
Abstract
Background
Social isolation and loneliness can occur in all age groups, and they are linked to increased mortality and poorer health outcomes. There is a growing body of research indicating inconsistent findings on the effectiveness of interventions aiming to alleviate social isolation and loneliness. Hence the need to facilitate the discoverability of research on these interventions.
Objectives
To map available evidence on the effects of in-person interventions aimed at mitigating social isolation and/or loneliness across all age groups and settings.
Search Methods
The following databases were searched from inception up to 17 February 2022 with no language restrictions: Ovid MEDLINE, Embase, EBM Reviews—Cochrane Central Register of Controlled Trials, APA PsycInfo via Ovid, CINAHL via EBSCO, EBSCO (all databases except CINAHL), Global Index Medicus, ProQuest (all databases), ProQuest ERIC, Web of Science, Korean Citation Index, Russian Science Citation Index, and SciELO Citation Index via Clarivate, and Elsevier Scopus.
Selection Criteria
Titles, abstracts, and full texts of potentially eligible articles identified were screened independently by two reviewers for inclusion following the outlined eligibility criteria.
Data Collection and Analysis
We developed and pilot tested a data extraction code set in Eppi-Reviewer. Data was individually extracted and coded. We used the AMSTAR2 tool to assess the quality of reviews. However, the quality of the primary studies was not assessed.
Main Results
A total of 513 articles (421 primary studies and 92 systematic reviews) were included in this evidence and gap map which assessed the effectiveness of in-person interventions to reduce social isolation and loneliness. Most (68%) of the reviews were classified as critically low quality, while less than 5% were classified as high or moderate quality. Most reviews looked at interpersonal delivery and community-based delivery interventions, especially interventions for changing cognition led by a health professional and group activities, respectively. Loneliness, wellbeing, and depression/anxiety were the most assessed outcomes. Most research was conducted in high-income countries, concentrated in the United States, United Kingdom, and Australia, with none from low-income countries. Major gaps were identified in societal level and community-based delivery interventions that address policies and community structures, respectively. Less than 5% of included reviews assessed process indicators or implementation outcomes. Similar patterns of evidence and gaps were found in primary studies. All age groups were represented but more reviews and primary studies focused on older adults (≥60 years, 63%) compared to young people (≤24 years, 34%). Two thirds described how at-risk populations were identified and even fewer assessed differences in effect across equity factors for populations experiencing inequities.
Authors’ Conclusions
There is growing evidence that social isolation and loneliness are public health concerns. This evidence and gap map shows the available evidence, at the time of the search, on the effectiveness of in-person interventions at reducing social isolation and loneliness across all ages and settings. Despite a large body of research, with much of it published in more recent years, it is unevenly distributed geographically and across types of interventions and outcomes. Most of the systematic reviews are of critically low quality, indicating the need for high quality reviews. This map can guide funders and researchers to consider the areas in which the evidence is lacking and to address these gaps as future research priorities.
PLAIN LANGUAGE SUMMARY
This evidence and gap map on in-person interventions to reduce social isolation and loneliness across all age groups found few studies of societal-level interventions, most research was from high income countries and the available reviews were of low quality
The EGM in brief
This report discusses the effectiveness of in-person interventions to reduce social isolation and loneliness in people across all ages. It emphasizes that the available evidence is not consistent and varies in support of interpersonal and community-based delivery interventions and health-related outcomes (loneliness, wellbeing, depression/anxiety), with most evidence coming from high-income countries.
What is this EGM about?
Social isolation and loneliness are becoming more significant public health issues associated with increased deaths and poorer health outcomes.
In-person interventions can help people who are at risk of feeling socially isolated and lonely by teaching them how to maintain their existing connections or form new ones. Policy makers are interested in knowing which interventions are effective in reducing social isolation and loneliness.
What is the aim of this EGM?
To present available evidence from systematic reviews and primary studies about the effects of in-person interventions to reduce social isolation and/or loneliness across all ages and settings.
What studies are included?
The EGM included 513 articles comprising 421 primary studies and 92 systematic reviews that evaluate the effectiveness of in-person interventions for reducing social isolation and/or loneliness. The studies had to report on the effect of in-person interventions and could be conducted in any setting.
What are the main findings of this gap map?
The evidence in this EGM varies with more evidence for interpersonal and community-based delivery interventions than interventions delivered at societal levels. Most measured outcomes include health-related outcomes of loneliness, well-being, and depression/anxiety. Specifically, there are evidence clusters for community-based interventions of group activities and interpersonal delivery interventions for changing negative thinking and feelings about social relationships. Most evidence comes from high-income countries including the US, UK, and Australia, with none from low-income countries. Most systematic reviews included in this EGM are of critically low quality, with less than 5% of high or moderate quality.
Less than 5% of included reviews reported outcomes about how well the interventions were implemented. Only two primary studies and one review assessed interventions delivered at the societal level and only one review assessed interventions for age-friendly communities.
While all age groups were represented, more reviews and primary studies were interested in older adults (60 years or above, 63%) than young people (24 years or below, 35%). Very few described how they identified people who were at-risk and even fewer assessed whether the effects of the interventions were different for populations experiencing inequities.
What do the findings of the map mean?
This EGM is a step toward identifying effective in-person interventions for reducing social isolation and loneliness for all age groups. Though a large body of evidence exists, with much of this research from more recent years, it shows variations, with a lack of high quality reviews. The map contributes to building an evidence base in the field by which funders and researchers can identify gaps in the evidence and then address these as future research priorities.
How up-to-date is this EGM?
We searched for relevant studies up until 17 February 2022.
BACKGROUND
Introduction
The problem, condition, or issue
Social isolation is the objective lack or paucity of social contact and infrequent interactions with others (Badcock et al., 2022; Donovan et al., 2020; Leigh-Hunt et al., 2017). Loneliness is a related concept defined as the subjective, negative feeling of inadequate meaningful connections resulting from an unmet need or discrepancy between desired and actual social relationships (Perlman et al., 1981; Prohaska et al., 2020). Loneliness has two components: an emotional component (unpleasant, negative feeling) and a social cognition component (perception of social disconnection from other people with a desire to be connected) (Badcock et al., 2022). Loneliness can also be a transient normal experience or chronic with negative physical and mental health consequences (Akhter-Khan et al., 2020; Qualter et al., 2015).
The two concepts, social isolation, and loneliness, are distinct; social isolation is objective and associated with social contact while loneliness is subjective and related to social connectedness (O'Rourke et al., 2018). One may occur without the other, although they are related and may also co-occur. People may have a large social network and feel lonely, while some with a small network may not.
Social isolation and loneliness can occur across all age groups and are associated with serious health consequences including anxiety and depression, cardiovascular disease, and premature mortality (Cené et al., 2022; Leigh-Hunt et al., 2017). One German cohort study of nearly 5000 middle-aged and older adults found that the risk of mortality is exacerbated when social isolation and loneliness co-occur (Beller et al., 2018). Poor relationships are associated with 32% increased risk of stroke, 29% increased risk of coronary heart disease (Cené et al., 2022; Valtorta et al., 2016), and 26% increased risk of all-cause mortality (Donovan et al., 2020; Holt-Lunstad et al., 2015). Incident depression and dementia have a bi-directional relationship with both social isolation and loneliness (Cené et al., 2022; Donovan et al., 2020) although several studies have reported that dementia is associated with loneliness than social isolation (Cené et al., 2022; Holwerda et al., 2014; Rafnsson et al., 2020). Both social isolation and loneliness are associated with negative health-related behaviors such as smoking and physical inactivity (Cené et al., 2022; Menec et al., 2020). The negative health impacts of social isolation and loneliness have been shown to increase health and social care service use (Cotterell et al., 2018; Windle et al., 2012). These negative impacts occur when contextual and risk factors affecting social relationships persist and individuals do not use appropriate coping strategies to address them (Akhter-Khan et al., 2022; Elder et al., 2012).
Since the onset of the COVID-19 pandemic, movement restriction policies have made social isolation and loneliness prominent global issues and a public health priority (Galvez-Hernandez et al., 2022; Holt-Lunstad 2022; WHO, 2021). The prevalence of severe loneliness increased by 15% and social isolation by 13% in adults 18 years or older across 101 countries during the pandemic (O'Sullivan et al., 2021). Small increases in the prevalence of loneliness were also observed in a recent synthesis of longitudinal studies during the COVID-19 pandemic (Ernst et al., 2022). The prevalence is hard to measure across the lifespan because of the lack of standardized measurement instruments and definitions, and the use of different cut-off points and age categories (Holt-Lunstad, 2022; Prohaska et al., 2020). A recent systematic review and meta-analysis on the prevalence of loneliness pre-COVID-19 pandemic across 113 countries (Surkalim et al., 2022) showed varying rates for adolescents (9.2% to 14.4%), young adults (1.8% to 9.4%), middle-aged adults (2.4% to 12%), and older adults (4.2% to 24.2%) depending on the country. A prevalence study in a German population-based adult cohort showed that social isolation increases with age from 5.4% (95% confidence interval [CI]: 4.7 to 6.0) in the youngest age group (18 to 39 years) to 21.7% (95% CI: 19.5 to 24.0) in the oldest age group (70 to 79 years) (Röhr et al., 2021). The global prevalence of social isolation in community-dwelling older adults was found to be 25% (95% CI: 21 to 30) (Teo et al., 2022). Studies have found a u-shaped association between age and loneliness with the highest levels of loneliness in younger and older people (Lasgaard et al., 2016; Yang et al., 2011), but few studies have focused on younger people. Although social isolation and loneliness are global issues, most of the studies were conducted in high income countries, especially in Europe, with very few in low-middle-income countries (Fakoya et al., 2020; Surkalim et al., 2022).
Both social isolation and loneliness are linked to less social support and can be triggered by situational factors such as adversity, significant life changes or transitions, such as moving away from home, starting a new job, becoming a parent, illness, and the death of a spouse or parent (Badcock et al., 2022; Elder et al., 2012; Lim et al., 2020; Qualter et al., 2022). They are associated with risk factors including individual factors (e.g., personality, maladaptive cognition, poor health, disability or mobility impairment, cognitive impairment), interpersonal or social factors (e.g., peer victimization or discrimination, poor relationship quality, quantity of friends or social contacts, living alone), socio-environmental factors (e.g., neighborhood deprivation, inaccessible location of residence, housing, cultural prejudice), and demographic factors (e.g., age, gender, educational level, low socio-economic status, unemployment) (Badcock et al., 2022; Elder et al., 2012; Lim et al., 2020; O'Sullivan et al., 2021; Qualter et al., 2022).
Many systematic reviews have evaluated the effectiveness of interventions to reduce social isolation or loneliness with conflicting findings demonstrating a need for better quality research (Masi et al., 2011; Victor et al., 2018; Williams et al., 2021). A number have focused on older adults, but social isolation and loneliness affect people across the life span, including young people (Qualter et al., 2015; Surkalim et al., 2022), with interventions designed specifically for them (Eccles et al., 2021). Most of the reviews have focused on people living in the community or long-term care settings (Fakoya et al., 2020; Grenade et al., 2008). There is limited research addressing social isolation and/or loneliness for patients in clinical settings (NASEM, 2020). Studies that consider hospitalized patients focus on screening and detection of loneliness and social isolation, the impact of social isolation and loneliness on health service use and which interventions may be used; hardly any focus on assessing the effectiveness of interventions to reduce social isolation and loneliness (Grenade et al., 2008; NASEM, 2020; Proffitt et al., 1993; Razai et al., 2020; Zamir et al., 2018).
The impact of interventions has been found to differ depending on population characteristics such as coping skills, needs, degree of loneliness, and contextual factors like age, socioeconomic status, health condition, and place of residence (Fakoya et al., 2020). Therefore, there is no one-size-fits-all approach, and it is important to tailor appropriate interventions to individuals’ needs and contexts (Akhter-Khan et al., 2020; Fakoya et al., 2020; Mann et al., 2017).
There are health equity issues related to social isolation and/or loneliness such as the gap in evidence from low-middle income countries (Surkalim et al., 2022), limited access to interventions caused by disabilities and lack of transportation, or limited programs in rural areas compared to urban areas (Dassieu et al., 2021; NASEM, 2020; Qualter et al., 2022). Social isolation and/or loneliness related to structural inequities (e.g., intersectional discrimination across race, gender, socioeconomic status; age-based discrimination and ethnic minorities), have a negative impact on health outcomes (Dassieu et al., 2021).
This current evidence and gap map identifies areas where evidence is available, as well as any gaps in research related to in-person interventions for social isolation and loneliness across any age.
The intervention
Different types of interventions for reducing social isolation (Dickens et al., 2011; Findlay, 2003), loneliness (Cohen-Mansfield et al., 2015; Eccles et al., 2021; Hagan et al., 2014; Jarvis et al., 2020; Mann et al., 2017; Masi et al., 2011; Veronese et al., 2021), or both social isolation and loneliness (Cattan et al., 2005; Gardiner et al., 2018; Poscia et al., 2018) have been described and assessed in several systematic and scoping reviews. However, there is a lack of a standardized framework for describing these interventions (Fakoya et al., 2020; Prohaska et al., 2020). Interventions for reducing social isolation and loneliness are often complex with multiple and interacting components, working through different potential mechanisms of action (Fakoya et al., 2020; Gardiner et al., 2018).
Several approaches have been used to categorize interventions in some reviews. The interventions have been categorized by the format or delivery mode or type as one-on-one or group-based (Cohen-Mansfield et al., 2015; Dickens et al., 2011; Fakoya et al., 2020; Findlay, 2003; Hagan et al., 2014; Masi et al., 2011; Poscia et al., 2018), or technology or non-technology (in-person) based (Eccles et al., 2021; Masi et al., 2011). They have also been categorized by the type, or strategy, being classified as interventions for social skills training, enhancing social support, enhancing social interaction or social cognition training (Masi et al., 2011). Other terms have been used as a rationale for categorization, such as the focus, nature or goal of the intervention (Cohen-Mansfield et al., 2015; Fakoya et al., 2020; Masi et al., 2011); the purpose, intended outcomes, and mechanisms by which interventions target social isolation and loneliness (Fakoya et al., 2020; Gardiner et al., 2018).
The scoping review by Mann et al. classifies interventions as direct (i.e., targeting loneliness and related concepts) or indirect (targeting wellbeing which impacts loneliness), and also articulates various levels of engagement for those delivering the interventions following the socio-ecological model: individual level, relationship and community level, and societal level (Mann et al., 2017).
Another scoping review (O'Rourke et al., 2018) classified interventions for reducing loneliness by their components into nine types: one-to-one personal contact, activity group, animal contact, skills course interventions, or varied/non-specific interventions, reminiscence, support group, model of care and public broadcast.
This evidence and gap map focuses on in-person interventions that are non-technology based and delivered face-to-face since there is a gap map on digital interventions for older adults (Welch et al., 2022b).
Why it is important to develop the EGM
The existing body of evidence for interventions to mitigate social isolation and/or loneliness is rapidly growing and characterized by small, low-quality trials, with inconsistent terminology and conclusions on their effectiveness (Eccles et al., 2021; Fakoya et al., 2020; Prohaska et al., 2020; Veronese et al., 2021) as well as equity-related issues. With the rapid growth of evidence in this sector, this evidence and gap map will demonstrate areas where evidence is available and areas where there are gaps that researchers, decision and policymakers could use to help select interventions and prioritize future research to fill gaps in research and to understand which interventions might work in which conditions. It will also improve the discoverability of evidence on different types of interventions and enhance their use for informed decision-making by stakeholders including health and social care providers, policymakers, citizens, caregivers, and patients.
Existing evidence and gap maps and/or relevant systematic reviews
There is rapidly expanding research on alleviating social isolation and/or loneliness since the COVID-19 pandemic. Several relevant systematic reviews have been conducted and included in three umbrella reviews (Boulton et al., 2021; Jarvis et al., 2020; Veronese et al., 2021). Boulton et al. found mixed evidence of effectiveness on loneliness for remote befriending, social support, and low intensity psychosocial interventions. Jarvis assessed various interventions addressing loneliness in older adults and found limited effect, with the greatest effect in a social cognition intervention. Veronese et al. reported low or very low-quality evidence of three interventions (meditation/mindfulness, social cognitive training, and social support) that reduced loneliness. A scoping review of reviews showed the lack of studies conducted in low-middle income countries (Fakoya et al., 2020).
One evidence and gap map has been conducted on remotely delivered digital interventions including befriending, social support, and low-intensity psychosocial interventions for social isolation and loneliness in older adults (Boulton et al., 2021). It showed mostly low-quality reviews and few studies on older people who are not caregivers or who do not have a particular chronic illness. Our group is currently working on another gap map on digital interventions for older adults with a broader scope of interventions and including caregivers (Welch et al., 2022; Welch et al., 2022b), but there is currently no mapping of evidence for in-person interventions to reduce social isolation and loneliness across all ages.
OBJECTIVES
This EGM aims to map available evidence on the effects of in-person interventions to reduce social isolation and/or loneliness across all age groups in all settings.
Specific objectives are as follows: To identify existing evidence from primary studies and systematic reviews on the effects of in-person interventions that are non-technology based and delivered face-to-face to reduce social isolation and/or loneliness across all age groups. To identify research evidence gaps for new high-quality primary studies and systematic reviews. To highlight evidence of health equity considerations from included primary studies and systematic reviews.
METHODS
We followed the Campbell Collaboration guidance for producing an evidence and gap map (White et al., 2020) described in our protocol (Welch et al., 2023).
Evidence and gap map: Definition and purpose
Evidence and gap maps are a systematic evidence synthesis product with a visual presentation of existing evidence relevant to a specific research question (Snilstveit et al., 2013; White et al., 2020). They display areas where evidence is available, areas where there are gaps in evidence, and the quality of existing evidence.
The evidence and gap map is typically a two-dimensional matrix with interventions as row headings and outcomes as column headings (Snilstveit, 2016; White et al., 2020). The studies with evidence on the corresponding intervention and outcome are shown within each cell of the matrix. This map will identify areas of evidence and any gaps in research related to using in-person interventions for social isolation and/or loneliness across all ages.
Framework development and scope
We developed an intervention-outcome framework by adapting our conceptual framework from the digital interventions EGM (Welch et al., 2022). We expanded the non-digital intervention and outcome categories to attain evidence-based, clear and distinct categories that are practical and useful to a broad audience by using several existing frameworks, reports, and reviews.
In consultation with stakeholders, we identified and reviewed other frameworks including the framework described by Masi (Masi et al., 2011), the framework for the Campaign to End Loneliness by Jopling (Jopling, 2020), the framework by Mann (Mann et al., 2017), the socio-ecological framework adapted by the World Health Organization for strategies to reduce social isolation and loneliness (WHO, 2021), the framework for evidence-based interventions for youth reporting loneliness (Qualter et al., 2022), and the social relationship expectations framework (Akhter-Khan et al., 2022). We also considered the National Academies of Sciences, Engineering, and Medicine Consensus study report on social isolation and loneliness in older adults (NASEM, 2020), the American Association of Retired Persons (AARP) Foundation report on social isolation (Elder et al., 2012), the taxonomy to evaluate social isolation and loneliness interventions developed by the Foundation for Social Connection, and three reviews on loneliness (Holt-Lunstad, 2022; Lim et al., 2020; Ogrin et al., 2021).
