
Abstract
Background
Societal changes have led to greater isolation and higher levels of loneliness particularly for older generations. Loneliness is a significant public health challenge leading to increased levels of poor mental health. Depression and anxiety are also increasing in prevalence amongst children and young people. Intergenerational activities are interventions designed to bring together older and younger generations with the purpose of allowing participants to utilise their experiences and skills, and to give participants a chance to experience the pleasure and excitement that occurs with the transmission of knowledge and skills from one generation to another. Intergenerational activities are therefore potential interventions that can address the growing problems associated with loneliness and lack of wellbeing.
Objectives
This systematic review aims to examine the impact of intergenerational interventions on the wellbeing and mental health in children and adolescents, and potential harmful effects. It also aims to identify areas for future research as well as key messages for service commissioners.
Search Methods
We searched an evidence and gap map published in 2022 (comprehensive searches conducted July 2021 and updated June 2023) to identify randomised controlled trials of intergenerational interventions that report mental health and wellbeing outcomes for children and young people.
Selection Criteria
Randomised controlled trials of intergenerational interventions that involved unrelated younger and older people with at least one skipped generation between them and reported mental health or wellbeing outcomes for children and young people were included in this review.
Data Collection and Analysis
We used standard methodological procedures expected by The Campbell Collaboration. We conducted data extraction and Cochrane risk of bias assessments in EPPI reviewer.
Main Results
While we identified 500 evaluations of intergenerational interventions, where the impact on participating children and/or young people was evaluated this was most often limited to assessing their impact on attitudes to aging. We identified five studies evaluating five different types of intergenerational interventions which included one-off sessions to ones that spanned a year measuring their impact on the mental health and wellbeing of children and/or young people. The purposes of the interventions differed, which included promoting social skills, preventing harmful behaviour and promoting learning. The ages of children also varied across the five studies, with one targeting younger children, two targeting younger teenagers and two targeting older teenagers. One study included socioeconomically disadvantaged children, and in the other studies the socioeconomic backgrounds of the children and young people were not described. The outcome measures used to evaluate the interventions varied with none of the studies measuring the same outcomes. One study showed improvements in wellbeing measures, and this was an intervention delivered to children in deprived neighbourhoods, where the intervention duration was for a year allowing the development of a greater depth of relationship between the younger and older participants. Four studies found no……. The included studies were at high risk of bias therefore raising uncertainty in the reliability of the findings. Underpinning theories that supported the development of the interventions and explained the mechanisms of effect were poorly described.
Authors' Conclusions
The evidence for the effectiveness of intergenerational interventions on the mental health and wellbeing of children and young people is limited and inconclusive. Few evaluations have sought to measure how intergenerational interventions impact children and young people and where this impact is measured the focus is usually limited to attitudes to aging. The evidence that has been collected is too heterogenous to allow synthesis of the findings. The underpinning theories to support their development are poorly described with no follow-up data to ascertain if benefits are maintained. Intergenerational interventions show promise but researchers have failed to measure how they impact on the mental health and wellbeing of children and young people. This is a serious limitation of the evidence base that needs to be addressed in robust and rigorous evaluations.
PLAIN LANGUAGE SUMMARY
Limited evidence and limited effects of intergenerational activities impact on the wellbeing and mental health of children and young people
The review in brief
Only five studies have evaluated the impact of intergenerational interventions on the wellbeing and mental health of children and young people, despite these types of interventions intending to have benefits for both younger participants, as well as older age participants. There is insufficient and inconclusive evidence to demonstrate that these interventions benefit children and young people. Evaluations need to improve the measurement of the impact of intergenerational interventions on children and young people.
What is this review about?
The number of older people experiencing isolation and loneliness has increased in many societies. Loneliness can lead to poor mental and physical health. Children and young people are experiencing increasing levels of anxiety and poor mental health. Intergenerational interventions aim to bring both older and younger people in purposeful shared activities. Intergenerational in this context means a generation is skipped between the older and younger participants. These have potential to reduce the growth in loneliness and decline in wellbeing for both older and young people. The impact of these types of interventions, and what elements contribute to their effectiveness are important to understand to inform practice and policy decisions.
What is the aim of this review?
This systematic review aims to identify and summarise all of the existing research that has been designed to explore how intergenerational activities affect the mental health and wellbeing of children and young people.
What are the main findings of this review?
This review includes only five studies that evaluate the effects of intergenerational activities on the mental health and wellbeing of children and young people. Three studies were undertaken in the USA and two in Europe. The duration of the interventions ranged from 1 day to 1 year. Their purposes also differed including; supporting learning, promoting positive behaviours and reducing harmful behaviours. They targeted different ages of children from younger children to teenagers. None of the studies evaluated the same outcomes so it was difficult to make comparisons between them. One study showed improvements in wellbeing measures, and this was an intervention delivered to children in deprived neighbourhoods, where the intervention duration was for a year allowing the development of a greater depth of relationship between the younger and older participants. Overall, evaluations of intergenerational interventions often fail to measure outcomes in children and young people, and there is not a consistent approach to measuring mental wellbeing outcomes that allows comparison or synthesis of the studies.
What do the findings of this review mean?
Although intergenerational interventions appear to have promise in improving mental wellbeing of children and younger people, existing evidence is very limited and is inconclusive. Future evaluations should seek to measure the impact on the mental health and wellbeing of children and young people to inform decision making.
How up-to-date is this review?
State here when the review authors searched for the included studies: ‘The review authors’ searched for studies up to 2021.
BACKGROUND
The problem, condition or issue
Description of the condition
Opportunities for social connection between generations in the UK have diminished over recent decades as a result of changes in the way that we live and work (Kingman, 2016; United for all Ages, 2017). Housing and economic changes have seen many younger people move to live in city centres whilst the older generation often live in towns and rural areas. A report published by the Intergenerational Foundation in 2016 (Kingman, 2016) suggests that in the 25 biggest cities within the UK only 5% of people who live in the same neighbourhood as someone under the age of 18 are over 65. Furthermore, even when people from different age groups do live in the same area, the decline in spaces such as libraries, youth clubs and community centres mean fewer opportunities to meet and mix socially with other generations outside their own families. Increased working hours, digital innovations that have excluded older generations, changes in family patterns, relationship breakdowns within families and migration are also believed to be contributory factors to generation segregation (Together, 2020).
