
Abstract
Personality development is characterized by increasing maturation, that is, people become more conscientious, agreeable and emotionally stable as they age. In late life, however, these trends seem to be reversed. Because many changes and transitions in older age are related to health, we investigated correlated changes in health problems and personality traits, the sources of health changes in later life and the directionality of effects. Our sample consisted of older adult twins, aged 64–85 years at time 1 (n = 410; 135 male/275 female; 134 monozygotic/63 dizygotic twin pairs), assessed at two different time points about five years apart, and we ran bivariate latent change and latent change twin model analyses. Increasing health problems were associated with decreases in agreeableness, extraversion, emotional stability and conscientiousness. Changes in health problems were only due to environmental influences, implying that the association between health and personality changes was exclusively environmental. Directional effects were largely absent, but health and personality were significantly related at the second measurement occasion (age 69–89 years). Our results support the link between health change and personality change in late life and spark the assumption of normative personality adaptations to deterioration of health status as a means of developmental regulation. Copyright © 2017 European Association of Personality Psychology
Despite essentially showing considerable stability across the lifespan, personality change is possible at every time point and at every age. Research on personality development shows that as people tackle life transitions, developmental tasks and new social roles, they develop more ‘mature’ personality characteristics, that is, they become more conscientious, agreeable and emotionally stable as they grow older. However, as people move from middle into older ages, the challenges and tasks of development change and seemingly lead to a halt on maturity–related personality changes (for a recent discussion regarding the use of the term ‘maturity’ in personality development, see Mund, Zimmermann, & Neyer, in press). Still, personality seems to be malleable even in oldest ages.
We argue that developmental trends for personality traits are closely related to changes in physical and subjective health and functioning in later life and that this relation might be instrumental for the maintenance of functioning in old age. We thus analyse associations between (change in) Big Five personality traits (neuroticism, extraversion, openness, agreeableness and conscientiousness) and (change in) different indicators of health problems (days of illness or hospitalization during the last six months and self–rated health problems) by assessing correlated changes and bidirectional effects. We hypothesize that increasing health problems are associated with reverse personality trends in old age. Moreover, we go further beyond previous research by estimating the extent to which genetic and environmental sources contribute to individual differences in health problem status and changes over time based on a longitudinal twin design. The latter has important implications for starting points in the search for potentially causing factors: inside or outside the individuals’ bodies and (or) minds.
Personality Changes in Later Life
Research within the framework of the Big Five personality traits (e.g. McCrae & John, 1992) shows that mean levels of agreeableness, conscientiousness and some facets of extraversion (e.g. assertiveness) increase, whereas other facets of extraversion (e.g. social activity), neuroticism and openness to experience decrease by trend as people grow older (Roberts, Walton, & Viechtbauer, 2006; see also Allemand, Zimprich, & Hertzog, 2007; Lucas & Donnellan, 2011; Specht, Egloff, & Schmukle, 2011). These mean level changes seem to reflect individuals’ adaptations to the challenges and tasks that are inherent in human development, such as starting work life or becoming parents (Hutteman, Hennecke, Orth, Reitz, & Specht, 2014; Roberts & Wood, 2006). On average, personality thus develops in the direction of a more socially functional individual from younger ages to middle adulthood, which is called the maturity principle of personality development (Roberts et al., 2006). Evidence supporting the general propositions of the maturity principle has accumulated (e.g. Bleidorn et al., 2013; Hudson & Roberts, 2016; Lodi–Smith & Roberts, 2007).
Even though the study of personality development past childhood and adolescence has evolved over the last decades, studies that include older adults remained rare for a long time. In recent years, however, more and more studies demonstrate that even in the later decades of life, personality development still takes place. Interestingly, those studies investigating the development of personality after midlife find trends opposing the original formulation of the maturity principle. For example, in a sample of older Scottish adults, Mõttus, Johnson, and Deary (2012) found a decline from age 81 to 87 years in extraversion, conscientiousness and agreeableness. The magnitude of these changes led the authors to conclude that personality development does not slow down in later life. In our own recent study with a sample of German twins aged between 64 and 85 years, we showed that over the course of five years, mean levels of neuroticism significantly increased, whereas conscientiousness and extraversion showed significant mean level decreases (Kandler, Kornadt, Hagemeyer, & Neyer, 2015). In addition, agreeableness and openness showed average declines by trend. These findings were closely mirrored by results by Wagner, Ram, Smith, and Gerstorf (2016) in a sample of German adults aged 70–103 years at the first assessment who participated in the Berlin Aging Study. Using time to death instead of chronological age, they reported decreases in extraversion and openness as well as increases in neuroticism at the very end of life.
