
Abstract
Background
Parental substance misuse is a pervasive risk factor for a range of detrimental outcomes for children across the life course. While a variety of interventions have been developed for this population, the existing evidence-base requires consolidation and consideration of the comparative effectiveness of different interventions to facilitate evidence-informed decisions between different intervention approaches.
Objectives
This review aimed to use network meta-analysis to synthesise the comparative effectiveness of psychosocial, legal, and pharmacological interventions for improving outcomes for children with substance misusing parents. Network meta-analysis was not possible; however, we synthesised the effects of a broad range of interventions on child psychosocial outcomes. Another aim was to examine potential moderators of the effects, yet this was also not possible due to data limitations. A secondary objective was to qualitatively synthesise economic, treatment completion, and treatment acceptability information for included studies.
Search Methods
Searches were performed in November 2020 and again in April 2021. Encompassing multiple disciplines, we searched 34 databases, 58 grey literature repositories, and 10 trial registers. Supplementary hand searches were conducted on 11 journals, along with harvesting the references of all included studies and existing reviews, and forward citation searching each report of all included studies. Study authors were contacted to obtain missing data.
Selection Criteria
Eligible studies included randomised and quasi-experimental evaluations of psychosocial, pharmacological, and/or legal interventions using either a placebo, no treatment, waitlist control, treatment-as-usual, or alternative treatment as a comparison condition. Study participants needed to be comprised of families with children under the age of 18 with one or more currently substance-misusing parents (or caregivers). Studies were required to evaluate the eligible intervention using a child-focused psychosocial outcome. If reported in eligible studies, the following secondary outcomes were also synthesised in the review: cost-effectiveness, treatment completion, length of time in treatment and acceptability of treatment (e.g., participant perspectives of the intervention). There were no restrictions placed on publication status or geographic location, however only research written in English was included.
Data Collection and Analysis
Standard methodological procedures were followed across all stages of the review, as guided by the published protocol for the review (Eggins et al., 2020). Due to the inability to conduct network meta-analyses, random effects pairwise meta-analyses with inverse variance were used to synthesise effects when two or more studies with conceptually similar interventions and outcomes were available. Results of the meta-analyses are displayed in forest plots, and separate analyses are provided for conceptually distinct outcomes and time-points of measurement. Sensitivity analyses are used to explore possible sources of heterogeneity in the absence of sufficient studies to conduct subgroup analyses.
Main Results
99 studies (reported in 231 documents) met review inclusion criteria, encompassing 22,213 participants. Most studies were conducted in the United States (k = 76), almost half were randomised controlled trials (k = 46), and the most common comparator was treatment-as-usual (k = 50). Interventions were evaluated using a large range of child psychosocial outcomes which broadly fell under: (a) child welfare; (b) child development; (c) child emotional and behavioural; and (d) educational domains. Intervention models were rarely only legal or pharmacological in nature, with most studies evaluating integrated psychosocial treatments with either pharmacology, coordinated health care, case-management, and/or judicial or child welfare oversight and coordination. Thirty-six meta-analyses and 227 single effect sizes were used to appraise the effectiveness of included interventions, based on 68 studies with sufficient data for effect size calculation. The size and direction of the effects varied across interventions, type of outcomes, and time-point of measurement. Twenty-seven meta-analyses and 186 single effect sizes suggested null effects. Only five single effect size estimates based on three studies indicated negative effects including: higher depressive and somatisation symptoms (parent-report), hopelessness (child-report), educational achievement difficulties (parent-report), and substantiated child protection reports for those engaged with interventions versus treatment-as-usual or no treatment. Nine meta-analyses and 36 single study effect estimates suggest that psychosocial, pharmacological and/or legal interventions have a positive effect on a range of specific child welfare, developmental, and emotional/behavioural outcomes for children. The risk of bias varied across domains and studies, which further lowers confidence in the results. Based on a subset of included studies, treatment completion tends to vary, yet cost-benefits can be achieved when intervening with children whose parents misuse substances.
Authors' Conclusions
Despite a large body of evaluation evidence, disparate outcomes, and missing data precluded analyses to formally examine the comparative effectiveness of psychosocial, legal, and pharmacological interventions for improving outcomes for children with substance misusing parents. The large amount of unreported (missing) data meant that many effect estimates were underpowered due to single studies and small sample sizes. The review findings suggest that interventions for families affected by parental substance misuse can be effective when they holistically address multiple domains such as parent wellbeing/mental health, parenting, children's wellbeing, and/or other factors impacting family wellbeing (e.g., housing).
PLAIN LANGUAGE SUMMARY
Psychosocial, pharmacological, and legal interventions have variable effects on the psychosocial outcomes of children whose parents misuse substances
Ninety-nine studies examined the effects of psychosocial, legal, and pharmacological interventions compared with treatment-as-usual (TAU) or other treatments for children in families affected by parental substance misuse. The quality of the evidence varies, and the effectiveness of interventions differs across outcomes and timing of measurement after intervention completion.
What is this review about?
Parental substance misuse is a pervasive risk factor for a range of detrimental outcomes for children across the life course. A range of interventions have been developed for this population, but the existing evidence-base requires consolidation to facilitate evidence-informed decisions between different intervention approaches.
This review synthesises the full array of psychosocial, pharmacological, and/or legal interventions for families affected by parental substance misuse, including interventions that integrate psychosocial, pharmacological, legal intervention approaches. The effectiveness of these interventions is assessed using a broad range of child psychosocial outcomes, including engagement with child protection agencies, development, psychological and behavioural wellbeing, and educational engagement and achievement.
What is the aim of this review?
This review aimed to consolidate and synthesise the effectiveness of psychosocial, pharmacological, and legal interventions on the psychosocial outcomes of children with substance misusing parents. The review synthesises evidence from 46 randomised controlled trials (RCTs) and 53 high-quality quasi-experiments.
What studies are included?
This review includes 99 studies, mostly conducted in the United States, spanning the period from 1984 to 2021. Included studies compare a psychosocial, pharmacological and/or legal intervention to TAU, an alternative treatment, or no treatment. All included studies examine the impact of the intervention upon completion, and a smaller number also examine effectiveness at later time-points (e.g., 6-months or more).
What are the main findings of this review?
The most robust findings from this review are drawn from 36 meta-analyses. These suggest that integrated interventions can reduce child abuse potential, the likelihood of out-of-home care (OOHC), and overall child emotional and behavioural difficulties in the short-term (small to medium sized effects). Integrated interventions typically combine psychosocial support for multiple areas of family wellbeing (e.g., parent substance misuse, parenting, child and parent psychological wellbeing), sometimes with pharmacological (e.g., opioid replacement therapy), legal components (e.g., Family Treatment Drug Courts [FTDCs]) and comprehensive case-management. These interventions can also increase the odds of parents retaining care of their children, enhance expressive language development, increase children's knowledge of substance misuse, and increase child prosocial behaviours in the short-term (small to medium sized effects). There is preliminary evidence that effects are maintained within 6 to 12 months post-intervention for total child emotional and behavioural difficulties (small sized effect). However, the evidence for effectiveness for other outcomes was less clear. At treatment completion, this includes: children's permanent placements (with parents, via adoption, or via long-term foster care/guardianship), some child development outcomes (cognition, receptive language, motor, and social skills), and some emotional/behavioural issues at posttreatment (e.g., externalising issues, internalising issues, level of anger, anxiety symptoms, depressive symptoms, self-concept, and locus of control). At follow-up from 3 to 18-months, evidence for effectiveness was less clear for child abuse potential, externalising issues, internalising issues, prosocial behaviours, and antisocial behaviours.
What is the quality of the evidence?
The quality of the evidence for psychosocial, pharmacological and/or legal interventions for children with substance misusing parents varies. This variation, along with large amounts of missing data, reduces the confidence that can be placed in the findings for many outcome categories.
What do the findings of this review mean?
The evidence for psychosocial, pharmacological, and/or legal interventions for families affected by parental substance misuse has not yet reached a point where clear conclusions can be made about the effectiveness of the full range of interventions across the full range of child psychosocial outcomes. However, there is reliable evidence for interventions that integrate parent substance misuse treatment with other components that simultaneously aim to alleviate vulnerability in other areas of the family ecology. The amount and quality of the evidence needs to continue growing so that policy makers and practitioners can make evidence-based decisions that are most likely to improve the lives of families affected by parental substance misuse.
How up-to-date is this review?
The review authors searched for studies that were reported through to April 2021.
BACKGROUND
The problem, condition or issue
An extensive body of literature documents the adverse outcomes of children who are raised in families with parental substance misuse. These include increased risk and reports of child abuse and neglect (Wekerle et al., 2007; Williams et al., 2011, Taplin et al., 2014), poor cognitive development and educational attainment (Lambert & Bauer, 2012; Park & Schepp, 2014; Richardson et al., 2015), psychopathology (Christoffersen & Soothill, 2003; Bountress & Chassin, 2015; Hser et al., 2014; McGovern et al., 2023; Marmorstein et al., 2009; Vidal et al., 2012), and adolescent substance misuse and antisocial behaviour (Burlew et al., 2013; Clark et al., 2005; King et al., 2006, 2009; Lambert et al., 2012, 2013; Walden et al., 2007).
Parental substance misuse typically co-occurs in the context of multiple risk factors across domains of parent and family functioning. These include parental psychopathology and criminality, domestic violence, and severe poverty (e.g., see Grella et al., 2006; Hser et al., 2015; Miller et al., 2013; Skinner et al., 2010). Thus, the accumulation and interplay between risk factors, rather than parental substance abuse per se, results in multiple and complex family environments that place considerable challenges on parents, which then contributes to poor child outcomes (e.g., see Conners et al., 2004; Nair et al., 2003; Velleman & Templeton, 2007). Neger and Prinz (2015) propose a conceptual framework with multiple interrelated pathways to explain how parental substance misuse directly and indirectly impacts risk factors predictive of poor child outcomes (see also Dunn et al., 2002; Eiden et al., 2014; Finger et al., 2014; Miller et al., 2014; Shorey et al., 2013; Twomey et al., 2013). For example, parents with substance misuse issues often have difficulty regulating negative emotional states or experience co-occurrence of mental health disorders (Whitaker et al., 2006; Smith et al., 2009), which can impact their capacity to assess and attend to their child's emotional wellbeing and needs (Borelli et al., 2010, 2012; Siqveland et al., 2014) or responsively parent their child according to child developmental needs (Velez et al., 2004; Slesnick et al., 2014). A history of trauma and childhood adversity is also common in parents with substance misuse problems (Hatzis et al., 2019) and this, combined with the risk factors above, make sensitive and responsive caregiving challenging (Hatzis et al., 2017). Importantly, deficits in parent emotional regulation and the capacity to responsively parent are key predictors of child abuse and maltreatment (Stith et al., 2009).
Global estimates indicate that approximately 5%–10% of all children are being raised in families with one or more parent who misuses alcohol or other drugs (Dawe et al., 2006; Jääskeläinen et al., 2016; Manning et al., 2009; Raninen et al., 2015; SAMHSA, 2014). This prevalence and the complexities and enduring challenges associated with parental substance misuse has led to the development of a range of approaches that aim to reduce risk factors, enhance family functioning, and improve child outcomes. Importantly, recent estimates suggest that for every dollar invested into substance misuse treatment, there are significant cost savings for society (Dalziel et al., 2015; National Institute of Drug Abuse, 2012; Public Health England, 2014). However, a critical limitation of the current evaluation and review literature is the lack of integration and synthesis of the relative effectiveness of different intervention models that aim to improve the outcomes for children with substance misusing parents. Without a clear understanding of the relative effectiveness of different intervention approaches, practitioners and policy-makers are limited in their ability to make informed and reliable choices between intervention models. Therefore, this review provides a comprehensive synthesis of psychosocial, pharmacological, and legal interventions in the context of parental substance misuse and the impact of these interventions on child psychosocial outcomes. Moreover, the review will provide a unique contribution by producing network diagrams of the extant evidence, along with a comparative examination of components across the different interventions that have been evaluated. The protocol for this review (Eggins et al., 2020) outlined a plan to conduct network meta-analyses which would have provided a quantitative synthesis of the comparative effectiveness of these different intervention approaches (see Hutton et al., 2015; Mavridis et al., 2015; Salanti, 2012; Wilson et al., 2016). Unfortunately, this analysis approach was not possible due to the nature of the existing evidence base (see Data Synthesis section).
The intervention
This review included all possible psychosocial, legal, and/or pharmacological interventions that explicitly aim to improve the psychosocial wellbeing of families in which at least one parent has either a current substance misuse problem or is in treatment for substance misuse problems. The focus of the review is on studies that examine the impact of psychosocial, legal, and/or pharmacological interventions on child psychosocial outcomes. For the purposes of this review, we draw on Maynard et al. (2015) and define a psychosocial intervention to be those that are implemented by professional practitioners (e.g., clinicians, social workers, teachers) across a variety of settings (e.g., homes, school, community, clinics, residential facilities, and/or hospitals) that aim to address psychological and social wellbeing more generally. Example psychosocial interventions are integrated models that address both parental substance misuse and other areas of difficulty such as parenting, family relationships, and/or emotion regulation (e.g., Barlow et al., 2019; Donohue et al., 2014; Lam et al., 2009). We draw on Eggins et al. (2020) and Mazerolle et al. (2018) and define a legal intervention to be ‘a strategy, technique, approach, activity, campaign, training, directive, or funding or organisational change that involves the criminal justice system' (p. 21). Example legal interventions include FTDCs (Zhang et al., 2019) and specific legislation that regulates the management of families affected by parental substance misuse (e.g., Sanmartin et al., 2020). We define pharmacological interventions to be medication or pharmacy-related approaches (e.g., buprenorphine or methadone) to treating parental substance misuse or its immediate effects on infants (e.g., neonatal abstinence syndrome [NAS]). A comprehensive description and synthesis of interventions that have been evaluated is provided in the ‘Included studies’ section.
How the intervention might work
Due to the wide range of interventions included in this review, there are a number of possible mechanisms by which interventions might work. In a general sense, interventions for substance misusing parents are likely to impact child outcomes by modifying or reducing the impact of known risk factors, including: parental psychopathology, parenting knowledge and skills, enhancement of the quality of the parent-child relationship, involvement in the criminal justice or child welfare systems, or impoverished environments. Different categories of interventions may impact child outcomes through more specific pathways. For example, interventions based on addiction disease models generally use a 12-step model, focusing on abstinence, psychoeducation, and knowledge as key mechanisms through which change can occur (for a review see Usher et al., 2015). In comparison, family-focused prevention models target risk and protective factors linked with parent substance misuse to generate change (for a review see Usher et al., 2015). Pharmacological interventions aim to reduce drug use, thereby reducing foetal exposure and improving birth and developmental outcomes (Minozzi et al., 2013). Legal interventions, such as FTDCs, aim to reduce the risks associated with parental substance misuse through providing support, whilst motivating behaviour change through incentives and penalties (Fay & Eggins, 2019). Therapeutic or psychosocial interventions also aim to improve child outcomes by reducing the risks associated with parental substance misuse, yet the theoretical models that underpin interventions in this category vary depending on the focus of the intervention (for reviews see Harnett & Dawe, 2012; Neger & Prinz, 2015). An emerging area in the literature is the examination of specific mechanisms of change underpinning interventions for families affected by parental substance misuse (e.g., Suchman et al., 2011, 2018; Dawe et al., 2021), with improvements in parent emotion regulation identified as a key avenue through which interventions impact child outcomes (see Dawe et al., 2021).
Why it is important to do this review
The current evaluation and review literature lacks integration and synthesis of the relative or comparative effectiveness of different intervention models that aim to improve the outcomes for children with substance misusing parents. Without a comprehensive and integrated synthesis of the extant evaluation literature, it is difficult for practitioners, policy-makers, and researchers to focus their resources and decision-making to improve the lives of children and families affected by parental substance misuse. Before conducting the systematic search for this review (mid-2021), at least 24 existing reviews were identified that (a) focused on interventions specifically for substance misusing parents and that (b) captured one or more studies that had assessed the impact of an intervention on child psychosocial outcomes. Additional reviews have been captured by and harvested within this systematic review (e.g., Ritland et al., 2020; Shan et al., 2020), and others have likely been published since the systematic search date for this review. Although not all reviews adhere to a full systematic review methodology, each employed at least two systematic review techniques (e.g., systematic search, specific inclusion criteria, qualitative or quantitative synthesis of studies) and can be considered less biased than narrative reviews in the area (e.g., see Choi, 2012; Marsh et al., 2011; Oliveros & Kaufman, 2011; Renk et al., 2015). These reviews highlight the range of interventions that have been evaluated, with variations in review focus according to the specific intervention under consideration and whether only child outcomes or multiple different types of outcomes are included. These reviews can be summarised as follows: One review examines the impact of home-visiting interventions during pregnancy and the postnatal period for women with substance misuse issues and their impact across a range of parental and child outcomes (Turnbull & Osburn, 2012); Three reviews focus on FTDCs for substance misusing parents with and their impact on child out-of-home placement (Llyod, 2015), child welfare system outcomes (Zhang et al., 2018), or child maltreatment outcomes (Eldred & Gifford, 2016); One review examines the impact of integrated interventions for substance misusing mothers and their impact on multiple child outcomes (Niccols et al., 2012); Four reviews focus on parenting interventions for substance misusing parents across multiple parent and child outcomes (Bowie, 2005; Moreland & McRae-Clark, 2018; Neger & Prinz, 2015; Peisch et al., 2018); Two reviews and one Cochrane protocol concentrate on child-focused preventative interventions for improving outcomes for children of substance misusing parents (Bröning et al., 2012) or alcohol misusing parents (Cuijpers, 2005; McLaughlin et al., 2014); Two Cochrane reviews examine the impact of pharmacological interventions during pregnancy on maternal and child outcomes in the context of alcohol misuse (Smith et al., 2009) and opioid dependence (Minozzi et al., 2013); and Several reviews capture a broad range of psychosocial interventions for parental substance misuse and their impact on multiple outcomes (including child outcomes) for either alcohol misuse during pregnancy (Lui et al., 2008; Scobie et al., 2017; Stade et al., 2009) or all types of parental substance misuse (Austin & Osterling, 2006; Calhoun et al., 2015; Heimdahl & Karlsson, 2016; Leppard et al., 2018; McGovern et al., 2021; Mitchell & Burgess, 2009; Murphy et al., 2017; Templeton et al., 2010; Usher et al., 2015).
The existing review literature is clearly extensive, yet there is variation in the degree of methodological quality and content coverage. In addition, variations in review methodological quality and gaps in content coverage reduce the ability to draw reliable conclusions about the effectiveness of interventions for improving psychosocial outcomes for children with substance misusing parents.
Methodological limitations of existing reviews
Perhaps the most important methodological limitation of existing reviews is the lack of quantitative syntheses. Very few the reviews used meta-analysis to synthesise the evaluation evidence (e.g., Minozzi et al., 2013; Niccols et al., 2012; Turnbull & Osburn, 2012; Zhang et al., 2018), despite the availability of evidence to do so for many. Rather, authors provide qualitative summaries of intervention effectiveness that are based on the raw differences, statistical significance, or effect sizes of individual studies. Although qualitative summaries are useful for assessing the breadth and qualities of intervention research, this methodology is inadequate for providing a reliable and precise estimate of an intervention impact (Borenstein et al., 2009; Littell et al., 2008).
An examination of the search methods for the existing body of reviews also highlights the need for an updated and more comprehensive systematic search. First, existing reviews may not provide an accurate representation of the most up-to-date intervention evidence because between 5 and 10 years have passed since the searches were conducted for many. Second, there may be potential biases in the existing reviews. Some authors excluded studies that found negative intervention effects or only reported study outcomes if they were statistically significant. Others introduced publication bias by either explicitly excluding documents not published in peer-reviewed journals, omitting searches for unpublished literature, or limiting searches to very few sources. In addition, some authors implemented restrictive searches, such as very limited search terms or multiple Boolean AND clauses. Third, most current reviews lack transparency in the reporting of searches and sensitive search strategies. Many authors do not explicitly report their exact search and how it was implemented during their systematic search. Collectively, these issues may lead to omitting important evaluation evidence or bias the conclusions of the reviews.
Content gaps in existing reviews
The current corpus of reviews does not provide complete coverage of the extant literature. Some reviews focus exclusively on mothers (e.g., Niccols et al., 2012), focus only on the prenatal period (e.g., Minozzi et al., 2013; Smith et al., 2009), or omit studies that contain child outcomes in the absence of parent-level outcomes (e.g., Neger & Prinz, 2015). Others focus on alcohol misuse and do not capture equivalent interventions for populations with illicit drug misuse issues (e.g., Cuijpers, 2005; Lui et al., 2008; Smith et al., 2009; Stade et al., 2009; Templeton et al., 2010).
However, the most important limitation is that the existing review literature does not permit valid conclusions to be made about the comparative impact of these interventions for children with substance misusing parents. Understanding the relative impact of different interventions for a particular population is helpful for informing the decision-making of both practitioners and policymakers (Hutton et al., 2015; Mavridis et al., 2015; Salanti, 2012). A relatively recent methodological development – network meta-analysis – provides an avenue for addressing this important question. Network meta-analysis (NMA), also known as multiple treatments meta-analysis, has been referred to as ‘the next generation evidence synthesis tool’ (Salanti, 2012, p. 80) and extends traditional pairwise meta-analytic techniques. NMA provides an approach for (a) quantitatively synthesising both direct and indirect effects of multiple interventions for a particular population or condition; and (b) ranking interventions according to their effectiveness, even in the absence of trials that have directly compared the treatments (Salanti, 2012; Mavridis et al., 2015). This synthesis technique requires a relatively large number of studies and also that the corpus of studies satisfies the underlying analytical statistical assumptions. In the absence of this, traditional pairwise meta-analyses with subgroup analyses are suitable to examine the variation in effectiveness according to predefined factors such as specific intervention components or modalities.
Our review will begin to address the abovementioned methodological quality and content coverage issues. Specifically, this review will both (a) enhance and update the existing body of reviews, and (b) attempt to synthesise the comparative impact of interventions on the psychosocial outcomes of children with substance misusing parents. Importantly, the review will enable policy makers and practitioners to make informed and reliable choices between intervention models.
OBJECTIVES
The overarching objective of this review is twofold. First, we aim to enhance and update existing reviews by comprehensively synthesising the full array of psychosocial, pharmacological, and legal interventions that aim to improve the psychosocial outcomes of children whose parents misuse substances. Second, we aim to use NMA or other quantitative synthesis approaches (e.g., meta-analyses and subgroup analyses) to integrate and examine the comparative impact of these interventions. Specifically, the review will address the following research questions: What is the comparative impact of psychosocial, pharmacological, and legal interventions for improving the psychosocial outcomes of children with substance misusing parents? Does the impact of interventions vary according to the child developmental period (e.g., infancy, early childhood, adolescence) or the type of (a) outcome measure; (b) substance misuse; (c) practitioner implementing the intervention; or (d) intervention setting? Does the impact of interventions vary by the country of implementation?
A secondary objective of the review was to qualitatively synthesise economic, treatment completion, treatment duration, and treatment acceptability data if reported by the authors of included studies.
METHODOLOGY
Criteria for including and excluding studies
Types of study designs
Studies were included in the review if they reported a quantitative impact evaluation of an eligible intervention using eligible participants and outcome measures. The impact evaluation must also have utilised a randomised experimental design or methodologically robust quasi-experimental design with an eligible comparison condition. Eligible comparison conditions were: placebo, no treatment, waitlist control, TAU, and alternative treatment.
Key research synthesists advise against using traditional research design labels when delineating an inclusion threshold for non-randomised studies in a systematic review (e.g., Higgins et al., 2012; Reeves et al., 2011). Rather, the suggestion is that inclusion thresholds should be based on the design features of studies due to (a) the variation and possible ambiguity across disciplines in relation to research design terminology; and (b) the likelihood that risk of bias will affect specific design features versus an overall research design category. For the purposes of this review, methodologically robust quasi-experimental designs were defined as those which permit causal inference by minimising threats to internal validity. For example, maximising treatment and comparison group equivalence through matching (e.g., propensity score matching), measurement of outcomes multiple times pre- and post-intervention to reduce maturation threats (e.g., interrupted time-series, cohort panel designs), or adjusting for confounding factors through statistical modelling (e.g., multiple regression, propensity score modelling). Due to serious threats to internal validity, single group studies with one pre-intervention and one post-intervention outcome measure were excluded from the review.
To be included in the meta-analyses, study authors must have reported sufficient data to calculate an effect size. Where sufficient data is not reported, the required data was sought by contacting the study authors. If the data was not provided by study authors, the study was excluded from meta-analyses, but was coded, assessed for risk of bias, included in the overall summary of studies.
Types of study participants
This review focused on families with children under the age of 18 with one or more currently substance-misusing parents. The primary research participants used in eligible impact evaluations were either substance misusing parent(s), children of substance misusing parents, or entire families characterised by parental substance misuse issues. For the purposes of this review, a parent was defined as an individual who is responsible for providing physical, emotional and/or financial care for a child. Teenage, biological, foster, adoptive, or kinship caregivers were eligible for inclusion. A child was defined as an individual between the ages of 0–18 years who is under the care of at least one parent, and a family was defined as at least one child and one parent.
Parents were classified as ‘currently substance misusing’ if they had been classified as such via standardised diagnostic criteria (e.g., DSM, ICD 10) or a self-report measure (e.g., AUDIT). In the absence of classification supported by diagnostic or self-report measures, studies were included if the authors explicitly labelled the research population as parents who misused substances or were in receipt of treatment for substance dependence (e.g., opioid replacement therapy or in a residential treatment facility for substance misuse). Parents were classified as substance misusing if they misuse alcohol, illicit drugs and/or prescription drugs. If the study sample was not comprised completely of substance misusing parents, we followed Turnbull and Osborn's (2012) approach, whereby the study sample must include at least 50% substance misusing parents to be included in the review.
Types of interventions
This review included all possible psychosocial, pharmacological, or legal interventions that explicitly aimed to improve the psychosocial wellbeing of families characterised by parental substance misuse. Possible categories of interventions were described in the protocol for the review (Eggins et al., 2020). Once all eligible studies had been identified, we used the TIDieR Checklist (Hoffmann et al., 2014) and the specific intervention components described by study authors to create an intervention taxonomy (see ‘Included studies’ section). This taxonomy guided our assessment of the transitivity assumption for network meta-analyses (Hutton et al., 2015). Based on existing literature in the area, we anticipated that the majority of the included studies would utilise a TAU comparison condition (e.g., methadone maintenance, case-management without the intervention under consideration). Interventions were included irrespective of whether it was initiated during the prenatal or postnatal period, however, to meet the participant eligibility criteria, interventions must have continued at least into the neonatal period to be included. In addition, studies were included if the intervention focused on the misuse of alcohol, illicit drugs, and/or prescription drugs.
Types of outcomes
Primary outcomes
To comprehensively synthesise the impact of eligible interventions on children with substance misusing parents, this review included a broad range of outcomes nested under the banner of ‘psychosocial wellbeing’. Outcomes were considered eligible if they were measured using standardised or non-standardised instruments or consisted of official, diagnostic, observation, or self-report data. The final outcome categorisation, including associated measurement methods, is provided in the ‘Included studies’ section. Examples of primary outcomes include, but was not limited to: Child development (e.g., language, cognitive functioning, educational outcomes); Child psychopathology (e.g., externalising/internalising behaviour, mental health diagnoses); Child maltreatment, abuse or neglect; Child antisocial behaviour (e.g., truancy, delinquency, illicit drug use); and/or Other child psychosocial wellbeing outcomes (e.g., self-esteem).
Secondary outcomes
The decision to utilise one intervention over another may rest on other considerations beyond the effectiveness of the intervention, such as intervention cost, resource intensity or degree to which participants accept or complete treatment. Therefore, if reported in eligible studies, the following secondary outcomes were also coded and synthesised: cost-effectiveness, treatment completion, length of time in treatment and acceptability of treatment (e.g., participant perspectives of the intervention).
Duration of follow-up
Studies were included irrespective of the length of follow-up after the intervention. Where the length of follow-up varied across studies, we grouped and synthesised studies according to similar follow-up durations. For example, short (e.g., 0–3 months post intervention), medium (>3 months, <6 months), and long-term follow-up (>6 months post intervention).
Types of settings and other inclusion criteria
There were no restrictions on the intervention setting or treatment format (e.g., inpatient, outpatient, community settings, family home, online or computerised, one-on-one or group settings). The review included intervention studies conducted in any geographical location or country, regardless of publication status. While studies published in any language were captured by the search, only studies written in English were included in the review (see ‘Differences between protocol and review’). A list of possibly eligible studies written in languages other than English are included in the ‘ Studies awaiting classification ’ reference list (Supporting Information: Appendix G).
Search methods for identifying studies
Supporting Information: Appendix B provides the full search record for the systematic search and Table 1 provides the search terms and structure. Wherever possible, this search was replicated across search locations, with some minor modifications to increase the specificity of searches in databases producing unmanageable results (e.g., use of proximity locators and using filters to exclude research using only animal models). Where the functionality of a search location did not permit complex search strategies, a simplified version of the search was utilised. Database functionality permitting, the search string was applied to the title, abstract, keyword and indexing term/subject heading search fields.
Systematic search terms and structure.
The search placed no limits on publication date, document language, or publication status. However, clearly ineligible document types were excluded from search results if the specific search location permitted this refinement (e.g., book reviews). Searches were performed in November 2020 and again in April 2021.
Electronic searches
To reduce disciplinary and publication bias, the systematic search covered multiple disciplines and search sources that captured both published and unpublished literature (see Table 2).
Electronic search locations.
Searching other resources
The following additional search strategies were also employed to identify eligible documents not already captured by the electronic search locations listed in Table 2: Reference harvesting of all eligible studies and previous reviews; Forward citation search/citation tracking for all eligible studies; Hand-searching the two most recent issues before the search date for the following journals to identify potentially eligible documents not yet indexed in academic databases: Addiction Child Abuse and Neglect Child Abuse Review Child and Adolescent Social Work Journal Child Maltreatment Children and Youth Services Review Journal of Drug Issues Journal of Experimental Criminology Substance Abuse
Data collection and analysis
Selection of studies
The first phase of assessing study eligibility entailed screening the titles and abstracts identified by the systematic search. After removing duplicates and clearly ineligible document types (e.g., book reviews), records captured by the systematic search were imported into DistillerSR review management software (Evidence Partners, 2021) for screening. A second check for duplicates was also conducted in DistillerSR and all duplicate references were quarantined. Title and abstracts (records) were then assessed in two stages of screening to accommodate the expertise of staff working on the project. The first stage required trained screeners to assess whether the record was (1) an ineligible document type (e.g., book review); (2) a duplicate; or (3) about human parental substance misusers and/or their children. Before independent screening, each screener was required to screen the same set of 50 titles/abstracts to assess understanding of the screening protocol and eligibility thresholds. The results of this pilot screening task suggested variable rates of false positive decisions, but negligible false negative decisions.
Although all efforts were made to remove ineligible document types and duplicates before screening, automated and manual cleaning can be less than perfect. Therefore, the first two exclusion criteria were used to remove ineligible document types and duplicates before screening each record on substantive content relevance. Records not excluded on any of the above criteria progressed to the second stage of title/abstract screening. The second stage of title/abstract screening required screeners to assess whether the record reported on an eligible intervention for substance misusing parents and/or their children. GoogleTranslate was used to translate and screen titles/abstracts written in languages other than English.
The DistillerSR software includes an artificial intelligence machine learning function whereby records are ranked according to the likelihood of eligibility based on the screening decisions that have been made by human screeners. Records are presented to screeners in order of their likelihood of inclusion to increase the efficiency of the review process, particularly for large reviews. As screening progresses, the software provides an estimate of the percentage of potentially eligible records that have been identified. Ranked title and abstract screening continued until the software estimated that 95% of the potentially eligible studies had been identified. At this point, iterative sets of 50 titles and abstracts (records), ranked in random order of presentation, were screened until a set of 50 records contained no records that were deemed eligible. This stopping criterion was reached after screening 43,104 records at the first stage of title/abstract screening and after screening 22,464 records at the second stage of title/abstract screening. After screening the random samples, DistillerSR continued to indicate that 95% of potentially eligible studies had been identified at the first stage of title/abstracts screening but increased to 98% for the second stage of title/abstract screening. Once reaching this stopping point at each stage of title/abstract screening, the records were deemed as excluded and did not progress further in the review screening process (see Figure 2).
An attempt was made to locate the full-text electronic document for each record retained at the title and abstract screening stage and, if found, was attached within DistillerSR before progressing to full-text eligibility screening. If full-text documents could not be located via existing university resources, they were ordered through the university libraries of the review authors or by contacting study authors. If the full-text document could not be sourced, the title and abstract were screened using the full-text eligibility criteria. For those records that could not be unequivocally excluded, the reference was included in the ‘ Studies awaiting classification ’ reference list (Supporting Information: Appendix G).
Full-text documents were screened for final eligibility according to the following exclusion criteria: Ineligible document type (e.g., book review) Document is not unique Ineligible participants Ineligible outcome measure(s) Not an impact evaluation of an eligible intervention using eligible participants or outcomes Ineligible research design
All efforts were made to remove ineligible document types and duplicates in prior screening stages, these types of records can sometimes progress into later stages, for example, where duplicate records are not adjacent to each other during screening or where screeners cannot unequivocally determine if record is ineligible based on the title and abstract. As such, the first two exclusion criteria were used to remove ineligible document types and duplicates before screening each document for final eligibility on the review inclusion criteria. For full-text documents written in languages other than English, we used GoogleTranslate to first translate the title and abstract (if not already in English) and determine if the document could be included or excluded using the full-text eligibility criteria. For those records that could not be unequivocally excluded using only the title and abstract, we listed the document in the ‘ Studies awaiting classification ’ reference list (Supporting Information: Appendix G). When DistillerSR indicated that 95% of all potentially eligible studies had been identified, iterative sets of 15 documents were screened until a set contained no eligible studies. This stopping point was reached after screening 6844 documents and all remaining documents were considered ineligible. At this point, DistillerSR indicated that 97% of potentially eligible studies had been identified. As an additional quality assurance measure, we utilised the ‘Check for errors’ feature in DistillerSR. The records identified by DistillerSR represented 0.07% of screenings at the first stage of title/abstract screening, 0.11% of screenings at the second stage of title/abstract screening, and 2.64% of screenings at the full-text screening stage (n = 235 in total). All were correct exclusions aside from a single incorrect exclusion, which was a secondary report of an existing study.
Data extraction and management
Eligible studies progressing from the full-text screening stage were independently coded by a single author (EE) using the coding protocol reported in Eggins et al. (2020), provided in Supporting Information: Appendix A. Although the review protocol specified that all studies would be independently double-coded, the number of identified studies rendered this approach unfeasible. However, effect size data was extracted from each eligible study independently by two review authors (EE, JB) and there was agreement in 245 of the 346 effect sizes (70.81%). Disagreements were resolved by discussion among review authors and re-examining the study full-text reports.
For risk of bias, 77.14% of the 35 RCTs used for effect estimates were independently double-coded (k = 27) by two authors (EE, JB, NCH, BT) and the remaining were independently coded by one author (EE). Of the double-coded RCTs, there was agreement in the overall risk of bias rating for 23 studies (85.19%). Close to 70% of the 33 quasi-experiments used for effect estimates were independently double-coded (k = 23) and the remaining were independently coded by one author (EE). Of the double-coded quasi-experiments, there was agreement in the overall risk of bias rating in 15 studies (65.22%). Disagreements in the overall rating and individual domains for each risk of bias instrument were resolved by discussion among review authors and re-examining the study full-text reports.
Broadly, studies were coded according to the following domains: General study characteristics (e.g., document type, study location) Participants (e.g., sample characteristics by condition) Intervention (e.g., intervention components, intensity, setting) Outcomes (e.g., conceptualisation, mode of measurement, time-points) Research methodology (e.g., design, unit and type of assignment) Effect size data Risk of bias
Assessment of risk of bias in included studies
Risk of bias for RCTs was assessed using the Cochrane randomised risk of bias tool (ROB 2; Sterne et al., 2019). Studies were rated across the following five domains as having ‘low’, ‘some concerns’, or ‘high’ risk of bias: (1) bias arising from the randomisation process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias due to measurement of the outcome; and (5) bias in the selection of the reported result. In line with the guidance for ROB 2, studies that did not contribute effect sizes to quantitative syntheses were not assessed (Cochrane Collaboration, 2021). Results of the risk of bias assessment for RCTs are presented in summary tables and in a risk of bias summary figure (see ‘Risk of bias in included studies’ section), generated using the Microsoft Excel macro-enable tool openly available via the Cochrane Collaboration.
For non-randomised quasi-experimental studies, we originally planned to use the Cochrane risk of bias tool for non-randomised studies (ROBINS-I; Sterne et al., 2016). However, due to the varied nature of the included quasi-experimental studies, this tool was not consistently appropriate across all included studies. To provide one cohesive assessment of bias across all included non-randomised studies, we utilised the Effective Public Health Practice Project (EPHPP) tool (Thomas et al., 2004). This tool is informed by the Cochrane Collaboration and other methodological scholars (Juni et al., 1999) and provides a ‘weak’, ‘moderate’, or ‘strong’ rating across six risk of bias dimensions: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection methods, and (6) withdrawals and drop-outs. A global rating of the study can also be given, whereby no ‘weak’ ratings allows a study to be rated as ‘Strong’ overall, one ‘weak’ rating allows a study to be rated as ‘Moderate’ overall, and two or more ‘weak’ ratings allows for a study to be rated as ‘Weak’ overall. To align the risk of bias assessment with the RCTs, we did not assess risk of bias for studies that did not contribute to quantitative syntheses of effect estimates.
In the protocol we specified a plan – data permitting – to examine the impact of risk of bias on effect estimates using sensitivity or subgroup analyses (Eggins et al., 2020). We specified that the approach taken to incorporate risk of bias in statistical analyses was dependent on the degree of variation in risk of bias across included studies. Because the risk of bias assessment (see ‘Risk of bias in the included studies’ section) found an overall high level of bias across all included studies, we did not conduct sensitivity analyses based on risk of bias.