There are many potential economic, social and political impacts of generations living separate and parallel lives, for example, higher health and social care costs, an undermining of trust between generations (Brown, 2014; Vitman, 2014), reduced social capital (Laurence, 2016) and a reliance on the media to form understanding of others' viewpoints (Edström, 2018; Vasil, 1993) and higher levels of anxiety and loneliness. Loneliness is a public health concern because of its detrimental impact on health, and in the UK, has led to the appointment of a Minister for Loneliness, to raise awareness of loneliness and help people to build connections and lead happier and healthier lives. Loneliness particularly affects young and older age groups. In the Office for National Statistics Community Life Survey, 2016 to 2017 (Office, 2018), 5% of adults in the UK felt lonely often or always and compared with all other age groups except the 25 to 34 years group those aged 16 to 24 were significantly more likely to report feeling lonely often or always. Social isolation and loneliness are strongly associated with depression, anxiety, self-harm and suicide attempts across the lifespan (John, 2018; Turecki, 2019).
Within this context, intergenerational activities offer important potential benefits for both younger and older people that cannot be underestimated. Intergenerational programmes bring together older and younger people for the purpose of allowing participants to utilise their experiences and skills, and to give participants a chance to experience the pleasure and excitement that occurs with the transmission of knowledge and skills from one generation to another (Radford, 2018).
Intergenerational interventions encompass diverse models of working, involving different populations of older and younger people, for different purposes. The intervention might, for example, offer shared activities with the aim of improving cognitive, health and social outcomes in older adults with dementia, learning in a community or online setting to promote reading in younger children, and exchange programmes between adolescents and elders to improve intergenerational understanding and attitudes.
Emerging evidence on the economic and social impact of the coronavirus (COVID-19) pandemic shows that young people aged 12–24 years constitute one of the worst-affected groups particularly in terms of the labour market and mental health outcomes (Leavey, 2020). Furthermore, young people are losing their ability to accumulate the assets needed for a smooth transition into adulthood with long term implications for their health and wellbeing throughout the life course (Leavey, 2020).
Mental wellbeing is intrinsically linked to enabling a child to achieve their full potential. Socio-ecological influences influencing the world of the child, and the environment surrounding them is a complex and dynamic interplay of risk and protective factors (United, 2017). For young children, in particular vulnerable young children, the disruption caused by the pandemic has been especially damaging, compounding existing inequalities (Ballard, 2020; Pierce, 2020). Nearly 800,000 children live with domestic abuse and 1.6 million live with parents with severe mental health conditions (Longfield, 2020). These numbers have increased significantly, as a result of secondary impacts of the pandemic on disadvantaged families in particular in terms of loss of income, and increased intimate partner violence (Anne, 2020). In addition, children's education has been disrupted, and a widening attainment gap is emerging between children from disadvantaged or vulnerable backgrounds and their peers (Longfield, 2020; Sinha, 2020). Intergenerational interventions have been shown to reduce anxiety and improve self-worth in children, and also to improve classroom behaviours and foster pro-social behaviours (Park, 2015).
Intergenerational interventions, and interventions that might improve social and mental wellbeing of children and young people have been identified as priority policy areas. The All Party Parliamentary Group on Social Integration in an interim report published in May 2019 (All Party Parliamentary Group on Social Integration, 2019), highlights four main policy areas through which stronger generational connections and communities could be fostered – community projects and initiatives, public services, housing and planning and technology.
Research questions related to intergenerational activities and connections identified in a research gap analysis, conducted by Public Health England and published in August 2020 (Public Health England, 2020), include ‘What is the impact of different intergenerational interactions at different stages of the life-course?’
Interventions that ameliorate the impact of adverse childhood experiences (ACEs) have been identified as priority areas for research during priority setting exercises for Sheffield, Greater Manchester and the Scottish Government as members of the SIPHER consortium (System-science Informed Public Health and Economic Research for Non-communicable Disease prevention) (MRC/SO37578/1). The James Lind Alliance prioritisation process has highlighted the need to identify effective early interventions or strategies for supporting children and young people to improve mental resilience.
A stakeholder group who were informed by findings from our own Evidence Gap Map (EGM) and mapping review (Campbell, 2023) identified the subsequent review question as both a priority knowledge gap and a priority question for commissioners and representatives of children and young people.
Searches of PROSPERO and of the Cochrane and Campbell Libraries were unable to identify either ongoing systematic reviews or EGMs intended for publication that would address this question.
The intervention
We use the definition of intergenerational practice developed by the Beth Johnson Foundation (http://www.ageingwellinwales.com/Libraries/Documents/Guide-to-Intergenerational-Practice.pdf).
‘Intergenerational practice aims to bring people together in purposeful, mutually beneficial activities which promote greater understanding and respect between generations and contributes to building more cohesive communities. Intergenerational practice is inclusive, building on the positive resources that the young and old have to offer each other and those around them’ Beth Johnson Foundation.
Intergenerational programmes and activities are as such interventions that can address some of the needs of both older people and children and young people. These interventions take many formats and are delivered in diverse settings, often by third sector organisations. Evidence suggests that such intergenerational activity can have a positive impact on participants (e.g., reducing loneliness and exclusion – for both older people and children and young people; improving mental health; increasing mutual understanding and tackling important issues such as ageism, housing and care).
How the intervention might work
Intergenerational programmes often develop organically and vary in many of their features, including differences in terms of the populations targeted, their purpose, settings in which they are delivered and duration.
Intergenerational interventions are rarely accompanied by programme evaluations and use of theory in intergenerational research is also limited (Kuehne, 2003).
As such while developmental and educational theories underpin arguments in favour of developing such intergenerational programmes (e.g., generativity as the developmental challenge of late adulthood) they are less apparent in terms of the programme mechanisms. Caspi (1984) first applied contact theory (Allport, 1954), which was developed in reference to interracial contact, to the intergenerational setting when he used it to shape an elderly volunteer programme at an elementary school. Contact theory proves a useful guide for intergenerational practitioners because its application fosters positive intergroup interaction, which is the goal of quality intergenerational programmes.
There are four original tenets of contact theory (Allport, 1954) with a fifth tenet specified by Pettigrew in 1998 (Pettigrew, 1998). When achieved, these tenets promote positive contact between members of disparate groups; in the intergenerational field, age is the key dimension of disparity. The five tenets include: support from authority, common goal, cooperation, equal group status, and opportunity for friendship. However, these theoretical principles are less helpful in explaining how intergenerational programmes might work to improve the mental health and wellbeing of children and younger people.
The Disengagement Theory of Aging ( Cumming, 1961) is also helpful in understanding the mechanisms that might lead to social isolation and how intergenerational interventions can mitigate against them. Aging, leads to an inevitable reducintion in ones abilities to come into contact with friends, and relations. Older people gradually loses ties with others in their society and become physically inactive and more lonely when compared to their younger counterparts. Social and economic conditions can influence the environments in which people age, where those with greater resources can access recreation and social activities that promote social engagement and maintain physical and mental wellbeing.
