizes for WAZ were same or lower than LAZ but followed similar patterns in which Arms 1 and 2 were greater than Arm 3.
Calcium vs. placebo
Jarjou et al. (2006) was excluded from meta-analysis because the study did not report outcomes reported by other studies in the same comparison. Outcomes reported by Jarjou et al. (2006) include: maternal vitamin D serum concentration, bone mineral accretion in infants, birthweight (grams) and other growth measures, blood pressure, urine biomarkers (urinary calcium, phosphours and titratable acid) and calcium concentration in breast milk. No significant differences were noted by the authors between the intervention and control groups in terms of breastmilk concentrations of calcium, infant birth weight, infant growth or bone mineral status during the first year of life.
Iron vs. placebo
Korkmaz et al. (2014) was excluded from the iron vs. placebo comparison because it reported no common outcomes reported by other studies that evaluated the same type of supplementation. Outcomes reported by the study's authors include: maternal weight and weight gain during pregnancy, serum albumin levels, and oxidative stress markers such as y-glutamyl transferase (GGT) levels. Oxidative stress markers, mainly GGT serum levels, were significantly higher in the iron intervention group compared to placebo (P < 0.001).
Vitamin A vs. placebo and Zinc vs. placebo
Prawirohartono et al. (2011): Although vitamin A vs. placebo and zinc vs. placebo are comparisons that have been meta-analysed in this review, Prawirohartono et al. (2011) reported outcomes that were not common with reported outcomes in the other studies. The primary outcomes were postnatal child growth in terms of weight-for-age (WAZ), height-for-age (HAZ), and weight-for-height (WHZ) scores. The study found no effect on WAZ, HAZ and WHZ of prenatal supplementation of vitamin A, a combination of vitamin A and zinc, or zinc alone, compared to placebo. Other outcomes included prevalence of low birthweight infants, small-for-gestational age infants, and preterm births; no significant differences were noted between the vitamin A supplementation group, the zinc only supplementation group, and the placebo group for these outcomes.
Vitamin B12 vs. placebo
Duggan et al. (2014) was the only study that reported the effects of vitamin B12 supplementation vs. placebo. This study primarily measured vitamin B12 concentrations (pmol/L) in maternal plasma and breast milk. Secondary outcomes included mode of delivery - Caesarean section, prevalence of low birthweight infants, mean birth weight and incidence of delivering an infant with intrauterine growth retardation (IUGR). Findings showed that women supplemented with vitamin B12 had higher vitamin B12 plasma concentrations, as well as, higher concentrations of vitamin B12 in their breastmilk. More mothers in the vitamin B12 arm underwent elective Caesarean section (18%) than mothers in the placebo group (10%) (P = 0.06). The frequency of LBW infants was not significantly different between the two groups. As well, mean birth weight did not differ significantly between the intervention and control arms. 25% of mothers in the vitamin B12 group delivered an infant with IUGR, compared to 34% of mothers in the placebo group (P = 0.11).
Sensitivity Analyses
A sensitivity analysis was conducted to examine if any of the meta-analyses were especially affected by the risk of bias assessments. Included studies that were assesed with a high risk of bias for one or more domain or studies that were assessed as unclear risk in two or more domains were removed from the meta-analyses to see if this had any effect on the effect estimates of the outcomes. Diogenes et al. (2013), Duggan et al. (2014); Hambidge et al. (2019), Gowachirapant et al. (2017), Prawirohartono et al. (2011) and Taherian et al. (2002) were not included in any meta-analyses, and thus sensitivity analysis of these studies rendered no effects on any outcomes.
For Comparison I: IFA vs. FA supplementation, two studies (Menendez et al., 1995; Zhao et al., 2015) were excluded; however, this exclusion did not significantly affect the findings for the outcomes.
For Comparison II: MMN vs. IFA supplementation, thirteen studies were excluded (Caulfield et al., 1999; Choudhury et al., 2012; Dijkhuizen et al., 2001; Friis et al., 2004; Hanieh et al., 2013; Huy et al., 2009; Kæstel et al., 2005; Moore et al., 2012; Muslimatun et al., 2001; Osrin et al., 2005; Ramakrishnan et al., 2003; Sunawang et al., 2009; Tofail et al., 2008). With the exclusion of Caulfield et al. (1999), Hanieh et al. (2013), Ramakrishnan et al. (2003), and Tofail et al. (2008), maternal serum/plasma folate concentration showed greater benefit with iron-folic acid supplementation compared to MMN (average RR -3.60; 95% CI -5.62 to -1.58), although this sensitivity analysis includes only one study. With the exclusion of Friis et al. (2004), Hanieh et al. (2013), Kæstel et al. (2005), Osrin et al. (2005), Ramakrishnan et al. (2003), Sunawang et al. (2009), Tofail et al. (2008) and Zagré et al. (2007), there is minimal change to the effect of MMN supplementation on the risk reduction of stillbirths, although the upper limit of the confidence interval just crossed the line of no effect (average RR 0.95; 95% CI 0.96 to 1.01; compared to the original analysis, average RR 0.91; 95% CI 0.86 to 0.98). Similarly, with the removal of Friis et al. (2004), Kæstel et al. (2005), Moore et al. (2012), Osrin et al. (2005), Ramakrishnan et al. (2003), Sunawang et al. (2009), Tofail et al. (2008) and Zagré et al. (2007), there is minimal change to the effect of MMN supplementation on the reduced risk of SGA infants, although the upper limit of the confidence interval just crossed the line of no effect (average RR 0.95; 95% CI 0.96 to 1.01; compared to the original analysis, average RR 0.93; 95% CI 0.96 to 1.01). With the exclusion of Huy et al. (2009) and Osrin et al. (2005), the average risk ratio for underweight status in children changes from average RR 0.95 (95% CI 0.84 to 1.07) to average RR 1.01 (95% CI 0.97 to 1.06). Although the confidence intervals for the effect estimates both before and after the sensitivity analysis crosses the line of no effect, exclusion of these studies seemed to show no effect of MMN supplementation on child underweight status. Removal of Hanieh et al. (2013) seemed to show no effect of MMN supplementation for child development outcome: verbal comprehension and language (standard mean difference -0.01; 95% CI -0.19 to 0.16).
