
Abstract
Background
Opportunities for social connection between generations have diminished over the last few decades around the world as a result of changes in the way that we live and work. The COVID-19 pandemic has exacerbated loneliness for many with young and old being kept apart for safety. The Public Health England prevention concordat for better mental health (Office for Health Improvement and Disparities) aims to bring a prevention-focused approach to improving public mental health. The concordat promotes evidence-based planning and commissioning to increase the impact on reducing health inequalities using sustainable and cost-effective interventions that impact on the wider determinants of mental health and wellbeing for children and young people and older people. Intergenerational activities could provide an opportunity to support both populations. In 2023, we produced an evidence and gap map to illustrate the amount and variety of research on intergenerational interventions and the gaps in research that still exist in this area. The review conducted here is based on the evidence in that map.
Objectives
This systematic review examines the impact of intergenerational interventions on the wellbeing and mental health of older people and identifies areas for future research as well as key messages for service commissioners.
Search Methods
We searched an evidence and gap map published in 2022 (comprehensive searches conducted July 2021 and updated June 2023) to identify randomised controlled trials of intergenerational interventions that report mental health and wellbeing outcomes for older people.
Selection Criteria
Randomised controlled trials of intergenerational interventions that involved unrelated younger and older people with at least one skipped generation between them and reported mental health or wellbeing outcomes for older people were included in this review.
Data Collection and Analysis
We used standard methodological procedures expected by The Campbell Collaboration. We conducted data extraction and Cochrane risk of bias assessments in EPPI reviewer. Where data allowed meta-analyses were conducted in STATA.
Main Results
This review includes 14 trials from six different countries. The trials had some important methodological weaknesses. Interventions were mainly delivered in-person and often in groups. They included visiting programmes, school volunteering programmes, music-based interventions and task-oriented interventions such as activities set in a multigenerational park, reminiscing activities, aggression management programmes, learning a language, making local environmental changes and in-school project work. Intergenerational interventions showed a small positive trend towards improving self-esteem (effect size [ES]: 0.33, 95% confidence interval [CI]: −0.35, 1.01) and depression (ES: 0.19, 95% CI: −0.23, 0.60) for older people participating. However, due to the small study sizes and low number of studies available, we cannot be confident about any effects. The results for other mental health and wellbeing outcomes are reported but due to little overlap in similar assessments across the studies, we could not combine them to assess the strength of evidence. There were no data about social isolation, spiritual health or sense of community. There are no long-term studies and no data on equity. We still know very little about what works and how or why. Whilst some interventions do use theories and logic to inform their development others do not. More exploration of this is needed.
Authors’ Conclusions
Commissioners and intervention developers should ensure interventions provide sufficient theoretical evidence for the logic behind the proposed intervention and should improve their consideration of equity within the interventions Research on intergenerational interventions need more consistent and agreed measures for reporting outcomes including community outcomes (core outcome sets). More understanding is needed on how best to measure ‘community’ outcomes. Research on intergenerational interventions should measure outcomes for BOTH the older and younger population engaged in the intervention—these may or may not be the same outcomes reflected in both populations. Further research is needed on the long-term impact of interventions on outcomes (whether participants need to keep being involved in an ‘intervention’ to continue to benefit) and sustainability of interventions beyond the initial funding of the research project. Supporting this our stakeholders highlighted that interventions that are initiated for research and then end (usually within a year) are not helpful.
PLAIN LANGUAGE SUMMARY
There is limited evidence of intergenerational interventions’ effects on mental health and wellbeing of older people
Intergenerational interventions are activities designed to bring younger and older people together, and may contribute to small improvements in self-esteem and levels of depression in older people.
However, this systematic review shows that it is not clear if these positive effects are consistent or last beyond the intervention. The evidence in this review also suggests that it is not clear if intergenerational interventions have any impact on quality of life, agitation, stress and loneliness in older people. There is no trial evidence looking at the effects of intergenerational interventions on social isolation for older people.
What is this review about?
Mental health and wellbeing, including loneliness, is a huge global issue, shared by younger and older people. The Covid-19 pandemic has increased loneliness for many, with generations being kept apart for safety.
Intergenerational interventions aim to promote greater understanding and respect between generations and help build communities. Intergenerational interventions can take many forms: school children visiting nursing home residents to share activities and stories, younger and older people coming together to share in music-based activities, older people volunteering in schools, and older people from outside the family helping/mentoring students.
This review looks at the impacts of intergenerational interventions related to the mental health and wellbeing of older people including depression, anxiety, quality of life, self-esteem, social isolation and loneliness. The review also looks at impacts on life satisfaction, agency (a sense of control and desire to do things in life), generativity (sense of purpose/meaning in life), happiness, intergenerational interaction or interaction with others, social activities, self perception, perceived emotional wellbeing, spiritual health, and sense of community.
What is the aim of this review?
This Campbell systematic review describes trials of intergenerational interventions that have reported on the mental health and wellbeing of older people, and how effective they were.
What studies are included?
This review includes 14 trials from six countries: USA, Japan, Italy, Spain, Australia and Canada. Interventions were mainly delivered in person and often in groups. They included visiting programmes, school volunteering programmes, music based interventions and task-oriented interventions such as activities set in a multigenerational park, reminiscing activities, aggression management programmes, learning a language, making local environmental changes and in-school project work.
The trials had some important weaknesses that may have affected their results.
What are the main findings of this review?
Intergenerational interventions showed a small positive trend towards improving self-esteem and depression for older people participating. However, due to the small study sizes and low number of studies available, we cannot be confident about any effects.
Results for other mental health and wellbeing outcomes are reported. There were no data about social isolation, spiritual health or sense of community.
The lack of consistent outcomes reported and the lack of studies on interventions that are similar or have similar elements means it is difficult to determine if any one intervention or element is effective for any given outcome.
How do these interventions work?
We still know very little about what works and how or why. Whilst some interventions do use known theories or techniques to articulate how something is thought to have an impact, others do not. It is therefore difficult to establish why any particular intervention might have an impact on any particular outcome.
What do the findings of this review mean?
The differences in the included studies means we cannot be certain that the findings are true and consistent across intergenerational activities. We need more robust research with larger numbers of participants who are studied for a longer period and after the intervention.
This field of study would also benefit from using agreed outcome measures consistently across interventions, to aid future comparisons and the development of research and practice.
How up-to-date is this review?
The review authors searched for studies up to July 2021 and searched again in June 2023 for new randomised controlled trials.
BACKGROUND
The problem, condition or issue
Although multigenerational families are reported to be on the increase recently in the US (Generations United, 2021), the number of multigenerational families with intergenerational support varies across rural and metropolitan areas and different cultures (ILC, 2012). In rural settings, intergenerational patterns of socialisation are often disrupted as younger people migrate to cities, missing opportunities to benefit from the knowledge and guidance of older family members. Opportunities for social connection between generations have diminished over the last few decades in the UK as a result of changes in the way that we live and work (Kingman, 2016; United for all Ages, 2017) and around the world Ending (Loneliness, 2022; Van Beek, 2022). Housing and economic trends have seen younger people move to live in city centres whilst the older generation live in towns and rural areas. A report published by the Intergenerational Foundation in 2016 (Kingman, 2016) suggests that in the 25 biggest cities within the UK only 5% of people aged over 65 live in the same neighbourhood as someone under the age of 18. Furthermore, even when people from different age groups do live in the same area, the decline in spaces such as libraries, youth clubs and community centres mean that there are fewer opportunities to meet and mix socially with other generations outside our own families. Increased working hours, improved technology, changes in family patterns, relationship breakdowns within families and migration are also believed to be contributory factors to generation segregation (Generations Working Together, 2019). There are many potential economic, social and political impacts of generations living separate and parallel lives, for example, higher health and social care costs, an undermining of trust between generations (Brown, 2014; Edström, 2018; Laurence, 2016; Vitman, 2013), reduced social capital (Laurence, 2016), a reliance on the media to form understanding of others’ viewpoints (Edström, 2018; Vasil, 1993) and higher levels of anxiety and loneliness. Loneliness is a huge global issue (Surkalim, 2022) and one that is shared by both younger and older people (Hong, 2023). The COVID-19 pandemic has exacerbated loneliness for many with young and old being kept apart for safety.
In the Office for National Statistics Community Life Survey, 2016 to 2017 (ONS, 2018) 5% of adults in the UK felt lonely (often or always). Similarly, in the US a survey conducted in 2018 found that almost half of 20,000 U.S. adults sometimes or always reported feeling alone with 40% of participants also reporting they sometimes or always feel that their relationships are not meaningful and that they feel isolated (Novotney, 2019). In the UK those aged 16–24 were also more likely than all other age groups (except the 25–34 years group) to report feeling lonely (often or always). Increased social isolation also reduces mental wellbeing (Hawkley, 2015) in older age and is further impacted by the pandemic due to the measures put in place to prevent spread of the virus. This was found to have an adverse impact on psychological outcomes including increased depression and anxiety (Robb, 2020; Zhou, 2020). There are a range of interventions designed to help older people who feel socially isolated and/or lonely including community support groups, visiting schemes, therapy/counselling schemes, and interventions to promote physical activity and other social activities (Dickens, 2011). Intergenerational interventions are one option that can combine social interaction and connection across generations using meaningful and engaged activities which can help to tackle feelings of loneliness and social isolation and improve wellbeing.
