
Abstract
Habitual self–control is defined as a trait–like personal resource factor that facilitates the enactment of difficult intentions. A 14–item Habitual Self–Control Questionnaire (HSCQ) was developed to assess this trait. Reliability, factorial validity, and criterion validity were assessed in five undergraduate student subsamples with an overall N of 2224. Internal consistency was .81 across the entire sample, and test–retest reliability was .83 over a one–month interval. The HSCQ showed a theoretically meaningful pattern in terms of convergent and discriminant validity and criterion validity in predicting a variety of health behaviours that relate to self–control, including exercise, dieting behaviour, binge eating and weight loss success. Further, the HSCQ contributed uniquely to the prediction of health behaviours beyond alternative self–control scales. In a longitudinal part of the study, the HSCQ added to the prediction of action plan completion and satisfaction beyond motivation and moderated the relationship between motivation and enactment of action plans as theoretically expected. In sum, the results provided strong evidence for the reliability and validity of the HSCQ and highlighted some theoretically meaningful differences to already existing measures of self–control. Theoretical implications are discussed. Copyright © 2012 John Wiley & Sons, Ltd.
From ancient Greek philosophy to modern psychology, the concept of self–control and its role in human agency has fascinated mankind. Self–control refers to a genuinely human ability to change the course of one's actions through deliberation. Many different models and definitions have been developed in an attempt to describe and explain what self–control entails. A common ‘denominator’ in most definitions seems to be the idea of a conflict between two competing behavioural tendencies: one based on a specific goal or norm, the other based on hedonistic drive. Further, most definitions share the notion that the goal–oriented or norm–oriented behaviour would not be enacted without effortful suppression of the competing desires or impulses, which, if unchecked, would win the battle. In this sense, self–control can be defined as an ability to reject strong concurrent urges to indulge in some hedonistic or impulsive behaviour that interferes with goal–oriented or norm–oriented activities.
Beyond these common grounds, definitions of self–control vary widely. Self–control has been used as a synonym for self–regulation (Carver & Scheier, 1982; Miller, Galanter, & Pribram, 1960), delay of gratification (Mischel, Shoda, & Peake, 1988), volition, willpower, strength of will (Baumeister, Roberts, & Hogan, 2001; Muraven & Baumeister, 2000), or simply a set of self–control skills or strategies (Kuhl, 1985; Mahoney, 1977; Skinner, 1953). Self–control also has been applied to a wide variety of human behaviours and defined in terms of the entity that is controlled, including such diverse targets as the control of emotions (Ochsner & Gross, 2005), impulses and desires (Zabelina, Robinson, & Anicha, 2007), morals (Baumeister & Exline, 1999), prejudice (Muraven, 2008), health behaviour (Glassman, Werch, & Jobli, 2007; Schroder & Schwarzer, 2005) and persuasion (Burkley, 2008).
Given the diversity of the ideas surrounding self–control as a human ability, the development of any new measure of self–control must start with an explication of its theoretical background and a definition of the domain to be assessed. In this paper, we introduce a new measure for the assessment of ‘habitual self–control’. As the name implies, the scale was developed to assess relatively stable individual differences in self–control. In the following, we first describe the theoretical background of the Habitual Self–Control Questionnaire (HSCQ) and define self–control on the background of this theory. Next, we review existing measures of self–control in the literature to outline unique features yielded in the new HSCQ. Finally, we report about the results of three studies testing the reliability and validity of the HSCQ.
The HSCQ has its roots in action control theory (Achtziger & Gollwitzer, 2010; Gollwitzer, 1993; Gollwitzer & Brandstaetter, 1997; Kuhl, 1985; Schwarzer, 1992). Action control theory (ACT) holds that motivation is insufficient to support ‘difficult’ intentions. Intentions are difficult to sustain if they do not derive from intrinsic desires or drives but require effort and the enactment of typically non–hedonistic behaviour. Difficult intentions require self–control because when compared with consummatory or impulse–driven behaviour the rewards are neither immediate nor an inherent part of their enactment. Typically, the rewards are delayed, depend on the achievement of a certain goal criterion or norm, and oftentimes require engagement in unpleasant behaviours, thus establishing an approach–avoidance conflict. Difficult intentions need to be protected against more pleasurable or impulse–driven action alternatives (Achtziger & Gollwitzer, 2010; Kuhl, 1985). ACT theorists coined the term ‘volitional control of action’ to explain this shielding of difficult intentions against more attractive action alternatives. Traditionally, the term ‘self–control’ has been used instead.
One problem with the self–control concept is explaining its source of energy. If an intention is ‘underpowered’ by motivation alone, additional factors must come into play to account for the energy required to apply self–control. According to ACT, self–control is powered by volition. Volition results from a specific kind of intention that needs to be distinguished from other forms of decisions. This type of intention is sometimes called ‘goal intention’, and it is characterised by a strong commitment (Achtziger & Gollwitzer, 2010; Heckhausen & Beckmann, 1990; Kuhl, 1985). With the same idea in mind, Henden (2008) uses the term ‘resolution’ to distinguish those intentions that are characterised by a strong commitment and thus, receive priority status from ordinary intentions without a specific commitment.
On the background of ACT, we propose that self–control can only be measured relative to the intentions a person has formed. For example, if a person is not interested in weight loss, self–control cannot be assessed in terms of body weight or the adoption and maintenance of a calorie–restricted diet, as suggested by some authors (Brandon, Oescher, & Loftin, 1990). Therefore, assessing self–control in terms of specific behaviours or achievements does not make sense unless an intention towards these behaviours or achievements has been established. A strong commitment to these intentions will facilitate self–control at the time of enactment when non–hedonistic characteristics of goal–directed behaviours are particularly likely to jeopardise action plans. Naturally, the more commitments a person has formed, the more likely this person will be to apply self–control to a wide variety of different behaviours and circumstances. However, although commitments can provide volitional energy enabling a person to shield a difficult intention against alternative desires, impulses and action tendencies, not all people are equally likely to stick to their resolutions or, alternatively, to form the strong and stable resolutions required for persistent goal pursuit, pointing to inter–individual differences in self–control ability (Baumeister, Heatherton, & Tice, 1994; Muraven & Baumeister, 2000).
What are the implications of ACT for the definition and measurement of inter–individual differences in self–control? To describe and assess this trait, we use the term ‘habitual self–control’ and define this construct as a relatively stable propensity towards persistent goal pursuit. We claim that self–control cannot be assessed independently from intentions. First, a goal must be implied when asking respondents to rate their self–control. Second, difficulties must be implied in terms of internal or external barriers, desires or temptations that render the enactment of an intention difficult. Third, self–control must be assessed in terms of a continued effort to act in accordance with one's resolutions.
Few measures of self–control exist in the literature, and none of them are based on ACT (for an excellent review of existing self–control measures, see Tangney, Baumeister, & Boone, 2004). One of the best–known and oldest measures of self–control is Rosenbaum's (1980) Self–Control Schedule developed to assess an individual's tendency to apply self–control methods to the solution of individual problems. This includes, for example, controlling depressed mood, unpleasant thoughts, nervousness, tension and anger, as well as the ability to divert one's attention from physical pain or hunger. Although this measure may well be able to predict and explain the absence of behavioural problems, it clearly focuses on societal norms of functioning and not on the likelihood to act in accordance with personal resolutions. Further, more recently, Tangney et al. (2004) introduced a new measure of self–control based on Baumeister's strength model of self–control (Baumeister, Vohs, & Tice, 2007). This measure was developed with the explicit purpose of testing the general success hypothesis or benefits hypothesis of self–control and targets four major domains of self–control: the control of thoughts, emotions, impulses and performance (Tangney et al., 2004). Among these domains, only the control of performance is directly relevant to self–control as defined on the background of ACT, and even performance is only relevant when it is linked to a commitment or resolution. Assessing the control of thoughts, emotions and impulses is nonessential in a measure of habitual self–control that focuses exclusively on goal pursuit unless these internal responses interfere with goal attainment and/or evolve as the direct target of a person's intention to change. Therefore, as long as control of emotions is not required to achieve a specific goal, assessing a person's affinity towards emotion control will add nothing to the prediction of goal attainment. From this perspective, like other self–control skills and strategies, the control of thoughts, emotions and impulses are subordinate to habitual self–control, defined as a propensity towards persistent goal pursuit. Emotion control, thought control and impulse control refer to specific skills that will increase the likelihood of success in goal attainment only if instrumentally applied towards a person's goals. In conclusion, a measure of habitual self–control should not be interchangeable with a dispositional measure of impulse control or emotion control, although these constructs and measures would most certainly overlap.