Measures of treatment effect
For continuous outcomes, Hedges' g (standardised mean differences, SMDs) and 95% confidence intervals were computed in RevMan web (The Cochrane Collaboration), using post-intervention or follow-up means and standard deviations. If means and standard deviations were not reported, we extracted all available data and attempted to calculate effect sizes using David B Wilson's effect size calculators.
In the review protocol, we specified an approach for using baseline adjusted means in the calculation of SMDs. We did not adopt this approach due to the variation across studies in terms of including baseline assessments of outcomes and intervention durations. Higgins et al. (2019) advise against combining SMDs using post-intervention and SMDs using change scores due to the differences in what the standard deviation reflects, particularly if there is variation in the length of time between baseline and post-intervention measures (as was the case with the studies included in our review). We acknowledge that there are methods for combining baseline adjusted effect sizes and post-only effect sizes and these will be used in future updates of the review.For dichotomous outcomes, odds ratios and 95% confidence intervals were computed in RevMan web (The Cochrane Collaboration) using the number of occurrences of the event (e.g., OOHC) and group sample sizes. If this data was missing from study reports, we followed the same procedure outlined in the ‘Dealing with missing data’ section below. The protocol specified that if we encountered a mixture of SMDs and ORs for the one meta-analysis that we would select the most common effect size amongst the studies to be synthesised so that the smallest number of effect sizes would require conversion. This issue was not encountered, but we will follow this approach in future updates of the review.
To ensure that the direction of the effects accurately represented and consistent in syntheses, we recorded the meaning of high or low scores for each outcome measure. For continuous outcomes where an increase in scores represented a detrimental outcome (e.g., poorer development), we multiplied the mean by −1.00 so that SMDs above zero represent an effect in favour of the intervention and SMDs less than zero represent an effect in favour of the comparison condition. For categorical outcomes, we adjusted the forest plot labels to reflect whether the direction of the effect was in favour of the treatment or comparison condition. For studies not included in meta-analyses and presented as single effect sizes, we only report the direction of the effect if the confidence intervals included zero for SMDs or 1 for ORs.
Unit of analysis issues
A plan for dealing with two unit of analysis issues was specified in the review protocol (Eggins et al., 2020). The first related to the synthesis of outcomes if studies reported more than one measurement time-point. We dealt with this issue by grouping outcome measurements into three categories: (1) post-intervention measurements <3-months after treatment completion; (2) short follow-up (subsequent measure after post-intervention within 3-months of intervention completion); (3) medium follow-up (>3 months, <6 months); and (3) long-term follow-up (>6 months post intervention). We then calculated and report effect estimates by these outcome time-points. Additional time-points were added as identified among included studies and are clearly reported in the Results section.
The second unit of analysis issue related to studies that contained clustering, such as assignment to conditions by study site or multiple cohorts of participants within conditions. To deal with this issue, we planned to adjust the standard error of the effect size using the method suggested by Fu et al. (2013) and Higgins et al. (2011). If the included study did not report the required intra-class correlation (ICC) coefficient, we had planned to use the approach taken by Barlow et al. (2016) to assess the impact of clustering on effect estimates. Specifically, in their systematic review of group-based parenting, Barlow et al. (2016) conducted sensitivity analyses to examine whether the results of their meta-analyses varied with ICCs of 0, 0.03, 0.02, and 0.1. Over half of the 100 included studies had probable or confirmed clustering (k = 54), such as clustering of multiple children within families, multiple recruitment and treatment sites, and multiple treatment cohorts within the treatment condition. None of the studies randomised participants by cluster, none reported ICC, and very little detail was reported on the exact size of the clusters to enable precise adjustments to effect size calculations. For this reason, we did not implement the methods related to clustering.
Two additional unit of analysis issues were identified during the review process. The first related to eight studies that included multiple treatment groups (Bartle-Haring et al., 2018; Dawe et al., 2007; Kelley & Fals-Stewart, 2002; Lam et al., 2008; Maguin, 1991; Quittan, 2004; Pirnia et al., 2017; Porges et al., 2018). To deal with this issue we followed the recommendations by Higgins, Li, and Deeks (2019) by selecting an approach that ‘avoids arbitrary omission of relevant groups and double-counting of participants’ (p. 148), such as combining treatment groups or separating comparisons into different analyses. Due to the differences in the treatments, it was not appropriate to combine treatment arms into a single intervention condition. Therefore, we selected the treatment that was most aligned with the review inclusion criteria and/or other studies included in the review, and we selected the comparison condition that was most aligned with the comparison conditions across a group of studies to be synthesised. However, for most studies, we also report supplementary effect estimates for treatment versus treatment, and the second treatment versus comparison. Table 3 provides a summary of how each study with multiple treatment groups was handled in the review.
Approach for handling studies with multiple treatment groups.
Abbreviation: TAU, treatment-as-usual.
A second unit-of-analysis issue identified related to a single study that reported data from multiple treatment cohorts/groups separately. Davis-Susser (1990) implemented the same child-focused group therapy programme with three small groups (n = 30 total) and compared them to a single comparison group (n = 10). To calculate effect sizes for this study, the three treatment groups were combined to create one mean and standard deviation using the formulae suggested by Higgins et al. (2021, section 6.5.2.10).
Criteria for determination of independent findings
There are two main areas of consideration for determining independence of study findings: multiple reports of the same study and multiple outcomes for the one study. To identify dependent studies, the final corpus of included studies was first examined for common authors and then common intervention names. Each potential secondary report was carefully examined to ensure that the dates and study methodology were equivalent. Additional verification of dependency was provided when studies had a trial registry that was cited in the report or where study authors referred to secondary reports of the study. Once dependency was identified, all studies were electronically linked in the DistillerSR software and all study reports were consulted for coding, data extraction, and risk of bias assessments. Each study was included only once in each meta-analysis. The protocol for the review specified the approach for combining conceptually similar outcomes from the same study, however, this issue was not identified. Future updates of the review will use the approach outlined in the protocol (Eggins et al., 2020).
Dealing with missing data
If no effect size could be calculated using the data reported by study authors, the corresponding author of the study was contacted to seek the required data. In the case that data could not be provided, the study was included in the study summaries, but excluded from the risk of bias assessment and any meta-analyses or effect estimates.
Assessment of heterogeneity
The review protocol outlined the approach for assessing heterogeneity for NMA. Because NMA was not possible, we assessed the heterogeneity in effect sizes using the approach described by Higgins et al. (2019) for standard pairwise meta-analysis. Heterogeneity was first assessed by examining the direction of the effects and the overlap of 95% confidence intervals for studies included in a meta-analysis. A statistically significant χ 2 test was interpreted as the presence of heterogeneity, but a nonsignificant χ 2 test was not necessarily interpreted as a lack of heterogeneity given the low power of this test when there are few studies or small sample sizes in a meta-analysis (Higgins et al., 2019). In addition, I 2 and τ 2 were used to quantify the extent that heterogeneity contributed to effect estimates. The rules of thumb provided by Higgins et al. (2019) were used to describe the extent of heterogeneity, whilst also being cautious about the certainty of these thresholds if there are a small number of studies included in the meta-analysis and direction and size of the individual effects. Specifically, an I 2 between 0% and 40% suggests a level of heterogeneity that might be important; a value between 30% and 60% may suggest moderate heterogeneity; a value of 50%–90% may suggest substantial heterogeneity; and a value of 75%–100% suggests considerable heterogeneity.
Assessment of reporting biases
The systematic search for this review was comprehensive by encompassing over 100 search locations and multiple supplementary search strategies to identify unpublished research. However, even this comprehensive search strategy does not ensure that all unpublished or unindexed research will be captured (i.e., the file drawer problem) or that all eligible results are included in syntheses (e.g., missing data, or non-reporting bias). Page et al. (2019) propose a framework for assessing reporting bias that includes an assessment of ‘known unknowns’ and ‘unknown unknowns’. The former relates to known potential biases in the review results due to missing effect size data and the latter relates to potential biases in the review results because eligible unreported studies are not identified or included. To assess the ‘known unknowns’ issue, we clearly report eligible studies with missing data for each synthesis. To assess the ‘unknown unknowns’ issue, we had planned to inspect funnel plots for asymmetry for syntheses with 10 or more studies (see Eggins et al., 2020). Because none of the syntheses included this number of studies, we did not carry out this analysis.
Data synthesis (primary outcomes)
NMA requires a sufficient number of effect sizes that compare (a) eligible treatments and comparison groups; and (b) eligible treatments with other eligible treatments (Wilson et al., 2016). These direct effect estimates (see Figure 1) can then be used to estimate indirect effects (i.e., compare interventions that have not been directly compared in existing evaluation studies). Reliable estimates of indirect effects requires meeting the transitivity assumption which is evaluated by assessing the consistency between direct and indirect evidence in a network. However, both direct and indirect evidence is only available when there are closed loops in a network. Within these closed loops, it is also important that studies are sufficiently similar so that effect estimates are not biased. For example, variations in the study populations or type of outcome measurements can undermine the transitivity assumption. In absence of closed loops or probable inconsistency, traditional pairwise meta-analyses with subgroup analyses can produce similar results (Wilson et al., 2016).
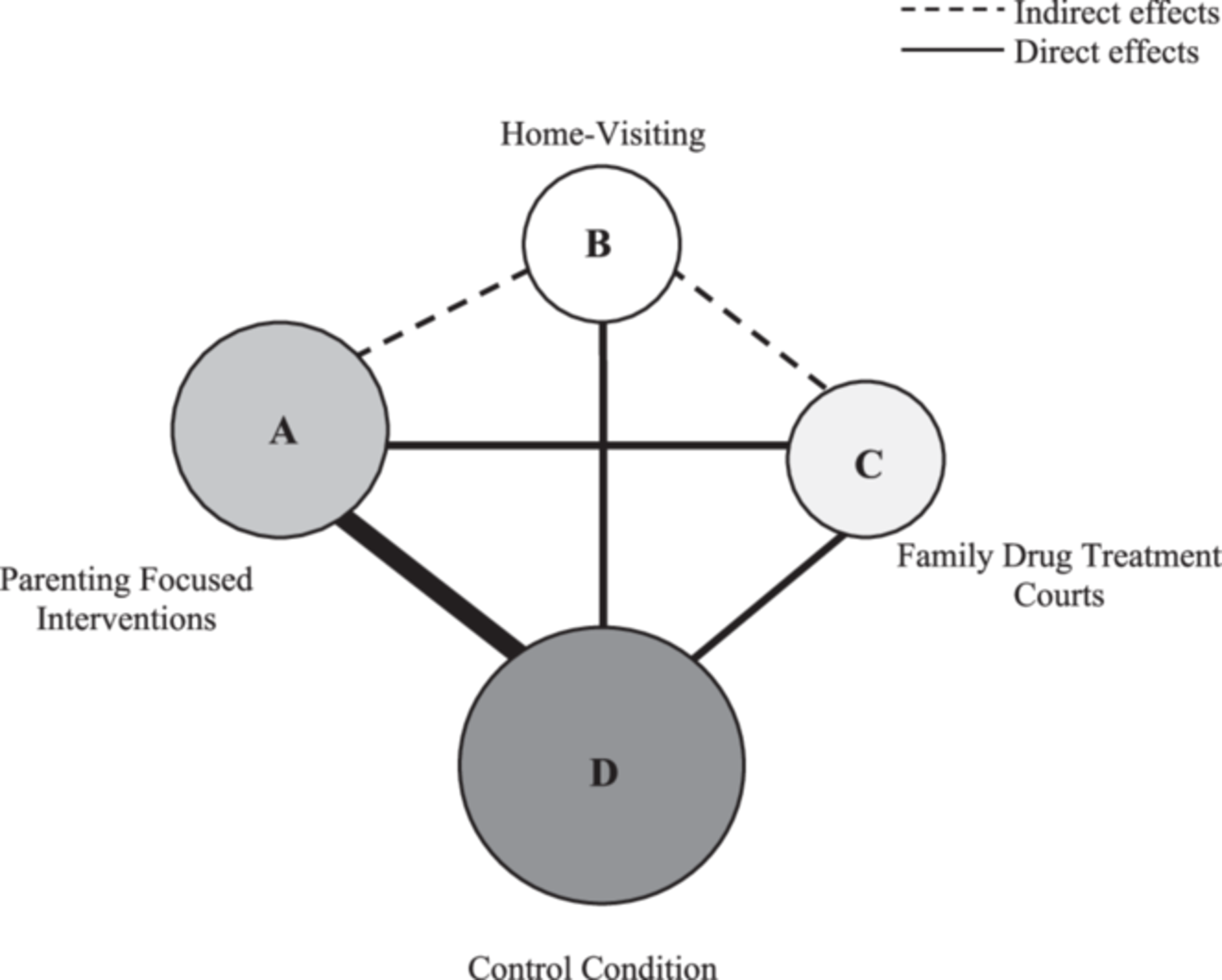
Hypothetical network geometry.
To assess whether NMA was a suitable synthesis approach, we first grouped all included studies according to conceptually similar outcome measures and measurement time-points. Four overarching outcome domains were identified, each of which had multiple sub-categories: child welfare, emotional and/or behavioural, developmental, and educational. These outcome domains and their sub-categories are outlined in Table 4.
Identified outcome domains and measurement methods.
Represents the number of studies per category regardless of measurement time-point or respondent. Studies in each synthesis are group by respondent and measurement time-point, so will contain a smaller number of studies.
Indicates measure is standardised with associated psychometric studies, norms, and/or clinical cut-offs.
Next, we closely examined the nature of the included studies and developed network geometries to ascertain whether the assumptions of NMA had been met. Supporting Information: Appendix C presents the network geometry for all outcome categories that included more than five studies with sufficient data to calculate effect sizes. Five outcome categories included five or more studies with sufficient data to calculate effect sizes: (1) child abuse potential (post-intervention); (2) cognition (post-intervention); (3) parent-reported total problem behaviours (post-intervention and short-term follow-up); (4) parent-reported child externalising behaviours; and (5) retaining parental care (post-intervention).
To construct the network diagrams, we classified each included study into an intervention and comparison category. It is important to note that participants in many of the included studies received both TAU and the intervention under consideration. Moreover, TAU in some studies could be considered an alternative treatment whereby participants in some studies received a clearly specified intervention that was labelled ‘treatment-as-usual’, such as methadone or engagement with an unenhanced ‘generic’ FTDC. Therefore, when developing the network diagrams, the full treatment received by both the intervention and comparison conditions were coded on the presence or absence of nine intervention components (see Table 5 below). The intervention and comparison arms within each study were then classified into mutually exclusive nodes representing the nature of the treatment approach. These nodes were then joined by lines if they had been directly compared in one or more studies. In other words, the nodes represent competing interventions and/or comparisons and the lines connecting the nodes reflect direct comparisons between nodes (Chaimani et al., 2013; Mavridis et al., 2015). The weight of the lines in the network diagrams represent the number of studies with the respective comparison and the size of the nodes reflect the number of participants included in the node.
Categories for Intervention Components.
Of the six networks constructed, four contained a single closed loop but these were based on single studies with very small sample sizes. In addition, effect modifiers were unevenly distributed across nodes (e.g., population, treatment intensity, outcome measurement) which undermines the transitivity assumption. Therefore, we concluded that traditional pairwise meta-analysis, with subgroup analysis (data permitting) was the most appropriate synthesis technique (Wilson et al., 2016). The results of the random-effects inverse variance meta-analyses are displayed in forest plots that include the mean effect size and corresponding 95% confidence intervals.
We developed an analysis plan informed by the nature of the included interventions, comparison conditions, type of outcome, and timing of outcome measurement. We used RevMan web to conduct meta-analyses where there were at least two independent studies that were sufficiently similar across these factors. First, we sorted studies into outcome categories, as summarised in Table 4, and their time-point of measurement after intervention completion. Second, we closely examined the nature of the interventions within each outcome category, using the framework provided in Table 5 to code and classify studies into cohesive categories (see ‘Included studies, Interventions’ section and Table 6 for additional detail). Where we judged that the interventions were conceptually and practically similar, we synthesised the studies with meta-analysis. For example, pharmacological studies with no psychosocial intervention components were not synthesised with studies evaluating integrated intervention models comprised of multiple psychosocial components with or without legal and/or pharmacological components. Finally, we were cognisant that the comparison conditions across the studies was variable, whereby what some authors termed TAU, other authors labelled a similar approach as an attentional control or alternative intervention. To determine the appropriateness of combining studies in a treatment–comparison meta-analysis and/or separately in a treatment–treatment meta-analysis, we examined the nature of the comparison conditions in a grouping of studies, ignoring the labels applied by study authors. If the comparison conditions were sufficiently similar, we combined them in a treatment–comparison pairwise meta-analysis. If studies clearly utilised an alternative treatment, these studies were synthesised separately with either single effect sizes or with meta-analysis if there were two more studies with sufficiently similar comparators. We acknowledge that this analysis approach does not permit direct comparisons between psychological, pharmacological, and legal interventions, which was a key objective for our review. Nevertheless, because many studies integrated psychological, pharmacological, and legal components, our analysis approach permits at least some conclusions to be made about the relative effectiveness of these interventions more generally.
Intervention categories for included studies (k = 99).
Data synthesis (qualitative and implementation-related outcomes)
If studies included based on primary outcomes also included supplementary data and analyses costs/benefits, treatment completion, treatment duration, and/or acceptability, we qualitatively synthesised this information, drawing only on studies that were included in quantitative estimates of effects. Multiple methods have been proposed for qualitative syntheses, but the development of explicit guidelines has been a long-term difficulty in the field (Booth et al., 2018; Noyes et al., 2019), complicated by the lack of thorough evaluation of mixed-method review approaches (Dixon-Woods et al., 2005, 2006; Popay et al., 2006; Pope et al., 2007). The ability to label the qualitative synthesis approach we chose for this review is also complicated by the variability in terminology and methodological overlap within available synthesis models (Booth et al., 2016; Pope et al., 2007).
We adopted Framework Synthesis (see Booth et al., 2016) to synthesise our secondary outcomes. This approach encompasses similar methods such as aggregate synthesis, content analysis, and framework analysis (see Booth et al., 2016; Booth & Carroll, 2015; Dixon-Woods et al., 2005, 2006; Dixon-Woods, 2011; Noyes et al., 2019; Popay et al., 2006). These approaches use systematic frameworks or rules to assemble data into distinct categories that are then synthesised using an assortment of methods, including tables, matrices, and/or text-based narrative summaries (e.g., see Belur et al., 2017; Petrosino et al., 2012). We extracted all data pertaining to costs/benefits, treatment completion, treatment duration, and treatment acceptability from eligible studies, which we then categorise and synthesise in tabular and textual formats. Specific subsections aligning to each category of secondary outcome are then used to provide an overview of the data in the tables (e.g., data collection approach, intervention, number of participants, findings).
Subgroup analysis and investigation of heterogeneity
The review protocol outlined the planned approach for conducting subgroup analyses and investigating heterogeneity. Due to the low number of studies across all syntheses, subgroup analyses were considered inappropriate due to the high likelihood of them being statistically underpowered (Deeks et al., 2019; Pigott, 2020). We acknowledge that it is possible to directly test for subgroup differences even with a small number of studies but decided to indirectly explore heterogeneity using sensitivity analyses due to the nature and number of potential effect modifiers. The following section outlines the approach we took for exploring heterogeneity via sensitive analyses. Future updates of the review will directly test for subgroup analyses, as specified in the protocol (Eggins et al., 2020).
Sensitivity analysis
If moderate to high levels of heterogeneity were detected, we examined the studies included in the meta-analysis for possible sources of heterogeneity. First, we coded all studies on the a priori specified moderator variables: child age, intervention setting, practitioners implementing the intervention, type of parental substance misuse, and type of outcome measurement. We then examined if any of the included studies was an outlier on these effect moderators. If so, we conducted sensitivity analyses to examine if the precision of the meta-analysis changed with the removal of the study. If the studies fell into mutually exclusive categories according to the a priori moderators, we divided studies according to these categories and conducted separate analyses. For both approaches, we report the original analysis and the results of the sensitivity analyses and/or separated analyses.
If the above approaches did not identify potential sources of heterogeneity or the studies did not differ according to the a priori moderators, we then examined other features of the studies that could isolate outliers or signal that the studies needed to be divided into separate analyses. Characteristics of studies that were considered included: research design (e.g., RCT vs. quasi-experiment), study population (e.g., mothers vs. both mothers and fathers), duration and intensity of the intervention, format of the intervention (e.g., group vs. individual), and specific intervention components (see Table 5). We then followed the same analytic approach as outlined above for the a priori moderators.
Treatment of qualitative research
Solely qualitative research was not synthesised in this review. However, where qualitative data was collected from participants regarding acceptability of the intervention, this is noted when synthesising secondary outcomes reported in the included studies.
RESULTS
Results of the search
The entire search identified 149,475 records, of which 92,788 were duplicates or written in languages other than English. The grey literature search captured 8345 records which were screened outside of reference management software. Of these records, 232 were deemed potentially eligible and were manually added to DistillerSR for eligibility screening. An additional 2106 records were harvested from the reference lists of included studies and the list of documents in Supporting Information: Appendix G, and from forward citation searching all included studies in Google Scholar. Figure 2 provides an overview of the screening stages, the number of exclusions, and the reasons for exclusions. The title, abstract, and citation details of all unique results captured by the systematic search of databases were imported into DistillerSR for screening. This resulted in 56,455 records that were processed in DistillerSR.
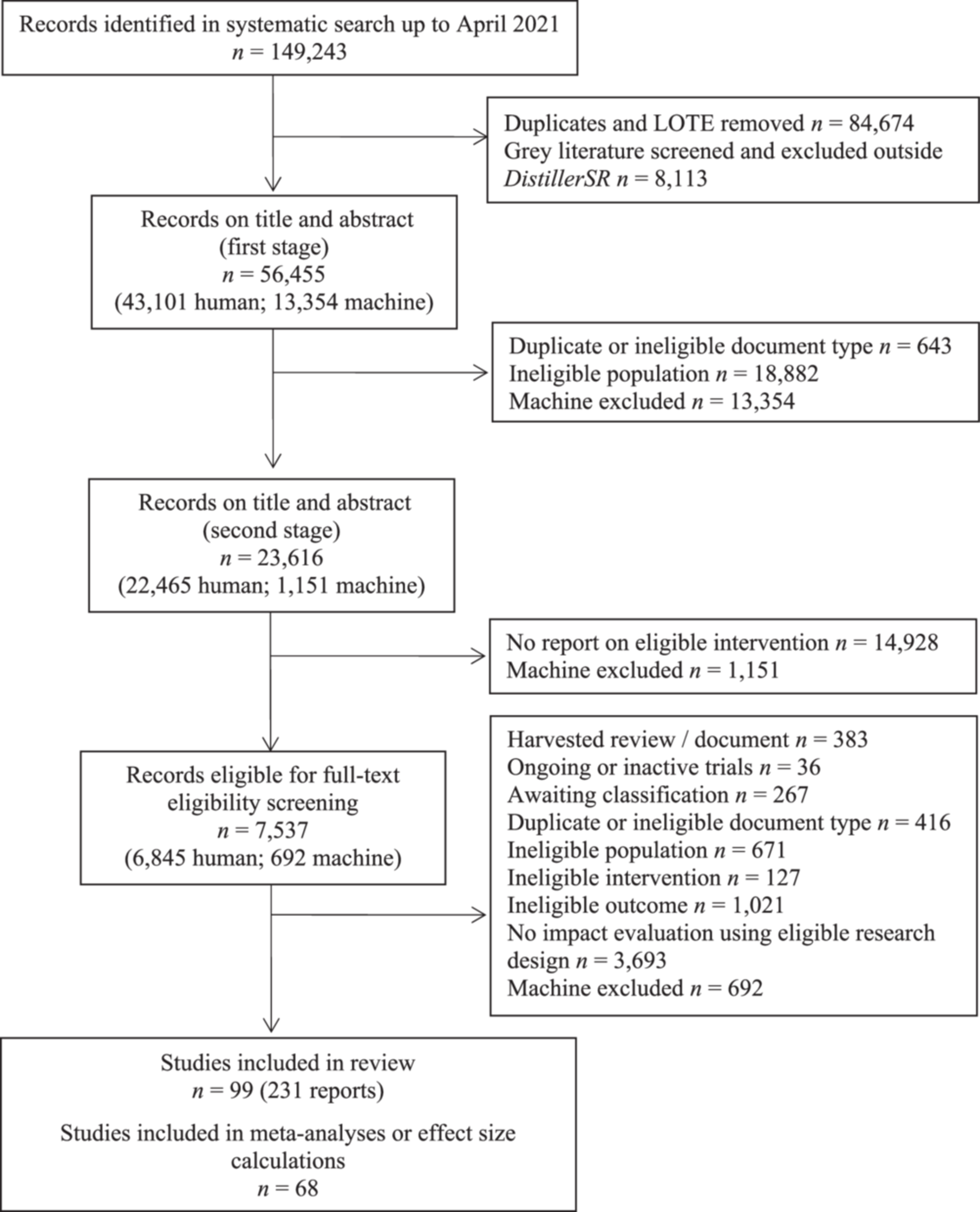
PRISMA flow diagram.
We manually screened 43,101 records at the first stage of title and abstract screening before reaching the stopping threshold specified in the ‘Selection of studies’ section. The remaining 13,354 records were classified as exclusions. Of the 23,616 records progressing to the second stage of title and abstract screening, we manually screened 22,465 records before reaching the stopping threshold specified in the ‘Selection of studies’ section. The remaining 1151 were classified as exclusions.
A total of 7537 records progressed to the full-text screening stage. Of these, 36 were potentially eligible ongoing or inactive trials (e.g., protocols or trial registers) and 383 were relevant reviews or summary documents that were harvested.
At the time of resubmitting after methods and peer-review, four of these trials were completed and will be included in the update planned for 2025.
Included studies
The 99 included studies (reported in 231 documents) encompassed a wide range of document types, including peer-reviewed journal articles (n = 153; 66.23%), conference presentations (n = 28; 12.12%), dissertations (n = 20; 8.66%), trial protocols or registries (n = 5; 2.16%), and book chapters, technical reports, or evidence summaries (n = 25; 10.82%). The following subsections summarise the nature of the included studies according to geographical location, funding source, research design, sample size and sociodemographic characteristics, intervention characteristics, and measured outcomes. Further details about the nature of the interventions are provided in the ‘Characteristics of included studies’ tables in Supporting Information: Appendix D.
Geographical location and funding
The vast majority of studies were conducted in the United States (k = 76), with the remaining studies distributed across the Iran (k = 5), United Kingdom (k = 4), Germany (k = 3), Australia (k = 3), Canada (k = 3), Spain (k = 2), Brazil (k = 1), India (k = 1), and South Korea (k = 1). Most studies reported receiving funding support (76%), usually from government departments (k = 51), philanthropic, corporate or community organisations (k = 15), or a mixture of both (k = 9).
Research designs
Close to half of the included 99 studies were RCTs (k = 46), and the remainder were matched (k = 22) and unmatched control group designs (k = 31). Most studies utilised a single treatment condition compared to a TAU comparison condition (k = 47), with studies varying greatly in the degree of detail about the exact nature of TAU. Three studies used waitlist control groups, but specified that participants received TAU in the interim, with six studies reporting use of a waitlist control without further specification. Ten studies specified a no treatment control group or a control group with no further specification. Six studies randomised participants to one of three treatment conditions and five studies allocated participants to either one of two treatment conditions or a TAU, waitlist control, or a control condition not otherwise specified. Twenty-seven studies utilised clearly specified alternative treatments, with some studies classifying these as attentional control conditions (e.g., Broning et al., 2019; Mitrani et al., 2010).
Recruitment, eligibility, and sample size
Studies varied substantially in the level of detail provided about recruitment processes, eligibility criteria, attrition, and sociodemographic characteristics of their sample. Most studies (k = 89) recruited participants in the post-partum period with direct intervention participants ranging from children only (k = 20); parents only (k = 13); or a combination of children, parents, and/or the entire family unit (k = 66).
The 99 studies included approximately 22,213 participants, excluding one outlier comprising 350,604 cases from a large-scale study of child welfare related legislation in the context of parental substance misuse across 50 American states between 2005 and 2017 (Sanmartin et al., 2020). To calculate this total number of participants, the number of participants at the first outcome measurement time-point was used, as this was the most consistently reported across all studies. Assigned total sample sizes ranged from 9 (Larson, 1989) to 4022 (Boles et al., 2007), with the one outlier study comprised of 350,604 cases (Sanmartin et al., 2020). For studies that clearly reported attrition from the point of assignment or start of treatment to posttreatment outcome measurement (78%), attrition for total samples were distributed across the following categories: 0% attrition (k = 44); ≤10% attrition (k = 10), ≤25% attrition (k = 13), and ≥25 but ≤47% attrition (k = 10). It should be noted that most of the studies with 0% attrition were retrospective case control studies using official data, which are arguably less prone to attrition. When attrition was clearly reported by group (77%), it was evenly distributed across treatment and comparison conditions in most cases (58). In 24 studies, there was a difference in attrition between groups of ≥5%, with (a) the attrition being larger in the treatment versus comparison group for 12 studies; and (b) the attrition being larger in the comparison versus treatment group for 10 studies. Of the 46 RCTs, 69.57% (k = 32) included a CONSORT flow diagram or clear descriptions of attrition and associated reasons from the point of assessment for eligibility to follow-up outcome measurements.
The recruitment process varied in terms of method and level of detail provided. Five of the 99 studies reported no clear recruitment process or source of study referral and a further 13 studies reported their referral source, but not the process of recruitment or assessment for study eligibility. Twenty-five studies retrospectively reviewed cases to form treatment and comparison groups and so did not describe physical recruitment processes. The remaining studies recruited participants following a positive drug/alcohol toxicology result (k = 1); researcher invitation at treatment sites (k = 6); information sessions or advertisements (k = 5); referral by practitioners in the community or health care settings, or upon enrolment for substance misuse treatment (k = 31); or a mixture of these approaches (k = 18). Specific referral sources included schools (k = 9); judges or criminal justice practitioners (k = 6); community-based social services (k = 10); practitioners at medical or substance misuse treatment facilities (k = 25); child welfare practitioners (k = 8); or a mixture of these sources (k = 14).
Sixteen of the 99 studies did not report eligibility criteria for study participation. For the remaining 83 studies, the number and nature of eligibility criteria varied. Most studies required that parents have either verified substance misuse or a specific substance use disorder (k = 70). Over a quarter of the included studies explicitly focused on mothers (k = 28), with 8 studies focusing recruitment on fathers, with 6 of these including supplementary recruitment of spouses or co-parents. Twenty-eight studies had child welfare related eligibility criteria, such as the child residing in OOHC, an open child welfare investigation, high-risk for entry into the child protection system, or specifically no child welfare involvement. Thirty-one studies also reported eligibility criteria that required at least one child resided with the participating parent or that there was frequent contact or a plan for reunification in place.
Close to half of the 99 included studies (k = 41) specified eligibility criteria related to child age, with 3 studies including any children under 16-years of age; 2 studies only including children <5 or 6 years-of-age; 3 studies specifying inclusion of children only <3 years; and 5 studies including infants at birth or <6-months of age. The remaining studies specified age ranges, which spanned from age 2 up to 16, with an average of 6.8 years covered by the age range included in the study.
A quarter of the included studies (k = 25) specified eligibility criteria pertaining to children's birth, health, and development, including: gestation at birth (i.e., number of weeks in utero), absence of major developmental disorders or health condition, or positive toxicology screening results. Twenty studies also specified eligibility criteria pertaining to the participating parent, including: absence of cognitive impairment, active psychosis, or other unstable mental or medical illness. Other less common eligibility criteria included absence of specific offences or types of abuse (e.g., child sexual abuse, active family violence), no current or past participation in similar interventions, specific participant written and spoken language (e.g., German, English), and geographical area restrictions (e.g., health districts or hospitals).
Parent and family-level sociodemographics
Ten of the 99 included studies reported no parent or family-level data aside from parental substance misuse, and 14 studies reported very limited parent or family-level data. Studies also varied in whether they reported parent sociodemographics by condition, for the overall sample, or both. Although not all studies explicitly excluded fathers, the vast majority of studies with at least partial parent sociodemographic data (k = 73) included mothers only or samples predominantly comprised of mothers (k = 53). Eleven studies included either fathers only or heterosexual couples as the parent participants. Mean parent age ranged from 18.1 to 45.3 years. Of the 48 studies that reported parent ethnicity, most reported white or Caucasian as the largest proportion of study participants (k = 33; 67.35%), with 14 studies reporting African American, American Indian, German, or Hispanic ethnicities as the largest proportion of study participants and a single study reporting an even distribution of ethnicities.
A third of the 99 included studies (k = 33) did not report the specific type of parental substance use. For studies that did report substance use (k = 67), 12 focused exclusively on alcohol misuse, 28 reported exclusively drug misuse (41.79%), and 25 reported both drug and alcohol misuse. Ten studies indicated that a proportion of parents within the sample were using some form of opioid maintenance therapy (often in addition to using other substances) or specified that included participants were enroled in opioid maintenance therapy. A total of 54 studies explicitly measured and/or reported parental substance misuse at baseline using one or more of the following measures: Structured interviews in standardised diagnostic format or developed for gathering a comprehensive drug history (k = 11); collateral or official data from medical records or child welfare (k = 16); toxicology screening (k = 2); Addiction Severity Index (k = 7); Timeline Follow Back (k = 3); other standardised measures such as the Severity Dependence Index, Drug Use Disorders Identification Test or Substance Abuse Subtle Screening Inventory (k = 4), or a mixture of modes (k = 17). Of the 45 studies that did not explicitly measure or report parental substance misuse at baseline, substance use was verified by one or more of the following: authors describing the sample as substance misusers (k = 2); official data from medical records or child welfare (k = 15); practitioner referral for substance misuse or current participation in treatment for substance misuse (k = 6); child-report of parental substance misuse (k = 5); or reported as meeting specific diagnostic criteria or level of use (k = 1). Fifteen of the 45 studies substantiated substance misuse using two or more of the aforementioned modes, with 8 of these studies also including parent self-report of problematic substance use (k = 6) and/or positive toxicology (k = 3).
Twenty-eight of the 99 included studies reported the number of children per family, and the average ranged from 1.67 to 4, with 2 studies reporting over half of the participants having >3 children. Thirty-seven studies reported marital status or family structure, and among these studies, the largest category was single-parent families or parents who reported being single, never married, or separated/divorced (k = 24).
Twenty of the 99 included studies reported data on parental comorbidities, comprised mostly of mental health diagnoses, symptomology, or use of psychopharmacology (k = 15). A smaller number of studies also reported data on adverse childhood experiences (e.g., child abuse; k = 4) or medical illnesses (e.g., HIV; k = 5). Twenty-one studies reported current or previous involvement with the child welfare system, with a further 20 studies that did not report child welfare data as part of the sample description, but where the parent or family were drawn or referred from child welfare.
Child sociodemographics
Seventy-three of the 99 studies reported child sociodemographic data beyond only age. Seventy-two studies reported mean child ages or proportions by child age. Based on the mean age or the largest proportional age category, the studies fell into the following categories: (a) <12-months (k = 19); (b) ≤3 years (k = 5); (c) ≥3 but ≤5 years (k = 8); (e) >5 but ≤10 years (k = 18); >10 years (k = 17); and (f) child ages spanning multiple categories, but under the age of 18 as the upper limit (k = 7). Other types of sociodemographic data reported for children included gender, ethnicity, birth information, and/or comorbid diagnoses. However, this information was only sporadically reported across the included studies and so full detail is provided only in the ‘Characteristics of included studies’ tables in Supporting Information: Appendix D.
Outcomes
Eligible outcomes were measured shortly after treatment completion (post-intervention) without a baseline measure for 24 of the 99 included studies, and with a baseline measure for 40 studies. Fifteen studies measured their first post-intervention outcome measure more than 3-months after treatment completion, and another 19 studies did not clearly specify the timing of the outcome post-intervention completion or used time-to-event designs whereby the post-intervention period varied by participants. Twenty-eight studies included at least one follow-up outcome measure after the initial post-intervention measure, and these ranged from 3-months to 10-years. Nineteen of these studies included a single follow-up time-point after the immediate post-intervention measure, 6 studies included 2 follow-ups, and 3 studies included 3 follow-ups.
As can be seen in Table 4 above, a wide variety of outcome measures were captured by the included studies. The number of conceptually distinct outcomes per study ranged from 1 (k = 27) to 25 (k = 1), with most studies (k = 62) reporting between 2 and 6 outcomes. The greatest number of studies reported an outcome falling into the child welfare domain which included standardised measures of child abuse potential and official child welfare data (k = 55). The next largest outcome category was emotional/behavioural (k = 50), followed by developmental (k = 22), and then educational (k = 10). In terms of mode of measurement, 12 studies utilised direct standardised neurodevelopmental or psychological assessment tools and 53 studies utilised self-report instruments that were either standardised or developed for the purposes of the research (either parent, child, or teacher-report format). A total of 43 studies reported at least one outcome comprised of official data (e.g., child welfare data).
Overall, there was a substantial amount of missing data across the 99 included studies. Missing data ranged from complete omission of results – aside from a statement of non-significance – to missing statistical data required to calculate effect sizes (e.g., standard deviations or equivalent). Of the 99 included studies only 68 reported data sufficient to calculate effect sizes for at least one outcome. Across these 68 studies, there was also variability in the completeness of data reported by different outcomes domains, whereby 12 studies with more than one eligible outcome did not report sufficient data to calculate effect sizes for all eligible outcomes. Attempts have been made to contact all study authors for missing data, and the most complete data as of December 2023 is reported here. Of studies with data missing for at least one eligible outcome (k = 43), the number of outcomes ranged from 1 to 15, with an unclear number of missing eligible outcomes in some studies because of the low level of detail provided for methods and results (e.g., generic reference to concepts measured and/or only single items from standardised questionnaires reported in results). Of these 43 studies with any missing data, 18 studies had missing data for a child welfare outcome, 7 studies had missing data for a child developmental outcome, 19 studies had missing data for a child behavioural or emotional outcome, and 7 studies had missing data for an educational outcome. The specific nature and extent of missing data is reported by outcome category in the ‘Effects of interventions’ section below.
