
Abstract
Background
The last two decades have seen a significant decrease in mortality for children <5 years of age in low and middle-income countries (LMICs); however, neonatal (age, 0–28 days) mortality has not decreased at the same rate. We assessed three neonatal nutritional interventions that have the potential of reducing morbidity and mortality during infancy in LMICs.
Objectives
To determine the efficacy and effectiveness of synthetic vitamin A, dextrose oral gel, and probiotic supplementation during the neonatal period.
Search Methods
We conducted electronic searches for relevant studies on the following databases: PubMed, CINAHL, LILACS, SCOPUS, and CENTRAL, Cochrane Central Register for Controlled Trials, up to November 27, 2019.
Selection Criteria
We aimed to include randomized and quasi-experimental studies. The target population was neonates in LMICs. The interventions included synthetic vitamin A supplementation, oral dextrose gel supplementation, and probiotic supplementation during the neonatal period. We included studies from the community and hospital settings irrespective of the gestational age or birth weight of the neonate.
Data Collection and Analysis
Two authors screened the titles and extracted the data from selected studies. The risk of bias (ROB) in the included studies was assessed according to the Cochrane Handbook of Systematic Reviews. The primary outcome was all-cause mortality. The secondary outcomes were neonatal sepsis, necrotizing enterocolitis (NEC), prevention and treatment of neonatal hypoglycaemia, adverse events, and neurodevelopmental outcomes. Data were meta-analyzed by random effect models to obtain relative risk (RR) and 95% confidence interval (CI) for dichotomous outcomes and mean difference with 95% CI for continuous outcomes. The overall rating of evidence was determined by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
Main Results
Sixteen randomized studies (total participants 169,366) assessed the effect of vitamin A supplementation during the neonatal period. All studies were conducted in low- and middle-income (LMIC) countries. Thirteen studies were conducted in the community setting and three studies were conducted in the hospital setting, specifically in neonatal intensive care units. Studies were conducted in 10 different countries including India (four studies), Guinea-Bissau (three studies), Bangladesh (two studies), and one study each in China, Ghana, Indonesia, Nepal, Pakistan, Tanzania, and Zimbabwe. The overall ROB was low in most of the included studies for neonatal vitamin A supplementation. The pooled results from the community based randomized studies showed that there was no significant difference in all-cause mortality in the vitamin A (intervention) group compared to controls at 1 month (RR, 0.99; 95% CI, 0.90–1.08; six studies with 126,548 participants, statistical heterogeneity I 2 0%, funnel plot symmetrical, grade rating high), 6 months (RR, 0.98; 95% CI, 0.89–1.07; 12 studies with 154,940 participants, statistical heterogeneity I 2 43%, funnel plot symmetrical, GRADE quality high) and 12 months of age (RR, 1.04; 95% CI, 0.94–1.14; eight studies with 118,376 participants, statistical heterogeneity I 2 46%, funnel plot symmetrical, GRADE quality high). Neonatal vitamin A supplementation increased the incidence of bulging fontanelle by 53% compared to control (RR, 1.53; 95% CI, 1.12–2.09; six studies with 100,256 participants, statistical heterogeneity I 2 65%, funnel plot symmetrical, GRADE quality high). We did not identify any experimental study that addressed the use of dextrose gel for the prevention and/or treatment of neonatal hypoglycaemia in LMIC. Thirty-three studies assessed the effect of probiotic supplementation during the neonatal period (total participants 11,595; probiotics: 5854 and controls: 5741). All of the included studies were conducted in LMIC and were randomized. Most of the studies were done in the hospital setting and included participants who were preterm (born < 37 weeks gestation) and/or low birth weight (<2500 g birth weight). Studies were conducted in 13 different countries with 10 studies conducted in India, six studies in Turkey, three studies each in China and Iran, two each in Mexico and South Africa, and one each in Bangladesh, Brazil, Colombia, Indonesia, Nepal, Pakistan, and Thailand. Three studies were at high ROB due to lack of appropriate randomization sequence or allocation concealment. Combined data from 25 studies showed that probiotic supplementation reduced all-cause mortality by 20% compared to controls (RR, 0.80; 95% CI, 0.66–0.96; total number of participants 10,998, number needed to treat 100, statistical heterogeneity I 2 0%, funnel plot symmetrical, GRADE quality high). Twenty-nine studies reported the effect of probiotics on the incidence of NEC, and the combined results showed a relative reduction of 54% in the intervention group compared to controls (RR, 0.46; 95% CI, 0.35–0.59; total number of participants 5574, number needed to treat 17, statistical heterogeneity I 2 24%, funnel plot symmetrical, GRADE quality high). Twenty-one studies assessed the effect of probiotic supplementation during the neonatal period on neonatal sepsis, and the combined results showed a relative reduction of 22% in the intervention group compared to controls (RR, 0.78; 95% CI, 0.70–0.86; total number of participants 9105, number needed to treat 14, statistical heterogeneity I 2 23%, funnel plot symmetrical, GRADE quality high).
Authors' Conclusions
Vitamin A supplementation during the neonatal period does not reduce all-cause neonatal or infant mortality in LMICs in the community setting. However, neonatal vitamin A supplementation increases the risk of Bulging Fontanelle. No experimental or quasi-experimental studies were available from LMICs to assess the effect of dextrose gel supplementation for the prevention or treatment of neonatal hypoglycaemia. Probiotic supplementation during the neonatal period seems to reduce all-cause mortality, NEC, and sepsis in babies born with low birth weight and/or preterm in the hospital setting. There was clinical heterogeneity in the use of probiotics, and we could not recommend any single strain of probiotics for wider use based on these results. There was a lack of studies on probiotic supplementation in the community setting. More research is needed to assess the effect of probiotics administered to neonates in-home/community setting in LMICs.
PLAIN LANGUAGE SUMMARY
Neonatal probiotic supplementation can improve infant illness and reduce death, but vitamin A does not, and may have adverse effects
Nutritional support during the 1st month of life is vital for the short- and long-term survival of the newborn. Neonatal nutrition interventions have the potential to decrease death and illness in young infants in LMICs.
What is this review about?
This review assesses the efficacy of synthetic vitamin A, dextrose, and probiotic supplementation during the neonatal period. These interventions were assessed separately and not in combination with each other.
This Campbell systematic review assesses the efficacy of three neonatal nutritional interventions that have the potential of reducing morbidity and mortality during infancy in LMICs: synthetic vitamin A, dextrose, and probiotic supplementation.
What studies are included?
Sixteen studies that assessed the effect of vitamin A supplementation during the neonatal period were included. Thirteen of these studies were conducted in the community setting and three studies were conducted in the hospital setting. All the included studies on neonatal vitamin A supplementation were conducted in LMICs. Most of the studies had a low ROB.
No experimental studies were found that evaluated the use of dextrose for the prevention or treatment of low blood sugar during the neonatal period.
Thirty-three studies assessed the use of probiotics during the 1st month of life. All included studies on probiotic supplementation were randomized and conducted in LMICs. Most of the included studies had a low ROB. The probiotics studies mainly included babies born early and/or with low birth weight, and these studies were mostly conducted in hospital settings.
Key results
Combined results from thirteen vitamin A studies conducted in the community settings showed that there was no significant effect of vitamin A supplementation for reduction of death in young infants at 1, 6, or 12 months of age. Neonatal vitamin A supplementation increases the risk of bulging fontanelle by 53%. The pooled data from probiotics studies showed that this intervention reduced the risk of death by 20% compared to controls. Further analysis showed that compared to controls, probiotic supplementation reduced the risk of a severe form of gastrointestinal illness in neonates called NEC by 54%. Probiotic supplementation also reduced the risk of blood infection called sepsis by 22% compared to controls. The quality grade ratings for these outcomes were “high.”
What are the main findings of the review?
Combined results from thirteen vitamin A studies conducted in the community settings showed that there was no significant effect of vitamin A supplementation for reduction of death in young infants at 1, 6, or 12 months of age. However, neonatal vitamin A supplementation increased the incidence of bulging fontanelle by 53%.
The pooled data from probiotics studies showed that this intervention reduced the risk of death by 20% compared to controls. Further analysis showed that compared to controls, probiotic supplementation reduced the risk of a severe form of gastrointestinal illness in neonates called NEC by 54%. Probiotic supplementation also reduced the risk of blood infection called sepsis by 22% compared to controls. The quality grade ratings for these outcomes were “high.”
What do the findings of this review mean?
Vitamin A supplementation during the 1st month of life does not reduce the risk of death during the 1st year of life in LMICs. However, neonatal vitamin A supplementation increases the risk of bulging fontanelle, which may cause damage to the brain.
We did not find any experimental studies from LMICs that assessed the use of dextrose gel supplementation during the 1st month of life for the prevention or treatment of low blood sugar.
Probiotic supplementation during the 1st month of life to babies born preterm and/or low birthweight can reduce the risk of death, blood infection and bowel sickness (NEC).
There was clinical heterogeneity in the use of probiotics and we could not recommend any single strain or combination of probiotics for wider use based of these results.
There is a lack of studies on probiotic supplementation in the 1st month of life in community settings. More research is needed to assess the effect of probiotics administered to neonates in home/community settings in LMICs.
How up-to-date is this review?
The review authors searched for studies published up to November 2019.
BACKGROUND
The decline in rates of neonatal (age, 0–28 days) mortality has been slower than the decline in child mortality between 1990 and 2016 (Alkema et al., 2014; Bhutta et al., 2015). Neonatal mortality accounted for 46% of child mortality in 2016 compared to 40% of all under-five mortality rates in 1990 (WHO, 2017a). Globally, the percentage of neonatal mortality is the highest in South Asia and Sub-Saharan Africa (Alkema et al., 2014). Optimal nutritional support during the neonatal period is vital to the short and long term survival of the newborn (Bhutta et al., 2013; WHO, 2017b). Poor nutritional status of neonates is a major cause of illness and can lead to poor growth, increased risk of infection, bleeding, and neonatal death (Bhutta et al., 2013; WHO, 2017b). The risk of morbidity and mortality during the neonatal period is higher in LMICs where many births happen at home and the prevalence of maternal malnutrition and incidence of low birth weight (birth weight <2500 g) and preterm birth (gestational age <37 weeks) is high (Bhutta et al., 2013; Lee et al., 2017; WHO, 2017b). This review focused on three nutritional interventions during neonatal periods that have the potential to reduce illness and death during infancy in LMIC.
Description of the condition
The approach to nutritional management of newborn depends on maternal nutritional status, comorbidities during pregnancy (such as gestational diabetes), pregnancy duration (term vs. preterm birth), events at birth (such as birth asphyxia), birth weight (low birth weight vs. normal birth weight) and available resources for postpartum care of the mother and the baby (such as skilled birth attendant, home vs. facility birth, availability of neonatal intensive care) (Bhutta et al., 2013; WHO, 2015, 2017a, 2017b). The most important nutritional intervention after birth is breastfeeding, which is covered in a separate Campbell review of this series. There are a number of other nutritional interventions that have been proposed in addition to breastfeeding. It is beyond the scope of this review to comprehensively evaluate all the possible nutritional interventions during the neonatal period. We limited our review to the following three interventions: neonatal synthetic vitamin A supplementation, oral dextrose gel supplementation, and probiotic supplementation during the neonatal period in LMIC. Below in this section and in the rest of the introduction, we describe the rationale and importance of reviewing these interventions.
Neonatal vitamin A deficiency (VAD)
Globally, about 190 million children and 19.1 million pregnant women are vitamin A deficient based on serum retinol levels (i.e., serum retinol <0.70 μmol/L) (WHO, 2009a). VAD is most prevalent in South Asia and Africa (Stevens et al., 2015). VAD is associated with increased risk of blindness, infections, and mortality (Imdad et al., 2017). Most of the newborns are vitamin A deficient and rely on supplementation from maternal breast milk (Haider et al., 2017). High prevalence of maternal VAD in LMICs increases the risk of neonatal VAD. There has been interest in vitamin A supplementation during neonatal period to assess if it reduces risk of illness and death (Haider et al., 2017; WHO, 2009b), as it has been shown to reduce morbidity and mortality in children 6–59 months of age (Imdad et al., 2017).
Hypoglycemia during the neonatal period
Hypoglycemia (low blood sugar) is common during the immediate neonatal period. The definition of neonatal hypoglycaemia varies. The American Academy of Pediatrics defines neonatal hypoglycaemia as blood glucose below 47 mg/dl (2.61 mmol/L); however, other societies such as the Pediatric Endocrine Society define neonatal hypoglycaemia as blood glucose <50 mg/dl (2.77 mmol/L; Thompson-Branch & Havranek, 2017; Thornton et al., 2015). Recurrent, severe, and/or persistent hypoglycaemia can lead to complications such as death; there is limited evidence to show that blood sugars below a certain level leads to long-term brain damage (Kaiser et al., 2015; McKinlay et al., 2017; Thornton et al., 2015). About 10–15% of otherwise healthy newborns have low blood sugar, and the rate is much higher among infants with additional risk factors such as large for gestational age, small for gestational age, low birth weight, preterm birth, infant of diabetic mother, and newborns with perinatal asphyxia (Thompson-Branch & Havranek, 2017). Additional risk factors for neonatal hypoglycaemia include neonatal sepsis, prolonged labor, and maternal medication use such as use of β-agonists and β-blockers (Thompson-Branch & Havranek, 2017). The recommended initial intervention to treat neonatal hypoglycaemia is to offer feeding in the form of breastfeeding followed by formula feeding if breastfeeding is unsuccessful. Persistent hypoglycaemia may require IV dextrose supplementation and admission to a neonatal intensive care unit (Thompson-Branch & Havranek, 2017; Thornton et al., 2015). In LMIC, where a significant proportion of births happen at home and incidence of low birth weight and preterm birth is high, prevention and treatment of hypoglycaemia encounters additional challenges (Singhal et al., 1991, 1992; WHO, 2017b; Williams, 1997). The instruments to test blood sugar might not be available in low-resource settings; In addition, formula, IV dextrose, and intensive care units might not be available to treat persistent and/or severe hypoglycaemia. Recent studies have tested simple interventions such as oral dextrose gel to treat neonatal hypoglycaemia and to prevent hypoglycaemia in high-risk newborns (Hegarty et al., 2016; Weston et al., 2016).