A trait concept of self–control as defined on the background of ACT has much to offer in the context of intention–based theories of behaviour such as the Theory of Planned Behaviour (Ajzen, 1991). Motivational models such as the Theory of Planned Behaviour have provided much insight in the cognitive processes leading to intention formation, including attitudes, subjective norms and perceived behavioural control but lack details regarding the processes and skills required to shield an intention against competing action tendencies and to strengthen the intention–behaviour congruence. Intentions can be expected to differ in their quality and their long–term motivational underpinnings dependent on the cost–benefit balance and ambivalence regarding goal–related behaviours, specifically if the required future actions are non–hedonistic. Rational decisions may fail when enactment turns out to be more difficult than foreseen. Therefore, without the inclusion of trait–like self–management skills and self–control abilities, motivational models of behaviour are limited in their ability to predict long–term maintenance of behaviour change such as required in the adoption of a healthy lifestyle.
The HSCQ was developed to assess individual differences in intention–behaviour congruency. In contrast to already existing measures of self–control (e.g., Rosenbaum, 1980; Tangney et al., 2004), the HSCQ focuses explicitly on action control and de–emphasises emotion–focused or coping–focused aspects of self–regulation. Originally developed and validated in German, the HSCQ was recreated in English and subsequently modified to test and improve its reliability. In German studies, the HSCQ showed internal consistencies between .71 and .79, a test–retest reliability ≥.63 over a six–month period and construct validity in predicting dieting behaviour in a sample of coronary artery bypass patients advised by their physicians to control their weight and adopt a healthy diet (Schroder & Schwarzer, 2005).
In the present paper, we report about the 14–item English version of the HSCQ and provide evidence for the reliability and construct validity of this measure. Although based on the same definition and background, the English version reflects a new development rather than a mere item–by–item translation of the German original (Schroder, Davies, Bennion, & Larsen, 2008). The English HSCQ was developed on the basis of an initial 18–item version that was gradually reduced over time, first to a 16–item, then to the current 14–item version. Item removal was guided by item–total correlations, which first led to the elimination of two items with rit−i < .25, then to the removal of two more items with inconsistent performance (rit−i) over several student samples. One item was slightly rephrased (item 11, see result section). In the present study, apart from presenting item and scale statistics and exploring the dimensionality of the 14–item HSCQ, the following hypotheses were tested:
The HSCQ measures a relatively stable and internally consistent trait, as indicated by internal consistency and test–retest reliability analyses. The HSCQ will show convergent validity with alternative measures of self–control but show sufficient uniqueness in terms of non–shared variance (r2 < .49) to justify its introduction as a distinct measure of self–control. In terms of discriminant validity, the HSCQ is expected to clearly differ from other measures of personality and emotional adaptation distinguished in the literature. In terms of criterion validity, the HSCQ is expected to predict health–related behaviours as long as they can be associated with a person's specific goals that typically require a conscious decision and commitment (healthy eating, weight control, exercise). In contrast, the HSCQ is not expected to predict recreational substance use (e.g. alcohol consumption, smoking) in persons without an explicit goal towards restraint. The HSCQ contributes to the prediction of intention enactment beyond motivational variables. The HSCQ moderates the relationship between motivation and goal attainment following the formulation of action plans. Specifically, if motivation alone is not sufficient to support the enactment of intentions, habitual self–control will improve the likelihood of successful completion of action plans.
Samples and measures
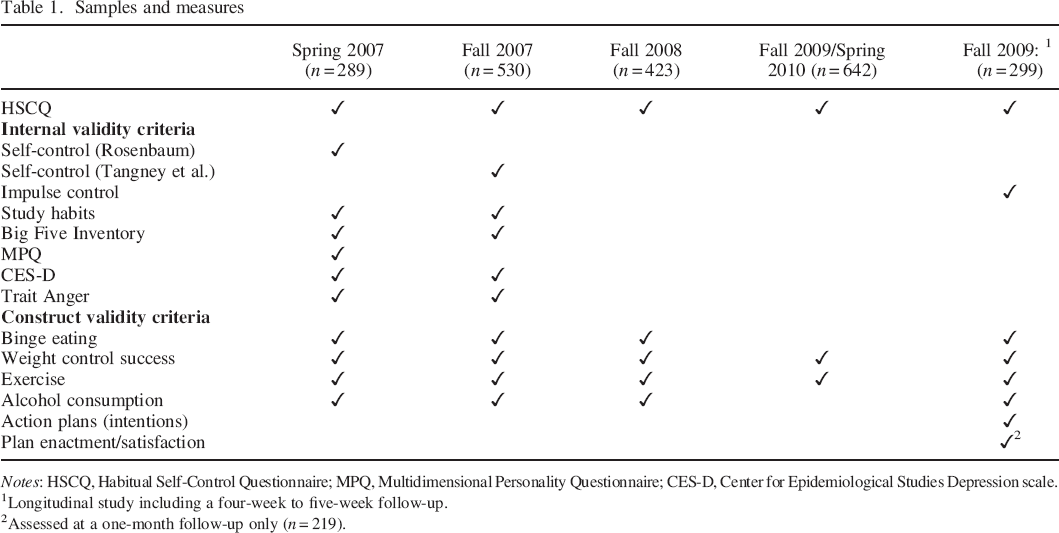
Notes: HSCQ, Habitual Self–Control Questionnaire; MPQ, Multidimensional Personality Questionnaire; CES–D, Center for Epidemiological Studies Depression scale.
Longitudinal study including a four–week to five–week follow–up.
Assessed at a one–month follow–up only (n = 219).
Method
Data were collected at a university in Northern Utah between Spring 2007 and Spring 2010, involving a total N of 2224 participants. Five distinct subsamples were recruited. Each received a different set of variables to test the diverse hypotheses of this study without placing extensive burden on study participants. Table 1 lists the samples and the measures collected in each. In the following section, characteristics of the combined sample are described.
Sample
The sample consisted of 939 male (42.3%) and 1279 female undergraduate students. Age ranged from 18 to 56 years (M = 20.29, SD = 3.46). Most of the students were white, non–Hispanic (n = 1987, 89.3%), with 109 (4.9%) Hispanics, 48 (2.2%) Asians, and 56 (2.5%) belonging to other ethnic/racial groups. Religious affiliations were self–reported as follows: 1789 (80.4%) were LDS (The Church of Jesus Christ of Latter Day Saints, reflecting the predominant religious affiliation in Northern Utah), 86 (3.9%) were Catholic, 26 (1.2%) were Protestant, and 115 (5.1%) belonged to other religious groups. Further, 188 participants (8.5%) indicated not being religious. Most students were single (n = 1960, 88.1%), with only 215 (9.7%) married and 31 (1.4%) divorced. Ninety–three participants (4.2%) had at least one child. The present study focuses on 2183 participants who completed the HSCQ.