For Comparison III: LNS vs. MMN supplementation, two studies (Huybregts et al., 2009; Moore et al., 2012) were excluded. With the removal of Huybregts et al., 2009, a 75% reduction in the risk of stillbirths was reported (average RR 0.25; 95% CI 0.08 to 0.78) by LNS supplementation compared to MMN. The original analysis showed no effect of LNS supplements on the risk reduction of stillbirths (average RR 0.47; 95% CI 0.12 to 1.81).
For Comparison IV: vitamin A vs. placebo, six studies were excluded (Darling et al., 2017; Kirkwood et al., 2010; Muslimatun et al., 2001; Semba et al., 2001; Tanumihardjo et al., 2002; West et al., 2011). With the removal of Kirkwood et al. (2010) and West et al. (2011), a greater effect of vitamin A supplementation on maternal mortality was observed (average RR 0.62, 9% CI 0.37 to 1.04) although the confidence interval crosses one. The original analysis showed no observed effect of vitamin A on maternal mortality (average RR 0.90; 95% CI 0.68 to 1.18). Similarly, with the removal of Kirkwood et al. (2010), Muslimatun et al. (2001) Semba et al. (2001) Tanumihardjo et al. (2002) and West et al. (2011), maternal serum/plasma retinol concentration showed greater improvement with vitamin A supplementation (average MD 0.38 umol/L; 95% CI 0.14 to 0.62), although this analysis comprised of only one study, compared to the original analysis (average MD 0.13 umol/L; 95% CI -0.03 to 0.30).
For Comparison V: zinc vs. placebo, exclusion of six studies (Ahmad et al., 2016; Castillo-Durán et al., 2001; Caulfield et al., 1999; Darling et al., 2017; Dijkhuizen et al., 2001; and Osendarp et al., 2000), showed no change in the findings for the outcomes.
For Comparison VI: iron vs. placebo, exclusion of six studies (Falahi 2010; Menendez et al., 1995; Ouladsahebmadarek et al., 2011; Tanumihardjo et al., 2002; Preziosi et al., 1997 and Zhao et al., 2015) showed no change in the findings for the outcomes.
For Comparison VII: vitamin D vs. placebo, exclusion of six studies (Hossain et al., 2012; Mohammad-Alizadeh-Charandabi et al., 2015; Sabet et al., 2012; Sablok et al., 2015; Sahu et al., 2009; Vaziri et al., 2016) showed no change in the findings for the outcomes.
For Comparison VIII: calcium vs. placebo, there were no studies to remove in the sensitivity analysis.
Post-Hoc Analysis based on declarations of conflict of interest
A post-hoc analysis was conducted to examine if any effect estimates were influenced by studies where a conflict of interest was declared. Five studies reported a conflict of interest (Ashorn et al., 2015; Dewey et al., 2009; Osrin et al., 2005; West et al., 2014; Zeng et al., 2008), and exclusion of these studies did not significant affect the findings for the reported outcomes.
DISCUSSION
Summary of main results
We identified 314 included papers across 72 studies (involving 451,723 women) as eligible for inclusion in this review; however, 64 studies (involving 439,649 women) contributed data to the analyses. This review summarizes the current evidence on the effect of several micronutrient and vitamin supplementations during pregnancy on fetal, infant, maternal and child outcomes. Of eligible studies, seven assessed IFA versus folic acid supplementation; thirty-four studies assessed MMN supplementation versus IFA supplementation or placebo; four studies assessed LNS supplementation versus MMN supplementation or placebo; thirteen studies assessed iron supplementation versus no iron or placebo; thirteen studies assessed zinc supplementation versus no zinc or placebo; nine studies assessed vitamin A supplementation versus no vitamin A or placebo; eleven studies assessed vitamin D supplementation versus no vitamin D or placebo; and six studies assessed calcium supplementation versus no calcium or placebo.
Supplementation with IFA compared to folic acid showed a large and significant effect on the risk of maternal anaemia in the third trimester of pregnancy, reducing the risk by 48% (average RR 0.52, 95% CI 0.41 to 0.66; studies = 5; participants = 15,540; moderate-quality evidence); and a smaller but significant, 12% reduction in the risk of low birthweight babies (average RR 0.88, 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; high-quality evidence).
MMN supplementation compared to iron with or without folic acid supplementation probably made no difference on maternal mortality (average RR 1.04 95% CI 0.71 to 1.51; studies = 7; participants = 75,051; moderate quality of evidence) and demonstrated no significant effect on perinatal mortality (average RR 1.00, 95% CI 0.90 to 1.11; studies = 16; participants = 92,769; high-quality evidence). MMN supplementation also did not have an important effect on maternal anaemia (average RR 0.95, 95% CI 0.82 to 1.10; studies = 16; participants = 23,556; high quality evidence) and had little effect on iron deficiency anaemia as well (average RR 1.12, 95% CI 0.62 to 2.02; studies = 4; participants = 1595; low-quality evidence). However, MMN supplementation in pregnancy, when compared to iron with or without folic acid, demonstrated a significant effect, a 15% reduction, on the risk of having a low birthweight baby (average RR 0.85, 95% CI 0.77 to 0.93; studies = 28; participants = 79,972). MMN supplementation also demonstrated a small and significant effect on the risk of stillbirths (average RR 0.91, 95% CI 0.86 to 0.98; studies = 22; participants = 96,772), and a smaller but significant effect on the risk of SGA infants (average RR 0.93; 95% CI 0.88 to 0.98; studies = 19; participants = 52,965). The risk of preterm births may have improved with MMN supplementation (average RR 0.96; 95% CI 0.91 to 1.01; studies = 29; participants = 99,855), although the confidence interval just crossed the line of no effect.
Regarding child outcomes, children of mothers who had been supplemented with MMN showed a significant effect on the risk of diarrhea in children (average RR 0.84; 95% CI 0.76 to 0.92; studies = 4; participants = 2,556) and a positive effect on executive function (standard MD 0.09; 95% CI 0.01 to 0.17; studies = 3; participants = 2,511).