Taken together, personality development in old age and at the end of life can be described by significant declines in extraversion, emotional stability and conscientiousness, as well as decreases for agreeableness and openness to experience (cf. Mroczek & Spiro, 2003; Wortman, Lucas, & Donnellan, 2012; but, see also Müller et al., 2016), even though there seems to be some heterogeneity between studies and in general a less elaborated empirical basis than for other ages (Specht, 2017). At first glance, these mean–level trends seem to follow the reverse pattern characterizing the maturity principle in younger adulthood and might be understood as indicators of declining overall functioning in old age. However, taking into account the developmental tasks and challenges that accompany old age, these changes might be expected and even functional in the face of late–life transitions (Kandler et al., 2015; Müller, Wagner, & Gerstorf, 2017).
The Interrelation between Health and Personality Changes in Later Life
Many of the challenges and changes in old age are related to changes in health and physical functioning. It is thus not surprising that besides the established influence of personality trait levels and changes on health indicators (for all Big Five traits and a large number of diseases and health problems, e.g. Turiano et al., 2012; Weston, Hill, & Jackson, 2015), evidence for the relationship between personality changes as a possible consequence of health changes has started to emerge. For example, studies show correlations between lower self–rated health and declines in extraversion and conscientiousness as well as increasing neuroticism in old age (e.g. Magee, Heaven, & Miller, 2013; Takahashi, Edmonds, Jackson, & Roberts, 2013). With regard to more objective indicators of health, Jokela, Hakulinen, Singh–Manoux, and Kivimäki (2014) found that after the onset of a chronic disease, participants from several representative studies showed declines in extraversion, openness, emotional stability and conscientiousness (see also Sutin, Zonderman, Ferrucci, & Terracciano, 2013).
Müller et al. (2016) performed growth curve analyses on three waves of data (three and two years apart, respectively) from participants of the Berlin Aging Study II that were aged 65 to 88 years. They found that higher physician–rated morbidity was related to increases in neuroticism, whereas poorer handgrip strength (as a measure of upper–body functioning) was associated with increases in neuroticism, decreases in openness and agreeableness, fewer increases in extraversion and steeper declines in conscientiousness. Most recently, Stephan, Sutin, Canada, and Terracciano (2017) found that in four large American samples with participants aged between 65 and 104 years, higher frailty (operationalized via a composite score including several indicators such as handgrip strength and walking speed) was related to increases in neuroticism and declines in extraversion, openness, agreeableness and conscientiousness over a time interval of eight years. Other studies have also reported relations between (changes in) health variables and Big Five traits to varying strength (e.g. Berg & Johansson, 2014; Mõttus et al., 2012; Mroczek & Spiro, 2003; Stephan, Sutin, Luchetti, & Terracciano, 2016; Wagner et al., 2016; Wettstein, Tauber, Wahl, & Frankenberg, 2017).
In sum, previous research suggests a systematic interrelation between decreases in specific Big Five personality traits (emotional stability, extraversion, openness, agreeableness and conscientiousness) and health declines as well as evidence for effects in both directions. Still, more research is needed to identify the driving forces, that is, the underlying genetic and environmental sources leading to concurrent personality and health changes in older age.
Genetic and Environmental Sources of Health and Personality Changes in Later Life
In order to understand the relationship between personality and health in later life, it is important to better understand their underlying sources. Behaviour genetic studies provide estimates of genetic and environmental sources of individual differences in specific characteristics and also in their change and stability. Unlike studies relying exclusively on environmental factors, behaviour genetic studies provide these estimates controlling for the respective other, that is, the role of the environment when controlling for genetic effects and vice versa. With regard to health in older age, studies mostly from Scandinavia have provided evidence for some genetic and also environmental influences. In a Danish study of twins aged 75 years and older, around 25% of the variance in self–rated health and hospitalization was due to genetic variation, whereas the remaining variance was due to individual–specific environmental factors (Christensen, Holm, McGue, Corder, & Vaupel, 1999). Within the same study, similar genetic contributions were found for individual differences in the level of physical functioning, whereas individual differences in change in physical functioning were entirely environmental until the last of four waves (Christensen, Frederiksen, Vaupel, & McGue, 2003). In a study comparing the genetic contributions to individual differences across adulthood, Harris, Pedersen, McClearn, Nesselroade, and Plomin (1992) found that whereas again around 25% of the variance in subjective health was due to genetic factors above the age of 70 years, variation in objective health indicators was not significantly attributable to genetic sources for this age group.