Six of the existing frameworks and reviews have adopted the socio-ecological framework when considering interventions to reduce social isolation and/or loneliness (Holt-Lunstad, 2022; Lim et al., 2020; Mann et al., 2017; Ogrin et al., 2021; Qualter et al., 2022; WHO, 2021). The socio-ecological framework has been used to explore the complex dimensions of other public health issues like violence and abuse (CDC, 2015; WHO, 2002) and health promotion (Wold et al., 2018). The model examines the relationship between risk and protective factors at different levels of influence including individual, relationship, community, and societal levels. The individual level focuses on personal characteristics that increase risks. The relationship level focuses on risk factors involving close social relationships with family and friends. The community level explores risk factors from wider social relationships in community settings such as schools, workplaces, and neighborhoods. The societal level of influence considers broad societal risk factors such as policies and cultural norms.
Social isolation and loneliness are associated with the lack of meaningful social connections which can occur at any of these four levels (Holt-Lunstad, 2018, Holt-Lunstad, 2022; Lim et al., 2020; Ogrin et al., 2021). Risk factors for social isolation and loneliness can be co-occurrent, inter-related, and can operate at multiple levels (Holt-Lunstad, 2022; Lim et al., 2020; Qualter et al., 2022). Interventions may target risk factors at multiple levels of the socio-ecological model by creating and maintaining meaningful social connections or a combination of other mechanisms, such as changing negative social cognition (i.e., changing negative thinking and feelings about social relationships) or providing support to enhance social interactions.
We considered non-technology-based interventions delivered in-person to alleviate social isolation and/or loneliness across all age groups in all settings. None of the existing frameworks or taxonomies provide mutually exclusive categories and subcategories for classifying the interventions for this evidence and gap map. They all demonstrate the complexity, diversity, and interdependencies of contextual or risk factors, and mechanisms that shape social relationships.
We therefore focused on delivery and classified interventions into five main categories based on who is providing the intervention and where it is provided: self-delivery, interpersonal delivery, community-based delivery, societal-level delivery, and multi-component or complex interventions. These intervention categories are further described in the conceptual framework.
Outcomes were based on the level of impact of interventions. The impact of social isolation and loneliness interventions depend on how well they were implemented, therefore, we considered both process indicators or implementation outcomes and other outcomes including health and psychosocial outcomes, indicators of social connections as well as cost and cost-effectiveness outcomes (Jopling, 2020; Windle et al., 2012). See Glossary of terms in Supporting Information Appendix 1.
Stakeholder engagement
We established an Advisory Board of key stakeholders to contribute toward defining the scope and developing the framework for the map as well as interpreting the findings. They include academics, advocates, policy and decision-makers, from relevant organizations (e.g., WHO, Canadian Red Cross, Global Initiative on Loneliness and Connection, US Foundation for Social Connection, and Ending Loneliness Together) who are involved in research and working to address social isolation and loneliness.
The Advisory Group met virtually on December 13 and 16, 2021 to discuss the scope of the evidence and gap map and existing frameworks that could be considered in developing the intervention-outcome framework for this evidence gap map. They met again in June 2022 to provide feedback on the framework. They were consulted by email to provide feedback on the revised framework and on the preliminary findings and draft map.
Conceptual framework
The conceptual framework (Figure 1) considers possible pathways for interventions to bring about expected changes and outcomes based on the understanding of the population risk factors and needs that may trigger social isolation or loneliness. It is based on theoretical underpinnings with the following key components: population contexts, risk factors, and needs that may trigger social isolation or loneliness. types of interventions required to address social isolation or loneliness, the mechanisms of change by which the interventions address social isolation or loneliness, and process indicators (e.g., acceptability) and outcomes (e.g., loneliness).
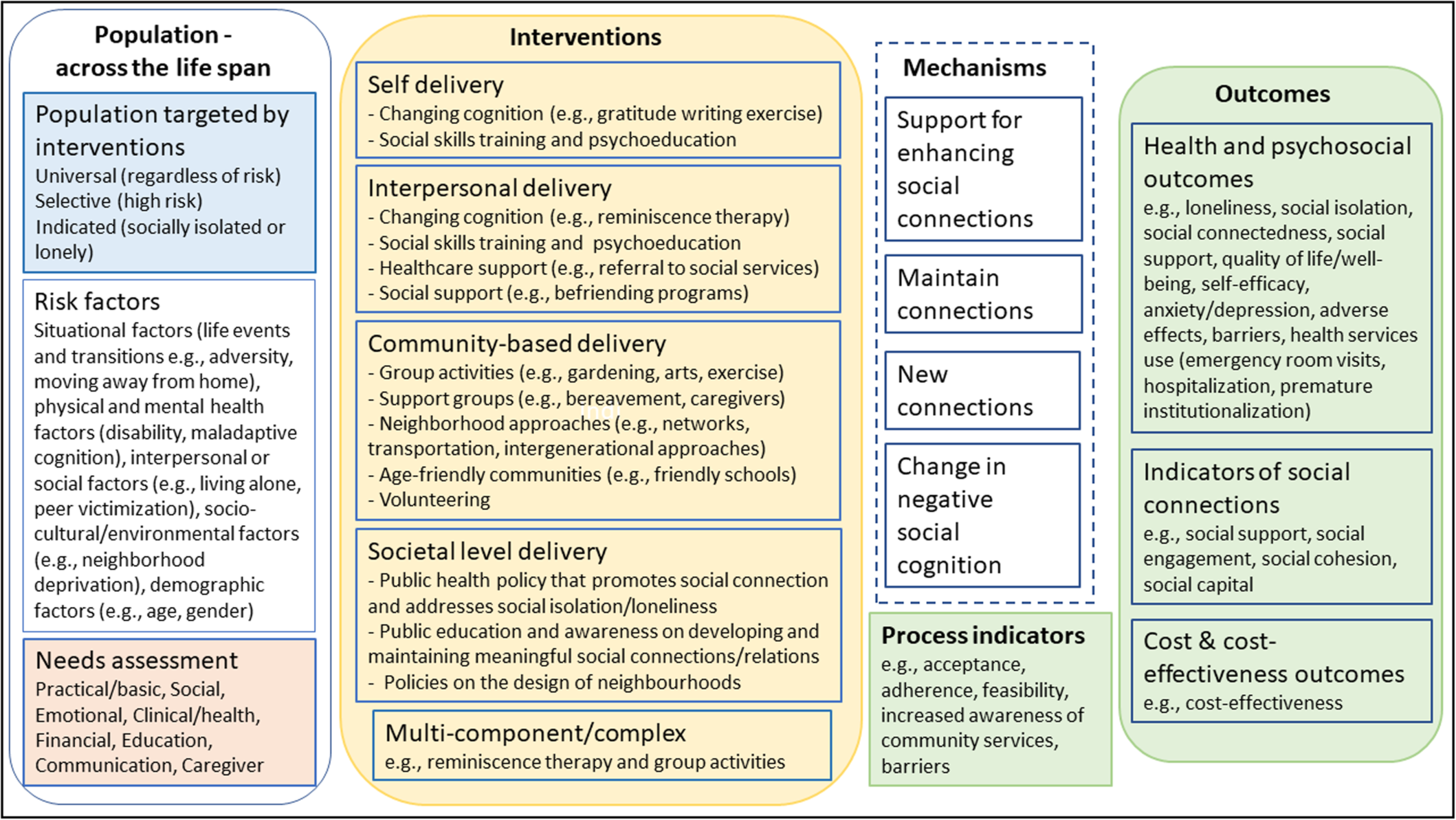
Conceptual framework.
Population targeted by interventions
Social isolation and loneliness are complex public health issues and their occurrence across the lifespan is influenced by individual contextual and risk factors, needs, expectations, and coping skills which are all inter-related and influence relationship ties (Akhter-Khan et al., 2022; Elder et al., 2012; Gardiner et al., 2018; O'Rourke et al., 2018; Qualter et al., 2022). Contextual and risk factors such as structural changes that may cause displacement (e.g., moving schools or wars), living situations (e.g., living alone or in a care facility such as orphanage, long-term care home), resources (available activities or social supports) affect people's motives, expectations, coping skills, and social relationships. Coping skills and social supports may be a protective factor if they allow people to promote their wellbeing or resilience. On the other hand, inadequate coping skills and social supports may be a risk factor for social isolation or loneliness.
Based on a public health approach, interventions may target anyone regardless of risk (universal), or target subpopulations at high risk (selective) or socially isolated or lonely people (indicated) (Springer et al., 2007). Categorizing target populations into these three orders gives a clearer picture and understanding of whom to prioritize and how to allocate resources more efficiently.
Risk factors
Social isolation or loneliness may be triggered in both young and old across the life span by situational factors such as significant life events or transitions (e.g., adversity, moving away from home, retirement, death of a spouse, friend, or relative) and may be associated with risk factors including physical and mental health factors (e.g., poor health, maladaptive cognition or cognitive decline, disability or impaired mobility, personality), interpersonal or social factors (e.g., living alone, peer victimization, social contacts, relationship quality), socio-cultural or environmental factors (e.g., neighborhood deprivation, inaccessible location of residence, cultural individualism, social discrimination, and stigma) and demographic factors (e.g., age, gender, socio-economic status) (Dahlberg et al., 2022; Elder et al., 2012; Lim et al., 2020; NASEM, 2020; Qualter et al., 2022).
Needs assessment
Socially isolated and lonely individuals across the lifespan may have unmet needs that can be due to low social support or disruption in social interactions with people at different levels—individual, group, community, or societal (Elder et al., 2012; Holt-Lunstad, 2022; NASEM, 2020; WHO, 2021). These needs may include basic needs (housing, nutrition and food security, and healthcare), social and emotional needs (social connections and companionship), financial, education (skills development and learning), communication, caregiver needs, home modifications and maintenance, domestic assistance, mobility, personal care, respite care and civic engagement (meaningfulness and status, the need for having a purpose in later life or being able to contribute usefully to society) (Abdi et al., 2019; Bedney et al., 2010; Bee et al., 2014; Eccles et al., 2021).
Social support is a major component of social connection and may be provided to meet different needs. Social support can take the forms of instrumental/tangible, informational, emotional, or belonging support (Elder et al., 2012; Holt-Lunstad, 2022; NASEM, 2020). It can be perceived, or actual support provided through social connections with other people and through different sectors including health, transportation, housing, work, nutrition, environment, education, leisure: arts and entertainment (Holt-Lunstad, 2022).
Loneliness is also associated with social relationship expectations that are influenced by personal, social, cultural, and historical contexts and include the availability of social contacts (proximity), feeling cared for and relying on others (support), feeling close, understood, and listened to (intimacy), sharing interests and enjoyable experiences (fun), having opportunities to contribute meaningfully (generativity) and feeling valued and actively included (respect) (Akhter-Khan et al., 2022). A discrepancy between expected and actual social relationships will result in loneliness.
It is important to assess and understand individuals’ specific contexts, risks, expectations, and needs to tailor appropriate interventions to reduce social isolation or loneliness (Akhter-Khan et al., 2022; Eccles et al., 2021; Fakoya et al., 2020; Jopling, 2020; Lim et al., 2020; Mann et al., 2017; NASEM, 2020).
Interventions
Interventions to reduce social isolation and/or loneliness are more effective when targeted to the individual's specific experience and context (such as triggers, risk factors, and accessibility to resources) (Eccles et al., 2021; Fakoya et al., 2020; Prohaska et al., 2020; Veronese et al., 2021). Interventions aimed at reducing social isolation may have different components than those aimed at reducing loneliness (O'Rourke et al., 2018). The interventions can be delivered through various modes to bring about changes at different levels—individual, relationship, community, and societal levels (Holt-Lunstad, 2022; Lim et al., 2020; Mann et al., 2017; Ogrin et al., 2021; WHO, 2021). In addition, one component of an intervention may target multiple factors (O'Rourke et al., 2018). It is therefore challenging to categorize interventions by the risk factors they target following the socio-ecological framework or by their mechanisms. In order to have mutually exclusive categories and subcategories on the evidence map, we classified interventions as follows, based on who is providing the intervention and where the intervention is provided.
Self-delivery: These are self-guided interventions that focus on addressing personal characteristics (biological and sociodemographic factors, e.g., socio-economic status) that may trigger social isolation or loneliness, through strategies that change the attitudes, beliefs, and behaviors of individuals. The purpose of these interventions is to affect changes in an individual that would result in reductions in isolation and loneliness. They can be facilitated with training, guidance, or available resources from the healthcare professionals. Examples include self-guided social cognitive interventions like cognitive behavioral therapy, mindfulness, or reminiscence therapy.
Interpersonal delivery: These are interventions that focus on building close meaningful personal relationships with family and others in the community, for example, friends, colleagues, neighbors, volunteers. They can be delivered by healthcare or social care professionals, volunteers, or other people in the individual's social network. The purpose/aim of these interventions is to affect changes in an individual or a specific relationship or network of relationships that would result in reductions in isolation and loneliness. They are accomplished through mechanisms including changing cognition, social skills training and psychoeducation, healthcare support, and social support. Examples include cognitive behavioral therapy, family therapy, social prescribing or friendship enrichment program.
Community-based delivery: These interventions are delivered by healthcare or social care professionals, community workers/volunteers, or other people within the same community setting. They can be delivered through neighborhood organizations, community-based healthcare, and social services or facilities. They focus on addressing risk factors in social settings and increasing opportunities for social interactions with others such as connecting to community group activities or peer support groups; neighborhood approaches like networks, transportation, meals on wheels; intergenerational approaches. They may also provide a supportive environment or encourage participation by improving access to amenities within the community e.g., built environment, age-friendly communities, and volunteering. These interventions can affect changes in an individual, a specific relationship or network of relationships, or changes in the community that would result in reductions in isolation and loneliness.
Societal level delivery: Focus on policies and laws that address societal risk factors like discrimination and stigma, socio-economic inequality or may seek to change social norms that prevent social connection such as policies addressing housing, employment, transportation and the environment. These interventions affect change(s) in broader society, resulting in reductions in isolation and loneliness. Examples include public awareness campaigns, coalition and partnership initiatives, or family-friendly policies.
Multi-component/complex: These are combinations of multiple components within the interventions involving the same/different types of delivery modes in the same study, for example, reminiscence therapy and group activities.
Mechanisms
Different pathways or mechanisms related to contextual or risk factors, motives, expectations, and coping skills have been identified through which interventions may reduce social isolation or loneliness. The interventions may improve and maintain existing relationships or enable people to create new connections (Akhter-Khan et al., 2022; Jopling, 2020; Mann et al., 2017) by addressing contextual or risk factors (Akhter-Khan et al., 2022; Lim et al., 2020; Ogrin et al., 2021). Some interventions aim to change one's outlook or negative social cognition (Akhter-Khan et al., 2022; Jopling, 2020; Mann et al., 2017; Masi et al., 2011; Ogrin et al., 2021) while others provide support to enhance social interactions (Mann et al., 2017; Masi et al., 2011; Ogrin et al., 2021). Some interventions involve building skills, purposeful activity, or implementing a philosophy of care within a facility (Akhter-Khan et al., 2022). Some interventions are complex and may address social isolation or loneliness through multiple or poorly specified mechanisms (Akhter-Khan et al., 2022; Holt-Lunstad, 2018; Lim et al., 2020).
Process indicators and outcomes
The potential of interventions to reduce social isolation or loneliness have been assessed through their acceptability, adherence, and feasibility. These process indicators determine progress toward outcomes such as health and psychosocial outcomes (e.g., loneliness, social isolation, social connectedness), indicators of social connections (e.g., social support, social engagement, social cohesion), as well as cost and cost-effectiveness outcomes. See Glossary of terms (Supporting Information Appendix 1).
We used this conceptual framework to define and code the intervention and outcome categories and subcategories for the two-dimensional matrix in the evidence and gap map.
Dimensions
Types of study design
We included on-going (protocols, trial registrations) and completed systematic reviews and primary studies with any study design that has a control group: randomized controlled trials, non-randomized studies including control before-after, and statistical matching quasi-experimental studies.
The inclusion of systematic reviews was based on the population, intervention, comparison, outcome (PICO) framework and if they met at least four of the five criteria of a systematic review as defined by Moher et al. (2015). That is, they describe adequate search methods used to identify studies, eligibility criteria for selection of studies, methods of critical appraisal of included studies, sufficient details or characteristics of included studies, and synthesis or analysis of findings of the included studies.
Eligible quasi-experimental designs included quasi-randomized studies, regression discontinuity designs, natural experiments, non-equivalent comparison group designs and interrupted series designs with at least three data points before and after a discrete intervention (Waddington et al., 2014).
We excluded any study designs with no control group such as longitudinal cohort studies and cross-sectional studies, and those studies with interrupted time series designs with less than six data points.
We included mixed methods studies, but exclusive qualitative research was excluded.
We included studies irrespective of their publication status (e.g., protocols, working papers).
Types of intervention/problem
We included any intervention which aims to reduce social isolation and/or loneliness that is delivered in-person regardless of the intensity, duration, and frequency of administration. We excluded digital or technology-based interventions.
Included interventions may be one-on-one or group based and were categorized based on our conceptual framework as self-delivery, interpersonal delivery, community-based delivery, societal-level delivery as well as multi-component or complex interventions. See Table 1 for subcategories and examples.
Types of interventions.
Comparison interventions included no interventions, other interventions, or usual care.
If reviews included a subset of interventions that is not eligible, we only coded studies with the eligible interventions.
Types of population
We considered any age group, people with or at risk of social isolation or loneliness, or the general population, whether based on case finding or screening for vulnerability or not.
Age groups include: <10 years (children) 10–24 years (adolescents/youth) 25–44 years (young adults) 44–60 years (middle-aged) 60–75 years (youngest-old) 75–85 years (middle-old) >85 years (oldest-old)
Types of outcome measures
We considered the following types of outcomes: health and psychosocial outcomes, indicators of social connections, cost and cost-effectiveness outcomes, and process indicators (or implementation outcomes).
We considered adverse effects of interventions such as psychological distress, safety, and others as described by the studies. Different measuring tools have been used for loneliness, social isolation, and related outcomes. See Table 2 for outcome categories and measurements.
Outcome categories.
We did not use outcomes as eligibility criteria; however, eligible studies and reviews must have assessed interventions with a primary objective to reduce social isolation and/or loneliness, and could have reported outcomes other than social isolation and loneliness. Studies and reviews were not included if the primary aim of the interventions assessed was not to reduce social isolation and/or loneliness. Those that assessed the effects of interventions on social isolation and/or loneliness as a primary outcome or considered other indicators of social connections, such as social support, social engagement, social cohesion, and social capital were also included.