Interventions
The included studies encompassed a variety of intervention models, that were most cohesively categorised by focus of the intervention and/or each of its components. In relation to the objectives of the review, 94 of the 99 included studies included an intervention component that was psychosocial in nature, 29 studies included a pharmacological intervention component, and 29 studies included a regulatory or legalistic intervention component. Almost a quarter of the 99 included studies (k = 22) integrated psychosocial and pharmacological intervention components, 26 studies integrated psychosocial and legal/regulatory components, and two studies integrated psychosocial, pharmacological, and legal/regulatory components (Hall et al., 2015a; Hall et al., 2021). No studies integrated only pharmacological and legal/regulatory components. Based on coding for the presence or absence of the intervention components detailed in Table 5, just over two-thirds of the 99 included studies (k = 67 studies) evaluated interventions that integrated two or more intervention components that were either psychosocial, pharmacological, and/or legal in nature.
Over half of the 99 included studies included an explicit substance misuse treatment component for parents (k = 58), with therapeutic approaches (k = 49) more common than pharmacological approaches (k = 25). Thirty-five studies included a parent-focused therapeutic component, with individual therapy not explicitly focused on substance misuse being the most common (k = 31), followed by couples or relationship focused therapeutic components (k = 16). Notably, 16 studies included treatment strategies focused on emotion regulation and/or mindfulness. Over half of the 99 included studies (k = 52) included a parenting component, with 41 studies including a parent-skills component and 28 studies including a component with a greater focus on the parent-child relationship and/or attachment. In terms of child-level focus, 35 studies included an intervention component focused on child health and/or development and a fewer number of studies (k = 29) included direct therapeutic intervention strategies for children. Half of the studies (k = 49 described case-management, advocacy, usual health services (e.g., prenatal and early childhood) as part of the intervention model. Finally, 29 studies described legalistic or child welfare related components as part of the intervention model (e.g., FTDC, mandated toxicology tests, ongoing safety planning).
To cohesively synthesise the intervention models, we used the coding of each study according to the intervention components described above and in Table 5 to compile an overall intervention categorisation provided in Table 6 below. Further details about the nature of the interventions are provided in the ‘Characteristics of included studies’ tables in Supporting Information: Appendix D. To construct Table 6, interventions were first broadly categorised according to the presence or absence of a substance misuse treatment component for parents, with 58 studies including an explicit substance misuse treatment component. Two common intervention components across the included studies were the integration of: (1) case-management, advocacy, usual health services (e.g., prenatal and early childhood), provision of practical support or referrals to other services; and/or (2) child welfare services or legal components. Therefore, studies were further categorised according to whether they integrated one or both of these approaches. Finally, studies were then categorised and grouped according to the presence of an intervention component focused on (1) therapeutic support for parents without a focus on substance use (e.g., mental health, couple relationships); (2) parenting skills or the parent-child relationship; (3) direct therapeutic or developmental support for children; and/or (4) therapeutic support for the entire family unit.
The largest category was child-focused interventions with (k = 7) and without (k = 20) parental substance misuse, and with or without case-management, legal, or child welfare components. Interventions in this category tended to be group-based interventions for children affected by parental substance misuse and aimed to support children and/or prevent future substance misuse (e.g., Broning et al., 2019; Dore et al., 1999; Hojjat et al., 2015; Roosa et al., 1989; Scheer, 1996). Other interventions in this category were individual therapeutic approaches such as narrative-informed therapy (Haight et al., 2010), music therapy (Porges et al., 2018), and pharmacological treatment for NAS (e.g., Bada et al., 2015; Flannery et al., 2020).
The next largest category was interventions that integrated parental substance misuse treatment with multiple treatment components focused on parent wellbeing, parenting, child psychological wellbeing, health and/or development, and overall family functioning (k = 21). Example interventions in this category include the Parents Under Pressure programme (Barlow et al., 2019; Dawe et al., 2007), the Strengthening Families programme (Brook et al., 2012; Johnson-Motoyama et al., 2013), the Focus on Families programme (Catalano et al., 1999), enhanced Family Behaviour Therapy (Donohue et al., 2014), and therapeutic communities that allow children to reside with parents and receive direct support or intervention (Stevens et al., 1998).
Another prominent category was interventions that integrated parental substance misuse treatment with parent-focused therapeutic components either for other issues (e.g., mental health) or parenting (k = 9). Examples of this type of approach included individual substance-focused therapy paired with couples therapy and/or parent skills training (Kelley & Fals-Stewart, 2002; Lam et al., 2008), group-based parent-skills training integrated with outpatient individual substance misuse services (e.g., counselling, monitoring; Cantania, 1985), mindfulness-informed individual therapy focused on substance misuse and parenting (Brown et al., 2021), and formal integration of manualised substance misuse and parent-skills training approaches (e.g., Saldana et al., 2015).
Interventions primarily focused on parental substance misuse, with or without case-management, legal, or child welfare components (k = 7) were also common. Example interventions in this category included: FTDCs without explicit family-focused treatment adjuncts (e.g., Boles et al., 2007; Burrus et al., 2011; Harwin et al., 2013; Worcel et al., 2008); coordination between child welfare professionals and substance misuse treatment providers (e.g., Hall et al., 2015, 2021). The remaining studies fell into smaller categories and examined at least one child, parent, and/or overall family focused intervention component with (k = 8) and without an integration of an explicit substance misuse treatment component (k = 25). Two studies did not report an explicit substance misuse treatment component for parents, and focused on a state-level legislation (Sanmartin et al., 2020) or integrated regulatory components with comprehensive case management (Ryan et al., 2016).
In terms of the timing of the intervention, 1 study included some participants who were pregnant at the point of beginning the intervention but who were due to give birth shortly after enrolment (Barlow et al., 2019), and 10 studies began the intervention prenatally and continued into the post-partum period. For the remaining 88 studies, the intervention was conducted either in the post-partum period or at some point before the child was 18 years of age. Interventions were most commonly delivered in a group format to parents or children (k = 22) or using a combination of formats, including: individual, group, couple, parent-child dyad, and overall family unit (k = 22). Nineteen studies delivered the intervention individually to a parent or child. The remaining studies either did not clearly report the intervention delivery format for all components of reported intervention (k = 20), delivered the intervention to either couples or adult family members (k = 2), or to individual families only (k = 14).
Intervention settings varied across the included studies, with 13 studies not clearly specifying an intervention setting at all. The greatest number of interventions were set in clinics, residential treatment facilities, or hospital settings (k = 33), followed by the family home (k = 15). Seventeen studies included a FTDC component in addition to services in settings outside the court, and the remaining interventions were either set in educational settings (e.g., schools, vocational colleges; k = 10); or a mixture of community, health, or home settings (k = 11).
Intervention duration ranged from less than 1-month up to 4 years, and the studies were distributed across the following categories: (a) <1-month (k = 5); (b) ≥1-month <3-months (k = 21); (b) ≥3-months <6-months (k = 24); (c) ≥6-months <12-months (k = 12); (d) ≥12-months <18-months (k = 13); and (e) ≥18-months or a range between 9 and 18-months (k = 10). Fourteen studies did not clearly specify the intervention duration. Of the studies that reported the number of treatment sessions or contacts (k = 40), these ranged from 6 to 80 in total. The frequency of contact during treatment was most commonly at least on a weekly basis weekly for those studies that reported this information (k = 48). A smaller number provided more frequent contact (e.g., daily, twice-weekly) or contact that titrated down over time (k = 18). Thirty-seven studies provided information on the duration of intervention contacts, but this usually varied by the specific intervention component (e.g., phone contacts vs. home-visits). Overall, duration of contacts ranged between 30 min to 2.25 h.
Eighty-six of the 99 studies provided information about the practitioners who implemented the interventions, although did not consistently report their profession or specific discipline. Of those studies that did, the type of practitioners included: psychologists or counsellors (k = 7); child welfare workers (k = 4); case workers or paraprofessionals (k = 3); social workers or family support workers (k = 5); nurses (k = 3); and teachers (k = 2). The remaining studies reported the use of multidisciplinary teams spanning medical, psychological, legal, child welfare, and/or other allied health disciplines (k = 31).
Excluded studies
Figure 2 highlights that, at full-text stage, most of the 7538 potentially eligible studies were excluded due to there being no evaluation of an eligible intervention using an eligible research design, followed by no report of an eligible outcome(s), use of an ineligible population, and then report of an ineligible intervention. A full list of all excluded studies is provided in the Supporting Information. In this section, we highlight themes in the full-text screening process which led to discussion and/or mediations of particular studies.
Although the review protocol specified attachment as a possible child psychosocial outcome, upon further consideration of the way attachment is measured, we did not include this outcome in the review. Attachment is generally measured in a dyadic manner, rather than a child-level manner, and so we considered attachment (and related parent-child and family functioning outcomes) to be a conceptually distinct category of outcomes than the child-level outcomes included in the review. We acknowledge that attachment, quality of the parent-child relationship, and family functioning are important outcomes linked with child psychosocial wellbeing, but do not consider them direct measures of child psychosocial wellbeing. This led to the exclusion of some studies that readers may anticipate being included in the review (e.g., Belt et al., 2012; Gannon et al., 2017; Hildebrandt et al., 2020; Lussier et al., 2010; Murnan et al., 2018; Porter et al., 2015; Stover, 2015; Suchman et al., 2008, 2010, 2011, 2018).
A number of studies also used samples with a history of substance misuse, used mixed samples including substance misusing parents, but did not report the percentage of the sample who were currently misusing. In the latter case, the intervention was not focused solely on substance misuse, so we could not assume the sample was comprised of parents with current substance misuse. Other studies measured parent substance use at baseline, but did not report sufficient information to determine the proportion of parents who were misusing substances. As such, all of these study types were excluded as we could not unequivocally verify current substance misuse in the proportion of the sample specified in the protocol (i.e., 50%, e.g., Anis et al., 2020; Barlow et al., 2013; Conners-Burrow et al., 2013; DeGarmo et al., 2013; Duggan et al., 2007; Grzegorzewska et al., 2011; Horigian et al., 2015; Santvoort et al., 2014).
Three other design issues also arose during full-text eligibility screening. First, we excluded studies where an evaluation of outcomes was conducted at a time-point when it was unclear if all participants had completed the intervention (e.g., Huebner et al., 2012; Jansson et al., 2007; Schuler et al., 2003; van Wormer et al., 2016). Second, we excluded studies where the comparison condition was comprised wholly or partly comprised of individuals who partially completed the treatment, were treatment refusers, or not currently misusing substances (e.g., Ashford, 2004; Fessinger et al., 2020; Gifford et al., 2016; Lindsey Mowery, 2013). Finally, we excluded studies where separate intervention models were combined into one treatment group to examine the impact on eligible outcomes (e.g., Boles et al., 2012; Grella et al., 2009). Collectively, these design issues were likely to influence effect estimates in an unpredictable way and were not studies that wholly fit our inclusion criteria.
Risk of bias in included studies
Randomised studies
The summary of the risk of bias assessments for randomised trials is provided in Supporting Information: Appendix E. The summary figure indicates that of the 35 RCTs that were included in effect estimates, no study was rated at low risk of bias overall, 8.57% were rated as having some concerns, and 91.43% were rated as having high overall risk of bias. The overall risk of bias rating uses the lowest rating across the 5 domains, meaning that if a study receives a rating of high risk for one of the 5 domains, the overall risk for that study will be rated as high.
The randomisation process domain assesses whether the study used an appropriate allocation sequence and concealed allocation sequence. Only one study was rated as high risk for this domain, due to using an alternating sequence (Ernst et al., 1999). Most studies (k = 20; 57.14%) were rated as having ‘some concerns’ because they did not explicate or conceal the random allocation sequence. The remaining 14 studies were rated as low risk of bias due to using an appropriate allocation sequence (as per the ROB 2 tool) that was definitively or likely concealed.
The deviations from intended intervention domain assesses whether bias has been introduced to the study because, for example, participants received an incorrect or additional intervention or did not receive the intervention as intended in some way (e.g., non-adherence by participants). Ratings on this domain are based on several components, including blinding, deviations due to the trial context, likelihood of the deviations influencing the outcome, balancing of the deviations between treatment and comparison groups, and appropriateness of the analysis to estimate the effect of the intervention (i.e., intention-to-treat or modified-intention-to-treat). It is important to note that almost all studies included in this review could not have blinded participants to the intervention given the participatory nature of the interventions, which would have included an informed consent process describing the different conditions. Lack of blinding is only one component of this risk of bias domain, and it is still possible for studies to obtain a low risk rating without blinding. Regardless, the signalling question related to blinding was not considered in the assignment of a rating for this domain unless the study was purely pharmacological in nature (e.g., Flannery et al., 2020). Eight studies (22.86%) were rated as having high risk of bias deviations from intended intervention either because (a) they reported deviations that were likely to affect the measured outcome or deviations that were not balanced between treatment and comparison groups; and/or (b) or because they used inappropriate analyses to assess the intervention effect (e.g., omitting participants who did not complete the intervention). Most studies (k = 15; 42.86%) were rated as having ‘some concerns’ because (a) there was no information on possible deviations or there were deviations where it was unclear regarding their affect the outcome; and (b) an appropriate analysis approach was specified by study authors (e.g., intent-to-treat). Twelve studies (34.29%) were rated as having low risk of bias on this domain because there was clear descriptions of monitoring fidelity and the results of these observations and the authors used an appropriate analysis approach was specified by study authors (e.g., intent-to-treat).
The missing outcome data domain assesses the degree and type of missing data for a study and whether that missingness introduces bias to the effect estimates. This domain received the largest number of low risk ratings of all 5 risk of bias domains, but also a large number of high risk ratings. The primary reason for the large number of high risk ratings (k = 17; 48.57%) was due to (a) high rates of missing outcome data as a result of participant attrition or no report of participant retention; and (b) inability to determine if the missing data depended on its true value or whether the missing data biased estimates of the effect (e.g., through sensitivity analyses, comparison of retained and lost participants). Nevertheless, 17 studies (48.57%) were rated as having low risk of bias on this domain because ≥95% of participants were retained and provided outcome data for eligible outcomes.
The measurement of the outcome domain assesses whether errors in measurement bias the estimates of treatment effect. Factors taken into consideration for this domain include: appropriateness of the measure for estimating the outcome, differential measurement approach between conditions, the person assessing the outcome and whether they are blind to participant assignment to conditions, and whether assessment of the outcome could be influenced by knowledge of group assignment. Although all studies used appropriate measures of outcomes, the vast majority of studies utilised self-report measures which can be influenced by knowledge of the intervention received, and this lead to downgrading many studies on this domain (k = 25; 71.43%). Five studies (14.29%) were rated as low on this domain because the outcome measure was official data which is arguably less prone to bias due to knowledge of the intervention or because the outcome measure was a standardised direct neurodevelopmental assessment, often administered by blinded assessors. The remaining 5 studies (14.29%) were rated as having either some concerns because they used a mixture of self-report and direct standardised direct neurodevelopmental assessments and/or official data and so the risk of bias varied depending on the outcome under consideration.
The selection of the reported result domain assesses whether bias has been introduced because the reported results have been selected due to direction, size, or statistical significance. This is different from selective non-reporting bias, such as statements of statistical non-significance with no accompanying data, which relates to the assessment of reporting bias. Examples of selective reporting of results include: failure to report data for all time-points, reporting a subset of all outcome measures, reporting particular subscales of a measure, or reporting a subset of data from specific outcome assessors (e.g., official data and omitting self-report data). Bias can also occur in this domain if authors conduct multiple different analyses of the data and do not report all results. A key part of assessing bias for this domain requires locating a priori trial protocols and comparing the protocol to subsequent study reports. Only one study (Barlow et al., 2019) had an accompanying protocol with an a priori analysis plan and so received a rating of low risk for this domain. Most studies (k = 32; 91.43%) were rated as having some concerns for this domain, as there was no unequivocal evidence of selection in the reported result(s). Two studies (5.71%) were rated as having high risk of bias for this domain due to omission of measured outcomes for some time-points, reporting only some subscales of a measure, or variability in results across study reports.
Non-randomised studies
Supporting Information: Appendix E provides a summary of the risk of bias assessments for non-randomised trials. To be consistent with the ratings of randomised trials, we have provided supplementary columns in the summary table to show the overall risk without considerating of the blinding domain and for taking a ‘weakest link’ approach (i.e., overall rating corresponds to the lowest domain rating). Based on an overall rating without consideration of the blinding domain, of the 33 non-randomised trials that were included in effect estimates, 40.42% (k = 14) of studies were rated as Strong (i.e., low risk of bias overall), 30.30% (k = 10) were rated as Moderate (some risk of bias overall), and 24.24% (k = 8) were rated as Weak (high overall risk of bias).
There was a fairly even distribution across the 33 studies between weak (k = 3; 9.09%), moderate (k = 19; 57.58%), and strong (k = 11; 33.33%) for the selection bias domain. Studies with a weak rating tended to utilise self-referral approaches or did not describe participant selection, did not report the number of participants who were referred and consented to the study (overall or between treatment and comparison groups), and/or reported a substantial loss of participants before allocation. Studies with a moderate rating used either random selection of participants or more systematic methods of participant selection (e.g., practitioner referral), but did not report the number of participants who were referred and consented to the study (overall or between treatment and comparison groups), and/or reported <80% or unclear loss of participants before allocation. Studies with a strong rating randomly selected participants from the target population and reported >80% retention of participants between consenting to the study and allocation to treatment and comparison groups.
Studies were mostly rated as moderate (k = 24; 72.73%) for the study design domain as they used observational approaches such a case-control design or a cohort analytic design (as per definitions in the EPHPP tool). Nine studies (24.27%) were rated as strong because the method of allocation to treatment and comparison and was prospectively determined by investigators. Most studies were rated as strong on the confounding domain (k = 23; 69.70%) due to a verified lack of differences between groups on possible confounding factors. Nine studies (27.27%) were rated as weak for the confounding domain because there were clear or unverifiable differences between the treatment and comparison group on either sociodemographics or baseline outcome measures that were not controlled with statistical analyses or research design (e.g., matching). One study was rated as moderate (3.03%) because study authors reported a difference between treatment and comparison participants on a key demographic variable (maternal age), but this was controlled within their statistical models. As to be expected with the type of interventions and topic area, no studies were rated as strong on the blinding domain and most studies (k = 25; 75.76%) received a moderate rating because the nature of the study design removed the possibility that participants were aware of the research question (i.e., retrospective case review using official data). Eight studies (24.24%) were rated as weak because the outcome measures were self-report and the nature of the research design meant that participants and study authors were likely aware of participant group allocation.
Similar to the selection bias domain, there was a relatively even distribution of studies across the weak (k = 9; 27.27%), moderate (k = 13; 39.39%), and strong (k = 11; 33.33%) categories for the data collection domain. Most studies used measures with known validity and reliability, or measures that are likely to be highly accurate (e.g., judicial decisions or official data). Those that were rated as weak tended to provide insufficient detail on the nature of outcome measures to permit assessment of their psychometric qualities. In line with the risk of bias assessment for RCTs, a large number of non-randomised studies were also rated as having risk related to attrition. Almost a quarter of the studies (k = 8; 24.24%) either did not clearly report attrition or reported attrition of >40% of the sample. Those that were rated as moderate on this domain (k = 20; 60.61%) retained 60%–79% of participants or utilised entire cohorts of participants drawn from official data (i.e., retrospective case control designs). To receive a rating of strong on this domain, studies needed to retain at least 80% of participants assigned to conditions, and this standard was reached for 5 (15.15%) included studies.
Effects of interventions
Primary outcomes
Child welfare domain
Fifty-five studies reported at least one outcome related to child welfare. Table 7 below provides a summary of the analyses conducted across all outcomes in the child welfare domain, and the subsections below provide additional detail about the analysis results and included studies. As described above in the ‘Data synthesis’ section, we developed an analysis plan informed by the nature of the included interventions, comparison conditions, type of outcome, and timing of outcome measurement. Meta-analyses were conducted where there were at least two independent studies that were sufficiently similar across these factors.
Child welfare outcome domain analyses and results.
Note: *Type of custody not reported, treated as out-of-home care; ¤Type of out-of-home placement not specified or foster care; §No reference to reunification or permanency.
Child abuse, maltreatment, or neglect
Thirteen studies measured the number of substantiated child abuse incidents, recurrence of child abuse incidents, intervention by child welfare services, open or active child welfare cases, and/or ‘involvement’ with child welfare services without further specification. Five of these studies did not report sufficient data to permit calculation of effect sizes, either due to missing data (e.g., standard deviations, exact n), unclear reporting of the timing of outcome measurements after intervention completion, or because not all participants had completed the intervention at the time official outcome data was collected (Boles et al., 2007; Carey et al., 2010b; Hall et al., 2015a, 2021; Kissick et al., 2015; Pollock & Green, 2015).
Of the studies with sufficient data for effect size calculation (Flannery et al., 2020; Green et al., 2007; Jansson et al., 2007; Lam et al., 2008; Penny & Pratt, 2011; Smirk et al., 2014; Summey et al., 2018), five studies measured active child welfare investigation or involvement, or open child welfare cases after intervention completion compared to TAU (Flannery et al., 2020; Lam et al., 2008; Penny & Pratt, 2011; Smirk et al., 2014; Summey et al., 2018). In terms of intervention models, one study examined the impact of a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training (Lam et al., 2008). The other three studies were predominantly focused on mothers (prenatally and/or postnatally) and children during the neonatal and/or infancy period. Penny and Pratt (2011) examined the impact of a formalised plan of clinical care approach for mothers identified as having substance misuse issues at the time of birth. The intervention was conducted during the first 12-months of the child's life and aimed to improve the coordination and delivery of services across multiple areas, including parent mental health and parenting. Smirk et al. (2014) examined the impact of an outpatient detoxification programme for mothers and babies, which also included alternate day home-visits, psychoeducation, and weekly outpatient assessments by a neonatologist (Smirk et al., 2014). Similarly, Summey et al. (2018) examined the impact of a multidisciplinary comprehensive programme for managing NAS in newborns (‘rooming in’, in and outpatient pharmacology, phone-based parenting support, developmental screening). A meta-analysis of these conceptually similar studies (Figure 3) indicated that the odds of having active child welfare involvement did not differ between families engaged versus not engaged with treatment (n = 611; OR = 0.54, 95% CI 0.10 to 3.01; Figure 3) and there was statistically significant heterogeneity among the effect sizes (τ 2 = 2.02; χ 2 = 21.89, df = 2, p < 0.0001; I 2 = 91%). There was no difference in the odds of child protective services involvement following engagement with a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training versus TAU (OR = 0.58, 95% CI 0.07 to 4.56).
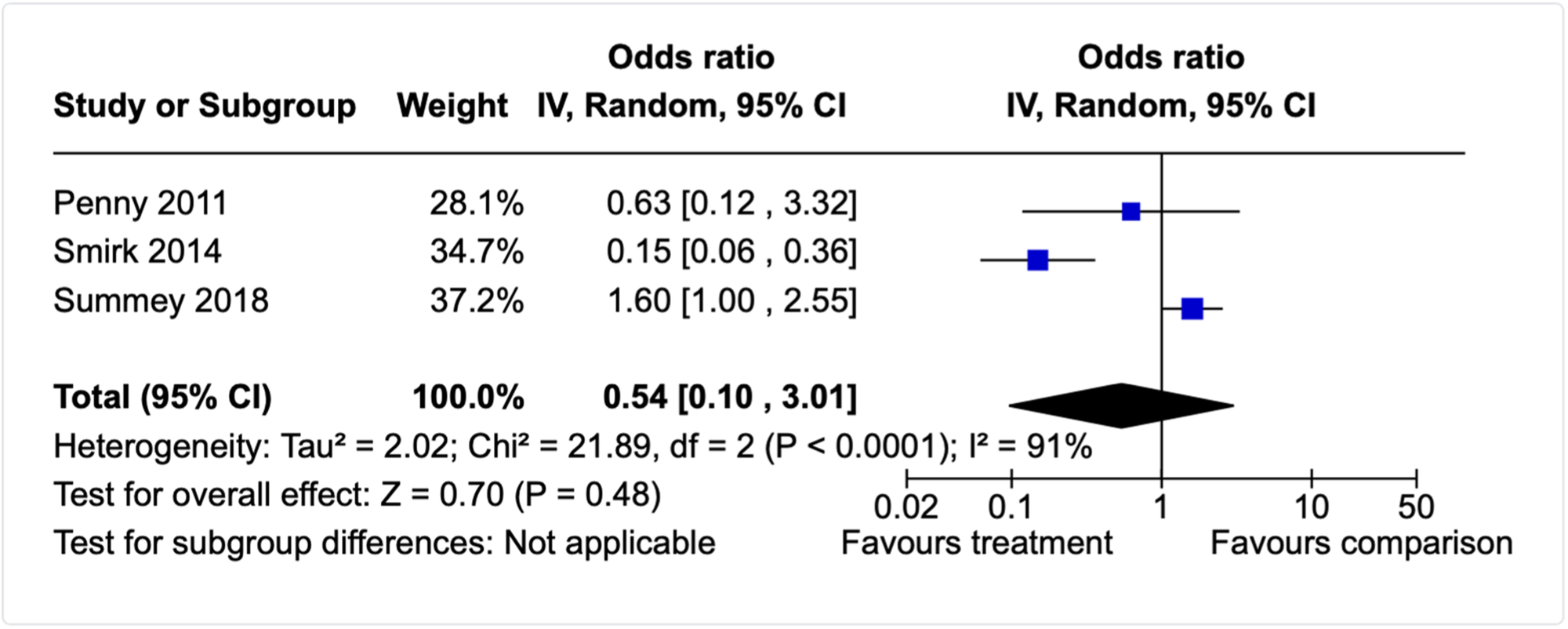
Forest plot for child welfare involvement meta-analysis (post-intervention, infancy focused interventions).
Another single study (Flannery et al., 2020) compared whether the rate of child welfare involvement differed for infants with NAS who were treated with methadone versus morphine more than 12-months after hospital discharge. The odds ratio (OR) for this study suggests there were no differences in likelihood of child welfare involvement between infants treated with methadone or morphine (n = 83; OR = 0.69, 95% CI 0.70 to 4.05).
Lam et al. (2008) also measured active child welfare involvement at 6- and 12-months after treatment completion and single odds ratios similarly indicated that the odds of having active child welfare involvement did not differ between families engaged versus not engaged with treatment (n = 20; 6-months: OR = 0.44, 95% CI 0.03 to 5.88; 12-months: OR = 0.58, 95% CI 0.07 to 4.56). Further, a single study by Green et al. (2007) measured the number of substantiated cases of abuse, maltreatment or neglect approximately 4-years after families completed FTDC programmes across 4 locations in the United States (n = 450). There were greater odds of a substantiated case of abuse, maltreatment, or neglect for families who engaged with a FTDC programme compared to TAU (OR = 1.74, 95% CI 1.06 to 2.85).
This effect was estimated by converting the % of cases with the outcome in the treatment and comparison group reported in the study into counts. Because the authors did not report decimal places, the treatment cases could have been 58 or 57 due to rounding. In addition, the report varied by stating both 14% and 15% of cases within the outcome in the comparison condition. To account for this, we calculated the comparison sample size by 0.145 (i.e., 200 × 0.145 = 29 cases). The OR reported above is for 57 cases in the treatment group, as this was the more conservative effect size (OR with 58 treatment cases: 1.78, 95% CI 1.09 to 2.91).
Child abuse potential
Twelve studies used standardised measures to assess the potential for child abuse either directly after intervention completion and/or at one or more follow-up time-points. Three of these studies (Luthar et al., 2000, 2007; Stover et al., 2019) did not report sufficient data to permit calculation of effect sizes, predominantly due to lack of standard deviations or incomplete reporting of statistical tests to allow alternate effect size calculation. Of the studies with sufficient data for effect size calculation (k = 8), 3 studies examined the examined the effectiveness of interventions without a parental substance misuse component, but at least one intervention component focused on parenting or family-functioning (Barlow et al., 2019; Black et al., 1994; Kim et al., 2019), and the remaining 5 studies integrated a parental substance misuse treatment component with at least one or more treatment components focused on the parent, child, and/or family unit (Brown et al., 2021; Dakof et al., 2010; Dawe et al., 2007; Donohue et al., 2014; Leakey, 2005). Studies could be further differentiated by the type of measure used and child population. Six studies used the validated Child Abuse Potential Inventory (brief or full) and focused on younger children (Barlow et al., 2019; Black et al., 1994; Brown et al., 2021; Dakof et al., 2010; Dawe et al., 2007; Donohue et al., 2014; Saldana et al., 2015), whereas two studies measured abuse potential using the Adult-Adolescent Parenting Inventory (AAPI-2; Kim et al., 2019; Leakey, 2005).
At the post-intervention time-point, child abuse potential, as measured by the Child Abuse Potential Inventory (brief or full), was lower for families with young children engaged with treatment compared to those who were engaged with TAU (n = 259; SMD = 0.36, 95% CI 0.12, 0.61). There was no heterogeneity detected (τ 2 = 0.00; χ 2 = 3.36, df = 4, p = 0.50; I2 = 0%), and we did not conduct subgroup analysis given that there were too few studies and because the distribution of possible effect modifiers was equivalent across the studies included in the meta-analysis. Figure 4 provides a forest plot of the distribution of effect sizes.
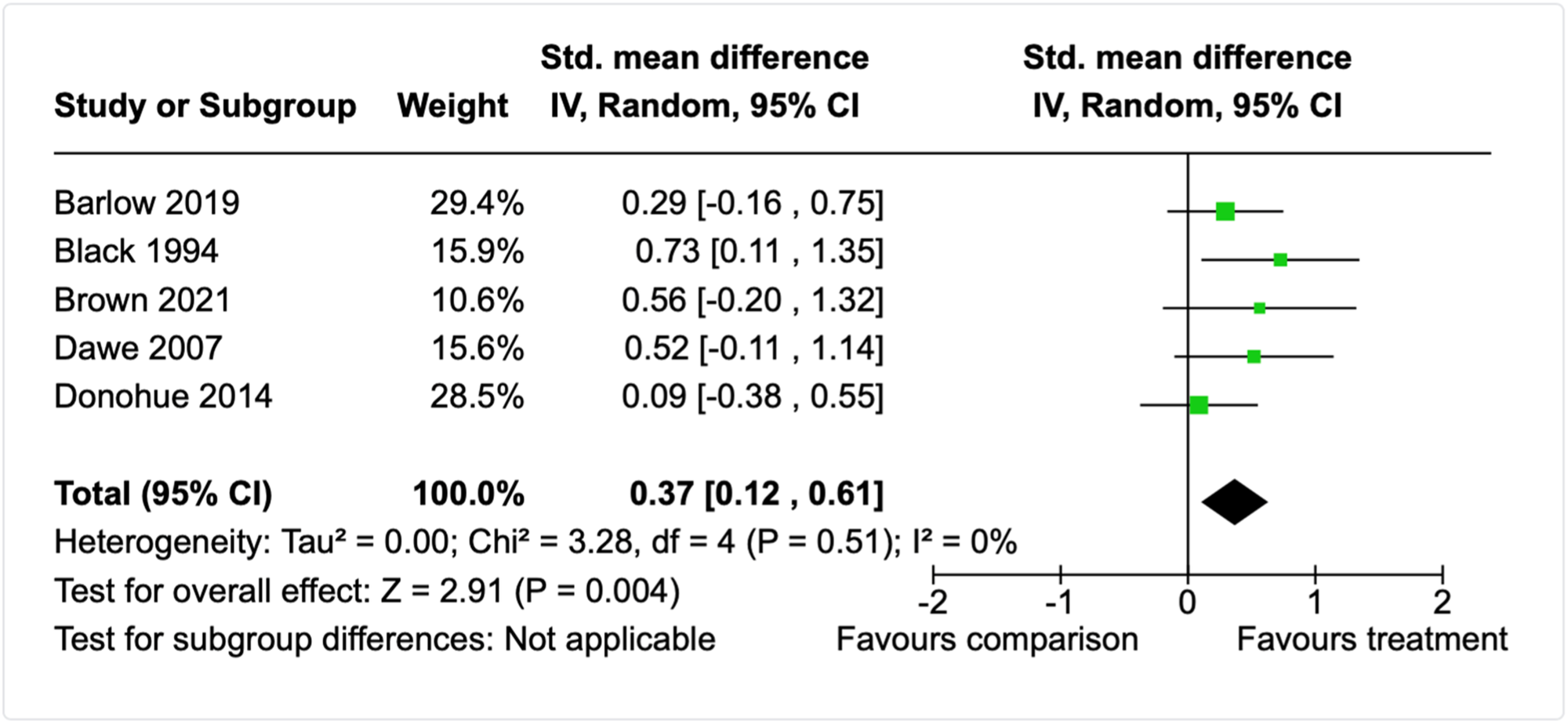
Forest plot for child abuse potential meta-analysis (post-intervention, young children).
At follow-up within 6-months of treatment completion, child abuse potential as measured by the Child Abuse Potential Inventory (brief or full) did not differ between families with young children engaged with treatment compared to those who were engaged with TAU (n = 272; SMD = 0.25, 95% CI −0.07 to 0.57). There was moderate but nonsignificant heterogeneity (τ 2 = 0.06; χ 2 = 6.83, df = 4, p = 0.15; I2 = 41%), yet too few studies to permit subgroup analyses (see Figure 5).
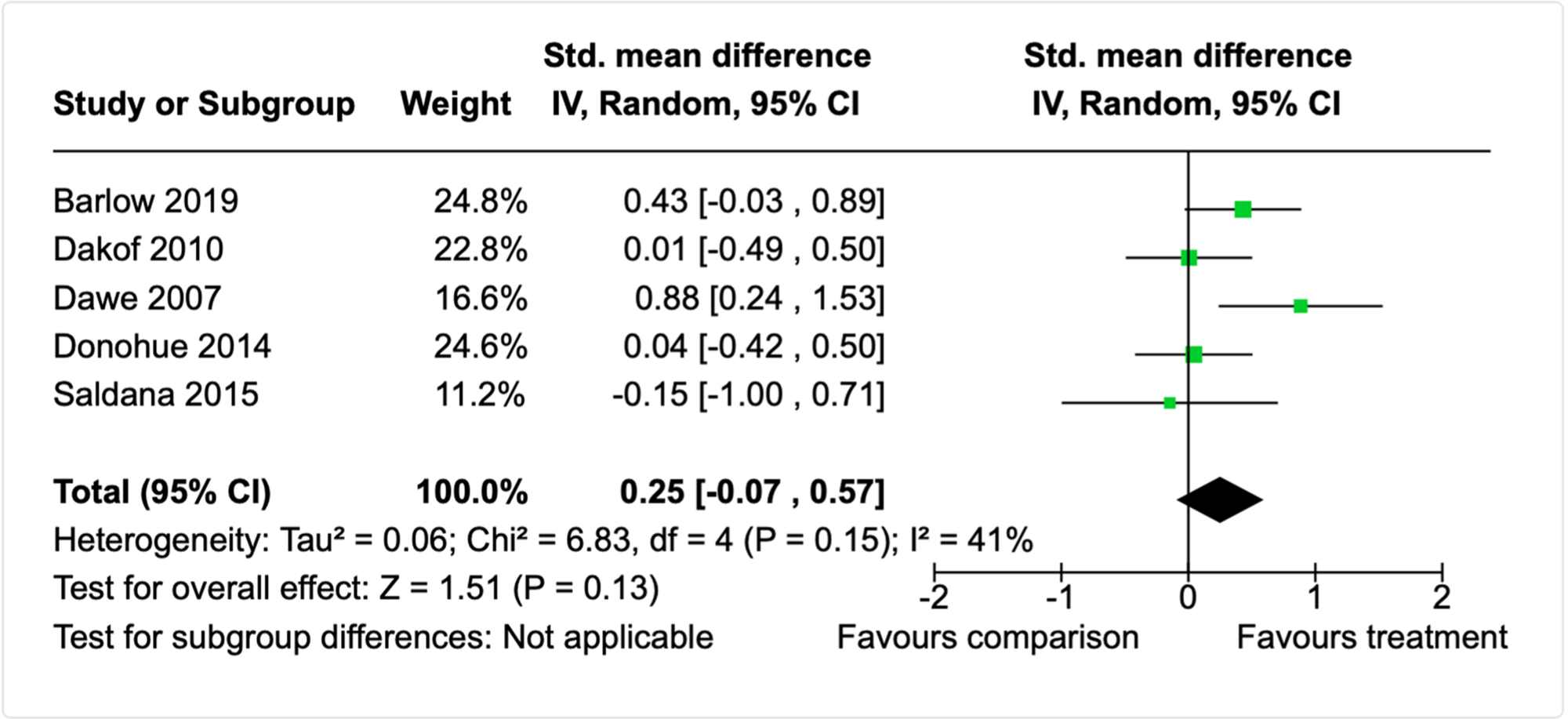
Forest plot for child abuse potential meta-analysis (follow-up, young children).
Examination of the a priori effect modifiers did not uncover any clear categories or outliers among the studies according to: child age, outcome measure, type of substance misuse, intervention setting, or practitioners implementing the intervention. Upon examining other features of the studies that may explain heterogeneity, one study differed from the others due to having a treatment duration of <3-months, compared to the other 4 studies with treatment duration of approximately ≥6-months (Dawe et al., 2007). A sensitivity analysis that removed this study increased the precision of the meta-analysis (SMD = 0.14, 95% CI −0.12 to 0.49) and reduced the heterogeneity (τ 2 = 0.00; χ 2 = 2.43, df = 3, p = 0.49; I2 = 0%). On its own, this study indicated that child abuse potential was lower 6-months following engagement with both methadone outpatient services and a family-focused multicomponent intervention in the home compared to TAU methadone outpatient services (SMD = 0.88, 95% CI 0.24, 1.53). The other 4 studies (Barlow et al., 2019; Brown et al., 2021; Donohue et al., 2014; Leakey, 2005) were otherwise similar to Dawe et al. (2007) in terms of population, point of intervention (post-partum), and an intervention approach that integrated parental substance misuse treatment with one or more treatment components that focused parent wellbeing, child health and development, parenting, and/or overall family-functioning. This result should be interpreted with caution and does not indicate that the particular intervention approach for Dawe et al. (2007) is more effective than the other studies measuring child abuse potential at longer-term follow-up.