Neonatal sepsis and NEC
Neonatal sepsis and NEC are neonatal morbidities that can be fatal (Oza et al., 2015; WHO, 2017b). Neonatal sepsis is the presence of an infection leading to systemic illness. Bacterial sepsis is common in LMIC and is a significant risk factor of morbidity and mortality in these countries (WHO, 2017a). NEC is a condition that occurs in newborns and can lead to intestinal injury and death. The extent of injury may vary from mucosal injury to full thickness intestinal wall injury. NEC happens most commonly in preterm babies and especially in extremely preterm babies (<28 weeks gestational age; AlFaleh & Anabrees, 2014; Patel & Denning, 2015). Multiple factors lead to the development of NEC in preterm infants including altered bacterial gut flora affecting the protective intestinal barrier, decreased intestinal motility, and the increased susceptibility of preterm infants to inflammation and infections (Patel & Denning, 2015). Recent studies have shown that an imbalance between commensal bacteria and pathogenic bacteria (intestinal dysbiosis) makes babies vulnerable to pathogenic bacterial growth in the intestine which then causes inflammation that may contribute to neonatal sepsis and/or NEC (Arrieta et al., 2014; Deshmukh et al., 2014; Gewolb et al., 1999; Panigrahi et al., 2017). There is an increasing interest in correction of intestinal dysbiosis by probiotics to prevent NEC and neonatal sepsis. Data from early studies on probiotic use in neonates from LMIC is encouraging (AlFaleh & Anabrees, 2014; Rao et al., 2016).
Description of the intervention
Neonatal vitamin A supplementation
Vitamin A is a term used for a subclass of the family of fat soluble compounds named retinoic acids. Vitamin A is found in nature in two forms, provitamin A carotenoids and preformed vitamin A, which is essential to human bodily function. Plant-based foods are the main source of provitamin A carotenoids, of which β-carotene is the most commonly known. Animal-based foods are the main source of preformed vitamin A (Bates, 1995; Haider & Bhutta, 2011). Vitamin A from animal sources (retinol, retinal, retinoic acid, and retinyl esters) is the most active form, and synthetic vitamin A retinol has been used in most intervention trials in the past (Haider & Bhutta, 2011; Imdad et al., 2017). Plant-based foods may not be an adequate source of vitamin A, as the gastrointestinal conversion ratio from carotenoid-to-retinol varies from 6:1 to 26:1 (US Institute of Medicine, Food and Nutrition Board). VAD may, therefore, exist in areas even when there is high consumption of plant-based foods such as in South Asia and Africa (Imdad et al., 2017; Stevens et al., 2015).
Oral dextrose gel supplementation during neonatal period
Dextrose gel is a thickened aqueous solution that contains the concentrated simple carbohydrate dextrose. It can be administered by direct application to oral, buccal, or sublingual mucosa and can increase blood sugars rapidly by absorption through the highly vascularized and thin mucus membranes of the oral mucosa (Hegarty et al., 2016). Detxrose gel is a low cost nonproprietary intervention, and the gel can be prepared in hospital pharmacies. The typical ingredients include water, glucose, a gelling agent, and preservatives (Hegarty et al., 2016). The decision to use dextrose gel in a neonate should be taken on individual basis and should be avoided in neonates with compromised neurological or respiratory status (Hegarty et al., 2016; Weston et al., 2016).
Probiotic supplementation during neonatal period
Prebiotics are supplements that promote the growth of commensal bacteria (AlFaleh & Anabrees, 2014; Panigrahi et al., 2017). Probiotics contain live bacteria that enrich pools of commensal bacteria (AlFaleh & Anabrees, 2014; Millar et al., 2003; Panigrahi et al., 2017). Synbiotics are a combination of prebiotics and probiotics and might have synergistic effect (Johnson-Henry et al., 2016, Nandhini et al., 2016; Panigrahi et al., 2017). These supplements are meant to optimise gut health and their hypothesized mechanisms of actions include enhanced gut barrier function, inhibition of gut colonization with pathogenic bacteria, improvement in colonization with healthy commensal bacteria that protect the infant from enteropathogenic infection through production of acetate, enhanced innate immunity, and increased maturation of the enteric nervous system (Rao et al., 2016). Recent data have shown that probiotic supplements can prevent the incidence of NEC in preterm babies (AlFaleh & Anabrees, 2014; Millar et al., 2003; Patel & Denning, 2015; van den Akker et al., 2018). There is also promising data on use of probiotocs/synbiotics for prevention of neonatal sepsis (Rao et al., 2016; Panigrahi et al., 2017). The most commonly used strains of probiotics include Lactobacillus and Bifidobacterium (Rao et al., 2016).
How the intervention might work
Neonatal vitamin A supplementation
Vitamin A has an effect on cell differentiation and helps maintain normal functioning of epithelial cells (Bates, 1995; Bhutta et al., 2013; Haider & Bhutta, 2011). It is considered anti-infective because it helps to maintain the protective epithelial barrier of the skin and mucosa, which protects the body from infections. Vitamin A helps in the regeneration of the epithelium and therefore maintains the integrity of the body's first line of defence. These mechanisms may help prevent infections in newborns (McCullough et al., 1999; Wolbach, 1933). Synthetic vitamin A supplementation has been shown to reduce morbidity and mortality in children 6–59 months of age (Imdad et al., 2017). The potential side effects of synthetic vitamin A supplementation include vomiting and bulging fontanelle (Imdad et al., 2016, 2017; Haider & Bhutta, 2011; Haider et al., 2017). Excess vitamin A supplementation can cause toxicity that presents in the form of a bulging fontanelle in children under 1 year, headaches, vomiting, diarrhea, loss of appetite, and irritability (Haider et al., 2017; Imdad et al., 2017).
Oral dextrose gel supplementation during neonatal period
The absorption of dextrose gel through the oral mucosa leads to entry of glucose into lingual veins and into the internal jugular vein. This pathway provides almost immediate delivery of glucose to the systemic circulation and bypasses first pass liver metabolism through the portal circulation. If proven effective in preventing and treating hypoglycaemia, dextrose gel can avoid the need of intravenous glucose and reduce separation of baby from mother (Hegarty et al., 2016; Weston et al., 2016). The intervention is simple enough that it does not require special skills (such as IV placement) and can be administered by community, lay health workers, or the caregiver herself. Potential adverse effects include vomiting, choking, gagging, respiratory distress, and delay of treatment for severe hypoglycaemia (Hegarty et al., 2016; Weston et al., 2016).
Probiotics supplementation during neonatal period
Newborn, and especially preterm, babies have immature intestines free of normal commensal bacteria that would normally protect them from developing NEC and sepsis by inhibiting the growth of pathogenic bacteria in the intestines (AlFaleh & Anabrees, 2014; Patel & Denning, 2015; Rao et al., 2016). Probiotics are used to proactively colonize the intestines with beneficial bacteria such as Lactobacillus species (Millar et al., 2003; Patel & Denning, 2015). Probiotics therefore reduce the growth of pathogenic bacteria which would otherwise increase the risk of NEC and sepsis. Also probiotics promote gut immunity by increasing IgA levels and contributing to improved mucosal barrier function (Patel & Denning, 2015). These protective mechanisms reduce intestinal permeability by producing a protective mucosal barrier against bacteria and increase the production of anti-inflammatory cytokines (Deshpande et al., 2017; Millar et al., 2003). Probiotics are especially protective in preterm babies with immature intestinal microbiomes and neonates on antibiotics; antibiotics may reduce bacterial diversity in the intestine and thus also dispose to colonization by pathogenic bacteria causing NEC. Prebiotics and probiotics can be given together in the form of a synbiotic to improve the gut flora and can potentially reduce all-cause neonatal mortality (Johnson-Henry et al., 2016; Panigrahi et al., 2017). Probiotics are considered safe; however, there are concerns regarding probiotic supplementation in extremely premature or immunocompromised neonates. A few cases of neonatal sepsis have been reported that were thought to be caused by probiotics (Dani et al., 2016).
Why it is important to do this review
Neonatal vitamin A supplementation
Randomized trials on neonatal vitamin A supplementation have produced conflicting results with some studies (mostly from South Asia) showing a mortality benefit while no major benefit in other studies (mostly from Africa) (Haider et al., 2017) and some studies showing even an increased risk of infant mortality in certain populations (Smith et al., 2016).The exact reason for this difference in results is not clear. Previous reviews (Haider et al., 2017; Gogia & Sachdev, 2009) and a WHO technical consultation (WHO, 2009b) have hypothesized on what factors may explain these varied results. Our group has previously published a Cochrane review on the evidence on neonatal vitamin A supplementation (Haider & Bhutta, 2011), and we wanted to update the previous review. The previous review included studies conducted in the community setting. In this review, we considered studies conducted in both the community and the hospital setting in LMIC. We also included neurodevelopment outcomes for this review that were not covered in the previous Cochrane review.
Oral dextrose gel supplementation during neonatal period
Oral dextrose gel has been studied in the prevention and treatment of neonatal hypoglycaemia in high-income countries (Hegarty et al., 2017; Weston et al., 2016); however, it was not clear if similar studies were available from LMICs. Our objective was to consider both randomized and nonrandomized observational studies with a control arm. We hypothesized that the use of dextrose may be more beneficial in LMIC than in high-income countries, as the incidence of neonatal hypoglycaemia might be higher in these countries due to an increased rate of preterm and low birth weight birth.
Probiotics supplementation during neonatal period
The effect of probiotic supplementation for the prevention of NEC and neonatal sepsis has been assessed in previous reviews (AlFaleh & Anabrees, 2014; Rao et al., 2016; van den Akker et al., 2018). Most of these reviews included studies from both high- and LMICs. Deshpande et al. (2017) reviewed studies from LMIC where neonates were supplemented with probiotics. More studies (Amini et al., 2017; Chowdhury et al., 2016; Guney-Varal et al., 2017; Hernández-Enríquez et al., 2016; Hussain et al., 2016) have been published since the publication of Deshpande et al.'s (2017) review. Overall, our objective was to assess the current evidence for the effect of probiotic supplementation during the neonatal period in the hospital and community setting in LMIC.
OBJECTIVES
Primary objectives
To determine the efficacy of the following interventions on neonatal morbidity and mortality: Synthetic vitamin A supplementation, Oral dextrose gel supplementation, and Oral probiotic supplementation.
A detailed description of background and methods for this review was published in the form of a protocol as Imdad et al. (2019).
METHODS
Criteria for considering studies for this review
Types of studies
We included the following study designs: Randomized controlled trials (RCTs), where participants were randomly assigned either individually or in clusters to intervention and comparison groups. Cross-over designs were also eligible for inclusion. Quasi-experimental designs, which include: Natural experiments: studies where nonrandom assignment was determined by factors that were out of the control of the investigator. One common type includes allocation based on exogenous geographical variation. Controlled before-after studies (CBA), in which measures were taken of an experimental group and a comparable control group both before and after the intervention. We also require that appropriate methods were used to control for confounding, such as statistical matching (e.g., propensity score matching or covariate matching) or regression adjustment (e.g., difference-in-differences, instrumental variables). Regression discontinuity designs; here, allocation to intervention/control was based upon a cut-off score. Interrupted time series studies, in which outcomes were measured in the intervention group at at least three time points before the intervention and after the intervention.
Types of participants
Participants for this review included neonates (aged 0–28 days) from LMICs. We included neonates regardless of their health status. This includes low birth weight and preterm babies. However, studies that focused on neonates with congenital anomalies were excluded. We considered studies that included older age population groups in addition to neonates only if we could disaggregate relevant data for the neonatal population. For example, a study might include infants up to 6 months of age. We included such a study if the disaggregated data were available for neonates (0–28 days). Even though we planned to assess later childhood outcomes, we did not plan to include studies that recruited participants after the neonatal period.
Types of interventions
The following interventions were included in the review: Neonatal vitamin A supplementation compared to no supplementation or placebo: we considered only oral synthetic vitamin A supplementation. There was no restriction on the dosage and frequency of the medicine. The comparison group could include a placebo or standard of care. Oral dextrose gel supplementation during the neonatal period compared to no supplementation: we placed no limits on the dose or frequency of the dextrose supplementation. We only considered dextrose gel as the intervention and excluded dextrose given in other forms such as intravenous, nasogastric tube, or mixed with infant formula. The reason to exclude forms other than dextrose gel was that administration of dextrose in those forms may require special circumstances (like trained staff to place an IV) or special delivery vehicles, such as formula, that may not be available in LMIC. The comparison group included placebo or standard of care. Neonatal oral probiotics/synbiotics compared to no probiotic supplementation: probiotics are live microbial organisms that are given to promote the growth of commensal gut bacteria and prevent the growth of pathogenic bacteria. Prebiotics are dietary supplements that promote the growth of commensal bacteria. Synbiotics are a combination of prebiotics and probiotics (Millar et al., 2003; Patel & Denning, 2015). We placed no limits on the dose or frequency of probiotics. We included studies that used probiotics and synbiotics supplementation and excluded studies that used only prebiotics. Comparison groups included placebo or standard of care.
Each of the above interventions (i.e., vitamin A, dextrose, or probiotics) was summarized separately, and the interventions were not compared to each other directly or indirectly.
Types of outcome measures
Primary outcomes
The primary outcomes were: All-cause neonatal mortality (death between 0 and 28 days of life) All cause infant mortality at 6 months (death between 0 days and 6 months of life) All-cause infant mortality at 12 months (death between 0 days and 12 months life).
We anticipated that studies might not report the outcomes in the follow-up period mentioned above for the primary outcomes. If a study did not report mortality outcomes at day 28, 6 months, or 12 months, we contacted authors for data for the same. If segregated data were not available from authors, we included mortality data as follows: mortality in the first 6 weeks of life was included as neonatal mortality at day 28; between 3 and 6 months was included as 6 months, and between 9 and 12 months was included as 12 months. If the follow up was not clear, we included the mortality data at the longest follow-up.
Secondary outcomes
The secondary outcomes included: Sepsis-specific mortality measured between 0 and 28 days, 0 days and 6 months, and 0 days and 12 months of life Neonatal sepsis (as defined by authors) in the first 6 weeks of life NEC as defined by authors VAD Prevention of Hypoglycemia (as defined by authors) during the neonatal period Treatment of Hypoglycemia (recurrence of hypoglycaemia after the episode treated) Any adverse reactions during the intervention period Serious adverse events Neurodevelopmental outcomes at 12 and 24 months and at the longest follow-up.