Studies and reviews assessing the effect of interventions on indicators of psychological wellbeing such as quality of life, anxiety or depression, with a focus on mental health rather than social isolation or loneliness were excluded.
Other eligibility criteria
Types of location/situation
We included all countries. We also classified the countries by the World Health Organization regions (African Region, Region of the Americas, South-East Asian Region, European Region, Eastern Mediterranean Region, Western Pacific Region) (WHO, 2019) and the World Bank classification by incomes: low income economies, lower-middle income economies, upper-middle income economies, and high income economies (World Bank, 2022).
We did not exclude primary studies and systematic reviews that do not report the countries.
Types of settings
We included all settings, for example, residential or personal home, nursing home or long-term care, assisted living facilities, orphanages, schools, workplaces, community centers, and medical facilities.
Search methods and sources
An Information Specialist (DS) designed the search strategy which was peer-reviewed through PRESS (Peer Review of Electronic Search Strategies) (McGowan et al., 2016). See Supporting Information Appendix 2 for the full search strategies. We searched the following databases from inception to February 17, 2022 with no date or language restrictions: Ovid MEDLINE, Embase, EBM Reviews—Cochrane Central Register of Controlled Trials, Global Index Medicus. We searched CINAHL via EBSCOhost, and the following databases as a combined search via EBSCO (Academic Search Complete, Global Health, and AgeLine, America: History & Life; American Antiquarian Society (AAS) Historical Periodicals Collection: Series 1; American Antiquarian Society (AAS) Historical Periodicals Collection: Series 2; American Antiquarian Society (AAS) Historical Periodicals Collection: Series 3; American Antiquarian Society (AAS) Historical Periodicals Collection: Series 4; American Antiquarian Society (AAS) Historical Periodicals Collection: Series 5; Art Full Text (H.W. Wilson); Art Index Retrospective (H.W. Wilson); Atla Religion Database with AtlaSerials;Bibliography of Indigenous Peoples in North America; Book Review Digest Retrospective: 1903-1982 (H.W. Wilson); Business Periodicals Index Retrospective: 1913-1982 (H.W. Wilson); Business Source Complete; Communication Source; Criminal Justice Abstracts; eBook Collection (EBSCOhost); EconLit; Education Source; Ergonomics Abstracts; Essay and General Literature Retrospective (H.W. Wilson); Film & Television Literature Index with Full Text; Financial Times; FSTA - Food Science and Technology Abstracts; GreenFILE; Historical Abstracts; Humanities & Social Sciences Index Retrospective: 1907-1984 (H.W. Wilson); Index to Legal Periodicals & Books Full Text (H.W. Wilson); Index to Legal Periodicals Retrospective: 1908-1981 (H.W. Wilson); Index to Printed Music; International Bibliography of Theatre & Dance with Full Text;International Political Science Abstracts; Library Literature & Information Science Full Text (H.W. Wilson); Library Literature & Information Science Retrospective: 1905-1983 (H.W. Wilson); Library, Information Science & Technology Abstracts; MLA Directory of Periodicals; MLA International Bibliography; New Testament Abstracts; Old Testament Abstracts; Philosopher's Index; Readers’ Guide Retrospective:: 1890-1982 (H.W. Wilson); Regional Business News; RILM Abstracts of Music Literature; Short Story Index Retrospective: 1915-1983 (H.W. Wilson);SPORTDiscus with Full Text).
We searched the ProQuest platform which includes 53 databases, the most directly relevant among them being: ASSIA, APA PsycArticles, PsycBooks, PsycInfo, Canadian Research Index, Eric, IBSS, Nursing and Allied Health, Publicly Available Content, Dissertations & Theses Global), the core collection of Web of Science including Conference Proceedings Citation Index, Korean Citation Index, Russian Science Citation Index, and SciELO Citation Index via Clarivate, and Elsevier Scopus.
In addition, we searched non-English databases including CNKI Chinese, ThaiJo (Thailand), CiNii-J-Stage (Japanese), CQVIP (China), Korean Social Science Data Center, MyCite (Malaysia). We translated terms for social isolation and loneliness and screened for relevant systematic reviews and controlled studies.
The reference lists of all included systematic reviews were not screened to identify additional studies due to lack of resources.
Analysis and presentation
Report structure
We followed the reporting structure of Campbell EGMs with the standard headings: abstract, plain language summary, background, methods, results, discussion, and conclusion.
This report includes the description of the study flow with included studies, excluded studies, and any studies awaiting assessment as well as the PRISMA study flow diagram. We also present the conceptual framework, tables, and figures summarizing the distribution of included primary studies and systematic reviews across all the coding categories. These categories include study designs, publication status, quality of systematic reviews, types of interventions, types of outcomes, population characteristics, settings, geographic distribution.
The evidence and gap map has interventions as the row dimension and outcomes as the column dimension. We use bubbles of different sizes to represent included primary studies and systematic reviews and different colors to distinguish primary studies and methodological quality of systematic reviews. The filters used in the map are based on the number of included studies and coded information. See a sample of the map in Figure 2.
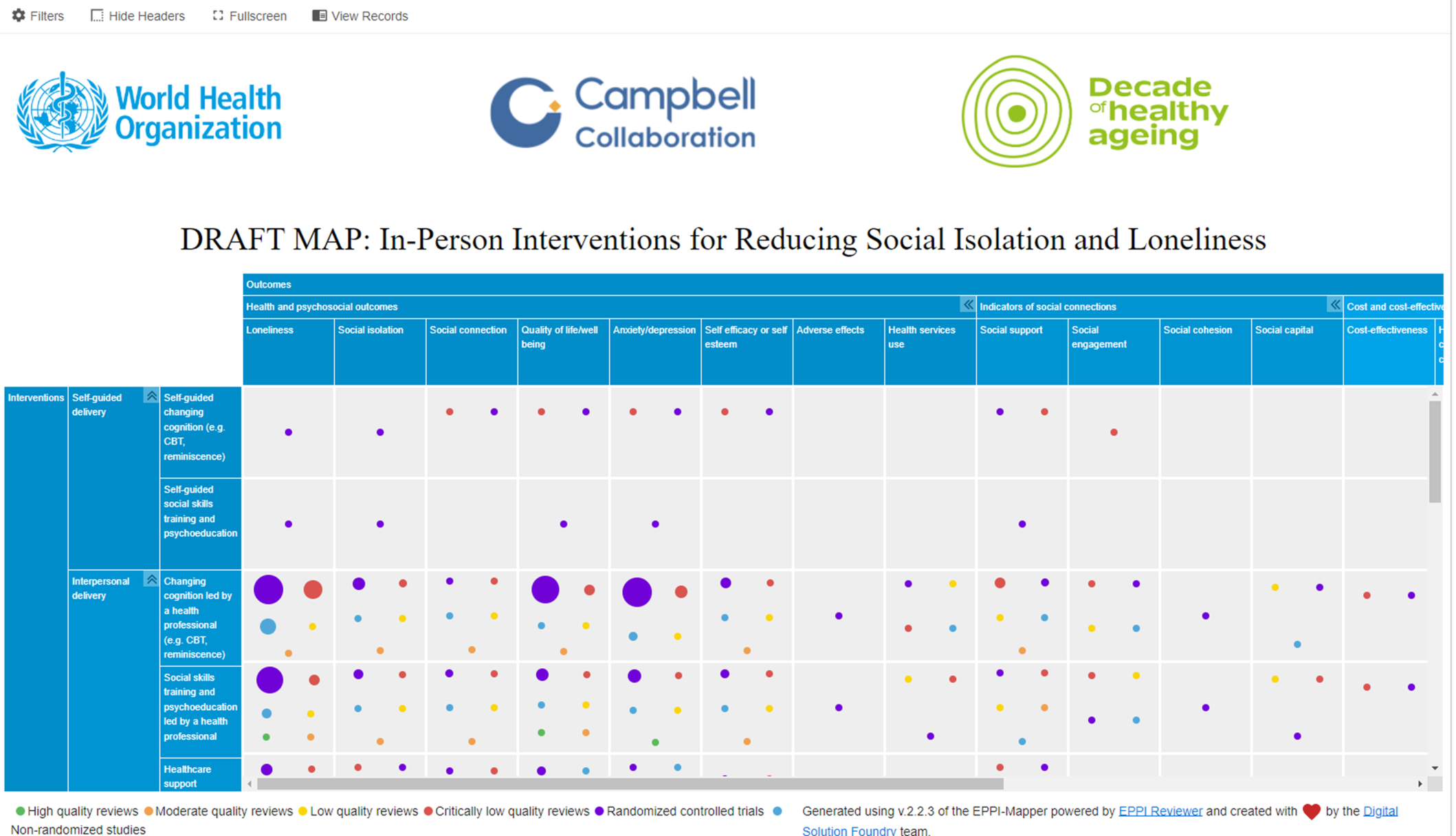
Sample map.
Filters for presentation
Additional dimensions of interest used as filters include: Study characteristics: the publication status of included studies, study design, countries where studies were conducted, World Bank classification by income (low income economies, lower-middle income economies, upper-middle income economies, high income economies), and WHO regions (African Region, Region of the Americas, South-East Asian Region, European Region, Eastern Mediterranean Region, Western Pacific Region), and setting (personal home, independent living/residential home, assisted living, long-term care/nursing home, orphanages, schools, workplaces, community centers, art gallery or museums, medical facilities, prisons), equity focus (study aimed at/focused on disadvantaged across any PROGRESS-Plus factors) and equity analysis (assessing any differences in effects (benefit or harm) across any PROGRESS-Plus factors). Intervention characteristics: focus (loneliness, social isolation, or both); format (group-based or one-on-one), sectors (clinical and population health, transport, housing, work, nutrition, environment, education, leisure: arts and entertainment, and spiritual care). Population characteristics: age groups, and other sociodemographic factors as well as needs.
Equity analysis
We assessed equity following the same methods used in the evidence and gap map on digital interventions to reduce social isolation and loneliness in older adults (Welch et al., 2022). We used the PROGRESS-Plus acronym to describe sociodemographic inclusion factors associated with health inequities (O'Neill et al., 2014). PROGRESS-Plus stands for Place of residence (urban/rural), Race/ethnicity/culture and language, Occupation, Gender or sex, Religion, Education, Socioeconomic status, Social capital, Plus: personal characteristics (e.g., age, disabilities), relationship features (e.g., exclusion from school, parent drug use), and time-dependent relationships (e.g., leaving the hospital, released from prison or other times when an individual might be temporarily disadvantaged).
We documented whether studies focused on populations who are at risk or experiencing barriers to health and social care or health inequities across any PROGRESS-Plus factors. For these studies, since interventions target different populations, we documented how potentially vulnerable populations, older people for instance, are defined and identified (e.g., using case finding, outreach, community-based programs, screening in primary care, through formal service network or agencies).
In addition, for each study, we assessed whether studies analyzed differential effects across PROGRESS factors for populations experiencing inequities. We also assessed subgroup analysis across additional (“Plus”) factors known to be important for special populations, including age, disability, social frailty, literacy, living status, and health status.
Dependency
We treated multiple reports of the same study as one study. A study with multiple outcomes and interventions was shown multiple times on the map (once for each outcome or intervention identified). Primary studies were mapped regardless of whether they are included in multiple systematic reviews. Systematic reviews were mapped to interventions and outcomes based on their PICO question.
Data collection and analysis
Screening and study selection
Pairs of reviewers used Machine learning text mining in Eppi-Reviewer web-based software program (Thomas et al., 2020) to screen titles and abstracts independently (EG, SD, EB, VB, TH, AW, AA, PD, JH, RD, SA, RI, LM, AAA, AJ, and FJ). We initially screened 10% of the titles and abstracts. The priority screening function developed a classifier based on the probability of inclusion determined from the preliminary screening results and presented the most likely studies to be included first. We manually screened all the articles to ensure all potentially eligible studies were captured for the full text screening stage which was also conducted by two reviewers independently.
We did not screen the reference lists of included systematic reviews as planned to identify additional studies that may have been missed in the database searches.
All screening was done following the eligibility criteria (see Appendix 3).
Data extraction and management
We developed and pilot tested a data extraction code set in Eppi-Reviewer for data collection (see Supporting Information Appendix 4). We used a set of included studies for testing. The same studies were coded by all the reviewers and the coding was assessed for agreement. Any discrepancies were discussed, and description of the coding criteria was modified for clarity as necessary. After the pilot test, members of the team (EG, SD, EB, VB, TH, AW, AA, PD, JH, RD, SA, RI, LM, AAA, AJ, and FJ) individually extracted and coded data. Some non-English papers (including Chinese, Mandarin, Korean papers) were coded by CWY, RY, and TAMTM. Automation and text mining was not used for coding.
We coded the study characteristics (study design, publication status, methodological quality assessment of systematic reviews), categories and subcategories of interventions and other intervention characteristics (focus, sectors, goals, and risk factors targeted), outcome domains and subdomains, population characteristics (using PROGRESS-Plus acronym), settings, locations (by country, WHO region, and World Bank income classification).
We coded how populations were recruited and whether they were selected based on disadvantages across any PROGRESS-Plus factors.
We also coded whether differential analysis across any PROGRESS-Plus factors was conducted in the studies and systematic reviews to understand any equity issues.
We did not contact authors of studies or systematic reviews for any missing information given the expected size of the map (over 300 studies).
Tools for assessing risk of bias/study quality of included reviews
Pairs of reviewers used the AMSTAR 2 tool (Shea et al., 2017) to assess the quality of systematic reviews independently. Any disagreements were resolved by discussion. Primary studies were not assessed for risk of bias or methodological quality following guidance for evidence maps (Snilstveit 2016; White et al., 2020).
Methods for mapping
We used the EPPI-Mapping tool (Digital Solution Foundry and EPPI_Centre, 2020) to develop the evidence and gap map. It is a tool to generate and visualize maps as an interactive HTML file on a web browser. The map is generated using exported data from EPPI-Reviewer, the software for managing and coding data.
RESULTS
Description of studies
Results of the search
Our search retrieved 15,698 records from databases and 100 from other sources. We screened 9704 titles and abstracts after duplicates and other ineligible studies were removed by automation tools. We identified 1244 potentially eligible articles and retrieved full texts of 1183 records that were assessed and 513 were included. See Figure 3 for the PRISMA flow diagram.
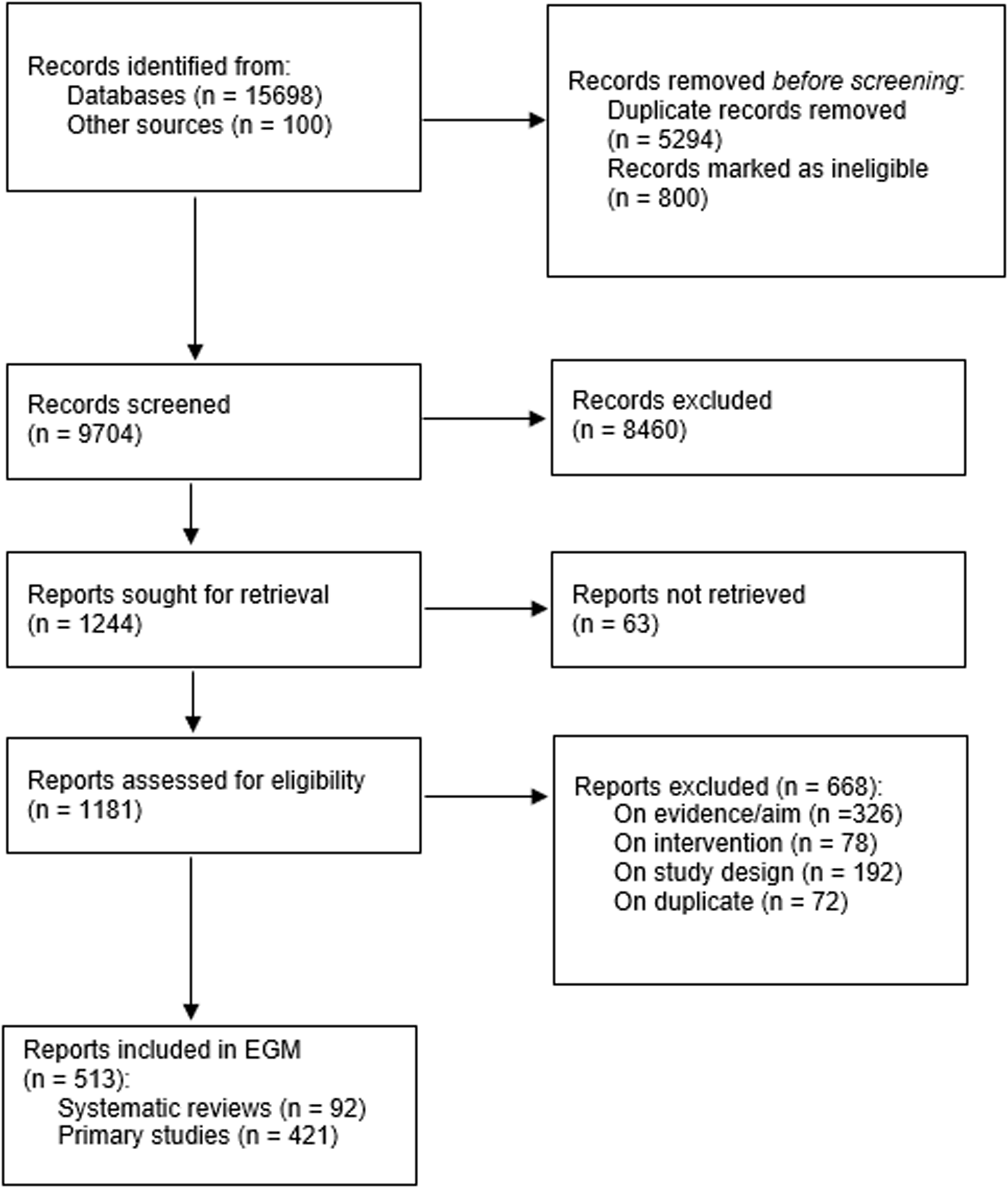
PRISMA flow diagram.
Excluded studies
A total of 670 studies were excluded during the full-text review phase due to an inappropriate aim (n = 327), intervention (n = 78), or study design (n = 192), and some as duplicates (n = 73) (Figure 3).
A list of key excluded studies can be found in the table for “Characteristics of excluded studies.” Three studies (Lee, 2014; Roessler, 2012; Scazufca, 2022) were excluded as the aim was not to reduce either social isolation or loneliness. Lee (2014) assessed the effects of a recall program on depression and self-esteem. Roessler et al. (2012) examined the effects of a physical activity and group counseling intervention on the quality of life in woman with polycystic ovary syndrome. Scazufca et al. (2022) assessed the effects of a psychosocial collaborative care intervention on depression in older adults who were disadvantaged socioeconomically.