Two studies included families with adolescents and measured child abuse potential using a measured focused on risk of adolescent child abuse (AAPI-2), which is distinctly different measure than for younger children (Kim et al., 2019; Leakey, 2005). One study evaluated the effectiveness of a Solutions Focused Behavioural Therapy model on adolescent abuse potential using a sample of substance misusing parents. The intervention was comprised of weekly individual sessions over the course of approximately 3-months. The other study examined the effectiveness of The Nurturing Program, which formed part of a therapeutic community where mothers with substance misuse issues reside with their children. The study specifically compared the effectiveness of the relationally focused programme with or without the integration of ‘nurturing time’, which was an experiential component that provided mother-child dyads the opportunity to practice the relationship building skills emphasised in the programme. In light of the qualitative differences between these two intervention approaches, they were not combined with meta-analysis. Upon completion of the intervention, abuse potential did not differ between parents who participated in the Solutions Focused Behavioural Therapy model compared to TAU on any of the 5 AAPI-2 subscales (see Table 7 above). Likewise, abuse potential did not differ between those who participated in the Nurturing Parenting Program with or without the nurturing time experiential component (see Table 7 above).
OOHC
Twenty-four studies reported a measure related to child OOHC, yet there was a substantial amount of missing data across the studies, with only 13 studies reporting sufficient data to calculate effect sizes (Abrahams et al., 2010; Butz et al., 2001; Donohue et al., 2014; Flannery et al., 2020; Forrester et al., 2008; Hall et al., 2014, 2015b, 2016; Harwin et al., 2013; Hünsler et al., 2013; Lawlor et al., 2020; Schaeffer et al., 2011; Smirk et al., 2014). For most studies with missing data, the main issue was missing standard deviations or n by groups, unclear reporting of the timing of outcome measurements after intervention completion, difficulty verifying if all participants had completed the intervention, or variation in follow-up periods across participants without appropriate time-to-event analyses. In the paragraphs that follow, the studies with missing data are omitted, however, Supporting Information: Appendix F provides a summary of studies with and without missing data by each outcome category.
Two studies (Donohue et al., 2014; Schaeffer et al., 2011) measured the number of days in child protective custody or OOHC. Donohue et al. (2014) examined the effectiveness of a home-based enhanced Family Behaviour Therapy intervention comprised of weekly home-based sessions over the course of 6-months. The mean number of days in child protective custody did not differ between families who participated in the enhanced Family Behaviour Therapy versus TAU at either post-intervention (n = 72; SMD = 0.21, 95% CI −0.21 to 0.67) or at follow-up <6-months later (n = 72; SMD = 0.25, 95% CI −0.22 to 0.71). The second study (Schaeffer et al., 2013) examined the effectiveness of the Building Strong Families intervention, which integrated Multisystemic Therapy for Child Abuse and Neglect (MST-CAN) and Reinforcement Based Therapy (RBT). At follow-up more than 12-months after treatment completion, there were no differences between the intervention and TAU participants in relation to the number of days children spent in OOHC (n = 43; SMD = 0.27, 95% CI −0.34 to 0.88).
Six studies assessed whether receiving treatment impacted the odds of children being in an OOHC placement. Three studies evaluated pharmacological interventions combined with either a rooming-in approach to treat infants with NAS or TAU in neonatal intensive care (Abrahams et al., 2010; Hünsler et al., 2013; Lawlor et al., 2020), one evaluated a FTDC model (Harwin et al., 2013), one evaluated a home-visiting intervention focused on mother and child health and wellbeing from birth until the child reached 18-months of age (Butz et al., 2001), and another examined the impact of an outpatient detoxification programme for mothers and babies, which also included alternate day home-visits, psychoeducation, and weekly outpatient assessments by a neonatologist (Smirk et al., 2014). A meta-analysis of the 6 studies indicated that the odds of a child being in OOHC with a nonrelative was lower for families engaged in treatment versus those engaged with TAU (Figure 6; n = 1607; OR = 0.62, 95% CI 0.41 to 0.93). Non-signficant heterogeneity among the effect sizes was detected (τ 2 = 0.08; χ 2 = 7.90, df = 5, p = 0.16; I2 = 37%).
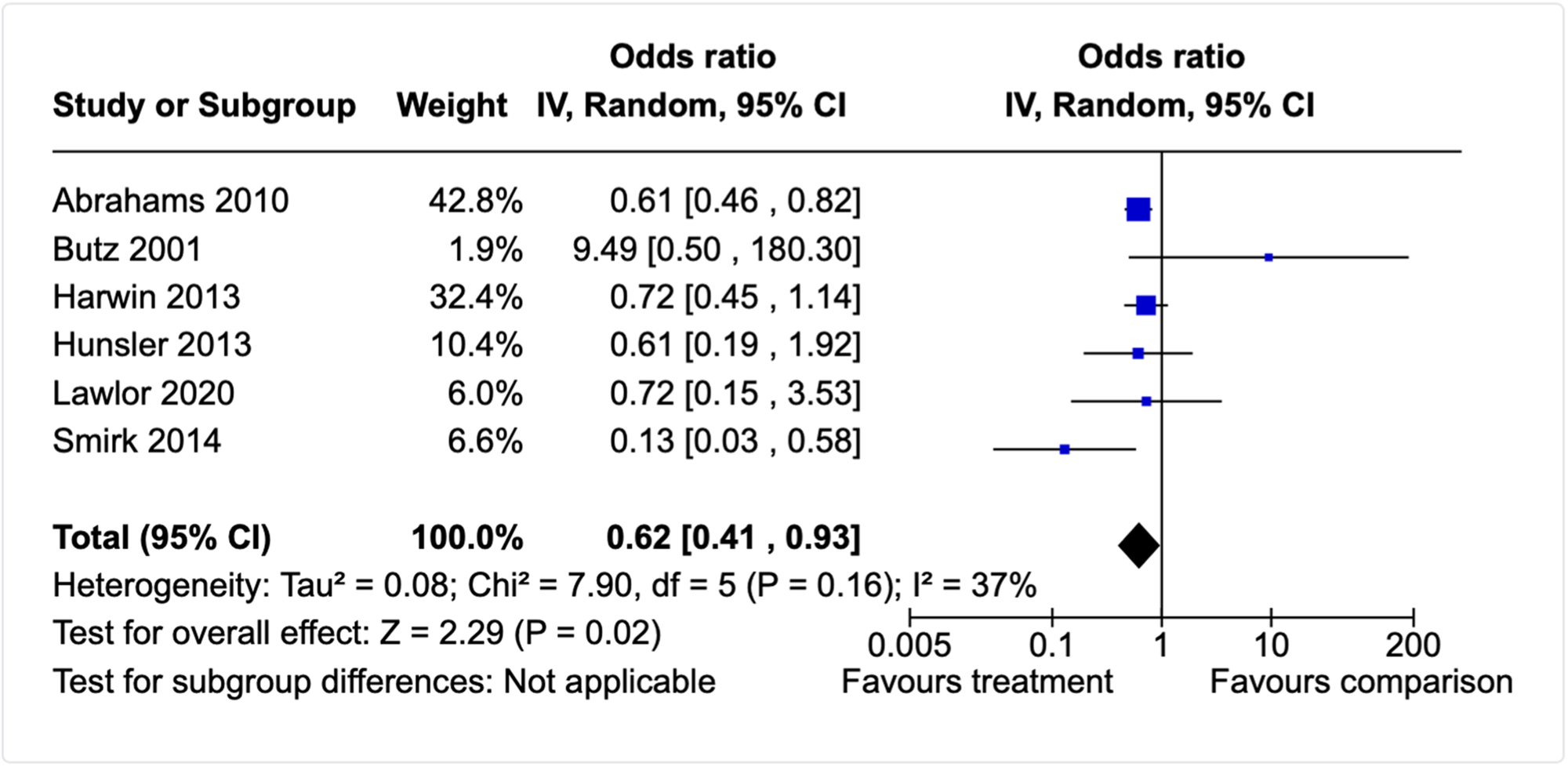
Forest plot for out-of-home care meta-analysis (post-intervention, infants and toddlers).
A single study (Flannery et al., 2020) compared whether the rate of OOHC differed for infants with NAS who were treated with methadone versus morphine more than 12-months after hospital discharge. There were no differences in the odds of OOHC between infants treated with methadone or morphine (n = 83; OR = 0.72, 95% CI 0.24 to 2.14). Similarly, Kelly et al. (2015) found that when mothers and infants participated in supported at-home weaning for treatment of NAS, there was no difference in odds of the infant being apprehended by child protection services (with no further specification of where the child was placed) compared to in-hospital weaning with additional support from a caseworker and public health nurse (n = 80; OR = 0.69, 95% CI 0.26 to 1.79).
Five studies examined the effect of interventions on the likelihood of a child being in the care of family members other than parents. Butz et al. (2001) examined whether a home-visiting intervention with mothers and their infants influenced the likelihood of placement in kinship care at 36-months of age (∼6 to 18-months after end the intervention) compared to TAU. There were no differences in the odds of kinship care for families who engaged with treatment versus TAU (n = 117; OR = 0.76, 95% CI 0.34 to 1.70).
Four studies compared alternate treatments for NAS (Hall et al., 2014, 2015b, 2016; Lawlor et al., 2020). Lawlor and collegues found that the odds of discharge to a family member did not different according to whether infant NAS was treated with a structured care-by-parent protocol involving rooming-in with the infant or TAU (OR = 1.00, 95% CI 0.26 to 3.86). Hall and colleagues found that the odds of discharge to a family member did not differ according to whether NAS was treated with (1) a stringent versus non-stringent weaning protocol (Hall et al., 2014; OR = 0.74, 95% CI 0.45 to 1.22); (b) a structured versus unstructured methadone weaning protocol (Hall et al., 2015; OR = 0.71, 95% CI 0.41 to 1.23); or (3) buprenorphine versus methadone (Hall et al., 2016; OR = 0.64, 95% CI 0.25 to 1.64). These same three studies also found that the odds of discharge to adoption or foster care did not differ according to whether NAS was treated with (1) a stringent versus non-stringent weaning protocol (Hall et al., 2014; OR = 1.13, 95% CI 0.67 to 1.90); (b) a structured versus unstructured methadone weaning protocol (Hall et al., 2015; OR = 0.96, 95% CI 0.55 to 1.69); or (3) buprenorphine versus methadone (Hall et al., 2016; OR = 0.64, 95% CI 0.25 to 1.64).
Two studies examined longer follow-up periods after treatment completion. Schaeffer et al. (2011) examined whether a multisystemic therapy approach (Building Stronger Families) impacted the likelihood of entering OOHC or the number of OOHC placements compared to TAU. Approximately 12–15 months after treatment completion, there were no differences in the likelihood of entering OOHC (n = 43; OR = 0.35, 95% CI 0.07 to 1.73) or the number of OOHC placements between the groups (n = 43; SMD = 0.29, 95% CI −0.32 to 0.90). Similarly, Forrester et al. (2008) examined if an intensive family preservation service (‘Option 2’) impacted whether children entered OOHC during a follow-up period of 3.5 years (range: 8 months–6.5 years, no statistically significant differences between groups on length of follow-up). There were no differences in the likelihood of entering OOHC (n = 368; OR = 0.95, 95% CI 0.59 to 1.54) between the groups.
Parental care
Thirteen studies examined if engagement with treatment impacted whether parents retained care or custody of their children (without specific reference to reunification or permanency). One study combined randomised and non-randomised treatment participants into reported counts for retention of parental care and so no effect size could be calculated (Ernst et al., 1999). Ten studies compared a psychosocial, pharmacological and/or legal intervention to a TAU condition at the post-intervention time-point (Abrahams et al., 2007, 2010; Butz et al., 2001; Forrester et al., 2008; Dakof et al., 2010; Hünseler et al., 2013; Lawlor et al., 2020; Singh et al., 2020; Stevens & Patton, 1998) and three studies compared alternate treatments (Hall et al., 2014, 2015b, 2016). One study compared a long-term therapeutic community with or without child(ren) residing with parents at 6-month post-discharge (Stevens et al., 1998) and another single study (Forrester et al., 2008) compared intensive family preservation service (‘Option 2’) to a TAU condition with a follow-up period of 3.5 years (range: 8 months–6.5 years, no statistically significant differences between groups on length of follow-up).
At post-intervention completion, the odds of parents retaining care of their children was significantly higher for parents engaged in treatment compared to TAU (n = 1702; OR = 1.54, 95% CI 1.14 to 2.09, see Figure 7). There was moderate but nonsignificant heterogeneity (τ 2 = 0.05; χ 2 = 8.72, df = 6, p = 0.19; I2 = 31%), yet too few studies to permit formal subgroup analyses to explore this heterogeneity.
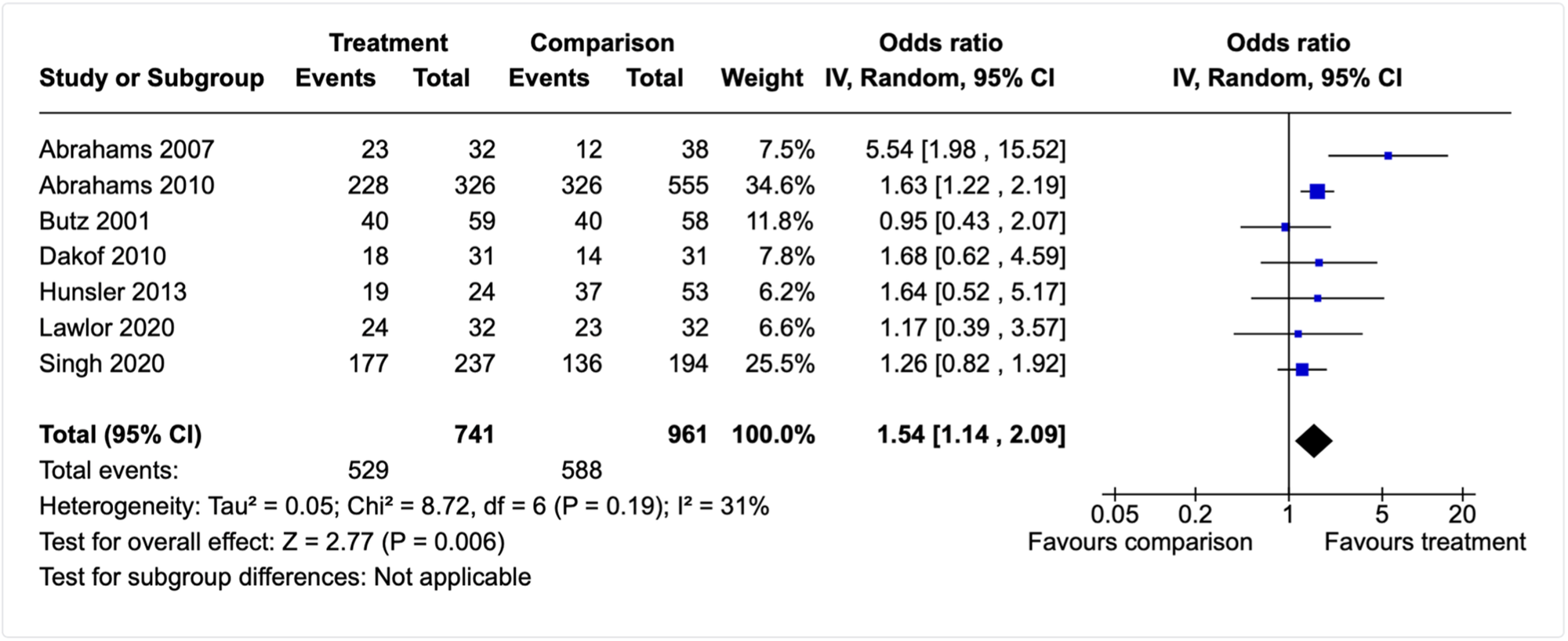
Forest plot for retaining parental care meta-analysis (post-intervention, all ages).
Upon examination of the seven studies, the nature of the interventions, and the a priori moderators specified for subgroup analysis, three main differences were identified across the studies. First, the studies could be divided by whether the intervention was focused in the prenatal/immediate birth or the postpartum period. Second, those focused on the prenatal/immediate birth period were also all conducted in health settings versus the post-partum studies that were set in community, home, and judicial settings. Third, all of the prenatal/immediate birth studies were also quasi-experiments versus the post-partum studies which were all RCTs. In light of this, and the inappropriateness of subgroup analysis, we chose to conduct two separate meta-analyses. The first included studies with interventions focused in the prenatal and immediate birth period and that were implemented in health settings (Abrahams et al., 2007, 2010; Hünsler et al., 2013; Lawlor et al., 2020; Singh et al., 2020). The second included studies where the intervention was focused on the post-partum period and not implemented in health settings (Butz et al., 2001; Dakof et al., 2010).
The odds of parents retaining care of their children were higher for parents who engaged in rooming-in with or without comprehensive prenatal care and/or pharmacological treatment for NAS (if required) compared to parents who engaged with TAU (n = 1523; OR = 1.66, 95% CI 1.14 to 2.43; see Figure 8). However, nonsignificant and moderate heterogeneity remained (τ 2 = 0. 07; χ 2 = 7.13, df = 4, p = 0.008; I2 = 44%) and no clear factors could be identified that would permit sensitivity analysis.
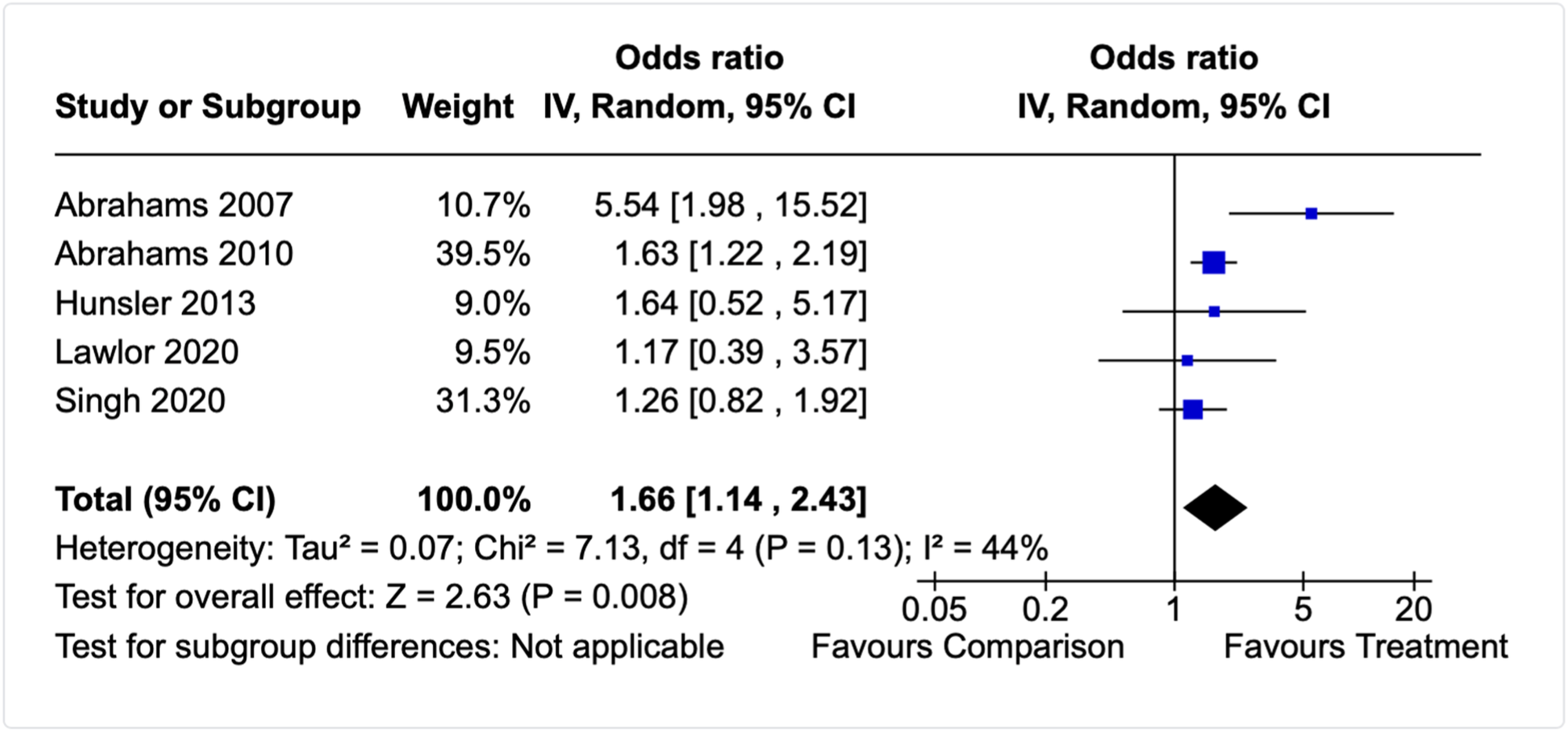
Forest plot for retaining parental care (prenatal/neonatal focus, post-intervention).
The odds of parents retaining care of their children was no different for parents who engaged in post-partum and early childhood treatments than for parents who engaged with TAU (Butz et al., 2001; Dakof et al., 2010; n = 179; OR = 1.18, 95% CI 0.63 to 2.18). In addition, there was no statistically significant heterogeneity in the distribution of effect sizes (τ 2 = 0.00; χ 2 = 0.78, df = 1, p = 0.38; I2 = 0%).
Stevens et al. (1998) examined whether residing in a long-term therapeutic community with or without children impacted whether mothers retained care of their children 6-months post-discharge. Findings from this single study suggest that the odds of mothers retaining care does not differ between mothers who do and do not have their children residing with them during treatment (n = 38; OR = 2.32, 95% CI 0.63 to 8.58). In comparison, Forrester et al. (2008) examined if an intensive family preservation service (‘Option 2’) impacted whether children remained with their parents at the end of a follow-up period of 3.5 years (range: 8 months–6.5 years, no statistically significant differences between groups on length of follow-up). Families engaged with Option 2 were more likely to be residing together than families engaged in TAU (n = 368; OR = 1.67, 95% CI 1.02 to 2.71).
Finally, in a series of studies examining different treatments for NAS, Hall and colleagues found that the odds of discharge to an infants' mother did not differ according to whether NAS was treated with (1) a stringent versus non-stringent weaning protocol (Hall et al., 2014; OR = 1.12, 95% CI 0.75 to 1.69); (b) a structured versus unstructured methadone weaning protocol (Hall et al., 2015; OR = 1.38, 95% CI 0.86 to 2.22); or (3) buprenorphine versus methadone (Hall et al., 2016; OR = 1.43, 95% CI 0.71 to 2.91).
Permanency
Thirteen studies reported permanency-related outcomes, yet only 7 of these studies reported sufficient data to calculate effect sizes (Boles et al., 2007; Chuang et al., 2012; Dakof et al., 2010; Harwin et al., 2018; Lloyd et al., 2021; Moore et al., 2020; Sagatun-Edwards, 2000; see Supporting Information: Appendix F for studies with missing data). Similar to other studies that use child welfare official data, the outcome time-point in relation to the intervention was often unclear or studies did not report appropriate time-to-event analyses to permit synthesis of studies examining time to permanency. Further, other studies only presented permanency data for children who had been reunified or who had experienced an OOHC rather than the entire randomised or assigned sample. These issues are likely to create biased effect estimates and their inclusion to estimate the effects of interventions is only recommended when appropriate data is available (e.g., Cox proportional hazards models, complete individual participant data; Deeks et al., 2019).
Of the 7 studies with sufficient data, 2 studies (Dakof et al., 2010; Harwin et al., 2018) assessed if engagement with an FTDC programme impacted whether children were permanently placed with a relative. At the post-intervention time-point, engagement with an FTDC did not increase the odds of children being placed permanently with relatives (n = 412; OR = 1.02, 95% CI 0.37 to 2.79; τ 2 = 0.31; χ 2 = 1.96, df = 1, p = 0.16; I2 = 49%). Harwin et al. (2018) also examined if engagement with an FTDC impacted whether or not children were in a permanent placement at all and found that at the closure of the case, engaging with the FTDC model did not increase the odds of children being in a permanent placement (n = 350; OR = 1.16, 95% CI 0.71 to 1.90).
Two studies examined if engagement with an FTDC model increased the likelihood of children being permanently placed with one or both parents (Harwin et al., 2018; Sagatun-Edwards, 2000). At treatment completion, engagement with an FTDC did not increase the odds of children being placed permanently with a parent (n = 439; OR = 1.24, 95% CI 0.84 to 1.81; τ 2 = 0.00; χ 2 = 0.42, df = 1, p = 0.52; I2 = 0%). Likewise, a meta-analysis of two studies (Boles et al., 2007; Sagatun-Edwards, 2000) indicated that engagement with a FTDC model did not increase the likelihood of permanency for children via a long-term foster parent/guardian or long-term placement (n = 4172; OR = 0.25, 95% CI 0.04 to 3.28; τ 2 = 2.52; χ 2 = 22.19, df = 1, p < 0.00001; I2 = 95%). Based on the Boles et al. (2007) study, comparison children were more likely than FTDC children to be placed with a guardian or in a long-term placement at 6-months follow-up (18-months after beginning the intervention; n = 3595; OR = 0.27; 95% CI 0.19 to 0.38), 12-months follow-up (n = 3595; OR = 0.24; 95% CI 0.17 to 0.34), or 24-months follow-up (n = 2990; OR = 0.32, 95% CI 0.22 to 0.45).
A meta-analysis of 3 studies (Boles et al., 2007; Harwin et al., 2018; Sagatun-Edwards, 2000) indicated that engagement with an FTDC model did not increase the likelihood of permanency via adoption (n = 4523; OR = 0.79, 95% CI 0.31 to 1.99; Figure 9) and there was no statistically significant heterogeneity in the distribution of effect sizes (τ 2 = 0.35; χ 2 = 4.37, df = 2, p = 0.11; I2 = 54%). Based on the Boles et al. (2007) study, however, comparison children were more likely than FTDC children to achieve permanency via adoption at 6-months follow-up (18-months after beginning the intervention; n = 3595; OR = 0.67; 95% CI 0.48 to 0.93), 12-months follow-up (n = 3595; OR = 0.60; 95% CI 0.43 to 0.83), or 24-months follow-up (n = 2990; OR = 0.64, 95% CI 0.46 to 0.89).
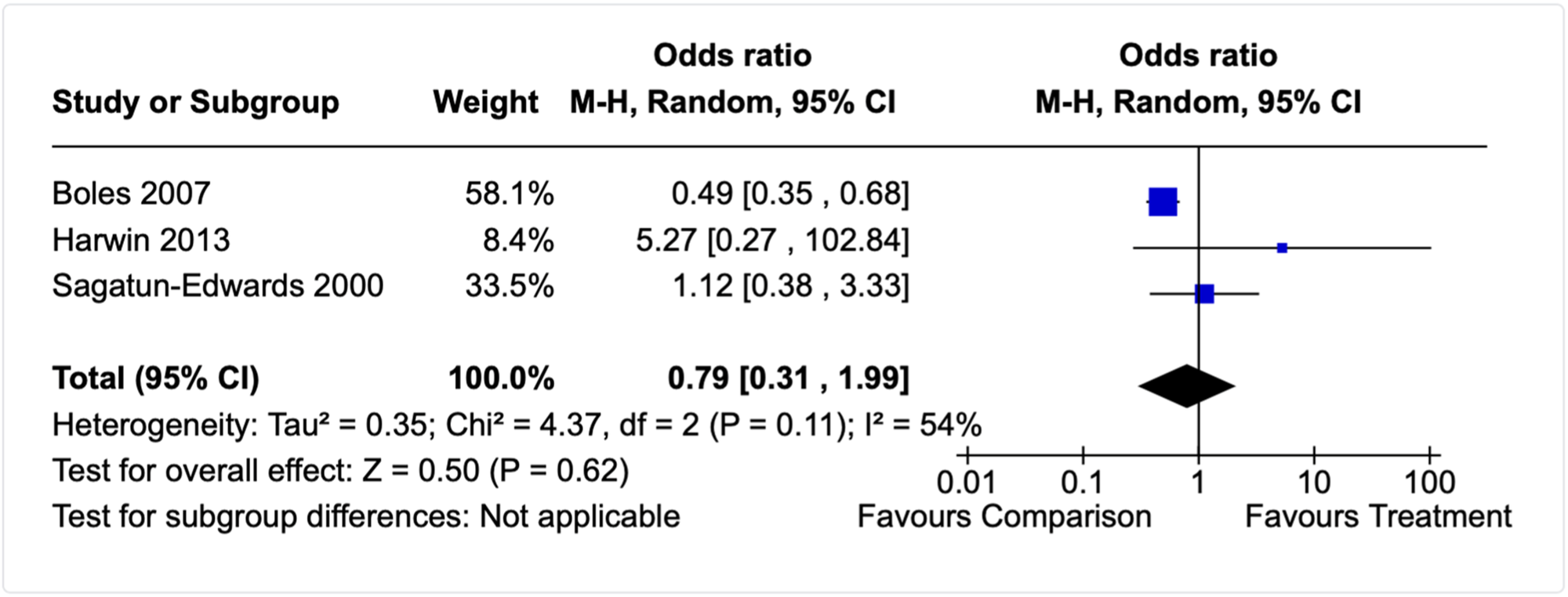
Forest plot for permanency via adoption meta-analysis (post-intervention, FTDC model).
Two other studies (Lloyd et al., 2021; Moore et al., 2020) used time-to-event data to examine whether engagement with an FTDC programme increased the likelihood of children exiting the child welfare system to a permanent placement. It was not appropriate to combine these studies with Harwin et al. (2013) as there was no fixed time-point in relation to the treatment for all participants (Deeks et al., 2019). Lloyd et al. (2021) appropriately analysed the data using a Cox proportional hazards model and found a medium to large effect, suggesting that the likelihood of a permanent child placement was higher for families engaged with a FTDC than for comparison cases who received TAU (unadjusted HR = 2.18, 95% CI 1.51 to 3.15). Similarly, Moore et al. (2020) analysed their data using a Cox regression model and found that the likelihood of a permanent child placement was higher for families engaged with a FTDC than for comparison cases who received TAU (adjusted OR = 2.76, p < 0.001 (CI not reported by authors)).
Finally, a single study analysed time-to-event data to examine whether engagement with an FTDC impacted the amount of time taken for children to reach a permanent placement (Chuang et al., 2012). Results of the authors' Cox proportional hazards model indicated that the time taken to achieve permanency was longer for families who had engaged with an FTDC compared to families who received TAU (HR = 0.52, robust SE = 0.10).
Reunification
Twenty-two studies reported reunification outcomes, however, only 6 reported sufficient data to calculate effect sizes (Boles et al., 2007; Brook et al., 2007; Lloyd et al., 2021; Quittan, 2004; Ryan et al., 2016; Sanmartin et al., 2020; see Supporting Information: Appendix F for studies with missing data). The studies with missing outcome data had issues similar to those reported for the other child welfare outcomes (see above). A particular issue with this outcome category was that not all children were removed from their parents at the beginning of the intervention, meaning that it was not possible for all families randomised or assigned to achieve the outcome. Further, studies did not consistently report if the reunification related to a removal prior or during the intervention, or whether the reunification was related to an initial or subsequent removals. These issues combined, rendered many of the studies unsuitable for estimating the effect of the intervention for this particular outcome.
Of the 6 studies with sufficient data to calculate effect sizes, 5 examined the impact of treatment on the rate of reunification. One study (Sanmartin et al., 2020) examined the impact of legislative responses to parental substance misuse whereby children are removed and placed into foster care. Specifically, Sanmartin and colleagues (2020) compared the rate of reunification for children under age 1 who had been removed due to parental substance misuse for 24 American states with such legislation to 26 American states without this type of legislation. Based on discrete time-hazard models, the likelihood of reunification with parent(s) after removal was lower in states with legislation that criminalises or classes parental substance misuse as child abuse compared to those states without the legislation (n = 350,604; HR = 0.95, 95% CI 0.94 to 0.96). The four remaining studies focused on rate of reunification included treatment and comparison groups where removal had occurred for all children due to parental substance misuse, but used different analytic methods and time-points, which precluded combining all three into one meta-analysis. Lloyd et al. (2021) examined whether engagement with an FTDC programme increased the likelihood of reunification, tracking families from the point of referral to the FTDC until an end date of 2019 (study period: October 2015–March 2019). The authors found that the likelihood of reunification during the study period was higher for families engaged with a FTDC than families receiving TAU (unadjusted HR = 3.92, 95% CI 2.42 to 6.33).
Boles et al. (2007), Ryan et al. (2016), and Quittan (2004) reported counts for reunification. Boles et al. (2007) and Quittan (2004) reported both post-intervention and follow-up data capturing multiple time-points between 6 and 18 months after intervention completion, whereas Ryan et al. (2016) began tracking families from the point of petition (initiated randomisation of cases) to 36-months later (i.e., approximately 24-month follow-up point). Boles et al. (2007) compared an FTDC model with parallel specialised treatment and recovery services to TAU (usual child welfare services), Quittan (2004) compared a standard FTDC model with a FTDC model enhanced with the Celebrating Families! intervention (cultural adaption of the Strengthening Families programme), and Ryan et al. (2016) compared TAU child welfare services to a Recovery Coaches model. There were no differences in the odds of reunification between a standard FTDC model and FTDC + Celebrating Families! at post-intervention (n = 51; OR = 1.53, 95% CI 0.46 to 5.02) or at the 6–12 month follow-up mark (OR = 1.28, 95% CI = 0.38 to 4.27). However, Ryan et al. (2016) found that the odds of reunification was higher for families assigned to Recovery Coaches compared to TAU (n = 3440; OR = 1.34, 95% CI 1.11 to 1.62) approximately 24-months after treatment completion (or 3-years after initial petition). Likewise, Boles et al. (2007) found that the odds of reunification was higher for families participating in an FTDC model with parallel specialised treatment and recovery services compared to TAU (usual child welfare services) at treatment completion (12-months after beginning treatment; n = 4084; OR = 2.85, 95% CI 1.94 to 4.18), at 6-months follow-up (n = 3595; OR = 2.64; 95% CI 1.87 to 3.71), 12-months follow-up (n = 3595; OR = 2.96; 95% CI 2.08 to 4.20), and 24-months follow-up (n = 2990; OR = 2.60, 95% CI 1.83 to 3.67).
A final study (Brook et al., 2007) compared the time taken to reunify for families engaged with an intensive service coordination treatment to families receiving TAU. Although reunification occurred at a faster rate for families engaged with treatment, the effect size representing the differences in trajectories was small and not statistically significant (Wilcoxon [Gehan] = 1.763, p = 0.1842).
Termination of parental rights
Six studies examined the effects of treatment using outcomes relating to termination of parental rights (Carey et al., 2010b; Dakof et al., 2009, 2010; Forrester et al., 2008; Green et al., 2007; van Wormer et al., 2016), however, only 3 studies reported sufficient data to calculate effect sizes. Studies with missing data generally did not clearly report the timing of outcome measurement in relation to treatment and so it was unclear whether all participants had completed the intervention and whether there was variability in when the outcome was measured after completion of the intervention. Two studies by Dakof and colleagues (2009, 2010) compared the FTDC model with either comprehensive case-management or a family-focused programme set in the home (Engaging Moms; Dakof et al., 2009, 2010). The initial quasi-experimental evaluation (Dakof et al., 2009) examined if the two approaches differed in relation to whether an application for termination of parental rights (TPR) had been filed and whether parents voluntarily surrendered their parental rights permanently. At treatment completion, the odds of a TPR application being filed were lower for families who participated in the FTDC+Engaging Moms approach than for families engaged with FTDC+case-management approach (OR = 0.28, 95% CI 0.11 to 0.74). There were no differences between the groups for voluntary and permanent surrender of parental rights (OR = 0.85, 95% CI 0.20 to 3.65). In the randomised evaluation of the FTDC+Engaging Moms model found that the odds of a child being placed in foster care or with a relative, along with TPR, did not differ between the treatment and comparison condition (foster: OR = 0.36, 95% CI 0.10, 1.34; relative: OR = 0.56, 95% CI 0.12, 2.57). The third study with sufficient data for effect size calculation also examined an FTDC model (Green et al., 2007) and tracked families for 5-years from enrolment (∼4-years after treatment completion). There were no differences between FTDC and comparison children in terms of whether the permanency type was termination of parental rights (n = 446; OR = 0.79, 95% CI 0.51 to 1.21).
Child development domain
Twenty-two studies included at least one measure of child development, across a range of areas, with most studies measuring cognition, language, and/or motor skills. Table 8 below provides a summary of the analyses conducted across all outcomes in the child development domain, and the subsections below provide further detail about the analysis results and included studies. As described above in the ‘Data synthesis’ section, we developed an analysis plan informed by the nature of the included interventions, comparison conditions, type of outcome, and timing of outcome measurement. Meta-analyses were conducted where there were at least two independent studies that were sufficiently similar across these factors.
Child development outcome domain analyses and results.
Abbreviations: BRI, Behavioural Regulation Index; GEC, Global Executive Composite; MCI, Metacognition Index.
Cognitive development
Eleven studies examined whether treatment impacted young children's cognition, yet three of these studies (Field et al., 1998; Jimenez, 2018; Kaltenbach et al., 1986) reported insufficient data to calculate effect sizes (e.g., no standard deviation or other statistical data to permit hand calculations). Five studies assessed intervention effectiveness using TAU comparison conditions and measured child cognition post-intervention when children were between 18 and 46 months (Black et al., 1994; Conerly, 1999; Ersnt et al., 1999; Kilbride et al., 2000; Porges et al., 2018). These interventions began at birth or early infancy and all focused on child health and development. None of the interventions included an intervention component focused on treating parental substance misuse, two included case-management (Ersnt et al., 1999; Kilbride et al., 2000), and two integrated a parent-focused therapeutic component (Black et al., 1994; Ersnt et al., 1999). A meta-analysis of these 5 studies indicated that early child cognition did not differ for those who had received treatment versus TAU (Figure 10; n = 245; SMD = 0.17, 95% CI −0.09 to 0.43) and there was little heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 1.82, df = 3, p = 0.77; I2 = 0%).