Our subgroup analyses that compared studies based on MMN formulation (UNIMMAP vs. Adapted UNIMMAP vs. non-UNIMMAP formulations) showed that MMN supplementation had a greater effect in reducing the risk of low birthweight among women in the subgroup of studies that used the UNIMMAP formulation (average RR 0.74; 95% CI 0.61 to 0.90; studies = 11), compared to studies that used adapted UNIMMAP (average RR 0.88; 95% CI 0.85 to 0.91; studies = 3) and non-UNIMMAP supplements (average RR 0.92; 95% CI 0.81 to 1.05; studies = 12; P for subgroup differences = 0.18). We also conducted a post-hoc exploratory analysis based on the number of components provided in the MMN supplement, specifically comparing studies that used MMN supplements containing >4 micronutrients to studies whose MMN formulation contained <or equal to 4 micronutrients. MMN supplements with more than 4 components showed a large significant effect on reducing the risk of having a low birthweight baby (average RR 0.79; 95% CI 0.71 to 0.88; studies = 19; participants = 68,138); whereas, MMN supplements with far fewer components indicated little to no effect (average RR 1.02; 95% CI 0.88 to 1.18; studies = 7; participants = 3,669) (Test for subgroup differences: Chi2 = 11.51; P = 0.0007).
When compared to MMN, LNS supplementation made no difference to perinatal mortality (average RR 1.01, 95% CI 0.62 to 1.65; studies = 3; participants = 2771; low-quality evidence) and probably did not impact the risk of low birthweight (average RR 0.92, 95% CI 0.74 to 1.13; studies = 4; participants 2727; moderate-quality evidence) or SGA (average RR 0.96, 95% CI 0.86 to 1.07; studies = 4; participants = 859).
Vitamin A supplementation compared to placebo made no difference to any outcome examined.
Zinc supplementation compared to placebo had no major effect on any outcome examined, with the exception of serum/plasma zinc levels, which were probably improved among mothers (average MD 0.43 umol/L; 95% CI -0.04 to 0.89; studies = 5; participants = 1,202), although the confidence interval crossed the line of no effect.
Iron supplementation, when compared to no iron or placebo, showed a large significant effect on maternal anaemia, reducing the risk by 47% (average RR 0.53, 95% CI 0.43 to 0.65; studies = 6; participants = 15,737; moderate-quality evidence) and a significant effect on low birthweight, reducing the risk by 12% (average RR 0.88, 95% CI 0.78 to 0.99; studies = 4; participants = 17,257; high-quality evidence), but had no important effect on perinatal mortality (average RR 0.88, 95% CI 0.71 to 1.08; studies = 4; participants = 17,464; moderate quality evidence).
When compared to placebo, supplementation with vitamin D may have reduced the risk of preterm births (average RR 0.64; 95% CI 0.40 to 1.04; studies = 7; participants = 1,262); however, it had no impact on SGA.
When compared to placebo, calcium supplementation probably improved rates of pre-eclampsia/eclampsia among mothers (average RR 0.45; 95% CI 0.19 to 1.06; studies = 4; participants = 9,616), but made no difference to other outcomes that were assessed in this review.
Overall completeness and applicability of evidence
This review included 72 studies that evaluated all forms of micronutrient and vitamin supplementation during pregnancy on maternal and child outcomes, of which 64 trials contributed data to pooled analyses. The remaining eight studies that could not be pooled with other studies were narratively synthesized. To our knowledge, this is the first systematic review that has compiled all evidence from 1995, across all low- and middle-income countries, regarding multiple forms of micronutrient and vitamin supplementation in one report, covering a wide breadth of outcomes, including maternal, fetal, infant outcomes pertaining to morbidity, mortality, nutrition and biochemical statuses, and child outcomes such as longitudinal developmental outcomes. Certain forms of supplementation could not be evaluated in this review given the insufficient number of studies per reported outcome; a minimum of three studies was required. While comparisons involving iodine, folic acid, vitamin B12 and vitamin D plus calcium supplementation could not be evaluated, this review comprehensively synthesized eight other important and common forms of supplementation, involving 439,649 pregnant women. It is important to note that while data regarding LNS supplementation was captured, there were still not enough studies to reliably evaluate its benefits compared to MMN supplementation; further research is highly recommended.
This review also aimed to assess effectiveness along with efficacy. Despite the numerous antenatal and maternal health programmes that exist in , the majority of programme evaluations did not fit our inclusion criteria related to study design (RCTs or quasi experimental studies). Thus, only two effectiveness trials were included: Friis et al. (2004) and Huy et al. (2009). A recent systematic review by Hossain et al. (2017) reviewed the evidence on health and nutrition programs aimed at reducing stunting in low- and middle-income countries. The authors found that while nutrition focused interventions are necessary, a combination of nutrition-specific interventions (e.g. maternal supplementation during pregnancy) and nutrition-sensitive interventions (e.g. social safety nets, maternal mental health and women's empowerment, to name a few) is most successful at reducing stunting in the child population. They listed health and nutrition during preconception, pregnancy and lactation, and micronutrient supplementation for mothers and children as important nutrition specific interventions, under which the interventions of this review fall. Given that stunting is an indicator of chronic malnutrition, and has long term, generational effects on maternal and child health, this highlights the importance of maternal supplementation interventions to improve the nutrition of mothers and children generally. The authors also noted that all of the studies included in this review were cross-sectional or observational in nature, which limits causality of findings. None of the programmes were designed with a true control area or group in which there was no intervention. As evaluation of micronutrient and vitamin supplementation continues, it is important to consider the design of these effectiveness studies and programmes so as to be included in future meta-analyses.
While we included longer-term outcomes in this review, such as those commonly reported in the under-five child and developmental outcomes, very few studies examine these outcomes in terms of maternal supplementation. Despite the few number of studies, our findings showed that MMN supplementation, compared to iron with or without folic acid, did improve diarrhea in children (studies = 4), child serum retinol concentrations (studies = 3), and executive function (studies = 3). A number of studies did report other child development outcomes, such as general intelligence (studies = 8) and motor function (studies = 7); however, there is significant diversity in the tests and scores used to measure, age of participants and time of assessment. While MMN supplementation showed little to no effect, the wide diversity of scores utilized by researchers and the range of ages evaluated may lend to difficulty in pooling results effectively. Apart from MMN supplementation compared to iron with or without folic acid, no other comparison in this review included studies that reported on long-term child outcomes.