The intervention
We use the definition of intergenerational practice developed by the Beth Johnson Foundation: Intergenerational practice aims to bring people together in purposeful, mutually beneficial activities which promote greater understanding and respect between generations and contributes to building more cohesive communities. Intergenerational practice is inclusive, building on the positive resources that the young and old have to offer each other and those around them (Beth Johnson Foundation, 2021).
Intergenerational programmes and activities may be promising interventions that can address some of the needs of both older people and children and young people. These interventions can take many formats and are delivered in diverse settings, often by third sector organisations. Although, evidence suggests that intergenerational activity can have a positive impact on participants (e.g., reducing loneliness and exclusion—for both older people and children and young people; improving mental health; increasing mutual understanding and tackling important issues such as ageism, housing and care) (Canedo-García, 2017), decisions to commission/fund any services are complex due to the lack of evidence regarding which programmes to fund and support.
Between July and December 2021, we produced an evidence and gap map (EGM) (Campbell Whear, 2023) to illustrate the amount and variety of research on intergenerational interventions and the gaps in research that still exist in this area. We have discussed the evidence from this map with our stakeholders and co-developed the research question for this review as an important question with both current and future relevance for ageing communities.
How the intervention might work
We have developed a logic model (Figure 1) to illustrate our understanding of how intergenerational activities might work to improve the mental health and wellbeing of older people. The logic model is based on discussions with the stakeholder group during the construction of the EGM (Campbell Whear, 2023). Ronzi (2018) describes evidence for numerous mediators involved in the mechanisms of intergenerational interventions for example activities such as reading to children, assisting young people in school and mentoring activities lead to older people feeling appreciated, valued and respected and being able to share an interest with others. This then leads to more positive attitudes towards ageing, improved self-esteem and confidence, happiness, enjoyment and satisfaction, which then encourages more social participation, increased social relationships, increased physical activity and decreased social isolation. Vieira (2016) suggests intergenerational practices could be divided into three main types: 1—those that bring generations together to promote intergenerational relationships (focused on solving the problem of the gap between generations); 2—those that combine the promotion of intergenerational relationships with an additional goal, such as, helping older people develop suitable IT skills; and 3—those that bring generations together because it seems a better way to achieve a secondary goal, such as local environment community projects.
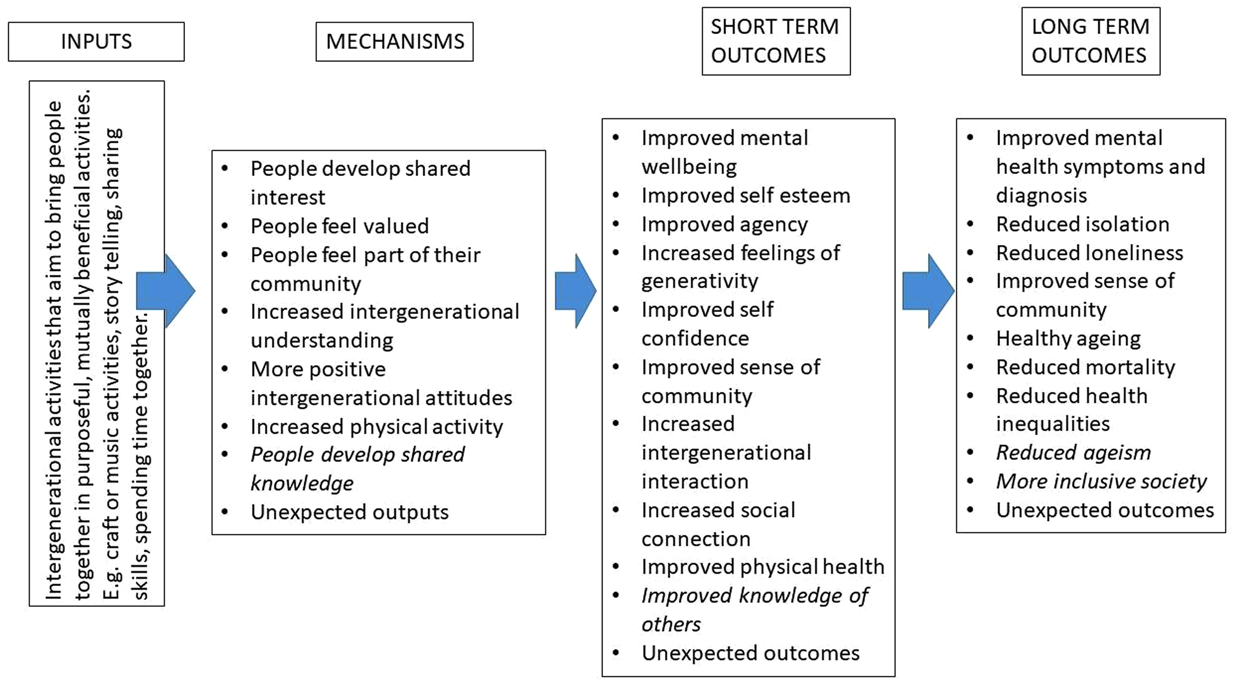
Logic model to illustrate how intergenerational activities might work to improve the mental health and wellbeing of older people.
The logic model indicates some of the ways that intergenerational activities (in their broader description/context) might work (mechanisms) to impact on various mental health and wellbeing outcome in the short and longer term. There are many areas that are not yet explored or evidenced, and we expect our review to help improve this knowledge.
Why it is important to do this review
The UK's All Party Parliamentary Group on Social Integration—Healing the generational divide report (APPGSI, 2019) offers a range of recommendations to alleviate the generational divide and over 50 voluntary organisations working with MIND (MIND, 2020) advocate for communities, organisations, agencies and the government to work together to respond to the mental health and wellbeing needs of the nation. Evidence-based intergenerational interventions may have a substantial role to play in this (Dickens, 2011).
It is not just the UK that has identified loneliness and social isolation as a major health risk. In May 2023 the US SurgeonGeneral released Social Connection—Current Priorities of the US Surgeon General (hhs.gov) identifying an ‘epidemic of loneliness and isolation’ that can cause physiological harms, including a 29% increased risk of heart disease; a 32% increased risk of stroke; and a 50% increased risk of developing dementia for older adults as well as those associated with mental health and wellbeing. In Australia 37% of 18–24 year olds are reported to feel lonely as well as one-third of adults aged over 60 years (Groundswell, 2022). The WHO/UN Decade of Health Ageing report (WHO's work on the UN Decade of Healthy Ageing [2021–2030]) also highlights the need to change how we think, feel and act towards age and ageing, and develop communities in ways that foster the abilities of older people—intergenerational interventions may be a place for both these things to happen.
Having conducted an EGM on intergenerational interventions we were able to identify areas where reviews have and have not already been conducted and areas where research was more or less prolific. We have identified reviews registered on PROSPERO that cover related areas such as meaningful engagement between adolescents and older people in a residential care setting (Laging, 2020) the design and best practice for intergenerational exchange programmes also between adolescents and older people (Webster, 2019) and features of intergenerational programmes and attitude changes between adolescents and older people (Ahmad, 2021).
We have been careful to ensure that our review does not duplicate existing reviews. There is some overlap with a recently published review (Krzeczkowska, 2021) on the effectiveness of intergenerational interventions, although this review included a wide range of study designs and reported on a wider range of outcomes (social, cognitive and health).
Our review includes only randomised controlled trials and is limited to mental health and wellbeing outcomes for older people. However, as our literature search was more comprehensive, we were able to identify a larger body of relevant evidence from randomised controlled trials. Furthermore, in response to stakeholder feedback, we explore the characteristics of intergenerational activities (e.g., type of activity, level of contact, setting, duration) as well as the theories underlying them to gain an understanding of the characteristics associated with a positive outcome for older people.
OBJECTIVES
This systematic review examines the impact of intergenerational interventions on the wellbeing and mental health of older people and identifies areas for future research as well as key messages for service commissioners.
We seek to answer the following research questions from randomised controlled trial studies: What is the effect of intergenerational interventions on the wellbeing and mental health of older people? What characteristics of intergenerational activities are associated with an impact on the wellbeing and mental health of older people? What are the underlying theories for the effectiveness of intergenerational activities in older people?
METHODS
Criteria for considering studies for this review
Types of studies
We included randomised control trials (RCTs) only as we wished to understand the effectiveness of these interventions. Control/comparator groups were usual care/no intervention, wait-list control or intervention but without the intergenerational component. We acknowledge that there is a wider array of intervention designs that can inform our knowledge about these interventions, but randomised trials are possible in this context, and so we wanted to understand the level of knowledge gained from these trials to date to more appropriately inform areas for future research and practice.