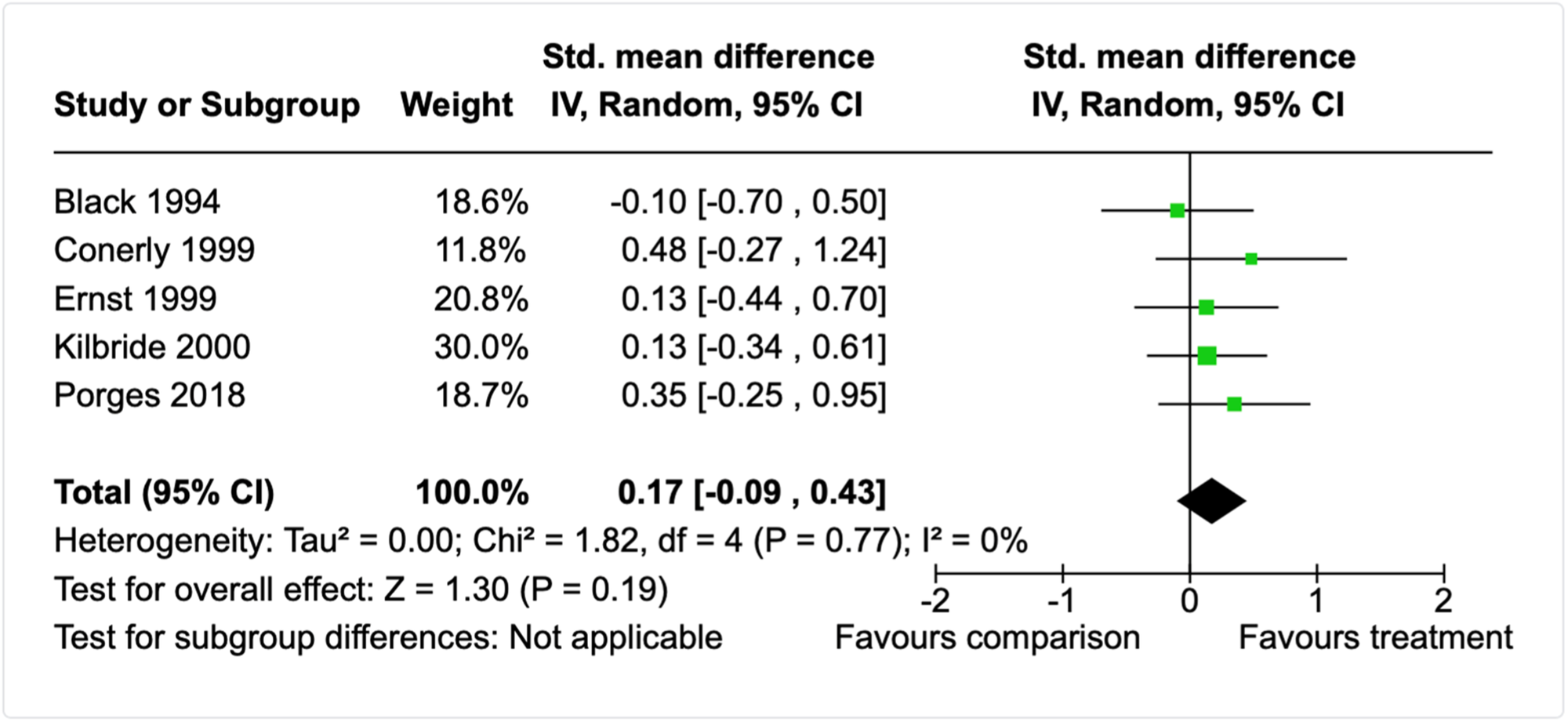
Forest plot for child cognition meta-analysis (post-intervention).
Three studies examined the impact of alternate treatments on child cognition and three of these were pharmacological interventions. The first study compared cognitive outcomes at age 12-months after treatment for NAS with either methadone or clonidine (Bada et al., 2015), and again there was no difference between treatments (n = 24; SMD = −0.05, 95% CI −0.85 to 0.75). The second study compared cognitive outcomes at age 18-months after treatment for NAS with either methadone or morphine (Flannery et al., 2020), and again there was no difference between treatments (n = 83; SMD = −0.10, 95% CI −0.53 to 0.33). The third study comparing alternative treatments examined the effectiveness of a child-focused developmental curriculum with young children with prenatal cocaine exposure delivered either one-on-one in the home twice a week or at in childcare group setting 5 days per week (Claussen et al., 2004). Mothers in both groups, who continued to experience significant psychosocial stressors (including substance use) also received other support services (e.g., medical care, social work services, transportation). Upon intervention completion, when children were approximately 36-months of age, there were no differences in cognition between the two treatment approaches (n = 96; SMD = −0.29, 95% CI −0.69, 0.11).
Executive functioning and hyperactivity
Five studies reported measuring child executive functioning, yet 2 did not report complete data for the executive function measure after intervention completion (Margolis et al., 2017; Sullivan, 1984). Kim et al. (2019) examined the impact of Solution Focused Behavioural Therapy for substance misusing parents – without inclusion of children – on child executive functioning measured via parent self-report on a standardised tool. At the post-intervention time-point, children of parents engaging with Brief Solution-Focused Therapy did not differ from parents engaged with TAU on: (1) a composite measuring global executive functioning (n = 75; SMD = −0.16, 95% CI −0.62 to 0.30); (2) a composite measuring ability to problem-solve, plan and organise, sustain working memory, and/or monitor performance (n = 75; SMD = −0.19, 95% CI −0.64 to 0.27); or (3) a composite measuring the ability to regulate behaviour (n = 75; SMD = −0.11, 95% CI −0.56 to 0.35). There was also no difference between groups on the 8 individual subscales that made up the executive functioning composites (see Table 8) or on another measure of attention (CBCL) completed by parents (see Table 8). Davis-Susser (1990) examined the impact of a child-focused group programme for children of alcoholics on two measures of child executive functioning measured via parent self-report on a standardised tool. At the post-intervention time-point, children engaging with the group programme did not differ from children who did not participate in the programme on: (1) a measure of attention (n = 40; SMD = −0.12, 95% CI −0.83 to 0.60); or (2) a measure of hyperactivity (n = 40; SMD = −0.28, 95% CI −1.00 to 0.44). The third study (Adelman, 1990) found that children engaging in a child-focused group therapy programme for children of alcohol-misusing parents did not differ on self-rated levels of self-directiveness than children of alcohol misusing parents who did not engage in treatment (n = 44; SMD = −0.16, 95% CI −0.76 to 0.43). While Sullivan (1984) did not report complete executive function outcome data, there was sufficient data for effect size calculation for a measure of hyperactivity. Sullivan (1984) examined the effectiveness of a therapeutic intervention for alcoholic parents compared to no treatment at 8-months follow-up. The intervention comprised 6 parent group therapy sessions, 6 child group therapy sessions, and 6 family therapy sessions focused on psychoeducation and supportive psychotherapy. There were no differences in the level of parent-reported levels of child hyperactivity after participating in the intervention compared to the no treatment control group (n = 33; SMD = −0.27, 95% CI −0.64 to 1.14).
Language development
Six studies examined whether treatment impacted young children's language development, yet one of these studies (Jimenez, 2018) reported insufficient data to calculate effect sizes (e.g., no standard deviation or other statistical data to permit hand calculations). Two studies assessed intervention effectiveness using TAU comparison conditions and measured child language post-intervention when children were between 18 and 46 months (Conerly, 1999; Porges et al., 2018). These interventions began at birth or early infancy and all focused on child health and development. None of the interventions included an intervention component focused on treating parental substance misuse or any other areas of family-functioning (e.g., parent wellbeing). A meta-analysis of these 2 studies indicated that receptive language development did not differ for those who had received treatment versus TAU (n = 84; SMD = 0.44, 95% CI −0.13 to 1.01) and there was modest but nonsignificant heterogeneity among the effect sizes (τ 2 = 0.06; χ 2 = 1.50, df = 1, p = 0.22; I 2 = 33%). However, children receiving early developmental intervention had better expressive language development upon treatment completed compared to children receiving TAU (n = 85; SMD = 0.55, 95% CI 0.08 to 1.01) and there was no heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 0.70, df = 1, p = 0.40; I2 = 0%).
Three studies examined the impact of alternate treatments on child language, two of which were pharmacological interventions. These were the same treatment-treatment studies described above in the ‘Child cognition’ section (Bada et al., 2015; Flannery et al., 2020; Claussen et al., 2004). Flannery et al. (2020) found no differences in language development for children 18-months after treatment for NAS with either methadone or morphine (n = 83; SMD = −0.10, 95% CI −0.54 to 0.33). Similarly, Bada et al. (2015) found no difference in language development 12-months after treatment for NAS with either methadone or clonidine, for either total language development (n = 24; SMD = 0.17, 95% CI −0.63 to 0.98); expressive language development; (n = 24; SMD = 0.06, 95% CI −0.74 to 0.86) or receptive language development (n = 24; SMD = 0.44, 95% CI −0.37 to 1.25). The third study comparing the centre- versus home-based developmental curriculum (Claussen et al., 2004) found that both expressive and receptive language were more developed in children who participated in the centre-based versus home-based intervention (Expressive: n = 96, SMD = −0.75, 95% CI −1.17 to −0.34; Receptive: n = 96, SMD = −0.48, 95% CI −0.89, −0.07).
Motor development
Seven studies examined whether treatment impacted young children's motor development, yet two of these studies (Field et al., 1998; Jimenez, 2018) reported insufficient data to calculate effect sizes (e.g., no standard deviation or other statistical data to permit hand calculations). Two studies assessed intervention effectiveness using TAU comparison conditions and measured child motor skills post-intervention when children were between 18 and 36 months (Black et al., 1994; Ersnt et al., 1999). Both interventions began at birth or early infancy and focused on child health and development. Neither study included an intervention component focused on treating parental substance misuse, one included case-management (Ersnt et al., 1999), and both integrated a parent-focused therapeutic component. A meta-analysis of these studies indicated that early child motor skills did not differ for those who had received the intervention versus TAU (n = 91; SMD = −0.16, 95% CI −0.57 to 0.26), and no heterogeneity was detected among the effect sizes (τ 2 = 0.00; χ 2 = 0.65, df = 1, p = 0.42; I2 = 0%).
Three studies examined the impact of alternate treatments on child motor skills and three of these were pharmacological interventions. These were the same treatment-treatment studies described above in the ‘Child cognition’ section (Bada et al., 2015; Flannery et al., 2020; Claussen et al., 2004). In contrast, Flannery et al. (2020) found no differences in motor skills for children 18-months after treatment for NAS with either methadone or morphine (n = 83; SMD = −0.25, 95% CI −0.68 to 0.19). Bada et al. (2015) also found no difference in motor development 12-months after treatment for NAS with either methadone or clonidine (n = 24; SMD = 0.19, 95% CI −0.61 to 1.00). The fourth study, which compared a centre- versus home-based developmental curriculum (Claussen et al., 2004) found that both fine and gross motor skills did not differ for children who participated in either the centre- or home-based intervention (Fine: n = 96, SMD = −0.12, 95% CI −0.52, 0.29; Gross: n = 96, SMD = −0.25, 95% CI −0.65, 0.16).
Sleep
Two studies measured child sleep problems. One was the study described above which compared a centre- versus home-based developmental curriculum (Claussen et al., 2004) and the other compared a parent and child-focused nurse home-visiting intervention to usual community care approximately 6 to 18-months after treatment completion (Butz et al., 2001). Claussen et al. (2004) found that the level of sleep problems did not differ for children who participated in either the centre- or home-based intervention (n = 96, SMD = −0.30, 95% CI −0.70, 0.10). Likewise, Butz et al. (2001) found that the level of sleep problems did not differ for children who received the home-visiting or usual community care at ∼18-months after treatment (n = 100, SMD = 0.21, 95% CI −0.18, 0.61).
Social skills
Eight studies reported child social skills as an outcome measure, however, three of these studies (Field et al., 1998; Margolis et al., 2017; Orte et al., 2015) reported insufficient data to calculate effect sizes (e.g., no standard deviation or other statistical data to permit hand calculations). One study utilised a child-report measure to examine the effectiveness of child-focused group therapy programme compared to a waitlist control group (Scheer, 1996). At the post-intervention time-point, children's self-reported social skills did not differ between those who were assigned to the intervention versus waitlist control condition (n = 30; SMD = 0.33, 95% CI −0.39 to 1.05).
Two studies compared psychosocial interventions to TAU conditions using parent-report measures of child social skills (Conerly, 1999; Kim et al., 2019). One study was a solution-focused individual therapy intervention for parents (Kim et al., 2019) and the other was a developmentally focused child and family early intervention programme (Conerly, 1999). Upon treatment completion, child social skills did not differ between the intervention and TAU conditions (n = 100; SMD = 0.11, 95% CI −0.29 to 0.52) and there was no heterogeneity detected in the distribution of effect sizes (τ 2 = 0.00; χ 2 = 0.64, df = 1, p = 0.42; I2 = 0%). A third study examined the effectiveness of a therapeutic intervention (Sullivan, 1984) for alcoholic parents compared to no treatment at 8-months follow-up. The intervention comprised 6 parent group therapy sessions, 6 child group therapy sessions, and 6 family therapy sessions focused on psychoeducation and supportive psychotherapy. For this study, parents rated their children's social skills lower in after participating in the intervention compared to the no treatment control group (n = 33; SMD = −0.73, 95% CI −1.46 to −0.01). The final study compared two alternative treatments and is detailed in the ‘Child cognition’ and subsequent sections (Claussen et al., 2004). At post-intervention, child social skills, as rated by parents, did not differ for children who participated in either the centre- or home-based intervention (n = 96, SMD = 0.19, 95% CI −0.22, 0.59).
Other child development measures
Four studies measured developmentally related outcomes that did not fit clearly under the abovementioned outcome categories. Flannery et al. (2020) found no differences in the odds that a family was engaged with early intervention services to support child development 18-months after treatment for NAS with either methadone or morphine (n = 83; OR = 0.95, 95% CI 0.39 to 2.30). The second study (Sullivan, 1984), described under ‘Child social skills’ above, utilised a comprehensive standardised and normed parent-report measure of numerous aspects of child development and functioning. In addition to social skills and other areas examined under the behavioural/emotional outcome domains, three other scales were developmentally related: Cerebral Dysfunction, Intellectual Screening, and Development. At 8-months follow-up, parents in the treatment and control groups did not differ in reports of their children's difficulties in these three areas (n = 33; Cerebral Dysfunction: SMD = −0.39, 95% CI −1.09 to 0.32; Intellectual Screening: SMD = −0.58, 95% CI −1.29 to 0.14; Development: SMD = −0.30, 95% CI −1.00 to 0.40). The third study in this outcome category assessed whether children's development was ‘within normal limits’ with no further specification (Penny & Pratt, 2011). This study compared usual early childhood health care to a multidisciplinary coordinated clinical pathway to care model for families affected by parental substance misuse with children from birth to 12-months. At the post-intervention time-point, children in the coordinated care and TAU groups did not differ in terms of whether they were developing within normal limits (n = 24; OR = 1.43, 95% CI 0.11 to 18.00). The final study (Adelman, 1990) found that children engaging in a child-focused group therapy programme for children of alcohol-misusing parents did not differ from children who did not engage in treatment based on a teacher-rated measure of extroversion which included concepts such as self-centredness, energy levels, and social skills (n = 44; SMD = −0.26, 95% CI −0.86 to 0.33).
Child emotional and behavioural domain
Fifty studies included at least one measure of an emotional or behavioural child outcome. A wide range of outcomes were captured under this domain, including both parent- and child-report measures. Table 9 provides a summary of the analyses conducted across all outcomes in the emotional and behavioural domain, and the subsections below provide further detail about the analysis results and included studies. As described above in the ‘Data synthesis’ section, we developed an analysis plan informed by the nature of the included interventions, comparison conditions, type of outcome, and timing of outcome measurement. Meta-analyses were conducted where there were at least two independent studies that were sufficiently similar across these factors.
Child behavioural and emotional domain analyses and results.
Total problems
Twenty-three studies examined the effectiveness of treatment using parent-report standardised measures that produce a composite for overall emotional and/or behavioural problems for children at their developmental age. Eight of these studies either reported no outcome data at all or insufficient data to calculate effect sizes (e.g., no standard deviation or other statistical data to permit hand calculations) (Barlow et al., 2019; Dore et al., 1999; Logan et al., 2001; Luthar et al., 2000, 2007; Margolis et al., 2017; Roosa et al., 1990; Sullivan, 1984). Of the studies with complete data (k = 15), 9 studies compared an eligible intervention to a TAU comparison condition at post-intervention, with 6 studies using both a post-intervention and short-term follow-up (≥3 months ≤6-months), and 3 studies also including a longer follow-up (>6-months ≤12-months). An additional two studies compared alternative treatments (Claussen et al., 2004 and Flannery et al., 2020 described above). Three studies included both a parent and child-report measure for total emotional and behavioural problems (Luthar & Suchman, 2000; Luthar et al., 2007; Margolis et al., 2017), but reported insufficient data to permit calculation of effect sizes (e.g., no standard deviations or other statistical data to permit hand calculations).
The meta-analysis of the 9 studies using a post-intervention outcome measure produced a small effect size, indicating that treatment was more effective than TAU for reducing emotional and behavioural problems (Figure 11; n = 567; SMD = 0.39, 95% CI 0.06 to 0.72). There was moderate and significant heterogeneity among the effect sizes (τ 2 = 0.17; χ 2 = 26.90, df = 8, p = 0.0007; I2 = 70%), yet too few studies to conduct subgroup analyses. To explore this heterogeneity, we first examined the included studies according to the a priori defined moderators: child age, type of outcome measure, type of parental substance use, intervention setting, and practitioners implementing the intervention. In terms of child age, 3 studies included children with a mean age of ≥3 but ≤5 years (Brown et al., 2021; Conerly, 1999; Dawe et al., 2007), whereas 5 studies included children with a mean age of >5 to ≤10 years (Catania, 1985; Dyba et al., 2019; Kelley et al., 2002; Kim et al., 2019). However, dividing the studies by age was considered inappropriate as proportions of study samples fell into both age categories. All studies used either well-validated standardised measure or a measure with associated psychometric data to establish its reliability and validity. All interventions were implemented by clinicians, mostly with postgraduate training. Four studies did not specify or report the specific type of parental substance misuse (Catania, 1985; Dawe et al., 2007; Dyba et al., 2019; Kim et al., 2019), 2 studies included alcohol misusing parents (Kelley et al., 2002; Satyanarayana et al., 2016), 2 studies included drug misusing parents (e.g., cocaine; Conerly et al., 1999; Kelley et al., 2002), and 1 study included polysubstance misusing parents (Brown et al., 2021). This meant we could not divide the studies easily by type of substance misused by parents. The intervention was predominantly implemented in the home for 2 studies (Brown et al., 2021; Dawe et al., 2007) but in clinics or community settings for 7 studies (Catania, 1985; Conerly, 1999; Dyba et al., 2019; Kelley et al., 2002; Kim et al., 2019; Satyanarayana et al., 2016). A sensitivity analysis removing the two studies predominantly set in the home reduced the precision of the meta-analysis (SMD = 0.34, 95% CI −0.04. to 0.73) and slightly increased heterogeneity (τ 2 = 0.20; χ 2 = 24.54, df = 6, p = 0.08; I2 = 76%). This suggested that the setting of the intervention may not have been the source of heterogeneity.
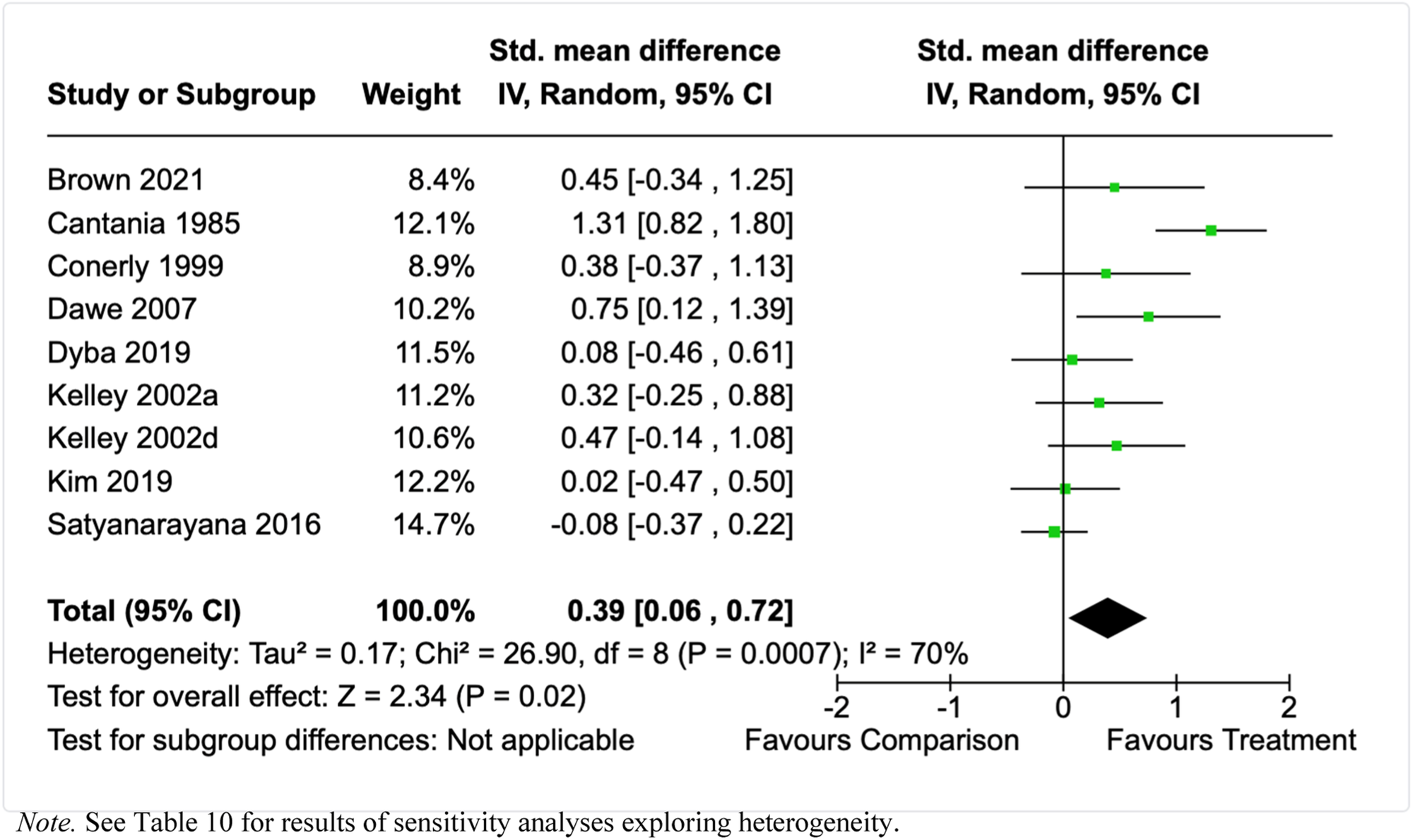
Forest plot for total problems meta-analysis (post-intervention, parent-report).
Because there were no clear outliers or cohesive categories in relation to a priori moderators, aside from intervention setting, we also examined the nature of the research designs and interventions to identify potential sources of heterogeneity. A range of possible sources of heterogeneity were identified, with the results of these sensitivity analyses presented in Table 10 below. Use of a non-randomised evaluation design, absence of a parental substance misuse treatment, an intervention duration of >6-months, or an intervention spanning prenatal and postnatal periods did not reduce heterogeneity in the results and reduced the precision of the meta-analysis. However, removal of the two studies that used a group delivery format (Cantania, 1985; Dyba et al., 2019) – compared to the others that were individual or a mix of delivery formats – reduced detected heterogeneity to non-significance and 28%, but the meta-analysis no longer reached statistical significance. Both of these studies evaluated an intervention with a parent-focus in terms of parental substance misuse and/or wellbeing, in addition to parent-skills training without an explicit focus on the parent-child relationship or attachment.
Sensitivity analyses by study features for total child behavioural and emotional problems.
Other studies were ≤6-months in duration.
At ≥3-months to <6-months follow-up, a meta-analysis of 7 studies (see Figure 12) indicated that parents engaged in treatment did not report lower levels of total child behavioural and emotional problems compared to those receiving TAU (n = 463; SMD = 0.28, 95% CI −0.03 to 0.60), and there was statistically significant heterogeneity among effect sizes (τ 2 = 0.10; χ 2 = 14.97, df = 6, p = 0.02; I2 = 60%). Similar to the post-intervention meta-analyses for total problems, we explored this heterogeneity by first examining the included studies according to the a priori defined moderators: child age, type of outcome measure, type of parental substance use, intervention setting, and practitioners implementing the intervention. In terms of child age, 1 study included children with a mean age of ≥3 but ≤5 years (Dawe et al., 2007), whereas 6 studies included children with a mean age of >5 to ≤10 years (Dyba et al., 2019; Kelley et al., 2002; Saldana et al., 2015; Satyanarayana et al., 2016). However, dividing the studies by age was considered inappropriate as proportions of study samples fell into both age categories. All studies used either well-validated standardised measure or a measure with associated psychometric data to establish its reliability and validity. All interventions were implemented by clinicians, mostly with postgraduate training. Four studies did not specify or report the type of parental substance misuse, 2 studies included alcohol misusing parents (Kelley et al., 2002; Satyanarayana et al., 2016), and 1 study included drug misusing parents (e.g., cocaine; Conerly, 1999). This meant we could not divide the studies easily by type of substance misused by parents. The intervention was implemented primarily in the home for 2 studies (Dawe et al., 2007; Saldana, 2015), in outpatient clinics or community settings for 4 studies (Cantania, 1985; Dyba et al., 2019; Kelley et al., 2002), and an inpatient setting for 1 study (Satyanarayana et al., 2016). A sensitivity analysis removing the two studies set in the home reduced the precision of the meta-analysis (n = 400; SMD = 0.24, 95% CI −0.11 to 0.59) and slightly increased heterogeneity (τ 2 = 0.10; χ 2 = 10.94, df = 5, p = 0.03; I2 = 63%). A sensitivity analysis removing the single study using an inpatient setting indicated that parents engaged in treatment reported lower levels of total child behavioural and emotional problems compared to those receiving TAU (n = 286; SMD = 0.40, 95% CI 0.10 to 0.69), with nonsignificant heterogeneity (τ 2 = 0.04; χ 2 = 7.46, df = 5, p = 0.19; I2 = 33%). This suggested that the divergent inpatient setting of the intervention may have been the source of heterogeneity.
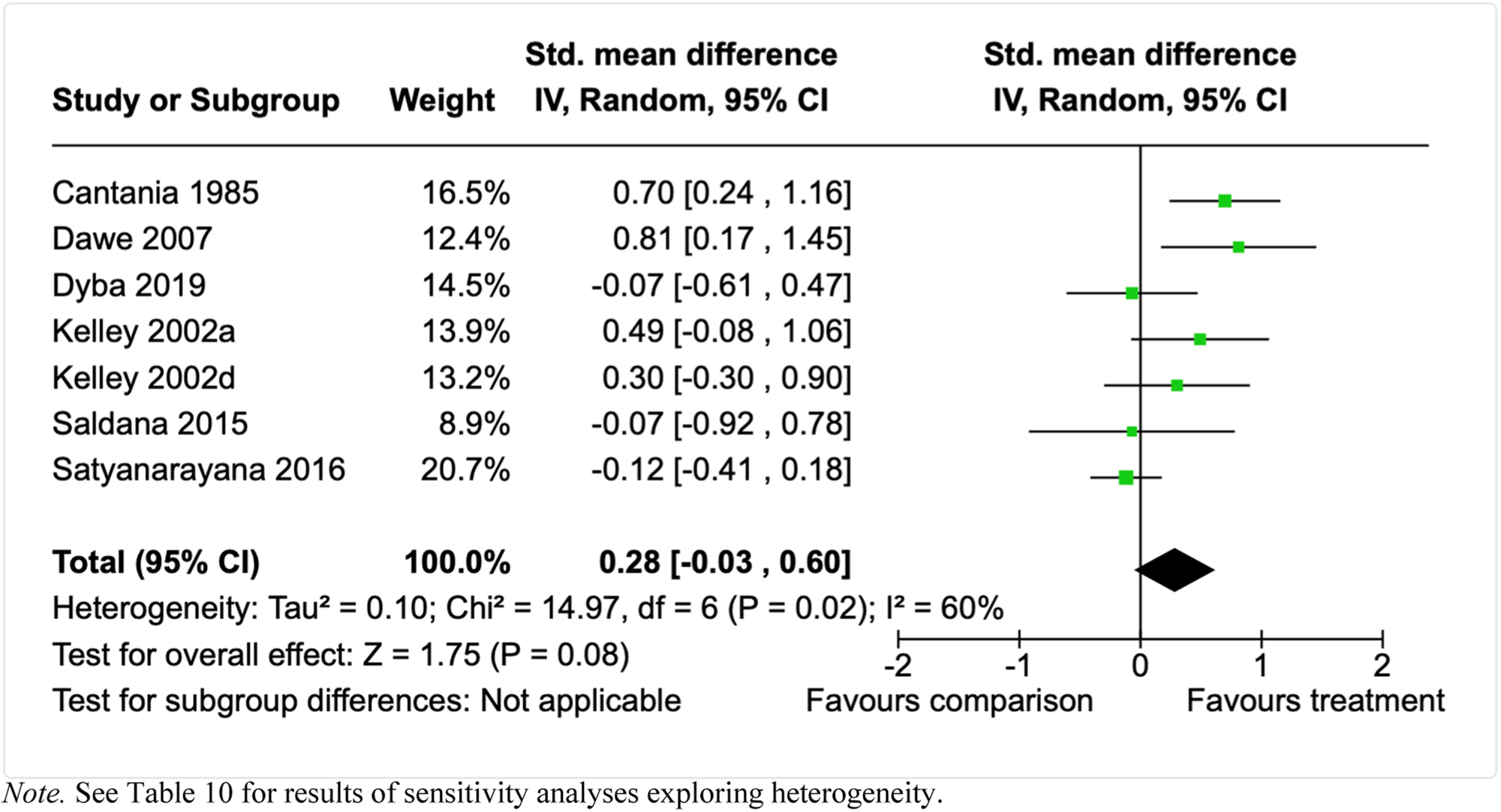
Forest plot for total problems meta-analysis (short follow-up, parent-report).
However, other potential sources of heterogeneity were tested with sensitivity analyses, with the results presented in Table 10. These indicated that (1) use of a non-randomised evaluation design or an an intervention spanning prenatal and postnatal periods (Dyba et al., 2019); (2) absence of a parental or couples focused treatment component (Cantania, 1985); (3) use of an explicit child health and/or development intervention component (Dawe et al., 2007); (4) or use of a group-only delivery format (Cantania, 1985; Dyba et al., 2019) did not reduce heterogeneity in the results or reduced the precision of the meta-analysis.
At ≥6-months follow-up, a meta-analysis of 3 studies (Kelley et al., 2002; Butz et al., 2001; see Figure 13) indicated that parents engaged in treatment continued to report lower levels of total child behavioural and emotional problems compared to parents receiving TAU (n = 192; SMD = 0.31, 95% CI 0.03 to 0.60), and this overall effect had nonsignificant and minimal heterogeneity (τ 2 = 0.00; χ 2 = 0.09, df = 2, p = 0.96; I2 = 0%). Two of these studies examined the effectiveness of 32 sessions of treatment for either paternal drug or alcohol misuse, which was comprised of 12 sessions of Behavioural Couples Therapy and 20 sessions of individual cognitive behavioural therapy (CBT) for fathers (Kelley & Fals-Stewart, 2002 [alcohol]; Kelley & Fals-Stewart, 2002 [drug]). The third study examined the effectiveness of a home-visiting intervention focused on parent and child wellbeing from birth until the child was aged 18-months (Butz et al., 2001).
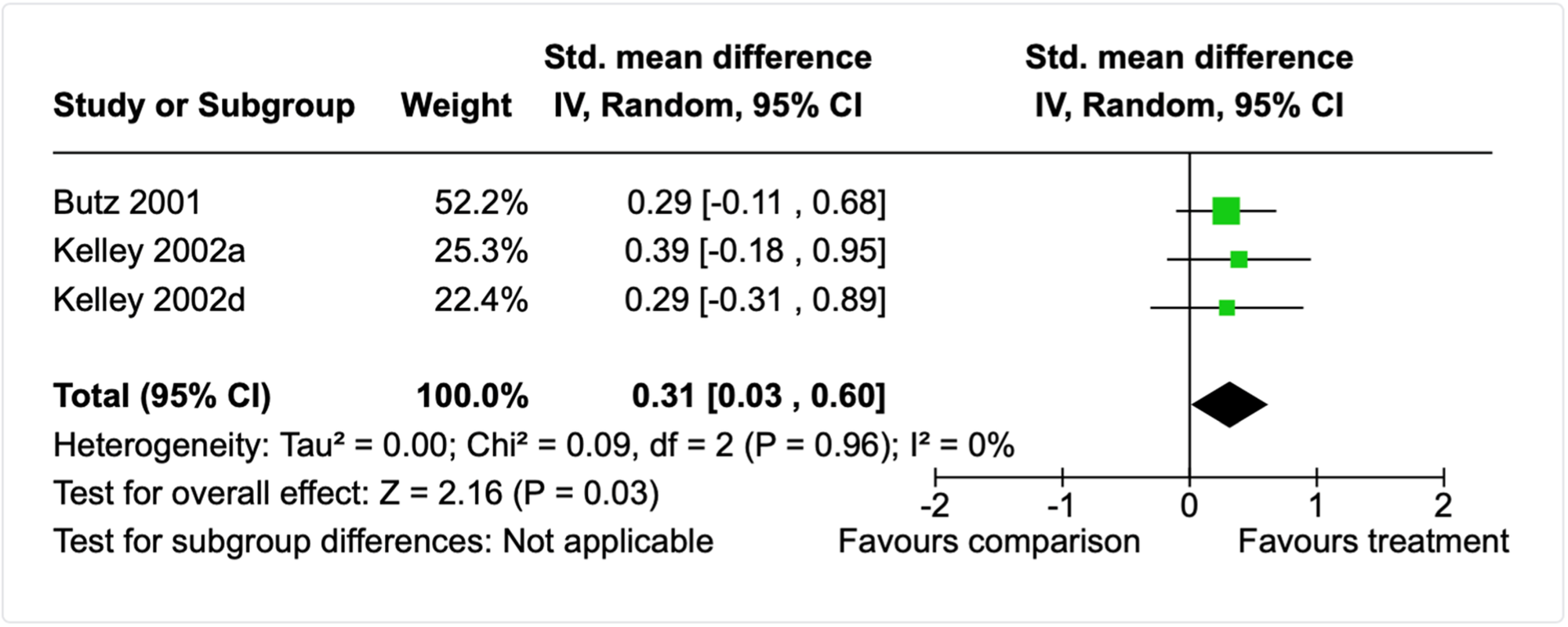
Forest plot for total problems meta-analysis (long follow-up, parent-report).
Two studies (Forrester et al., 2008; dos Reis Viela et al., 2016) reported the number of participants who scored in the clinical range of the instrument used to measure total child emotional and behavioural problems. The Forrester et al. (2008) study is described in previous sections and reported the number of children who scored in the clinical range for the Strengths and Difficulties Questionnaire. The authors found that the odds of having clinical levels of emotional/behavioural problems did not differ for children engaged versus not engaged with treatment (n = 27; OR = 2.00, 95% CI 0.38 to 10.58). Dos Reis Viela et al. (2016) examined the impact of a school-based intervention model that provided mental health support and a range of other activities aiming to prevent substance use in children being raised in families affected by substance misuse. The authors found that children engaged with treatment were less likely to obtain a score in the clinical range for total emotional/behavioural problems, as reported by caregivers (n = 101; OR = 0.24, 95% CI 0.10 to 0.57).
Two studies compared alternative treatments using a measure of total child emotional and behavioural problems, the intervention for both of which are described in sections above. Flannery et al. (2020) found no differences in parent reported total problem behaviours 18-months after treatment for NAS with either methadone or morphine (n = 77; SMD = 0.00, 95% CI −0.45 to 0.45). Claussen et al. (2004) found that, at post-intervention, child behavioural and emotional problems, as rated by parents, did not differ for children who participated in either the centre- or home-based child development intervention (n = 96, SMD = −0.16, 95% CI −0.56, 0.24).
One study examined whether participating in a therapeutic group in the school setting impacted overall teacher-reported behavioural problems for children with alcohol misusing parents (Adelman, 1990). At post-intervention children engaging with this intervention did not differ from children who did not (n = 44; SMD = 0.04, 95% CI −0.55 to 0.63).
Externalising
19 studies examined the effectiveness of treatment using parent-report standardised measures that produce a composite for child externalising problems. Three studies had missing data, by either reporting no between group data or only data for participants with scores over a particular threshold on the outcome measure (Bartle-Haring et al., 2018; Pirnia, 2019; Margolis et al., 2017). Of the studies without missing data (k = 15), 11 studies compared an eligible intervention to a TAU comparison condition at post-intervention, 3 studies used both a post-intervention and short-term follow-up (≥3 months ≤6-months), and 5 studies also included a longer follow-up (>6-months ≤12-months). An additional two studies compared alternative treatments (Claussen et al., 2004 and Flannery et al., 2020 described above). In addition, one study provided both a child- and parent-report measure of externalising problems (Mitrani et al., 2010) and another provided teacher-reported externalising behaviours (Adelman, 1990).