According to protocol, subgroup analyses were conducted for primary outcomes permitting data availability. Subgroup analyses were conducted for the MMN vs. IFA, zinc vs. placebo and iron vs. placebo comparisons for geographical region, dose of iron (mg) in the MMN or IFA supplement, and MMN supplement composition. However, subgroup analyses could not be conducted based on a variety of other descriptive measures including maternal age, sex of infant, baseline nutritional status of the mother, duration of intervention and dose of intervention, with the exception of the subgroup analysis based on MMN composition (UNIMMAP vs. adapted UNIMMAP vs. non-UNIMMAP formulations). As such, conclusions could not be drawn regarding the optimal doses and especially, duration of supplementation. Given that the majority of all included studies in this review recruited only pregnant women who began supplementation mostly during the first and second trimester, and not those in the preconception period, this review cannot comment on the importance of preconception supplementation, and its short and long-term effects on maternal, fetal, infant, and child health outcomes. This is a notable limitation given the breadth of evidence supporting the importance of preconception health in mothers to reduce maternal and child morbidity and mortality related to pregnancy (Dean et al., 2014, Lassi et al., 2014, Mason et al., 2014). A systematic review by Dean et al. (2014) examined the role of preconception and peri-conception interventions in mothers in all economic settings, including micronutrient and vitamin supplementation, and concluded that greater positive impacts and benefits for mother and child may be noticed if preconception supplementation was implemented for all women of reproductive age, compared to periconception supplementation. It is possible that the lack of effect of supplementation on mortality outcomes such as maternal, infant, and perinatal mortality, and remaining uncertainty of the effects of micronutrient supplementation on preterm births, miscarriage, and congenital anomalies, might be due to supplementation beginning too late. Especially in low- and middle-income settings where the majority of women have poor nutritional status and health prior to conception, preconception care and supplementation may have great impact and benefit on maternal, infant and child health outcomes in these populations.
Post-hoc exploratory analyses were also conducted, comparing studies that provided strictly the micronutrient in question to studies who provided additional micronutrients along with the supplement (mainly iron and folic acid as prenatal standard of care). The aim was to dissociate possible differences in the true effects of the micronutrient itself, without the possible modifier effects of other micronutrients. This data disaggregation is unique to this review. Post-hoc analyses were conducted for the following comparisons: zinc vs. placebo, iron vs. placebo, vitamin D vs. placebo and calcium vs. placebo. These analyses did demonstrate differences in the true effects of the micronutrients itself for certain outcomes, such as zinc serum/plasma concentration, maternal iron deficiency, and pre-eclampsia/eclampsia, where provision of strictly zinc, iron and calcium, respectively noted greater improvements compared to supplementation with additional micronutrients. The calcium vs. placebo comparison showed that additional micronutrients had greater benefit for stillbirths, preterm births and mode of delivery - Caesarean section; which further substantiates the support for multiple micronutrient supplementation during pregnancy. For the MMN vs. IFA comparison, post-hoc analyses were conducted for certain outcomes to dissociate possible differences in MMN supplements containing many components, the common definition of a MMN supplement, compared to the review's definition of a MMN supplement, which was any supplement containing at least three micronutrient/vitamin components. Generally, MMN supplements with a greater number of micronutrients performed better in terms of improving maternal and child health outcomes, especially for outcomes like low birthweight, stillbirth, and SGA.
Another limitation of this review is our exclusion of certain populations, including women who were anaemic, women at high risk of pregnancy disorders, or those who had chronic illnesses, because many of these conditions are quite prevalent in maternal populations living in low- and middle-income countries. As a point of distinction, we excluded studies that had specifically recruited these groups of women, though understand that many of these conditions (e.g. anaemia) are present in the women included within these analyses. As a result, for some of our outcomes, we may not have seen similar effects on maternal and infant outcomes as reported by other reviews, who mostly did include these populations. For example, a recent systematic review, Smith et al. (2017) disaggregated data by maternal anaemia status, and reported a larger effect by MMN supplementation on birth outcomes in women with poorer nutritional status than women who were non-anemic. Given our exclusion criteria, our review did not have enough studies to comment and disaggregate data by factors such as maternal nutritional status at baseline, and thus this review is unable to identify specific groups that may benefit the most from different types of supplementation. Similarly, our review is also unable to examine data and comment on the adolescent population due to data limitations. Our inclusion criteria included healthy pregnant women of any age, which would certainly capture pregnant adolescents given adolescent pregnancies are common in low- and middle-income countries. However, none of our studies, though they included adolescent participants, disaggregated data by age group. Thus, this review is unable to identify if specific effects of maternal supplementation exist in this particular demographic. These may be considerations for future updates and research.
Another limitation was our lack of ability to disaggregate birth outcomes by sex. Recent evidence highlights differences for certain outcomes between female and male infants. Smith et al. (2017) noted that MMN supplementation consistently reduced mortality in female infants by 15% compared to their male counterparts. Similarly, Christian et al. (2005), also reported a significant 17% reduction in infant mortality amongst female infants compared to their male counterparts who saw no reduction. Biological mechanisms are still unclear, but some studies (Lee et al., 2009, West et al., 2014) postulate that the difference in mortality might be caused by difference in birth size between sexes. This might be an important consideration in a future update of this review, to consider the sex differences for important outcomes, especially mortality, across all forms of micronutrient and vitamin supplementation; Smith et al. (2017) and Christian et al. (2005) solely evaluated MMN versus IFA supplementation.
Quality of the evidence
Risk of bias assessment was conducted for individual studies based on the following criteria: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants, personnel and outcome assessment (performance bias and detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other potential forms of bias. Each of these categories were assessed as high or low risk, or unclear risk, if there was insufficient information to make any judgement. To evaluate the quality of the available evidence in this review, assessment by outcome was conducted using the GRADE methodology, as outlined in the methods. A 'Summary of Findings' table was created for the primary outcomes of maternal anaemia, maternal mortality, perinatal mortality and low birthweight for Comparisons I to VIII. For Comparison I (IFA vs. FA), we graded low birthweight as high quality, and down-graded maternal anaemia and perinatal mortality to moderate-quality for funnel plot asymmetry, possibly indicating publication bias.