Procedures
Recruitment commenced through announcements in undergraduate classes where students could sign up for the study and received information on how to access the online survey on Blackboard using their student ID. Students provided informed consent online by indicating they had read and understood the consent form posted on the home page and agreed to participate. Consent was required to access the survey. Completing the survey took about an hour for each sample, and students received extra credit or course credit for their participation. All procedures were approved by the Institutional Review Board.
In Sample 5, recruited in Fall 2009, those who had completed the online survey received an invitation to participate in a second assessment session to be completed four weeks later. The second assessment offered the opportunity to assess test–retest and predictive validity of the HSCQ. Interested participants were asked to provide contact information to allow for reminder emails and phone calls four weeks later when the second survey was made available. The second survey included the same measures as the initial online survey. In addition, the longitudinal design in this sample allowed testing for individual differences in intention–behaviour congruence. For this purpose, the initial survey included a section asking participants to describe three distinct action plans (intentions) for the subsequent four–week period. Participants were instructed to report on action plans that would not be easy to perform and/or maintain, such as exercising three times a week, increasing vegetable/fruit intake, reducing time spent on computer games, or studying more regularly. Participants were informed that ‘typically such action plans refer to something that bothers you or is important to you or your future but does not come easily or “naturally” to you’. Also, participants were advised to be as specific as possible in formulating their intentions. Guided by examples, participants specified three intentions (open answer) and subsequently rated each in terms of importance and subjective certainty of completion (self–efficacy) on a scale from 0 to 100. At the four–week follow–up, participants reported about their performance in a personalised action plan completion survey, which they received by email. They were asked to return this survey as an email attachment in Blackboard prior to receiving access to the remaining parts of the follow–up survey. Participants received additional course credit or extra credit for their participation in the follow–up survey.
Measures
Habitual self–control questionnaire
The 14 items of the HSCQ were formulated to reflect an intention or commitment to complete a task and to assess the person's perceived ability to stick to their intentions. Because intentions can differ widely across individuals, the items remain unspecific with regard to the type of goal or behaviour target, leaving it up to the respondent to apply the item to a goal or task of personal relevance. Two items were specifically included to emphasise the trait nature of the HSCQ. One item assesses a general attitude toward self–control in contrast to the preference for a more spontaneous lifestyle (item 11). Another item assesses self–control in retrospect asking about the person's perceived ability to control unwanted habits in the past (item 14). In all samples, the HSCQ was presented with a 5–point response scale with 1 = disagree strongly, 2 = disagree a little, 3 = neither agree nor disagree, 4 = agree a little, and 5 = agree strongly. Items 4, 8, 9, 11 and 13 were negatively phrased (indicating lack of self–control) and had to be reversed. A total score was created by summing the items of the HSCQ after reversing the negatively phrased items and substituting single missing responses with the individual item mean. Item content, item statistics, reliability and validity information are reported in the results section.
Alternative self–control scales
Two alternative measures of self–control were employed to test for convergent validity. Participants in Spring 2007 completed the Self–Control Schedule (SCS) of Rosenbaum (1980). The SCS is a 36–item measure assessing the tendency to apply self–control strategies to behavioural problems. Internal consistencies reported in the literature typically ranged between .72 and .91, and test–retest correlations over four weeks and 11 months were reported as .86 and .77, respectively (Fischer & Corcoran, 1994). Sample items are ‘When I do a boring job, I think about the less boring parts of the job and about the rewards I will receive when I finish’ and ‘By changing my way of thinking, I am often able to change my feelings about almost anything’. The items were presented with 6–point response scales ranging from +3 (= very characteristic of me) to −3 (= very uncharacteristic of me). Cronbach's alpha was .87 in the present sample. Further, participants recruited in Fall 2007 completed the 36–item Self–Control Questionnaire (SCQ) developed by Tangney et al. (2004). The SCQ is broader in range than the HSCQ and contains four domains of self–control including thoughts, emotions, impulses and performance. Tangney et al. define the construct assessed by the SCQ as the ability to override inner responses as well as to interrupt undesired behavioural tendencies (such as impulses). A sample item is ‘I am good at resisting temptation’. As suggested by the authors, the SCQ was presented with a 5–point response scale ranging from 1 = not at all to 5 = very much. The authors report high internal consistencies of alpha = .89 and a test–retest reliability of .89 over a three–week period. Validity was established by correlating self–control with a variety of criterion measures indicating that people with high SCQ scores display higher grade point averages, greater psychological adjustment, fewer behavioural problems such as binge eating and alcohol abuse and better interpersonal skills (Tangney et al., 2004). Coefficient alpha was .90 in the present study.
Impulsiveness versus impulse control
Participants in the longitudinal study conducted in Fall 2009 completed a revised 30–item version of the Barratt Impulsiveness Scale (BIS–11) developed by Patton, Stanford, and Barratt (1995). Like the previously mentioned self–control measures, the BIS–11 was found to be multidimensional, involving six first–order and three second–order factors (attentional impulsiveness, motor impulsiveness, and directional (non–planning) impulsiveness). The authors reported good internal consistencies ranging from .79 to .83 for the total BIS across a variety of samples. Discriminant validity was shown with significantly greater mean scores among substance abuse and general psychiatry patients than among undergraduate students. In the present sample, the internal consistency of the BIS–11 was α = .83. Item scores were reversed and summed, with low scores indicating impulsiveness and high scores indicating greater impulse control.
Self–regulation strategies (study habits)
As an additional indicator of convergent validity, a measure of study habits was employed in both the Spring and Fall 2007 samples, using the 28–item Self–regulation Strategy Inventory developed by Cleary (2006). The Self–regulation Strategy Inventory assesses three major factor–analytically derived dimensions of self–regulation among students: management of environment and behaviour, seeking and learning information, and maladaptive regulatory behaviour. Items of the latter factor have to be reversed before an overall sum score is computed. Cleary reported high internal consistencies (.92) for the total sum score. Further, convergent, discriminant and criterion validity were established by the author (2006). A sample item is ‘I make sure no one disturbs me when I study’. Responses were given on a 7–point response scale ranging from 1 (= never) to 7 (= always). Cronbach's alpha was .89 in the present sample.
The Big Five Inventory
We used the 44–item Big Five Inventory (BFI) created by John, Donahue, and Kentle (1991) to establish construct validity of the HSCQ. The BFI assesses five dimensions of personality: Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness. All items in the BFI begin with the phrase ‘I see myself as someone who …’. This phrase is followed by options such as ‘is talkative’ (extraversion) or ‘is original, comes up with new ideas’ (openness). Internal consistencies of the BFI average above .80 with individual subscales typically ranging from .75 to .90 (John & Srivastava, 1999). Test–retest reliabilities range from .80 to .90, with an average of .85 over three months. Convergent and divergent relationships with other Big Five instruments were used to establish validity. Validity of the BFI factor structure was confirmed through multitrait–multimethod analyses of the BFI in English and Spanish (Benet–Martinez & John, 1998). In the present study, internal consistencies were .85 for extraversion (eight items), .77 for agreeableness (nine items), .78 for conscientiousness (nine items), .82 for neuroticism (eight items), and .72 for openness (10 items). Convergence of the HSCQ was expected with only the conscientiousness subscale. The other subscales were used to establish discriminant validity.