Cumming, 1961) is also helpful in understanding the mechanisms that might lead to social isolation and how intergenerational interventions can mitigate against them. Aging, leads to an inevitable reducintion in ones abilities to come into contact with friends, and relations. Older people gradually loses ties with others in their society and become physically inactive and more lonely when compared to their younger counterparts. Social and economic conditions can influence the environments in which people age, where those with greater resources can access recreation and social activities that promote social engagement and maintain physical and mental wellbeing.
We have developed a logic model (Figure 1) to illustrate our understanding of how intergenerational activities might work to improve the mental health and wellbeing of children and adolescents. The logic model is based on discussions with the stakeholder group during the construction of the evidence EGM (Campbell, 2023) and previously published literature (Ronzi, 2018). The logic model shows how intergenerational interventions can lead to a sense of being valued, of belonging, paving the way for greater self esteem, social connection and wellbeing. The mechanisms and impact may vary for different age groups of children and also for children experiencing very different life circumstances.
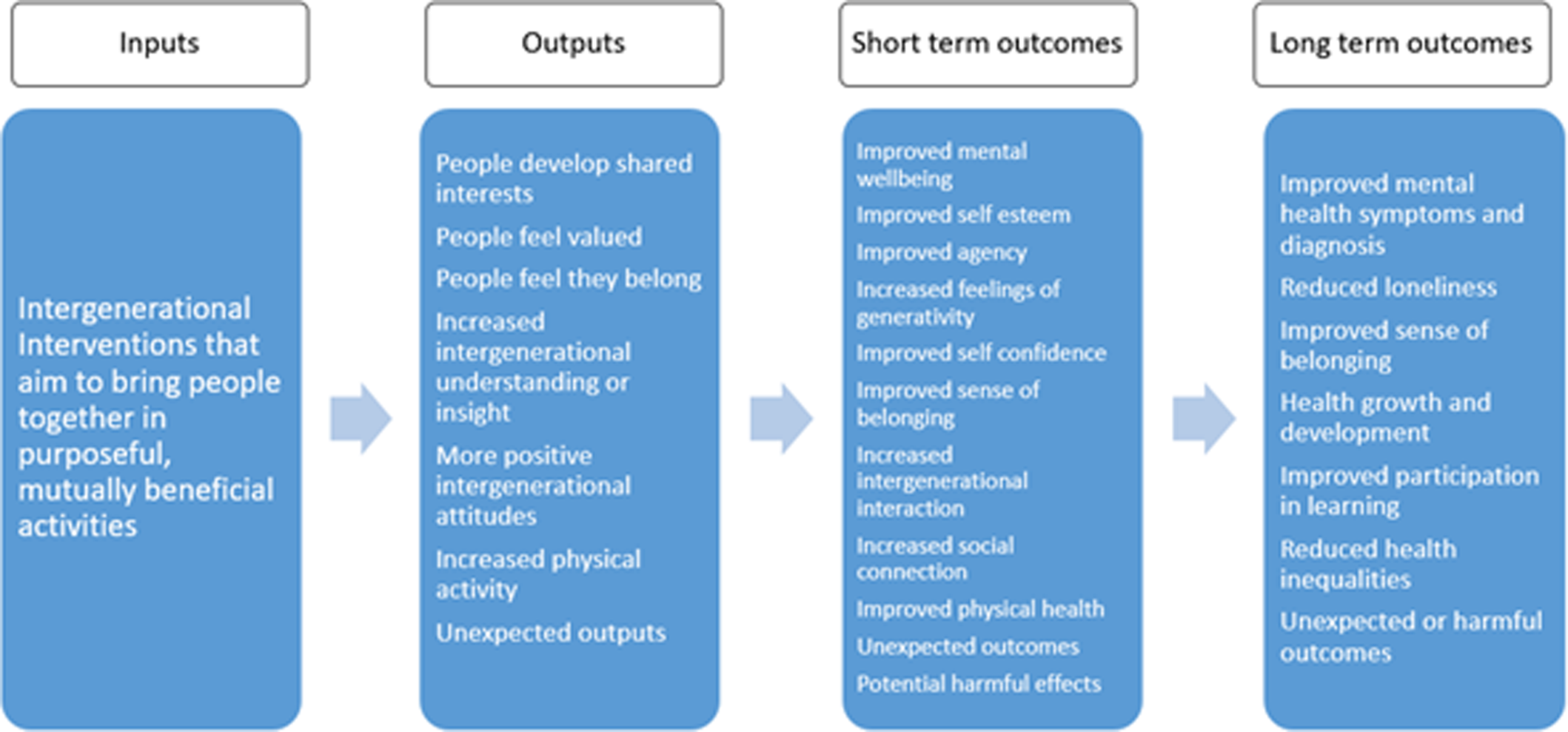
Logic model to illustrate how intergenerational activities might work to improve the mental health and wellbeing of children and young people.
Why it is important to do this review
The state of the UK's generational divide is described in the All Party Parliamentary Group on Social Integration. Healing the generational divide – Interim report on intergenerational connection (APPG, 2019). This report offers a range of recommendations to alleviate the generational divide and intergenerational interventions form a significant part of this.
If intergenerational interventions could also make a difference to mental health and wellbeing – something that has really suffered across the generations particularly over the pandemic then their role in society and each community could be far greater. ‘A New Social Contract for a mentally healthier society’ a report written by Mind (MIND, 2020) in partnership with over 50 voluntary organisations advocates for communities, organisations, agencies and the government to work together to respond to the mental health and wellbeing needs of the nation, evidence based intergenerational interventions may have a substantial role to play in this.
Other UK National Government policies such as the NHS Long Term Plan (NHS, 2019) and the NHS Personalised Care agenda (NHS, 2020) also advocate for sustainable interventions that can appeal to all ages in a whole population approach to personalised care for both mental and physical wellbeing.
Many local authorities have signed up to Public Health England prevention concordat for better mental health (England, 2020) which aims to bring a prevention-focused approach to improving public mental health. The concordat promotes evidence-based planning and commissioning to increase the impact on reducing health inequalities using sustainable and cost-effective interventions that impact on the wider determinants of mental health and wellbeing.
Local governments are also interested in ways to enable or secure positive intergenerational communities and to help generations and multiple agencies work together to improve mental health and wellbeing (‘Generations working together’), and local health and wellbeing board strategies. Globally, there are organisations committed to developing intergenerational programmes, with the purpose of improving the lives of children, youth and older adults (generations united https://www.gu.org/who-we-are/, Australian Institute for International Practice https://aiip.net.au/). This review will contribute to informing practice, and to promoting research to address gaps in knowledge.
Having conducted an EGM on intergenerational interventions we were able to identify areas where reviews have and have not already been conducted and areas where research was more or less prolific. We have identified reviews registered on PROSPERO that cover related areas such as meaningful engagement between adolescents and older people in a residential care setting (Bridget et al., 2020) the design and best practice for intergenerational exchange programmes also between adolescents and older people (Webster, 2019) and features of intergenerational programmes and attitude changes between adolescents and older people (Forbes, 2021).