The term neurodevelopment is a composite term that refers to cognitive, neurologic, and/or sensory outcomes. The term neurodevelopment may include intellectual disability as measured on the Mental Developmental Index of the Bayley Scales of Infant Development; gross motor delay measured on Gross Motor Function Classification System, and hearing and vision loss requiring amplification devices.
In order to be eligible for inclusion in the review, a study should have reported at least one of the primary or secondary outcomes. This was assessed at the full-text review stage.
Duration of follow-up
We included all participants in eligible studies that had outcomes of interest measured. There were no restrictions based on the duration of exposure, duration of follow-up, or timing of the outcome measurement. If the duration of treatment exceeded the neonatal period (i.e., 28 days), we considered another 2 weeks maximum but did not include studies in which the treatment went beyond 6 weeks of supplementation. We included mortality outcomes measured at 28 days, 6 months, 12 months of life, and at the longest follow-up as reported by authors.
Type of settings
We included studies conducted in LMIC. Low-income countries were defined as those with a gross national income (GNI) per capita of USD 1005 or less in 2016, and middle-income economies were those with a GNI per capita between USD 1006 and 3955 in 2016 (World Bank, 2017).
Search methods for identification of studies
The identification of studies included various methods, such as electronic and other sources. We did not exclude any based on the outcome at the screening stages.
Electronic searches
The electronic search for relevant studies was done in the following databases: PubMed, CINAHL, LILACS, SCOPUS, and CENTRAL (Cochrane Central Register for Controlled Trials).
Appendix 1 gives the search strategy for PubMed, CINAHL, LILACS, SCOPUS, and CENTRAL. It includes keywords and MeSH terms as appropriate. This approach includes a search strategy for the population (neonates) and interventions of interest. We planned to run searches for each intervention separately. We first ran the search for the population, which is the same for each intervention. Then we ran the search for each intervention. We then combined both searches by using “AND” and kept the searches in a separate EndNote file.
An example of a search strategy for vitamin A for PubMed was as follows:
(((((“Vitamin A”[Mesh]) OR (Vitamin A[tiab] OR Aquasol A[tiab] OR Retinol[tiab] OR All Trans Retinol[tiab] OR All-Trans-Retinol[tiab] OR Vitamin A1[tiab] OR Vitamin A 1[tiab] OR 11-cis-Retinol[tiab] OR 11 cis Retinol[tiab] OR Tretinoin[tiab])AND Supplement*[tiab]))AND ((“Infant”[Mesh] OR “Premature Birth”[Mesh]) OR (Neonat*[tiab] OR neo nat*[tiab]) OR (newborn* OR new Born*[tiab] OR newly born*[tiab]) OR (preterm[tiab] OR preterms[tiab] OR pre term[tiab] OR pre terms[tiab]) OR (premature*[tiab] AND (birth*[tiab] OR born[tiab] OR deliver*[tiab])) OR (low[tiab] AND (birthweight*[tiab] OR birth weight*[tiab])) OR (lbw[tiab] OR vlbw[tiab] OR elbw[tiab]) OR infant*[tiab] OR (baby[tiab] OR babies[tiab])))) NOT (“Animals”[Mesh] NOT (“Animals”[Mesh] AND “Humans”[Mesh]))
We applied restriction of “humans” to searches. We did not apply any restrictions on searches based on outcomes, study design, or language. There was no restriction on date of publication.
The searches were conducted for vitamin A on December 10, 2018 (updated on November 13, 2019); probiotics on February 8, 2019 (updated on November 27, 2019); and dextrose on April 25, 2019 (updated on November 26, 2019).
Searching other resources
Other resources included the search for ongoing trials at www.clinicaltrials.gov and WHO's ICTRP trials database. We also searched websites of international agencies such as WHO (including WHO's Reproductive Health Library), UNICEF, Global Alliance for Improved Nutrition (GAIN), International Food Policy Research Institute, International Initiative for Impact Evaluation (3ie), Nutrition International (NI), World Bank, USAID and USAID affiliates (e.g., FANTA, SPRING), and the World Food Programme.
Grey literature search sources included NI, GAIN, International Food Policy and Research Institute (IFPRI), and the WHO library database (WHOLIS).
We searched the reference lists of all included studies. We did citation searches of included studies in Google Scholar and Web of Science. We also searched the reference sections of previously published systematic reviews and the latest published studies. We contacted the experts and authors of the newest published studies to ask about any additional studies. Duplicates were removed.
Data collection and analysis
Selection of studies
Two authors independently screened titles/abstracts using prespecified inclusion/exclusion criteria. A full text was reviewed for the studies selected in the initial screening, and the same inclusion/exclusion criteria were applied. If there was a conflict about the inclusion of a study between the two reviewers, a third reviewer (ZAB) was consulted. We used a web-based software “Covidence” (Covidence, 2019) to do both title/abstract and full-text screening. This software allows simultaneous independent screening of studies, and inter-reviewer reliability can be assessed by checking the number of conflicts in the resolved conflict page following each stage of screening.
Description of methods used in primary research
We expected that the majority of the included studies would be randomized or cluster-randomized. We extracted the information on study design explicitly and made a careful differentiation between experimental and observational studies. We aimed to analyze randomized and nonrandomized studies separately.
Criteria for determination of independent findings
We anticipated that authors might report the results of a study in multiple publications. We coded such trials as a single study to avoid double counting of the data and included all the relevant outcomes decided a priori for this review. If a pilot study was done before the larger study, we included the two studies separately unless the data from the pilot study was included in the main trial. When a clinical trial registration number was available for a study, we searched that number on PubMed to locate all the published studies linked to that trial number.
Data extraction and management
Details of study coding categories
The data from included studies were abstracted into a standardized data abstraction form by two authors. We extracted data in duplicates, and any discrepancies were resolved by discussion firs. A third reviewer (ZAB) was consulted if the conflict existed after the initial discussion.
The data extraction sheet had the following information. General study information: authors, publication year, study design Study setting: World Bank region, country, World Bank income level, city/town, urban/urban slum/rural/mixed setting, duration of data collection, date of data collection Study population: sample size recruited, sample size analysed, female (%), description of participants (i.e., inclusion/exclusion criteria applied to recruitment) Intervention characteristics: type of intervention, duration of intervention, unit of randomization (where applicable), dose, frequency of provision, duration of follow up, attrition rate Quality assessment
Each quantitative outcome sheet contained the following: Subgroup (if applicable) Subgroup sample size Outcome type Outcome units Outcomes Outcome measure treatment group Outcome measure comparison group Standard deviation Effect size: Effect measure 95% CI
Assessment of ROB in included studies
We used the Cochrane ROB tool (Higgins & Green, 2011) for randomized studies. The Cochrane ROB tool includes the following items: Selection bias: random sequence generation and allocation concealment Performance bias: blinding of participants and personnel Detection bias: blinding of outcome assessment Attrition bias: incomplete outcome data Reporting bias: selective reporting Other sources of bias
Two authors independently performed the ROB assessments for each study. A third reviewer was involved to resolve any disagreements (ZAB). An overall score was not provided.
Measures of treatment effect
We performed a meta-analysis for the synthesis of quantitative data when the included studies had comparable participants, interventions, and outcomes. We did not assess the effect on outcome across the interventions, such as is done in network meta-analysis. Each intervention was analysed separately. We analysed continuous and dichotomous data separately. For dichotomous outcomes, results were presented as summary risk ratios with 95% CI. We combined risk ratios (events per child) and rate ratios (events per child year) for incidence data because of their similar interpretation and scale. For continuous outcomes, we presented the summary results as the mean difference with 95% CI when data were available on the same scale across the studies. We used the standardized mean difference with 95% CI when data were presented in different scales across the studies.
To avoid reviewer bias, we planned to predetermine the preference for specific data for certain outcomes. For example, for mortality outcomes, we gave preference to denominators in the following order: number with the definite outcome known, number randomized, and child-years. For morbidity data such as neonatal sepsis where both survivors and nonsurvivors might have contributed data, we gave preference to child years, number with the definite outcome known, and number randomized. For randomized trials, we gave preference to data that required the least manipulation by authors or inference by reviewers. We extracted the raw values (e.g., means and SDs) and built the intention-to-treat (ITT) analysis where applicable.
We anticipated that cause-specific morbidity or mortality data might not be readily available, as febrile illness due to respiratory, urinary, or central nervous system infection during the neonatal period are often categorized under a broader term of neonatal sepsis (WHO, 2017b).
Unit of analysis issues
As we planned to include multiple interventions, all interventions and outcomes within those interventions, were meta-analyzed separately.
For randomized trials, we meta-analyzed individual and cluster-randomized trials in the same analysis. We assessed analyses in the cluster-randomized trials to ensure that clustering was appropriately accounted for within the analysis of the primary study, such that study precision was not over or under-estimated within our analysis. If the authors adjusted for cluster randomization, no further adjustment was made. In case a cluster-randomized study was not adjusted by primary authors, we adjusted effect estimates by using the mean cluster size (M) and the intra-cluster correlation coefficient (ICC) to calculate the design effect as follows: design effect = 1 + (M − 1) ICC. We then used the design effect to adjust the study data such that a trial was reduced to its effective sample size or standard error of the summary estimate was inflated. We used the ICC given in the published studies. If the ICC was not available from the published study, we contacted the authors for the same. If the ICC was not available from the authors, we used ICC from the similar studies done in the similar region and on a similar population or took it from the previously published reviews (Haider et al., 2017).
Multiple-arm trials
We included studies with multiple intervention arms, but we only included the arms that were eligible for the review. We selected one pair (with appropriate intervention and control group) that satisfied the inclusion criteria of the review and excluded the rest. In case there were more than two groups eligible for inclusion, we combined these groups into a single pair-wise comparison. In multiple-arm trials using two different doses of the same intervention, we combined the two groups to avoid double counting the participants in the control group.
Dealing with missing data
Any missing data were noted including loss to follow-up and dropouts. The reasons for the missing data were taken from the studies, and if it was not mentioned in the studies, the authors were contacted for the same. If the authors reported the adjusted values for missing data, we used the adjusted values.
Assessment of heterogeneity
Statistical heterogeneity was assessed using τ 2, I 2, and significance of the χ 2 test. We also assessed statistical heterogeneity by visually inspecting the forest plots.
Assessment of reporting biases
A funnel plot and its symmetry were used to assess publication bias if the number of included studies for intervention was more than 10. If the funnel plot was suggestive of publication bias, we further investigated the publication bias with the use of Egger's test (Higgins & Green, 2011).
Data synthesis
Synthesis procedures and statistical analysis
We used the software Review Manager 5.3 (Review Manager, 2019) to conduct the statistical analysis. For randomized trials, we followed the ITT analysis. If ITT was not available, and the author reported the analyses as specified in the protocol, we reconstructed the data to create an ITT analysis.
We used a random-effect model to account for expected heterogeneity in the intervention, comparisons, or setting within studies included in a given synthesis. We used the generic inverse variance method of meta-analysis for fixed effect models and random effect models. This method of meta-analysis gives weight to studies based on their variance in a way that a study with low variance gets a high weight and vice versa.
We interpreted the results of the meta-analysis based on p value at the 95% confidence level (a value <0.05 was considered statistically significant) and reported both significant and nonsignificant results. For subgroup analysis, we used an interaction test to determine if there was a relevant difference in effect across subgroups.
We assessed the quality of overall evidence using the GRADE approach. This method of quality assessment considers study type, within-study ROB (methodological quality), directness of evidence, heterogeneity, precision of effect estimates, and risk of publication bias (Guyatt et al., 2011). We rated the quality of the body of evidence for each key outcome as “high,” “moderate,” “low,” or “very low.”
Subgroup analysis and investigation of heterogeneity
Neonatal vitamin A supplementation
Although we had planned a number of subgroup analyses for neonatal vitamin A supplementation; however, a recent IPD analysis (West et al., 2019) covered both individual and study level subgroup analyses, so we did not perform any subgroup analysis for vitamin A supplementation at this stage
Neonatal probiotic supplementation
Gestational age: term and preterm Strains used in probiotics: single strain versus multiple strain and of type of strain used in each probiotic Strains used in probiotics: contains Lactobacillus versus Bifidobacterium versus both Settings: community-based versus hospital setting Type of feedings: breastmilk versus formula milk versus mixed.
Oral dextrose gel supplementation
Gestational age: term and postterm versus late preterm (35–36 weeks) versus moderately preterm (30–34 weeks) versus extremely preterm (<30 weeks) Dose: equal or <200 mg/kg versus >200 mg/kg Frequency: one versus more than one dose Time of administration: ≤1 h of age versus after 1 h of age versus after 2 h of age.
Sensitivity analysis
High quality studies versus low quality studies. The quality of study was subjectively based on the ROB assessment. Even though we considered all the domains included in the Cochrane ROB tool, we gave higher importance to sequence generation and allocation concealment, as most of the outcomes for this review were objective, and it was less likely that the results of the included studies would have been biased by a lack of blinding. Random versus fixed effect models. We chose this sensitivity analysis to assess if the summary estimates will change significantly based on use of random versus fixed effect model. There is no exact criterion to choose between the two models, and we wanted to make sure that estimates were not significantly different between the two models.
Treatment of qualitative research
We did not plan to include qualitative research.
Summary of findings and assessment of the certainty of the evidence
Summary of findings' tables
We constructed “Summary of findings” tables for all of the primary outcomes using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria (GRADEpro GDT 2015). These covered consideration of within-study ROB (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias. We rated the certainty of evidence for each key outcome as “high,” “moderate,” “low,” or “very low.” The GRADE evidence is described in Table 1. Nonrandomised studies were initially rated as “low” quality. If there were no serious methodological flaws, we upgraded the evidence for studies with a large magnitude of effect; presence of a dose response relationship; and effect of plausible residual confounding.
Effect of probiotic supplementation during neonatal period: Subgroup analysis
We used GRADE and prepared the summary of findings tables for the following primary outcomes: Stillbirth defined as baby born with no signs of life at or after 28 weeks' gestation Perinatal mortality (stillbirth and deaths ≤7 days) Neonatal mortality (death < 28 days) Infant mortality (deaths between 0 and 12 months) Under-five mortality (deaths between 0 and 59 months) Miscarriage Mean maternal body mass index
RESULTS
Description of studies
Results of the search
Figure 1 shows the PRISMA flow diagram for our literature search.