Types of participants
We included studies that include older adults and children and young people but were particularly interested in outcomes related to older people.
No age boundary restrictions were applied, but we sought information from studies that suggested there was at least one skipped generation between older and younger participants. Studies in which participants are related by family or marriage were excluded. Inclusion was not be determined by age cut-offs but by the included studies’ own definition of ‘older people’ and ‘younger people’. The participants of these studies did not have to have reported feelings of loneliness or social isolation.
Types of interventions
We included any intervention that sought to bring older and younger people together intentionally with the purpose of achieving positive health and/or social and/or educational outcomes. These might include reminiscence programmes, buddy systems, storytelling, school-based interventions, arts-based interventions and digital interventions.
We used the Depth of Intergenerational Engagement Scale (Kaplan, 2004) as the framework for the interventions. The Depth of Intergenerational Engagement Scale places programmes and activities on a continuum, with points that correspond to different levels of intergenerational engagement, ranging from initiatives that provide no direct contact between age groups (point 1) to those that promote intensive contact and ongoing opportunities for intimacy (point 7). Examples of intergenerational initiatives fitting into each point on the scale are described below (Table 1).
Depth of Intergenerational Engagement Scale (Kaplan, 2004).
Programs fitting into all points on this continuum provide positive experiences for interacting with persons in other age groups. However, for this project interventions in levels 1 and 2 are outside the scope of our review due to the lack of direct interaction between the generations, all other levels are included.
Types of outcome measures
Only studies that include at least one type of outcome relating to mental health or wellbeing in older people will be included.
Primary outcomes
To address Research Question 1 (What is the effect of intergenerational interventions on the wellbeing and mental health of older people?) our primary outcomes included all outcomes reported using a standardised measure (a measure with reported/known reliability and validity) to assess mental health and wellbeing such as depression, anxiety, quality of life, self-esteem, social isolation and loneliness.
Secondary outcomes
To address Research Question 1 our secondary outcomes included other indicators of mental health and wellbeing that are less likely to be captured by standardised measures and more likely to be captured by individual/bespoke questions or observations. For example, reports of life satisfaction, agency, generativity (sense of purpose/meaning in life), happiness, intergenerational interaction/interaction with others, social activities self-perception, perceived emotional wellbeing, spiritual health, and sense of community.
To address Research Question 2 (What characteristics of intergenerational activities are associated with a positive impact on the wellbeing and mental health of older people?) we used information on intervention characteristics such as setting, context, intensity, duration etc.
To address Research Question 3 (What are the underlying theories for the effectiveness of intergenerational activities in older people?) we used information on the underlying theories reported within the included studies.
Duration of follow-up
Any duration.
Types of settings
Any setting or context.
Publication status
We did not exclude studies on the basis of publication status.
Search methods for identification of studies
Searches were conducted to populate the EGM (Campbell Whear 2023) from which this review originates. For the map we searched MEDLINE (via OvidSp), EMBASE (via OvidSp), PsycINFO (via OvidSp), CINAHL (via EBSCOHost), Social Policy and Practice (via OvidSp), Health Management Information Consortium (via OvidSp), Ageline (via EBSCOhost), ASSIA (via ProQuest), Social Science Citations Index (via Web of Science), ERIC (via EBSCOhost), Community Care Inform Children, Research in Practice for Children, ChildData (via Social Policy and Practice), the Campbell Library, the Cochrane Database of Systematic Reviews and the CENTRAL database to populate the EGM between 22 July and 30 July 2021 using terms for intergenerational practices. As we were seeking to identify the richest possible evidence base, we did not place any language or date restrictions on the searches. Our search strategies for the EGM are available in Supporting Information: Appendix 1.
Electronic searches
For the subsequent review in June 2023 we reran the database strategies from the date of the last search for the EGM (July 2021) on the CENTRAL database of randomised controlled trials, and on the databases MEDLINE, PsycINFO, and AgeLine with the addition of a search filter for randomised controlled trials. These databases were selected based on the completion of a search summary table (Bethel, 2021) following the EGM which indicated where relevant studies were found. We also carried out citation searching (forwards and backwards) any included studies.
Searching other resources
For the EGM we also searched for grey literature via relevant organisation websites (Age UK, Age International, the Centre for Ageing Better, Barnardo's, Children's Commission, UNICEF, Generations Working Together, the Intergenerational Foundation, Linking Generations and The Beth Johnson Foundation), conference abstracts via the Conference Proceedings Citation database, and dissertations via ProQuest Dissertations and Theses Global. These searches were updated as above.
To find any published literature not captured by the databases we reviewed the included studies within relevant systematic reviews and hand searched the Journal of Intergenerational Relationships.
Data collection and analysis
Selection of studies
Studies were identified from the relevant domains of our EGM (Campbell Whear, 2023) and screened against the eligibility criteria independently by two reviewers. Methods for study selection used to populate the EGM can be found in the report (Campbell Whear, 2023).
Data extraction and management
Once relevant studies were identified data extraction was undertaken by one reviewer and checked by a second with discrepancies resolved by discussion with arbitration by a third reviewer were necessary. Data extraction sheets were developed in EPPI-Reviewer and piloted by two reviewers on a sample of papers. We extracted the following data: Publication details, sample size, population details—including details required in the PROGRESS Plus criteria (O'Neill, 2014), intervention and comparator details including type of activities undertaken, setting, duration, intensity, timing and mode of delivery—as detailed in the TIDieR checklist (Hoffman, 2014), outcome measures, and outcome data. We also extracted details of the underlying theories and logic as described by the authors in the introduction and method sections of included papers.
Assessment of risk of bias in included studies
One reviewer conducted critical appraisal which was checked by a second, with all discrepancies resolved through discussion. We conducted critical appraisal in EPPI-Reviewer and used the already incorporated Cochrane Risk of Bias tool (Higgins, 2019).
Assessment of equity in included studies
We used the PROGRESS Plus framework (O'Neill, 2014) to guide data extraction of participant characteristics of eligible and targeted populations within the included studies.
Description of interventions used in included studies
We used the TIDieR checklist (Hoffman, 2014) to describe the interventions used in included studies. The TIDieR checklist contains 12 items that cover the information required to comprehensively describe an intervention and its implementation.
Unit of analysis issues
Dealing with missing data
Where data were not available within the published papers, the authors were contacted, and this information was requested. Where authors did not provide the requested information these studies were excluded from the meta analysis but included in the review.
Assessment of reporting biases
Too few trials were included in any one meta-analysis to support use of funnel plots. Reporting biases at outcome level were assessed via inspection of included studies.
Data synthesis
We anticipated a disparate and heterogeneous body of evidence in terms of the aim of the intervention, the population, intervention, comparator and outcomes.
We conducted meta-analysis for outcomes that had three or more contributing studies and followed the Synthesis Without Meta-analysis (SWiM) reporting guidance for the remaining synthesis (Campbell, 2020). All studies in the meta analyses only reported one measure of each of the outcomes and thus each study only contributed one effect size per meta-analysis.
Studies are tabulated and grouped according to outcomes, using the logic model to inform decisions on groupings where appropriate. Tables are used to describe the heterogeneity within and across the included studies.
We have used a standard metric (effect size) for each outcome measure where possible. Where meta-analysis has not been possible, we have used effect size estimates. We have used pre-reported effect sizes from the studies included in meta analysis using a random effects model Stata.
All outcomes were estimated using standardised mean differences (Cohen's d).
Where meta-analysis was appropriate heterogeneity was described using the I 2 statistic and the Q test. Subgroup analysis could not be performed due to the variation in intervention design. No sensitivity analyses were planned. Given the variation across studies, we used the random effects model. We report the estimate of χ 2 and the confidence intervals for the overall mean effect size.
Where studies were combined with different scales, we ensured that higher scores for continuous outcomes all have the same meaning for any particular outcome and explained the direction of interpretation.
Summary of findings and assessment of the certainty of the evidence
We did not include Summary of findings or assessments of the certainty of the evidence.
Stakeholders
The following individuals have contributed to the project through the advisory group: Ronald Amanze; David Truswell—Executive Director of Dementia Alliance for Culture and Ethnicity, Peter Daniels—former Chief Happiness Officer at Humanitas Deventer, Professor Sir Muir Gray—Director of the Optimal Ageing Programme; Iain Lang—University of Exeter; Vicki Goodwin—University of Exeter; Jo Day—University of Exeter; Aideen Young—Centre for Ageing Better; Dylan Kneale—UCL; Ruth Garside—University of Exeter; Claire Goodman—University of Hertfordshire; Tracey Howe—Cochrane Campbell Global Ageing Partnership; Oliver Rashbrook Cooper—Public Health England; Kelvin Yates—AgeUK Cornwall; Nathan Hughes—University of Sheffield; Debbie Hanson—Sheffield City Council; Laura Abbott—Chilypep; Hannah Fairbrother—University of Sheffield; Kerry Albright—UNICEF; Rachel Staniforth—Public Health; Girish Vaidya—Sheffield Children's NHS Foundation Trust; Sally Pearse—Sheffield University.