To sum up, previous studies have shown some links between genetic differences and variation in health level in old age with more consistent results for subjective health than for objective indicators of health. The genetic component in subjective health may reflect genetic differences in personality traits to some degree (Weiss, Bates, & Luciano, 2008), because personality differences may impact how individuals see themselves and their health condition. However, the primary source of health differences and, in particular, in case of individual differences in health change appears to be environmental. Generally, behaviour genetic findings on health change in older age are scarce, and thus, the roles of genetic and environmental factors are not well understood.
With regard to the aetiology of individual differences in personality change, we found in our previous study (Kandler et al., 2015) that interindividual differences in intraindividual personality change were mostly due to environmental sources not shared by twins, which is in line with theoretical accounts of personality plasticity across the entire lifespan: personality traits might change at any age because of life experiences (e.g. Roberts, Wood, & Caspi, 2008). Consequently, if individual differences in changes in health status would be primarily due to environmental sources, and if changes in health problems and changes in personality would accompany each other, this would indicate that environmental influences are the primary driving force underlying the association between health changes and personality changes in old age (instead of genetically driven individual differences in resilience or health deterioration). Combining behaviour genetic analyses of health in older age with research on personality change in older age is thus warranted to understand their driving and mutual sources. Findings on the aetiology of both personality and health change—whether genetic or environmental—have important implications for the search of potential causing factors—within or outside the individual. Knowing more about these causing factors ultimately provides orientation for prevention and intervention studies.
The Current Study
The current study added to the stream of research linking health and personality by analysing associations between change in Big Five personality traits and change in different indicators of health problems. This research is especially relevant for the understanding of personality development, because the study of correlated changes in personality and related variables is so far underrepresented in this line of research (Allemand & Martin, 2016). We hypothesized that increasing health problems are associated with reverse personality trends, that is, increases in neuroticism and decreases in conscientiousness, agreeableness, extraversion and openness in old age. By using bivariate latent change models, we could focus on concurrent changes in health and personality as well as on whether the initial level of one variable predicts change in the other controlled for initial correlations. Because there is evidence for both directions of causality, we expected that the longitudinal direction between health and personality is bidirectional. Evidence that changes in personality traits in old age are systematically related to changes in health conditions facilitates theory building and the further integration of personality change in old age in theoretical frameworks of lifespan development (e.g. Baltes, Lindenberger, & Staudinger, 2006). This informs future studies that investigate the underlying mechanisms to better understand the developmental (co–)dynamics of personality and health in old age.
We further estimated the extent to which genetic and environmental sources contributed to individual differences in health problem status and change over time based on a longitudinal twin design. In line with previous studies (e.g. Christensen et al., 2003), we expected that individual differences in health change are entirely due to environmental sources. As a consequence, and in line with the finding that individual differences in personality change in old age were primarily due to environmental sources (Kandler et al., 2015), the association between health change and personality change must be due to environmental sources. Genetically identical individuals (i.e. monozygotic (MZ) twins) would thus become more dissimilar regarding the developmental co–dynamics of personality and health due to environmental experiences. We thereby not only shed light on the sources of health in late life but also contribute to the understanding of the relationship between health changes and personality changes in a comprehensive way. Combining a longitudinal study with a behaviour genetic design enabled us to narrow down explanations for the relationship between personality and health in later life by providing estimates of environmental effects controlled for genetic effects (and vice versa).
We investigated the sources of individual differences in health status and change as well as the interrelation between health and personality over time with the help of a sample of older adult twins in their 60s to 80s that provided personality and health–related information at two measurement occasions about 4.5 years apart. We included a subjective measure of health (SHP) and the frequency of health problems (FHP) in days (i.e. days of illness and hospitalization) during the last six months as differential indicators of health. Even though the latter construct does not represent actual objective information (such as physician ratings), it is less dependent on the subjective feeling of a person and thus separable from purely subjective variables and also less susceptible to related biases. The two constructs represent conceptually different facets of health with distinguishable empirical relations to personality and other variables (Turiano et al., 2012; Wettstein et al., 2017).