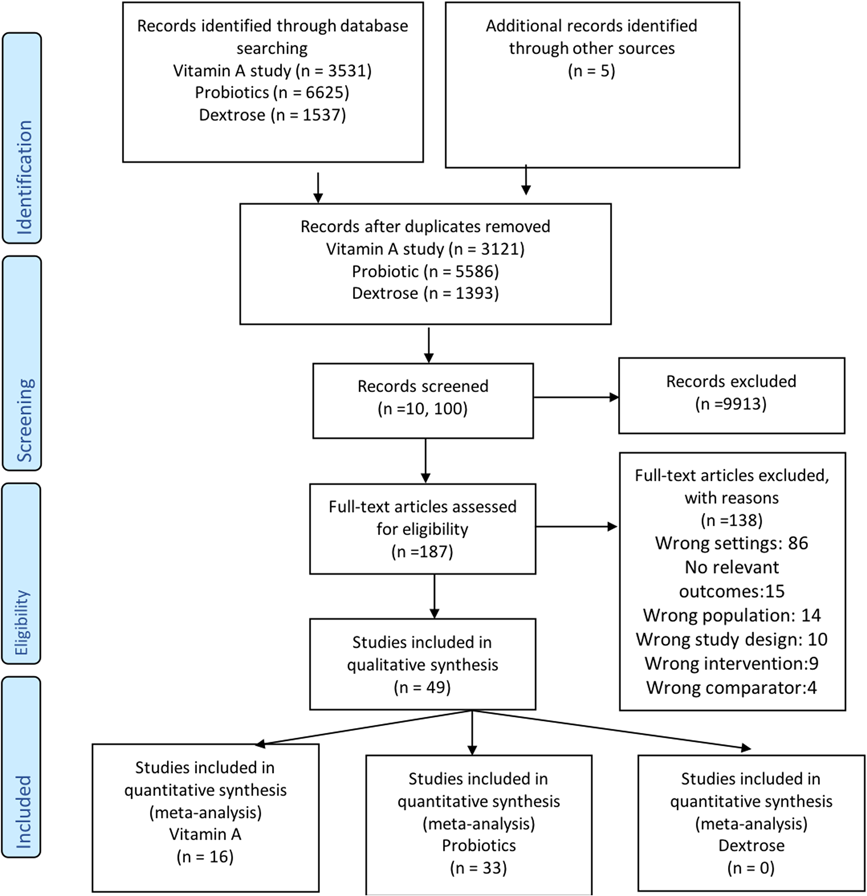
PRISMA flow diagram
Vitamin A supplementation during neonatal period
Sixteen studies reported in 45 publications assessed the effect of neonatal vitamin A supplementation (Ahmad et al., 2019; Basu et al., 2019; Benn et al., 2008, 2010, 2014; Edmond et al., 2015; Giridhar et al., 2019; Humphrey et al., 1996; Klemm et al., 2008; Malaba et al., 2005; Masanja et al., 2015; Mazumder et al., 2015; Rahmathullah et al., 2003; Soofi et al., 2017; Sun et al., 2019; West et al., 1995). These studies included a total of about 16,366 participants. All the studies were RCTs and published in a peer-reviewed journal.
Dextrose gel supplementation during neonatal period
We did not identify any studies that assessed the use of dextrose gel supplementation during neonatal period for prevention or treatment of hypoglycaemia in LMIC.
Probiotic supplementation during neonatal period
Thirty-three studies reported in 37 publications evaluated the effect of probiotic supplementation during the neonatal period and included a total of 11,595 participants (probiotics, 5854 and controls, 5741; Amini et al., 2017; Braga et al., 2011; Chowdhury et al., 2016; Cooper et al., 2017; Cui et al., 2019; Dashti et al., 2014; Demirel et al., 2013; Dilli et al., 2015; Dongol Singh et al., 2017; Dutta et al., 2015; Fernández-Carrocera et al., 2013; Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Hussain et al., 2016; Kaban et al., 2019, Mazumder et al., 2015; Nandhini et al., 2016; Guney-Varal et al., 2017; Oncel et al., 2014; Panigrahi et al., 2017; Rojas et al., 2012; Roy et al., 2014; Samanta et al., 2009; Shashidhar et al., 2017; Sinha et al., 2015; Sari et al., 2011; Serce et al., 2013; Shadkam et al., 2015; Saengtawesin et al., 2014; Tewari et al., 2015; Xu et al., 2016).
Three of the studies were available in the form of abstracts (Hariharan et al., 2016; Huaxian, 2013; Rehman et al., 2018). The rest of the studies were published in a peer-reviewed journal.
Included studies
The characteristics of included studies are available in the table Characteristics of included studies.
Vitamin A supplementation during neonatal period
Type of studies
All the included studies were RCTs. Thirteen studies were individually randomized (Ahmad et al., 2019; Basu et al., 2019; Benn et al., 2008, 2010, 2014; Edmond et al., 2015; Giridhar et al., 2019; Humphrey et al., 1996; Malaba et al., 2005; Masanja et al., 2015; Mazumder et al., 2015; Rahmathullah et al., 2003), and three studies were cluster-randomized (Klemm et al., 2008; Soofi et al., 2017; Sun et al., 2019; West et al., 1995). Three trials had multiple arms of interventions (Benn et al., 2010, 2014; Malaba et al., 2005).
Country
Studies were conducted in 10 different countries with four studies conducted in India (Basu et al., 2019; Giridhar et al., 2019; Mazumder et al., 2015; Rahmathullah et al., 2003), three studies in Guinea-Bissau (Benn et al., 2008, 2010, 2014), two studies in Bangladesh (Ahmad et al., 2019; Klemm et al., 2008), and one each in China (Sun et al., 2019), Ghana (Edmond et al., 2015), Indonesia (Humphrey et al., 1996), Nepal (West et al., 1995), Pakistan (Soofi et al., 2017), Tanzania (Masanja et al., 2015), and Zimbabwe (Malaba et al., 2005).
Settings
Thirteen studies were conducted in the community setting, while three studies were conducted in the hospital setting (Basu et al., 2019; Giridhar et al., 2019; Sun et al., 2019).
Participants
Most of the studies included live born infants who were otherwise healthy. One study included only low birth weight babies (Benn et al., 2010), two studies included newborns with very low birth weight (Basu et al., 2019; Giridhar et al., 2019), and one study included extremely premature babies (Sun et al., 2019). The sample size of each study ranged from 120 (Giridhar et al., 2019) to 44,948 (Mazumder et al., 2015).
Dose
Most of the included studies for the use of neonatal vitamin A supplementation used a dose of 50,000 IU. Rahmathullah et al. (2003) gave 24,000 IU daily, and Benn et al. (2010) used 25,000 IU. Benn et al. (2014) compared doses of 50,000 IU versus 25,000 IU. Basu et al. (2019) used a daily dose of 1,500 IU.
Comparison
In all the included studies for neonatal vitamin A supplementation a placebo was given to the control group.
Probiotic supplementation during neonatal period
Type of studies
All the studies that evaluated the effect of probiotic supplementation during the neonatal period were individual RCTs. Two studies had multiple intervention groups (Dilli et al., 2015; Dutta et al., 2015). One of these studies compared different combinations of probiotics with prebiotics (Dilli et al., 2015), and the other study compared different doses of probiotics (Dutta et al., 2015). For the study by Dilli et al. (2015), we included the data in a way that the only difference between the two groups was probiotics. For the study by Dutta et al. (2015), we combined all the groups that compared different doses and compared them with the placebo to avoid double-counting of the placebo group data.
One study included neonates with and without exposure to human immunodeficiency virus (HIV; based on maternal history of HIV). We included the data for these groups separately in the meta-analysis (Niekerk et al., 2015 (HIV exposed); Niekerk et al., 2015 (HIV nonexposed).
Country
Studies were conducted in 13 different countries with 10 studies conducted in India (Dutta et al., 2015; Hariharan et al., 2016; Mazumder et al., 2015; Nandhini et al., 2016; Panigrahi et al., 2017; Roy et al., 2014; Samanta et al., 2009; Shashidhar et al., 2017; Sinha et al., 2015; Tewari et al., 2015), six studies in Turkey (Demirel et al., 2013; Dilli et al., 2015; Guney-Varal et al., 2017; Oncel et al., 2014; Sari et al., 2011; Serce et al., 2013), three studies each in China (Cui et al., 2019; Huaxian, 2013; Xu et al., 2016) and Iran (Amini et al., 2017; Dashti et al., 2014; Shadkam et al., 2015), two each in Mexico (Fernández-Carrocera et al., 2013; Hernández-Enríquez et al., 2016) and South Africa (Cooper et al., 2017; Niekerk et al., 2015 (HIV exposed)), and one each in Bangladesh (Chowdhury et al., 2016), Brazil (Braga et al., 2011), Colombia (Rojas et al., 2012), Indonesia (Kaban et al., 2019), Nepal (Dongol Singh et al., 2017), Pakistan (Hussain et al., 2016), and Thailand (Saengtawesin et al., 2014).
Settings
All the studies were conducted in the hospital setting except for three studies where participants were followed in the community setting (Cooper et al., 2017; Dongol Singh et al., 2017; Panigrahi et al., 2017).
Participants
Only one study (Cooper et al., 2017) included neonates that were full term. The rest of the studies included participants that were either low birth weight, preterm, or both. The participants were recruited from neonatal intensive care units except in three studies (Cooper et al., 2017; Dongol Singh et al., 2017; Panigrahi et al., 2017), where participants were recruited from the community.
The intervention
Thirteen studies used a single strain of probiotics (Cui et al., 2019; Demirel et al., 2013; Dongol Singh et al., 2017; Hernández-Enríquez et al., 2016; Hussain et al., 2016; Kaban et al., 2019; Oncel et al., 2014; Rojas et al., 2012; Roy et al., 2014; Serce et al., 2013; Shadkam et al., 2015; Tewari et al., 2015; Xu et al., 2016), and 13 studies used a preparation that contained multiple strains of probiotics (Amini et al., 2017; Braga et al., 2011; Chowdhury et al., 2016; Dashti et al., 2014; Dutta et al., 2015; Fernández-Carrocera et al., 2013; Hariharan et al., 2016; Niekerk et al., 2015 (HIV exposed); Roy et al., 2014; Saengtawesin et al., 2014; Samanta et al., 2009; Shadkam et al., 2015; Sinha et al., 2015). Five studies used a preparation that had a probiotic + prebiotic (synbiotic) (Cooper et al., 2017; Dilli et al., 2015; Guney-Varal et al., 2017; Nandhini et al., 2016; Panigrahi et al., 2017); among these five studies, three studies (Cooper et al., 2017; Dilli et al., 2015; Panigrahi et al., 2017) used a probiotic preparation that had a single strain of bacteria, and the other two studies used a preparation that had multiple strains of bacteria (Guney-Varal et al., 2017; Nandhini et al., 2016). One study did not report the strain of probiotic supplementation (Huaxian, 2013).
Ten studies used a probiotic preparation that contained Lactobacillus (Cooper et al., 2017; Cui et al., 2019; Dongol Singh et al., 2017; Hernández-Enríquez et al., 2016; Kaban et al., 2019; Oncel et al., 2014; Panigrahi et al., 2017; Rojas et al., 2012; Roy et al., 2014; Shadkam et al., 2015), and two studies used a preparation that contained Bifidobacterium (Dilli et al., 2015; Hussain et al., 2016). Fourteen studies used a preparation that had both Lactobacillus and Bifidobacterium (Amini et al., 2017; Braga et al., 2011; Chowdhury et al., 2016; Dashti et al., 2014; Fernández-Carrocera et al., 2013; Guney-Varal et al., 2017; Hariharan et al., 2016; Nandhini et al., 2016; Niekerk et al., 2015 (HIV exposed); Roy et al., 2014; Saengtawesin et al., 2014; Samanta et al., 2009; Shashidhar et al., 2017; Sinha et al., 2015). Three studies used Saccharomyces boulardii (Demirel et al., 2013; Serce et al., 2013; Xu et al., 2016), and one study used Bacillus clausii (Tewari et al., 2015).
The probiotics were mostly given with breastmilk or formula feedings and started when the baby was able to tolerate minimal enteral feeds. The duration and dose of probiotic supplementation varied among the studies.
Comparison
Sixteen studies used a placebo (Cui et al., 2019; Dashti et al., 2014; Demirel et al., 2013; Dilli et al., 2015; Dongol Singh et al., 2017; Dutta et al., 2015; Kaban et al., 2019; Niekerk et al., 2015 (HIV exposed); Oncel et al., 2014; Panigrahi et al., 2017; Rojas et al., 2012; Roy et al., 2014; Serce et al., 2013; Shadkam et al., 2015; Sinha et al., 2015; Tewari et al., 2015); the rest of the studies used a control group receiving standard of care only.
Outcomes
All the studies reported data for at least one outcome that could be included in the meta-analysis. Twenty five studies reported data for all-cause mortality, 29 studies reported data for NEC, and 21 studies reported data for the incidence of neonatal sepsis. See Section 5.3 for more details.
Excluded studies
Overall, 138 studies were excluded. See the Characteristics of excluded studies for reasons for exclusion of studies.
Among excluded studies, 86 studies were excluded because of the wrong settings, and most of these studies were conducted in high-income countries. Fifteen studies were excluded because no relevant clinical outcomes were available from the abstract or full text of the studies. Fourteen studies were excluded for the wrong population, and 10 studies were excluded because of the wrong study design. Nine studies had a wrong intervention, and four studies had a wrong comparator.
ROB in included studies
Vitamin A supplementation during the neonatal period
Figure 2 shows the ROB in the 16 included studies that addressed vitamin A supplementation during the neonatal period.