Multidimensional Personality Questionnaire–Brief Version
Convergent and discriminant validity was further tested with the Multidimensional Personality Questionnaire–Brief Version (MPQ–BF) in Sample 1. This scale provides a greater number of factor–analytically derived personality dimensions than those yielded in the BFI (Patrick, Curtin, & Tellegen, 2002). The MPQ–BF assesses 11 primary traits: well–being, social potency, achievement, social closeness, stress reaction and alienation, aggression, control, harm avoidance, traditionalism, and absorption. We hypothesised that the HSCQ would converge primarily with achievement and, to a lesser degree, with the MPQ–control scale, which focuses more on ‘foresight’ than action control. Reliabilities ranged from .75 to .84 in Patrick et al. (2002) and from .67 (for traditionalism) to .85 (for well–being) in the present study.
Depression
The well–known and widely used Center for Epidemiological Studies Depression scale (CES–D; Radloff, 1977) was used to assess depression. The 20–item CES–D has well–established reliability and validity (Conerly, Baker, Dye, Douglas, & Zabora, 2002; Devins, Orme, Costello, & Binik, 1988; Hann, Winter, & Jacobsen, 1999). Participants were asked to evaluate their feelings over the last week (7 days) using a 4–point scale ranging from 1 = rarely or none of the time (less than one day) to 4 = most or all of the time (five to seven days). Cronbach's alpha was .91 in the present sample.
Trait anger
The 10–item Trait Anger subscale of the State–Trait–Anger Expression Inventory (Spielberger, 1988) was used to assess a general tendency to experience anger. Spielberger reported internal consistencies > .80 over a variety of samples. He also established convergent and discriminant validity using several studies. The items were presented with a 4–point response scale ranging from 1 = almost never to 4 = almost always. In the present study, the internal consistency was .81.
Health–related behaviours
A variety of behavioural indicators were assessed to test for criterion validity and establish differential predictive validity of the HSCQ relative to other self–control scales. Health–related behaviours were assessed with five items and a brief eating disorder scale. Alcohol consumption was assessed with three items. The number of standard drinks consumed on a typical drinking day was estimated by participants on an 11–point scale from 0 to 10 or more drinks. Further, both the frequency of alcohol consumption and binge drinking (i.e. having ≥5 drinks on a single day) were assessed on a 7–point response scale with the response options never, less than once per month, once per month, two to three times per month, once a week, two to five times a week, and every day or almost every day. Time spent exercising was assessed with a 5–point scale from less than 30 minutes per week to more than 5 hours per week. Further, participants were asked about intentional weight loss and weight loss success. Participants indicating they had tried to lose 10 or more pounds of body weight (n = 976) were asked to rate the success of their weight loss attempt on a 5–point scale ranging from 1 = not at all successful (gained everything back or even put on more weight to 5 = extremely successful (I reached my weight goal). Finally, binge eating was assessed with a six–item subscale of the Anorexia–Bulimia Inventory (ABI; Stein, 2006). A sample item reads ‘The more I struggle to keep my weight down, the more I seem to have eating sprees’. Reliability and validity evidence was provided in a variety of studies (Stein, 2006). The items were presented with a 4–point rating scale ranging from 1 never to 4 very often. The internal consistency was .84 in this study.
Action plans: Motivation, completion and satisfaction
Participants in Fall of 2009 who agreed to complete the longitudinal part of the study were asked to write down three personally important action plans that they intended to complete within the subsequent four–week period. Participants were specifically instructed to focus on action plans that were not already part of their current habits and are not easy to perform or maintain. 1 For each action plan, participants were asked to rate both its importance and their self–efficacy to complete the action plan with the following two questions. ‘How important is it to you to complete this intention? Please rate on a scale from 0 to 100 with 0 = Not at all important and 100 = of UTMOST importance.’ ‘How certain are you that you will actually complete your intention? Please rate on a scale from 0 to 100, with 0 = completely uncertain (or 0% certain) and 100 = 100% certain.’ A sum score was created for each person, indicating overall motivation to complete their action plans.
At the one–month follow–up, participants were presented with their personal action plans and asked to rate for each of them (i) the degree of completion and (ii) the degree of their satisfaction with their performance. These questions were ‘To what degree did you complete your action plan as intended?’ and ‘How satisfied are you with your performance?’ Participants rated completion and satisfaction by entering a number between 0 and 100 into an answer box, with 0 meaning not at all completed/satisfied and 100 indicating 100% completion/satisfaction. Completion items and satisfaction items were averaged across all three personal action plans to create an overall action plan completion score and a summary satisfaction score, respectively.
Results
Reliability and dimensionality of the Habitual Self–Control Questionnaire
Item statistics and scale statistics are reported across the entire sample in Table 2. Item–total correlations ranged from .32 to .53 with an overall internal consistency of α = .81. The observed sum scores of the HSCQ ranged from 18 to 69 with a mean of 49.6 (SD = 8.0) and a possible range of 14 to 70. Test–retest reliability, assessed over a one–month period with a subset of the sample was rtt = .83 (n = 221).
Item and scale statistics (means, standard deviations), corrected item–total correlations and principal axis factoring factor loadings (n = 2162)
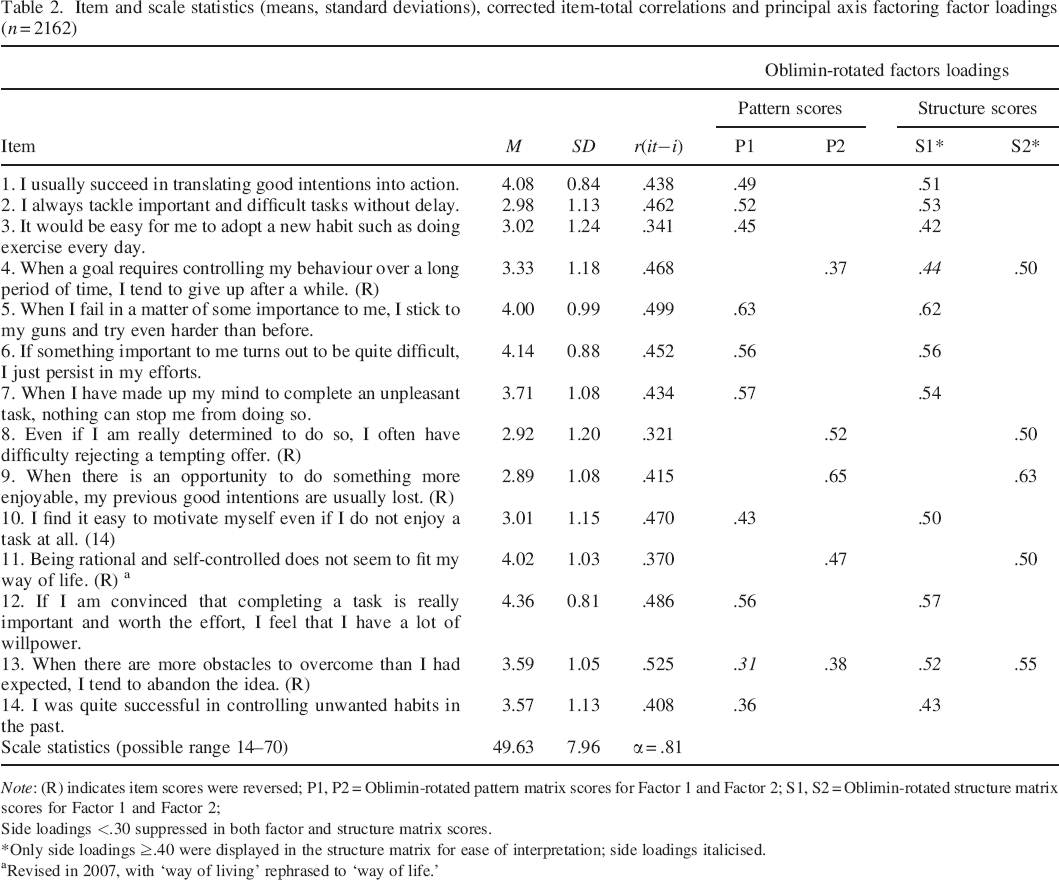
Note: (R) indicates item scores were reversed; P1, P2 = Oblimin–rotated pattern matrix scores for Factor 1 and Factor 2; S1, S2 = Oblimin–rotated structure matrix scores for Factor 1 and Factor 2;
Side loadings <.30 suppressed in both factor and structure matrix scores.