One study (Lin et al., 2020) was excluded as the intervention group received horticultural therapy through 3D virtual reality.
Four studies were excluded for an incorrect study design (Fokkema & van Tilburg, 2007; Low et al., 2015; Mächler et al., 2022; Purewal et al., 2017). Fokkema and van Tilburg (2007) was a literature review of intervention to reduce loneliness that did not report using a systematic search. Low et al. (2015) was a primary study with no control group that assessed the effect of the Lifestyle Engagement Activity Program (LEAP) in older adults in aged care. Purewal et al. (2017) was a systematic review of companion animal studies that looked at association as opposed to effectiveness. Mächler et al. (2022) was a primary study that investigated the views of patients following participation in a holistic care program which aims to increase social activity instead of measuring effectiveness.
Studies awaiting classification (if applicable)
We were unable to find the full texts of 63 articles that were potentially eligible. See references of Studies awaiting classification.
Synthesis of included studies
We included 513 articles that utilized in-person interventions aimed at reducing loneliness and/or social isolation. Of these articles, 421 were primary studies and 92 were reviews presented in the evidence and gap map. The primary studies included both randomized controlled trials (n = 310, 74%) and non-randomized studies (n = 111, 26%).
Most of the publications for both the reviews and primary studies were completed (reviews: n = 86, 93%; primary studies: n = 350, 83%). Ongoing registered trials or protocols (reviews: n = 6, 7%; primary studies: n = 68, 16%) and conference abstracts (reviews: n = 0, 0%; primary studies: n = 3, 1%) were less common (Table 3).
Characteristics of included studies.
Of the included publications, around half were published in the past 5 years (reviews: n = 58, 63%; primary studies: n = 216, 51%). More specifically, the highest number of reviews and primary studies were published in 2021 (reviews: n = 26, 28%; primary studies: n = 73, 17%) and 2020 (reviews: n = 14, 15%; primary studies: n = 51, 12%) (Figure 4).
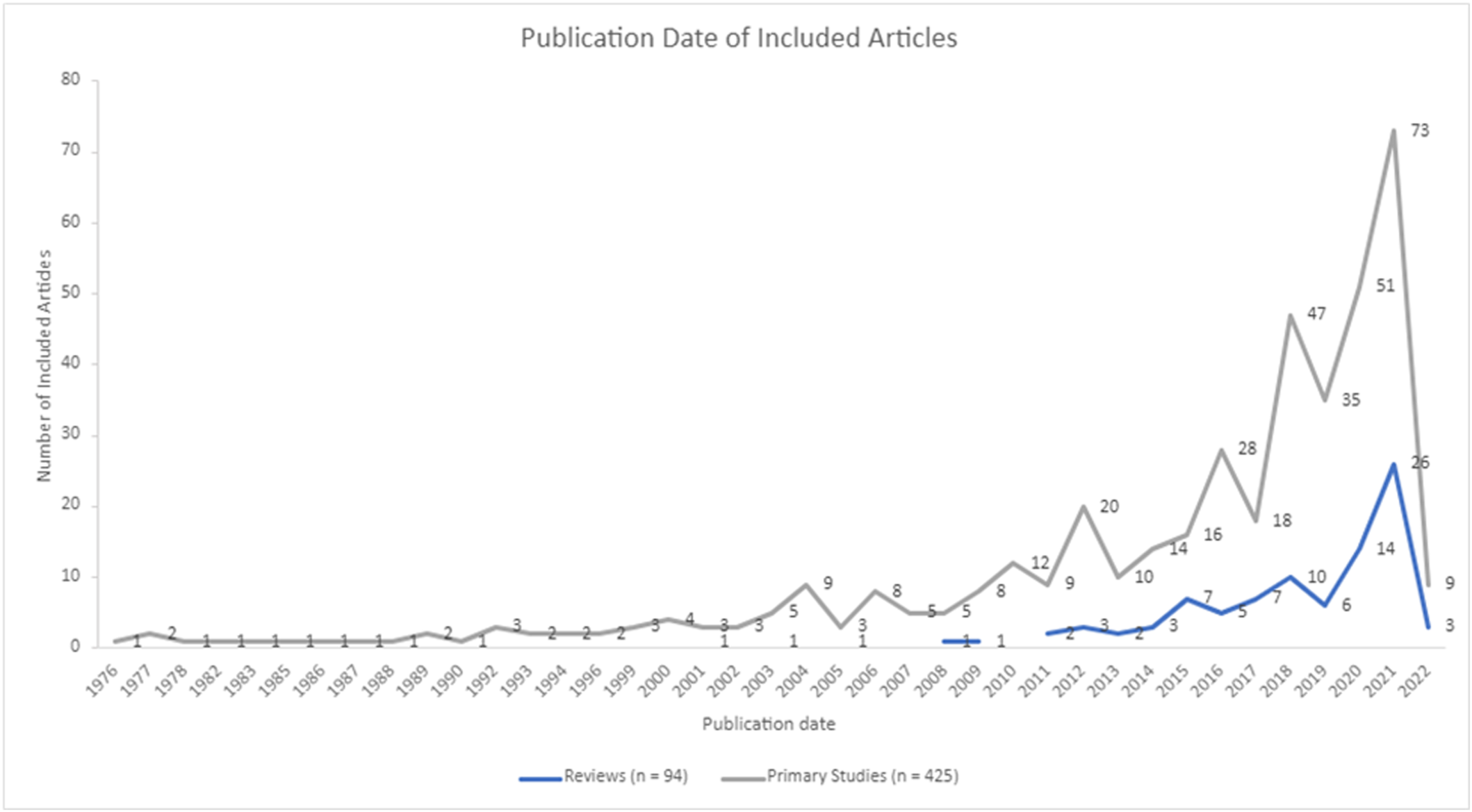
Publication year of included studies.
Interventions
To be included in this EGM, interventions had to be focused on addressing either loneliness (reviews: n = 33, 36%; primary studies: n = 272, 65%), social isolation (reviews n = 28, 30%; primary studies: n = 82, 19%) or both (review: n = 31, 34%; primary studies: n = 67, 16%).
The included interventions were delivered using a group format (reviews: n = 74, 80%; primary studies: n = 335, 80%) or one-on-one (reviews: n = 51, 55%; primary studies: n = 103, 24%). For articles that included both group and one-on-one formats (reviews: n = 43, 47%; primary studies: n = 23, 5%), both options were coded. Few articles did not specify the format (reviews: n = 10, 11%; primary studies: n = 6, 1%).
The included articles involved interventions delivered across various sectors including clinical and population health, transport, housing, work, nutrition, environment, education, leisure: arts and entertainment, and spiritual care. Clinical and population health was the most reported sector (reviews: n = 74, 80%; primary studies: n = 295, 70%), followed by leisure (reviews: n = 40, 43%; primary studies: n = 112, 27%) and education (reviews: n = 22, 24%; primary studies: n = 52, 12%). Environment (reviews: n = 1, 1%; primary studies: n = 6, 1%), housing (reviews: n = 2, 2%; primary studies: n = 5, 1%) and transport (reviews: n = 2, 2%; primary studies: n = 0, 0%) were the least reported sectors. For interventions delivered across multiple sectors, all relevant sectors were coded (Figure 5).
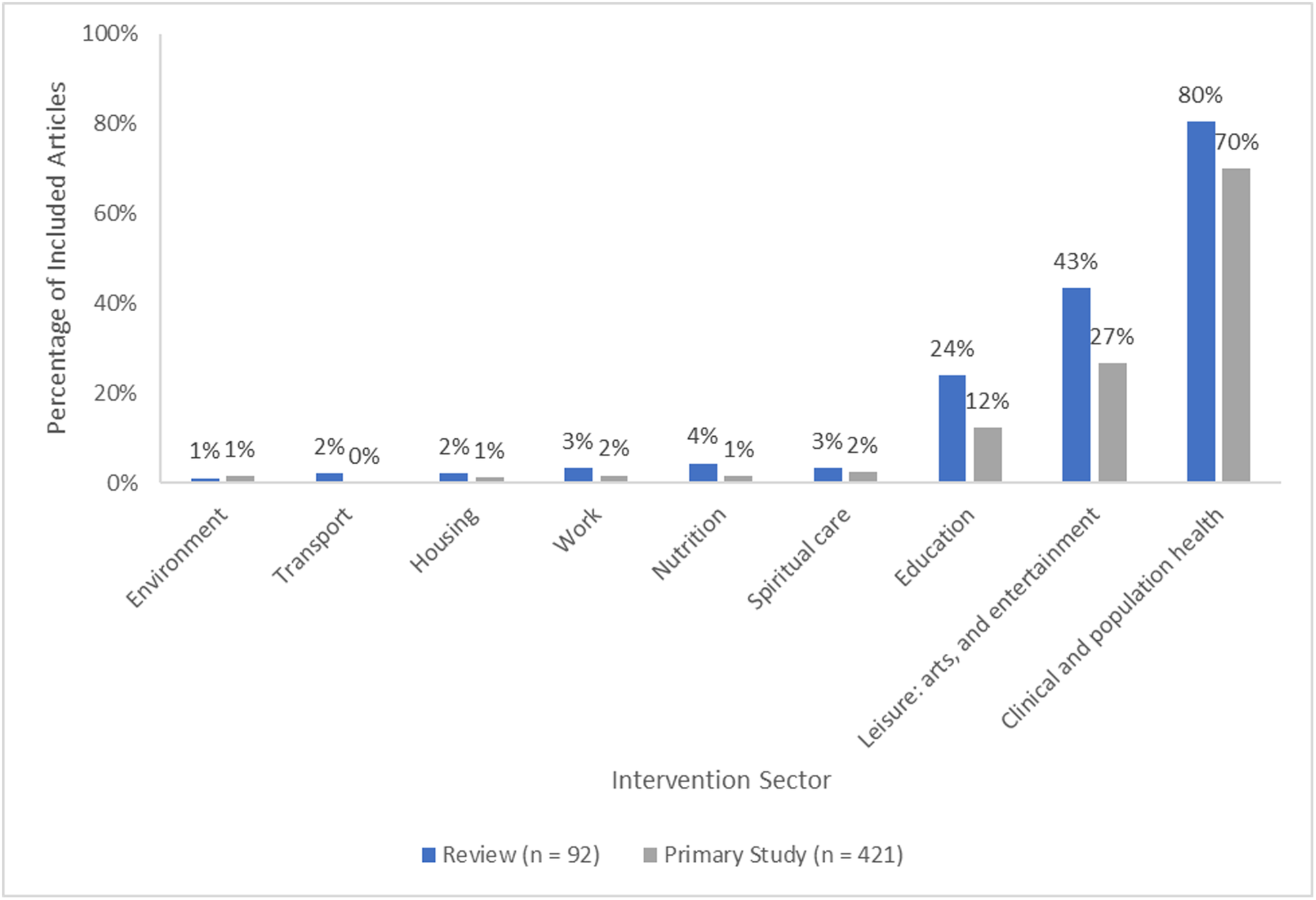
Intervention sector reported in included articles.
The interventions were organized using the following categories according to who was administering the intervention: self-delivery interventions (reviews: n = 3, 3%; primary studies: n = 11, 3%), interpersonal delivery interventions (reviews: n = 72, 78%; primary studies: n = 284, 67%), community-based delivery interventions (reviews: n = 61, 66%; primary studies: n = 176, 42%), and societal level delivery interventions (reviews: n = 1, 1%; primary studies: n = 2, 0.48%). Some interventions involved multiple delivery strategies and were coded as complex (reviews: n = 5, 5%; primary studies: n = 47, 11%) in addition to all relevant delivery strategies. For example, an intervention that combined cognitive behavioral therapy and social support group was coded as both an interpersonal delivery and a community-based delivery intervention, as well as a multi-component/complex intervention (Figure 6).
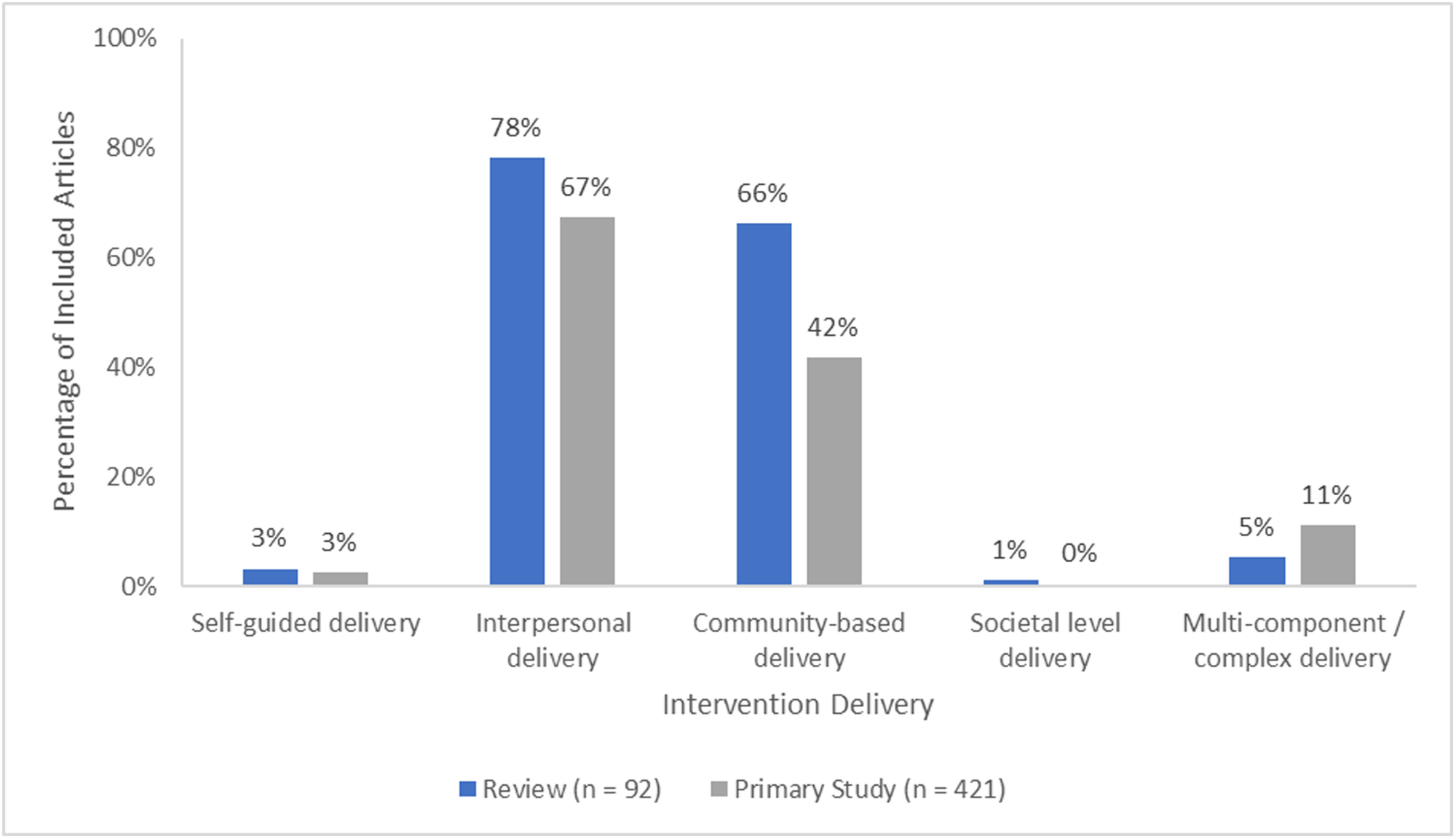
Intervention delivery method reported in included articles.
Each intervention category included multiple subcategories. The few interventions that used a self-delivery mode were further categorized into two subcategories: self-guided interventions for changing maladaptive cognition (reviews: n = 3, 3%; primary studies: n = 6, 1%) and self-guided social skills training and psychoeducation (reviews: n = 0, 0%; primary studies: n = 5, 1%) (Figure 7).
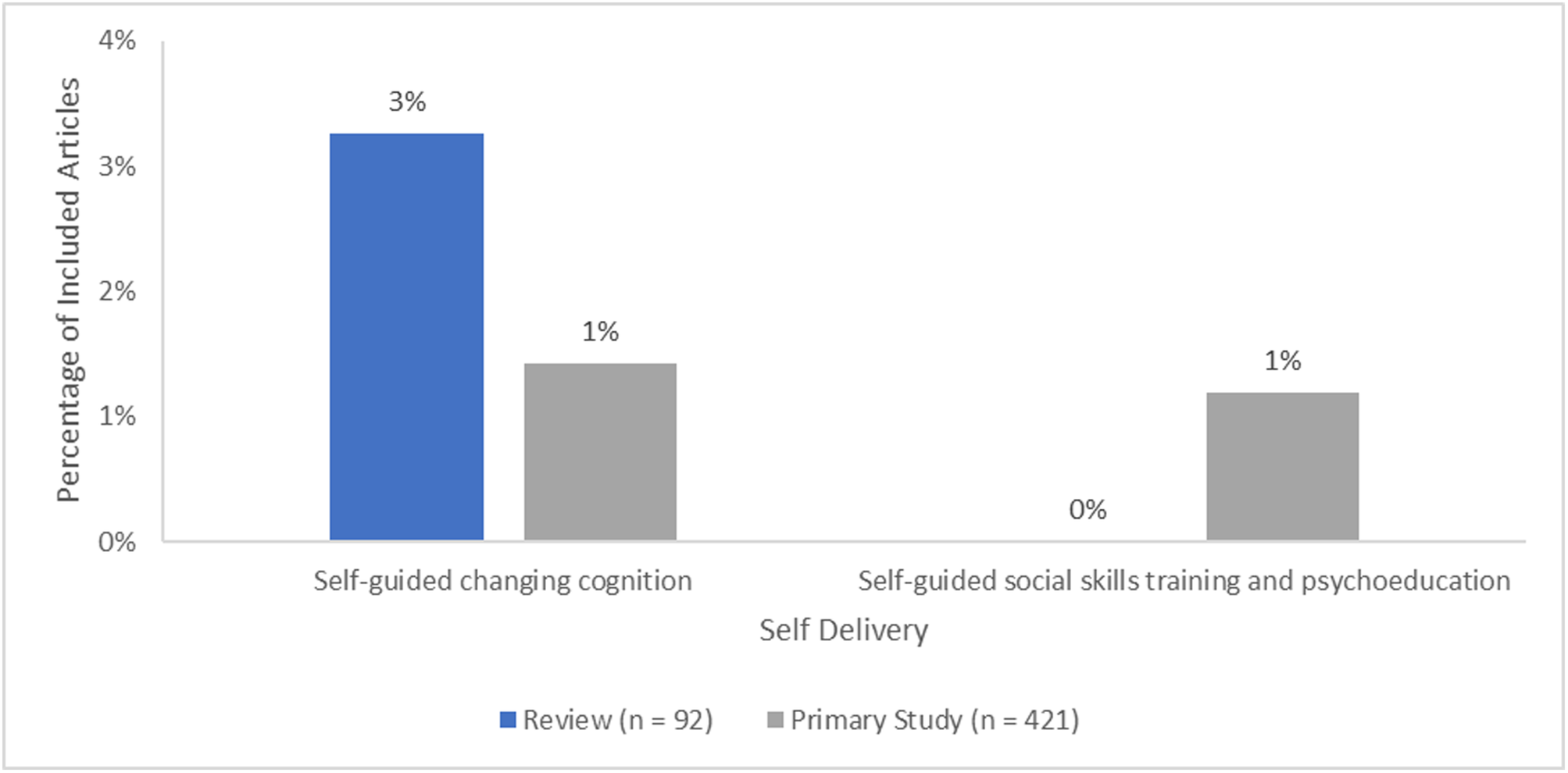
Self delivery interventions reported in included articles.