Method
Sample
The sample was drawn from the Genetically Oriented Lifespan Study on Differential Development (GOLD). The GOLD study is a longitudinal twin study designed to investigate the aetiology of individual differences in traits, motives, self–referential cognitions and volitional control in old age (Geppert & Halisch, 2001). A more detailed description of the sampling procedure and sample used in the current analyses can be found in Kandler et al. (2015) where we already presented analyses on the patterns and sources of the development of the Big Five personality traits that are related to the findings of the current study. The complete data with labelled variables used in the current study are available in the Open Science Framework (Kandler, Hagemeyer, Neyer, & Kornadt, 2017, October 25: https://osf.io/r96hg/). These data can be used to reproduce the results presented in this study. However, because the GOLD dataset is not public domain, requests for data use for own research projects should be sent to the authors.
At the first point of time [time 1 (T1)], the sample consisted of 410 individuals (135 male and 275 female) aged between 64 and 85 years (M = 71.32) and included 134 complete MZ and 63 complete dizygotic (DZ) same–sex twin pairs with a mean age of M = 71.32 (range: 64–85 years). After an interval of about five years (M = 4.5 years), 324 (79%) individuals (115 male and 209 female) including 148 complete twin pairs (101 MZ and 47 DZ pairs) with a mean age of M = 75.63 (range: 68–89 years) participated in a second assessment [time 2 (T2)]. About 17% of the participants that did not take part in the second assessment died between T1 and T2, and overall, dropout tended to be larger for older people and women. Missing–completely–at–random tests (Little, 1988) showed, however, that dropout could be assumed to be randomly distributed (χ2 = 412.30; df = 387; p = .18).
Measures
Personality traits
Big Five personality traits were assessed with the German 60–item Neuroticism–Extraversion–Openness Five–Factor Inventory (Borkenau & Ostendorf, 1993; Costa & McCrae, 1992). Participants rated their traits on a 5–point scale from 1 (does not describe me at all) to 5 (describes me very well). Consistent with our previous study, we used latent variable scores. For that purpose, the items on each scale were assigned to two parcels as quasi–parallel tests with equal means and standard deviations (see Kandler et al., 2015, and Table S1 and S2 in the Supporting Information for means, standard deviations, internal consistencies and rank–order continuities of parcel scores, as well as split–half reliabilities and rank–order continuities of true scores based on these parcels). The use of quasi–parallel parcels allowed us to control for error of measurement.
Frequency of health problems
As a measure of FHP, we used composite scores and latent variable scores based on three reports. For the past six months, participants reported the number of days they could not attend work or go about their daily chores because of sickness (T1: M = 2.51, SD = 9.27, Min = 0, Max = 100; T2: M = 3.77, SD = 12.69, Min = 0, Max = 160), the number of days they were hospitalized (T1: M = 1.60, SD = 5.79, Min = 0, Max = 56; T2: M = 2.66, SD = 11.53, Min = 0, Max = 160) and the number of days they stayed in a health clinic due to physical health problems (T1: M = 0.87, SD = 5.07, Min = 0, Max = 42; T2: M = 1.33, SD = 9.72, Min = 0, Max = 160), respectively (e.g. ‘In the past six months, how many days have you been hospitalized due to physical health problems?’). The original scores were logarithmized to obtain scores with a less right–skewed distribution. This strategy reduced the skewness of the FHP from 6.77 to 2.95 at T1 and from 10.46 to 2.24 at T2. The internal consistency of composite scores (T1: M = 0.32, SD = 0.73, Min = 0, Max = 4.16; T2: M = 0.44, SD = 0.84, Min = 0, Max = 4.83) based on these three–item measures was acceptable: α = .71 at T1 and α = .69 at T2.
Subjective health problems
As subjective assessments of health problems, three self–reports on recent feelings of fatigue, weariness, sickness and health were used. Participants rated two of these items (‘Have you felt sick recently?’ and ‘Have you felt exhausted and not fit recently?’) on a scale from 1 (not at all) to 4 (a lot more than usual). The third item (‘Have you felt very good and in the best of health recently?’) had to be rated on a scale from 1 (better than usual) to 4 (much worse than usual). The values from these three items were used to generate composite scores (T1: M = 5.48, SD = 1.42, Min = 3, Max = 11; T2: M = 5.83, SD = 1.76, Min = 2, Max = 12). The internal consistency of composite scores was acceptable to good: α = .75 at T1 and α = .84 at T2. 1
Preliminary analyses
All initial and preparatory analyses were conducted with the statistical package IBM
Based on composite scores of SHP and FHP, we found significant mean–level change for both scores over time (Table 1; see also Table S3 in the Supporting Information for item–level t–tests and separate composite–level t–tests for twin A and twin B subsamples). Health problems increased over time and showed rather low differential stability indicating large individual differences in change. The correlations between the composite scores were r = .38 [p < .001; 95% confidence interval (CI): .25, .69] at T1 and r = .44 (p < .001; 95% CI: .32, .54) at T2, indicating a moderate association within time. The cross–time correlations were r = .16 (p = .005; 95% CI: .05, .26) between the FHP at T1 and SHP at T2 as well as r = .07 (p = .19; 95% CI: −.03, .19) between SHP at T1 and the FHP at T2, indicating that the FHP predicted current SHP but not vice versa (see also Table S4 in the Supporting Information for item–level correlations within and between measurement occasions).