Only side loadings ≥.40 were displayed in the structure matrix for ease of interpretation; side loadings italicised.
Revised in 2007, with ‘way of living’ rephrased to ‘way of life.’
Dimensionality of the HSCQ was initially determined with an exploratory factor analysis (principal axis factoring, PAF) based on data from the entire sample of 2162 participants who had complete data on all 14 HSCQ items. Three eigenvalues >1 were found (4.135, 1.308 and 1.081) explaining together 46.6% of the variance in the items and 32.5% of the variance in the communalities. The scree plot (included in Figure 1) indicated that either a single factor or a three–factor solution should be retained. To decide on the number of factors to be retained, parallel analysis was performed following the procedures described in Hayton, Allen, and Scarpello (2004). Results (shown in Figure 1) indicated that only the first two eigenvalues exceeded the respective averaged eigenvalues that resulted from repeated random data reconstructions. Because only the first two factors exceeded the eigenvalues that occurred at random, the two–factor solution was adopted. In a subsequent PAF analysis with Oblimin rotation, a two–factor solution was enforced. Results of the rotated pattern and structure matrix are shown in Table 2. According to these results, the first factor combined positively phrased items (i.e. those for which high agreement indicated high self–control), whereas the second factor grouped negatively phrased items (i.e. items for which disagreement indicated self–control). Accordingly, the first factor was interpreted as ‘perceived self–control’ and the second factor as ‘perceived lack of self–control’.
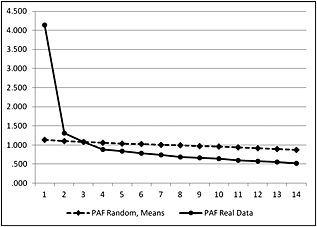
Plot of actual versus randomly generated eigenvalues (principal axis factoring, PAF).
Although positively and negatively phrased items loaded on different factors, these factors did not appear to reflect on different content aspects of self–control. Because we intended to calculate a single sum score, we performed confirmatory factor analysis via LISREL 8.80 (Jöreskog & Sörbom, 2006) to determine whether a single factor solution would provide a satisfactory fit. We also compared the single factor solution with a two–factor solution whose specifications were driven by the results of the exploratory factor analysis, allocating positively phrased items to one factor and negatively phrased items to the second factor. Given the large sample size (N = 2162) both models deviated significantly from the data (χ2 = 1298.73, df = 77, p < .001, and χ2 = 919.44, df = 76, p < .001 for the one– and two–factor solutions, respectively). Apart from Chi2–based statistics, which are heavily affected by sample size, the two–factor model provided a satisfactory fit to the data with goodness of fit (GFI) = 0.94, adjusted goodness of fit (AGFI) = 0.91, comparative fit index (CFI) = 0.95, normed fit index (NFI) = 0.95, root mean square error of approximation (RMSEA) = 0.075; and standardised root mean square residual (SRMR) = 0.048. The one–factor model exceeded the recommended cut–off for RMSEA (>0.08) with a value of 0.092 but otherwise provided an acceptable model fit with GFI = 0.91, AGFI = 0.88, CFI = 0.93, NFI = 0.92 and SRMR = 0.059.
Any model allocating items to a higher number of factors as pre–determined through exploratory factor analysis will have an advantage over a one–factor model. In addition, lack of model fit of the one–factor model appeared to be primarily driven by the assumption of uncorrelated errors, which could not be retained. With a sample size of 2162 participants, any error correlation ≥.0425 was significant. Error correlations ranged from |.001| to a maximum of |.231|, explaining between 0% and 5.34% of the variance in any two items involved. In subsequent steps, five error correlations were freed for estimation one at a time to improve model fit, guided by modification indices provided by LISREL 8.80. This resulted in a satisfactory model fit for the one–factor model with χ2 = 816.06, df = 72, p < .001, GFI = 0.95, AGFI = 0.92, CFI = 0.96, NFI = 0.95, RMSEA = 0.076 and SRMR = 0.046. Of interest, modification indices highlighted the same five error correlations in the two–factor model as relevant for model fit improvement. The resulting model fit for the two–factor model was χ2 = 591.91, df = 71, p = .001, AGFI = 0.94, GFI = 0.96, CFI = 0.97, NFI = 0.97, RMSEA = 0.06; SRMR = 0.04. Because acceptance of only five out of a total of 182 possible error correlations led to an acceptable fit for the one–factor model and because the two–factor model did not produce a content–specific meaningful solution, we decided to focus on a total sum score for the HSCQ in all subsequent analyses.
Convergent and discriminant validity
In two samples (Spring and Fall of 2007), participants completed a variety of personality and affect scales used to evaluate the internal validity of the HSCQ. Correlations and factor–analytical results are displayed in Table 3. As hypothesised, the HSCQ converged with alternative self–control scales with correlations between .60 and .68 and showed strong positive relationships with measures of goal orientation (i.e. conscientiousness, achievement). The internal validity of the HSCQ was further tested in a varimax–rotated factor analysis (PAF) performed with data from the Spring 2007 sample, which also included the MPQ. Six factors were extracted explaining 59.1% of the variance in the measures. The HSCQ had the strongest loading on Factor 1, which also combined primary loadings of the two alternative self–control scales, self–regulation strategies, BFI Conscientiousness and MPQ Achievement. The remaining factors were identified as a stress/depression factor (F2), an anger/aggressiveness factor (F3), a sociability factor (F4), openness to experience (F5) and a cautiousness factor (F6). Interestingly, Rosenbaum's (1980) Self–Control Schedule showed a strong negative side loading on Factor 2, revealing an emotion control component apparently not represented in the HSCQ. Further, although showing a substantial loading of .48 on Factor 1, the MPQ–control scale was found to converge more strongly with the MPQ–harm avoidance scale. This fits well with the contents of MPQ–control scale, summarised as being cautious, careful, reflective, sensible, rational, organised, planning ahead, and trying to anticipate events (Patrick et al., 2002).
Convergent and discriminant validity coefficients with measures of Samples 1 and 2: bivariate correlations and factor–analytic results
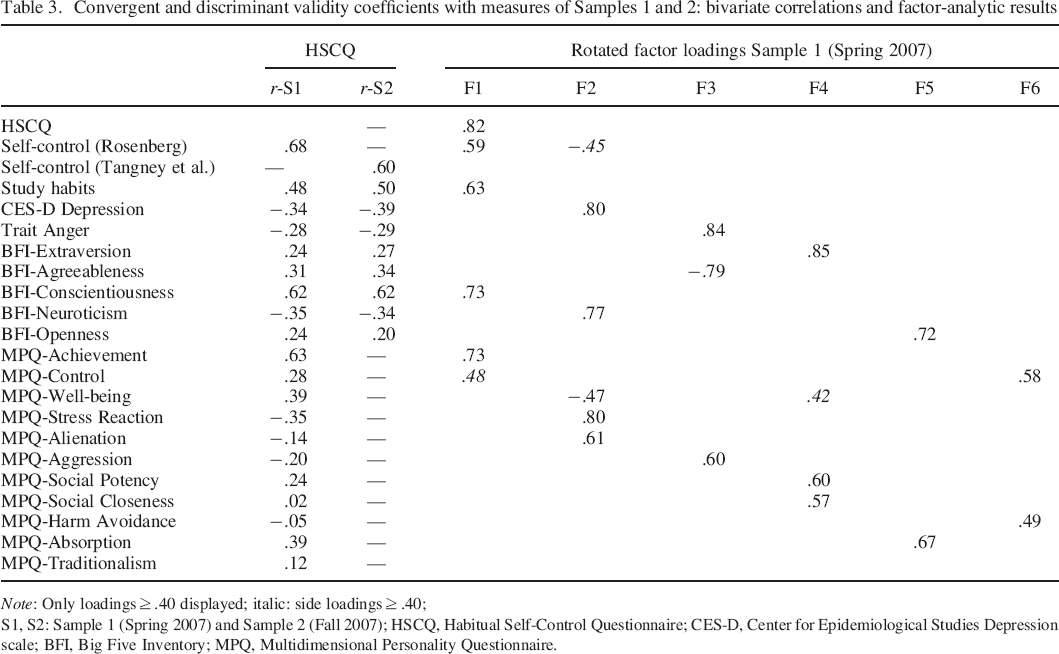
Note: Only loadings ≥ .40 displayed; italic: side loadings ≥ .40;
S1, S2: Sample 1 (Spring 2007) and Sample 2 (Fall 2007); HSCQ, Habitual Self–Control Questionnaire; CES–D, Center for Epidemiological Studies Depression scale; BFI, Big Five Inventory; MPQ, Multidimensional Personality Questionnaire.