Interpersonal delivery interventions had four subcategories: changing cognition, social skills training and psychoeducation, healthcare support, and social support. For both reviews and primary studies, changing cognition (e.g., cognitive behavioral therapy, psychotherapy) was the most reported (reviews: n = 52, 57%; primary studies: n = 151, 36%), while healthcare support was the least reported (reviews: n = 10, 11%; primary studies: n = 30, 7%). Some studies used multi-component interventions that involved multiple interpersonal delivery interventions (reviews: n = 40, 43%; primary studies: n = 32, 8%) so all relevant categories were coded (Figure 8).
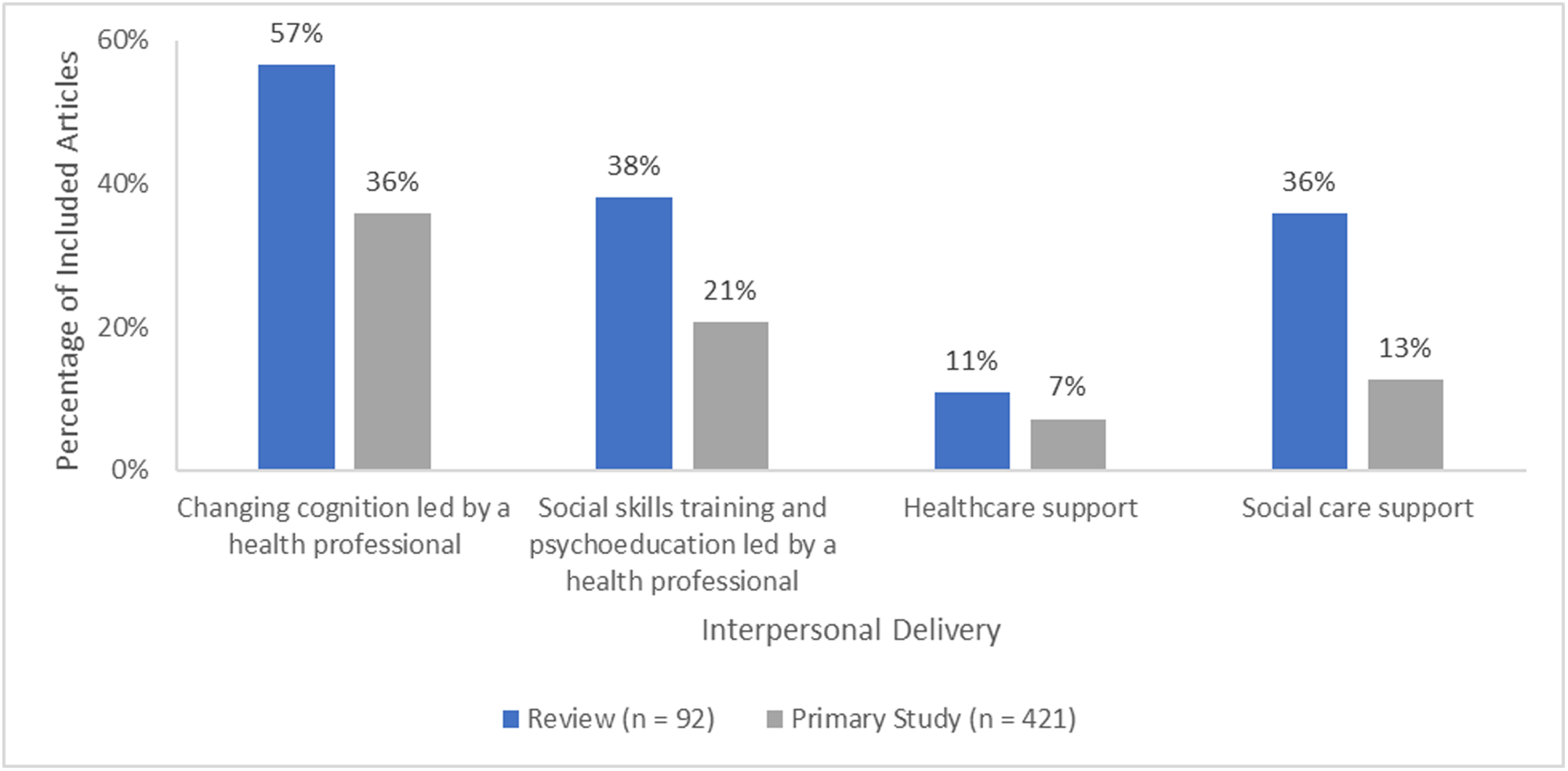
Interpersonal delivery interventions reported in included articles.
Interventions with a community-based delivery mode were organized into five subcategories: group activities, support groups, neighborhood approaches, age-friendly communities, and volunteering. Group activities were most common for both reviews and primary studies (reviews: n = 40, 43%, primary studies: n = 106, 25%). Interventions to promote age-friendly communities (reviews: n = 1, 1%, primary studies: n = 0, 0%) and volunteering interventions (reviews: n = 8, 9%, primary studies: n = 2, 0.48%) were the least common. Some studies used multi-component interventions that involved multiple community-based delivery interventions (reviews: n = 22, 25%; primary studies: n = 9, 2%) so all relevant categories were coded (Figure 9).
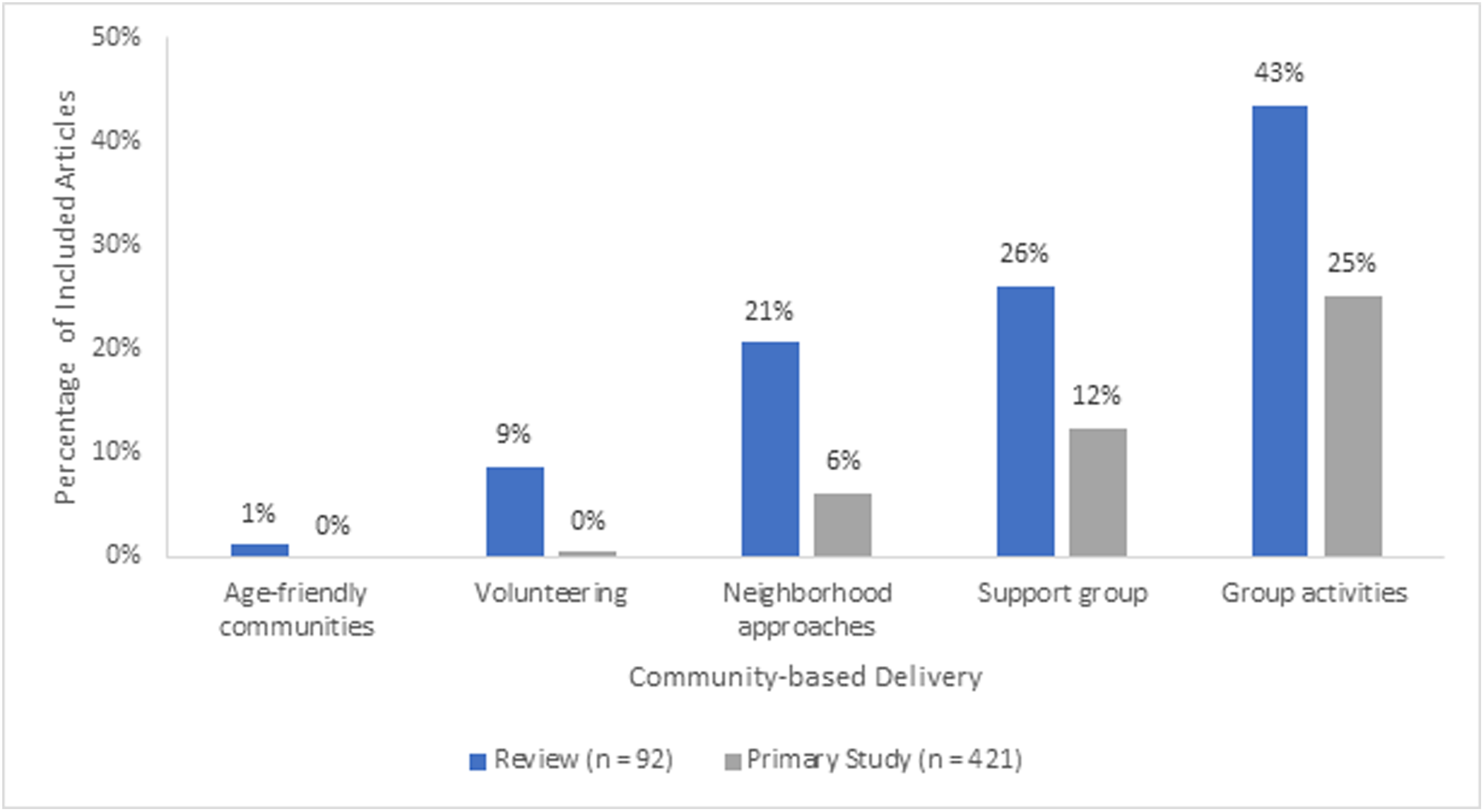
Community-based delivery interventions reported in included articles.
Societal-level delivery interventions focusing on policies and norms encompassed four subcategories: public health policy that promotes social cohesion and inclusion, public education and awareness of social relationships, policies on the design of neighborhoods, and funding relevant research. Evidence across all four subcategories was very sparse with no reviews or studies reporting on public education and awareness of social relationships or funding relevant research. Only one primary study reported on public health policy that promotes social cohesion and inclusion (n = 1, 0.24%) and one on policies on the design of neighborhoods as an intervention (n = 1, 0.24%). Only one review reported about policies on the design of neighborhoods (n = 1, 1%).
Outcomes
The outcome framework consisted of four categories, each with a differing number of subcategories. These categories included: health and psychosocial outcomes, indicators of social connections, cost and cost-effectiveness outcomes, and process indicators or implementation outcomes. For studies that looked at more than one outcome, all relevant outcomes were coded. Most reviews and primary studies reported at least one health and psychosocial outcome (reviews: n = 91, 99%; primary studies: n = 417, 99%). Few reviews and primary studies reported cost and cost-effectiveness outcomes (reviews: n = 3, 3%; primary studies: n = 6, 1%) or process indicators or implementation outcomes (reviews: n = 3, 3%; primary studies: n = 34, 8%) (Figure 10).
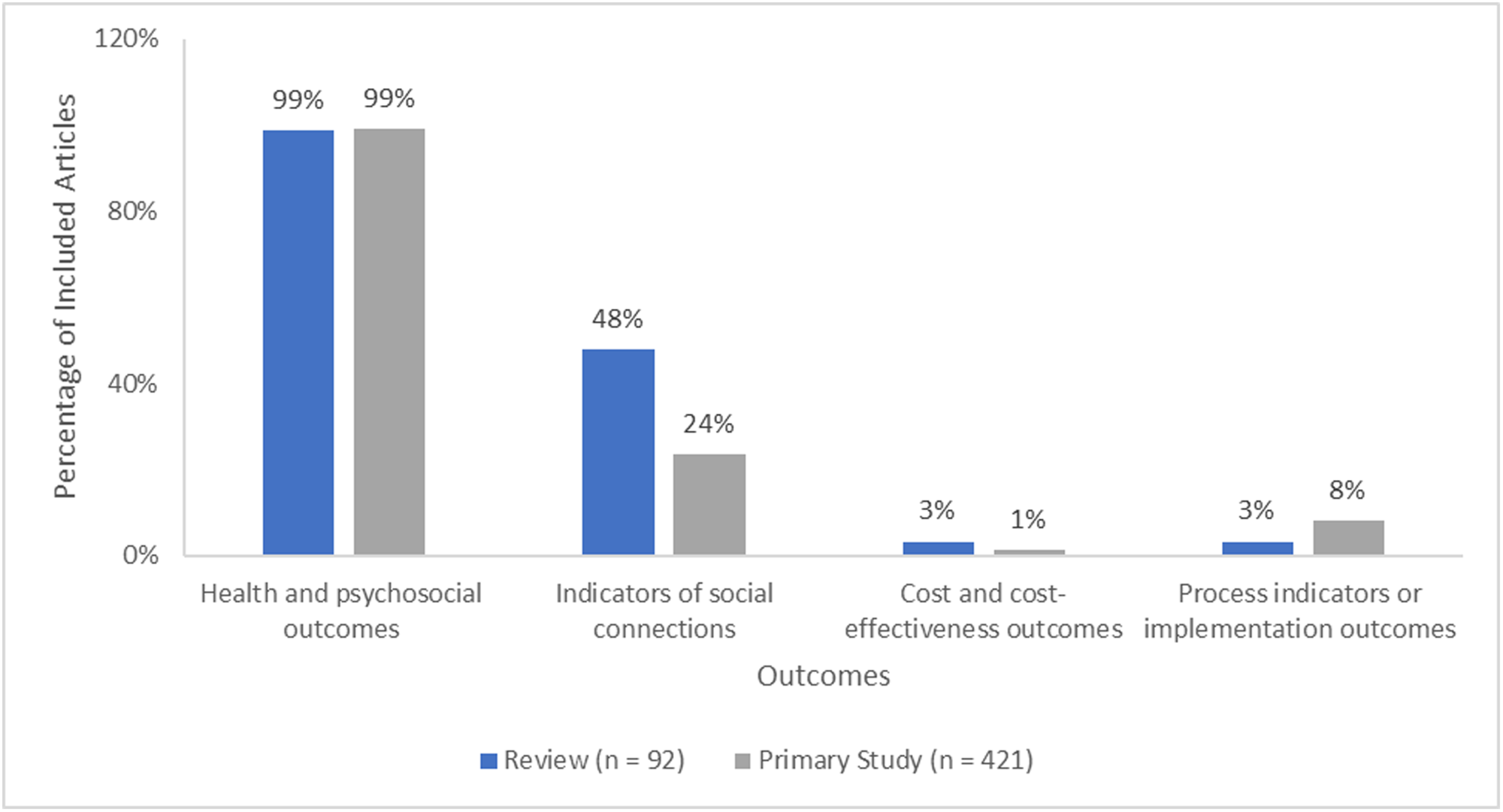
Outcomes reported in included articles.
Health and psychosocial outcomes consisted of eight subcategories: loneliness, social isolation, social connectedness, quality of life/well-being, anxiety/depression, self-esteem or self-efficacy, adverse effects, and health services use. Loneliness was the health and psychosocial outcome reported most often (reviews: n = 67, 73%; primary studies: n = 325, 77%), followed by anxiety/depression (reviews: n = 48, 52%; primary studies: n = 181, 43%), and quality of life/well-being (reviews: n = 42, 46%; primary studies: n = 179, 43%). Adverse effects (reviews: n = 2, 2%; primary studies: n = 7, 2%) and health services use (reviews: n = 4, 4%; primary studies: n = 16, 4%) were the least reported health and psychosocial outcomes (Figure 11).
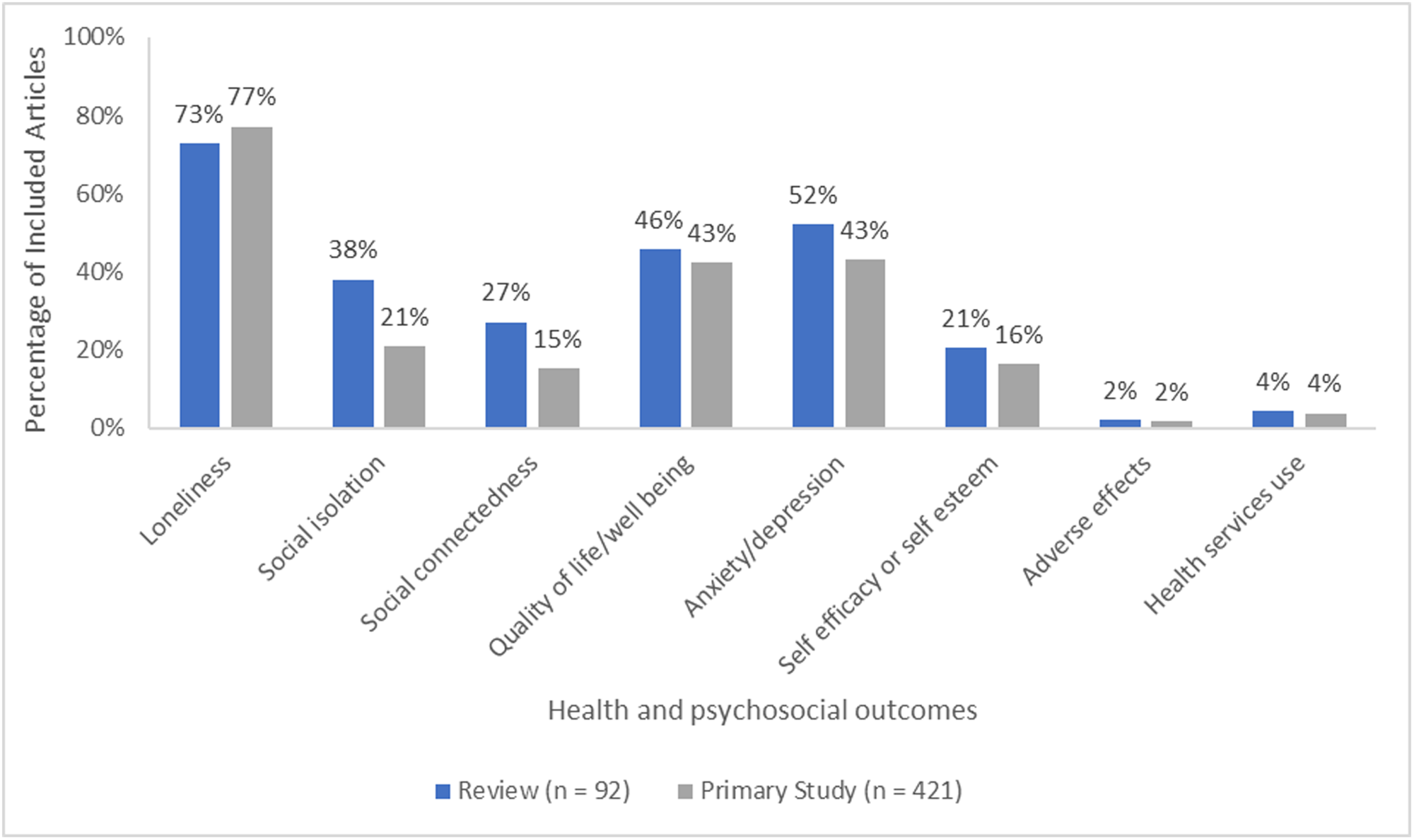
Health and psychosocial outcomes reported in included articles.