Mean–level change and rank–order stability for frequency of health problems and subjective health problems
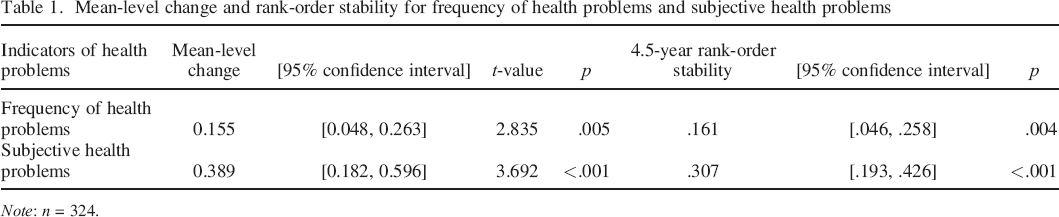
Note: n = 324.
We did not find significant age differences in health problems within measurement occasions. Neither linear nor nonlinear associations between age and health problems at both T1 and T2 were significant at p < .05: linear correlations ranged between r = −.10 (p = .09; 95% CI: −.15, −.04) and r = .09 (p = .12; 95% CI: −.03, .20), whereas associations between squared age and health problems ranged between r = −.10 (p = .09; 95% CI: −.15, .04) and r = .09 (p = .13; 95% CI: −.03, .20). In addition, neither did we find any sex differences (female = 0 and male = 1) in health problems nor links between health problems and sex × age interactions: correlations ranged between r = −.07 (p = .18; 95% CI: −.14, .02) and r = .08 (p = .13; 95% CI: −.03, .20).
As our sample size was limited and we wanted to base our analyses on maximum statistical power for statistical inferences, we treated each twin as individual in the combined sample for our main analyses. However, the calculation of standard errors in the context of twin data ignoring the dependence of data within twin pairs may lead to estimates that are either too large or too small (depending on the underlying twin correlation structure) and, hence, to p–values that might be lower or larger than warranted. Therefore, we additionally ran analyses based on twin A and twin B subsamples. Each sibling of a twin pair (including single twins) was assigned to one of the two subsamples based on birth–order information such that members of a twin pair did not enter the same subsample. The correlations between twins’ birth order (first born = 1 and second born = 0) and all personality parcel variables as well as all health problem item variables were not significant (p < .05) and ranged between r = −.10 (p = .08; 95% CI: −.22, .01) and r = .11 (p = .06; 95% CI: .00, .22).
Main analyses
All main analyses were based on latent variable modelling approaches controlling for variance due to error of measurement (i.e. controlling for item–specific components in case of health problems and parcel–specific components in case of personality traits). These analyses were run using structural equation modelling (SEM), which were conducted with the add–on software
Univariate latent change model analyses
To estimate average developmental trends and differences in individual trajectories of the FHP and subjectively experienced health problems over time, we first performed latent change model analyses (McArdle, 2009) and thus modelled FHP and SHP as latent variables on the basis of their indicating three items, respectively. In these SEM analyses (Figure 1), latent variable scores at T1 and T2 were decomposed into level and change scores. The level variable's mean represents the baseline average of true scores at T1 and its variance reflects interindividual differences in individual true scores at T1, whereas the change variable's mean represents the average true score change and interindividual differences in linear intraindividual true score changes over time. The level and change variables have to be correlated to interpret the latent change variable as true change (Steyer, Eid, & Schwenkmezger, 1997). Even though we did not find correlations between health problems and age as well as sex within T1 and T2, age and sex may be associated with change in health conditions. Therefore, we additionally allowed for correlations of level and change with sex and age at T1.