Correlations with behavioural indicators (criterion validity)
Table 4 provides information regarding the criterion validity of the HSCQ in predicting health–related behaviours and the respective correlations of alternative self–control scales across the four samples in which behavioural criterion measures were assessed. A pattern emerged, showing the greatest predictive validity of the HSCQ with bingeing (r = −.23 to –.37) and past success in weight control (r = .22 to .35) and weak but reliable relationships with self–reported time spent exercising (r = .14 to .22). The HSCQ turned out to be a poor and unreliable predictor of alcohol consumption with two of the alternative measures of self–control (SCS and Impulse Control) clearly outperforming the HSCQ. This pattern emerged more clearly in hierarchical regressions testing the incremental variance explained by each the HSCQ and the alternative self–control scales included in three of the samples (see Table 5). With the exception of Rosenbaum's SCS, which did not differ greatly from the HSCQ in predicting health behaviours, the alternative scales explained substantial incremental variance in alcohol consumption beyond the HSCQ (SCQ: 3.7% to 5.6%; impulse control: 2% to 9.4%) with no additional significant contribution of the HSCQ in any analysis involving self–reported drinking. In contrast, the HSCQ explained unique variance in binge eating, weight control and exercise beyond the alternative measures with contributions of up to 8.3% for bingeing, 12.4% for past success in weight control and up to 3.6% of the variance in exercise. In contrast, none of the alternative self–control scales provided any significant contribution in predicting these outcomes beyond the HSCQ. 2
Correlations with behavioural criterion measures: results for HSCQ and alternative self–control scales
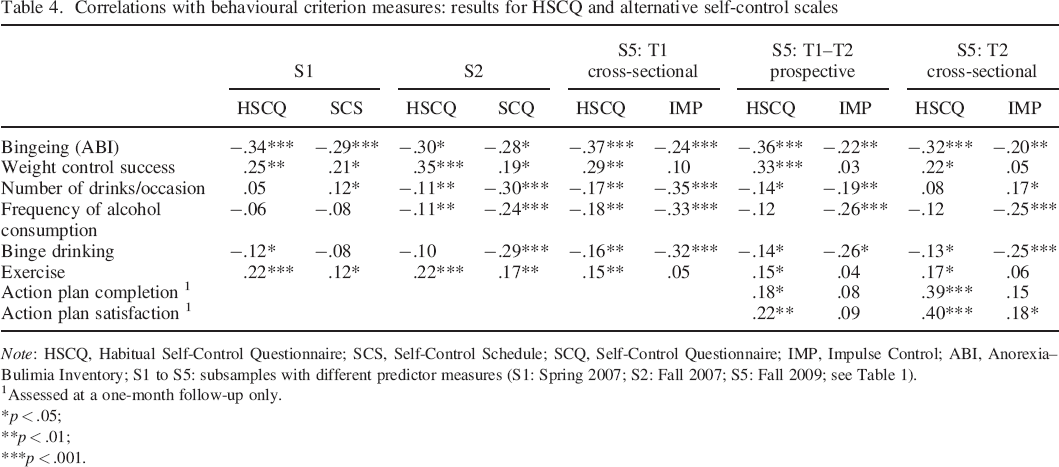
Note: HSCQ, Habitual Self–Control Questionnaire; SCS, Self–Control Schedule; SCQ, Self–Control Questionnaire; IMP, Impulse Control; ABI, Anorexia–Bulimia Inventory; S1 to S5: subsamples with different predictor measures (S1: Spring 2007; S2: Fall 2007; S5: Fall 2009; see Table 1).
Assessed at a one–month follow–up only.
p < .05;
p < .01;
p < .001.
Incremental variance explained in hierarchical regressions: comparison of HSCQ and alternative self–control measures
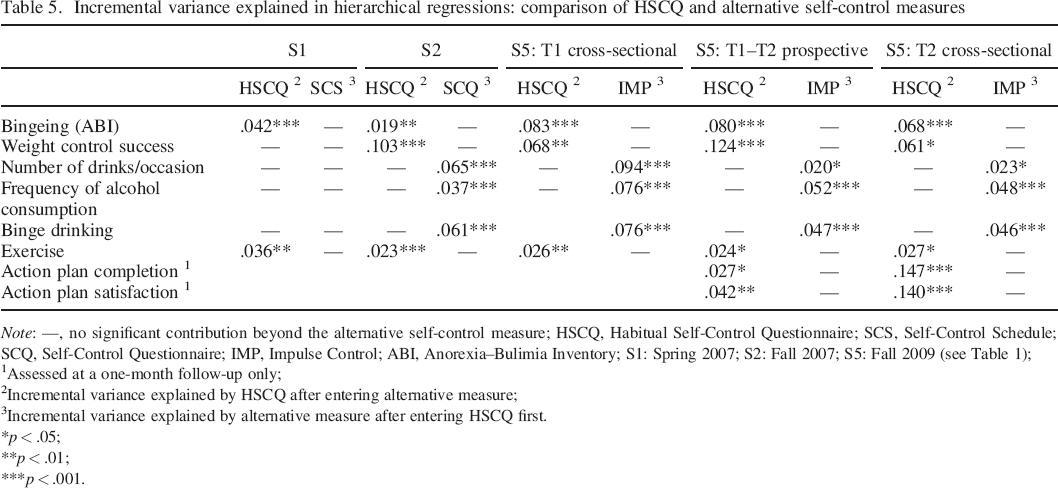
Note: —, no significant contribution beyond the alternative self–control measure; HSCQ, Habitual Self–Control Questionnaire; SCS, Self–Control Schedule; SCQ, Self–Control Questionnaire; IMP, Impulse Control; ABI, Anorexia–Bulimia Inventory; S1: Spring 2007; S2: Fall 2007; S5: Fall 2009 (see Table 1);
Assessed at a one–month follow–up only;
Incremental variance explained by HSCQ after entering alternative measure;
Incremental variance explained by alternative measure after entering HSCQ first.
p < .05;
p < .01;
p < .001.
Further evidence for differential criterion validity emerged in the longitudinal part of the study with measures of action plan completion. The HSCQ, as opposed to the impulse control scale, predicted action plan completion and was a stronger predictor of completion satisfaction. The HSCQ explained unique variance in these outcomes beyond impulse control. Vice versa, no unique variance was explained by impulse control in these criterion measures.