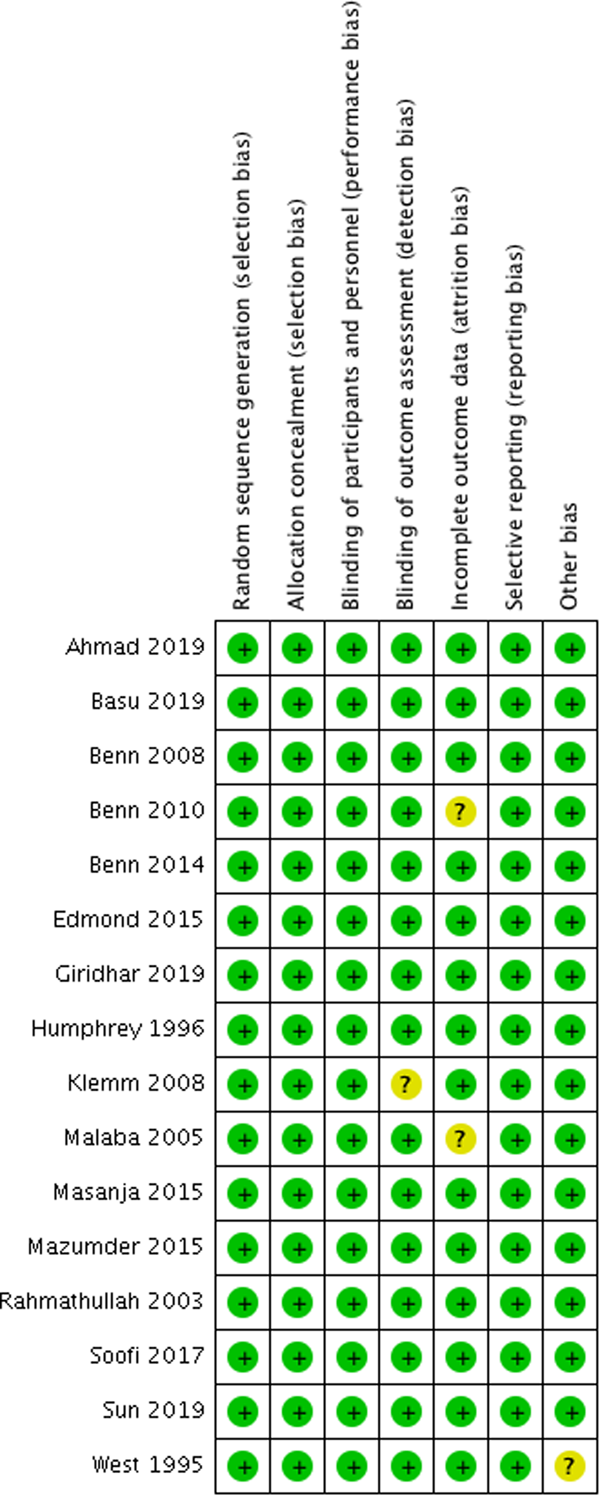
Risk of bias: neonatal vitamin A supplementation
Probiotic supplementation during the neonatal period
Figure 3 show the ROB in the 33 included studies that addressed probiotic supplementation during the neonatal period.
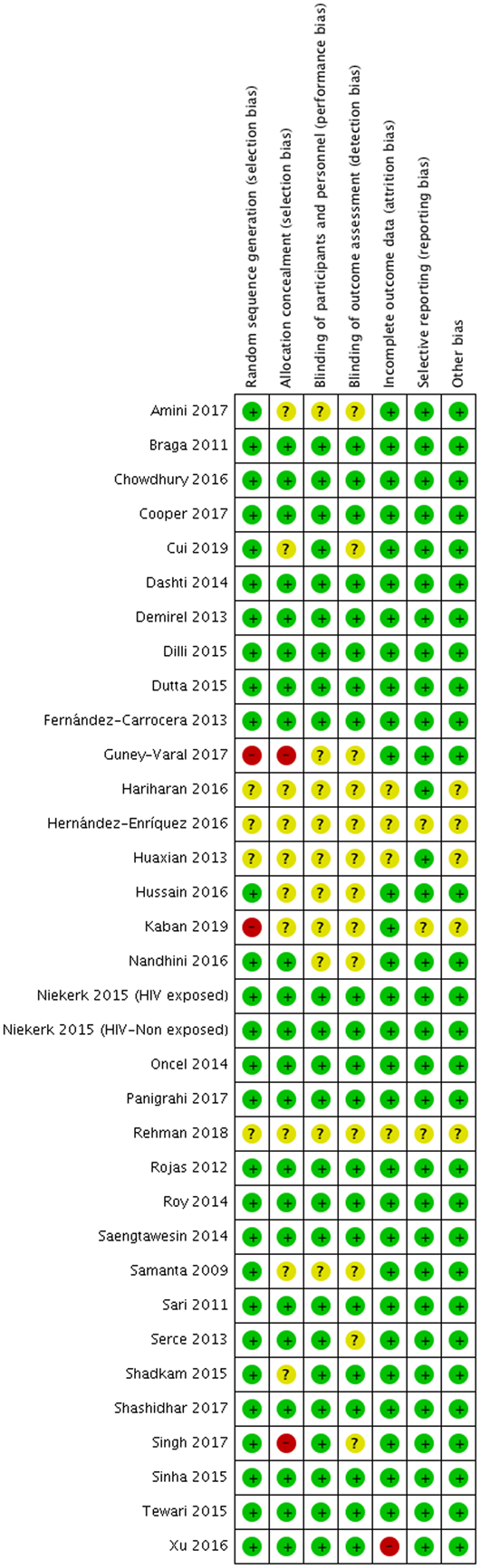
Risk of bias: probiotic supplementation during neonatal period
Allocation (selection bias)
Vitamin A supplementation during the neonatal period
All the studies for vitamin A supplementation were at low ROB for sequence generation and allocation concealment.
Probiotic supplementation during the neonatal period
Two studies were judged to be at high ROB due to inadequate randomization (Guney-Varal et al., 2017; Kaban et al., 2019), and four studies did not provide enough information to allow a judgment about methods of randomization; these were labelled as having an unclear ROB (Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Rehman et al., 2018). The rest of the studies had a low ROB for sequence generation.
Two studies were considered at high ROB due to inability to conceal the allocation (Dongol Singh et al., 2017; Guney-Varal et al., 2017). Ten studies had an unclear ROB, as these studies did not provide enough information to assess methods of allocation concealment (Amini et al., 2017; Cui et al., 2019; Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Hussain et al., 2016; Kaban et al., 2019, Rehman et al., 2018; Samanta et al., 2009; Shadkam et al., 2015). The rest of the studies had a low ROB for allocation concealment.
Blinding (performance bias and detection bias)
Vitamin A supplementation during neonatal period
None of the included studies for neonatal vitamin A supplementation was at increased ROB for blinding.
Probiotic supplementation during neonatal period
Ten studies had an unclear ROB due to blinding of the participants (Amini et al., 2017; Guney-Varal et al., 2017; Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Hussain et al., 2016; Kaban et al., 2019; Nandhini et al., 2016; Rehman et al., 2018; Samanta et al., 2009). The rest of the studies had a low ROB due to the inability to do blinding of the participants.
Thirteen studies had an unclear ROB for blinding of the outcome assessors (Amini et al., 2017; Cui et al., 2019; Dongol Singh et al., 2017; Guney-Varal et al., 2017; Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Hussain et al., 2016; Kaban et al., 2019; Nandhini et al., 2016; Rehman et al., 2018; Serce et al., 2013; Samanta et al., 2009). The rest of the studies had a low ROB.
Incomplete outcome data (attrition bias)
Vitamin A supplementation during the neonatal period
All studies were at low risk for attrition bias except two studies that had an unclear ROB (Benn et al., 2010; Malaba et al., 2005).
Probiotic supplementation during the neonatal period
Most of the studies had a minimal loss to follow-up. One study was at high ROB where more than 20% of the participants were lost to follow-up (Xu et al., 2016). Four studies had an unclear ROB, as there was not enough information to make an assessment in these studies (Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Rehman et al., 2018).
Selective reporting (reporting bias)
Vitamin A supplementation during neonatal period
All studies were considered to have low ROB for selective outcome reporting.
Probiotic supplementation during neonatal period
Most of the studies reported all relevant outcomes, and we did not consider any particular study at high ROB. Three studies had unclear ROB for selective outcome reporting (Hernández-Enríquez et al., 2016; Kaban et al., 2019; Rehman et al., 2018).
Other potential sources of bias
Vitamin A supplementation during neonatal period
No study was considered at high ROB due to other reasons.
Probiotic supplementation during neonatal period
No other major source of ROB was noted. Five studies had unclear ROB due to limited available information (Hariharan et al., 2016; Hernández-Enríquez et al., 2016; Huaxian, 2013; Kaban et al., 2019; Rehman et al., 2018).
Effects of interventions
VItamin A supplementation during neonatal period
All-cause mortality during the neonatal period
Five studies from community settings reported the effect of vitamin A supplementation on all-cause neonatal mortality. These combined results showed no significant difference between the intervention and the control group (RR, 0.99; 95% CI, 0.90–1.08; six studies, 126,548 participants, heterogeneity: τ 2 = 0.00; χ 2 = 3.64, (p = 0.46); I 2 = 0%). The grade rating for this outcome was “high.” Summary of findings Table 2.
Vitamin A compared to placebo for neonatal health
Abbreviations: CI, confidence interval; OR, odds ratio; RR, risk ratio.
Sensitivity analysis: Fixed effect model
Use of a fixed effect model did not change the summary estimate for neonatal mortality (RR, 0.99; 95% CI, 0.90–1.08).
All-cause mortality at 6 months
Twelve studies from community settings reported the data for the effect of neonatal vitamin A supplementation on all-cause mortality at 6 months. The combined results showed no difference between the intervention and control group (RR, 0.98; 95% CI, 0.89–1.07; 12 studies, 154,940 participants; heterogeneity: τ 2 = 0.01; χ 2 = 19.14, (p = 0.06); I 2 = 43%). The Grade rating for this outcome was “high.” Summary of findings Table 2. A funnel plot for publication bias was symmetrical.
Sensitivity analysis: Fixed effect model
Use of a fixed effect model led to minimal change in the summary estimate (RR, 0.97; 95% CI, 0.91–1.03).
All-cause mortality at 12 months
Eight studies from community settings reporting on the impact of neonatal vitamin A supplementation reported data for all-cause mortality at 12 months (RR, 1.04; 95% CI, 0.94–1.14; eight studies, 118,376 participants; Heterogeneity: τ 2 = 0.01; χ 2 = 12.99, df = 7 (p = 0.07); I 2 = 46%]. We rated this evidence as high certainty Summary of findings Table 2.
Sensitivity analysis: Fixed effect model
Use of a fixed effect model did not change the summary estimate significantly (RR, 1.02; 95% CI; 0.96–1.08).
Three studies from hospital settings also reported data on mortality. The time to event for mortality was not clear in these studies. We did not pool data from the hospital-based studies with other studies, as the community-based studies had participants that were very different from hospital-based studies. We briefly describe the results of these studies below.
A study by Basu et al. (2019) reported the primary outcome; this was a composite incidence of all-cause mortality and oxygen requirement for 28 days. The results showed a reduction in mortality in the vitamin A group compared to the control group (RR, 0.44; 95% CI, 0.23–0.84).
No difference in mortality was reported by Sun et al. (2019) in the Vitamin A group versus placebo (RR, 0.49; 95% CI, 0.45–5.32).
Similarly, no difference was noted in all-cause mortality by Giridhar et al. (2019) (RR, 2; 95% CI, 0.63–6.30).
Adverse outcomes: Bulging fontanelle
Six studies reported on the effect of neonatal vitamin A supplementation on incidence of bulging fontanelle. The combined results showed a 53% increased risk of bulging fontanelle in the intervention group compared to control (RR, 1.53; 95% CI, 1.12–2.09; heterogeneity: τ 2 = 0.08; χ 2 = 14.20, (p = 0.01); I 2 = 65%). We have high certainty in this evidence. Summary of findings Table 2.
Adverse outcomes: Vomiting
The combined results from six studies showed that neonatal vitamin A supplementation did not increase the risk of vomiting (RR, 1.00; 95% CI, 0.93–1.07; heterogeneity: τ 2 = 0.00; χ 2 = 3.90, (p = 0.42); I 2 = 0%).
Vitamin A deficiency
One study from the community setting (Benn et al., 2008) reported VAD at 6 weeks and 4 months post neonatal supplementation. No significant difference was noted between the two groups at 6 weeks (RR, 0.94; 95% CI, 0.75–1.19) or 4 months (RR, 1.02; 95% CI, 0.64–1.62).
Another study from the hospital setting (Giridhar et al., 2019) showed a significant decrease in VAD in the intervention group compared to control (RR, 0.09; 95% CI, 0.024–0.38).
Neurodevelopment outcomes
Two studies reported long-term neurodevelopmental outcomes after use of vitamin A supplementation during the neonatal period. As the outcomes measured and duration of follow up were different, we did not pool the studies.
Humphrey et al. (1996) reported on neurodevelopmental outcomes at 3 year follow-up after neonatal vitamin A supplementation by using Bayley Scales of Infant Development. The study authors analysed the data for children with (n = 91) and without (n = 432) bulging fontanelle who received vitamin A versus placebo. The results showed that neonatal vitamin A supplementation did not have any adverse effect on development in the presence or absence of bulging fontanelle. Neonatal vitamin A supplementation had a positive effect on all developmental scores. The reported developmental scores addressed developmental areas such as orientation-engagement, emotional regulation, and motor quality.
Klemm et al. (2008) reported data on neurodevelopmental outcomes 8 years after vitamin A supplementation. The authors followed a cohort of participants (n = 1613) who either directly received neonatal vitamin A or whose mother received vitamin A during pregnancy. The results showed no significant difference in intelligence, memory, and motor function; however, when the neonates and their mothers were supplemented with vitamin A versus placebo, it increased their performance in reading, spelling, and math computation.
Probiotic supplementation during the neonatal period
Data were available for the effect of probiotic supplementation for all-cause mortality, NEC, sepsis, and sepsis-specific mortality.
All-cause mortality at longest follow-up
Twenty-five studies that included 10,998 subjects (probiotics 5548, control 5450) reported data for all-cause mortality for the effect of probiotic supplementation on all-cause mortality. Our meta-analysis found a reduction of 20% in all-cause mortality in the probiotic group compared to control (RR, 0.80; 95% CI, 0.66–0.96; heterogeneity: τ 2 = 0.00; (p = 0.55); I 2 = 0%) (Figure 4). The number needed to treat was 100. The GRADE rating for this outcome was “high.” Summary of findings Table 3.