OBJECTIVES
This systematic review examines the impact of intergenerational interventions on the wellbeing and mental health in children and adolescents and identifies areas for future research as well as key messages for service commissioners.
We sought to answer the following research questions: Are intergenerational activities effective in improving the wellbeing and mental health of children and adolescents? What characteristics of intergenerational activities are associated with a positive impact on the wellbeing and mental health of children and adolescents? What are the underlying theories for the effectiveness of intergenerational activities in children and adolescents?
METHODS
Criteria for considering studies for this review
Types of studies
We included randomised control trials (RCTs) only. This decision was informed by the results of the EGM (Campbell, 2023), which identified eligible RCTs and provide the most reliable source of evidence to address questions of effectiveness. Randomised controlled trials have particular value when questions of effectiveness are being asked, using methods that ensure the effects evaluated can be attributed to the intervention.
Types of participants
We included studies that include older adults and children and young people.
No age boundary restrictions were applied. We included studies that suggest there is at least one skipped generation between older and younger participants. Studies in which participants were related by family or marriage were excluded. No age cut-offs were defined and eligibility was based on criteria used by the included studies of ‘older people’ and ‘young people’.
Types of interventions
Any intervention that brings older and younger people together intentionally with the purpose of achieving positive health and/or social and/or educational outcomes. These include reminiscence programmes, buddysystems, storytelling, school-based interventions and arts based interventions. We used the Depth of Intergenerational Engagement Scale (Kaplan, 2004) as the framework for the interventions. The Depth of Intergenerational Engagement Scale places programmes and activities on a continuum, with points that correspond to different levels of intergenerational engagement, ranging from initiatives that provide no direct contact between age groups (point 1) to those that promote intensive contact and ongoing opportunities for intimacy (point 7).
Interventions at levels 1 and 2 were not included in this review as they do not involve bringing people together, but simply information giving (Table 1).
Examples of intergenerational initiatives fitting into each point on the scale are described below.
Programmes fitting into all points on this continuum provide positive experiences for interacting with persons in other age groups. However, if the aim is ambitious, such as changing attitudes about other age groups, building a sense of community, enhancing self-esteem, or establishing nurturing intimate relationships, a commissioner should focus on programmes that fit into levels 4–7 on the scale. Programmes would take place over an extended period of time, would last anywhere from a few months to many years, and would provide extensive interaction opportunities.
Types of outcome measures
Primary outcomes
The primary outcomes for this review are the wellbeing and mental health of children and young people. Well-being is a concept that is not defined consistently within the literature (Amerijckx & Humblet, 2014). For the purposes of this review, we regard well-being in children and young people as a multi-dimensional concept including subjective sense of well-being, material well-being, health and safety, education, peer and family relationships, behaviours and risks (Adamson & Bradshaw, 2007). Many tools are available to assess mental health and wellbeing in children and young people. We included all outcomes reported using a standardised measure to assess mental health and wellbeing in children and young people.
Secondary outcomes
To address Research Question 1 our secondary outcomes included other indicators of mental health and wellbeing such as assessments of behaviour, physical growth, development and educational outcomes. We also extracted data on any reported adverse outcomes, such as development of negative attitudes, or the effects on children who have experienced ACES where the older person may inadvertently repeat an earlier relationship deficit that the child experienced.
We excluded studies where no outcomes related to child wellbeing or mental health were reported.
Types of settings
Studies undertaken in any setting or context were included.
Search methods for identification of studies
Searches were conducted to populate the EGM (Campbell, 2023) from which this review originates. We have set up automated alerts to identify additional relevant literature which we will use to update the map as the project progresses; any studies identified during this process will be screened for eligibility in the review. We undertook an update search before submission of this review.
Electronic searches
We searched MEDLINE (via OvidSp), EMBASE (via OvidSp), PsycINFO (via OvidSp), CINAHL (via EBSCOHost, Social Policy and Practice (via OvidSp), Health Management Information Consortium (via OvidSp), Ageline (via EBSCOhost), ASSIA (via ProQuest), Social Science Citations Index (via Web of Science), ERIC (via EBSCOhost), Community Care Inform Children, Research in Practice for Children, ChildData (via Social Policy and Practice), the Campbell Library, the Cochrane Database of Systematic Reviews and the CENTRAL database to populate the EGM in July 2021 and updated in July 2023 using terms for intergenerational practices. We were seeking to identify the richest possible evidence base, therefore we did not place any language or date restrictions on the searches. The process of searching and populating the EGM was the source of RCTs included in this review. Our search strategies for the EGM are available in Supporting Information: Appendix 1.
Searching other resources
We also searched for grey literature via relevant organisation websites (Age UK, Age International, the Centre for Ageing Better, Barnado's, Children's Commission, UNICEF, Generations Working Together, the Intergenerational Foundation, Linking Generations, Generations united and The Beth Johnson Foundation), conference abstracts via the Conference Proceedings Citation database, and dissertations via ProQuest Dissertations and Theses Global.
To find any published literature not captured by the databases we reviewed the included studies within relevant systematic reviews and hand searched the Journal of Intergenerational Relationships.
Data collection and analysis
Selection of studies
Studies were identified from the relevant domains of our evidence and gap map (Campbell, 2023) and screened against the eligibility criteria independently by two reviewers. Methods for study selection used to populate the evidence and gap map can be found in the protocol (Campbell, 2023).
Data extraction and management
Once relevant studies had been identified data extraction was undertaken by one reviewer and checked by a second with discrepancies being resolved by discussion and arbitration by a third reviewer were necessary. Data extraction sheets were developed in EPPI-Reviewer and piloted by two reviewers on a sample of papers. We extracted the following data: Publication details, study design, sample size, population details, intervention and comparator details including type of activities undertaken, setting, duration, intensity, timing and mode of delivery, outcome measures, and outcome data. We also extracted details of the underlying theory of change as described by the authors.
Assessment of equity in included studies
We used the PROGRESS Plus framework (O'Neill, 2014) to guide and structure data extraction to describe the socio-demographic characteristics of eligible populations in the included studies. We used this information to describe and assess categories of disadvantage. We also extracted contextual information relevant to potential categories of disadvantage, where available.
Description of interventions used in included studies
We used the TIDieR checklist (Hoffmann, 2014) to describe the interventions used in included studies. The TIDieR checklist contains 12 items that cover the information required to comprehensively describe an intervention. Using the checklist we extracted data on: the name of the intervention, the rationale, what materials and procedures were used, who delivered the intervention, how, where, when and how much, any tailoring or modifications used and any measures of adherence or fidelity.
Assessment of risk of bias in included studies
One reviewer performed the critical appraisal which was then checked by a second reviewer, with discrepancies resolved through discussion. We used the Cochrane risk of bias tool to appraise randomised controlled trials (Higgins, 2019).