The Habitual Self–Control Questionnaire as a predictor and moderator of the motivation–behaviour relationship in the completion of action plans
The HSCQ was supposed to contribute uniquely to the prediction of action plan completion and satisfaction beyond motivation (H4). In addition, a moderator effect of the HSCQ on the relationship between motivation and performance was proposed with the expectation that habitual self–control will facilitate enactment if motivation is insufficient (H5). In order to test the moderator hypothesis, the sum score of the motivation items and the HSCQ scores were standardised, and an interaction term was created by multiplying the two standardised predictor variables. Intention completion, assessed on a percentage scale and averaged across all three action plans, ranged from 13% to 100% (M = 66.1, SD = 19.7) and performance satisfaction ranged from 7.5% to 100% (M = 64.0, SD = 22.6). The two dependent variables (action plan completion and satisfaction) were standardised as well to define the effects of the predictors in terms of differences in standard deviation units.
Two hierarchical regressions were performed, entering motivation in the first step, the HSCQ in the second step and their interaction in the last step. The results are summarised in Table 6. All three predictors contributed significantly to the prediction of intention completion and performance satisfaction. Both motivation and habitual self–control were positively related to the outcomes. Intention–specific motivation, summarised over the three action plans, explained 3.7% of the variance in completion and 1.9% of the variance in satisfaction. Habitual self–control, accounted for an additional 2.9% of the variance in completion and 3.9% of the variance in satisfaction and the interaction between HSCQ and motivation explained an additional 3.5% of the variance in completion and 3.2% of the variance in satisfaction. Figure 2 depicts these interactions. The HSCQ appeared to compensate for motivational deficits in supporting enactment of intentions and satisfaction with enactment. If motivation was high (z = 1), completion and satisfaction were both high, irrespective of participants’ scores on the HSCQ. However, when motivation was low (z = −1), both performance and performance satisfaction depended on habitual self–control, confirming the compensatory role of habitual self–control in the completion of difficult action plans when motivational underpinnings are too weak.
Hierarchical regressions testing predictor and moderator effects of HSCQ, assessed at Time 1, on action plan completion and satisfaction at follow–up in Sample 5 (n = 182)
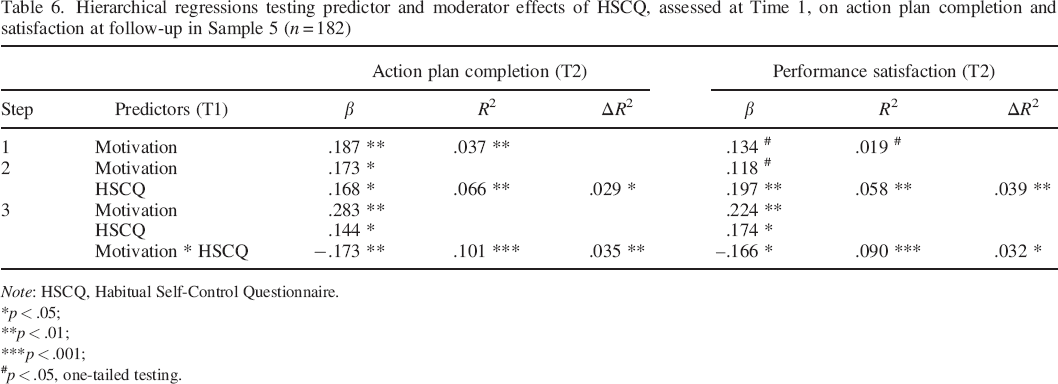
Note: HSCQ, Habitual Self–Control Questionnaire.
p < .05;
p < .01;
p < .001;
p < .05, one–tailed testing.
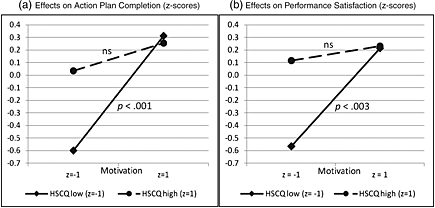
Interaction between habitual self–control and plan–specific motivation on action plan completion and performance satisfaction. HSCQ, Habitual Self–Control Questionnaire.
Figure 2 depicts the simple slopes of motivation on action plan completion and satisfaction for different levels on the HSCQ. Motivation displayed an important and significant effect only among people with low self–control scores. The simple slope for motivation at −1 SD below the mean of the HSCQ was β = .456 (SE = 0.127, p < .001) for action plan completion and β = .39 (SE = 0.129, p < .003) for satisfaction. In contrast, when scores on the HSCQ were high, motivation lost much of its predictive value in the longitudinal analyses. The simple slope of motivation at +1 SD of the HSCQ was β = .11 (SE = 0.073, ns) for action plan completion and β = .058 (SE = 0.074, ns) for satisfaction.
Summary and Discussion
In this study, we introduce the HSCQ as a theory–based measure of relatively stable inter–individual differences in self–control. The HSCQ is based on two assertions of action control theory. First, that motivation may not suffice to support the enactment of difficult intentions, which typically involve non–hedonistic behaviours and an approach–avoidance conflict (Kuhl, 1985; Schroder, 1997; Schroder & Schwarzer, 2005). Second, that people differ in their skills and abilities to overcome the barriers that render the enactment of their intentions more difficult (Kuhl, 1985, 1994). Accordingly, the HSCQ has a relatively narrow focus on action control and ignores other aspects typically assessed in self–control scales, such as the control of cognitions, emotions and impulses (Patton et al., 1995; Rosenbaum, 1980; Tangney et al., 2004). Although controlling affective states, thought processes, and impulses may describe relevant skills in supporting the enactment of an intention, they are irrelevant in the context of action control when not used strategically towards the achievement of a specific goal. Accordingly, we proposed that these control skills and strategies are subordinate to self–control, defined as an affinity towards persistent goal pursuit and therefore should not be targeted as measures of habitual self–control in the HSCQ.
The results of this study provide initial evidence for the reliability and validity of the HSCQ as a measure of habitual self–control. With an internal consistency of .81, the HSCQ demonstrates satisfactory reliability. A one–month test–retest reliability of .83 provides evidence for stability of HSCQ scores, supporting the notion of a trait measure. The HSCQ is not one–dimensional. Factor analyses indicated the presence of two highly correlated components in the HSCQ. However, the apparent heterogeneity of the HSCQ appears to be primarily a result of item polarity, separating positively phrased from negatively phrased items. Similar effects of item wording have been observed in other well–known trait measures such as the State–Trait–Anger Expression Inventory (Vigneau & Cormier, 2008) and the Life Orientation Test (Herzberg, Glaesmer, & Hoyer, 2006; Scheier & Carver, 1985). Beyond this polarity interpretation of the two–component structure of the HSCQ, there is no indication that the two factors represent theoretically and practically meaningful sub–dimensions of habitual self–control. Further, the one–factor model produced an acceptable fit, indicating no reason to reject the calculation of a single sum score.
Given the lack of content–specificity in the two statistically derived dimensions and the fact that a one–dimensional model provided a reasonable fit to the data, we decided against the development and validation of two subscales for the HSCQ and recommend retaining a single sum score for the HSCQ in future research. The theoretically restricted content domain of the HSCQ, based on the background of ACT, supports this decision. Theoretically meaningful sub–dimensions may be easier to derive from the self–control scales of Rosenbaum (1980) and Tangney et al. (2004), which explicitly and intentionally assess a variety of diverse self–control skills and abilities specifically pertaining to the control of emotions, thoughts and impulses that are not targeted in the HSCQ.