Of the 11 studies using a post-intervention outcome measure, 4 were direct therapeutic interventions for children of substance misusing parents aged >5 but ≤13 years (Davis-Susser, 1990; dos Reis Viela et al., 2016; Haight et al., 2010; Scheer, 1996), and were meta-analysed separately to the other 7 studies which did not integrate a child-focused treatment component. Instead, these 7 studies were focused on parent wellbeing, parental substance misuse, parenting skills or a combination of these foci (Brown et al., 2021; Guo et al., 2016; Kim et al., 2019; Lam et al., 2008; Maguin, 1991; Mitrani et al., 2010; Stanger et al., 2011).
One of the child-focused studies could not be combined with the other 3 child-focused studies (dos Reis Viela et al., 2016) because the authors reported the number of children scoring in the clinical range for externalising problems rather than mean scores like the other three studies. The remaining 3 studies (Davis-Susser, 1990; Haight et al., 2010; Scheer, 1996) were meta-analysed with results indicating that child externalising problems, as reported by parents, did not differ between children who participated in a psychosocial treatment versus those that did not (see Figure 14; n = 85; SMD = 0.22, 95% CI −0.24, 0.67). There was no detected heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 0.51, df = 2, p = 0.78; I2 = 0%). For the dos Reis Viela et al. (2016) study, children engaged with the school-based intervention model treatment aiming to prevent substance use in children of substance misusing parents were less likely to obtain a score in the clinical range for externalising problems compared to children not engaged in TAU (n = 101; OR = 0.29, 95% CI 0.12 to 0.68).
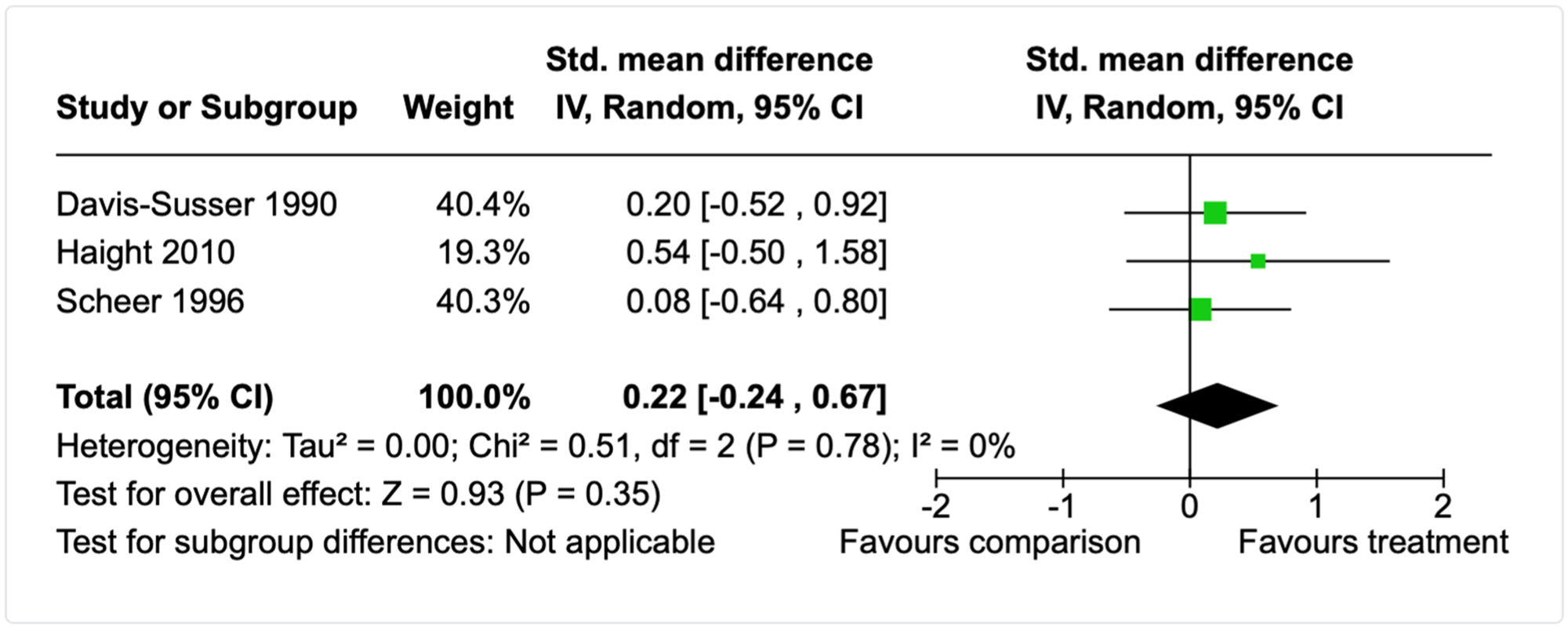
Forest plot for externalising problems meta-analysis (post-intervention, child-focused interventions, parent-report).
Likewise, the meta-analysis of the 7 parent-focused studies (see Figure 15) found that child externalising problems did not differ between parents who engaged with a psychosocial treatment compared to TAU or no treatment (n = 281; SMD = 0.17, 95% CI −0.07, 0.41). There was no detected heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 4.53, df = 6, p = 0.61; I2 = 0%). For the Lam et al. (2008) study, female partners of the alcohol misusing fathers also completed the same measure for child externalising problems. The results suggested no differences between the psychosocial treatment that integrated individual treatment for fathers with parent-focused intervention with female partners compared to TAU (n = 20; SMD = 0. 37, 95% CI −0.51 to 1.26).
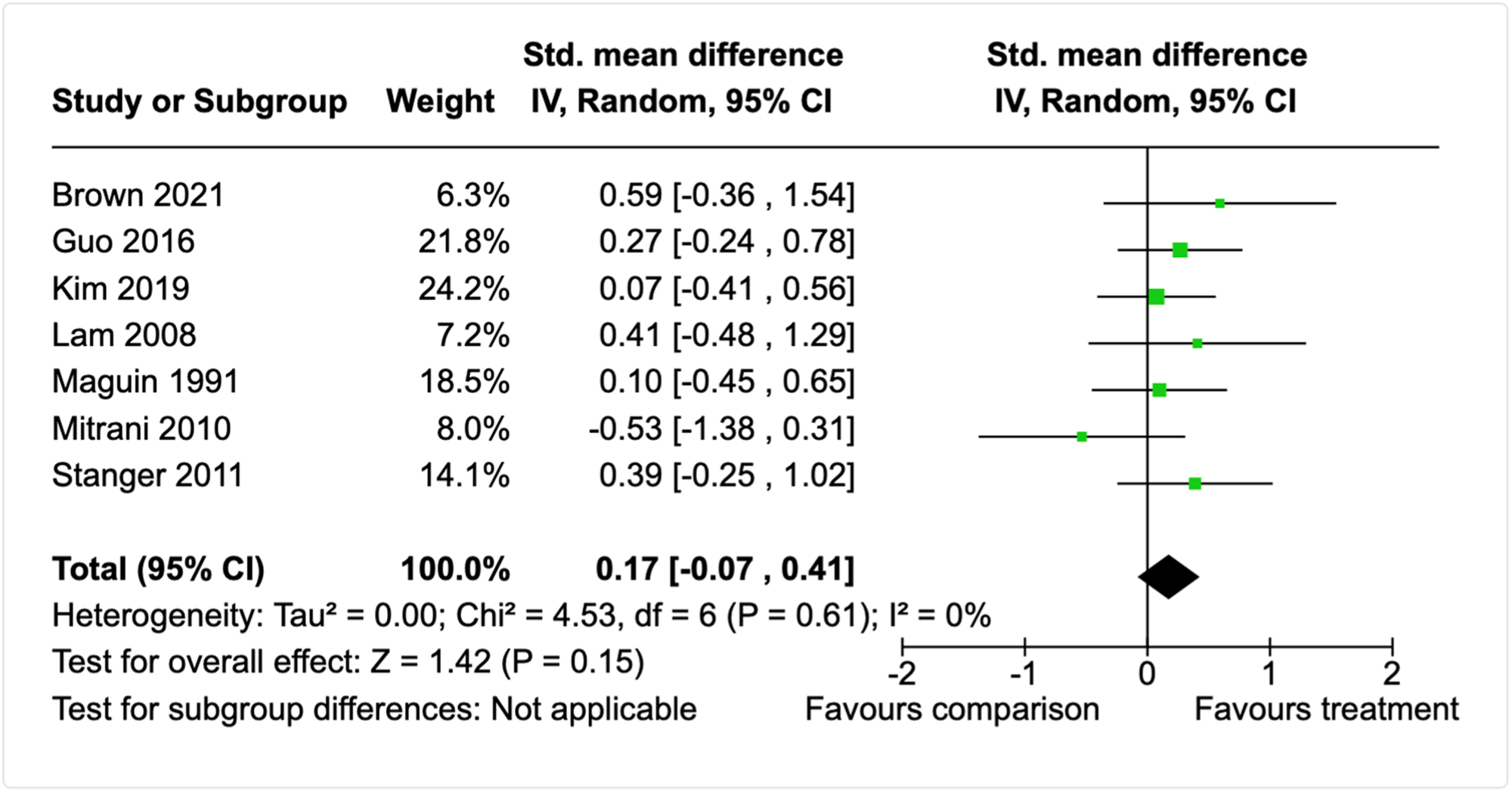
Forest plot for externalising problems meta-analysis (post-intervention, parent-focused interventions, parent-report).
Three studies tracked parent-reported externalising behaviour at short-term follow-up, approximately >3 months but ≤6-months after treatment completion. Mitrani et al. (2010) examined the impact of a family-focused Structural Ecosystems Therapy for substance misusing mothers with HIV. Guo et al. (2016) examined the effectiveness of supplementing housing with Ecologically-Based Treatment for homeless substance-misusing mothers. Lam et al. (2008) examined the impact of a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training. A meta-analysis of these studies (see Figure 16) found no differences in externalising problems between the intervention and TAU children at short-term follow-up (n = 101; SMD = 0.18, 95% CI −0.23 to 0.58). There was no detected heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 0.28, df = 2, p = 0.87; I2 = 0%). For the Lam et al. (2008) study, female partner reports suggested no differences in child externalising problem at short-term follow-up between the treatment compared to TAU (n = 20; SMD = 0.44, 95% CI −0.45 to 1.33). Mitrani et al. (2010) also included a child-report measure of externalising behaviours and there were no differences between groups at post-intervention (n = 24; SMD = −0.81, 95% CI −1.68 to 0.05) or short-term follow-up (n = 21; SMD = −0.23, 95% CI −1.24 to 0.77).
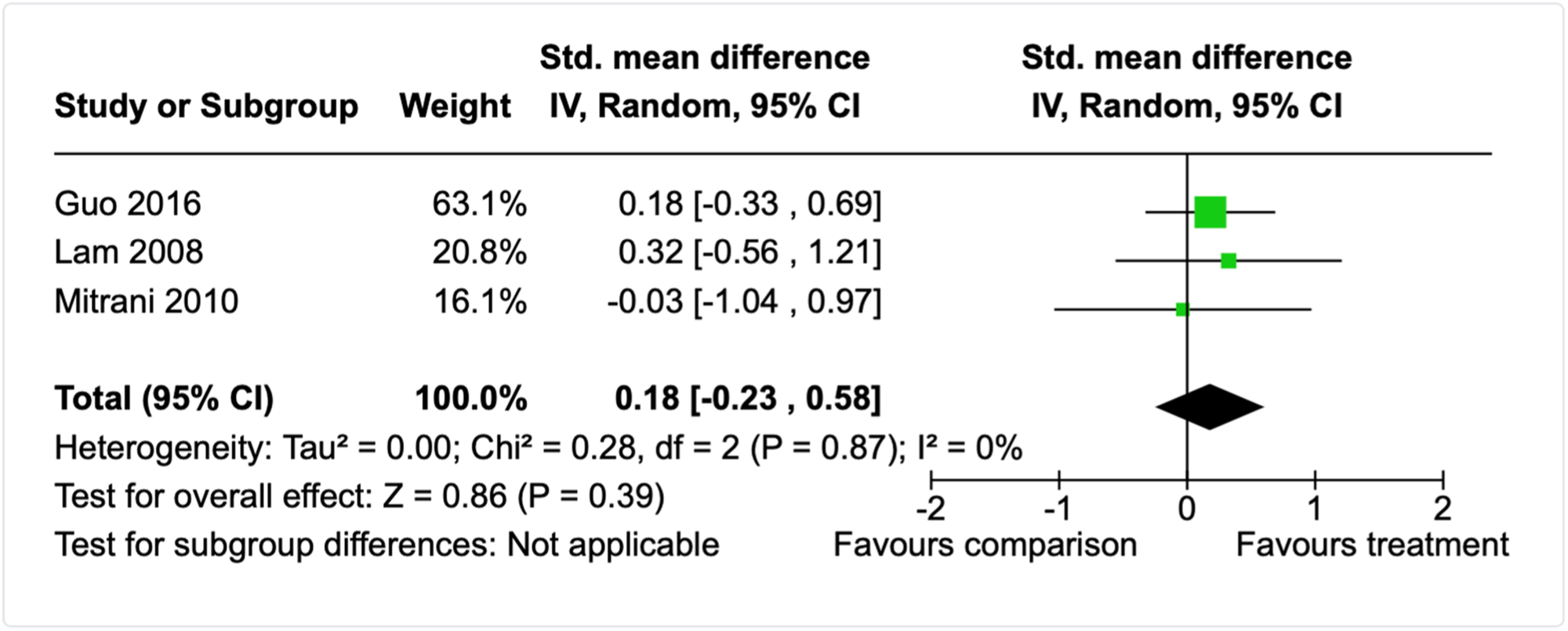
Forest plot for externalising problems meta-analysis (short follow-up, parent-focused interventions, parent-report).
Five studies also included a longer-term follow-up ≥6-months after a psychosocial treatment (Butz et al., 2001; Lam et al., 2008; Maguin, 1991; Mitrani et al., 2010; Sullivan, 1984). All but one study (Lam et al., 2008) examined the effectiveness of interventions that included both child and parent involvement, and integrated one or more components focused on parent-wellbeing, parenting, child health and development, child psychological wellbeing, and/or overall family functioning. None included a case management, legalistic, or child welfare component. A meta-analysis of these 4 conceptually similar studies (see Figure 17) indicated that child externalising problems, as reported by parents, did not differ for participants who engaged in a psychosocial treatment versus those who received TAU (n = 208; SMD = −0.07, 95% CI −0.55, 0.41). However, there was statistically significant and moderate heterogeneity among the effect sizes (τ 2 = 0.14; χ 2 = 7.77, df = 3, p = 0.05; I2 = 61%). A single effect size for the Lam et al. (2008) study (see above) suggested no differences in externalising problems – as reported by participating fathers – between the intervention and TAU children at the 12-month follow-up point (n = 20; SMD = 0.40, 95% CI −0.48 to 1.29). There was also no difference between intervention and TAU children when the mother was the respondent (n = 20; SMD = 0.34, 95% CI −0.55 to 1.22).
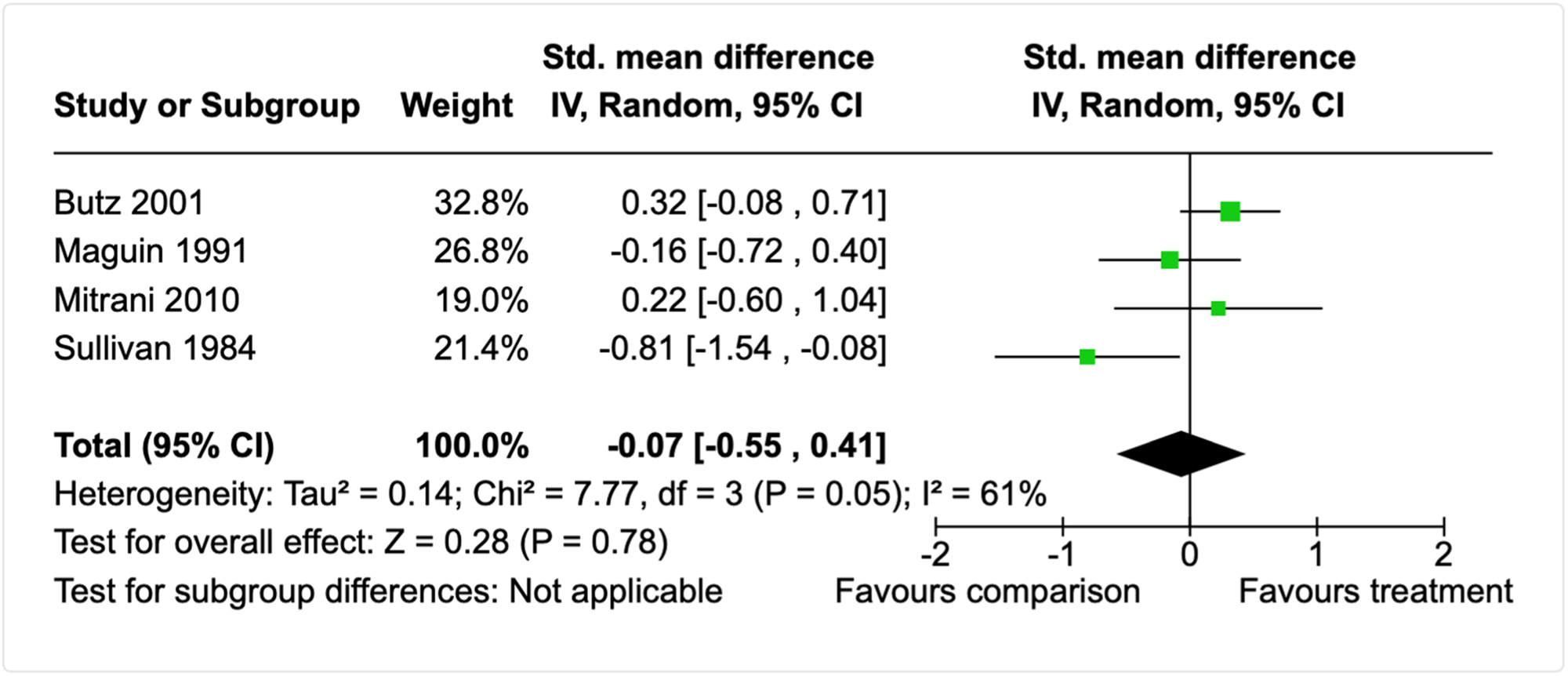
Forest plot for externalising behaviours meta-analysis (long follow-up, parent-report).
Mitrani et al. (2010) also included a child-report measure of externalising behaviours and there were no differences between groups at long-term follow-up (n = 25; SMD = 0.13, 95% CI −0.68 to 0.95). A single study compared child externalising difficulties 18-months after treatment for NAS with either methadone or morphine (Flannery et al., 2020). The effect size for this study indicated no differences between the alternate treatments (n = 77; SMD = −0.03, 95% CI −0.48 to 0.42).
As there were too few studies to conduct subgroup analyses, we first assessed the 4 studies on the a priori moderators to identify any clear outliers or categories among the studies. All studies used either well-validated standardised measure or a measure with associated psychometric data to establish its reliability and validity. All interventions were implemented by clinicians, mostly with postgraduate training. Two studies only reported information on parental alcohol misuse (Maguin, 1991; Sullivan, 1984) but did not appear to exclude those using drugs, whereas the other two reported polysubstance use for parents (Butz et al., 2001; Mitrani et al., 2010). The intervention was implemented in the home for 1 study (Butz et al., 2001), but in a mixture of what appeared to be community settings for the other 3 studies (Maguin et al., 1991; Mitrani et al., 2010; Sullivan, 1984). In terms of child age, 3 studies included children over the age of 3 years (Maguin et al., 1991; Mitrani et al., 2010; Sullivan, 1984), yet the same study that was set in the home, also differed from the other 3 studies by including children only from birth (Butz et al., 2001). Removal of this study from the meta-analysis slightly increased the precision of the meta-analysis (n = 109; SMD = −0.26, 95% CI −0.80 to 0.28), but only slightly reduced heterogeneity (τ 2 = 0.10; χ 2 = 3.64, df = 2, p = 0.16; I2 = 45%).
We then proceeded to examine other features of the studies, including the research design, study populations, and characteristics of the interventions. We identified that one of the studies was a non-randomised study and also implemented an intervention of a much shorter duration than the other three studies (Sullivan, 1984). Removal of this study from the meta-analysis increased the precision of the meta-analysis (n = 176; SMD = 0.17, 95% CI −0.13 to 0.46) and substantially reduced heterogeneity (τ 2 = 0.00; χ 2 = 1.91, df = 2, p = 0.38; I2 = 0%). These sensitivity analyses suggest the heterogeneity in effect sizes for child externalising problems may be due to the nature of the evaluation methodology, age of the children involved, and/or features of the specific intervention approach.
Four studies also reported results for individual subscales that comprised the externalising composite from the Child Behaviour Checklist (CBCL) (Butz et al., 2001; Claussen et al., 2004; Kim et al., 2019) or other measures (Personality Inventory for Children; Sullivan, 1984). Butz et al. (2001) used a version of the CBCL for younger children which uses an aggressive and a destructive subscale to make up the externalising composite. At the post-intervention time-point (6 to 18-months after treatment completion), 3-year-old children of parents who engaged with a home-visiting intervention did not differ from parents who received TAU on aggressive behaviour (n = 100; SMD = 0.36, 95% CI −0.03 to 0.76) or destructive behaviour (n = 100; SMD = 0.12, 95% CI −0.27 to 0.52). Kim et al. (2019) used a version of the CBCL for older children which uses an aggressive and a rule-breaking subscale to make up the externalising composite. The rule-breaking subscale results are reported in the ‘Antisocial behaviour’ subsection below. On the aggression subscale at post-intervention, there was no difference between children of parents who participated in a Solutions Focused Behavioural Therapy intervention comprised of weekly individual parent sessions over the course of approximately 3-months versus those who received TAU (n = 67; SMD = 0.02, 95% CI −0.46 to 0.51). Similarly, the single study that compared a centre- or home-based child development intervention (described above, Claussen et al., 2004; n = 96) found that, at post-intervention, children did not differ on parent-rated destructive behaviours (SMD = −0.10, 95% CI −0.50, 0.30); aggressive behaviours (SMD = −0.18, 95% CI −0.58, 0.22); or disruptive behaviours (SMD = −0.36, 95% CI −0.76, 0.05). Sullivan (1984) examined the effectiveness of a therapeutic intervention for alcoholic parents compared to no treatment at 8-months follow-up. The intervention comprised 6 parent group therapy sessions, 6 child group therapy sessions, and 6 family therapy sessions focused on psychoeducation and supportive psychotherapy. There were no differences in the level of parent-reported levels of child aggression after participating in the intervention compared to the no treatment control group (n = 33; SMD = 0.64, 95% CI −0.08 to 1.36).
The single study using a teacher-report measure (Adelman, 1990) examined whether participating in a therapeutic group in the school setting impacted overall teacher-reported externalising behaviour (aggression) for children with alcohol misusing parents. At post-intervention children engaging with this intervention did not differ from children who did not (n = 44; SMD = 0.13, 95% CI −0.46 to 0.73).
Internalising
Fourteen studies examined the effectiveness of treatment using parent-, child-, or teacher-report - standardised measures that produce a composite for child internalising problems. Two studies had missing data, by either reporting no between group data or only data for participants with scores over a particular threshold on the outcome measure (Bartle-Haring et al., 2018; Margolis et al., 2017). Nine studies compared an eligible intervention to a TAU comparison condition at post-intervention only, 3 studies included both a post-intervention and short-term follow-up (≥3 months ≤6-months), and 4 studies also included a longer follow-up (>6-months ≤12-months). An additional two studies compared alternative treatments (Claussen et al., 2004; Flannery et al., 2020; described above). Further, two studies provided both a child- and parent-report measure of internalising problems (Luthar et al., 2007; Mitrani et al., 2010). However, only one of these reported sufficient data to calculate effect sizes (Mitrani et al., 2010).
Similar to externalising behaviours, 3 of the 9 studies using a post-intervention outcome measure were direct therapeutic interventions for children of substance misusing parents aged >5 but ≤10 years (Haight et al., 2010; Scheer, 1996; dos Reis Viela et al., 2016). These were analysed separately to the other 6 studies which did not integrate a child-focused treatment component described above (Brown et al., 2021; Guo et al., 2016; Kim et al., 2019; Lam et al., 2008; Mitrani et al., 2010; Stanger et al., 2011). The meta-analysis of the 2 child-focused studies indicated that child internalising problems, as reported by parents, did not differ between children who participated in a psychosocial treatment versus those that did not (n = 45; SMD = 0.15, 95% CI −0.54, 0.84). There was minimal detected heterogeneity among the effect sizes (τ 2 = 0.06; χ 2 = 1.29, df = 1, p = 0.26; I2 = 23%). For the dos Reis Viela et al. (2016) study, children engaged with the school-based intervention model treatment aiming to prevent substance use in children of substance misusing parents were less likely to obtain a score in the clinical range for internalising problems compared to children not engaged in TAU (n = 101; OR = 0.15, 95% CI 0.06 to 0.39).
The meta-analysis of the 6 parent-focused studies (see Figure 18) found that child externalising problems did not differ between parents who engaged with a psychosocial treatment compared to TAU or no treatment (n = 220; SMD = 0.16, 95% CI −0.10, 0.43). There was no detected heterogeneity among the effect sizes (τ 2 = 0.00; χ 2 = 3.75, df = 5, p = 0.59; I2 = 0%). For the Lam et al. (2008) study, female partners of the alcohol misusing fathers also completed the same measure for child internalising problems. The results suggested no differences between the psychosocial treatment that integrated individual treatment for fathers with parent-focused intervention with female partners compared to TAU (n = 20; SMD = 0.39, 95% CI −0.50 to 1.26).
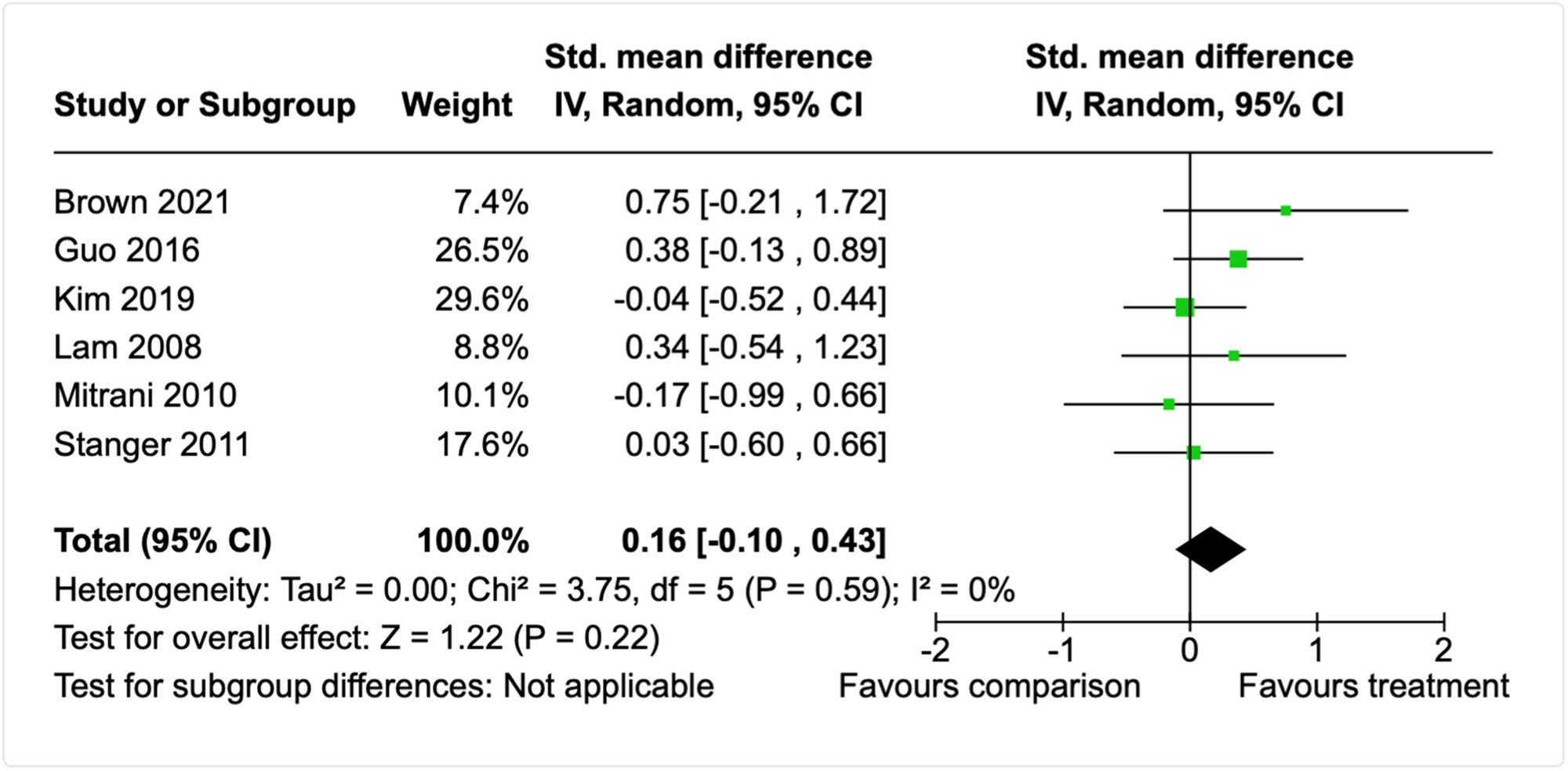
Forest plot for internalising behaviours meta-analysis (post-intervention, parent-report).
Three studies—described in the previous section—tracked parent-reported internalising behaviour at short-term follow-up (Guo et al., 2016; Lam et al., 2008; Mitrani et al., 2010). A meta-analysis of these studies (Figure 19) found no differences in internalising problems between the intervention and TAU participants at short-term follow-up (n = 101; SMD = 0.23, 95% CI −0.17 to 0.65). For the Lam et al. (2008) study, female partner reports suggested no differences in child internalising problem at short-term follow-up between the treatment compared to TAU (n = 20; SMD = 0.33, 95% CI −0.55 to 1.22). Mitrani et al. (2010) also included a child-report measure of internalising behaviours and there were no differences between groups at post-intervention (n = 24; SMD = −0.51, 95% CI −1.36 to 0.33) or short-term follow-up (n = 21; SMD = −0.22, 95% CI −1.23 to 0.79).
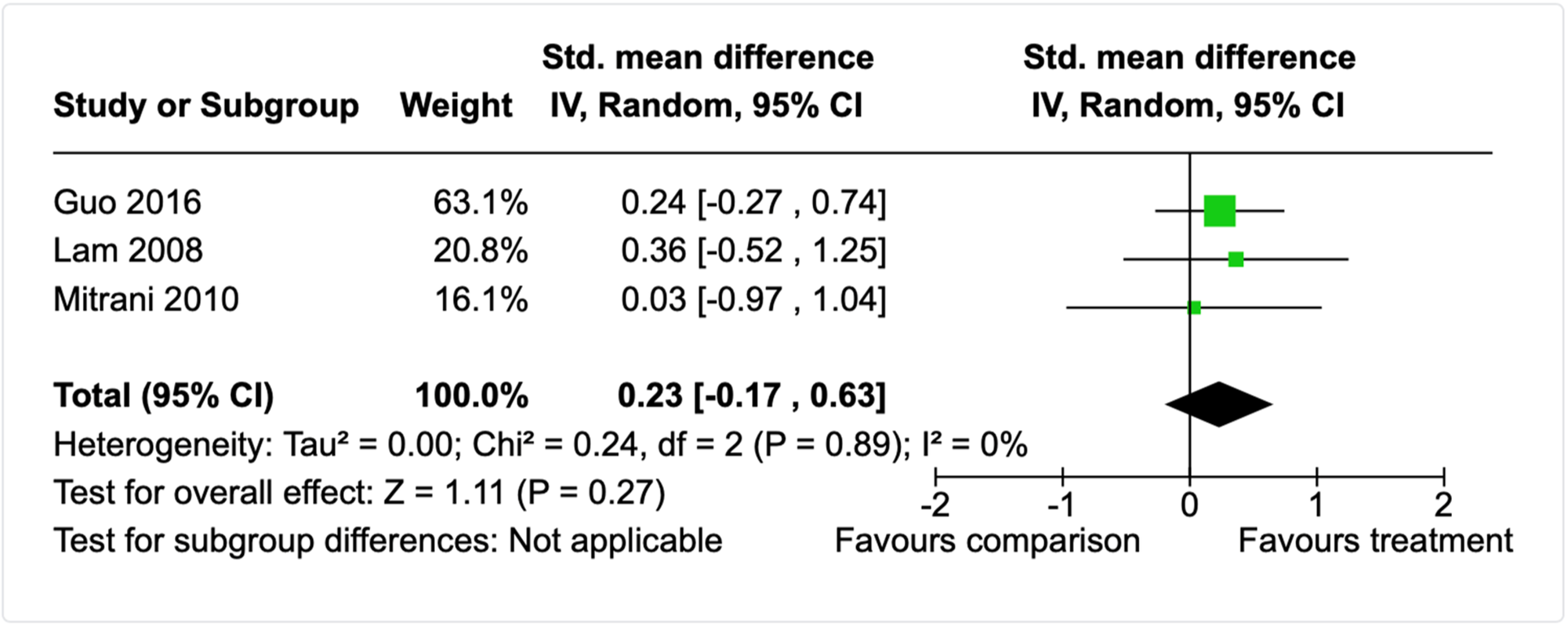
Forest plot for internalising behaviours meta-analysis (short follow-up, parent-report).
Four studies also included a longer-term follow-up ≥6-months after a psychosocial treatment (Butz et al., 2001; Lam et al., 2008; Mitrani et al., 2010; Sullivan, 1984). All but one study (Lam et al., 2008) examined the effectiveness of interventions that included both child and parent involvement, and integrated one or more components focused on parent-wellbeing, parenting, child health and development, child psychological wellbeing, and/or overall family functioning. None included a case management, legalistic, or child welfare component. A meta-analysis of the 3 conceptually similar studies (see Figure 20) indicated that child internalising problems, as reported by parents, did not differ for participants who engaged in a psychosocial treatment versus those who received TAU (n = 158; SMD = −0.10, 95% CI −0.93, 0.74). Similar to the externalising meta-analysis which also contained these studies, there was statistically significant and high heterogeneity among the effect sizes (τ 2 = 0.43; χ 2 = 10.02, df = 2, p = 0.0007; I2 = 80%). As there were too few studies to conduct subgroup analyses, we assessed the 3 studies on the a priori moderators to identify any clear outliers or categories among the studies. All studies used either well-validated standardised measure or a measure with associated psychometric data to establish its reliability and validity. All interventions were implemented in similar settings in the United States by clinicians usually with postgraduate training. Removal of the one study that was a quasi-experiment (Sullivan, 1984) increased the effect size and changed the direction to favouring treatment, and also reduced the confidence intervals and heterogeneity (n = 125; SMD = 0.31, 95% CI −0.05, 0.66; τ 2 = 0.00; χ 2 = 0.07, df = 1, p = 0.79; I2 = 0%). A single effect size for the Lam et al. (2008) study, which examined the impact of a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training suggested no differences in internalising problems between the intervention and TAU children at the 12-month follow-up point (n = 20; SMD = 0.34, 95% CI −0.54 to 1.23). There was also no difference between intervention and TAU children when the mother was the respondent (n = 20; SMD = 0.37, 95% CI −0.40 to 1.15).
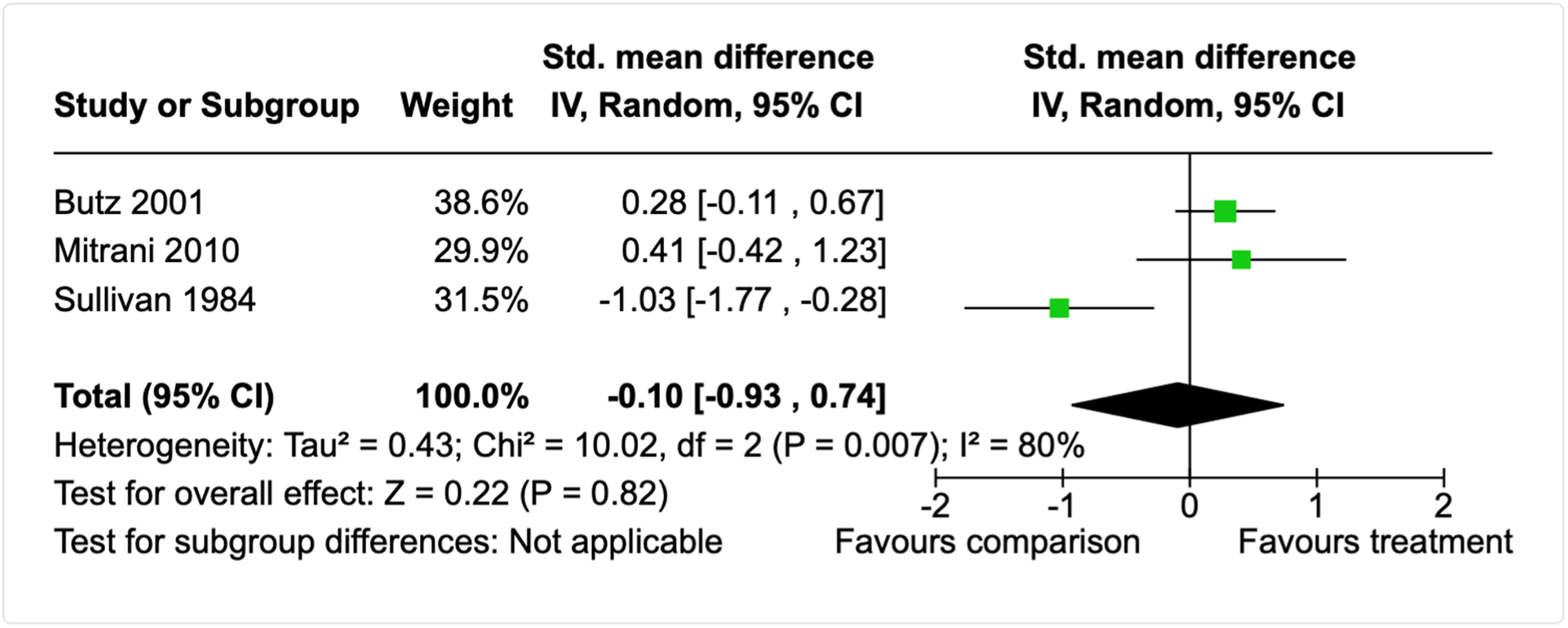
Forest plot for internalising behaviours meta-analysis (long follow-up, parent-report).