Measures of treatment effect
In our protocol we planned to undertake a meta-analysis if appropriate. We planned to calculate Hedges g from means and standard deviations in the first instance.
Given the expected variation across studies, we anticipated using the random effects model and reporting the estimate of chi-squared and the prediction interval for the overall mean effect size.
If studies had multiple arms, where different types of intergenerational intervention were compared with a control, we would have considered pooling the two interventions groups.
Unit of analysis issues
If the included RCTs had used cluster randomisation, we would have undertaken a sensitivity analysis to explore the effects of these studies on the review conclusions. Where included cluster randomised studies failed to report using an appropriate multilevel model to take into account clustering design, we would have sought to undertake an approximate analysis of the cluster-randomised trial using the intraclass correlation coefficient (ICC). If the ICC was not available in the published report, we would have identified external estimates drawn from similar studies (Higgins, 2022). If an ICC was used, only similar studies with similar outcomes would have been included.
Criteria for determination of independent findings
Where there are multiple reports of a single study, these will be reported and linked in the review. Each will have full data collection. Where there are multiple conceptually similar outcomes, the one that is most frequently used across the included studies will be used for the meta-analyses (López-López, 2018). All of the outcomes relating to mental health and wellbeing will also be reported narratively.
Dealing with missing data
If the data was not available within the published papers, we planned to contact study authors to request missing information. No authors needed to be contacted to provide missing data.
Assessment of heterogeneity
If there had been sufficient similarity in the type of interventions and populations being studied, meta-analyses would have been undertaken.
Effect size heterogeneity would be examined using the I 2 statistic. Where there is substantial heterogeneity (>50%), random effects meta-analyses would have been used. Heterogeneity would also be explored using sub-group analysis based on the level of level of intervention.
Assessment of reporting biases
The small number of included studies means that tests for funnel plot asymmetry cannot be used to determine potential reporting bias in this review (Sterne et al., 2011).
Data synthesis
Our approach to undertaking and reporting the methods used for data synthesis was guided by the Synthesis Without Meta-analysis (SWiM) reporting guidance (Campbell, 2020). Meta-analysis was not possible due to the heterogeneity of the interventions, populations and outcomes that were measured. Studies were tabulated and grouped according to, population and intervention characteristics and outcomes, using the logic model to inform decisions on groupings where appropriate. Tables will be used to describe the heterogeneity within the included ei. Where possible, standard metrics for each type of outcome measure were determined.
Sensitivity analysis
We did not undertake a sensitivity analysis in this review.
Treatment of qualitative research
None will be included.
Summary of findings and assessment of the certainty of the evidence
We did not include Summary of findings and assessment of the certainty of the evidence.
RESULTS
Description of studies
Results of the search
Using the EGM created in Spring 2022 and updated in July 2023 (Campbell, 2023) we identified 5 RCTs for inclusion. A further 11 studies were excluded as they did not report outcomes for CYP (Cardona, 2002; Chippendale, 2015; George, 2011; Rook, 2003; Shkilnyk, 1984; Gruenewald, 2016; Low, 2015; Giglio, 2006; Dawson, 2017; Shkilnyk, 1984; Thornton, 2017) (see Figure 2).
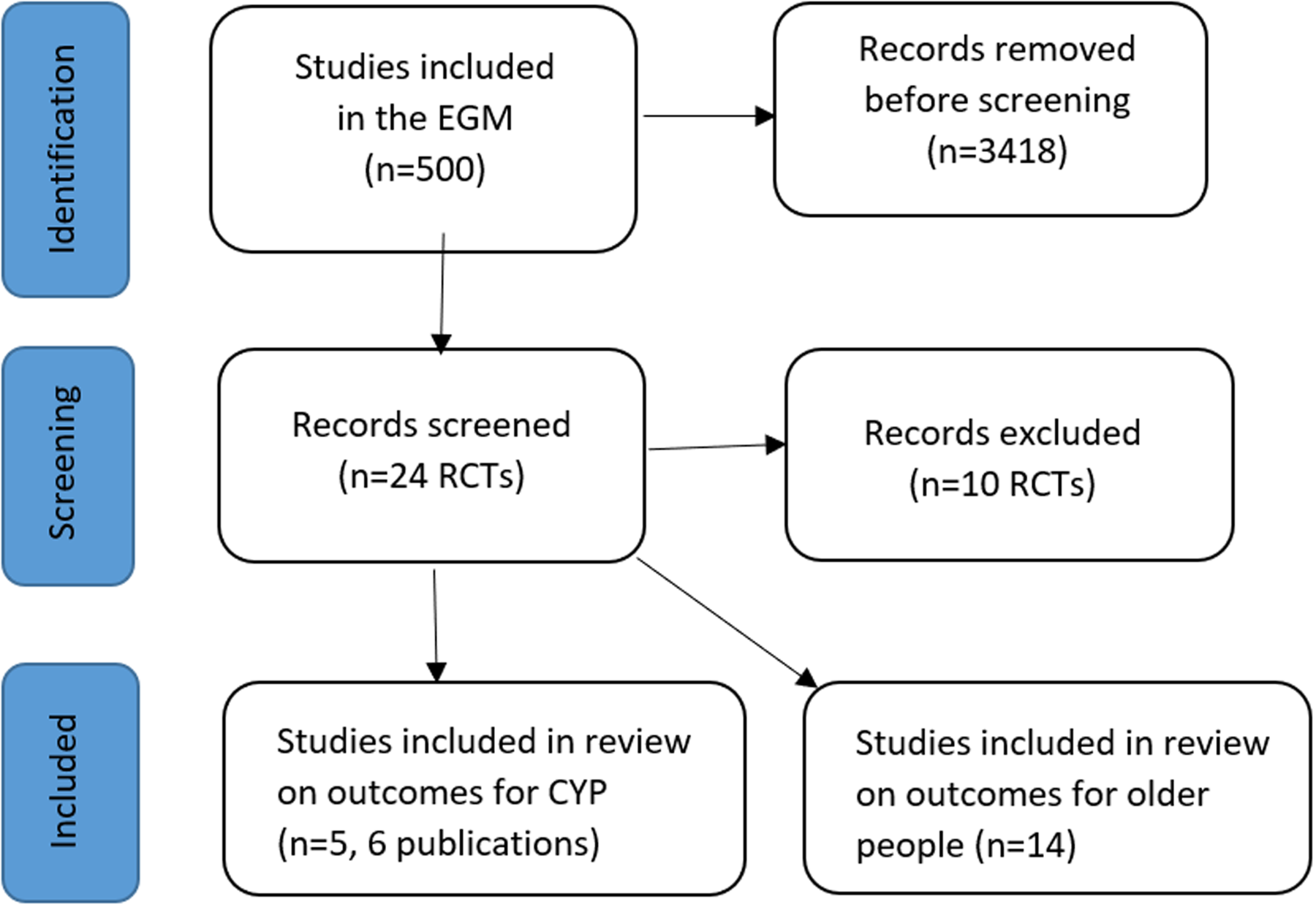
PRISMA flow diagram.