Indicators of social connections consisted of the following subcategories: social support, social engagement, social cohesion, and social capital. Social support (reviews: n = 36, 39%; primary studies: n = 82, 19%) and social engagement (reviews: n = 14, 15%; primary studies: n = 20, 5%) were the most reported indicators of social connections. Social cohesion (reviews: n = 0, 0%; primary studies: n = 2, 0.48%) and social capital (reviews: n = 2, 2%; primary studies: n = 6, 1%) were reported in few articles (Figure 12).
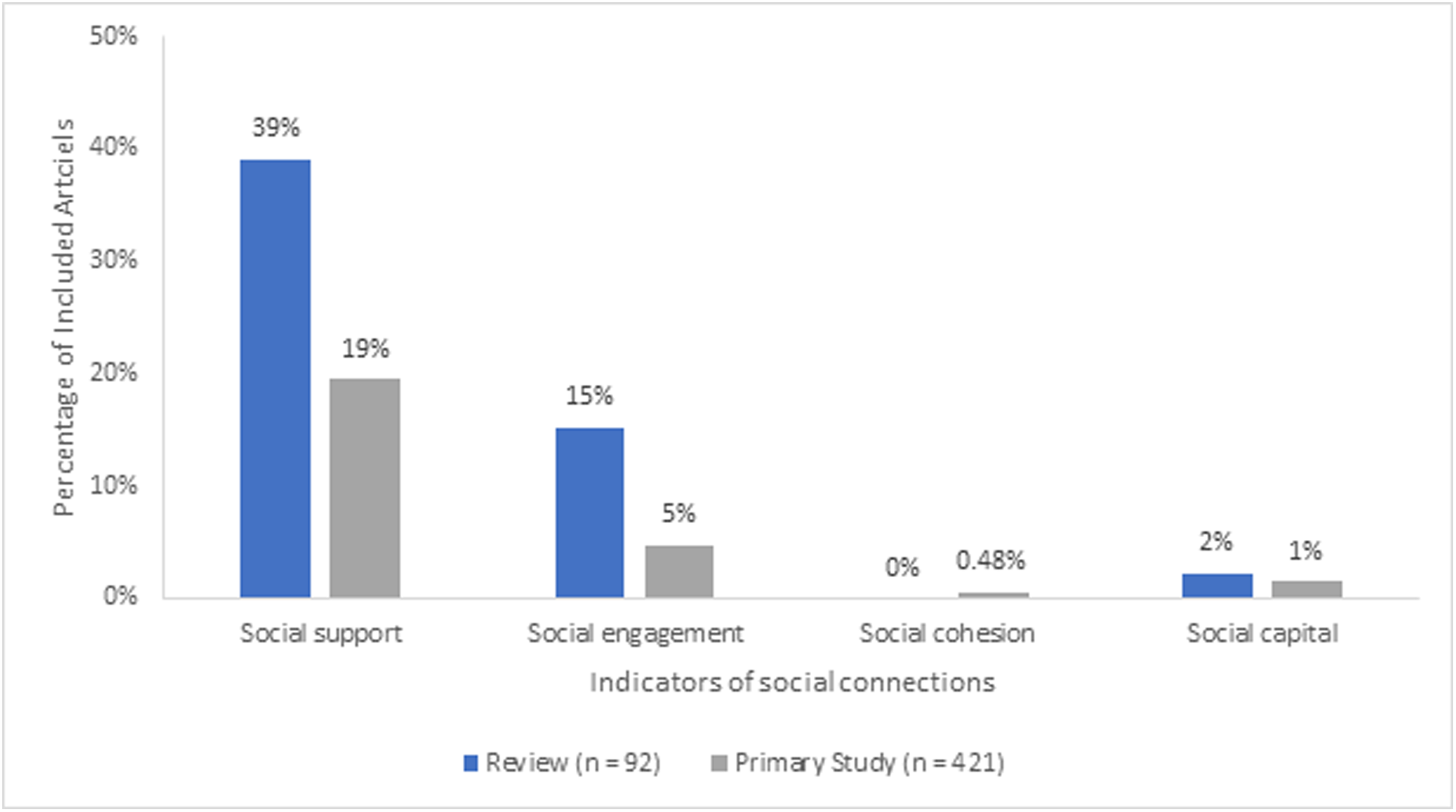
Indicators of social connections reported in included articles.
Cost and cost-effectiveness outcomes category had three subcategories: cost-effectiveness, cost per participant, and healthcare or social care utilization costs. Cost effectiveness (reviews: n = 3, 3%; primary studies: n = 5, 1%) was the most assessed, while healthcare or social care utilization costs (reviews: n = 1, 1%; primary studies: n = 2, 0.48%) and cost per participant (reviews: n = 1, 1%; primary studies: n = 2, 0.48%) were assessed in very few articles (Figure 13).
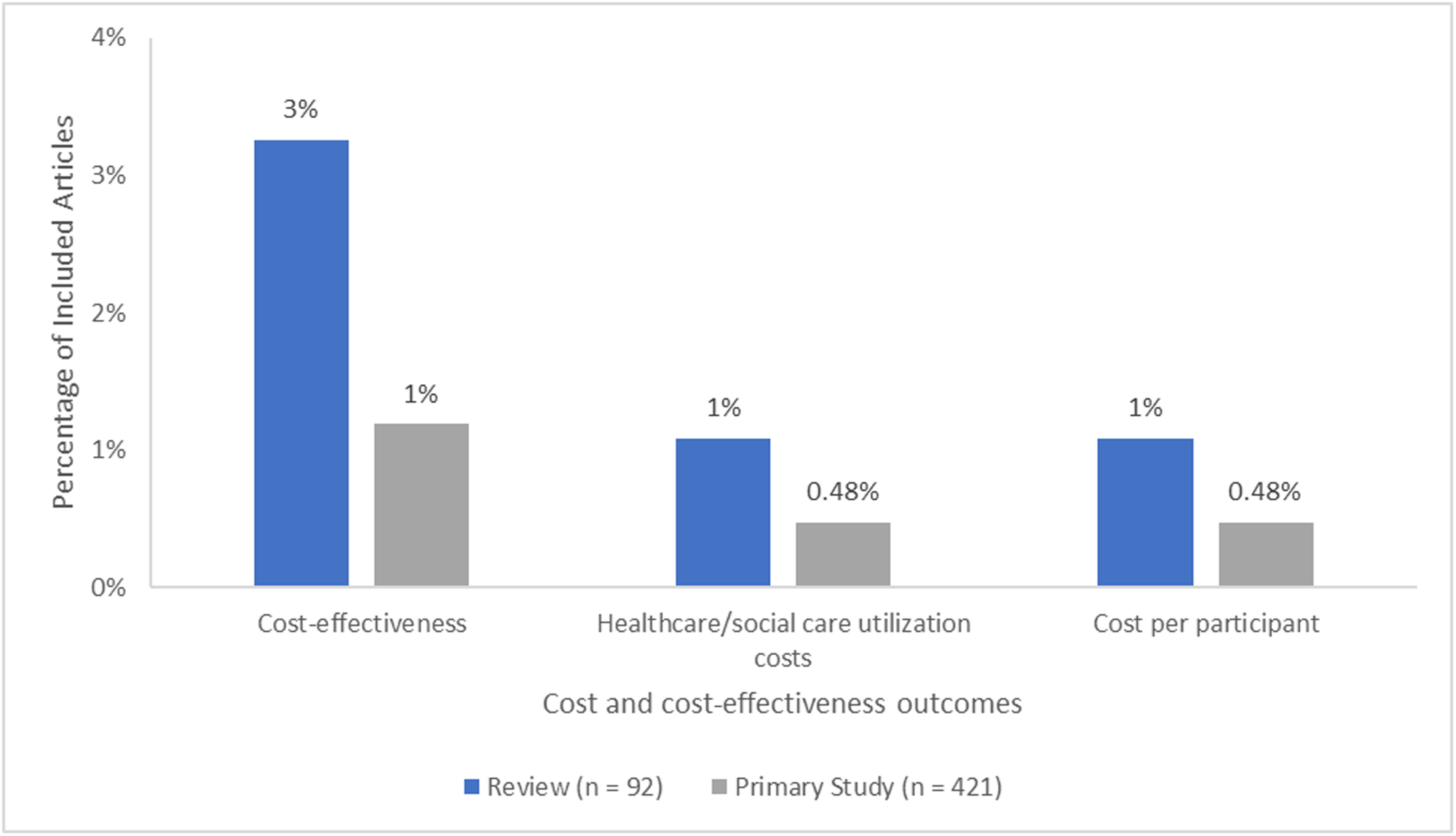
Cost and cost-effectiveness outcomes reported in included articles.
Process indicators or implementation outcomes consisted of the following subcategories: acceptance, adherence, and feasibility. More primary studies than reviews looked at these process indicators, with only one review reported to have looked at adherence, feasibility, and increased awareness of community services (n = 1, 1%). Acceptance (n = 21, 5%), feasibility (n = 15, 4%), and adherence (n = 14, 3%) were most common among the primary studies (Figure 14).
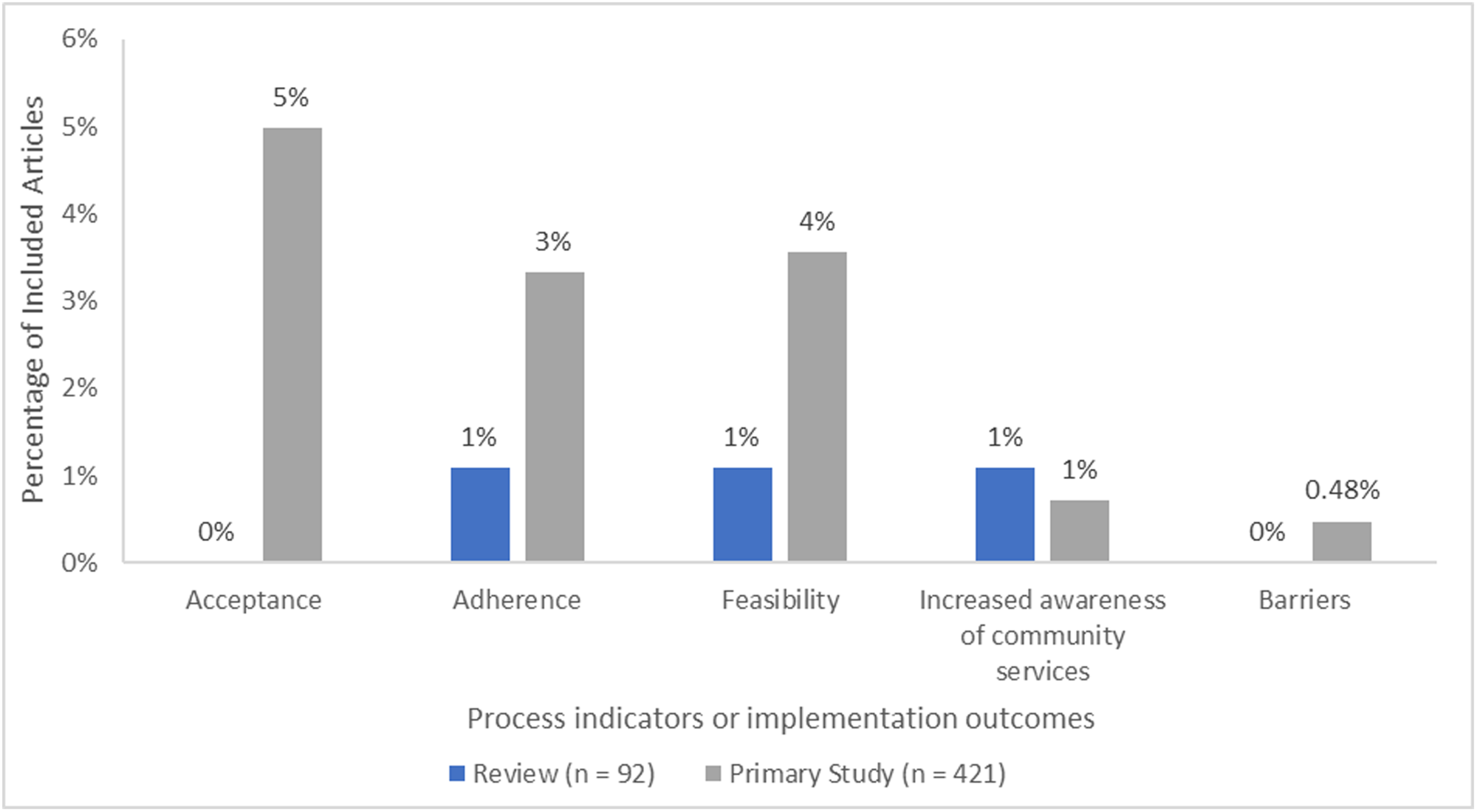
Process indicators or implementation outcomes reported in included articles.
Risk of bias in included reviews
Review quality was assessed using the AMSTAR2 Quality Assessment tool. Most reviews were classified as either low (n = 19, 21%) or critically low (n = 63, 68%). High (n = 1, 1%) (Reichow et al., 2012) and moderate (n = 3, 3%) (Bee et al., 2014; Jarvis et al., 2020; Moore et al., 2018) quality reviews were uncommon. Review protocols (n = 6, 6%) were not assessed (Figure 15).
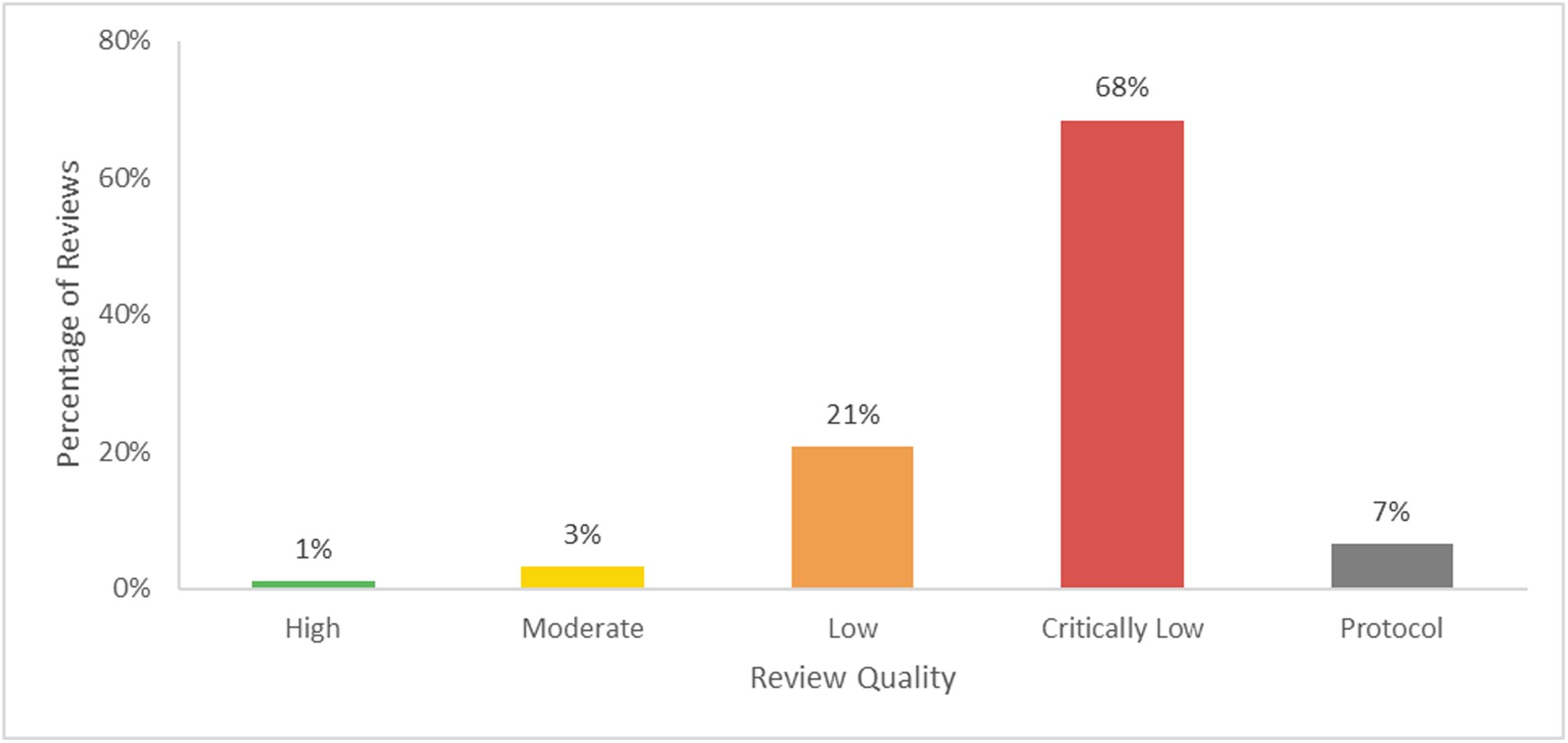
Quality assessment of included reviews (n = 92).
The critical domains that were most poorly met were domain 2 (not explicitly reporting that review methods were established before the conduct of the review in 64%) and domain 7 (not providing a list of excluded studies and their justification of exclusion in 83%).
Additional dimensions
Region
This EGM identified publications from 50 different countries across the globe. For the primary studies, the countries where the interventions were conducted were coded. For reviews, the countries specified for their included studies were coded. It should be noted that if a review included multiple studies conducted in the same country, that country was only coded once. If one primary study was included in multiple reviews the country was coded for each review.
The most common countries were the USA (reviews: n = 46, 50%; primary studies: n = 113, 27%), the UK (reviews: n = 32, 35%; primary studies: n = 35, 8%), China (reviews: n = 14, 15%; primary studies: n = 44, 10%), and Australia (reviews: n = 15, 16%; primary studies: n = 31, 7%) (Figure 16).