Members of the ‘Only Connect!’ network also contributed throughout the project. The group has local, national and international members from the care sector, local government, academia, schools and leading organisations involved in providing intergenerational activities. Members of the group brought their experiences of working with older people, people living with dementia and young people with experience of taking part in intergenerational activities.
During the production of the EGM we convened four whole project meetings to include stakeholders and advisory group members to assist with interpretation and understanding, including, making adjustments to the logic model and comments on the report. The second of these meetings identified and confirmed the topic for this review. The fourth meeting incorporated initial feedback on the review findings, logic model and approach to reporting equity characteristics. We have used a newsletter and other methods of sharing ideas and suggestions such as JamBoard to ensure that as many views and perspectives are captured as possible Table 2
Stakeholder engagement.
Abbreviation: EGM, evidence and gap map.
RESULTS
Description of studies
Results of the search
Using the EGM created in spring 2022 (Campbell Whear, 2023) we found 14 includable RCTs. After two reviewers independently screened these results their data and information was extracted independently using EPPI reviewer EPPI reviewer. All papers that reported a relevant outcome were included in this review. There was one study with two papers (Carlson, 2008; Fried, 2004) that reported that it had collected data on the outcome of depression, but this data was not reported in any of the published papers, we contacted the authors to request this data, but we did not receive a response—therefore this study was excluded as it had no relevant outcome data. The updated searches found 241 references to screen at title and abstract stage of these 16 were then screen at full text stage. After full text screening no additional studies were included though two ongoing studies were identified Digital Buddy: Digital Inclusion for the Elderly; INTEGRITY. Forward and backward citation chasing of these included studies revealed no further includable studies (Figure 2).
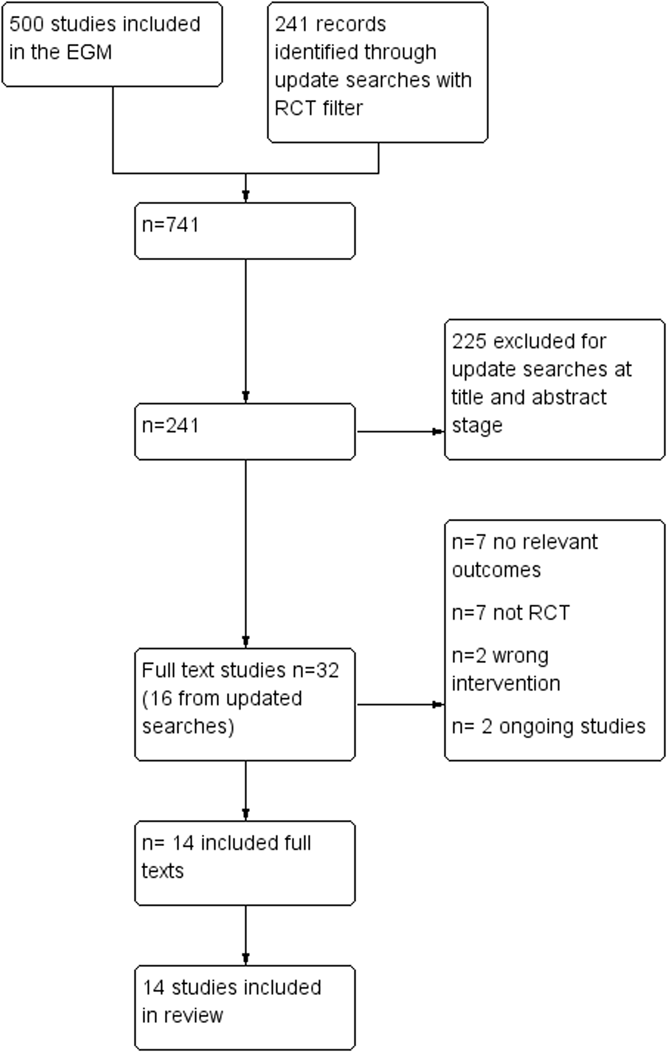
Prisma flow diagram from evidence and gap map (EGM). RCT, randomised control trial.
Included studies
The number of included studies in this review is 14 (Table 3).
Study characteristics.
Location of studies
Of the 14 the majority (n = 10) were conducted in the USA. One study was conducted in each of the following countries: Canada, Japan and Australia with another study conducted across two countries (Italy and Spain).
Population characteristics
Although intergenerational interventions by their nature involve at least two population generations, only three of these intervention studies were specifically targeted at both older people and younger people and children. However, outcomes were reported for both generations in half of the studies. The older people involved in the included studies were generally reported as being 65 years and above, although some were targeted at younger ages (50 years and above); others did not describe the age range or indicated a broader characteristic such as ‘retired’ (n = 2). There were five interventions that involved young people aged 12–18 years, two that involved young people aged 18–30 years, two that involved children aged 6–11 years, two that involved children aged 0–5 years and two that involved children and young people across more than one age group (one study did not report the ages of the children (Rook, 2003).
Study/sample size
The studies sizes ranged from 16 to 702 people with five studies (Gruenewald, 2016; Rook, 2003; Sakuri, 2018; Shkilnyk, 1984; Sipsas-Herrmann, 2000) including a combined sample larger than 100 people. The number of younger people included in these studies ranged from three to 194 with four studies unable to report the number of younger people included as they were part of a school sample. The number of older people included in these studies ranged from 13 to 702.
Equity characteristics
We used the PROGRESS Plus framework (O'Neill, 2014) to guide data extraction of participant characteristics of eligible and targeted populations within the included studies. We hoped to use this information to describe and assess categories of disadvantage based around place of residence, race/ethnicity, occupation, gender, religion, education, socioeconomic status, social capital, other personal characteristics, for example, cognitive decline, and relationship features, however, the information we were able to retrieve was very limited.
From the information we were able to retrieve we could identify that of the 14 studies, four specifically targeted older people with cognitive decline (Detmer, 2020; George, 2011; Giglio, 2006; Low, 2015), one study specifically targeted their intervention for Italian children in secondary school and older people in a residential care home in Spain (Carcavilla, 2020), four studies specifically excluded older people with cognitive decline (Carcavilla, 2020; Cardona, 2002; Gruenewald, 2016; Sakuri, 2018), two studies targeted older people living in their own homes (Chippendale, 2015; Sakuri, 2018), two studies targeted low income areas/populations (Rook, 2003; Thornton, 2017), two studies required a good level of functional language/literacy skills (Gruenewald, 2016; Thornton, 2017) and one study targeted children with a physical disability in hospital (Rook, 2003).
In terms of descriptions of sample populations much of the information we would hope to present in the PROGRESS Plus framework is missing. The most commonly reported characteristics were around race/ethnicity, gender, socioeconomic status, education and other selected personal characteristics like cognitive decline or physical impairments. However, even within these descriptions the information available is limited, and they are not necessarily accounted for in the analysis of the results. We have presented the information we were able to find in Supporting Information: Appendix 2.
Intervention characteristics
The majority (n = 10) of the interventions were Level 5 (demonstration projects lasting a limited period) (Carcavilla, 2020; Cardona, 2002; Chippendale, 2015; Dawson, 2017; Detmer, 2020; George, 2011; Giglio, 2006; Rook, 2003; Shkilnyk, 1984; Thornton, 2017) of the Depth of Intergenerational Engagement Scale (Kaplan, 2004), with three at Level 6 (Gruenewald, 2016; Sakuri, 2018; Sipsas-Herrmann, 2000) and one at Level 7 (Low, 2015).
The interventions were largely delivered in-person with one conducted online (Carcavilla, 2020). Interventions were often delivered in groups (n = 6) with some interventions having both group and individual elements (n = 6), two interventions were delivered on an individual basis. The interventions were delivered in a range of settings including schools (n = 5), care homes (n = 4), Hospital (n = 1), shared facilities (n = 1), nursery setting on a university campus (n = 1), community settings (n = 1) and assisted living centres (n = 3). Some interventions took place in more than one setting (Carcavilla, 2020; Giglio, 2006; Sakuri, 2018).
The interventions described were delivered over varying timescales ranging from 3 weeks to 1 year, with some studies reporting outcomes over three Rook 2003 and 6 years Sakuri 2018. Most studies (n = 11) were conducted over less than 6 months so had only short term outcome data and had no identifiable long term follow-up plans.
Three interventions took the form of visiting programmes (Rook, 2003; Shkilnyk, 1984), three were school volunteering programmes (George, 2011; Gruenewald, 2016; Sakuri, 2018), two were music-based interventions (Detmer, 2020; Giglio, 2006), and the rest were task-oriented involving physical activities in a multigenerational park (Dawson, 2017), reminiscence activities (Chippendale, 2015), activities to reduce aggression (Sipsas-Herrmann, 2000), learning language skills (Carcavilla, 2020), making local environmental changes (Thornton, 2017) and school project work separate to general volunteering in schools (Cardona, 2002).