Three studies also reported results for specific internalising behaviour subscales that contribute to the internalising composite from the CBCL (Butz et al., 2001; Claussen et al., 2004; Kim et al., 2019) or the Personality Inventory for Children (Sullivan, 1984). At the post-intervention time-point (6 to 18-months after treatment completion), 3-year-old children of parents who engaged with a home-visiting intervention (Butz et al., 2001) differed from parents who received TAU on withdrawn behaviour (n = 100; SMD = 0.51, 95% CI 0.11 to 0.91), but not on anxious-depressed behaviour (n = 100; SMD = 0.35, 95% CI −0.04 to 0.75) or somatic complaints (n = 100; SMD = 0.15, 95% CI −0.24 to 0.54). Similarly, the study that compared a centre- or home-based child development intervention (described above, Claussen et al., 2004; n = 96) found that, at post-intervention, children did not differ on parent-rated anxious-depressed behaviours (SMD = 0.06, 95% CI −0.34, 0.46) withdrawn behaviours (SMD = −0.08, 95% CI −0.48, 0.32), or somatisation (SMD = 0.04, 95% CI −0.36, 0.44). Likewise, Kim et al. (2019) found that older children of parents who engaged with a Solution Focused Behavioural Therapy for substance misusing parents did not differ to children of parents assigned to TAU at post-intervention on withdrawn-depressive behaviours (n = 67; SMD = 0.02, 95% CI −0.47 to 0.50), anxious-depressive behaviours (n = 67; SMD = −0.03, 95% CI −0.52 to 0.45), or somatic complaints (n = 67; SMD = −0.08, 95% CI −0.59 to 0.43). Sullivan (1984) examined the effectiveness of a therapeutic intervention for alcoholic parents compared to no treatment at 8-months follow-up. The intervention comprised 6 parent group therapy sessions, 6 child group therapy sessions, and 6 family therapy sessions focused on psychoeducation and supportive psychotherapy. There were no differences in the level of parent-reported somatic concerns in their children (n = 33; SMD = −0.12, 95% CI −0.82 to 0.58) after participating in the intervention compared to the no treatment control group. However, there were higher levels of somatisation overall in the treatment versus control group (n = 33; SMD = 0.99, 95% CI 0.24 to 1.73).
Mitrani et al. (2010) also included a child-report measure of internalising behaviours and there were no differences between groups at long-term follow-up (n = 25; SMD = 0.01, 95% CI −0.74 to 0.27). A single study compared child internalising difficulties 18-months after treatment for NAS with either methadone or morphine (Flannery et al., 2020). The effect size for this study indicated no differences between the alternate treatments (n = 77; SMD = 0.02, 95% CI −0.42 to 0.47).
Prosocial behaviour
Four studies evaluated the impact of psychosocial interventions using a parent-report measure of child prosocial behaviours compared to either a TAU comparison condition (Dawe et al., 2007; Maguin, 1991; Margolis et al., 2017) or an alternate treatment (Claussen et al., 2004, described above). Margolis et al. (2017) did not report sufficient data to calculate effect sizes and also combined child- and parent-report measures into their summary statistics for their measure of prosocial behaviours. Maguin (1991) recruited alcohol misusing fathers and their spouses to evaluate an intervention that combined parent-skills training with couples-based therapy focused on substance misuse, parent wellbeing, and relationships issues. Dawe et al. (2007) recruited parents from methadone clinics to evaluate a comprehensive home-based intervention that integrated components focused on parental substance misuse, parental wellbeing (e.g., emotion regulation and mindfulness), parenting skills, quality of the caregiving relationship, and overall family functioning. Both studies also integrated case management. A meta-analysis of these two studies found that children of parents receiving integrated psychosocial interventions were observed to display more prosocial behaviours than children whose parents received TAU at post-intervention (n = 92; SMD = 0.47, 95% CI 0.06 to 0.89). This effect was not maintained at 6-month follow-up (n = 92; SMD = 0.57, 95% CI −0.16 to 1.30) and there was nonsignificant and moderate heterogeneity among the effect sizes (τ 2 = 0.18; χ 2 = 2.91, df = 1, p = 0.09; I2 = 66%).
Antisocial behaviour
Eight studies included a measure of antisocial behaviour to evaluate psychosocial interventions (Catalano et al., 1999; Davis-Susser, 1990; Kim et al., 2019; Logan et al., 2001; Maguin, 1991; Peitler, 1980; Ryan et al., 2016; Sullivan, 1984), with all but four (Catalano et al., 1999; Logan et al., 2001; Ryan et al., 2016; Peitler, 1980) using parent-report instruments. Three studies did not report sufficient data to calculate effect sizes (Logan et al., 2001; Peitler, 1980; Ryan et al., 2016).
The study using the child-report measure (Catalano et al., 1999) examined the effectiveness of the Focus on Families intervention, an intensive 9-month family-focused intervention integrating home-based case management with weekly parent groups focused on parental substance misuse, parenting skills, emotion regulation, and strategies for preventing child substance misuse. Children also attended 12 of the 32 group sessions to facilitate skills practice. Children participating in Focus on Families did not differ from children receiving TAU on a 9-item scale measuring self-reported delinquency at the 6-month follow-up (n = 104; SMD = 0.34, 95% CI −0.05 to 0.73) or the 12-month follow-up (n = 100; SMD = 0.15, 95% CI −0.25 to 0.55).
The four studies with parent-report antisocial behaviour measures used measures of delinquency or antisocial behaviours that varied in seriousness. One reported a rule-breaking subscale from a standardised measure of child behavioural problems (Kim et al., 2019), another constructed a composite of delinquent behaviours from a range of standardised measures (Maguin, 1991), another reported a delinquency subscale from a comprehensive standardised measure of childhood personality features (Sullivan, 1984), and the final study (Davis-Susser, 1990) used a Conduct Disorder subscale from a validated measure (Revised Behaviour Problem Checklist). The study using the rule-breaking subscale (Kim et al., 2019) found no difference between those who participated in a Solutions Focused Behavioural Therapy intervention comprised of weekly individual parent sessions over the course of approximately 3-months versus those who received TAU (n = 67; SMD = 0.13, 95% CI −0.35 to 0.61). Similarly, the study using the composite (Maguin, 1991) found no difference in parent-reported child delinquent behaviours between those who received no treatment and those who participated in combined parent-skills training with couples-based therapy focused on substance misuse, parent wellbeing, and relationships issues (n = 51; SMD = 0.09, 95% CI −0.46 to 0.64). This study also included a follow-up measure that aligned with the follow-up measure of Sullivan (1984) (the post-intervention data was not reported for this study). This third study, which used the subscale from the standardised personality measure (Sullivan, 1984) evaluated a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions. A meta-analysis of these 2 studies indicated that parent-reported childhood delinquency does not differ between participants who receive no intervention versus those who engage with psychosocial interventions comprised of parent and child components at 6–8 months follow-up (n = 83; SMD = −0.23, 95% CI −0.66 to 0.21; τ 2 = 0.00; χ 2 = 0.09, df = 1, p = 0.77; I2 = 0%). Davis-Susser (1990) examined the effectiveness of a child-focused group therapy programme and found that participating children did not differ in terms of conduct disorder symptoms compared to a control group not receiving therapy (n = 40; SMD = −0.30, 95% CI −1.02 to 0.42).
Substance use and related measures
Seven studies included a measure related to either child substance use (Bartle-Haring et al., 2018; Catalano et al., 1999; Gance-Cleveland et al., 2008; Logan et al., 2001) or knowledge and attitudes related to substance misuse (Broning et al., 2019; Larson, 1989; Sullivan, 1984). Three of these studies (Bartle-Haring et al., 2018; Gance-Cleveland et al., 2008; Logan et al., 2001) did not report sufficient data to permit effect size calculation at all (e.g., no between group outcome data or results of statistical tests to allow effect size calculation). Another of the studies did not report sufficient data to permit effect size calculation at 6- and 12-month follow-up (Catalano et al., 1999), but sufficient data at a 5-year follow-up. This study evaluated the Focus on Families intervention (see above) and found that the odds of having any type of substance abuse or dependence diagnosis did not differ between treatment and comparison conditions (see Table 9).
In relation to the studies examining child knowledge and/or attitudes about substance misuse, one found that children who engaged with the parent-child-family intervention (see previous section, Sullivan, 1984) did not differ on their self-reported knowledge and attitudes about substance use upon treatment completion (n = 33; SMD = −0.58, 95% CI −1.30 to 0.13) or approximately 8-months later (n = 33; SMD = −0.37, 95% CI −1.07 to 0.34). The remaining studies evaluated child-focused interventions. Broning et al. (2019) evaluated a group resilience programme for substance misusing parents (alcohol and drugs) and Larson (1989) evaluated a group psychodrama intervention for children of alcohol misusing parents. A meta-analysis of these studies indicated that children self-reported higher levels of knowledge about substance misuse upon treatment completion (n = 197; SMD = 0.78, 95% CI 0.46 to 1.05; τ 2 = 0.00; χ 2 = 0.38, df = 1, p = 0.54; I2 = 0%). Based on the Broning et al. (2019) study only, this effect was maintained approximately 6-months later (n = 176; SMD = 0.46, 95% CI 0.15 to 0.76).
Anxiety
Seven studies included a measure of child anxiety to evaluate psychosocial interventions with either a teacher-report measure (Adelman, 1990), parent-report measures (Bartle-Haring et al., 2018; Pirnia et al., 2017a, 2017b; Sullivan, 1984), child-report measures (Lam et al., 2008; Scheer, 1996), or a mixture of both (Davis-Susser, 1990). Two studies did not report between-groups effect size data or results of statistical tests that could be used to calculate an effect size (Bartle-Haring et al., 2018; Prinia et al., 2017b).
The single study using a teacher-report measure (Adelman, 1990) examined whether participating in a therapeutic group in the school setting impacted overall teacher-reported anxiety for children with alcohol misusing parents. At post-intervention children engaging with this intervention did not differ from children who did not (n = 44; SMD = −0.10, 95% CI −0.70 to 0.49). Two of the three studies utilising a child-report measure examined the effectiveness of child-focused group therapy programmes compared to control groups not receiving therapy (Davis-Susser, 1990; Scheer, 1996), and a meta-analysis of these studies found that there were no differences between groups (n = 70; SMD = −0.44, 95%CI −0.95 to 0.08), with no heterogeneity detected (τ 2 = 0.00; χ 2 = 0.02, df = 1, p = 0.90; I2 = 0%). The third study using a child-report measure (Lam et al., 2008) examined the impact of a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training. Single effect sizes suggested no differences in child-reported anxiety between intervention and TAU children at the post-intervention (n = 20; SMD = 0.51, 95% CI −0.38 to 1.40), 6-month follow-up (n = 20; SMD = 0.47, 95% CI −0.42 to 1.36), or 12-month follow-up points (n = 20; SMD = 0.48, 95% CI −0.41 to 1.37).
The 3 studies using parent-report measures of child anxiety could not be combined with meta-analysis due to conceptually different interventions and comparison conditions. As such, single effect sizes for each study are presented here and in Table 9. One study compared alternate treatments (Pirnia et al., 2017a) and found that, at post-intervention, child anxiety (as rated by parents) did not differ for mother-child dyads who participated in either a CBT group programme versus a Parent-Child Interaction Therapy (PCIT) intervention targeting high-potency cannabis users (n = 50, SMD = −0.44, 95% CI −1.00, 0.12). Although a waitlist control group was included in this study, the data for these participants was not reported to allow for a comparison between the treatments and the waitlist control participants. Sullivan (1984) evaluated a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions and found that those engaged in treatment did not differ from those receiving no treatment on parent-rated anxiety approximately 8-months post treatment completion (n = 33; SMD = −0.54, 95% CI −1.25 to 0.17). Likewise, Davis-Susser (1990) found no difference in parent-rated anxiety for children who participated in a group therapy programme for children of alcoholics compared to children receiving no treatment (n = 40; SMD = −0.28, 95% CI −1.00 to 0.44).
Depression
Twelve studies included a measure of child depression behaviour to evaluate psychosocial interventions. One study used a parent-report instrument (Sullivan, 1984) and 11 used child-report instruments. Six of the studies using child-report instruments either did not report outcome data for the depression measure or did not report sufficient data to calculate effect sizes (Bartle-Haring et al., 2018; Gance-Cleveland et al., 2008; Logan et al., 2001; Luthar et al., 2007; Peitler, 1980; Roosa et al., 1990). Four of the remaining five studies with a child-report measure of depression were all child-focused group psychosocial interventions (Adelman, 1990; Davis-Susser, 1990; Hyun et al., 2010; Scheer, 1996). However, Adelman (1990) used a measure of hopelessness (symptom of depression), whereas the other 3 studies used validated measures of multiple depressive symptoms. A meta-analysis of these 3 studies indicated symptoms of depression did not differ for children participating in a child-focused group therapy compared to children not receiving treatment (Figure 21; n = 98; SMD = −0.34, 95% CI −1.27 to 0.59). Substantial heterogeneity was detected between effect sizes (τ 2 = 0.53; χ 2 = 9.16, df = 2, p = 0.001; I2 = 78%) and the only difference between the studies based on a priori moderators was that the study by Hyun et al. (2010) was conducted in Korea with only males, and was slightly longer in duration (10-weeks vs. 8-weeks for the other 2 studies). A sensitivity analysis removing this study found that symptoms of depression were significantly lower for children participating in a child-focused group therapy compared to children not receiving treatment (n = 70; SMD = −0.77, 95% CI −1.48 to −0.05) and the heterogeneity between effect sizes reduced (τ 2 = 0.12; χ 2 = 1.81, df = 1, p = 186; I2 = 45%).
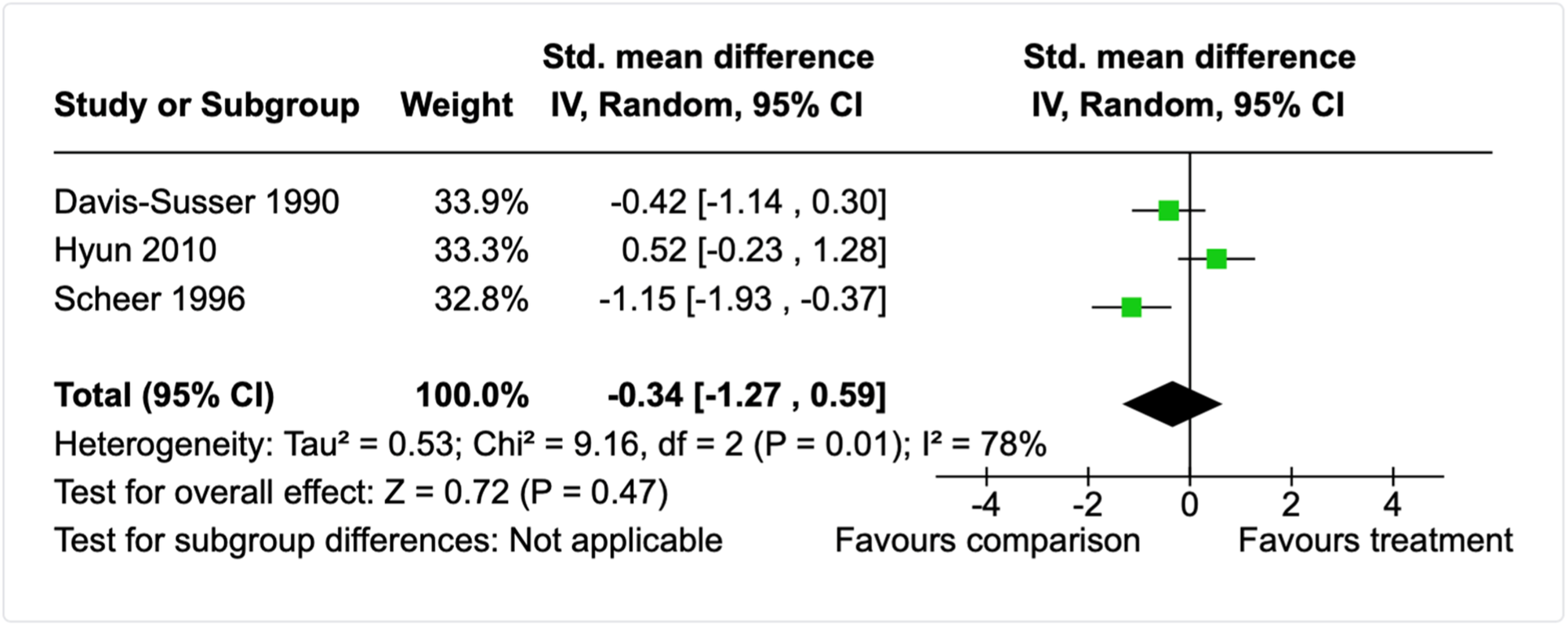
Forest plot for depressive symptoms meta-analysis (post-intervention, child-report).
Adelman (1990) found that children engaging with a school-based group therapeutic intervention had higher levels of hopelessness compared to children who did not participate (n = 44; SMD = −0.61, 95% CI −1.22 to 0.00). The remaining study using a child-report measure (Lam et al., 2008) examined the impact of a parent-focused intervention comprised of individual therapy for fathers with children aged 8–12 years and behavioural couples therapy for their female partner that integrated parent-skills training. Single effect sizes suggested no differences in child-reported depressive symptoms between intervention and TAU children at the post-intervention (n = 20; SMD = 0.55, 95% CI −0.35 to 1.45), 6-month follow-up (n = 20; SMD = 0.54, 95% CI −0.36 to 1.43), or 12-month follow-up point (n = 20; SMD = 0.51, 95% CI −0.39 to 1.40).
In relation to the studies with a parent-report measures, one study (Sullivan, 1984) found that child depressive symptoms were lower for those receiving no treatment and those who participated in a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions (n = 33; SMD = −0.81, 95% CI −1.53 to −0.08).
Trauma
Only one study reported a child trauma outcome measure. With a small RCT, Haight et al. (2010) examined the effectiveness of individual narrative-informed therapy with children affected by parental substance misuse. At post-intervention, children receiving treatment did not differ from children in a waitlist control group on a parent-report measure of child trauma symptoms (n = 15; SMD = 0.00, 95% CI −1.01 to 1.01).
Socioemotional functioning
Eight studies included measures of child socioemotional functioning or competencies, with 4 studies including child-report measures (Adelman, 1990; Broning et al., 2019; Luthar & Suchman, 2000; Roosa et al., 1990), three including parent-report measures (Barlow et al., 2019; dos Reis Viela et al., 2016; Finkelstein et al., 2005), and one including a child-, parent-, and teacher-reported versions of the same measure (Orte et al., 2008). Only two studies reported sufficient data to permit effect size calculation (Adelman, 1990; dos Reis Viela et al., 2016). The studies with missing data had issues ranging from missing standard deviations or insufficient results of statistical tests to permit alternative avenues effect size calculation (e.g., Luthar & Suchman, 2007; Orte et al., 2008), or incomplete outcome data due to the measure not being appropriate to a large portion of the study sample due to child age (Barlow et al., 2019). The studies by Finkelstein et al. (2005) and Orte et al. (2008) are included under this outcome category, however, the measures used by the authors contain multiple composites meaning that if the complete data had been reported, these studies would likely be included under multiple outcome domains. Broning et al. (2019) provided data for other outcomes upon author contact but were unable to provide data for all requested outcomes.
The dos Reis Viela et al. (2016) study found no differences in the odds of scoring in the clinical range for caregiver-rated total competencies for children engaging with a school-based intervention model providing mental health support and a range of other preventative activities than children assigned to the control condition (n = 101; OR = 2.00, 95% CI 0.76 to 5.29). Adelman (1990) found that children engaging with a school-based group therapeutic intervention did not differ on overall self-reported adjustment compared to children who did not participate (n = 44; SMD = −0.43, 95% CI −1.03 to 0.17).
Mood, psychological wellbeing, emotion regulation, and symptoms of psychopathology
Nine studies reported miscellaneous measures of mood, child psychological wellbeing, emotion regulation and/or symptoms of psychopathology. Two of these studies reported insufficient data for calculating effect sizes (Gance-Cleveland et al., 2008; Pirnia, 2019).
Broning et al. (2019) compared the effectiveness of a child-focused group resilience programme (TRAMPOLINE) to a play-based educational attentional control condition and reported multiple outcomes using numerous outcomes, including general psychological wellbeing and physical stress symptoms. The authors were able to provide missing data to permit effect size calculation for physical stress symptoms. Children participating in the TRAMPOLINE intervention reported lower levels of physical stress symptoms compared to children who engaged the play-based attentional control activities at post-intervention (n = 181; SMD = 1.46, 95% CI 0.32, 2.60) and at 6-months follow-up (n = 172; SMD = 2.25, 95% CI 1.03 to 3.47). Pirnia et al. (2019) also provided a measure of stress (cortisol) to evaluate the impact of PCIT compared to no treatment in mother-child dyads, yet reported no outcome data to permit effect size calculation.
Two studies assessed the effectiveness of child-focused therapy groups using child-reported measures of happiness (Hojjat et al., 2015; Gance-Cleveland et al., 2008), however only one study reported sufficient data to permit effect size calculation. Hojjat et al. (2015) found that adolescents with substance misusing parents who participated in a group assertiveness training programme had higher overall levels of happiness (n = 57; SMD = 0.67, 95% CI 0.14 to 1.21).
Two studies assessed the effectiveness of child-focused therapy groups using child-reported measures of anger (Adelman, 1990; Hojjat et al., 2017). A meta-analysis of these studies indicated no difference in levels of state anger (intensity at point in time) between treated and untreated children (n = 104; SMD = 1.42, 95% CI −1.94 to 4.77; τ 2 = 5.73; χ 2 = 47.40, df = 1, p < 0.00001; I2 = 98%). Similarly, there was no difference in the levels of trait anger (predisposition towards anger) between treated and untreated children (n = 104; SMD = 1.39, 95% CI −2.15 to 4.93; τ 2 = 6.38; χ 2 = 51.70, df = 1, p < 0.00001; I2 = 98%). Both meta-analyses had significant heterogeneity. We examined this heterogeneity based on a priori moderators and found that the studies differed on age of the participants. Hojjat et al. (2017) finding a large effect size favouring the treatment for adolescent males, whereas Adelman (1990) found no differences between treated and untreated primary school children. Single effect sizes for the specific subscales of the validated anger scale reported in Adelman (1990) also indicated no differences between treated and untreated children (see Table 9).
Davis-Susser (1990) found that psychotic-related behaviours did not differ between children who participated in a child-focused group therapy intervention versus those who did not (n = 40; SMD = −0.09, 95% CI −0.80, 0.63). Likewise, Kim et al. (2019) found no differences between participants who received a parent-focused Solution Focused Behavioural Therapy (Kim et al., 2019) and TAU on parent-reported child thought problems (n = 67; SMD = −0.26, 95% CI −0.74 to 0.23). However, Sullivan (1984) found that children who engaged with a psychosocial intervention comprised of 6 child, 6 parent, and 6 family therapy sessions had lower psychosis symptomatology compared to children who received no treatment (n = 33; SMD = −1.08, 95% CI −1.83 to −0.33).
Isolation and social support
Three studies evaluated group psychosocial interventions for children of substance misusing parents using either a measure of child-report social support (Broning et al., 2019), child-reported loneliness (Dore et al., 1999), or teacher-reported problematic isolation behaviours. Broning et al. (2019) and Dore et al. (1999) did not report sufficient data to calculate effect sizes. Adelman (1990) found no differences on teacher-reported problematic isolation behaviours for children engaging with a school-based group therapeutic intervention versus children who did not participate (n = 44; SMD = −0.03, 95% CI −0.63 to 0.56).
Coping and resilience
Twelve studies evaluated predominantly child-focused psychosocial interventions using measures under the broad category of coping and resilience. Under this category of outcomes, we included assertiveness, self-esteem, self-worth, self-concept, self-efficacy, locus of control, resilience, coping behaviours, and measures explicitly labelled resilience by authors. Many of the studies in this category had missing data that precluded effect size calculation and/or meta-analysis.
Hojjat et al. (2015) found that adolescents with substance misusing parents who participated in a group assertiveness training programme had higher levels assertiveness (n = 57; SMD = 1.13, 95% CI 0.57, 1.69) compared to adolescents receiving no treatment. Four studies included measures of child-reported locus of control (Davis-Susser, 1990; Dore et al., 1999; Larson, 1989; Sullivan, 1984), yet one did not report data to permit effect size calculation (Dore et al., 1999). At 8-months follow-up Sullivan (1984) found that children who engaged with a psychosocial intervention comprised of 6 child, 6 parent, and 6 family therapy sessions did not differ from children who received no treatment on their self-reported locus of control (n = 33; SMD = −0.06, 95% CI −0.75 to 0.64). A meta-analysis of the two studies evaluating child-focused group therapy interventions (Davis-Susser, 1990; Larson, 1989) found that treated children who participated in a child-focused therapy group did not differ from children who received no treatment on their self-reported locus of control (n = 49; SMD = −0.27, 95% CI −0.91 to 0.37; τ 2 = 0.00; χ 2 = 0.18, df = 1, p = 0.67; I2 = 0%).
Six studies included child-report measures of self-concept (Adelman, 1990; Broning et al., 2019; Dore et al., 1999; Hyun et al., 2010; Scheer, 1996; Sullivan, 1984), yet only three of these reported outcome data and/or sufficient data to calculate effect sizes (Adelman, 1990; Hyun et al., 2010; Scheer, 1996). A meta-analysis of these three studies suggests that children participating in a child-focused group therapy programme did not differ in how positively they viewed themselves than children who did not receive the programme (Figure 22; n = 103; SMD = −0.38, 95% CI −1.32 to 0.57). There was significant heterogeneity between the effect sizes (τ 2 = 0.56; χ 2 = 10.56, df = 2, p = 0.005; I2 = 81%) and the only clear difference between the studies based on a priori moderators was that Hyun et al. (2010) was conducted in Korea and the other two studies were conducted in the United States. Removal of the Hyun et al. (2010) study from the meta-analysis suggested that children participating in a child-focused group therapy programme tended to report a less positive view of themselves than children who did not receive the programme (n = 75; SMD = −0.81, 95% CI −1.29 to −0.34) and heterogeneity between effect sizes reduced (τ 2 = 0.00; χ 2 = 0.85, df = 1, p = 0.36; I2 = 0%).
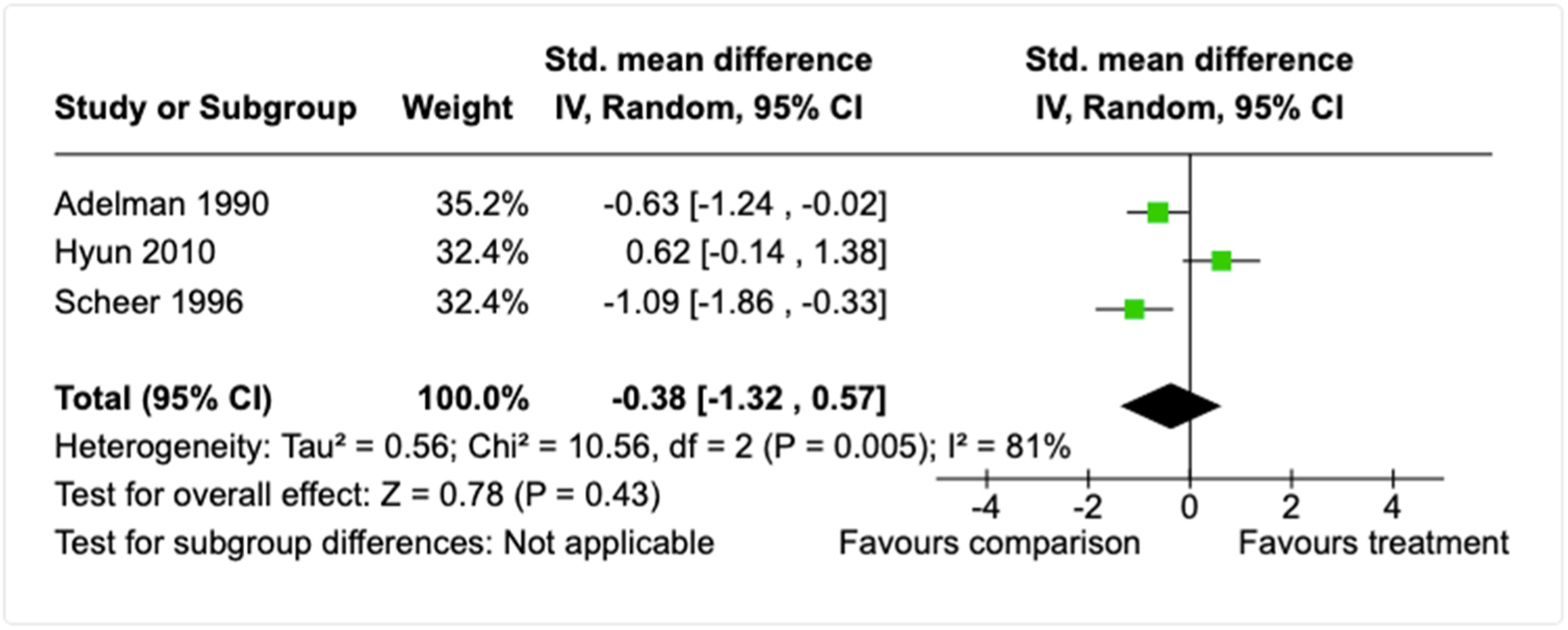
Forest plot for self-concept meta-analysis (post-intervention, child-report).
Four studies used self-esteem and/or self-worth measures to evaluate child-focused therapy models. Sorensen (1993) evaluated the impact of a child-focused group with adolescent boys in group foster care homes using an unstandardised measure of self-esteem. Peitler (1980) evaluated the effectiveness of a child-focused group for boys held at a hospital where fathers were being treated for alcoholism using a measure self-worth. Neither of these studies reported sufficient data to enable calculation of effect sizes.
Haley (1992) culturally adapted an existing measure of self-esteem to evaluate the impact of a child-focused therapeutic group at school with primary-school aged children of alcohol misusing parents. The single effect size for Hayley (1992) indicates that children who participated in the treatment had higher levels of self-esteem than children who did not participate (n = 60; SMD = 0.96, 95% CI 0.43 to 1.50). This effect was consistent for all but one subscale (social self-esteem) of this measure that represent different aspects of self-esteem (see Table 9). A fourth study by Hyun and colleagues (2010) evaluated the effectives of a group CBT programme for adolescent males using a measure of self-worth. The authors found that adolescents participating in the CBT group programme did not differ in levels of self-worth compared to adolescents receiving a ‘brief education on mental health’ (p. 204) at post-intervention (n = 28; SMD = 0.33, 95% CI −0.42 to 1.08).
Two studies evaluated psychosocial interventions using child-reported measures of resilience. The first was a longitudinal follow-up of the Focus on Families evaluation study approximately 10-years after the intervention (Skinner et al., 2009). The authors created a metric of functional resilience comprised of three items: (1) enrolment in school or being employed; (2) absence of substance abuse or dependence; and (3) lack of criminal justice involvement within the previous 5-years. Unfortunately, the authors did not report sufficient data to enable computation of an effect size for this study. The second study by Hyun and colleagues (2010) evaluated the effectives of a group CBT programme for adolescent males and found that adolescents participating in the CBT group programme did not differ in levels of resilience compared to adolescents receiving a ‘brief education on mental health’ (p. 204) at post-intervention (n = 28; SMD = 0.09 95% CI −0.65 to 0.83). Three studies also examined the effectiveness of child-focused psychosocial group programmes on children's self-reported coping, but none of the studies reported sufficient data to enable calculation of effect sizes (Broning et al., 2019; Gance-Cleveland et al., 2008; Roosa et al., 1990).
Sexual risk behaviours
One study examined the long-term effectiveness of the Focus on Families model (see above) on sexual risk-taking behaviours approximately 10-years after the intervention (Skinner et al., 2014). The authors created a dichotomous measure of risk based on whether the participant had not used condoms consistently during sexual encounters, if they reported more than two sexual partners in the last 12-months, or if they reported having sex outside a committed relationship. In addition, the authors measured participants' number of sexual partners, their sexual activity outside of a committed relationship, whether they had had sex in exchange for money or drugs, had received diagnosis of a sexually transmitted infection, or had a partner who was an intravenous drug-user in the previous 12-months. The authors found that the odds of any of the above sexual risks were no different between those who participated in Focus on Families compared to those who did not (see Table 9).
Wellbeing and functioning specifically linked to parental substance misuse
Two studies (Broning et al., 2019; Davis-Susser, 1990) used measures pertaining to child wellbeing and functioning specifically in relation to parental substance misuse to evaluate child-focused group therapies. Broning et al. (2019) measured coping behaviours relating to parental substance misuse, as well as child-reported distress and isolation relating to parental substance misuse. Data was provided by the authors for the latter two measures. Children participating in the TRAMPOLINE intervention did not differ from children who engaged the play-based attentional control activities on the measure of distress at post-intervention (n = 202; SMD = 0.13, 95% CI −0.15, 0.42) or at 6-months follow-up (n = 173; SMD = 0.23, 95% CI −0.08, 0.54). In comparison, children participating in the TRAMPOLINE intervention reported lower levels of isolation compared to children who engaged the play-based attentional control activities at post-intervention (n = 166; SMD = 0.55, 95% CI 0.23, 0.87), but this effect was not sustained at the 6-months follow-up (n = 164; SMD = 0.22, 95% CI −0.10, 0.54).
Davis-Susser (1990) examined whether a child-focused therapy group for children of alcoholics impacted coping behaviours relating to the alcoholic parent(s). At post-intervention, parents rated whether children appeared to demonstrate a range of coping behaviours (e.g., express their feelings about misuse). Children participating in the group programme did not differ in their coping behaviours in comparison to children who received no treatment (n = 40; SMD = −0.08, 95% CI −0.80, 0.64).
Child educational domain
Ten studies included at least one educational outcome (Adelman, 1990; Broning et al., 2019; Catalano et al., 1999; Claussen et al., 2004; Gance-Cleveland et al., 2008; Logan et al., 2001; Luthar et al., 2000; Orte et al., 2015; Roosa et al., 1990; Sullivan, 1984), yet only four studies reported outcome data or sufficient data to permit effect size calculation (Adelman, 1990; Catalano et al., 1999; Claussen et al., 2004; Sullivan, 1984). Table 11 below provides a summary of the analyses conducted across all outcomes in the education domain, and the subsections below provide further detail about the analysis results and included studies.
Child educational domain analyses and results.
Adelman (1990) found no differences on teacher-reported concerns about achievement, teacher-report concerns academic capabilities, official school attendance, or Grade Point Averages for children engaging with a school-based group therapeutic intervention versus children who did not participate (see Table 11). However, children engaging with the therapeutic group had higher grades regarding their conduct at school (n = 44; SMD = 0.67, 95% CI 0.06 to 1.28).
Sullivan (1984) reported assessing both teacher- and parent-report measures at post-intervention and 8-months after treatment completion, yet only reported partial parent-report outcome data at the follow-up time-point. No differences were found between those who received no treatment to those who received a psychosocial intervention comprised of 6 child, 6 parent, and 6 family therapy sessions on the learning problems subscale of a comprehensive measure of multiple areas of child functioning (n = 33; SMD = −0.61, 95% CI −1.33 to 0.10). However, children receiving treatment were rated by their parents as having higher levels of achievement difficulties than those who received no treatment (n = 33; SMD = −0.83, 95% CI −1.56 to −0.10).
The third study (Catalano et al., 1999) used a child-report measure to evaluate the effectiveness of the Focus on Families intervention (see ‘Child substance use’ section) and found that children in the treatment and comparison groups did not report any differences in their level of academic achievement at either 6-months (n = 104; SMD = 0.15, 95% CI −0.23 to 0.54) or 12-months follow-up (n = 100; SMD = −0.24, 95% CI −0.63 to 0.16). Likewise, treatment and comparison children did not differ on their reported levels of school attachment at 6-months (n = 104; SMD = 0.05, 95% CI −0.33 to 0.44) or 12-months follow-up (n = 100; SMD = −0.21, 95% CI −0.61 to 0.19).
The fourth study is a longitudinal follow-up of the children from the evaluation the centre- versus home-based early intervention programme (Claussen et al., 2004, see ‘Child cognition’ section). Using official data, the children were tracked into middle school to determine if there were any differences between the intervention models on the following outcomes: truancy, whether they were receiving special education services, specific categories of special education (Code J: Emotionally Handicapped; Code K: Specific Learning Disability; Code T: Developmentally Delayed), Passing grades (A–C), failing grades (D–F). By middle-school, the odds of truancy, specific categories of special education, passing grades, or failing grades were not higher or lower for children who received the more intensive centre-based intervention versus children who received the less intensive home-based intervention. However, children who received the more intensive centre-based intervention were less likely to be receiving special education services (n = 113; OR = 0.39, 95% CI 0.15, 0.99).
Cost-Benefits, treatment acceptability, and implementation considerations
Costs and benefits
Of the 68 studies utilised to generate effect estimates, 12 reported measures of costs and/or benefits for the intervention. Table 12 provides an overview of the data extracted from these studies. Costs and/or cost savings data was mainly available for comprehensive intervention models that integrate parental substance misuse treatment with other treatment components for parents, children, and the overall family unit. Excluding the one study with only cost data, all interventions produced savings or cost benefits compared to usual services.
Summary of cost and benefit secondary outcomes.