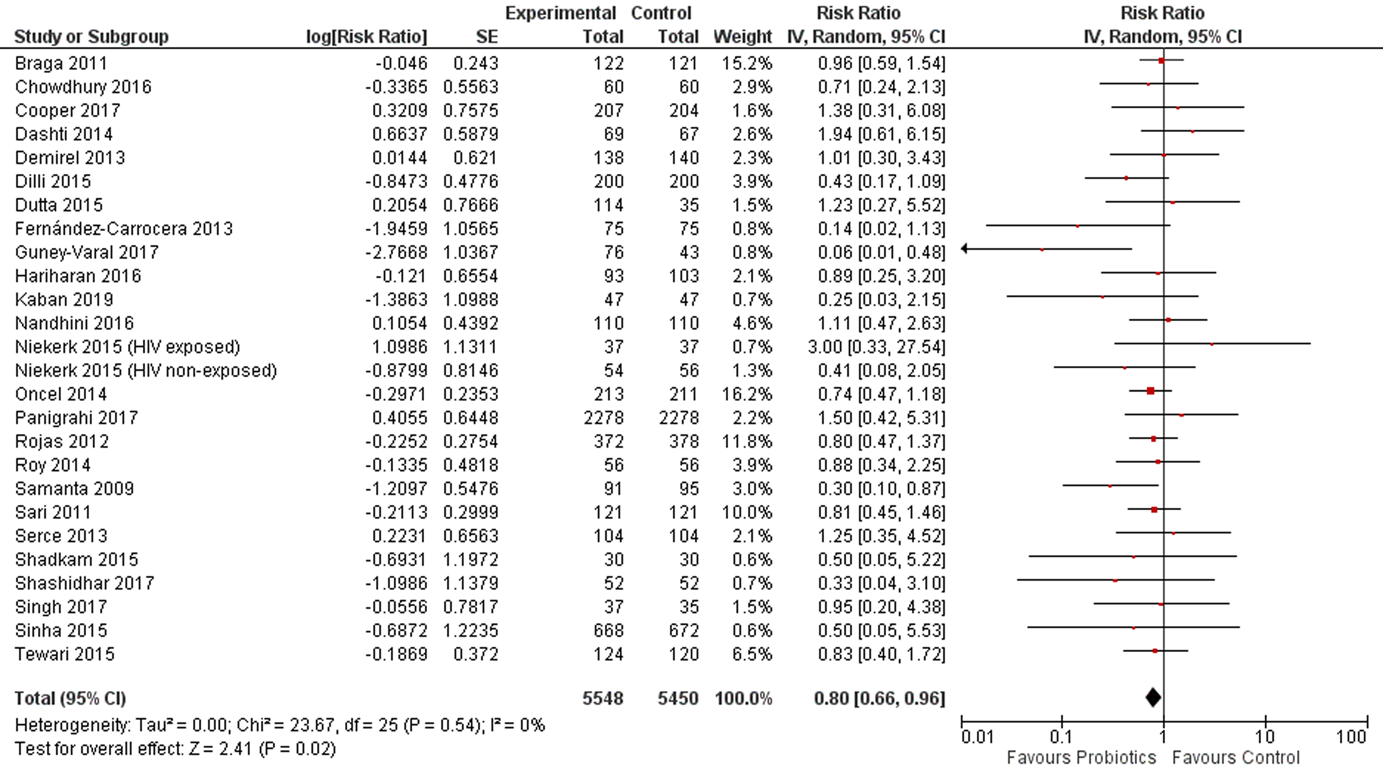
(Analysis 2.1) Forest plot of comparison: 2 probiotics versus control, outcome: 2.1 all-cause mortality
Probiotics supplementation during neonatal period
Even though three (Dongol Singh et al., 2017; Fernández-Carrocera et al., 2013; Kaban et al., 2019) of the included studies in the analysis had high ROB related to randomizations, the exclusion of these studies did not have much effect on the magnitude of the summary estimate or its statistical significance.
I 2 was 0%.
All-cause mortality is an objective outcome and there were no concerns about the indirect measurement of the outcome.
The confidence interval of the summary estimate did not include 1.
I 2 was 23% and the p. value for heterogeneity was 0.16.
The I 2 was 24%.
Publication bias
A funnel plot for publication bias looked symmetrical (Figure 5).
(Analysis 2.1) Funnel plot of comparison: 2 probiotics versus Control, outcome: 2.1 All-cause mortality
Subgroup analyses
Table 1 gives the summary of data for subgroup analyses. For the outcome of all-cause mortality, data were available to perform subgroup analyses based on settings (hospital vs. community-based studies), type of probiotics (single strains vs. multiple strain vs. synbiotic), type of participants (term vs. preterm/low birth weight), type of feeding (breastfeeding vs. formula feeding vs. mixed feeding), and probiotic preparation (preparation containing Lactobacillus vs. Bifidobacterium vs. both Lactobacillus and Bifidobacterium vs. S. boulardii). No significant difference was noted among the subgroups; however, the number of studies varied for each group within the subgroup analysis.
Sensitivity analysis
Random versus fixed effect models
Use of a fixed-effect model did not change the summary estimate for the effect of probiotics on all-cause mortality (RR, 0.80; 95% CI, 0.66–0.96; heterogeneity: χ 2 = 22.55, (p = 0.55); I 2 = 0%) Analysis 2.7.
Risk of bias
Exclusion of three studies (Dongol Singh et al., 2017; Fernández-Carrocera et al., 2013; Kaban et al., 2019) that were at high ROB for randomizations/allocation concealment did not change the summary estimate to a great extent, and results remained statistically significant Analysis 2.8.
Incidence of NEC
This outcome was reported by twenty-nine studies that included a total of 5574 (probiotics, 2843; control, 2731) participants. The combined results showed that the probiotics group had a relative reduction in NEC prevalence of 54% compared to control group (RR, 0.46; 95% CI, 0.35–0.59; heterogeneity: τ 2 = 0.11; (p = 0.12); I 2 = 24%) (Figure 6). The number needed to treat was 17. We have high certainty in this evidence. Summary of findings Table 3.
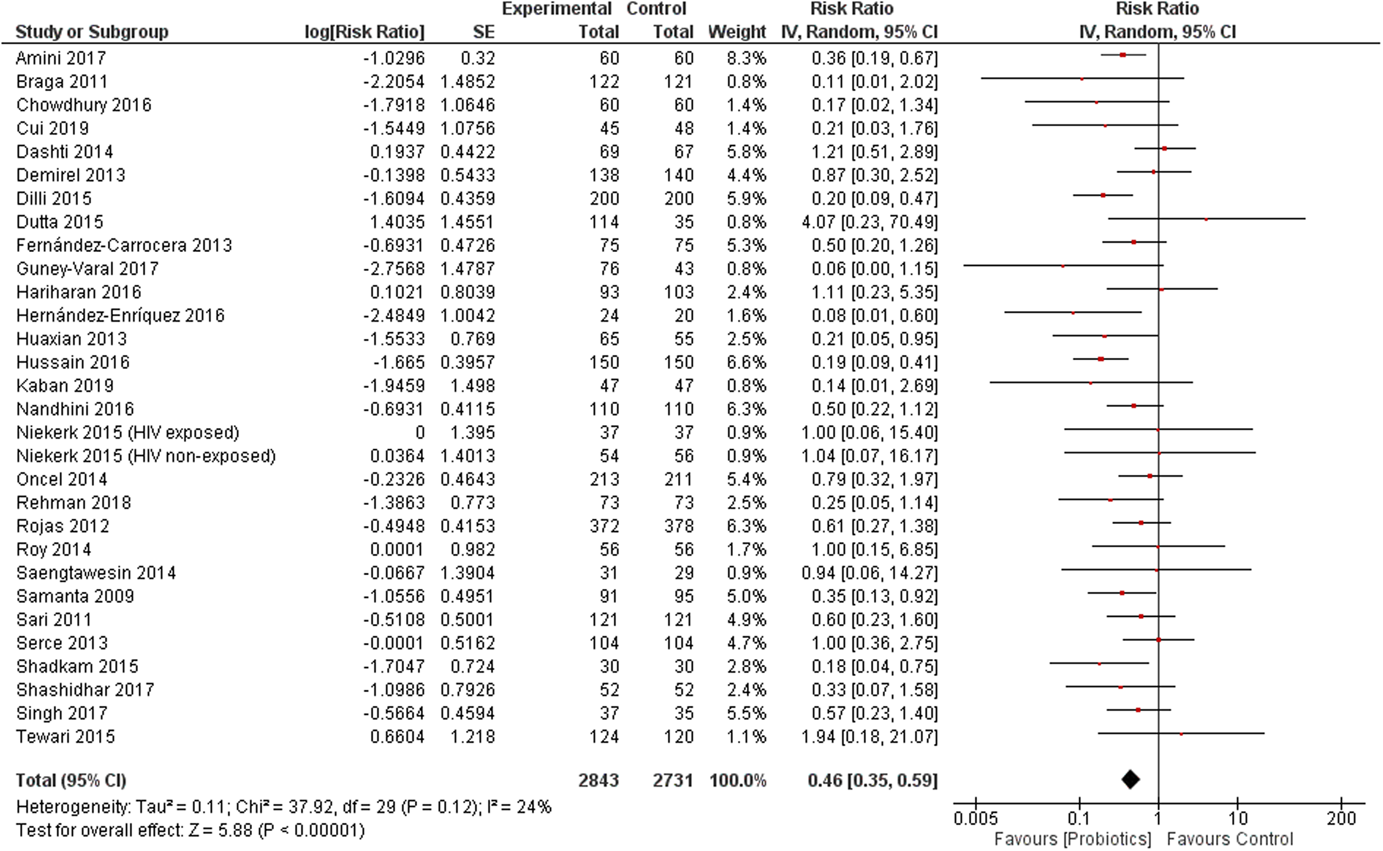
(Analysis 2.9) Forest plot of comparison: 2 probiotics versus control, outcome: 2.9 necrotizing enterocolitis (any type)
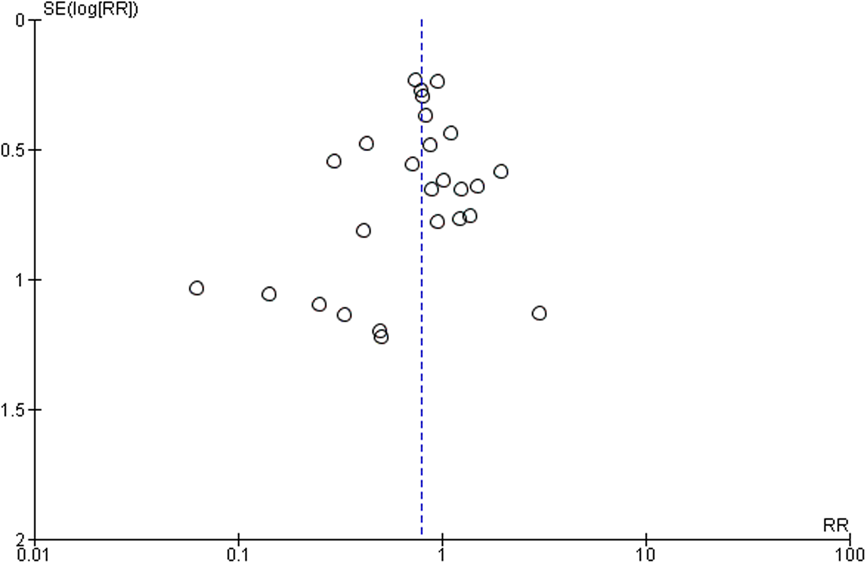
Publication bias
A funnel plot for publication bias looked symmetrical.
Subgroup analyses
Table 1 shows the results of subgroup analyses. For NEC, data were available to perform the following 3 subgroup analyses: type of probiotics (single strain vs. multiple strain vs. synbiotic), type of feeding (breastfeeding vs. formula feeding vs. mixed feeding), and probiotic preparation (preparation containing Lactobacillus vs. Bifidobacterium vs. both Lactobacillus and Bifidobacterium vs. S. boulardii). No significant difference was noted among the subgroup analyses except the one based on probiotics preparation (p value for subgroup difference 0.05). The probiotics preparation that has Lactobacillus in it, either as a single strain (RR, 0.39; 95% CI, 0.25–0.61; 13 studies) or in combination with Bifidobacterium (RR, 0.44; 95% CI, 0.36–0.68; 13 studies), had a significant effect compared to Bifidobacterim alone (RR, 0.20; 95% CI, 0.09, −0.47) or S. boulardii alone (RR, 0.94; 95% CI, 0.45–1.95; two studies). This subgroup analysis should be interpreted carefully, as the number of studies was not uniformly distributed among all the subgroups, and the statistical difference might be due to the small number of studies in two of the subgroups.
Sensitivity analyses
Random versus fixed effect models
The use of a fixed effect model did not change the summary estimate for the effect of probiotics on NEC (RR, 0.45; 95% CI, 0.37–0.56; heterogeneity: χ 2 = 37.92, df = 29 (p = 0.12); I 2 = 24%).
Risk of bias
The exclusion of three studies (Dongol Singh et al., 2017; Fernández-Carrocera et al., 2013; Kaban et al., 2019) with a high ROB due to randomization/allocation concealment did not change the summary estimate significantly.
Incidence of neonatal sepsis
The effect of probiotics on the incidence of neonatal sepsis was reported by 21 studies that included 9105 (probiotics, 4606; control, 4499) participants. The combined results showed a statistically significant reduction in incidence of sepsis of 22% in the intervention group compared to control (RR, 0.78; 95% CI, 0.70–0.86; heterogeneity: τ 2 = 0.01; (p = 0.16); I 2 = 23%). The number needed to treat was 14. The grade rating for this outcome was “high.” Summary of findings Table 3.
Publication bias
A funnel plot for publication bias looked symmetrical.
Subgroup analysis
Table 1 shows the results of subgroup analyses. Subgroup analysis could be done for the incidence of neonatal sepsis according to study setting, type of probiotic (single strain vs. multiple strain vs. synbiotic), type of feeding (breastfeeding vs. formula feeding vs. mixed feeding), and probiotic preparation (preparation containing Lactobacillus vs. Bifidobacterium vs. both Lactobacillus and Bifidobacterium vs. S. boulardii). Only the type of feeding differed among subgroups, probiotic supplementation seemed to have a significant effect for the prevention of neonatal sepsis when the supplementation was given to babies who received breastmilk only (RR, 0.76; 95% CI, 0.61–0.83; 8 studies) or breastmilk in combination with formula milk (RR, 0.76; 95% CI, 0.64–0.90; seven studies), p value for subgroups difference was 0.04.