Included studies
Only 5 studies (Carcavilla, 2020; Detmer, 2020; Kessler, 2007; LoSciuto, 1996; Sipsas-Herrmann, 2000) (6 publications (Kessler, 2007; LoSciuto, 1996; Sipsas-Herrmann, 2000; Taylor, 1999; Carcavilla, 2020; Detmer, 2020)) met our inclusion criteria. Two publications reported the results of the same study (LoSciuto, 1996; Taylor, 1999). Three studies (Sipsas-Herrmann, 2000; Carcavilla, 2020; Detmer, 2020) measured and reported mental health and wellbeing outcomes for both older people and CYP and therefore are included in this review and in our accompanying review of the impact of interventions in older people (Whear, 2023). The 5 studies evaluated 5 different intergenerational interventions. Four were based in school settings (LoSciuto, 1996; Taylor, 1999; Sipsas-Herrmann, 2000; Kessler, 2007; Carcavilla, 2020), with two interventions (LoSciuto, 1996; Taylor, 1999; Sipsas-Herrmann, 2000) aimed to prevent negative behaviours (drug use and aggression), one intervention (Carcavilla, 2020) involving the use of on-line conversations to support language learning between secondary school students and older people in care home settings, and another (Kessler & Staudinger, 2007) involving young people and older people working on a project together. One intervention (Detmer, 2020) involved younger, preschool children and utilised music to promote positive interactions. Three studies (Detmer, 2020; LoSciuto, 1996; Sipsas-Herrmann, 2000; Taylor, 1999) were conducted in the USA, one (Carcavilla, 2020) in Italy and Spain and one (Kessler, 2007) in Germany.
Participants
The five included studies (Carcavilla, 2020; Detmer, 2020; Kessler, 2007; LoSciuto, 1996; Sipsas-Herrmann, 2000; Taylor, 1999) varied widely in the numbers of participants recruited (Table 2) with numbers ranging from 32 to 729 CYP, and 15 to 90 older people. In one study (LoSciuto, 1996; Taylor, 1999) the number of older people was not reported. One study (Detmer, 2020) included children in preschool (aged 3–4 years), two (LoSciuto, 1996; Sipsas-Herrmann, 2000; Taylor, 1999) included young adolescents (11–12 year) and two (Carcavilla, 2020; Kessler, 2007) included young people in their mid-teens. In two studies (Carcavilla, 2020; Kessler, 2007) all of the CYP were female, in two (LoSciuto, 1996; Sipsas-Herrmann, 2000; Taylor, 1999) the proportion of male and female participants was nearly equal and in one (Detmer, 2020) gender was not reported.
Stakeholder engagement.
Abbreviations: C, control group; F, female; I, intervention group; M, male; NR, not reported; SD, standard deviation.
In one study (LoSciuto, 1996; Taylor, 1999) the intervention was delivered in a school, within an area with a high proportion of people with low socioeconomic status from minority groups. Otherwise, no interventions specifically targeted children experiencing adversity, evaluating the effects on CYP's mental health and wellbeing.
The ages of the older participants ranged from 60 to 98 years across the five studies. In one study (Kessler, 2007) all of the older people were female, and in two (Carcavilla, 2020; Sipsas-Herrmann, 2000) where the gender of older people was reported, there was a higher proportion of female participants. In two studies (Carcavilla, 2020; Detmer, 2020) the older people were frail or experiencing age-related decline in their physical and cognitive functioning. In both of these studies the older people were living in either a care home or sheltered housing.
Interventions
The interventions were very different in their purpose, methods of delivery, duration and components. Table 3 summarises the interventions.
Participants.
Two studies (Carcavilla, 2020; Detmer, 2020) were designed to improve learning and also promote mutually beneficial interactions, and three to promote pro-social behaviour or reduce negative behaviours. LoSciuto (1996) and Taylor (1999) evaluated a programme (Across Ages) designed to reduce drug abuse among youth at risk due to the environment in which they lived. Another project (SCARE) was designed to equip young adults with skills to better manage anger and aggression (Sipsas-Herrmann, 2000).
The duration of the programmes varied from a one off event (Kessler, 2007), to 6 weeks (Carcavilla, 2020), 8 weeks (Sipsas-Herrmann, 2000), 12 weeks (Detmer, 2020) and 56 weeks (LoSciuto, 1996; Taylor, 1999). Aside from the one off event, the frequency of contact was once or twice weekly. Where specified, the duration of the contact sessions ranged from 30 min to 90 min.
We have classified the types of intergenerational activity using The Depth of Intergenerational Engagement Scale (see Table 1) which places programmes and activities on a continuum, with points that correspond to different levels of intergenerational engagement, ranging from initiatives that provide minimal contact, one-off event (point 3) to those that promote intensive contact and ongoing opportunities for intimacy (point 7) (Kaplan, 2004).
Of the included studies, one (Kessler, 2007) was classified as a level 3 where older and younger people meet each other, as part of a one-time experience. Three (Carcavilla, 2020; Detmer, 2020; Sipsas-Herrmann, 2000) were classified as level 5 demonstration projects. This is where an intergenerational activity is delivered over a defined period of time. Depending on project goals and objectives, the intergenerational exchange and learning can be intensive. These initiatives are often implemented on an experimental or trial basis, and frequently depend on external funding. One (LoSciuto, 1996; Taylor, 1999) was classified to be a level 6 intervention which are ongoing intergenerational programmes, that is, programmes from the previous category that have been deemed successful and valuable from the perspective of the participating organisations and the clientele are incorporated as an integral part of their operation. This extends to programme and staff development such as preparing individuals to work with populations of various age groups.
The content of the included programmes was as follows:
Smile Connect Carcavilla (2020) (Italy/Spain) evaluated a programme that linked older frail people in nursing homes in Spain, with secondary school adolescents in Italy who were learning Spanish. The students and older people used video conferencing as the medium and the programme was designed to help students practice and improve their Spanish language skills, reduce negative stereotypes of older people. The older people were given training to prepare them for their roles as language teachers.
Intergenerational Music Therapy Detmer (2020) (USA) included a music therapy session, led by music therapists in a group setting. The children were aged 4–5 years and older people supported the activities in the session.
The intervention was designed to improve young children's literacy and older peoples physical functioning and self worth.
Social Interaction Kessler (2007) (Germany) This programme was run as single events that brought older people and teenagers together to work in group and one to one on a problem solving task.