Treatment duration and completion
Of the 68 studies utilised to generate effect estimates, there was variable levels of information regarding treatment completion, treatment engagement, and specifications of the actual treatment duration or intensity (frequency and number of contacts). Data was extracted from each study regarding treatment completion rates and level of attendance. This data is provided alongside the intended duration and intensity of treatments in Tables 13 and 14. Treatment completion ranged from 100% to 43% and lower completion rates did not appear to be related to the duration or intensity of treatments. For example, there appears to be a relatively varied distribution of shorter and longer interventions among studies with higher and lower completion rates. Of the studies that reported measures of the amount of intended treatment that was completed (i.e., number of sessions), the rates ranged from 50% to 99%.
Summary of treatment duration and completion secondary outcomes.
Summary of treatment duration and completion secondary outcomes (retrospective studies or no completion data).
Note: Treatment duration is not reported for pharmacological studies, as there are existing comprehensive reviews that synthesise the full corpus of literature for length of stay and treatment duration. If presented here, the data would represent only those studies that have a child psychosocial outcome and data on treatment completion and duration (i.e., a biased subset).
Earlier reports of this RCT provide description data about treatment engagement and completion for a subsample of demonstration clients (Testa et al., 2003), these are not reported here as the estimates are not for the overall evaluation used for effect estimates.
Retrospective case control study.
Treatment acceptability
Of the 68 studies utilised to generate effect estimates, 13 gathered participants' and/or practitioners' perceptions of the intervention being evaluated. Table 15 provides an overview of the data extracted from these studies. Acceptability data was available for a range of intervention models and treatment participants consistently reported that they were satisfied with the intervention and/or perceived the intervention as being helpful. Common themes regarding characteristics of the interventions that were valued by participants included: (1) supportive, dependable, strengths-based, and non-judgemental relationships with practitioners; (2) developing emotion regulation (e.g., mindfulness) and parenting skills; (3) flexible support tailored to their needs; (4) connection with other children affected by parental substance misuse. For some studies, participants suggested providing ongoing aftercare following treatment completion. Themes from practitioner data include the importance of: (1) initial training, ongoing professional development, and ongoing clinical supervision; (2) close attention to time and resource management in light of family complexity; (3) consistent, fair, and transparent processes (particularly interventions set in a legal context).
Summary of treatment acceptability secondary outcomes.
DISCUSSION
Summary of main results
The objective of this systematic review was to synthesise the comparative effectiveness of psychosocial, pharmacological, and legal interventions for improving the psychosocial outcomes of children in families affected by parental substance misuse. We searched over 100 databases, websites, and trial registries to locate eligible studies, and supplemented this comprehensive search with additional search strategies (e.g., reference harvesting and forward citation searching). From over 56,000 records captured by the search, a total of 99 studies (published in 231 documents) met the review inclusion criteria, with 68 studies included in effect estimates represented in either single effect sizes or meta-analyses.
The included studies predominantly compared an eligible intervention to a TAU condition, with 27 studies comparing two alternative treatments. Included studies were classified on the presence or absence of nine intervention components to develop a typology that would facilitate the network meta-analytic approach specified in the review protocol. From this categorisation process, we identified that interventions were rarely only legal or pharmacological in nature, and that most studies integrated psychosocial treatments with either pharmacology, coordinated health care, case-management, and/or judicial or child welfare oversight and coordination.
A wide range of child psychosocial outcomes were captured by the 99 included studies and broadly fell into (1) child welfare, (2) child developmental, (3) child emotional and behavioural, and (4) child educational domains. These broad outcome domains each included multiple conceptually distinct outcomes which were synthesised separately. The mode of outcome measurement included official data, child-report instruments, parent-report instruments, and standardised neurodevelopmental assessments.
Once we grouped the available effect size data from the 99 included studies into outcome categories, only five outcome categories contained at least five studies to attempt construction of network geometries. As to be expected with a low number of studies, these network geometries were based on very small sample sizes and violated the assumptions required for NMA. Therefore, the evidence was synthesised with traditional meta-analysis and/or single effect size estimates, depending on the nature of the studies for each conceptually distinct outcome.
Overall, we conducted 36 meta-analyses and calculated 226 effect sizes where only one study was available. A further six studies contributed time-to-event effect sizes that were directly extracted from the study reports. Of the 36 meta-analyses (see Table 16), most assessed intervention effectiveness at the post-intervention time-point, with eight based on outcome measures at follow-up. In comparison, the effect estimates based on single studies were split between post-intervention outcome measurement (<3-months after intervention completion) and follow-up outcome measurements that ranged from 4-months to 5-years. In the subsections below, we summarise the main findings under each of the child welfare, development, emotional and behavioural, and educational outcome domains. It is important to emphasise that findings of no difference from meta-analyses and single effect sizes does not indicate that the included interventions had no effect. Rather findings of no clear differences suggest that the effect for intervention participants in comparison to (usually) TAU remains uncertain.
Results of all meta-analyses across outcome domains.
Effect size is an odds ratio.
The impact of psychosocial, pharmacological, and legal interventions on child welfare outcomes
Specific outcomes captured under this domain were: (1) child abuse, maltreatment, or neglect; (2) duration in child protective custody; (3) entry into out-of-home or kinship care; (4) number of out-of-home placements; (5) retaining parental care; (6) placement permanency (with parents or other carers); (7) reunification with parents; (8) termination of parental rights; and (9) child abuse potential. A total of 56 studies reported one or more of these child welfare outcomes, yet a substantial amount of missing data across these studies limited the number of studies within each outcome category and the subsequent ability to conduct meta-analyses. Overall, the findings were mixed depending on the outcome and time-point under consideration.
The findings for the child abuse, maltreatment, or neglect outcome category mostly indicated no differences between those who received an eligible intervention or TAU at post-intervention and follow-up. A meta-analysis of three studies focused in the prenatal and/or antenatal period indicated that the odds of child welfare investigation or involvement was no different between families who engaged in an intervention that integrated one or more psychosocial and/or pharmacological components versus families who received TAU. Similarly, a single study integrating parental substance misuse treatment with other psychosocial treatment components for both mothers and fathers found no difference in the odds of child protective services involvement at post-intervention or 6- and 12-month follow-ups versus treatment as usual. Similarly, a single study also indicated that the likelihood families being involved with child welfare did not differ according to the type of pharmacological treatment for NAS (methadone vs. morphine). However, an FTDC study (n = 450) suggested that odds of a substantiated child protection case approximately 4 years after treatment completion were greater for those engaged with the FTDC versus TAU. It is possible that engagement with FTDC may increase the level of supervision, and subsequently, reports to child welfare agencies.
The findings were more mixed for OOHC outcomes. A meta-analysis of four studies indicated that the likelihood of child children being in OOHC care was lower when their parents engaged in an intervention that integrated one or more psychosocial, pharmacological and/or legal components than TAU. Yet, a series of single studies indicated no differences in the effectiveness of comprehensive multicomponent interventions versus TAU on the following outcomes: mean number of days in child protective custody at post-intervention or follow-up; number of days children spent in OOHC 12 or more months after treatment completion; entering OOHC between more than 6-months after treatment; or the number of OOHC placements 12–15 months after treatment completion. A series of single studies compared alternate treatments for NAS and found no differences between the treatments in relation to the odds of infants being in OOHC (with family members, foster/adoptive care).
The findings were also mixed for the retention of parental care outcome category. A meta-analysis of seven studies indicated that parents retaining care of their children at the post-intervention time-point was more likely if they engaged in an intervention that integrated one or more psychosocial, pharmacological and/or legal components than TAU. Due to heterogeneity in the effect sizes for this meta-analysis, the seven studies were divided into (1) studies focused primarily in the postpartum period and with a health focus and (2) studies that extended into older aged children with more of a developmental and psychosocial intervention focus. These two separate meta-analyses revealed that interventions focused in the prenatal and/or neonatal period were effective for increasing the odds of parents retaining care of their children at the post-intervention time-point, yet the odds of retaining care was no different for families engaged in psychosocial interventions beyond infancy versus TAU. The follow-up effects are less clear. At 6-months post-discharge, mothers did not differ in the odds of retaining care depending on whether they had their children residing with them during treatment (single study). Yet engaging with an intensive family preservation service increased the odds of parents retaining care of their children 3.5 years after treatment completion (single study).
There were also variable findings for the permanency outcome domain. Meta-analyses indicated that FTDC models do not increase the odds of achieving permanency with either a parent or a relative at the post-intervention time-point. An additional single study indicated that the odds of achieving a permanent placement (no carer type specified) also did not differ between families engaged with an FTDC or TAU. Likewise, meta-analyses suggested that permanency via long-term guardianship or adoption was just as likely for families engaged with FTDC models compared to families engaged with TAU at the post-intervention time-point. Yet, based on a single effect sizes, the odds of permanency via long-term guardianship or adoption was higher for families engaged with FTDC models versus TAU at 6, 12, and 24 month follow-ups. It is important to note that placement stability is an important consideration for child wellbeing. The finding that there were greater rates of permanency via long-term guardianship in children whose parents were engaged in FTDC may indicate that for these children, biological parents were considered incapable of providing the requisite care in the long term. It is also possible, however, that there was a greater tendency to move to guardianship and adoption within the FTDC environment. Both possibilities warrant further research.
A series of single studies with relatively larger sample sizes used time-to-event data to examine the effectiveness interventions within a legal framework and interventions using comprehensive care coordination models. While the length of time taken to achieve permanency was longer for those engaged with FTDC models, the odds of exiting the child welfare system and achieving reunification were higher for families engaged FTDCs versus TAU upon intervention completion and at 6, 12, and 24 month follow-ups. Similarly, the odds of reunification were higher for families 24-months after engagement with a Recovery Coach model compared to TAU, but the time taken to reunify did not differ between families engaged with comprehensive care coordination versus TAU. Notably, a single study with a very large sample size (n = 350,604; Sanmartin et al., 2020) suggested a lower rate of reunification for children in American states with legislation promoting the removal of children from substance misusing parents compared to states without this legislation.
In terms of child abuse risk, a meta-analysis of five studies suggests that parents engaged with comprehensive family-focused interventions report lower child abuse potential than families receiving TAU. This effect was not maintained at follow-up within 3 to 6 months after treatment completion.
The impact of psychosocial, pharmacological, and legal interventions on child developmental outcomes
Specific outcomes captured under this domain were: (1) cognition; (2) executive function; (3) language; (4) motor skills; (5) social skills; (6) sleep; and (7) miscellaneous measures of development (e.g., whether development is within normal limits). A total of 22 studies reported one or more of these child development outcomes, but over a quarter of these studies had missing data.
Regarding cognition, a meta-analysis of five studies, and single effect sizes from three studies, suggest that that child cognition does not clearly differ between: families engaged with interventions focused on child health and development and/or parent wellbeing versus TAU; or infants treated with methadone or morphine for NAS; infants treated with morphine or clonidine for NAS. Similarly, a single study suggest that child executive function does not differ between families where the parent engaged in Brief Solution-Focused Therapy versus TAU or a child-focused therapy group versus TAU. Likewise, single studies suggest no differences in levels of (1) specific executive functions (e.g., attention, self-directiveness, or hyperactivity) in children who participate in child-focused group programme for children of alcoholics versus those receiving no treatment (parent- or child-report); or (2) parent-reported hyperactivity in children who engaged with an intervention comprised of family-, parent-, and child-focused components versus those who received no treatment.
However, meta-analysis of two studies indicates that children develop better expressive language skills following an intervention focused on the health and development of children with substance misusing parents versus TAU. A single study also suggests that children prenatally exposed to cocaine may develop better expressive language skills when they are engaged with a centre-based group developmental curriculum beginning in infancy compared to a home-based one-on-one curriculum. Although, another single study suggests that expressive language at 12-months of age does not differ between infants treated for NAS with either morphine or clonidine. A slightly different pattern of effects was found for receptive language. No differences were found for receptive language between those receiving an intervention focused on child health and development versus TAU. Yet children engaged with the centre-based developmental curriculum and infants receiving morphine for NAS showed better receptive language skills than children engaged with the home-based developmental curriculum and infants receiving clonidine for NAS.
Based on single studies and one meta-analysis with two studies, motor skills did not differ between children who received: (a) morphine versus clonidine for NAS; (b) methadone versus morphine for NAS; or (c) a centre group-based versus home-based one-on-one developmental curriculum. Again, based on single studies and one meta-analysis with two studies, social skills and sleep difficulties did not differ between children when (a) substance misusing parents and/or their families engaged in psychosocial interventions versus TAU; or (b) when children received a centre group-based versus home-based one-on-one developmental curriculum. Based on a single study, children who participated in a child-focused group therapy programme at school did not differ from children of alcohol misusing parents who did not engage in treatment on a teacher-rated measure of extroversion which included concepts such as self-centredness, energy levels, and social skills.
The impact of psychosocial, pharmacological, and legal interventions on child emotional and behavioural outcomes
Specific outcomes captured under this domain were: (1) composite measures of overall behavioural and emotional problems; (2) externalising behaviours; (3) internalising problems, including depression and anxiety; (4) prosocial behaviours; (5) delinquent behaviour; (6) substance use; and (7) a range of other miscellaneous measures of emotional and behavioural functioning (e.g., locus of control, trauma symptoms). A total of 51 studies reported one or more of these child outcomes, but like the other outcome domains, a large portion of these studies had missing data and were not included in the quantitative syntheses.
Regarding total problems, a meta-analysis of nine studies suggests that when families receive treatment for parental substance misuse, children have less behavioural and emotional problems upon treatment completion than children from families who receive TAU. Supported by subsequent meta-analyses, this effect was not sustained in the short-term 3 to 6-months after treatment completion, but was at the 6 or more months after treatment completion. Exploratory sensitivity analyses at this follow-up time-point suggested that variation among effect sizes reduced and the overall effect on total problems maintained with the removal of the only study conducted in an inpatient setting with fathers only.
A single study of comprehensive family support model found that the odds of scoring in the clinical range on a standardised measure of child behavioural and emotional problems did not differ from TAU. Participation in a child-focused therapy group in the school setting had lower odds of scoring in the clinical range for a standardised measure of child behavioural and emotional problems in one study yet did not impact the degree of teacher-reported overall child behavioural problems for another similar study. Further, the findings for total emotional and behavioural problems were not extended to single studies that compared alternative treatments (methadone vs. morphine for treatment of NAS or centre-based group vs. home-based individual developmental curriculum). Meta-analyses and single study effect estimates indicate that the findings also did not extend to externalising or internalising behaviours, irrespective of measurement time-point, whether the outcome was based on child- or parent-report, or whether the interventions were predominantly focused on the child or the family unit. The only exception was a single study which found that children engaged with a school-based intervention model treatment aiming to prevent substance use in children of substance misusing parents were less likely to obtain a score in the clinical range on a standardised measure of child internalising problems compared to children not engaged in TAU.
For the remaining behavioural and/or emotional outcome domains, the effects varied by the type of outcome and most effects are based on single studies or meta-analyses with only two studies. Results suggest that the impact of engagement with a psychosocial intervention that focus on the child, parent, and/or family units does not clearly differ from TAU or no treatment for the following child outcomes at post-intervention or follow-up: aggression, anxiety, antisocial behaviour, child-reported depression, child-reported anger, socioemotional functioning, trauma symptoms, locus of control, self-concept, self-worth, resilience, distress or coping in relation to parental substance misuse, child substance abuse or dependence, or risk sexual behaviours. A single study evaluating a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions, compared to no treatment, found higher levels of parent-reported child depressive symptoms and somatisation more than 6-months after treatment completion. These findings diverge from other single studies which found either lower no differences in child somatisation and specific internalising symptoms (e.g., withdrawal, depressive-anxious symptoms) between psychosocial treatment and comparison groups or lower withdrawn-depressed symptoms in children within psychosocial treatment versus comparison groups. Another single study found that children engaging with a school-based group therapeutic intervention reported higher levels of hopelessness compared to children who did not participate. These iatrogenic results should be treated with utmost caution because they are based on single studies with a very small sample sizes (n = 33 and 44 respectively).
In comparison, a meta-analysis of two studies found that an integrated treatment approach leads to higher levels of parent-rated prosocial behaviours than TAU upon treatment completion. However, this effect was not maintained at 3 to 6-month follow-up and was not found in a study comparing a centre-based group versus home-based individual developmental curriculum. A large single study of a child-focused therapeutic group found that children reported lower levels of isolation due to parental substance misuse and lower levels of stress at post-intervention and 6-month follow-up compared to children who received an attentional control play-based group programme. Based on a meta-analysis of two studies children who participate in a child-focused therapy programme self-report higher levels of knowledge about substance misuse upon treatment completion compared to children who did not participate. Based on one the studies included in the meta-analysis, this effect was maintained approximately 6-months later. Yet a smaller single study found no difference in the level of children's knowledge and attitudes regarding substance use following psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions, compared to no treatment. Finally, single studies of child-focused group interventions suggest that adolescents who engage in these interventions report higher levels of happiness, assertiveness, and self-esteem upon treatment completion compared to no treatment. A single study evaluating a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions, compared to no treatment, found lower levels of parent-reported child psychosis symptomatology symptoms more than 6-months after treatment completion. Though this differed from another single study which found no difference in psychosis symptoms in children who participated in a child-focused group therapy intervention versus those who did not.
The impact of psychosocial, pharmacological, and legal interventions on child educational outcomes
Specific outcomes captured under this domain were: (1) child- and parent-reports of academic achievement; (2) child-rated attachment to school; and (3) parent ratings of child learning difficulties. Nine studies reported one or more of these child educational outcomes, and only four were included in the quantitative synthesis. A single study suggested that children may have more academic achievement difficulties (as rated by parents) following participation a psychosocial intervention comprised of 6 parent, 6 child, and 6 family therapy sessions compared to no families receiving no treatment. This result should be treated with utmost caution it is based on a single study with a very small sample size (n = 33). This same effect was not found for parent-rated learning difficulties. An additional single study assessing the comprehensive Focus on Families intervention found no differences between treatment and comparison participants on child-reported academic achievement or attachment to school at either 6 or 12-months post-intervention. Another single study found no differences on official educational outcomes approximately 5 years after either a home- or centre-focused early intervention before age 3. A final study found no differences on teacher-reported concerns about achievement, teacher-reported concerns academic capabilities, official school attendance, or Grade Point Averages for children engaging with a school-based group therapeutic intervention versus children who did not participate. However, children engaging with the therapeutic group received higher grades regarding their conduct at school.
Consideration of costs-benefits and other implementation issues
Twelve studies reported data related to the costs and/or benefits of interventions, which overwhelmingly illustrated savings or cost benefits versus usual services. Treatment completion was variably reported across the corpus of studies used to generate effect estimates, and ranged from 43%–99%. Thirteen studies gathered participants' and/or practitioners' perceptions of the intervention being evaluated. Emerging themes suggest that participants place value on intervention characteristics, such as intervention flexibility and tailoring and specific intervention components (e.g., emotion regulation, parenting skills, connecting with others who have lived experience). Practitioner-focused themes highlighted the importance of training and ongoing professional development, resource management, and clear consistent implementation processes.
Overall completeness and applicability of the evidence
There are several issues that limit the completeness and applicability of the evidence captured by this review. First, a large portion of included studies did not report sufficient data to calculate effect sizes which subsequently reduced the size of the quantitative syntheses. In turn, this likely impeded our ability to conduct NMA and our ability to conduct subgroup analyses in the context of traditional meta-analyses. Subsequently, we are unable to draw well supported conclusions about the comparative effectiveness of different intervention approaches to improve outcomes for children in families affected by parental substance misuse. Relatedly, for many of the outcomes, effect estimates were based on single studies with small sizes, which again limits our ability to draw firm conclusions about intervention effectiveness for many of the outcomes captured by the review. Notably, a group of four studies with sample sizes ranging from 33 to 96 participants produced 34.8% of the 227 effect estimates for outcomes based only on single studies. Another slightly larger study (Catalano et al., 1999) produced another 9.7% of effect estimates for outcomes based on single studies. These same five studies contributed to between three and four of the 36 meta-analyses. This means that for many outcomes, we can only draw very tentative conclusions based on intervention models from single studies that (a) simultaneously treat children and parents (Catalano et al., 1999; Sullivan, 1984); (b) focus on treating parents (Kim et al., 2019) or children (Adelman, 1990) only; or (c) focus on child development from infancy to toddlerhood, with some practical and case-management support for mothers (Claussen et al., 2004).
Second, the majority of the studies were conducted in the United States which means that there is currently little understanding about whether the interventions synthesised in this review would have the same or different effects in other geographical settings. Third, there was a prominent absence of fathers across the corpus of studies. Although studies did not categorically exclude fathers, there was a notable absence of father-reported data or mention of fathers across the included studies. Fourth, there was very limited outcome data for multiple areas known to be affected by parental substance use, including education and subsequent child substance use. This is likely related to the included studies mostly being concentrated in the early childhood years. Fifth, there is also a significant lack of longer-term follow-up, with only 19 outcomes having both post-intervention and follow-up measures. Of these, two were based on single studies and 12 only had single studies at follow-up after a meta-analysis was conducted for the post-intervention measurement. Five outcome categories included multiple studies that were meta-analysed at the post-intervention and follow-up time-point, albeit usually with a reduced number of studies at follow-up. Collectively, these issues limit the generalisability of the review findings and restrict conclusions about the effectiveness of interventions for children in families affected by parental substance misuse. Further, the lack of follow-up may have hindered the ability to detect effects that might be more likely to emerge over time, such as developmental, psychological, and behavioural changes.
A final limitation of this review is that 3 years have elapsed since the systematic search. This means that eligible studies published in late 2021 through to early 2024 likely exist and, if so, could potentially impact the estimates of effectiveness for psychosocial, pharmacological, and legal interventions for improving the outcomes of children affected by parental substance misuse. An updated review, in the new future, will ensure the most recent evidence is captured and synthesised. This is planned for 2025.
Quality of the evidence
Although over three quarters of the included studies were RCTs or quasi-experimental studies with matched intervention and comparison groups, there were notable methodological issues for many of the studies which reduces the quality of the overall evidence synthesised in the review. The studies had variable levels of bias, with all studies rated as high on at least one domain. In addition, only 11 of the 36 meta-analyses contained more than three studies and only 10 meta-analyses included more than 300 total participants. Some of the meta-analyses also had unexplained heterogeneity, which suggests that effectiveness of interventions may vary by unobserved factors. Further, many effect estimates are based on single studies with small sample sizes and there was a substantial amount of missing data across the corpus of included studies. Together, these issues reduce the certainty in the conclusions made about the effectiveness of psychosocial, legal, and pharmacological interventions for families affected by parental substance misuse and whether these intervention models impact child psychosocial outcomes.
However, it is important to acknowledge the efforts to date. The fact that there are 99 RCTs and relatively rigorous quasi-experimental trials with such a vulnerable population is commendable. Conducting research with such hard-to-reach populations creates complexities over and above difficulties already inherent when evaluating complex psychosocial interventions in applied settings (e.g., Hindmarch et al., 2015; MacLachlan et al., 2021). Therefore, while there is a need to continuing growing the evidence, the existing corpus of evidence does permit some important conclusions to be made about how engaging with parents and families can have positive impacts on child psychosocial outcomes.
Potential biases in the review process
This review used a broad and comprehensive systematic search, substantial outreach to study authors, and double coding of effect sizes and risk of bias assessments, which collectively reduce potential biases in the review process. However, we acknowledge 3 possible issues that could introduce bias into the review process. First, we did not synthesise studies written in languages other than English. To reduce potential bias, we have included a list of all potentially eligible studies written in languages other than English in the ‘ Studies awaiting classification ’ reference list (Supporting Information: Appendix G). Second, we used automated screening based on machine learning for a small portion of title/abstract and full-text screening due to the vast number of records captured by the search. Automation in systematic reviews is gaining momentum so that up-to-date evidence syntheses can be produced for health and social issues in a timely way (e.g., see Shemilt et al., 2022). We used a systematic stopping rule before invoking automated screening and inbuilt cross-checking functions within DistillerSR, yet we acknowledge that the machine learning embedded within DistillerSR software may not have accurately classified all records that were not manually screened. This may have resulted in missed studies. Third, we did not calculate effect sizes that adjusted for baseline measures or controlled for confounders. This may have reduced the precision of some studies that reported sufficient data to calculate these adjusted effect estimates.
Agreements and disagreements with other studies or reviews
While there are many existing reviews that capture some of the same studies that were captured for this review, no review exists that captures the breadth of interventions and outcomes that are covered by this review. Prior reviews capture pockets of studies that are included in this review (e.g., FTDCs in Zhang et al., 2018). However, few existing reviews use meta-analysis or standardised effect sizes to estimate treatment effects at all or that align with the analyses undertaken in this review. Many existing reviews rely on narrative synthesises or vote-counting approaches based on statistical significance of individual study findings, both of which undermine the ability to arrive at rigorous and unbiased conclusions about intervention effectiveness (e.g., Bowie, 2005; Lloyd, 2015; Neger & Prinz, 2015). Across the existing body of reviews, authors frequently highlight the limited amount of high-quality evaluation evidence and depending on the research question and synthesis approach, authors have reached varying conclusions about overall effectiveness. More rigorous systematic reviews tend to align with the current review by concluding that the existing evidence limits the ability to draw solid conclusions or find mixed evidence for effectiveness (e.g., Bröning et al., 2012; Calhoun et al., 2015; McGovern et al., 2021; Krahn et al., 2018; Moe et al., 2013; Turnbull & Osborn, 2012; Zhang et al., 2018). Reviews with less systematic methodologies and/or without meta-analyses range from concluding that existing interventions show promise for improving child outcomes (e.g., McCalman et al., 2017; MacVicar et al., 2019; Niccols et al., 2012; Templeton et al., 2010) to concluding that here is insufficient evidence to ascertain effectiveness (e.g., Bowie, 2005; Peisch et al., 2018; Ritland et al., 2020; West et al., 2020).
In terms of the conclusions of individual studies, the effect sizes mostly aligned with the individual studies captured by the review. In some instances, meta-analyses contained a set of studies with mixed individual findings which translated into a significant overall effect favouring the intervention (e.g., retaining parental care meta-analysis), but in other cases generated a null effect (e.g., child abuse potential follow-up meta-analysis). We also identified a pattern where studies did not clearly identify or summarise statistically meaningful effects (positive or negative) for all measured outcomes, or focused on within group changes over between group differences, or compared raw statistics without any statistical analysis. This meant that some effect sizes did not appear to clear align with overall study findings summarised by the authors in-text but did align when directly referencing the data and results of statistical tests. While changes in outcomes with reference to an intervention are important, this type of single-group assessment produces biased estimates of effectiveness when not considered alongside the relevant comparison condition (e.g., no treatment, TAU, alternative treatment).
AUTHORS' CONCLUSIONS
Implications for practice
This review highlights the significant work that has been achieved to date in the development and evaluation of interventions to improve the lives of families affected by parental substance misuse. It is encouraging that there are many models from which practitioners can choose from when treating families affected by parental substance use. Most of these interventions integrate treatment of parental substance misuse with other treatment components aiming to alleviate vulnerability in other areas known to be impacted by parental substance misuse (e.g., parent emotion regulation, child health and development). Based on meta-analyses, the most robust finding from this review is that integrated psychosocial interventions – which may or may not contain pharmacological or legal components – can reduce child abuse potential, reduce the likelihood of OOHC, increase the likelihood of parents reunifying or retaining care of their children, enhance expressive language development, increase child prosocial behaviours, and reduce overall child emotional and behavioural difficulties in the short-term. There is also preliminary indications that effects are maintained within 6 to 12 months post-intervention for total child emotional and behavioural difficulties. Depending on the outcome of interest or rationale for intervening with a family affected by parental substance misuse, practitioners need to be mindful of the limitations in the evidence in terms of reliable estimates of effectiveness.
It is also important to acknowledge that we know less about the effectiveness of the full range of interventions in different geographical settings outside of the United States. While there is evidence to support the transportability of parenting interventions (Gardner et al., 2016), this evidence is based on standalone parenting programmes implemented with lower-risk populations. Complex interventions with families affected by substance misuse may not be as easily transported to other geographical settings, particularly so when considering the nuances in the social care, child welfare, and legal systems across different nations (Cameron & Freymond, 2006; Gilbert, 2012). Though there is some preliminary evidence of transportability of complex interventions based on the findings of this review. For example, the Parents Under Pressure programme was found to be effective in both Australia (Dawe & Harnett, 2007) and the United Kingdom (Barlow et al., 2019), and FTDC models were found to be effective on some outcome measures in the United States (e.g., Boles et al., 2007) and in the United Kingdom (Harwin et al., 2018).
The vulnerable nature of families affected by parental substance misuse necessitates the implementation of evidence-based policies and treatments that are most likely to generate sustained changes for families. There are substantial social and financial burdens to broader society when families are not adequately supported. For example, recent estimates suggest that the costs of child abuse and neglect and other adverse childhood experiences – a common concomitant issue accompanying parental substance misuse – are comparable to the costs of major diseases (Bellis et al., 2019; Dalziel et al., 2015). Economic evaluations do suggest that both parent-focused substance misuse treatment interventions and comprehensive evidence-based interventions for families affected by parental substance misuse can generate significant cost savings (e.g., see Barlow et al., 2019; Dalziel et al., 2015; Ruger & Lazar, 2012). To achieve the most positive outcomes for families affected by parental substance misuse, it is vital that policy and practice prioritises access to the interventions with the most rigorous evidence (Doyle et al., 2021). The findings of this review suggest that the most rigorous evidence is available for integrated interventions that simultaneously focus treatment on multiple levels of the family ecology.
Implications for research
This review highlights the need for ongoing research efforts to confidently ascertain the effectiveness of psychosocial, legal, and pharmacological interventions for improving psychosocial outcomes of children in families affected by substance misuse. Despite well-established guidelines for reporting clinical trials (i.e., CONSORT; Boutron et al., 2008) and for adequately describing interventions used in evaluation research (i.e., TIDieR, Hoffmann et al., 2014), only a portion of the included studies aligned with these standards. In many cases there was incomplete reporting of the intervention and participants, along with complete omission or inadequate reporting of the results. Considering the large costs associated with implementing and evaluating complex social interventions, this is problematic in terms of cost-effectiveness of finite resources and also introduces barriers to our understanding of the true effectiveness of interventions to improve family outcomes.
To advance the field, further rigorous trials, including replications, are needed. Moreover, making concerted efforts to track families for longer periods will also enable evidence-based policy and practice for how and when families might need longer-term support. There is also an urgent need to examine whether existing interventions are suitable and effective in locations other than the United States. Other important contextual moderators to understand more fully include poverty, ethnicity, substance of misuse, and other intervention characteristics (e.g., intervention intensity, implementing practitioners). However, an examination of the included studies highlights the difficulties in retaining participants and retaining complete outcome data when conducting research with families affected by parental substance misuse. Consequently, the small sized samples that are often recruited for this hard-to-reach population are further impeded when attempting statistical analyses to determine treatment effectiveness or complex analyses of changes in multiple constructs over time. It is commendable that the retention rates for many of the trials is comparable to parenting research without such vulnerable hard-to-reach populations (Chacko et al., 2016). Moving forward, a key consideration when designing trials will be researchers building in costs and processes for recruiting and retaining families from this hard-to-reach population (Bonevski et al., 2014; Hindmarch et al., 2015; MacLachlan et al., 2021; Webb et al., 2017). Particular attention also needs to be given to reducing the barriers to accessing treatment and maintaining engagement, such as stigma and limited financial resources (Barnett et al., 2021; Schamp et al., 2021).
This review demonstrates that we need further evidence to conclusively endorse the full range of possible interventions that are available for families affected by parental substance misuse. Further, there is variation in the effectiveness depending on the outcome under consideration and some evidence that interventions may not sustain initial gains in the long-term. Given the large number of ‘null findings’ found by this review, it is tempting to draw the conclusion that ‘nothing works’ compared to TAU. However, an alternative hypothesis can be drawn from the results, which could be examined in future research. The sample characteristics for the studies included in this review highlight the cumulative level of risk for families affected by parental substance misuse. Research also demonstrates the multilayered vulnerability and the chronic nature of substance misuse (Fleury et al., 2016; Heilig et al., 2021). This may mean that time-limited interventions that focus on isolated areas of family functioning (e.g., substance misuse, parenting, or child wellbeing only) might not be sufficient to generate change or sustain long-term treatment gains. Unfortunately, most family support systems across the globe tend to focus on providing the most intensive support at the time of crisis, for example, when children are at high risk of being removed (Bezeczky et al., 2019). When substance misusing parents come into contact with the child welfare system, usual care tends to have a narrow and short-term focus on abstinence and commonly behaviourally informed parenting approaches (Renk et al., 2015). Research suggests that complex vulnerable families often have repeat engagements with child welfare-initiated interventions over time and that this type of engagement is costly (Davidson et al., 2019). Yet a common view is that given the cumulative adversities faced by families affected by dual child welfare and parental substance misuse issues, treatment needs to take a trauma-informed approach that comprehensively supports parents and pays attention to the quality of thendividualg relationship (Collier, 2021; Renk et al., 2019; Hatzis et al., 2019). It would be beneficial to examine in future research if triaging the nature and duration of family support according to level of need is a more cost-effective and beneficial approach for families affected by parental substance misuse. For example, emerging research suggests that short ‘booster’ treatments can help sustain the effects of interventions over time (Kolko & Lindheim, 2014; Tolan, 2014). Other research has begun to explore post-reunification service models to stabilise families and promote resiliency (Rushovich et al., 2021).
Overall, the body of evaluation evidence is weakened by large amounts of missing data, substantial variations in the quality of reporting, limited follow-up assessments, and a concentration of research in the United States. There is clearly an urgent need for ongoing high-quality evaluation research that follows established reporting standards (Boutron et al., 2008; Montgomery et al., 2018), integrates follow-up assessments, and tests whether interventions can achieve the same outcomes in different settings. Building on the existing evidence-base with these issues in mind will, in turn, permit more certain conclusions about the effectiveness psychosocial, legal and/or pharmacological interventions for families affected by substance misuse. While acknowledging the complexities of undertaking research in this field, and the enduring vulnerabilities of substance misusing parents, this review highlights that change is possible and that there is evidence for improving outcomes for children affected by parental substance misuse. The advantage of undertaking a systematic review of this scope and focus is to highlight where gains have been made and to underscore the methodological rigour that needs to be adopted going forward.
Footnotes
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the support of the following research support staff: Tessa Clarkson, Abby Kortlang, Sadhvi Krishnamoorthy, Lachlan McDougall, Liuissa Zhen, and Melissa Wyllie. The authors also gratefully acknowledge the editorial support from the Campbell Collaboration Social Welfare Coordinating Group, along with the thoughtful feedback from reviewers.
CONTRIBUTIONS OF AUTHORS
All the authors developed the content and contributed to systematic review methods. The work for completing review was distributed among authors as follows: Systematic search, including harvesting, forward citation searching, and hand-searches: EE, SR Title/abstract screening: EE, NCH, BT Literature retrieval: EE, SR, JB Full-text screening: EE, SR, JB Full-text and effect size coding: EE, JB, SR Risk of bias assessments: EE, JB, NCH, BT Analyses: EE, DBW Mediations (collaborative): EE, SD, DBW Preparation of manuscript: EE, SD, DBW, SR
DECLARATIONS OF INTEREST
Sharon Dawe has been involved in the development and evaluation of the Parents Under Pressure programme (PuP). PuP has been evaluated in families with parental substance misuse issues and these studies were included in this review. To minimise any potential biases, Sharon Dawe did make any independent screening decisions, code studies, or assess risk of bias during the review process. Elizabeth Eggins and David B. Wilson both hold editorial roles with the Campbell Collaboration Crime and Justice Coordinating Group. As this review is registered with a different coordinating group, Elizabeth Eggins and David B. Wilson were not privy to the editorial process or decision-making process pertaining to this review.
PLANS FOR UPDATING THE REVIEW
We plan to update this review every 3–5 years, with the first update planned for 2025.
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
We made eight deviations between the protocol and the review. First, due to resources, we did not include studies written in languages other than English unless we could verify that they were secondary reports of included studies that were written in English. Second, we needed to make some minor changes to search locations due to either the source no longer being available or severe functionality issues which made searching and/or exporting from the source unfeasible. The specific deviations are listed in ![]() below.
below.
Third, we did not contact prominent scholars relevant to the review topic to enquire about eligible studies not yet published or disseminated, in a general sense. We did, however, attempt contact with over 100 authors to either gather missing data, locate full-text versions of studies we could not source, and to confirm eligibility for the review. We also implemented multiple other search strategies, which reduces the likelihood that potentially eligible studies were unidentified.
Fourth, we did not include attachment outcome measures in the review. Although our protocol listed attachment as a primary outcome variable, it is generally measured in a dyadic manner, which differs to the child-level variables included in the review. We believe that attachment is a measure that could be included in a future review that also considers other dyadic parent-child and family measures (e.g., emotional availability, HOME scale).
Fifth, we used a two-stage title and abstract screening process, rather than the single stage outlined in the protocol. This allowed us to triage staff working on the projects to their level of expertise and knowledge of the area and reduce the level of documents proceeding to the more time-intensive full-text eligibility screening stage.
Sixth, all studies were not independently double-coded. Independent double coding is a highly desirable rather than mandatory MECCIR standard and due to resources and the high number of included studies, we were unable to conduct full independent double coding. We did, however, double code all effect size data and double coded 70%–80% of risk of bias assessments.
Seventh, we changed the risk of bias assessment tool for quasi-randomised studies due to variation in the suitability of the ROBINS-I tool across all included studies (see ‘Assessment of risk of bias in included studies’ section. Changing to a different, well-established tool, allowed us to use the one risk of bias assessment tool for all quasi-experimental studies, which helps to convey the results clearly.
Eighth, our protocol specified that we would use baseline data in effect size calculation, yet given the variation in use of baseline data and the variable availability of correlations between time-points (which is required in the calculations), we decided against this approach. Instead, we used post-intervention and follow-up time-points in all effect size calculations (see ‘Measures of treatment effect’ section). We hope to utilise more complex methods to adjusted and unadjusted effect sizes, along with accompanying sensitivity analyses, in future updates of the review.
SOURCES OF SUPPORT
REFERENCES
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.