The focus of the interventions was also varied, some focused on one particular skill or activity such as developing language Carcavilla 2020, music skills (Detmer, 2020; Giglio, 2006), environmental activities (Thornton, 2017), professional skills/understanding for students (Chippendale, 2015), reading (Sakuri, 2018) and mentoring/anger management (Sipsas-Herrmann, 2000). Whilst others tended to use multiple activities, such as arts and craft, exercise, sharing meals, storytelling, maths and playing games to encourage interactions more generally.
Those involved in providing/delivering interventions ranged from researchers (Dawson, 2017), volunteers (Sipsas-Herrmann, 2000), trained students (Thornton, 2017), care home staff (George, 2011; Low, 2015), to occupational therapists (Chippendale, 2015) or music therapists (Detmer, 2020; Giglio, 2006). Some studies did not report who delivered the intervention (Carcavilla, 2020; Cardona, 2002; Gruenewald, 2016; Rook, 2003; Sakuri, 2018; Shkilnyk, 1984).
Six studies reported intentionally tailoring the intervention, these were mainly to be able to adjust to the setting or more functional requirements to allow the intervention to take place (Carcavilla, 2020; Dawson, 2017; Sakuri, 2018; Shkilnyk, 1984; Sipsas-Herrmann, 2000) and one reported being able to tailor the activity/topic to the interests of the older person (Thornton, 2017).
Other modifications to interventions were largely unclear or not reported. Two studies reported making some changes (Low, 2015; Thornton, 2017) these accounted for changes in the activities or the availability of staff or participants during the intervention.
Intervention fidelity was reported in half of the studies (Chippendale, 2015; Dawson, 2017; Low, 2015; Rook, 2003; Sakuri, 2018; Sipsas-Herrmann, 2000; Thornton, 2017) but measures of fidelity were focused around participant attendance and attrition. Two studies reported using more detailed measures to inform intervention fidelity (Low, 2015; Thornton, 2017) which included conducting surveys, focus groups and observations informing how the intervention was delivered and received and aspects affecting implementation. However, the impact of fidelity concerns were rarely discussed in the results of the study (Table 4).
Intervention characteristics.
Excluded studies
We obtained our included studies from the EGM which has an RCT filter and filters for relevant outcomes, so no studies were excluded through screening, however, two studies were excluded from analysis as they provided no data on an outcome they reported (Carlson, 2008; Fried, 2004). From the update searches 16 studies were excluded at the full text stage because they did not report a relevant outcome (n = 7), they were not RCTs (n = 7), they were not an includable intervention (n = 2) or were ongoing studies with no data yet available (n = 2).
Risk of bias in included studies
We used the Cochrane Risk of Bias tool to understand the level of potential bias in these RCTs (Figure 3).
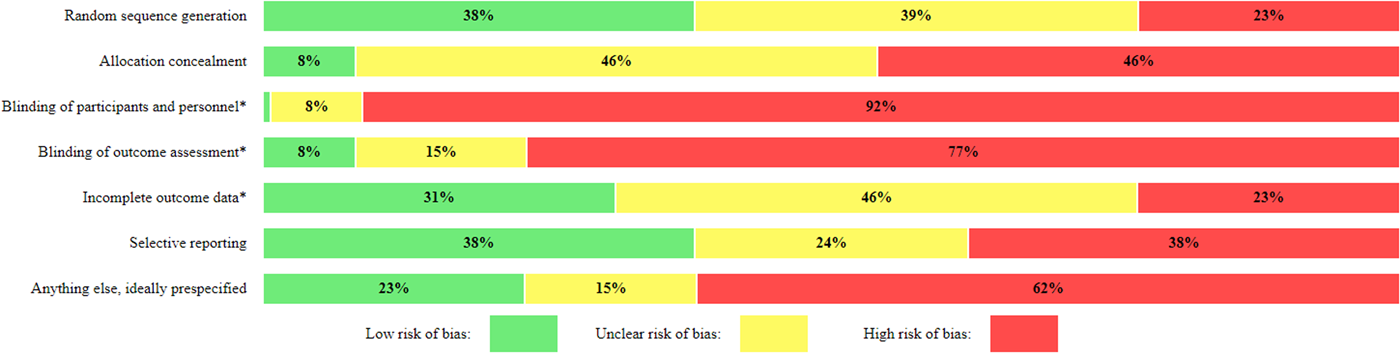
Risk of bias summary.
All the included studies are at high risk of bias. Most studies scored positively (with low risk of bias) on only two items or fewer (out of seven items). Areas of particular concern are blinding of participants, personnel and outcome assessment, allocation concealment and sample size. Blinding of participants and personnel is particularly difficult in socially based complex interventions where it will be obvious to participants and those around them that they are in an intervention (of some kind). This risk can be appeased to some extent by blinding outcome assessors but in most of the included studies the tools used to gather data were in self report form or the person collecting the data was aware of the participant's grouping. Even if this domain is excluded from the risk of bias analysis the overall judgement for the risk of bias in these studies would not change substantially. The reporting of methods of allocation concealment was absent in most studies, studies were generally small (from 16 to over 700) and sample size calculations were reported in only two of the 14 studies (Chippendale, 2015; Low, 2015) (Figure 4).
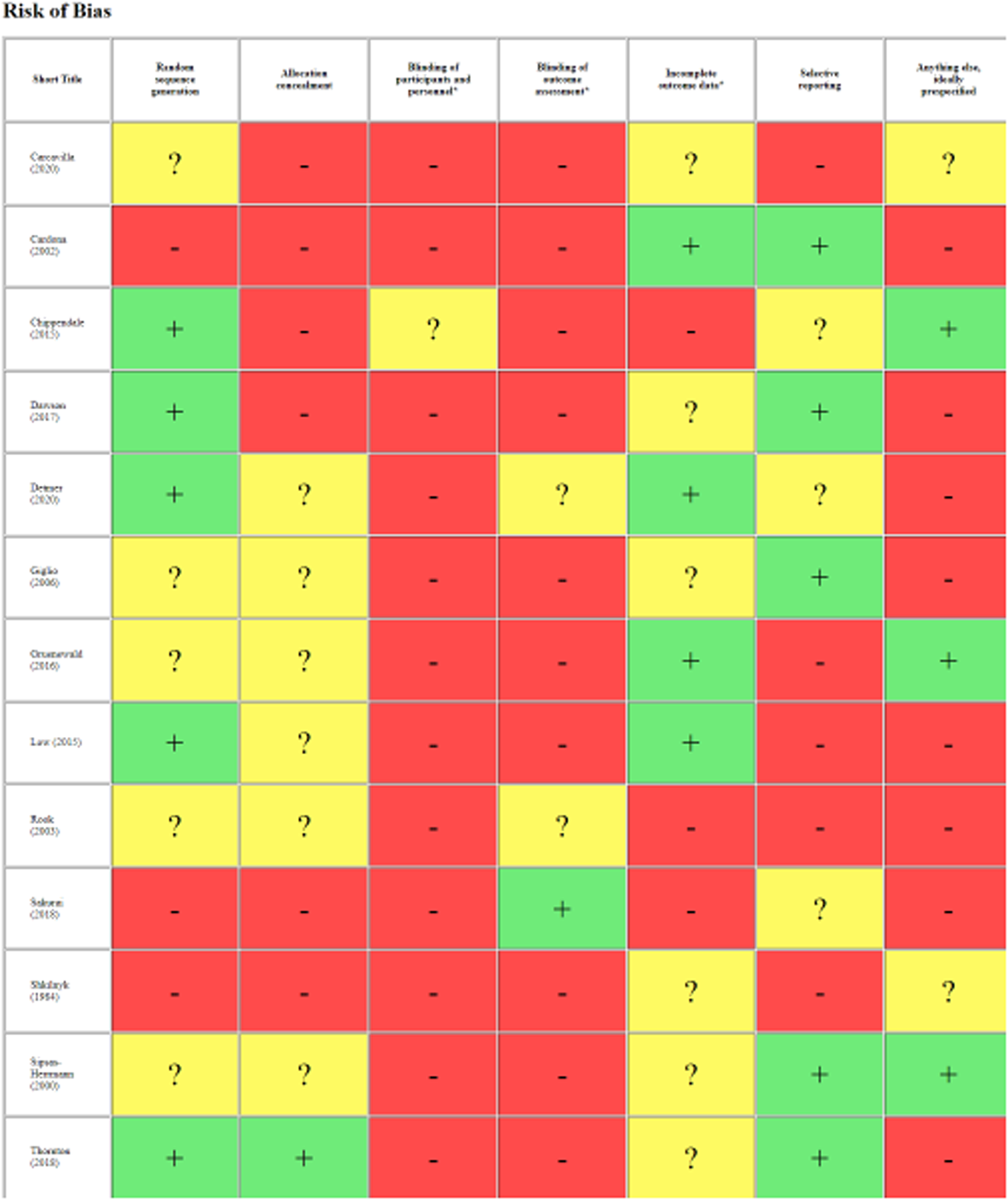
Risk of bias table.