For Comparison II (MMN vs. IFA), maternal anaemia, low birthweight and perinatal mortality were assessed as high-quality, while maternal mortality was downgraded by one to moderate-quality because the confidence interval of the point estimate fails to exclude important harm. Maternal iron deficiency anaemia was graded very low for large heterogeneity, the small number of events and a potential publication bias as indicated by funnel plot asymmetry. For Comparison III (LNS vs. MMN), low birthweight was downgraded to moderate quality, and perinatal mortality was downgraded to low-quality because the risk of bias assessment was high or unclear for a substantial proportion of studies in the outcomes. Perinatal mortality was further downgraded due to the small number of events and because the confidence interval of the point estimate failed to exclude important harm. For Comparison IV (Vitamin A vs. placebo), maternal mortality was downgraded by two to low-quality because a substantial proportion of studies were assessed as high or unclear risk of bias, low number of events, and the confidence interval crossed the threshold for decision making. For Comparison V (Zinc vs. placebo) was downgraded to moderate quality for the outcome low birthweight because the confidence interval of the point estimate does not exclude important harm. For Comparison VI (Iron vs. Placebo), both low birthweight and perinatal mortality were graded high quality while maternal anaemia was downgraded by one to moderate-quality due to funnel plot asymmetry, indicating possible publication bias. Comparison VII (vitamin D vs. placebo) reported no primary outcomes. For Comparison VIII (calcium vs. placebo), the outcome low birthweight was graded as high quality.
A sensitivity analysis was conducted to examine if any of the meta-analyses were especially affected by the risk of bias assessments. Included studies that were assessed with a high risk of bias for one or more domain or studies that were assessed as unclear risk in two or more domains were removed from the meta-analyses to see if this had any effect on the effect estimates of the outcomes. Diogenes et al. (2013), Duggan et al. (2014), Hambidge et al. (2019), Gowachirapant et al. (2017), Prawirohartono et al. (2011) and Taherian et al. (2002) were not included in any meta-analyses, and thus sensitivity analysis of these studies rendered no effects on any outcomes. Overall, sensitivity analyses did not significantly affect the findings for the majority of outcomes across all comparisons. An additional post-hoc analysis was conducted to examine if any effect estimates were influenced by studies where a conflict of interest was declared. Five studies reported a conflict of interest (Ashorn et al., 2015; Dewey et al., 2009; Osrin et al., 2005; West et al., 2014; Zeng et al., 2008), and exclusion of these studies did not significant affect the findings for the reported outcomes.
Potential biases in the review process
As per systematic review guidelines, all results screening, data extraction, and risk of bias assessments were completed in duplicate by two independent review authors. Given that the Cochrane methodology was closely followed, it is unlikely that this review is affected by biases in the review process. One potential bias may be the selection of pre-1995 as a cut-off date. For certain micronutrients, such as vitamin A, a number of studies evaluating their supplementation and effects on maternal, infant and child health outcomes were conducted pre-1995.
Agreements and disagreements with other studies or reviews
To better support our explanations within this section, we have provided a table that compares our findings to those of recent and related Cochrane reviews. Please see Table 17.
Comparison table of systematic reviews
MMN vs. IFA
The findings of this review on the reduction of LBW as a result of MMN supplementation corroborate those of other systematic reviews (Bhutta et al., 2012; Christian et al., 2005; Kawai et al., 2011; Keats et al., 2019; Margetts et al., 2009; Ramakrishnan et al., 2012). In comparison to the most recent Cochrane update, Keats 2019 found that MMN supplementation led to a 12% reduction (average RR 0.88; 95% CI 0.8 to 0.91) in the risk of LBW across 19 studies; our findings report a slightly greater reduction (average RR 0.85; 95% CI 0.77 to 0.93; participants = 79,972) in a pooled analysis of 28 studies. MMN supplementation did not have a significant effect on perinatal mortality and maternal mortality, which is similar to the findings of other systematic reviews, including the most recent update of the Cochrane review (Kawai et al., 2011; Keats et al., 2019; Ramakrishnan et al., 2012). The RR estimates for perinatal mortality and maternal mortality in this review were the same as those reported in Keats et al. (2019): 1.00 (0.90 to 1.11); studies = 16; participants = 92,769 and 1.04 (0.71 to 1.51); studies = 7; participants = 75,051, respectively. Keats et al. (2019) reported an average RR of 1.04 (95% CI 0.94 to 1.15; studies = 10), for the outcome maternal anaemia, which is similar to our finding, despite that we included more studies (average RR 1.02; 95% CI 0.82 to 1.10; studies = 16; participants = 23,556).
Subgroup analysis comparing studies based on MMN formulation showed that MMN supplementation with more components (UNIMMAP or supplements with >4 micronutrients) lend to improved birth outcomes in pregnant women compared to MMN supplementation with fewer components (non-UNIMMAP or supplements with <or equal to 4 micronutrients), especially for outcomes such as low birthweight. Ramakrishnan et al. (2012) meta-analyzed 16 studies that compared supplementation of women during pregnancy with five or more micronutrients compared with supplementation with three or fewer micronutrients, while Bhutta et al. (2012) compared 7 studies whose MMN supplements had >5 components versus <3 supplements. Both reviews noticed a more effective reduction in risk of low birthweight and SGA infants in studies that provide MMN supplements with >than three micronutrients, compared to studies with few components in their MMN supplements, which aligns with this review.
Although not primary outcomes in our review, commonly reported outcomes in other systematic reviews include stillbirth, preterm birth, SGA, and neonatal mortality. Our findings demonstrate a greater reduction in the risk of stillbirths (average RR 0.91; 95% CI 0.86 to 0.98; studies = 22; participants = 96,772) when compared to other reviews; Ramakrishnan et al. (2012) showed no beneficial effect, while Keats et al. (2019) showed a minimal reduction (average RR 0.95; 95% CI 0.90-1.01; studies = 17). We found that MMN supplementation slightly improved preterm birth (average RR 0.96, 95% CI 0.91 to 1.01; studies = 29; participants = 99,855), while Keats et al. (2019) found a similar reduction (average RR 0.95, 95% CI 0.90 to 1.01; studies = 19). For SGA, our review showed an 7% reduction in the risk of SGA (average RR 0.93; 95% CI 0.88 to 0.98; studies = 19; participants = 52,965], which was similar to Keats et al. (2019) (average RR 0.92; 95% CI 0.88 to 0.97; studies = 17) and Smith et al. (2017) (average RR 0.94 95% CI 0.90 to 0.98; studies = 16). However, greater reductions in SGA with MMN supplementation were reported in Ramakrishnan et al. (2012) (average RR 0.83, 95% CI 0.73 to 0.95) and Kawai et al. (2011) (average RR 0.85, 95% CI 0.78 to 0.93). Consistent with several other reviews (Bhutta et al., 2012; Christian et al., 2005; Kawai et al., 2011; Keats et al., 2019; Margetts et al., 2009; Ramakrishnan et al., 2012; Smith et al., 2017) we found that MMN supplementation has no important effect on neonatal mortality.