Sensitivity analysis
Random versus fixed effect models
Use of a fixed effect model had a minimal effect on summary estimates for the effect of probiotics on the incidence of neonatal sepsis (RR, 0.79; 95% CI, 0.73–0.85; heterogeneity: χ 2 = 26.06, df = 20 (p = 0.16); I 2 = 23%).
Risk of bias
No significant difference was noted when two studies (Fernández-Carrocera et al., 2013; Kaban et al., 2019) with a high ROB were excluded from the analysis Analysis 2.21.
Sepsis specific mortality
Two studies reported the data for sepsis specific mortality. The combined results showed a reduction of sepsis specific mortality of 89% in the intervention group compared to control (RR, 0.21; 95% CI, 0.04–1.01; heterogeneity: τ 2 = 0.00; χ 2 = 0.91, df = 1 (p = 0.34); I 2 = 0%). This is limited by a wide CI of the estimate including 1.
Adverse events
No adverse event was reported in any of the included studies.
Neurodevelopmental outcomes
Two studies assessed neurodevelopmental outcomes after neonatal probiotic supplementation. We did not perform a meta-analysis for these outcomes, as these studies used different scales.
Sari et al. (2011) reported the data for neurodevelopmental outcomes at 18–22 months post neonatal probiotic supplementation for extremely low birth weight infants. Their results did not show any difference in growth and neurodevelopmental outcomes between the two groups. The growth outcomes were reported as weight (probiotic group 10.5 ± 1.7 kg vs. control 10.5 ± 1.7 kg, p value .92), length (probiotic group 79.4 ± 7.8 cm vs. control 81.0 ± 5.3 cm, p value .32), and head circumference (probiotic group 47.5 ± 6.5 cm vs. control 46.7 ± 1.8 cm, p value .53). The neurodevelopmental outcomes were reported as mental development index (probiotic group 90.7 ± 15.5 vs. control 90.4 ± 14.5, p value .88) and Psychomotor Development Index (probiotic group 95.4 ± 17.2 vs. control 93.2 ± 16.4, p value .39).
Oncel et al. (2014) also followed a cohort of extremely low birth weight infants after neonatal supplementation with probiotics or placebo. There was no significant difference in the neurodevelopmental outcomes at 18–24 months of age post supplementation, mental development index (probiotic 81 (median), 49 (min) to 124 (max) vs. placebo 82, 53–128; p value .48) or Psychomotor Development Index (probiotic 80, 49–112 vs. placebo 79, 49–107; p value .67).
DISCUSSION
Summary of main results
This review evaluated three neonatal nutritional interventions. Vitamin A supplementation during the neonatal period in the community setting did not have any significant effect on all-cause mortality at 1, 6, or 12 months. We did not identify any studies from LMICs that assessed the use of dextrose gel for the treatment or prevention of neonatal hypoglycaemia. Probiotic supplementation during the neonatal period mainly given to low birth weight and preterm babies was shown to reduce all-cause mortality, NEC, and neonatal sepsis.
Overall completeness and applicability of evidence
The evidence of neonatal vitamin A supplementation included 16 studies, and the number of participants in these studies exceeded 150,000. Overall, most of the included studies were at low ROB across many of the ROB items assessed using the Cochrane ROB scale. The statistical heterogeneity in the pooled data for mortality outcomes at 6 and 12 months was noted for neonatal vitamin A supplementation; however, the value of I 2 was <50%. Subgroup analyses done in a recent IPD analysis could potentially explain the reasons for heterogeneity and are discussed in Section 6.5.
The results for the use of probiotics during the neonatal period seem very promising. Almost all the studies in this meta-analysis included preterm and/or low birth weight neonates. The effect of probiotics on all-cause mortality was reported in 25 studies, and the analysis included more than 10,000 participants. The forest plot showed a homogenous effect in favor of the intervention with I 2 of 0%. We think that this effect is biologically plausible, and the most likely pathway of reduction in neonatal mortality from probiotic supplementation is via a reduction in sepsis and NEC, as shown in Analysis 2.15 and Analysis 2.9, respectively. We also think that these results are less likely due to bias. The studies by Guney-Varal et al. (2017), Kaban et al. (2019), and Dongol Singh et al. (2017) were at high ROB due to inadequate randomization methods. The exclusion of these three studies from meta-analysis for the effect of probiotics on all-cause mortality did not change the summary estimate significantly (RR, 0.82; 95% CI, 0.68–0.99). A funnel plot for publication bias was symmetrical. The use of a fixed versus random effect model also did not change the results significantly. In addition to these observations, the fact that the effect of probiotics on the reduction of neonatal sepsis and NEC was mostly homogenous (I 2 of 23% and 24%, respectively) indicates that the use of probiotics could be beneficial for babies with low birth weight and preterm birth. We notice, however, that there was significant clinical heterogeneity in the dose, duration, and strains of probiotics used; this indicates that more research is needed to determine the appropriate dose and duration of probiotic supplementation in neonates.
The use of probiotics for the prevention of NEC, sepsis, and mortality in preterm and/or low birth weight babies has been debated in the past. The use of probiotics was advocated after the publication of a Cochrane review in 2011 (Alfaleh et al., 2011, later updated in 2014, AlFaleh & Anabrees, 2014) that showed that probiotics reduced NEC (stage II or more) (RR, 0.35; 95% CI, 0.24–0.52) and mortality (RR, 0.40; 95% CI, 0.27–0.60) in preterm/low birth weight neonates (Ofek Shlomai et al., 2014; Robinson, 2014). Others challenged the appropriateness of the meta-analysis in the setting of clinical heterogeneity (Mihatsch et al., 2012; Mihatsch, 2011) and called for large trials before this intervention could be recommended in clinical practice (Mihatsch, 2011). This led to two large clinical trials, the ProPrems trial conducted in Australia and New Zealand (Jacob et al., 2013) and the PiPS trial conducted in the United Kingdom (Costeloe et al., 2016). The ProPrem trial used a mixture of probiotics (Bifidobacterium infantis, Streptococcus thermophilus, and Bifidobacterium lactis) and included 1099 preterm (<32 weeks) and very low birth weight (<1500 g) neonates. The results of the ProPrems trial showed that the use of probiotics did not reduce the incidence of sepsis and mortality, but did reduce the incidence of NEC (RR, 0.46; 95% CI, 0.23–0.93) (Jacob et al., 2013). The PiPS trial included 1315 neonates between the gestational age of 23–30 weeks who were randomised within 24–48 h to a single probiotic (Bifidobacterium breve BBG-001) or placebo. The results of the PiPS trial showed no difference between the intervention and the control group for the outcomes of NEC (RR, 0.93; 95% CI, 0.68–1.27), sepsis (RR, 0.97; 95% CI, 0.73–1.29), or death (RR, 0.93; 95% CI, 0.67–1.30) (Costeloe et al., 2016). The results of these trials were surprising in the setting of known evidence from meta-analyses of the available studies. A closer look at the results of the PiPS trial showed that there was significant contamination of the control group, as about 49% of the neonates from the control group had the same type of probiotic bacteria in their stool as those who were in the intervention group. This decreased the power of the study, and it was argued that a potential lack of effect might be explained by the cross-contamination of the control group (Deshpande et al., 2016; McKinlay et al., 2016). The debate of appropriateness of probiotic supplementation in the neonatal period has continued, and a recent network meta-analysis concluded that there is not enough evidence in favor of either a single or a mixture of strains of probiotics that could be suggested for routine clinical use for the prevention of NEC, sepsis, and/or mortality in preterm/low birth weight babies (van den Akker et al., 2018).
Our review focused on studies from LMIC. The effect of probiotic supplementation on mortality, sepsis, and NEC was significant when we pooled studies from these countries only. We noticed clinical heterogeneity in the use of probiotics in terms of type of probiotics, single versus multiple strains used, and baseline interventions such as the use of breastmilk. We think that the use of a meta-analysis is appropriate to pool these studies, as the primary target of all the studies was the same, that is, correction of dysbiosis. We further demonstrated that subgroup analysis based on certain clinical factors reveals no significant difference in results. We notice, however, the relative lack of studies from the community setting. This is likely due to the increased rate of community over hospital-based births in LMIC. For this reason, we read the results of a community-based study by Panigrahi et al. (2017) with great interest. This study was the largest study conducted on the use of probiotics (synbiotics) and had a sample size of 4556; this is three times larger than the sample size of the PiPS trial. Panigrahi et al. (2017) used a synbiotic which was a mixture of the probiotic Lactobacillus plantarum ATCC-202195 and the prebiotic fructooligosaccharide. This study recruited neonates who were at least 35 weeks of gestation and weighed at least 2000 g from rural settings from India. The results of the study showed a significant reduction in the primary outcome (combination of sepsis and death) in the intervention group compared to control (RR, 0.60; 95% CI, 0.48–0.74), culture-positive and culture-negative sepsis, and lower respiratory tract infections (Panigrahi et al., 2017). More such community-based studies are needed from other countries examining term, preterm, and low birth weight infants.
Are probiotics safe for use during the neonatal period? We did not find any substantial evidence of adverse events with the use of probiotics in neonatal age group. It is important, however, to consider the safety considerations of probiotic supplementation in this vulnerable population. Probiotics are not regulated as a medication and are thus susceptible to variations in quality within and between countries. If not carefully produced and handled, probiotics may also contain pathogenic contaminants that may then lead to neonatal sepsis. Probiotic supplementation has been linked to both bacterial (Dani et al., 2016) as well as fungal sepsis (Vallabhaneni et al., 2014). Despite their rare occurrence, neonates receiving probiotics should be followed in a registry to ensure any reporting and observation of the potential risk of sepsis in a large sample size in the real world setting.
Quality of the evidence
The GRADE quality of evidence was considered high for most of the outcomes for neonatal vitamin A and probiotic supplementation. The GRADE method of assessment of overall evidence considers the type of study, ROB, statistical heterogeneity, indirectness, and imprecision of the summary estimates as well as the risk of publication bias (Guyatt et al., 2011).
All the included studies for neonatal vitamin A supplementation were randomized and had minimal ROB. The statistical heterogeneity for pooled studies for neonatal vitamin A supplementation was noticeable but was not significant enough to decrease our confidence in the summary estimate. Similarly, the CIs around the summary estimate were narrow, and there was no increased risk of publication bias for studies that assessed neonatal vitamin A supplementation.
All the included studies for neonatal probiotic supplementation were also randomized. High ROB was noted for three of the included studies (Dongol Singh et al., 2017; Fernández-Carrocera et al., 2013; Kaban et al., 2019), but exclusion of these studies did not change the results of any of the outcomes, including all-cause mortality, NEC, and neonatal sepsis. The pooled results were mostly homogenous, and the summary estimates were precise with narrow CIs. The funnel plots for publication bias were symmetrical for the outcomes of all-cause mortality, NEC, and neonatal sepsis.
Potential biases in the review process
We used standard methods of Campbell and Cochrane collaborations to conduct the review. Two review authors screened the titles and abstracted the data from the included studies. Our inclusion/exclusion criteria were decided a priori, and a peer reviewed protocol was published giving details of methods of conduct of this review.
We performed two posthoc subgroup analyses for the effect of probiotic supplementation during the neonatal period. This analysis was based on the type of feeding, as our team thought it was essential to establish any differential effect of probiotics when the intervention was delivered with breastmilk or formula or both. The results for this analysis were similar among the subgroups for outcomes of all-cause mortality and NEC; however, there was significant heterogeneity among subgroups for the outcome of neonatal sepsis Analysis 2.18. A close examination of the data showed that the difference among subgroups was due to the group where the status of the feeding was “unclear.” Exclusion of this subgroup showed a homogenous protective effect in the case of breastmilk or formula milk-fed babies against neonatal sepsis (data not shown). So, we think that probiotics may have a significant protective effect against neonatal sepsis, NEC, and mortality irrespective of the type of food offered. The second posthoc subgroup analysis was based on study setting. We were interested in knowing if the probiotics had a similar effect on infants born in the hospital setting compared to those in the community setting. We were interested in this analysis because a significant number of births happen at home in LMIC. There were a limited number of studies conducted in the community setting that addressed the effect of probiotics; therefore, no solid conclusion could be drawn at this time for any of the outcomes.
Agreements and disagreements with other studies or reviews
The effects of neonatal vitamin A supplementation have been reviewed in two Cochrane reviews (Darlow et al., 2016; Haider et al., 2017). The Cochrane review by Haider et al. (2017) focused on randomized studies from the community setting only. We considered studies from both community and hospital settings. We updated the literature search and found one additional study from the community setting (Ahmad et al., 2019) and added three studies from the hospital setting (Basu et al., 2019; Giridhar et al., 2019; Sun et al., 2019). The studies from hospital settings were done in the neonatal intensive care setting for very low birth weight babies. We did not pool the results of these studies with those of the community-based studies. The Cochrane review on neonatal vitamin A supplementation for very low birth weight infants included 11 trials and reported a reduction in risk of death or oxygen requirement at 1 month of age (RR, 0.93; 95% CI, 0.88–0.99). Of the three studies we included in our review from LMIC, only one study showed a reduction in composite outcome of incidence of all-cause mortality and oxygen requirement for 28 days (RR, 0.44; 95% CI, 0.229–0.844)] from vitamin A supplementation in very low birth weight infants (Basu et al., 2019). The new study for neonatal vitamin A supplementation from the community was small and included 306 participants. The addition of this study did not change the results significantly compared to those published in the 2017 Cochrane review (Haider et al., 2017).
An individual participant meta-analysis of neonatal vitamin A studies conducted in the community setting was published during the preparation of this review (West et al., 2019). This review addressed multiple subgroup analyses both at the study- and individual-level characteristics and used the original data from individual trials to pool the studies. The overall results were similar to our results for all-cause mortality at 6 and 12 months (West et al., 2019). The subgroup analysis based on study-level characteristics showed that neonatal vitamin A supplementation significantly reduced 6-month mortality among the trials conducted in South Asia (RR, 0.87; 95% CI, 0.77–0.98) but not in Africa; they also showed a potential for increased risk of mortality in African countries (RR, 1.07; 95% CI, 1.00–1.15). Further subgroup analyses showed that neonatal vitamin A supplementation reduced all-cause mortality in the context of moderate or severe maternal VAD (defined as 10% or higher proportion of women with serum retinol <0.7 μmol/L or 5% or more women with night blindness) (RR, 0.87; 95% CI, 0.80–0.94), in settings where baseline (control group) early infant mortality was 30 or more per 1000 live births (RR, 0.91; 95% CI, 0.85–0.98), and in the context of lack of maternal education (>32% mothers had no schooling) (RR, 0.88; 95% CI, 0.80–0.96). The subgroup analyses conducted based on individual-level characteristics such as sex, birth weight, gestational age and size, age at dosing, parity, time of breastfeeding initiation, maternal education, and maternal vitamin A supplementation did not show any significant differential effect of neonatal vitamin A supplementation compared to placebo for these groups. As most of the subgroup analyses that we prespecified in our review were addressed in this study (West et al., 2019), we did not repeat these analysis in our current study.