Effects of interventions
Synthesis of results
We have structured this section of the report based on the original research questions asked.
Research Question 1: What is the effect of intergenerational interventions on the wellbeing and mental health of older people?
Primary outcomes
The range of outcomes reported in the studies included in this review varied greatly. The following six outcomes: depression (n = 3), anxiety (n = 1), quality of life (n = 2), self-esteem (n = 4), agitation (n = 1) and loneliness (n = 1), reflect the primary outcomes that we aimed to capture to assess mental health and wellbeing in older people. Social isolation was not captured in the included studies.
From the data collected from these studies we have been able to conduct a meta analysis for the outcomes of self-esteem (Figure 5) and depression (Figure 6). The interventions consist of different intergenerational activities, had measurements taken at different time points, and with only one study per activity as evidence we cannot imply that these results would be consistent across other studies. Random effects analysis has been used in the two meta-analyses listed below.
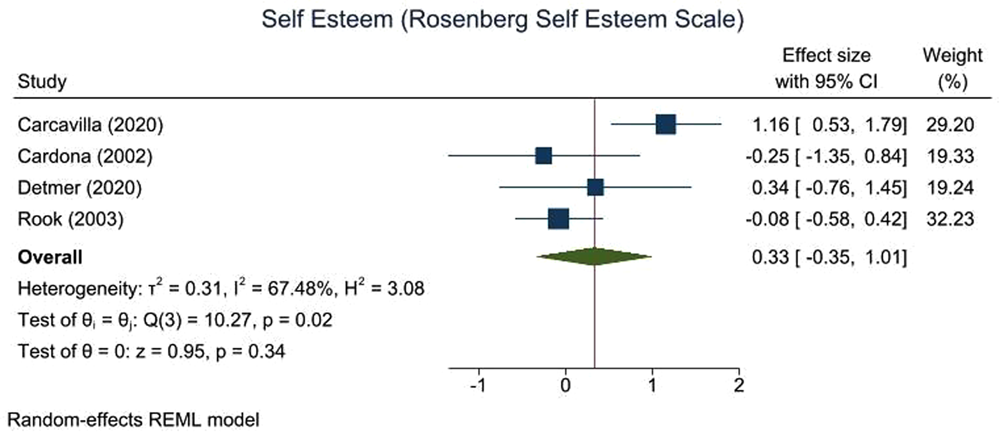
Self-esteem.
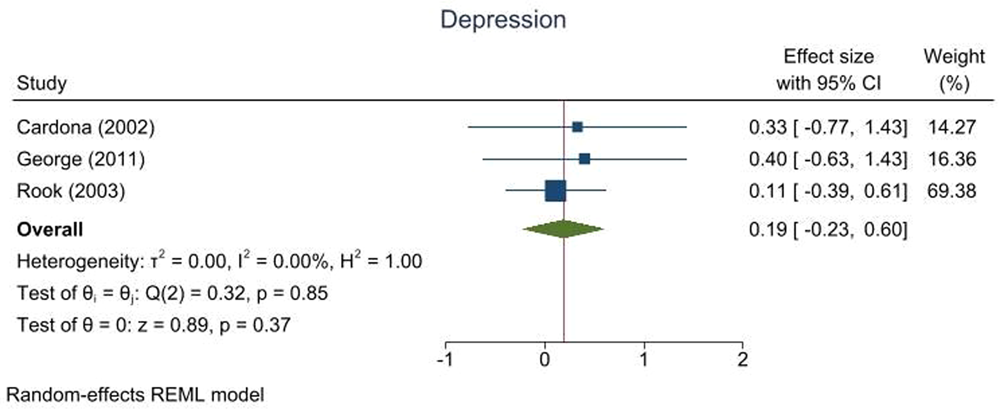
Depression.
Quality of life, stress, agitation and loneliness were all measured in only one study. Meta-analysis was therefore not possible; the effectiveness data are presented in Table 5.
Primary outcomes not in meta-analysis.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
The results of these studies suggest no effect or even some small negative effects (quality of life and loneliness) in older people taking part in intergenerational interventions.
Self-esteem
The results for self-esteem across four studies (n = 254 older people) suggest a non-statistically significant (ES: 0.33, 95% CI: −0.35, 1.01, I 2: 67.5%) trend towards small improvements in self-esteem for the older adults participating in an intergenerational intervention. The studies all used the Rosenberg Self Esteem Scale but measured the outcome at different time points. It is difficult to say if this change is clinically meaningful, but from a public health perspective at a general population level an effect size of 0.2 is considered a small and an effect size at 0.5 is considered a medium but meaningful change. Although the interventions were all Level 5 on the Depth of Engagement Scale (Kaplan, 2004) they involved a wide range of intergenerational activities. For example, one was a language learning activity with adolescents run online over 6 weeks, self-esteem was measured at 2 weeks postintervention (Carcavilla, 2020), one was a foster grandparent programme where older people visited children with long-term health conditions in hospital over 3 years, self-esteem was measured at 1 year postintervention (Rook, 2003), and two were visiting programmes—one based around music with pre-school children over 12 weeks Detmer 2020 and one based around specific joint projects (art, music or exercises) with older children over 3 weeks (Cardona, 2002), both with self-esteem measured at 1 week post intervention.
Depression
The results for depression across three studies (n = 208 older people) suggest little or no impact (ES: 0.19, 95% CI: −0.23, 0.60, I 2: 0%), with a range of intergenerational activities (though again all Level 5 on the Depth of Engagement Scale) (Kaplan, 2004) presented. It is difficult to say if this change is clinically meaningful, in one study (Cardona, 2002) the change in the intervention group was such that the older people went from reporting moderate levels of depression to mild levels of depression which might be considered meaningful, but their result did not differ significantly from the control group. From a public health perspective an effect size of 0.2 at a general population level is considered a small but meaningful change. Depression was measured using different tools and time points across the studies the Geriatric depression scale at 1 week post intervention (Cardona, 2002); the Beck Depression Inventory at 1 week post intervention (George, 2011); and the Centre for Epidemiological Studies-Depression scale at 1 year post intervention (Rook, 2003). One was a language learning activity with adolescents run online over 6 weeks (Cardona, 2002), one was a foster grandparent programme where older people visited children with long-term health conditions in hospital over 3 years (Rook, 2003), and one was an Intergenerational school with mixed ages of children running over 5 months (George, 2011). Although there is a trend towards some positive impacts on depression across the studies the results (both individually and collectively) are not statistically significant.
Secondary outcomes
The following 12 outcomes were reported in at least one study: positive and negative affect, agency, self-efficacy, self-worth, enjoyment, personal growth, behaviour (intergenerational interactions and engagement), cognitive activity, pleasure, sadness, community, and social activity. Indicators of mental health and wellbeing such as spiritual health and sense of community were not reported in any of the included studies. Due to the inconsistency in data and outcomes, meta-analysis was considered inappropriate.
We grouped the reported outcomes into summary themes: personal growth, cognitive function, community, affect and engagement/interaction. Groupings were developed and checked with stakeholders who broadly agreed with the names and groupings. The name ‘Personal growth’ for the first group of outcomes was reviewed a number of times, but we ultimately agreed to keep it as it was helpful to highlight that older people can benefit from personal growth too.
Personal growth
The outcomes included in this theme reflect concepts around personal growth or understanding of self. Seven studies measured 12 outcomes associated with aspects of personal growth, with effect sizes ranging from 0.18 (small) to 0.80 (large) providing some preliminary evidence that intergenerational interventions might have a positive effect on aspects of a person's sense of self. The results suggest that a person's sense of worth or utility or productivity can be increased by participating in an intergenerational intervention whether that be reminiscing and sharing stories with younger people (Chippendale, 2015), volunteering in schools more generally (George, 2011; Gruenewald, 2016) or working on specific tasks with children (Sipsas-Herrmann, 2000; Thornton, 2017) (Table 6).
Personal growth.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
Cognitive function
Cognitive function was measured in two studies (George, 2011; Sakuri, 2018) using the MMSE (Mini Mental State Examination) typically used to assess cognitive decline. In Table 7 we can see medium to large effect sizes indicating a cognitive benefit for those participating in an intergenerational intervention versus those taking part in an intervention without an intergenerational element. One study even finds positive impact on cognitive function after 6 years of the intervention (Sakuri, 2018)—suggesting potentially lasting effects at least for that particular intergenerational reading intervention (where older adults read picture books to school children aged 4–11years).
Cognitive function.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
Community
Outcomes centring around the impact of intergenerational interventions on the community were lacking with only two studies measuring community related aspects (Table 8). One study (Low, 2015) reported a reduction in the Brief Sense of Community Scale in older adults involved in an intergenerational intervention that involved children visiting a nursing home. The Brief Sense of Community Scale measures psychological sense of community such as group membership and shared emotional connection. In comparison, the other study (Rook, 2003) reported a large positive effect on the number of new relationships gained by those participating in that intergenerational intervention. Although the number of new relationships indicates an increasing community for an individual it may not reflect a ‘sense’ of community. Although both interventions involved children visiting older adults (one in a nursing home [Low, 2015] and the other in a hospital [Rook, 2003]), there are many possible reasons for the difference in findings, for example, the size of the sample (N = 40 vs. 108), the outcome measure used, the participant characteristics (older people vs. older people living with dementia) or the time point (1 week vs. 1 year).