There are several possible reasons for these differences. Firstly, our review included a greater number of studies. Second, in Ramakrishnan et al. (2012), MMN must have contained at least five micronutrients, whereas we included any supplement with at least three. Third, Kawai et al. (2011) included maternal populations that were undernourished, while our review only included healthy populations as participants. Kawai et al. (2011) noted that MMN supplementation resulted in greater reductions in maternal and infant outcomes, such as low birthweight, mortality and SGA in anaemic pregnant woman compared to non-anaemic pregnant women. Therefore, it is possible that baseline maternal nutritional status may be an important modifier of the effect of MMN supplementation on maternal and infant outcomes.
LNS vs MMN
For LNS versus MMN supplementation, the findings of this review corroborate the findings of a recent Cochrane review (Das et al., 2018). Both demonstrated little to no impact on LBW (average RR 0.92; 95% CI 0.74 to 1.13; studies = 4; participants = 2,727; Das et al. (2018) average RR 0.92; 95% CI 0.74 to 1.13; studies = 3), preterm birth (average RR 1.15; 95% CI 0.93 to 1.42; studies = 4; participants = 2,953; Das et al. (2018) average RR 1.15; 95% CI 0.93 to 1.42; studies = 3), SGA (average RR 0.96; 95% CI 0.86 to 1.07; studies = 4; participants = 2,716; Das et al. (2018) average RR 0.95; 95% CI 0.84 to 1.07; studies = 3), and neonatal mortality (average RR 0.81 95% CI 0.45 to 1.45; studies = 3; participants = 2,727; Das et al. (2018) average RR 0.88 95% CI 0.36 to 2.15; studies = 1).
Iron vs Placebo
Our findings also corroborate those of a recent review conducted by Peña-Rosas et al. (2015), who looked at iron supplementation compared to placebo or no treatment. Our findings show that iron or IFA supplementation, compared to no iron, reduces maternal anaemia (average RR 0.53; 95% CI 0.43, to 0.65; studies = 6; participants = 15,737) and LBW (average RR 0.88; 95% CI 0.78 to 0.99; studies = 4; participants = 17,257). Comparatively, Peña-Rosas et al. (2015) reported a slightly greater reduction in maternal anaemia (average RR 0.29; 95% CI 0.19 to 0.47; studies = 14) and a greater reduction in LBW (average RR 0.63; 95% CI 0.30 to 1.32; studies = 6). In terms of preterm birth, Peña-Rosas et al. (2015) indicated a greater reduction in the risk of preterm births due to iron supplementation in mothers (average RR 0.82; 95% CI 0.58 to 1.14; studies = 6); compared to this review (average RR 0.94; 95% CI 0.63 to 1.41; studies = 6; participants = 18,419). Some of these difference may be due to the fact that Peña-Rosas et al. (2015) included studies with anaemic populations at baseline, whereas these studies would have been excluded in this review as the focus was on healthy pregnant participants.
IFA vs FA
Our findings also corroborate those of a recent review conducted by Peña-Rosas et al. (2015), who looked at iron-folic acid supplementation compared to folic acid alone. Both reviews reported similar reductions in the risk of LBW infants (average RR 0.88; 95% CI 0.78 to 0.99; studies =4; participants = 17,257; Peña-Rosas et al. (2015) average RR 0.88; 95% CI 0.78 to 1.00; studies = 4), and preterm births (average RR 0.96; 95% CI 0.64 to 1.44; studies = 5; participants = participants = 17,637; Peña-Rosas et al. (2015) average RR 0.97; 95% CI 0.87 to 1.08; studies = 4). While perinatal mortality was not an outcome reported in Peña-Rosas et al. (2015), our results are similar for neonatal mortality (average RR 0.85; 95% CI 0.55 to 1.31; studies = 3; participants = 15,794; Peña-Rosas et al. (2015) average RR 0.91; 95% CI 0.71 to 1.18; studies = 4), whereby there was no significant reduction. Peña-Rosas et al. (2015) reported a greater reduction in the risk of maternal anaemia (average RR 0.34; 95% CI 0.21 to 0.55; studies = 2) compared to our findings (average RR 0.52; 95% CI 0.41 to 0.66; studies = 5; participants = 15,540).
Zinc vs Placebo
Compared to Ota et al. (2015), a recent review of zinc supplementation, our review found that zinc supplementation did not have an important effect on LBW (average RR 1.08 95% CI 0.94 to 1.25; studies = 10; participants = 4,633). However, Ota et al. (2015) showed a 7% reduction in the risk of LBW (average RR 0.93 95% CI 0.78 to 1.12; studies = 14). In terms of preterm births, our review found a minimal effect of zinc supplementation on the reduction of preterm births (average RR 0.97, 95% CI 0.80 to 1.17; studies = 11; participants = 5,017), while Ota et al. (2015) showed a greater reductive effect (average RR 0.86; 95% CI 0.76 to 0.97; studies = 16). Ota et al. (2015) includes additional studies, which may lend to a greater certainty in these results compared to our own. These studies were not eligible for inclusion in our review because they were conducted in high-income settings, included wrong patient populations, or could not be retrieved.