Oral dextrose as a treatment of hypoglycaemia and prevention of hypoglycaemia in high-risk neonates has been evaluated in two Cochrane reviews (Hegarty et al., 2017; Weston et al., 2016). The review by Weston et al. (2016) addressed treatment of neonatal hypoglycaemia and included two studies, one from New Zealand and another from Ireland. They did not show any major difference in episodes of hypoglycaemia between the two study groups. The review by Hegarty et al. (2017) addressed the prevention of hypoglycaemia in high-risk neonates and included one study from New Zealand. The included study showed a significant reduction in hypoglycaemia episodes in the intervention group compared to control (RR, 0.76; 95% CI, 0.62–0.94). No randomized study was available from LMIC in either of the two reviews mentioned above. We updated the searches and did not find any study from LMIC.
Other reviews have been published that assess the effect of probiotic supplementation during the neonatal period. A Cochrane review was published in 2011 (Alfaleh et al., 2011) with an update in 2014 (AlFaleh & Anabrees, 2014). This has not since been updated. The Cochrane review included studies from LMIC and high-income countries and concluded that probiotic supplementation reduced NEC (stage II or more) (RR, 0.43; 95% CI, 0.33–0.56) and mortality (RR, 0.65; 95% CI, 0.52–0.81) but showed no effect for nosocomial sepsis (RR, 0.91; 95% CI, 0.80–1.03). More studies have been published since the publication of the 2014 Cochrane review update. Deshpande et al. (2017) reviewed studies from LMIC that addressed probiotic supplementation during the neonatal period. This review included twenty-three studies and concluded that probiotic supplementation reduced all-cause mortality (RR, 0.73; 95% CI, 0.59–0.90), NEC (RR, 0.46, 95% CI, 0.34–0.61), and neonatal sepsis (RR, 0.80; 95% CI, 0.71–0.91). We included thirty-three studies and updated the meta-analyses. With this new data, the magnitude and the statistical significance remained the same, but the summary estimates became more precise for the outcomes of all-cause mortality, NEC, and sepsis. We also conducted additional subgroup analyses that were not previously performed.
AUTHORS' CONCLUSIONS
Implications for practice
Neonatal vitamin A supplementation in the community setting does not appear to reduce infant mortality at 1, 6, or 12 months of age. Vitamin A supplementation during neonatal period increases the risk of bulging fontanelle. No data were available for dextrose gel supplementation for the prevention or treatment of neonatal hypoglycaemia in LMIC.
Probiotic supplementation is a promising intervention and can reduce all-cause mortality, neonatal sepsis, and NEC in low birth weight and/or preterm babies in LMIC in the hospital setting. Though we observed no adverse effects, infants receiving probiotics should be entered into a registry in order to observe any concerns for safety in large sample sizes in the real world setting.
Implications for research
There was significant clinical heterogeneity in terms of strains and dose of probiotics used in the included studies. More studies are needed to decide upon the right strain and optimal dose and duration of probiotics supplementation. Most of the included studies for probiotics supplementation were conducted in preterm/low birth weight babies in the neonatal intensive care unit. It is not clear if the similar protective effects would be seen when probiotics are given in the community setting or to term babies. It is also unclear if the supplementation of prebiotics and probiotics together (synbiotics) is more effective than probiotics alone. More studies are needed to answer these questions and to assess the effect of dextrose supplementation for the prevention and treatment of neonatal hypoglycaemia in LMIC.
Footnotes
ACKNOWLEDGEMENTS
We would like to thank Connor Appelman for his help with the screening of titles for dextrose supplementation.
CONTRIBUTIONS OF AUTHORS
Aamer Imdad, Deepika Ranjit wrote the first draft of the protocol. Gamael S. S. Surin participated in the design of the search strategy and writing of the protocol. Abigail Smith and Sarah Lawler designed the search strategy. Aamer Imdad wrote the manuscript for the final review. Aamer Imdad, Faseeha Rehman, Evans Davis, Gamael S. S. Surin, Deepika Ranjit, and Suzanna L. Attia helped with data extraction and analysis. Suzanna L. Attia and Aamer Imdad edited the manuscript. Zulfiqar A. Bhutta supervised and gave feedback for the design of the protocol and the main review.
DECLARATIONS OF INTEREST
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
The planned subgroup analyses for vitamin A were not conducted, as the same analyses were available from a recent IPD analysis (West et al., 2019). We did not use EPOC methodology for the ROB assessment, as all the included studies were RCTs and the Cochrane ROB assessment tool was used for the same. We did two posthoc subgroup analyses for probiotic supplementation during the neonatal period. These included type of feeding and study setting. We did the sensitivity analysis for ROB based on sequence generation and allocation concealment.
PUBLISHED NOTES
DATA AND ANALYSES
|
|
|
|
|
|
|
All-cause mortality |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
All-cause mortality: subgroup analysis: settings |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
Hospital based |
23 | 4691 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.65, 0.94] |
|
Community based |
3 | 6307 | Risk ratio (IV, Random, 95% CI) | 1.25 [0.51, 3.05] |
|
All-cause mortality: subgroup analysis: type of probiotics |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
Preparation contain a single strain of probiotics |
9 | 2242 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.61, 1.05] |
|
Preparation contained multiple strains of probiotics |
12 | 3050 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.58, 1.09] |
|
Preparation contained synbiotics (prebiotics + probiotics) |
5 | 5706 | Risk ratio (IV, Random, 95% CI) | 0.69 [0.29, 1.61] |
|
All-cause mortality: subgroup analysis: type of participants |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
Study include preterm/low birth weight babies |
25 | 10587 | Risk ratio (IV, Random, 95% CI) | 0.79 [0.65, 0.95] |
|
Study included term infants only |
1 | 411 | Risk ratio (IV, Random, 95% CI) | 1.38 [0.31, 6.08] |
|
All-cause mortality: subgroup analysis: type of feedings |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
Baby received breastmilk only |
14 | 7721 | Risk ratio (IV, Random, 95% CI) | 0.81 [0.62, 1.05] |
|
Baby received formula milk only |
1 | 411 | Risk ratio (IV, Random, 95% CI) | 1.38 [0.31, 6.08] |
|
Baby recieved both both breastmilk and formula milk |
8 | 2385 | Risk ratio (IV, Random, 95% CI) | 0.69 [0.48, 0.99] |
|
Type of feeding was unclear |
3 | 481 | Risk ratio (IV, Random, 95% CI) | 1.33 [0.63, 2.81] |
|
All-cause mortality: subgroup analysis: probiotics preparation |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
Preparation contained Lactobacillus |
10 | 7002 | Risk ratio (IV, Random, 95% CI) | 0.82 [0.63, 1.05] |
|
Preparation contained Bifidobacterium |
1 | 400 | Risk ratio (IV, Random, 95% CI) | 0.43 [0.17, 1.09] |
|
Preparation contained both Lactobacillus and Bifidobacterium |
13 | 3110 | Risk ratio (IV, Random, 95% CI) | 0.71 [0.47, 1.08] |
|
Preparation contained Saccharomyces boulardii only |
2 | 486 | Risk ratio (IV, Random, 95% CI) | 1.12 [0.46, 2.71] |
|
All-cause mortality: sensitivity analysis: fixed effect models |
26 | 10998 | Risk ratio (IV, Fixed, 95% CI) | 0.80 [0.66, 0.96] |
|
All-cause mortality: sensitivity analysis: risk of bias |
26 | 10998 | Risk ratio (IV, Random, 95% CI) | 0.80 [0.66, 0.96] |
|
High Risk of bias for randomisation/allocation concealment |
3 | 285 | Risk ratio (IV, Random, 95% CI) | 0.27 [0.05, 1.40] |
|
Low or Unclear Risk of bias for randomisation/allocation concealment |
23 | 10713 | Risk ratio (IV, Random, 95% CI) | 0.82 [0.68, 0.99] |
|
Necrotizing enterocolitis (any type) |
30 | 5574 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.59] |
|
Necrotizing enterocolitis: subgroup analysis: probiotic preparation |
30 | 5574 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.59] |
|
Preparation contained Lactobacillus |
13 | 2738 | Risk ratio (IV, Random, 95% CI) | 0.39 [0.25, 0.61] |
|
Preparation contained Bifidobacterium |
1 | 400 | Risk ratio (IV, Random, 95% CI) | 0.20 [0.09, 0.47] |
|
Preparation contained both Lactobacillus and Bifidobacterium |
14 | 1950 | Risk ratio (IV, Random, 95% CI) | 0.49 [0.36, 0.68] |
|
Preparation contained Saccharomyces boulardii only |
2 | 486 | Risk ratio (IV, Random, 95% CI) | 0.94 [0.45, 1.95] |
|
Necrotizing enterocolitis: subgroup analysis: type of feeding |
30 | 5574 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.59] |
|
Baby receieved breastmilk only |
13 | 1945 | Risk ratio (IV, Random, 95% CI) | 0.43 [0.31, 0.59] |
|
Baby receieved formula milk only |
1 | 93 | Risk ratio (IV, Random, 95% CI) | 0.21 [0.03, 1.76] |
|
Baby received both breastmilk and formula milk |
9 | 2445 | Risk ratio (IV, Random, 95% CI) | 0.55 [0.33, 0.92] |
|
Type of feeding was unclear |
7 | 1091 | Risk ratio (IV, Random, 95% CI) | 0.41 [0.17, 1.00] |
|
Necrotizing enterocolitis: subgroup analysis: type of probiotics |
30 | 5574 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.59] |
|
Preparation contained a single strain of probiotics |
12 | 2679 | Risk ratio (IV, Random, 95% CI) | 0.48 [0.30, 0.76] |
|
Preparation contained multiple strains of probiotics |
15 | 2156 | Risk ratio (IV, Random, 95% CI) | 0.48 [0.35, 0.67] |
|
Preparation contained synbiotics (prebiotics + probiotics) |
3 | 739 | Risk ratio (IV, Random, 95% CI) | 0.28 [0.12, 0.67] |
|
Necrotizing enterocolitis: sensitivity analysis: fixed effect models |
30 | 5574 | Risk ratio (IV, Fixed, 95% CI) | 0.45 [0.37, 0.56] |
|
Necrotizing enterocolitis: sensitivity analysis: risk of bias |
30 | 5574 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.59] |
|
Low or unclear risk of bias for randomisation/allocation concealment |
27 | 5289 | Risk ratio (IV, Random, 95% CI) | 0.46 [0.35, 0.61] |
|
High risk of bias for randomisation/allocation concealment |
3 | 285 | Risk ratio (IV, Random, 95% CI) | 0.33 [0.09, 1.13] |
|
Neonatal sepsis |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Neonatal sepsis: subgroup analysis: settings |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Hospital based |
19 | 3209 | Risk ratio (IV, Random, 95% CI) | 0.83 [0.76, 0.91] |
|
Community based |
2 | 5896 | Risk ratio (IV, Random, 95% CI) | 0.67 [0.49, 0.91] |
|
Neonatal sepsis: type of probiotics |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Preparation contained single strain of probiotics |
8 | 1328 | Risk ratio (IV, Random, 95% CI) | 0.84 [0.74, 0.96] |
|
Preparation contained multiple strains of probiotics |
9 | 2482 | Risk ratio (IV, Random, 95% CI) | 0.81 [0.68, 0.97] |
|
Preparation contained synbiotics (prebiotics + probiotics) |
4 | 5295 | Risk ratio (IV, Random, 95% CI) | 0.67 [0.54, 0.83] |
|
Neonatal sepsis: subgroup analysis: type of feeding |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Baby received breastmilk only |
8 | 6961 | Risk ratio (IV, Random, 95% CI) | 0.71 [0.61, 0.83] |
|
Baby received formula milk o nly |
2 | 218 | Risk ratio (IV, Random, 95% CI) | 0.59 [0.22, 1.56] |
|
Baby received both formula and breastmilk only |
7 | 1401 | Risk ratio (IV, Random, 95% CI) | 0.76 [0.64, 0.90] |
|
Type of feeding was unclear |
4 | 525 | Risk ratio (IV, Random, 95% CI) | 0.95 [0.82, 1.09] |
|
Neonatal sepsis: subgroup analysis: probiotic preparation |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Preparation contained Lactobacillus |
11 | 7068 | Risk ratio (IV, Random, 95% CI) | 0.74 [0.62, 0.87] |
|
Preparation contained Bifidobacterium |
1 | 400 | Risk ratio (IV, Random, 95% CI) | 0.81 [0.60, 1.09] |
|
Preparation contained both Bifidobacterium and Lactobacillus |
6 | 1026 | Risk ratio (IV, Random, 95% CI) | 0.83 [0.68, 1.02] |
|
Preparation contained Saccharomyces boulardii only |
3 | 611 | Risk ratio (IV, Random, 95% CI) | 0.73 [0.57, 0.94] |
|
Neonatal Sepsis: Sensitivity analysis: Fixed Effect Model |
21 | 9105 | Risk ratio (IV, Fixed, 95% CI) | 0.79 [0.73, 0.85] |
|
Neonatal sepsis: sensitivity analysis: risk of bias |
21 | 9105 | Risk ratio (IV, Random, 95% CI) | 0.78 [0.70, 0.86] |
|
Low or unclear risk of bias for randomization/allocation concealment |
19 | 8892 | Risk ratio (IV, Random, 95% CI) | 0.79 [0.71, 0.87] |
|
High risk of bias due to randomization/allocation concealment |
2 | 213 | Risk ratio (IV, Random, 95% CI) | 0.47 [0.25, 0.90] |
|
Sepsis specifc mortality |
2 | 4672 | Risk ratio (IV, Random, 95% CI) | 0.21 [0.04, 1.01] |