Community.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
Affect
The theme ‘Affect’ reflects various elements of emotion, five aspects of affect were measured across three studies (Carcavilla, 2020; Dawson, 2017; Low, 2015). In Table 9 we can see that the effect sizes range from 0 to 0.64 (medium positive effect). Interestingly, the two studies we have data for both indicate a small-medium positive effect on positive emotions such as pleasure, and both report either no effect or a positive effect on negative emotions (i.e., reduce level of negative emotions in the intervention group [Carcavilla, 2020]). However, the interventions were different (one an online interaction for language practice [Carcavilla, 2020], the other a visiting programme in a nursing home [Low, 2015]) and engaged different populations (one with teenagers in education and older adults in a care home [Carcavilla, 2020], the other with pre-schoolers and older people living with dementia [Low, 2015]).
Affect.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
Engagement/interaction
A total of 12 different outcomes related to engagement in activities and intergenerational interactions were measured by four studies (Detmer, 2020; Giglio, 2006; Low, 2015; Shkilnyk, 1984). One study reports intergenerational interactions (Giglio, 2006) using eight measures including verbal interaction, spontaneous touching, spontaneous hand holding and spontaneous hugging, both during and shortly after a music intervention. Effect sizes range from 0.50 (medium effect) to 3.32 (large effect) although these results are from a small sample size. The results for level of engagement presented in Table 10 are a little more diverse with some positive trends and some negative—this may reflect the level of engagement required by an intervention or a change in activity or the way engagement is measured in a particular study. For example, active engagement appears to be lower than the control group in the final session of Grand Friends (Low, 2015) whereas in previous weeks it had been higher than the control group—the authors suggest this is due to a change in the activity in the final week which was a party—the usual structured activities were not in place.
Engagement/interaction.
Note: NB spontaneous tapping is a negative behaviour outcome the Effect size reported here suggests it is reduced with the intervention.
Abbreviations: 95% CI, 95% confidence interval; ES, effect size; N, sample size; SE, standard error.
Data on intergenerational interactions (or dyads) is missing from two studies (Detmer, 2020; Shkilnyk, 1984)—these interactions were observed over time but not compared to the control group within their studies. Both studies report an increase in intergenerational interactions over time.
Research Question 2: What characteristics of intergenerational activities are associated with a positive impact on the wellbeing and mental health of older people?
To address Research Question 2 we planned to use information on intervention characteristics such as setting, context, intensity, duration etc. However, due to the small number of eligible studies, and the variation in interventions and outcomes it has not been possible to determine which intervention characteristics are associated with a positive impact on the wellbeing and mental health of older people.
Research Question 3: What are the underlying theories for the effectiveness of intergenerational activities in older people?
In the literature regarding the theories behind intergenerational interventions several theories are highlighted, some more common than others (Jarrott, 2011; Kuenhe, 2014).
Many of the studies do not explicitly refer to named theories that have informed the development or logic of the intervention but use language or logic that reflects the notion or sentiment of relevant theories. Table 11 documents each intervention, its aim and the theories that are implicitly or explicitly cited within the papers. The most commonly reported (named) theory is Erikson's Theory of Psychosocial Development which was explicitly mentioned in three studies (Chippendale, 2015; Dawson, 2017; Sipsas-Herrmann, 2000). Kuenhe (2014) states ‘More specifically, it has been suggested that Erikson's seventh stage of psychosocial development, generativity versus stagnation, fits well with an intergenerational approach Kuenhe 2014. According to Erikson, generativity involves perceiving one's self as connected with a future that will survive and continue after one is gone, giving of self to the future, and a hope that the future is secure’ (Erikson, 1982 as cited in Kuenhe 2014). However, the most common theory implied by intervention logic descriptions is Contact Theory which was identified in 12 of the 14 intervention descriptions. Again, described by Kuenhe (2014) Contact Theory states ‘social contact between segregated groups can facilitate more accurate perceptions and reductions in prejudice, but suggest this occurs only under certain conditions….’ (Allport, 1954 as cited by Kuenhe, 2014) specifies four key conditions necessary for optimal contact: equal group status within the situation; common goals; intergroup cooperation; and the support of authorities, law, or custom (Kuenhe, 2014).
Implicit and explicit program theories.
As each intervention is, by its nature, complex it isn't unexpected to find multiple theories discussed within one intervention. It is concerning that named theories are not more evident in the literature—this suggests that those developing/testing interventions have not properly considered the underlying theory of change.
DISCUSSION
Summary of main results
This systematic review found 14 randomised controlled trials looking at the impact of intergenerational interventions on the mental health and wellbeing of older people. The quality of the trials and the length of follow-up is poor as is the reporting of equity characteristics. Many relevant outcomes have been studied but often with very little overlap across studies. The exceptions to this are the outcomes of self-esteem and depression which have been measured in three or more studies. The effect size for self-esteem indicates a small positive impact, the effect size for depression indicates little/no impact, but the results are not certain due to the small samples sizes and few studies available. The lack of overlap of outcomes and the lack of studies on similar interventions or interventions with similar elements means it is difficult to determine if any, one intervention or intervention characteristic is more or less effective for any given outcome. The primary objectives of many of these studies was not to influence wellbeing, nevertheless, there is some indication that wellbeing was improved. There are likely to be many factors that will influence participants wellbeing as a result of participating in these types of interventions (Jarrott, 2021).
However, this information is useful as it can help us to begin to understand if an intervention isn't appropriate for a particular setting, population activity or to achieve a particular outcome. For example, Grand Friends (Low, 2015) is an intergenerational intervention where young children visit older people living with dementia in their care home. The results we have been able to report for this study suggest that whilst this intervention may have been able to reduce levels of agitation and increase some reports of pleasure, it did not have the same beneficial effects on quality of life, sadness or improvements in engagement. The rationale for this intervention was that increased engagement during the activity would meet needs for meaningful activity and social engagement and result in improvements in quality of life and sense of community and in decreased agitation amongst those with dementia symptoms who participate in Grand friends in comparison to a control group with no interaction. This may indicate that whilst some of the desired outcomes were achieved—others were not, and that perhaps engagement during an activity was not the method by which this intervention works, or perhaps the activities set were not appropriate to promote the right level of engagement.
Overall completeness and applicability of evidence
Overall, the state of the evidence for intergenerational interventions is patchy with poor methodological quality. Consequently, it is difficult to describe what does and doesn't work to improve mental health and wellbeing outcomes in older adults using intergenerational activities. This is partly explained by the wide variation of interventions and intervention elements and characteristics. Although, as we see here, there are studies using randomised controlled trial designs—due to the complex nature of intergenerational interventions conducting studies of this kind is complicated and costly and often outcomes are only measured after a short follow-up period. This means that there are very few studies of effectiveness of these interventions, and we can't be confident of what the effects of intergenerational interventions are in older people. From the research presented here there are many gaps which still need to be filled. We need to understand much more about the different elements of interventions as well as the interventions as a whole, and we need to better understand what individual and community outcomes can be influenced by these and how. To date there is not enough information to have good summary level evidence of effectiveness. These gaps illustrate the challenges of standardising curricula and programming and being able to generalise findings across the natural variation of intergenerational interventions.
Whilst the theories identified in some of the included studies are described in the intergenerational literature more generally, many studies lacked detail of the named theories underlying the intervention.
Quality of the evidence
The overall quality of the evidence is poor. The most limiting factor being the blinding of participants, personnel and outcome assessment, allocation concealment and sample size. Although these trials may be demonstration projects testing to see if something works or not most failed to report power calculations to ensure the appropriate sample size was achieved. We also saw that the outcomes measured were so variable that a lot of the research could not be brought together in meta-analyses. More consistent and agreed measure for reporting outcomes would benefit future research in this area. We also noted that despite the intervention involving two groups of people, in some studies the younger generation were considered part of the intervention and so the impact of being involved in the intervention on them was not measured. This is a serious ethical consideration both in terms of participation of research and research waste.
Equity
We used the progress plus framework (O'Neill, 2014) to establish what information and characteristics were captured and/or targeted in this body of evidence. In summary, many of the equity characteristics were not reported. Commonly but inconsistently, reported characteristics of the populations involved in the studies were gender and race/ethnicity, with some reporting on levels of education and socioeconomic status, other personal characteristics that were commonly reported were cognitive decline and physical health impairments. However, although these characteristics are recorded they are not necessarily accounted for in the analysis or subgroup analysis of the results.