Across Ages LoSciuto (1996); Taylor (1999) (USA) This mentoring programme, matched older people to one or two students. They met with them in both group and one to one settings with the purpose of helping to build their resistance to drug abuse, and to build their skills to deal with challenges encountered in the urban poor environment in which they lived. The activities included working together on art and craft activities, playing games, working on environmental projects, and visiting care homes. The older people were rigorously selected and given regular training and a payment each month.
SCARE (Student Created Aggression Replacement Education) Sipsas-Herrmann (2000) (USA) The objective of this programme was to provide early adolescents with life skills to manage emotions, particularly anger and aggression. Older people were trained to deliver the intervention and were assigned to work with groups of 8–12 students in pairs. Ongoing support and training was provided to the older people delivering the intervention.
Comparator groups
Comparison groups also differed across the studies. One study (Detmer, 2020) used a wait-list control group, that commenced the intervention after the intervention group had completed the intervention. The wait-list group received a shortened version of the intervention. In the other studies the control group received an alternative intervention, or one that did not include working with older people. One study (LoSciuto, 1996) included three arms, two groups received the intervention but only one which included mentoring by an older adult. The control group received no intervention. Two studies (Carcavilla, 2020; Sipsas-Herrmann, 2000) used an alternative intervention as the control group (Table 3 for a summary of the interventions).
Theoretical support for interventions and how they might work
All of the included interventions are underpinned by theory (‘reason-giving’) that informs the format of the intervention and the expected outcomes (Davidoff, 2015). For example, the theory that ageist attitudes in young people can be challenged and thus altered, by positive interactions with older people underpins many of the designs of intergenerational interventions (Table 4).
Summary of theoretical frameworks.
The five included studies each adopted different approaches to positively influencing children and young people's wellbeing and mental health. In two studies (Kessler, 2007; Carcavilla, 2020) the young people gain a sense of value and wellbeing, through engaging with and/or providing emotional support and empathy to an older adult. In one study the benefits for the young person comes from their improved learning (literacy) (Detmer et al., 2020). In two the benefits for young people come through both learning and developing social skills through the formation of a relationship and mentoring, with older people acting as both a support and an example to the young person. There was no consistency in the theoretical approaches cited by the authors to support the programme.
Risk of bias in included studies
The overall risk of bias in the included studies was high with only. one small study (32 children) describing adequate methods of randomisation, and blinding at outcome assessment (see Figure 1).
In three studies (LoSciuto, 1996; Taylor, 1999; Kessler, 2007; Carcavilla, 2020) although the method of allocation to groups was described as randomised, the methods were not described. In one (Sipsas-Herrmann, 2000) the process was not randomised for all of the participants. Only one study (Detmer, 2020) was considered at low risk of bias for randomisation, describing using a randomisation table to undertake randomisation.
None of the studies described efforts to ensure adequate allocation concealment. Only one study (Detmer, 2020) included blinding of outcome assessment.
Attrition of study participants was described in one study (Sipsas-Herrmann, 2000), however it is unclear if there was an intention to treat analysis. In another, it was not clear which groups lost participants in the follow-up, and there was no intention to treat analysis (LoSciuto, 1996).
Overall, the quality of the included studies means that we can have limited confidence in the findings reported and introduces a risk of bias.
Effects of interventions
Note: ‘Effects of interventions’ heading will be removed at publication stage.
Synthesis of results
The focus of this review is the impact of intergenerational interventions on the mental health and wellbeing of young people. We included diverse measures of wellbeing, including measurement of positive behaviours, education, subjective well-being, peer and family relationships and material well-being reflecting the multi-dimensional nature of well-being (Adamson & Bradshaw, 2007). We excluded studies that only evaluated changes in attitudes to aging amongst the children and young people.
None of the studies used a common measure to evaluate the outcome of the intervention on the younger participants. The heterogeneity between the interventions, and the outcomes used to measure their impact prevented pooling of study outcomes. The variety of wellbeing attributes and the measures used are shown in Table 5. The included studies used validated measures such as the PANAS (Positive and Negative Affect Scale) (Carcavilla, 2020), RAND (Measure of Health Related Quality of Life) (LoSciuto, 1996; Taylor, 1999), STAXI (State-Trait Anger Expression Inventory), AGVQ (Attitude Towards Guns and Violence Questionnaire) (Sipsas-Herrmann, 2000), PPVT (Peabody Picture vocabulary Scale) and also tools designed for the study such as letter name and sound recognition (Detmer, 2020). Another study used willingness to volunteer as a measure of pro-social behaviour (Kessler, 2007).
Outcomes measured in each included study.
Note:
Learning and school outcomes (Table 6)
Summary of outcomes.
Note: NS: p value > 0.05; CG, control group; IG, intervention group.
One study that evaluated the effectiveness of the Intergenerational Music Therapy (Detmer, 2020) which was led by music therapist in a group setting with children aged 4–5 years and older people supported the activities in the session, reported on three learning outcomes – the Peabody Picture Vocabulary Test – III (PPVT); letter name (LN) and letter sound (LS) – and found that although there were some improvement in terms of changes from baseline in one of the two intervention groups (involving younger children where older people supported young children with literacy learning) for one outcome only, there was no evidence of a difference between groups for any outcome.
A further study that examined the effectiveness of the Across Ages 44 mentoring programme, which matched older people to one or two students, found no impact on attitudes toward school (NS).
Positive emotions/prosocial behaviour
One study evaluating the Smile Connect (Carcavilla, 2020) programme that linked older frail people in nursing homes in Spain, with secondary school adolescents in Italy who were learning Spanish to control aggression in themselves found no significant impact on positive (NS) or negative (NS) emotions.
A year long, school based programme (SCARE) (Sipsas-Herrmann, 2000), designed to help young people reduce their anger and control aggression in themselves and that used the STAXI measures of Trait Anger and Anger Control found some improvements from baseline measures but there was no significant difference between the two groups in outcome scores (NS). There was, however, an improvement in the AGVQ (Attitudes Toward Guns and Violence Questionnaire) between the intervention group (IG) and (C) (p = 0.038) and the two different versions of the intervention (IGa and IGb) (p = 0.002).
An evaluation of the Social Interaction (Kessler, 2007) programme, which was run as single events that brought older people and teenagers together to work in group and one to one on a problem solving task, found a significant impact on prosocial behaviour in terms of willingness to volunteer (p, 0.001).
One study that examined the effectiveness of the Across Ages (LoSciuto, 1996; Taylor, 1999) mentoring programme, which matched older people to one or two students, found a trend favouring the intervention group in), mental wellbeing (p = 0.58) and a significant improvement in attitudes toward substance misuse (p = 0.042).