Vitamin A vs. Placebo
Similar to McCauley et al. (2015), there were very few studies that assessed vitamin A supplementation versus no vitamin A or placebo. In terms of maternal mortality, our findings (average RR 0.90 95% CI 0.67 to 1.18, studies = 3; participants = 124,002) are in accord with McCauley et al. (2015) (average RR 0.88, 95% CI 0.65 to 1.20; studies = 4) in that vitamin A supplementation does not improve maternal mortality. As well, both review report no effect of vitamin A supplementation on risk reduction of stillbirths (average RR 1.01; 95% CI 0.96 to 1.07; studies = 3; participants = 115,223; McCauley et al. (2015) average RR 1.04; 95% CI 0.98 to 1.10; studies = 2).
Vitamin D vs placebo
Several recent reviews have looked at the effects of vitamin D supplementation on pregnancy outcomes, against which many of our findings are aligned. We found that vitamin D, compared to placebo, may reduce preterm birth (average RR 0.64 95% CI 0.40 to 1.04; studies = 7; participants = 1,262). This finding differs from that which were reported in Roth et al. (2017) (average RR 1.00 95% CI 0.77 to 1.30; studies = 15), and by Palacios et al. (2019), a recent update to the De-Regil et al. (2016) Cochrane review (average RR 0.66; 95% CI 0.31 to 1.30; studies = 7). In terms of SGA, our findings (average RR 0.93, 95% CI 0.57 to 1.53; studies = 3; participants = 851) were not similar to Roth et al. (2017), which showed a significant reduction in risk of SGA (average RR 0.60, 95% CI 0.40 to 0.90; studies = 5). A possible reason for this might be that we excluded studies with patient populations that were unhealthy or had am explicitly reported micronutrient deficiency, such as vitamin D deficiency; whereas, Roth et al. (2017) included all studies that evaluated vitamin D supplementation compared to placebo, regardless of health status of the maternal populations. Including populations who are micronutrient-deficient at baseline may modify the effect of the intervention. While not a primary outcome in this review, caesarean section as a mode of delivery is a common outcome reported across many vitamin D supplementation studies and reviews. Our results show little to no effect on this outcome (average RR 1.05, 95% CI 0.94 to 1.18; studies = 5; participants = 1,063), similar to Roth et al. (2017) (average RR 1.02; 95% CI 0.93 to 1.12; studies = 17), and Palacios et al. (2019) (average RR 0.98, 95% CI 0.80 to 1.21; studies = 10).
Calcium vs Placebo
Our findings show that calcium supplementation compared to placebo probably improves rates of pre-eclampsia/eclampsia among mothers (average RR 0.45; 95% CI 0.19 to 1.06; studies = 4; participants = 9,616). Hofmeyr et al. (2018) reported similar effects for pre-eclampsia (average RR 0.45; 95% CI 0.31 to 0.65; studies = 12), though confidence intervals around our estimate are much wider, lending to more uncertainty around the pooled effect. Both this review and Hofmeyr et al. (2018) reported effects of calcium supplementation on the reduction of preterm birth; however Hofmeyr et al. (2018) reported a great reduction in preterm birth (average RR 0.76; 95% CI 0.60 to 0.97; studies = 9) compared to our findings (average RR 0.84; 95% CI 0.65 to 1.08; studies = 4; participants = 9,933). Lastly, our findings on the reduction of low birthweight as a result of calcium supplementation compared to placebo differs from that reported by a recent systematic review by Hofmeyr et al. (2018). Our findings show no effect of calcium supplementation on the reduction in the risk of low birthweight in the intervention group compared to the control group (average RR 0.99; 95% CI 0.95 to 1.04; studies = 3; participants = 9,498), while Hofmeyr et al. (2018) found a 15% reduction in the risk of low birthweight. The differences may be explained by the different inclusion criteria for participants between the reviews. While this review excluded participants who had a reported risk for a hypertensive disorder, such as pre-eclampsia, Hofmeyr et al. (2018) included these participants, as well as, those who were reported at screening to be calcium-deficient. These differences at baseline may have contributed to greater effects of supplementation in studies reported by Hofmeyr et al. (2018) compared to our findings.
AUTHORS' CONCLUSIONS
Implications for practice
The findings of this review suggest that micronutrient and vitamin supplementation improves certain maternal, fetal, infant and child outcomes. Across all comparisons, it was noted that micronutrient and vitamin supplementation have little to no effect on mortality outcomes, specifically maternal, neonatal and perinatal mortality, which is consistent with observations from other systematic reviews. Generally, the findings of this review support micronutrient and vitamin supplementation in all women irrespective of maternal nutritional status during pregnancy, especially in low- and middle-income settings, as it provides improvements in maternal, fetal and infant outcomes. This review also shows that MMN supplementation should be considered as the preferred option for standard prenatal care, when compared to IFA. This is especially evident for outcomes such as stillbirths, SGA and low birthweight. MMN supplementation also showed possible effects on preterm births. Novel findings of this review are the improvements of diarrhea and serum/plasma retinol in children with MMN supplementation, although more research is required to interpret these results with greater reliability. IFA or iron supplementation seem to be better options compared to other micronutrients for improving maternal anaemia. LNS supplementation compared to MMN supplementation showed no improved effect on maternal and child outcomes; however, very few studies were included. Further study is needed to understand LNS supplementation compared to MMN supplementation. Calcium supplementation may reduce the risk of pre-eclampsia and eclampsia in pregnancy. Vitamin A supplementation indicated a slight improved effect on serum/plasma retinol in mothers, while zinc supplementation seems to have minimal effect on maternal and infant outcomes.
Implications for research
Given that the benefits of micronutrient and vitamin supplementation have been well corroborated by many other systematic reviews, future research should now consider conducting more detailed analyses to identify optimal dosages and formulations of micronutrient supplements, and duration of supplementation. Similarly, consideration should be made to identifying specific groups of mothers that could benefit from different forms of supplementation, including different dosages, based on maternal nutritional status at baseline or screening (e.g. by maternal BMI, stature, or anaemia status). A specific group about which focused and disaggregated data is needed are pregnant adolescents, who may have modified supplementation effects and needs compared to pregnant adult women.
While this review notes improvements in certain child health outcomes, few studies conduct follow-up evaluations amongst their child participants. Future research should consider evaluating longitudinal outcomes in the under-five child and older children on health and early childhood development. It would be beneficial to evaluate the long-term effects of micronutrient and vitamin supplementation during pregnancy, especially given that evidence indicates that certain child outcomes are indicators for chronic health issues and possible generational effects, such as stunting as an indicator of chronic malnutrition.