Potential biases in the review process
In this review we decided to only include randomised controlled trials as they provide the best evidence to address effectiveness questions and the EGM suggested there were sufficient studies available. However, due to the variability in the types of intergenerational intervention and the elements they consist of it is possible we are missing out on information that other study designs could have provided to further inform research questions 2 and 3. Future research should consider what the best study design might be and what information it is important to capture and how long for. Intergenerational interventions are by nature complex, so they need funding for the best and most informative research to be conducted, for example, pragmatic trial designs developed to evaluate complex social interventions may be applicable.
It is also interesting to note that most of the interventions included in the review were categorised as level 5 interventions (on the Depth of Engagement scale [Kaplan, 2004])—these are ongoing intergenerational activities over a defined period of time and are often implemented on an experimental or trial basis, and frequently depend on external funding. This is perhaps something that might be a construct of how long and for what research funding is provided. The impact is that we are missing evidence from trials that measure outcomes on a longer term basis and that many interventions only last while the research funding does which means the efforts behind setting up the intervention are lost along with the relationships that have formed and any other potential benefits.
The themes used in describing the outcomes were named by RW in an attempt to best capture and group the outcomes that were reported, these are the groupings and names we found helpful in this work. However, they could be re-grouped and re-named from another perspective.
Agreements and disagreements with other studies or reviews
In comparison to a similar review conducted in 2021 (Krzeczkowska, 2021) we found nine more randomised controlled trials in this area. However, our conclusions about the need for more research of a better standard is in agreement with theirs. Their review incorporates broader study designs, and although they suggest general trends and positive benefits on outcomes these can also not yet be formally concluded.
Similarly to Jarrott (2021) we noted the often small sample sizes, the need for more rigorous evaluation and the need to include outcomes measures for younger generation participants as well as parents and carers. Over the last 20 years several (∼10) theories have been identified as informing the development of intergenerational interventions (Jarrott, 2011; Kuenhe, 2014). In 2014 Kuehne (Kuenhe, 2014) found that over time the use of theories in intervention development is increasing and that of the 10 theories identified Contact theory and Erikson's theory of psychosocial development are the most commonly reported theories along with the Theory of personhood. Similarly, in the studies included in our review we found Erikson's theory of psychosocial development to be the most common named theory and Contact theory the most commonly implied theory (though the latter is subject to reviewer bias). Whilst not many of the ∼10 theories previously highlighted in the literature could be identified in the included studies in this review it is possible that elements of them and other theories are present, just not obviously identifiable. However, newly developed interventions would benefit from taking account of known theories and how they can influence the content, structure and outcomes of the interventions they intend to provide.
AUTHORS’ CONCLUSIONS
Implications for practice and policy
Intergenerational interventions show some promise but lack sufficient research across the variety of interventions and outcomes means we are unclear what their potential may be.
Plans for intervention sustainability would benefit any effective interventions (suggested or existing).
Commissioners and intervention developers should ensure interventions provide sufficient theoretical evidence for the logic behind the proposed intervention.
Commissioners and intervention developers should improve their consideration of equity within the interventions.
More understanding is needed on how best to measure community related outcomes and what is really meant by this.
Implications for research
Research on intergenerational interventions needs more consistent and agreed measures for reporting individual outcomes and community outcomes (core outcome sets).
More understanding is needed on how best to measure ‘community’ outcomes.
Trialists should be performing power calculations to adequately power studies to understand how interventions may impact different members of society differently (equity) and how any impact remains for the long term.
Research methods would benefit from establishing outcomes for a given population from a variety of perspectives to overcome issues of bias from the lack of blinding of measures recorded by self report.
Research on intergenerational interventions should measure outcomes for BOTH the older and younger population engaged in the intervention—these may or may not be the same outcomes reflected in both populations.
Further research is needed on the long term impact of interventions on outcomes (whether participants need to keep being involved in an ‘intervention’ to continue to benefit) and sustainability of interventions beyond the initial funding of the research project—our stakeholders highlighted that interventions that are initiated for research and then end (usually within a year) are not helpful.
Footnotes
ACKNOWLEDGEMENTS
We would like to acknowledge the engagement and support of our stakeholders: Professor Sir Muir Gray—Director of the Optimal Ageing Programme; Iain Lang—University of Exeter; Vicki Goodwin—University of Exeter; Jo Day—University of Exeter; Aideen Young—Centre for Ageing Better; Claire Goodman—University of Hertfordshire; Tracey Howe—Cochrane Campbell Global Ageing Partnership; Oliver Rashbrook Cooper—Public Health England; Kelvin Yates—AgeUK Cornwall; Nathan Hughes—University of Sheffield; Debbie Hanson—Sheffield City Council; Laura Abbott—Chilypep; Hannah Fairbrother—University of Sheffield; Kerry Albright—Unicef; Rachel Staniforth—Public Health; Girish Vaidya—Sheffield Children's NHS Foundation Trust; Sally Pearse—Sheffield University; and members of the Only Connect steering group.
CONTRIBUTIONS OF AUTHORS
Content: ERC is a practitioner and consultant based in Plymouth and Project Manager at The Sensory Trust where she works on the Creative Spaces in the Community Project. This project uses nature and outdoor spaces to encourage older people with dementia to become more active, build social networks and foster independence. Previously she founded the multi-award winning Penryn Memory Café and led a memory café in York for 2 years whilst at University. She has recently completed the International Certificate in Intergenerational Practice provided by Generations Working Together and the University of Granada. SC is Commissioning Manager at NHS Kernow Clinical Commissioning Group and has an interest in the role of intergenerational programmes and activities in health and social care. RS is an advanced public health specialist at Cornwall Council with an interest in the role of intergenerational programmes and activities in health and social care specifically in relation to the mental health of older adults. RF is an older man living with dementia who has experience of intergenerational programmes. Systematic review methods: JTC is an expert in evidence synthesis and health policy research. She is co-chair and editor of the Ageing Group of the Campbell Library and co-director of the Cochrane Campbell Global Ageing Partnership. RW is an expert in evidence synthesis methods. FC is editor of the Children and Adolescent Group of the Campbell Collaboration. She has over 20 years of experience in evidence synthesis. DK is an expert in synthesising evidence for social policy and developing methods to enhance the use of evidence in decision making. GJMT is an expert in evidence synthesis with skills in quantitative and qualitative synthesis methods. RG is an expert in qualitative synthesis methods. Statistical analysis: GJMT is an expert in evidence synthesis with skills in quantitative and qualitative synthesis methods. Information retrieval: MR is an information specialist with experience in health services research, methods editor for the Ageing Group of the Campbell Library and a member of the Campbell Information Retrieval Methods Group. AS is a Senior Information Specialist, with extensive experience of literature searching and information management for systematic reviews and other types of evidence syntheses on a wide range of topics.
DECLARATIONS OF INTEREST
ERC, members of our advisory group and members of the Only Connect steering group are involved in the delivery of intergenerational activities and programmes.
PRELIMINARY TIMEFRAME
We plan to submit the systematic review for peer review in December 2022.
PLANS FOR UPDATING THIS REVIEW
Once completed the systematic review will be updated as resources permit.
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
In our protocol we said we would set up automated search alerts to identify additional relevant literature which we will use to update the map as the project progresses; any studies identified by this process will be screened for eligibility in both the map and the review, however this has not yet been completed.
We used the Cochrane Risk of Bias tool instead of ROB2 as the variation in the outcomes reported (and therefore inability to group outcomes for meta-analysis) was such that the extra level of detail required in the ROB2 seemed disproportionate to the value that it would give for the synthesis required in this review.
As well as extracting information on the theories identified by the authors of the studies we also attempted to identify theories that were implied in the text, though we accept there are weaknesses to this approach.
PUBLISHED NOTES
|
|
| Risk of bias table |
| Cardona 2002 |
|
|
| Risk of bias table |
| Chippendale 2015 |
|
|
| Risk of bias table |
| Dawson 2017 |
|
|
| Risk of bias table |
| Detmer |
|
|
| Risk of bias table |
| George 2011 |
|
|
| Risk of bias table |
| Giglio 2006 |
|
|
| Risk of bias table |
| Gruenewald 2016 |
|
|
| Risk of bias table |
| Low 2015 |
|
|
| Risk of bias table |
| Rook 2003 |
|
|
| Risk of bias table |
| Sakuri 2018 |
|
|
| Risk of bias table |
| Shkilnyk 1984 |
|
|
| Risk of bias table |
| Sipsas-Herrmann 2000 |
|
|
| Risk of bias table |
| Thornton 2017 |
|
|
| Risk of bias table |
| Footnotes |
| Characteristics of excluded studies |
| Carlson 2008 |
|
|
| Fried 2004 |
|
|
| Footnotes |
|
|
|
|
|
|
|
|
Sally Chan |
|
|
|
|
The INTErGenerational intervention taRgeting fraIlTY trial (INTEGRITY) |
|
|
|
|
|
|
|
|
SOURCES OF SUPPORT
No sources of support provided
NIHR, UK
The systematic review is funded by the National Institute for Health Research (NIHR) Evidence Synthesis Programme NIHR 133097 and NIHR 133172 and supported by the National Institute for Health Research (NIHR) Applied Research Collaboration South West Peninsula. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
REFERENCES
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.