DISCUSSION
Summary of main results
Five randomised controlled trials met the inclusion criteria, despite a large body of evidence located and included in the mapping review and EGM (Campbell, 2023). This review focuses on the impact of intergenerational interventions on the mental health and wellbeing of children and young people, and this outcome was infrequently measured in the young participants. We found that the types of interventions ranged from one-off sessions to ones that spanned a year, and where the goals also differed. The goals included promoting social skills, preventing harmful behaviour and promoting learning. The CYP included in the studies also varied, with one targeting younger children and two targeting younger teenagers and two targeting older teenagers. Only one study targeted socioeconomically disadvantaged children, and in the other studies the socioeconomic backgrounds of the children and young people are not described. We also found that the outcome measures used to evaluate the effectiveness of the interventions also varied, with none of the studies measuring the same outcomes making comparisons across studies difficult. Only one study showed improvements in wellbeing measures, and this was an intervention delivered to children in deprived neighbourhoods, where the theory underpinning the intervention included developing resilience and where the intervention duration was for a year allowing the development of a greater depth of relationship between the CYP and older person.
Overall completeness and applicability of evidence
The evidence for the effectiveness of intergenerational interventions on the mental health and wellbeing of children and young people is limited and inconclusive. Too few evaluations have sought to measure how intergenerational interventions impact children and young people and where this impact is measured the focus is usually limited to attitudes to aging. The evidence that has been collected is too heterogenous to allow synthesis of the findings. The underpinning theories to support their development are poorly described with no follow-up data to ascertain if benefits are maintained.
We used the PROGRESS plus framework to describe which characteristics were captured and/or targeted in the RCT research on intergenerational interventions. Many equity characteristics were not reported. Gender was the most commonly reported characteristic of the CYP involved in the studies. This was not accounted for in the analyses.
We also looked to see if any of these characteristics were specifically targeted by the interventions captured in this review. Only one study (LoSciuto, 1996) targeted CYP in socioeconomically deprived neighbourhoods.
Quality of the evidence
The heterogeneity in the interventions, and measures, and overall poor quality of the study designs of the included studies means that there is insufficient evidence to demonstrate that interventions improve the wellbeing of children and young people. There is a need for robust evaluations of interventions, and particularly the assessment of these interventions on the mental health and wellbeing of children and young people. Currently the value of these interventions for children and young people, beyond measuring the impact on attitudes to the elderly, is rarely considered, and remains poorly tested. While there is a perception of potential benefit, this has not been demonstrated in this review.
Potential biases in the review process
This review only included randomised controlled trials and therefore has not drawn on other sources of evidence that may yield insights into intervention effectiveness. However, by focusing on RCTs as a robust method of demonstrating the effect of intergenerational interventions we have shown that even studies that use an RCT methodology lack rigorous evidence to support their use.
Social care interventions, may evolve and become embedded within a system without formal evaluation. We anticipate that our review may not represent current practice. It does highlight the lack of the strong evidence necessary to support funding and investment. It also demonstrates a need for evaluations that allow useful reflection on which elements support intervention effectiveness.
A further limitation of this review is that we limited our inclusion criteria to studies that reported mental health and well-being outcomes. It is possible that these outcomes were measured but not reported. While this will not change the conclusions of our review, it should be noted that the limited number of included studies may reflect selective reporting of outcomes.
Agreements and disagreements with other studies or reviews
We identified 26 systematic reviews that were included in the EGM (Campbell, Whear, et al., 2023), very few explored the impact of intergenerational interventions on children and young people's outcomes. Reviews that considered the impact of intergenerational interventions on children and young people, focused on studies that evaluated the impact on attitudes to older people and aging (Gualano et al., 2018). A scoping review (Giraudeau & Bailly, 2019) found that evaluation of intergenerational interventions focused on attitudes, behaviours, confidence and competence in children while focusing on the mental, physical and quality of life impact on older people. Two reviews (Peters et al., 2021) (Jarrott et al., 2021) highlight the lack of evidence to support intergenerational interventions and the need to demonstrate their potential impact on mental and social wellbeing. All current reviews support our finding, that there is a need for rigorous implementation research to further advance evidence based intergenerational practice. Intergenerational practice, has as a central tenet, the need to be mutually beneficial for both generations. It is clear from our review that to date, the measured impact on children and young people has largely focused on assessing attitudes to aging, not on CYP health and wellbeing. If policymakers and practitioners want to advocate for the implementation of intergenerational interventions, the value of these types of interventions for children and young people need to be more effectively sought, measured and demonstrated.
AUTHORS' CONCLUSIONS
Implications for practice and policy
Intergenerational interventions show promise but researchers have failed to measure how they impact on the mental health and wellbeing of children and young people. This is a serious limitation of the evidence base that needs to be addressed in robust and rigorous evaluations. Appropriate tools need to be used in evaluating these types of interventions to ensure the outcomes that matter are measured, and also to build evaluation that observes their longer term effects. Only a limited number of evaluations have been undertaken focusing only upon a small number of the many types of interventions developed. As a result there is little evidence to identify what features of intergenerational interventions contribute to greater effectiveness. The theoretical basis upon which intergenerational interventions are designed are frequently omitted from a description of the intervention. A better understanding of their effectiveness components will facilitate progressive improvements in these interventions. Commissioners and intervention developers should ensure interventions provide sufficient theoretical evidence for the proposed intervention. There is a pressing need to identify outcomes that are important and measurable to assess the impact of these interventions on communities.
Implications for research
Research on intergenerational interventions needs consistent and agreed measures for reporting outcomes including community outcomes. Study sample sizes need to be larger to understand how interventions impact different members of society differently and how any impact remains for the long term. Research methods would benefit from establishing outcomes for a given population from a variety of perspectives to overcome issues of bias from the lack of blinding of self report measures by self report. Research on intergenerational interventions should measure outcomes for BOTH the older and younger population engaged in the intervention – these may or may not be the same outcomes reflected in both populations. Further research is needed on the longevity of outcomes (whether participants need sustained involvement in an ‘intervention’ to continue to benefit) and sustainability of interventions beyond the initial funding of the research project – interventions that are initiated for the duration of a research project and then end (usually within a year) are not helpful.
Footnotes
ACKNOWLEDGEMENTS
Acknowledge the contribution of people not listed as authors of the review, including any assistance from the Campbell Coordinating Group.
CONTRIBUTIONS OF AUTHORS
FC, JTC and AB designed the methods for the review. FC and RW undertook the development of the protocol. LW and JB offered topic expertise in the preparation of the review protocol. AS, MR provided expertise in the search strategy. AT provided expertise on dissemination plans.
DECLARATIONS OF INTEREST
Please declare any potential conflicts of interest. For example, have any of the authors been involved in the development of relevant interventions, primary research, or prior published reviews on the topic?
SOURCES OF SUPPORT
DIFFERENCES BETWEEN PROTOCOL AND REVIEW
None.
REFERENCES
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.