Future research should also consider disaggregating data by sex for infant and child outcomes, as increasing evidence has shown sex-specific differences for certain morbidity and mortality outcomes. Better understanding of the biological mechanisms behind these sex-specific differences should also be considered in future research. However, it is important to note that these sex-specific differences should not be used as evidence to encourage selective supplementation of mothers during pregnancy; regardless of fetal sex, all mothers should receive the standard of care and micronutrient and vitamin supplementation provided by programmes within their setting. Lastly, future programmes and effectiveness studies should consider designs other than observational as methods of evaluation, and should consider a true comparison or control area. This may lead to more robust evidence and a stronger causality of findings in these large-scale programmes.
CONTRIBUTIONS OF AUTHORS
Emily Keats and Aamer Imdad have methodological, statistical, and information retrieval expertise. Zulfiqar Bhutta has content expertise. Christina Oh, Tamara Chau and Dina S. Khalifa received training in systematic review methods.
DECLARATIONS OF INTEREST
The authors are not aware of any conflicts of interest arising from financial or researcher interests.
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
An exploratory post-hoc analysis was included, for both primary and secondary outcomes, comparing studies that provided strictly the single micronutrient to studies that provided additional micronutrients along with the micronutrient in question (e.g. studies that strictly provided calcium and studies that provided calcium with iron-folic acid as the standard of care). The aim of this analysis was to dissociate the true effects of the micronutrient itself from the possible modifier effects of the additional micronutrients. For the MMN vs. IFA comparison, a post-hoc analysis was conducted comparing studies that provided MMN supplements with >4 micronutrients to studies that provided supplements with only 3 or 4 micronutrients.
PUBLISHED NOTES
Characteristics of studies
Characteristics of included studies
Ahmad 2015
Risk of bias table
Aminisani 2009
Risk of bias table
Asemi 2013
Risk of bias table
Asemi 2016
Risk of bias table
Ashorn et al. 2015
Risk of bias table
Belizán 1997
Risk of bias table
Bhutta 2009
Risk of bias table
Castillo-Durán 2001
Risk of bias table
Caulfield 1999
Risk of bias table
Charandabi 2015
Risk of bias table
Choudhury 2012
Risk of bias table
Christian 2003
Risk of bias table
Cox 2005
Risk of bias table
Darling et al. 2017
Risk of bias table
Dewey 2009
Risk of bias table
Dijkhuizen 2001
Risk of bias table
Diogenes et al. 2013
Risk of bias table
Duggan et al. 2014
Risk of bias table
Etheredge 2015
Falahi (2010)
Risk of bias table
Fawzi et al. 2007
Risk of bias table
Friis 2004
Risk of bias table
Gowachirapant 2017
Risk of bias table
Hafeez 2005
Risk of bias table
Hambidge 2019
Risk of bias table
Hanieh 2013
Risk of bias table
Hossain et al. 2012
Risk of bias table
Huy 2009
Risk of bias table
Huybregts 2009
Risk of bias table
Jarjou et al. 2006
Risk of bias table
Kæstel et al. 2005
Risk of bias table
Khan 2016
Kirkwood 2010
Risk of bias table
Korkmaz 2014
Risk of bias table
Kumar 2009
Risk of bias table
Liu et al. 2013
Risk of bias table
López-Jaramillo 1997
Risk of bias table
Menendez 1995
Risk of bias table
Merialdi 2004
Risk of bias table
Moore 2012
Risk of bias table
Muslimatun 2001
Risk of bias table
Naghshineh 2016
Risk of bias table
Osendarp et al. 2000
Risk of bias table
Osrin et al. 2005
Risk of bias table
Ouladsahebmadarek 2011
Risk of bias table
Prawirohartono et al. 2011
Risk of bias table
Preziosi 1997
Risk of bias table
Ramakrishnan et al. 2003
Risk of bias table
Roberfroid et al. 2008
Roth 2013 (AViDD)
Roth et al., 2018 (MDIG)
Risk of bias table
Saaka 2009
Risk of bias table
Sabet 2012
Risk of bias table
Sablok 2015
Risk of bias table
Sahu et al. 2009
Risk of bias table
Semba et al. 2001
Risk of bias table
Sorouri 2016
Risk of bias table
Summit 2008
Risk of bias table
Sunawang 2009
Risk of bias table
Taherian 2002
Risk of bias table
Tanumihardjo 2002
Risk of bias table
Tofail et al. 2008
Risk of bias table
Vaziri 2016
Risk of bias table
Villar 2006
Risk of bias table
West et al. 1999
Risk of bias table
West et al. 2011
Risk of bias table
West 2014
Risk of bias table
Zagré 2007
Risk of bias table
Zeng et al. 2008
Risk of bias table
Zhao 2015
Ziaei et al., 2007
Ziaei et al., 2008
Characteristics of excluded studies
Characteristics of studies awaiting classification
Characteristics of ongoing studies
Evidence of funnel plot asymmetry, indicating possible publication bias.
Confidence interval of point estimate fails to exclude important harm.
Wide variance of point estimates and large I2.
Small number of events.
Evidence of funnel plot asymmetry indicating possible publication bias.
Risk of bias for a substantial proportion of studies was high or unclear
Confidence interval of point estimate fails to exclude important harm
Small number of events
Evidence of funnel plot asymmetry, indicating possible publication bias.
Confidence interval of point estimate does not exclude important harm.
Risk of bias for a substantial proportion of studies were high or unclear.
Low number of events.
Confidence interval of point estimate crosses the threshold for decision. making.
Additional tables
DATA AND ANALYSES
IFA vs Folic Acid
MMN vs IFA
LNS vs MMN
Vitamin A vs. Placebo
Zinc vs. Placebo
Iron vs. Placebo
Vitamin D vs. Placebo
Calcium vs. Placebo
MMN vs. IFA: Subgroup analysis for primary outcomes
Iron vs. Placebo: Subgroup analysis for primary outcomes
Zinc vs. Placebo: Subgroup analysis for primary outcomes
SOURCES OF SUPPORT
Internal sources
Centre for Global Child Health at The Hospital for Sick Children, Canada
Grant Number: OPP1137750
External sources
Bill & Melinda Gates Foundation, Other
Feedback