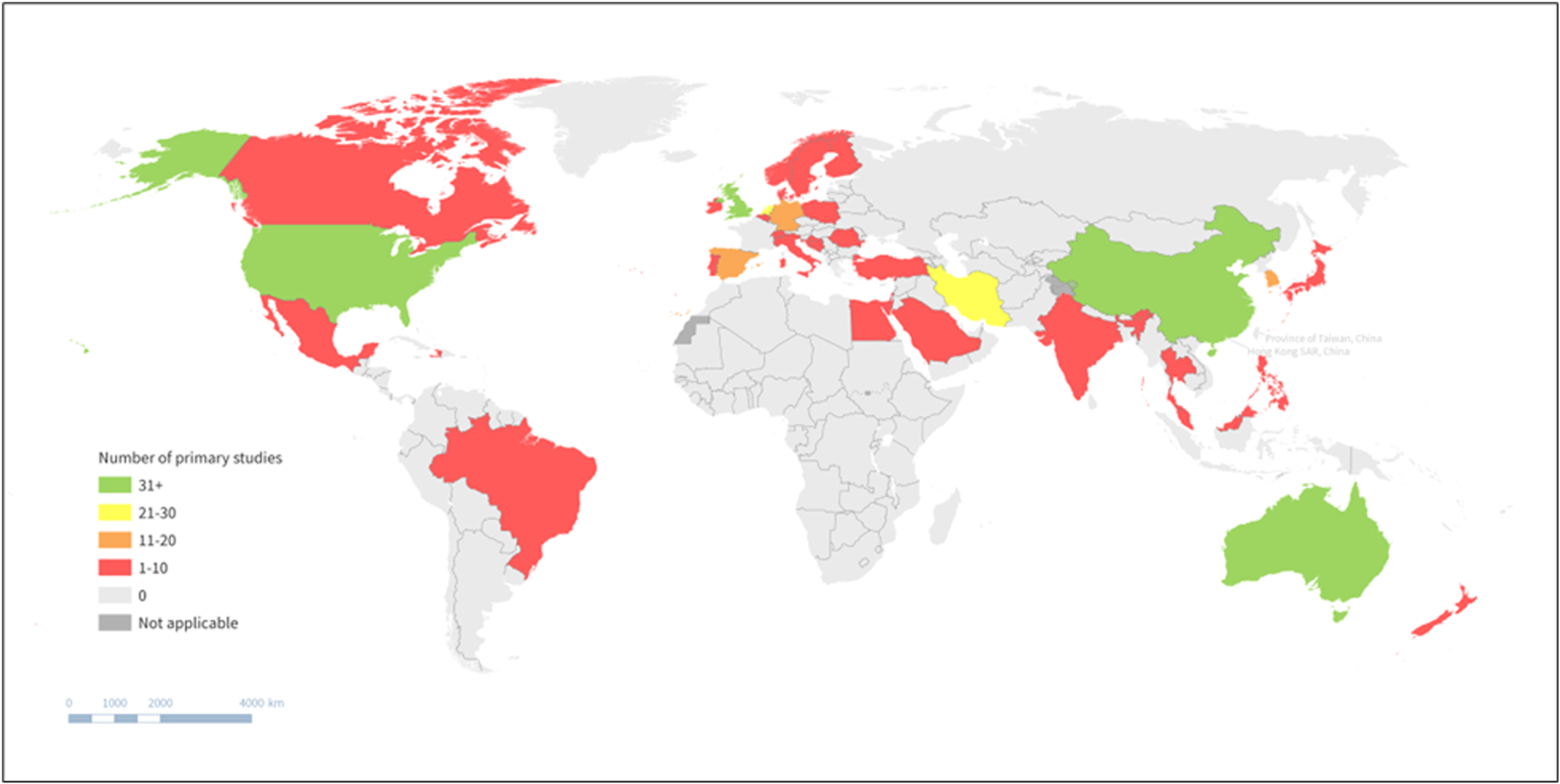
Geographic heatmap of included primary studies.
The location in which the interventions took place were further categorized using the World Health Organization (WHO) regions and the World Bank income classification. Most studies were conducted in the European Region (reviews: n = 59, 64%; primary studies: n = 138, 33%), followed by the Americas (reviews: n = 47, 51%; primary studies: n = 126, 30%), and then the Western Pacific Region (reviews: n = 42, 46%; primary studies: n = 124, 29%). Few studies were conducted in the African Region (reviews: n = 1, 1%; primary studies: n = 1, 0.24%). Over a quarter of the reviews included studies from multiple regions (reviews: n = 25, 27%) so all relevant regions were coded (Figure 17). Some reviews did not report the countries of their included studies and therefore the relevant WHO Region and World Bank Income Classification could not be determined (n = 15, 16%).
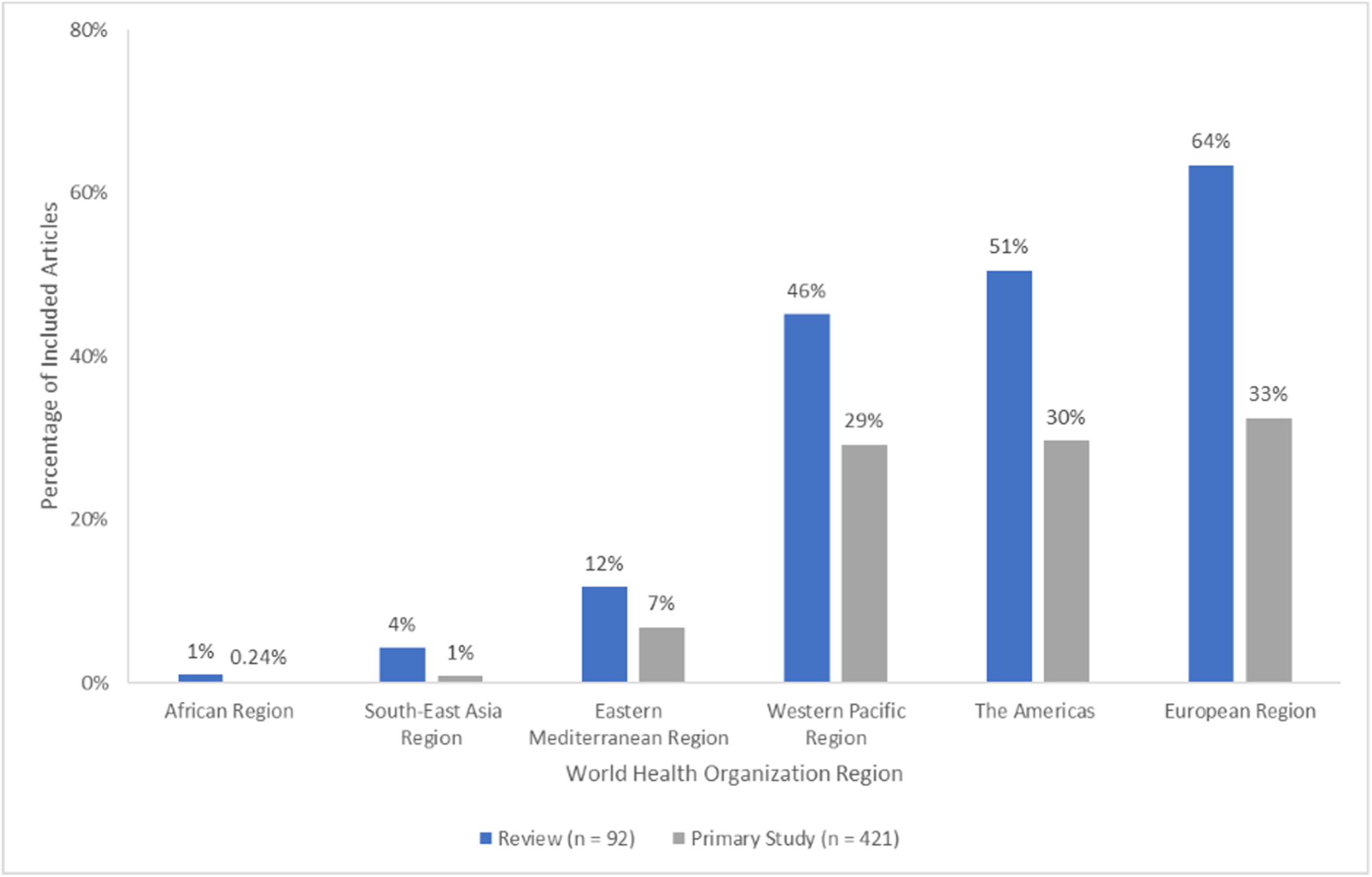
World Health Organization regions reported in included articles.
The World Bank Income Classification coding matches that of the WHO Region coding, as most studies were conducted in the European Region and the Americas, which consist mostly of high-income countries. Countries with high-income economies (reviews: n = 72, 78%; primary studies: n = 320, 76%) were reported most often, followed by upper-middle income countries (reviews: n = 28, 30%; primary studies: n = 67, 16%), then lower-middle income countries (reviews: n = 15, 16%; primary studies: n = 34, 8%). No studies took place in low-income countries. All relevant income classifications were coded for reviews that included primary studies from multiple countries with various income classes (reviews: n = 29, 31%) (Figure 18).
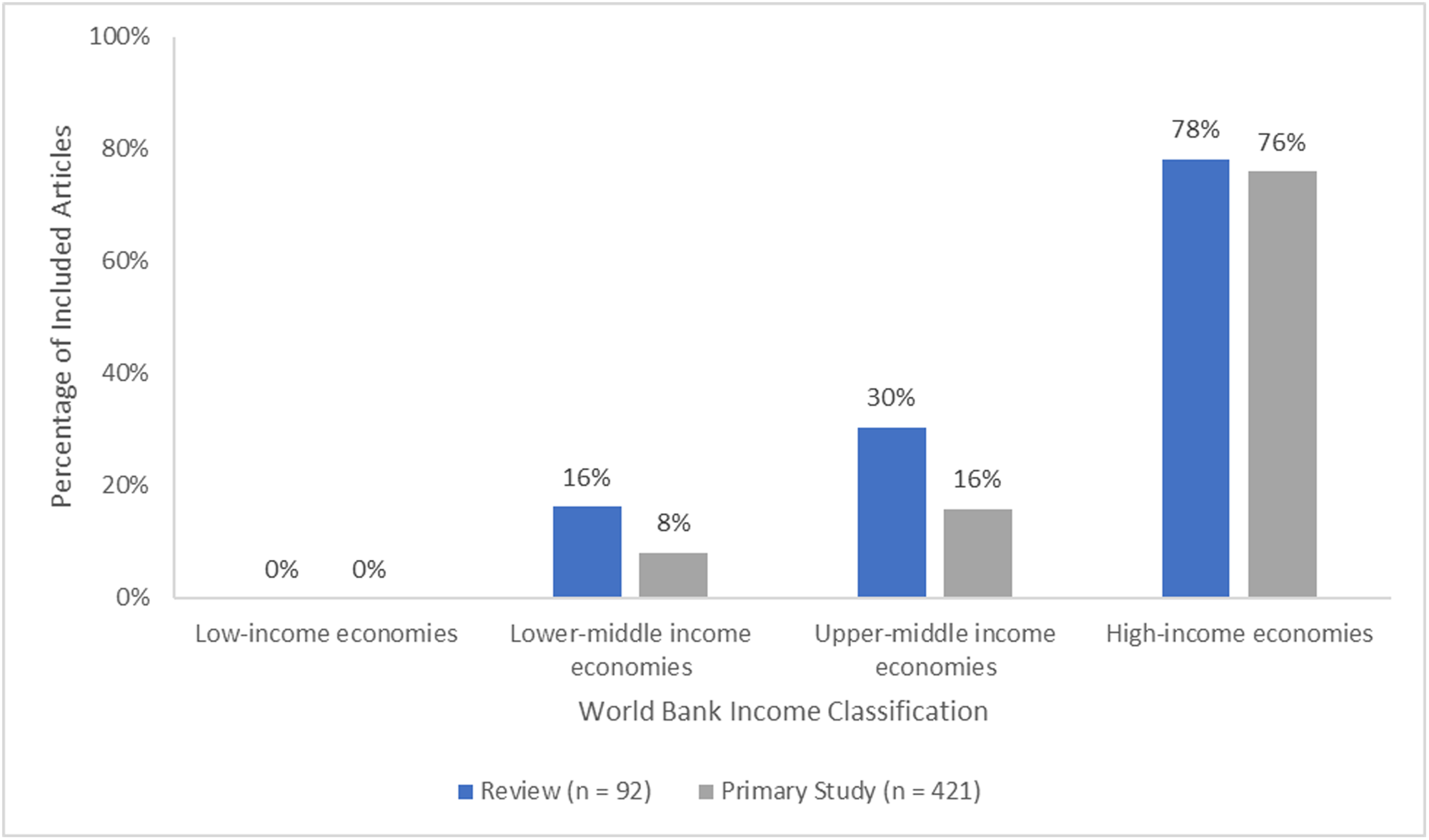
World Bank income classification of countries in included articles.
Settings
Many articles did not specify the setting (reviews: n = 56, 61%; primary studies: n = 134, 32%) that the intervention was administered in. Of those that did specify the setting, community settings, such as a community center or a park, were the most common (reviews: n = 24, 26%; primary studies: n = 90, 21%). Long-term care, or nursing homes were the second most reported setting (reviews: n = 23, 25%; primary studies: n = 53, 13%). Only one review reported the setting to be a prison (n = 1, 1%), and only 2 primary studies reported the setting to be an orphanage (n = 2, 0.48%). For studies involving interventions administered in multiple settings (reviews: n = 32, 34%; primary studies: n = 24, 6%), all relevant settings were coded (Table 4).
Intervention setting reported in included articles.
Participants needs
The needs of the participants in the included studies were identified. Social and emotional needs were the most prevalent (reviews: n = 89, 97%, primary studies: n = 401, 95%), followed by learning a new activity or language (reviews: n = 14, 15%; primary studies: n = 42, 10%) and clinical/health needs (reviews: n = 5, 5%; primary studies: n = 55, 13%). No reviews or primary studies reported participant needs for respite care. For studies involving populations with multiple needs (reviews: n = 22, 34%; primary studies: n = 123, 29%), all relevant needs were coded (Table 5).
Needs of participants reported in included articles.
Participant characteristics (PROGRESS-Plus)
We documented all PROGRESS-Plus factors described for participants in the included reviews and primary studies. Among the PROGRESS-Plus factors, age (reviews: n = 61, 65%; primary studies: n = 387, 92%) and gender or sex (reviews: n = 58, 63%; primary studies: n = 356, 85%) were the most reported. No reviews reported the religion of participants (Table 6).
Population sociodemographic characteristics reported in included articles.
Participant ages were arranged into groups based on life stages, such as childhood, adolescence, or middle-aged adulthood. Most reviews and primary studies included older adults between the ages of 60–75 (reviews: n = 55, 60%; primary studies: n = 226, 54%). Young adults aged 25–44 were the age group that was the least represented (reviews: n = 24, 26%; primary studies: n = 119, 28%) among adults. Among young people, adolescents aged 10–24 were the most represented (reviews: n = 25, 27%; primary studies: n = 135, 32%), while children under the age of 10 were included in the least articles (reviews: n = 11, 12%; primary studies: n = 34, 8%). All age groups were represented and more than half of the studies involved multiple age groups (reviews: n = 63, 70%; primary studies: n = 263, 63%). Around a third of the reviews and some primary studies did not report the age of participants (reviews: n = 33, 35%; primary studies: n = 39, 9%) (Figure 19). Overall, more reviews and primary studies combined focused on older adults ≥60 years (n = 307, 60%) than young people ≤24 years (n = 176, 34%).
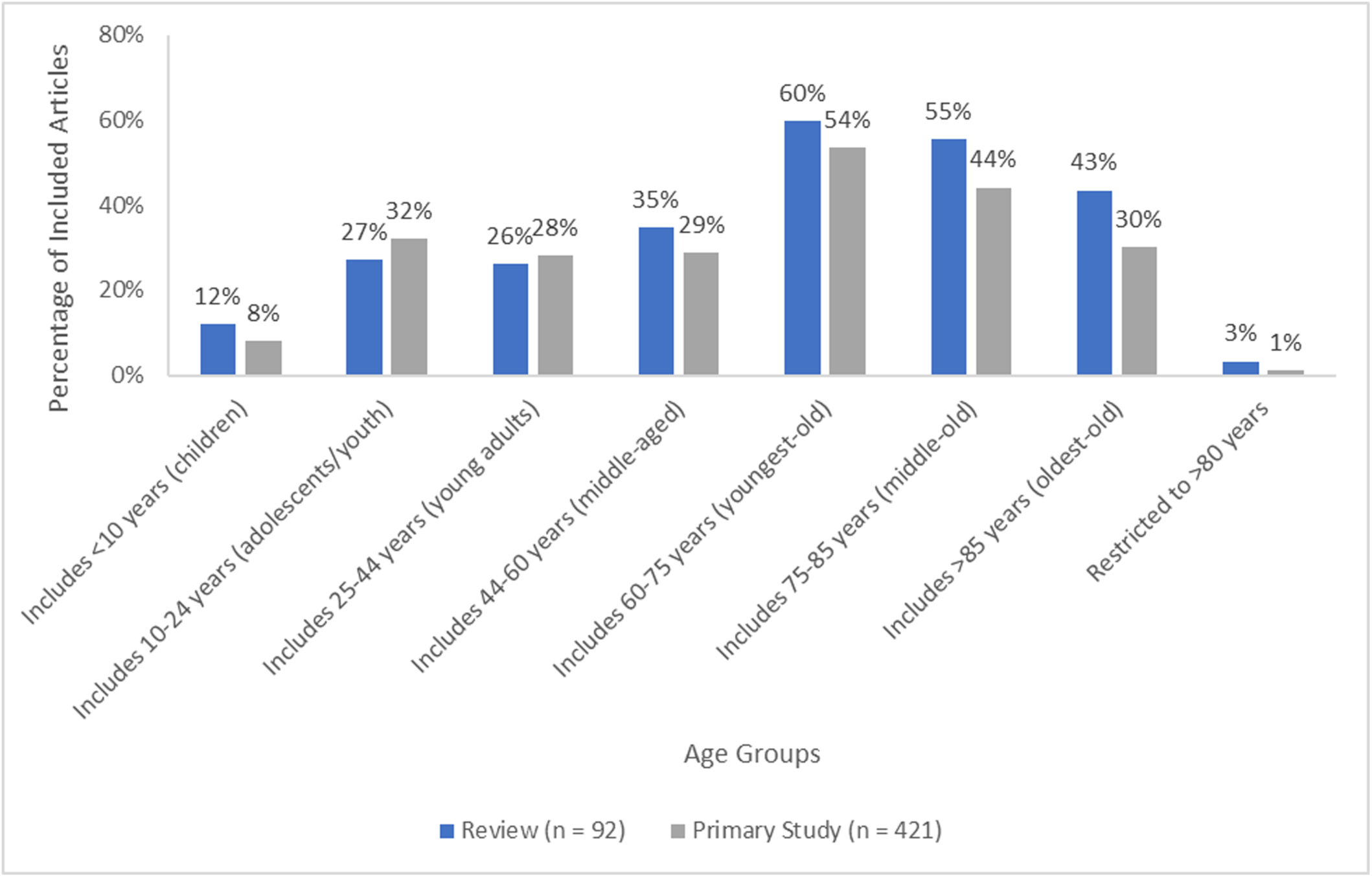
Age of participants reported in included articles.
Of the studies involving children or adolescents (reviews: n = 25, 27%; primary studies: n = 151, 36%), no reviews and few primary studies reported parental status (reviews: n = 0, 0%; primary studies: n = 12, 8%). Less than 5% of the primary studies reported children to have single parents (n = 6, 4%) or working parents (n = 6, 4%).