Correlational and factorial analyses provided strong evidence for convergent and discriminant validity of the HSCQ, supporting the expectations formulated in Hypothesis 2. The HSCQ clearly converged with already existing self–control scales but not to the degree to claim that the HSCQ measures exactly the same entity targeted by the SCS and the SCQ. The HSCQ shared between 36% and 46% of the variance with these measures but showed equally strong convergence with ‘performance’ measures such as the MPQ achievement and with the BFI conscientiousness scale. In the context of a great variety of trait measures, the HSCQ established a common component with these scales and could be clearly distinguished from measures of emotional distress, sociability, agreeableness/aggression and other well–known personality dimensions. Interestingly, the PCA results indicated a strong negative side loading of the Rosenbaum's SCS on a stress/depression factor. This confirms a component of ‘emotion control’ yielded in the SCS that the HSCQ does not appear to share with its narrower focus on persistent goal pursuit.
Despite its strong overlap with alternative measures of self–control, the HSCQ also demonstrated uniqueness in predicting diverse behavioural criterion measures. In Hypothesis 3, we reasoned that the HSCQ, as a measure of persistent goal pursuit, should be particularly useful in predicting behaviours that can be expected to be either positively or negatively related to explicit behavioural intentions. This includes, for example, intentional weight loss through dieting, engaging in exercise, and the control of binge eating, indicating out–of–control behaviour that is typically of severe concern for the person involved. In contrast, alcohol consumption should be less predictable by the HSCQ in persons without an explicit goal towards restraint. We found strong evidence supporting this pattern. The HSCQ was negatively associated with binge eating behaviours and positively associated with self–reported weight loss success in the past. The HSCQ also predicted exercise behaviour but was a weak and unreliable predictor of various measures of alcohol consumption. In comparison, alternative self–control scales were usually less efficient in predicting dietary and exercise behaviours and superior in predicting alcohol consumption. Hierarchical regressions produced a remarkably reliable pattern, demonstrating uniqueness of the HSCQ in predicting dietary, weight loss and exercise behaviours, whereas alternative measures usually explained unique variance in drinking behaviours with no additional contributions of the HSCQ. In this regard, the SCQ of Tangney et al. (2004) behaved much like the BIS (Patton et al., 1995), likely referring to a shared impulse control component not specifically targeted in the HSCQ.
Further predictions referred to the theoretical validity of the HSCQ in supporting the enactment of intentions (H4) and moderating the relationship between motivational strength and enactment (H5). For this purpose, we asked study participants to formulate three ‘action plans’ for the subsequent one–month period that were important to them but not easy to enact (i.e. would require self–control). We also assessed importance (valence) of action plans and confidence (self–efficacy) of enactment, which served as indicators of motivational strength. Enactment was assessed at the one–month follow–up with two questions regarding the level of completion and participants’ satisfaction with their enactment. Hierarchical regressions confirmed that the HSCQ contributed to the prediction of enactment and satisfaction beyond motivational variables (H4). Further, we found the theoretically expected interaction between motivation and habitual self–control on predicting the enactment of action plans (H5). Specifically, habitual self–control was particularly beneficial in supporting enactment when motivation alone was not sufficient to support an intention. These results indicate compensatory effects of habitual self–control when motivation is weak or insufficient—as can be expected in the context of ‘difficult’ intentions that are often characterised by an approach–avoidance conflict or limited self–efficacy beliefs.
As emphasised in the introduction, behavioural intentions do not always involve a strong goal commitment, leading to a sub–optimal or unstable motivational basis for subsequent behaviour. In this context, it may be important to distinguish between motivational factors that drive a decision from those that ultimately support enactment. Decision making about ‘difficult’ (non–hedonistic) behavioural intentions is usually driven by rational considerations, such as ‘when I diet I will be more healthy and fit, less likely to get diabetes and heart disease and fit better in my clothes’, or, more generally, by ‘I should’ considerations. At the time of decision making, these rational aspects are likely to be most salient. In contrast, enactment is at least equally driven by factors such as current desires, cravings, inertia, pleasure seeking, and the like. If such factors are not countered by a strong goal commitment, they will weaken the underlying motivation and make it more difficult to form a sustainable intention. It is then more likely that these barriers ‘win the battle’ at the time of enactment when the non–hedonistic aspects of the goal–directed actions become particularly salient. Therefore, it makes sense that people whose motivation and determination is strong at the time of decision making (i.e. have built a strong commitment despite ambivalence about the required behaviours) are less in need to muster self–control when occasions arise to act upon their intentions. In contrast, if a decision is made with less enthusiasm, less self–efficacy and/or more misgivings regarding the planned behaviour, habitual self–control can make a difference in overcoming those barriers.
It may be surprising that, overall, plan–specific motivation and habitual self–control did not explain more than about 10% of the variance in plan enactment and enactment satisfaction. Several aspects may have played a role in preventing stronger prediction. First, action plans were not created spontaneously. Instead, they were formulated in response to our request. Participants certainly focused on action plans that were of personal relevance and reflected their values and goals. However, the request to formulate action plans to be enacted within a one–month period still created a somewhat artificial setup not comparable with a true self–initiated decision–making process. Second, most participants in this study were undergraduate students in their first year at college whose lives and social context had changed considerably, requiring orientation, adaptation and re–adjustment that could easily interfere with specific action plans. In sum, the correspondence between the theoretical predictors and actual performance may not have been stronger than in the likewise externally cued New Year's resolutions. Nevertheless, the results of this study indicate that habitual self–control interacts with motivation in a theoretically meaningful way. Our findings are strengthened by similar results obtained in a longitudinal study with coronary artery bypass patients, in which the uptake of a heart–healthy diet was the dependent variable. Habitual self–control, assessed with a German version, predicted dietary behaviour at follow–up above and beyond patients’ intention and moderated the intention–behaviour relationship in the same way as evidenced in the present study: When intentions were not sufficiently supported by motivational factors, habitual self–control supported the adoption of a heart–healthy diet, pointing to compensatory effects (Schroder & Schwarzer, 2005). The similarities with the German sample of older surgical patients strengthen our confidence in the generalizability of the results obtained with the English version among college students.
In summary, the current study supports the conclusion that the HSCQ is a reliable and valid measure of individual differences in self–control. Limitations of the present study include the exclusive use of student samples from a region in Utah where the population is predominantly affiliated with the LDS Church. However, we believe that both the substantial size of our sample and the fact that 83% of the US population regard themselves as religious, with a strong predominance of Christian–based religions, allow generalisation to other student samples within the USA. Findings with an adult sample enrolled in a dietary intervention provide further support for the reliability and predictive validity of the HSCQ in a different population (Schroder et al., 2008). An additional limitation relates to the assessment of behavioural criterion variables in terms of self–report only. However, the assessment of individual goals and self–reports of goal completion in the longitudinal part of our study deviates from the use of mere self–rating scales and provides at least an approximation to more objective validation criteria.
The strengths of the study may be seen in the large sample size, the use of a great variety of criterion measures and the strong theoretical background of the HSCQ. With only 14 items, the HSCQ may be more efficient and feasible for clinical applications than its longer counterparts without sacrificing reliability. We acknowledge that already existing measures of self–control may be more in line with the much broader everyday understanding and use of the term self–control than the definition that we offered based on the background of action control theory. However, we believe that a distinction between the control of goal–directed action and the control of emotion and impulses has much to offer to social scientists. People high in impulse or emotion control are not necessarily those who are most successful in acting upon their commitments and vice versa. Thus, an advantage of the HSCQ over already existing measures of self–control may be seen in its theoretical background that is particularly suited to add to already existing intention–based models of behaviour. Behaviour theories such as the theory of reasoned action, or its successor, the theory of planned behaviour (Ajzen, 1991; Ajzen & Fishbein, 1980), can gain much from a theoretically well–founded measure that may be able to explain why some people show greater congruence between intention and behaviour than others and that filters out other marginal aspects of action control such as the control of emotion.