Health condition of participants
Participants were reported as having specific health conditions in 226 articles (reviews: n = 41, 44%; primary studies: n = 185, 44%). Since depression is commonly associated with social isolation and loneliness, we presented it separate from other mental disorders. For reviews, mental health disorders such as schizophrenia, psychosis, bipolar disorder, neuropsychiatric disorders, attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), or post-traumatic stress disorder (PTSD), but not including depression, were most reported (n = 14, 15%), followed by non-communicable diseases such as cardiovascular diseases, diabetes, or cancer (n = 12, 13%). No reviews reported participants with communicable diseases, psychological or social frailty, care dependence, discharge from hospital, or those in end-of-life/palliative care. For primary studies, non-communicable diseases were most reported (n = 63, 15%), followed by depression (n = 42, 10%). Discharge from the hospital and end-of-life or palliative care were reported in one primary study each (n = 1, 0.24%). All conditions were coded for studies involving participants with multiple conditions (reviews: n = 24, 26%; primary studies: n = 40, 16%) (Table 7).
Health conditions of participants reported in included articles.
Equity analysis
All but two reviews and 14 primary studies reported an equity focus on populations disadvantaged across PROGRESS-Plus. The most frequently reported focus was age with nearly 60% of reviews and primary studies focused on age (reviews: n = 53, 57%; primary studies: n = 247, 59%). The next most reported equity foci were loneliness (reviews: n = 40, 43%; primary studies: n = 204, 49%), health status (reviews: n = 20, 22%; primary studies: n = 116, 27%), social isolation (reviews: n = 32, 34%; primary studies: n = 52, 12%), and living situation (reviews: n = 16, 17%; primary studies: n = 69, 16%), respectively. Religion was the least reported focus, with only one primary study reporting it as a focus (n = 1, 0.24%). Two thirds of the articles focused on populations disadvantaged across multiple progress factors (reviews: n = 59, 63%; primary studies: n = 281, 67%) (Table 8).
Equity focus across PROGRESS-Plus factors reported in included articles.
Included articles used various strategies to identify participants at risk for social isolation or loneliness. Case-finding was the most common strategy for reviews (n = 11, 12%), while outreach was the most common for primary studies (n = 90, 21%), followed by case-finding (n = 77, 18%). Some of the articles utilized multiple strategies to recruit participants that were disadvantaged (reviews: n = 8, 9%; primary studies: n = 34, 8%). Most reviews and a quarter of the primary studies did not specify a strategy (reviews: n = 70, 76%; primary study: n = 105, 25%) (Figure 20).
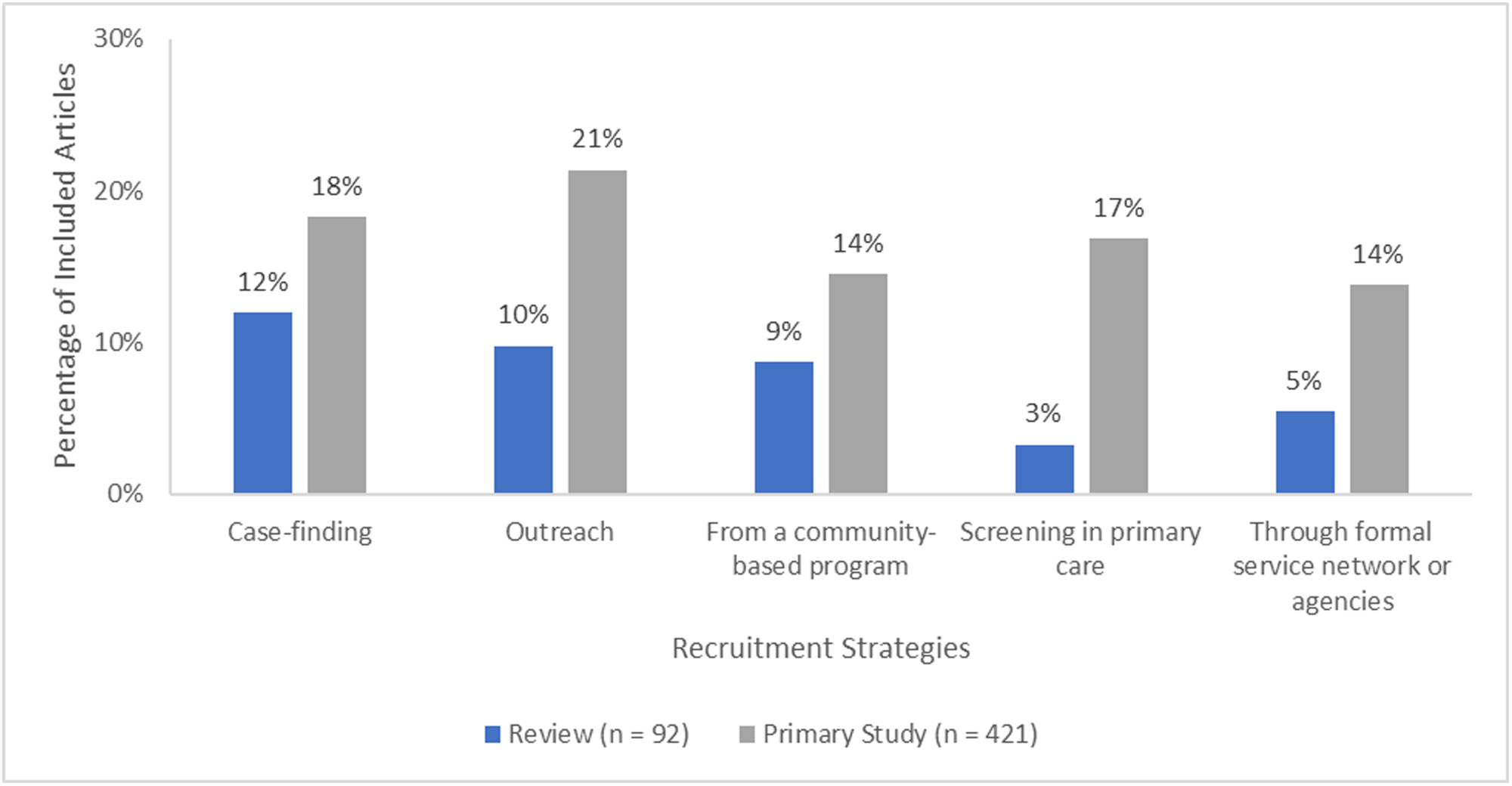
Recruitment strategies for at-risk populations reported in included articles.
Though many articles reported an equity focus, few conducted an analysis of the effects across PROGRESS-Plus. More primary studies than reviews performed a subgroup or regression analysis. Of the primary studies that performed an analysis, analysis by gender or sex was the most common (n = 13, 3%), followed by health status (n = 9, 2%), social capital (n = 7, 2%), and age (n = 5, 1%). For the reviews, analysis by age and health status (both n = 2, 2%) were most common. No reviews or primary studies performed an analysis to assess differences in effects across occupation or education. Few articles conducted an analysis of the intervention effectiveness across multiple PROGRESS-Plus factors (reviews: n = 1, 1%; primary studies: n = 10, 2%) (Table 9).
Equity analyses across PROGRESS-Plus factors conducted in included articles.
DISCUSSION
Summary of main results
This evidence and gap map has 513 included articles, majority of which are primary studies (n = 421), and the remaining of which are reviews (n = 92). Most articles were conducted in high-income countries in the European region, the Americas or the Western Pacific region. The vast majority were published between 2018 and 2022, with over 60% of reviews and 50% of primary studies having been completed in this period. However, many of these reviews are of critically low or low quality.
There is an uneven distribution of the evidence across the intervention and outcome mapping framework, with a similar pattern of evidence and gaps seen between the reviews and primary studies. Most reviews and primary studies assessed interpersonal delivery and community-based delivery interventions. Interventions for changing cognition and group activities were the most common.
Health and psychosocial outcomes were the most assessed, especially loneliness, anxiety/depression, and quality of life. Social support and social engagement were the most assessed indicators of social connections.
All age groups were represented but more studies and reviews disproportionately focused on older adults ≥60 years (60%) than young people ≤24 years (34%). Although many reviews and primary studies had an equity focus on populations disadvantaged across PROGRESS-Plus factors, only few focused on reaching vulnerable populations across the PROGRESS factors. Most focused on reaching vulnerable populations across the Plus factors, such as populations at risk of social isolation or loneliness, age, health status, and living situation. However, few described how at-risk populations were recruited and even fewer performed an analysis to assess differences in effects across PROGRESS-Plus factors for populations experiencing inequities.
People using this map will be able to find all systematic reviews and primary studies of the interventions of interest. However, they need to be aware that systematic reviews and primary studies with multiple interventions or intervention components are coded as relevant for each intervention.
Areas of major gaps in the evidence
Major gaps were identified in societal level delivery interventions focusing on norms, laws, and policies (e.g., public health policies that promote cohesion and inclusion). Community-based delivery interventions focusing on structural changes in the community to improve opportunities for social interactions or access to amenities (e.g., age-friendly communities with well-maintained sidewalks, stairs that have railings, recreational facilities, accessibility ramps) were lacking. Some outcomes were hardly assessed such as some indicators of social connections (social capital and social cohesion), cost and cost-effectiveness, and barriers of implementation or access of interventions. The quality assessment with AMSTAR2 showed a major gap in high or moderate quality reviews.
Social isolation and loneliness are major public health concerns that can be addressed through collaboration with other sectors. Most of the evidence is from the clinical and population health sector with major gaps in other sectors including transportation, housing, work, nutrition, environment, and spiritual care indicating the need for more collaboration across sectors to effectively alleviate social isolation and loneliness.
There were gaps in the geographic distribution of studies with limited evidence available for Africa and none in low-income countries.
Potential biases in the mapping process
The search strategy for identification of potentially eligible studies was comprehensive and covered published literature until February 2022. Rigorous methods were used to identify eligible studies and reviews, and to assess review quality, including screening title and abstract, and full text for inclusion in duplicate, as well as assessment of review quality using AMSTAR2 in duplicate, with all conflicts resolved via consensus. However, we did not assess the quality of primary studies and the certainty of the evidence is therefore inconclusive.
The research question was on the effectiveness of in-person face-to-face interventions for reducing social isolation and loneliness, and we only included study designs which assessed effectiveness. Outcomes were not used as eligibility criteria, only the study population, intervention, study aim and study design. Studies assessing the effects of in-person face-to-face interventions on social isolation and loneliness and other indicators of social connections such as quality of life or depression/anxiety were included.
Our search may not have captured all gray literature or unpublished and more recently published eligible studies or reviews. No language restrictions were applied to the search, but mainly English-language databases were searched, and it is possible some relevant studies published in non-English languages may have been missed. Furthermore, reference lists of included systematic reviews were not screened, and therefore some additional eligible studies may not have been identified. In addition, we did not contact authors for missing information which may limit the mapping of evidence.
Lastly, mapping the interventions into the mutually exclusive categories of the conceptual framework developed for this evidence and gap map was challenging due to the lack of consistency between articles with respect to terminology, as well as lack of a standardized framework for the classification of interventions for social isolation and loneliness. The socio-ecological framework has been adopted in most existing frameworks and reviews, but it does not allow for mutually exclusive categorization of interventions since it examines risk and protective factors that occur and interact across levels. We therefore developed a pragmatic approach to categorize interventions focusing on who delivered the interventions and where they were delivered.
Limitations of the EGM
This evidence and gap map does not include primary studies without a control group, nor studies with a qualitative design or association studies. While these studies may provide valuable information about interventions to reduce social isolation and loneliness, they do not assess the effectiveness of these interventions.
Most included articles do not focus on reaching populations vulnerable across PROGRESS-Plus factors, such as place of residence (urban/rural), race/ethnicity (ethnic minority groups), gender/sex (LGBTQIA2S+ populations), religion, socioeconomic status, living alone and caregivers. While focusing on addressing the needs of those at risk or experiencing social isolation and/or loneliness, the elderly, or children, those with a disability or health condition, there are other vulnerable populations who are disadvantaged across the PROGRESS factors that may also be socially isolated or lonely and could benefit from targeted interventions.
Less than 10% of all included articles assessed process indicators or implementation outcomes, which means there is limited evidence regarding barriers to implementation of these interventions, as well as their acceptability, feasibility, and participant adherence.
In addition, only two non-randomized studies and one moderate quality review assessed societal level delivery intervention, thus there is limited evidence regarding the effectiveness of these interventions. Although many studies and reviews assessed community-based delivery interventions, there is limited evidence of the effectiveness of interventions focusing on structural community changes to reduce social isolation or loneliness since only one review considered interventions to promote age-friendly communities.
A higher proportion of included reviews and studies focused on older adults than young people. Social isolation and loneliness have been studied more in adults than young people (Eccles et al., 2021) and most of the existing frameworks we found focused on the experiences of older adults; only one focused on children. There is therefore limited information about differences that might exist between older adults and younger people's experience of social isolation and loneliness.
Stakeholder engagement throughout the EGM process
We sought input from stakeholders from organizations interested in social isolation and loneliness as described in the methods section (Stakeholder engagement)and there were no changes with stakeholder engagement throughout the EGM process.
AUTHORS’ CONCLUSIONS
Implications for research, practice and/or policy
Social isolation and loneliness are growing public health concerns, which have been highlighted by the COVID-19 pandemic with respect to lockdowns, as well as by the surge of research appearing in more recent years. This evidence and gap map shows the available evidence regarding in-person interventions to alleviate social isolation or loneliness within any age group. Of the 92 systematic reviews that were included in this map, nearly 70% were of critically low quality, and over 40% have been published since 2020, with most included reviews being published in 2021. Much of the evidence is clustered around interpersonal delivery and community-based delivery interventions, which reported on health and psychosocial outcomes or indicators of social connectedness. Most of these interventions focused on an individual perspective by reducing loneliness or anxiety/depression symptoms, and/or improving participant quality of life/well-being. Most included articles focused on reaching vulnerable populations across the Plus factors, such as populations at risk of social isolation or loneliness, age, health status, and living situation.
Major gaps in the evidence can be seen in research that looks at interventions based on structural community changes (e.g., age-friendly communities with well-maintained sidewalks, stairs that have railings, recreational facilities, accessibility ramps) and societal-level changes. There were gaps in research assessing process indicators for outcomes, such as acceptance, adherence, barriers, and feasibility of intervention implementation. With the rise in levels of social isolation and loneliness (Ernst et al., 2022; O'Sullivan et al., 2021), it is important to not only consider the efficacy of interventions which aim to alleviate social isolation and loneliness, but also the feasibility and barriers to implementing these interventions, as well as their acceptability by participants. Very few reviews and primary studies described how at-risk populations were recruited and even fewer performed an analysis to assess differences in effects across PROGRESS-Plus factors for populations experiencing inequities. Moreover, much of the research was done in high-income or upper-middle-income countries, specifically in the United States, United Kingdom, China, Australia, and the Netherlands, with no research conducted in low-income countries. Loneliness and social isolations are common issues but complex to resolve—we need whole systems solutions and therefore interventions that only utilize one type of approach may be effective only in a specific population/community. To combat loneliness and social isolation more effectively, we need effective strategies and solutions across all sectors working in synergy with each other.
Despite recent increases in evidence in the past years, there is an uneven distribution, with most focusing on interpersonal delivery or community-based delivery interventions which aim to alleviate loneliness or symptoms of depression/anxiety or improve participant quality of life/well-being. The majority of published systematic reviews are of critically low quality, emphasizing the need for more high-quality reviews.
This evidence and gap map contributes toward building an evidence base that can be used to inform future policy decisions, as well as guide future researchers and funders to fill in some of the identified evidence gaps.
Footnotes
ACKNOWLEDGMENTS
We gratefully acknowledge the participation of stakeholders in our stakeholder consultation.
This project was funded by the World Health Organization.
CONTRIBUTIONS OF AUTHORS
Content: VW, ETG, NH, SB, SD, EdG, JHL, ML, MLim, KM, PQ, CC, PH, CM EGM methods: VW, ETG, PH, CM, SD, VB, AA, EB, MB, PD, RD, JH, TH, AJ, FJ, LM, WYC, RMY, TAMTM, AW, AAA, RI, SA Information retrieval: DS
DECLARATIONS OF INTEREST
Vivian Welch is editor-in-chief of the Campbell Collaboration. The editorial process was handled by an independent editor and VW had no input in the editorial process or decisions.
Julianne Holt-Lunstad and Michelle Lim were co-investigators on the KIND challenge intervention aimed at reducing loneliness which was sponsored by the app Nextdoor.
Dr. Kate Mulligan has been a contract consultant for the Canadian Red Cross, a provider of in-person interventions to reduce social isolation and loneliness. She has also been involved in intervention projects related to social prescribing with the Alliance for Healthier Communities.
Pamela Qualter was involved in two reviews used to gather data for the current evidence gap review; she was not involved in any primary research in the subject area of the review.
Mathias Lasgaard was involved in one review used to gather data for the current evidence gap review.
Sierra Dowling is the managing editor of the Campbell Ageing Coordinating Group, but the editorial process was handled by another managing editor.
Paul Hebert is the Chief Medical and Science advisor for the Canadian Red Cross.
Christopher Mikton works for the World Health Organization which has helped fund this evidence and gap map.
Elizabeth Ghogomu, Wan Yuen Choo, Raudah Mohd Yunus, Tengku AM Tengku Mohd, Niobe Haitas, Sivan Bomze, Simone Dahrouge, Edward Garcia, Victoria Barbeau, Tarannum Hussain, Ella Beveridge, Arpana Wadhwani, Ali Al-Zubaidi, Payaam Desai, Jimmy Huang, Rebecca Doyle, Sarah Allam, Rayan Ibrahim, Leen Madani, Abdulah Al Ameer, Alyssa Jearvis, Mostafa Bondok, Fatima Jahel and Douglas M. Salzwedel, have no conflicts of interest.
PLANS FOR UPDATING THE EGM
The EGM will be updated every 2 years.
SOURCES OF SUPPORT
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
We did not screen the references of included systematic reviews to identify additional primary studies because of time constraints.
CHARACTERISTICS OF STUDIES
| Study | Reason for exclusion |
|---|---|
| Fokkema et al., 2007 | Study design (not a systematic review of effectiveness) |
| Lee, 2014 | Evidence/aim (not to reduce social isolation or loneliness) |
| Lin et al., 2020 | Intervention (digital) |
| Low et al., 2015 | Study design (a non-comparative primary study) |
| Mächler et al., 2022 | Study design (a non-comparative primary study) |
| Purewal, 2017 | Study design (not a systematic review of effectiveness) |
| Roessler, 2012 | Evidence/aim (not to reduce social isolation or loneliness) |
| Scazufca, 2022 | Evidence/aim (not to reduce social isolation or loneliness) |
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.