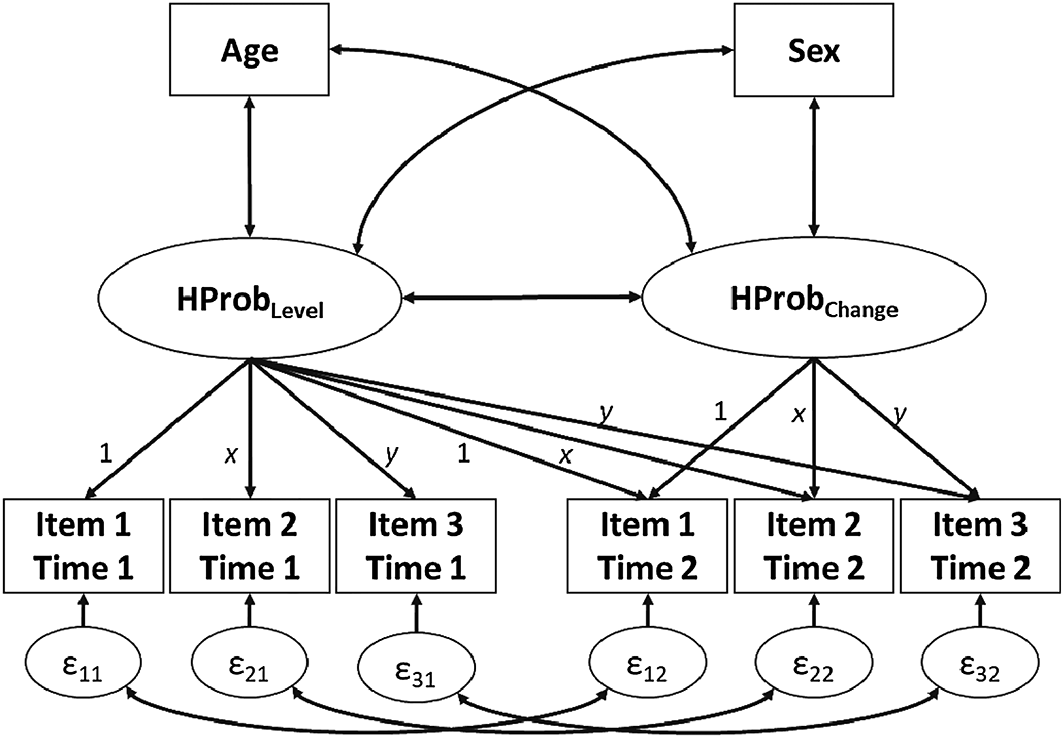
Univariate latent change model of health problems (HProb): the means of item 1 are fixed to zero, and the means of items 2 and 3 (as well as the item loadings on the level and slope variables) are constrained to be equal across measurement occasions in order to estimate means and variance in level and change scores. Measurement error components (ε) of items 1–3 are allowed to correlate across measurement occasions. Individual differences in item scores at time 2 are decomposed into variances due to level, change, two times the covariance between level and change and measurement error. Level and change variables are allowed to correlate with age and sex.
Latent change twin model analyses
Univariate latent change model analyses are informative about average and variance in true score change in health conditions. The combination with a twin model, however, additionally allows for estimations of the genetic and environmental sources of individual differences in intraindividual changes as well as in baseline true scores in a variable of interest. These latent change twin model analyses (Figure 2) can disentangle additive genetic factors (A) from components due to environmental influences shared (C) and not shared (E) by twins controlled for unsystematic error variance (ε). The estimation of the additive genetic variance component is based on the difference in the proportion of segregating genes shared between MZ twin siblings (100%) and DZ twin siblings (on average 50%) and on the assumptions that components of environmental influences are equal for MZ and DZ twin pairs. The model also assumes the absence of assortative mating of twins’ parents with respect to the variables investigated and also rests on the assumption of no interplay between genetic and environmental factors. Consequently, larger MZ compared with DZ twin correlations regarding the level and change in health problems are attributable to differences in the genetic similarity of MZ and DZ twins indicating additive genetic influences on individual differences in level and change. Even though the model also assumes the absence of nonadditive genetic effects, estimates of additive genetic effects derived from twin models are good estimations of broad–sense genetic influences including additive and nonadditive genetic factors (Hill, Goddard, & Visscher, 2008). Shared environmental influences are indicated when the MZ and DZ twin correlations are significant but do not differ markedly in size, whereas nonshared environmental influences are substantial when MZ twin correlations are rather low. 3
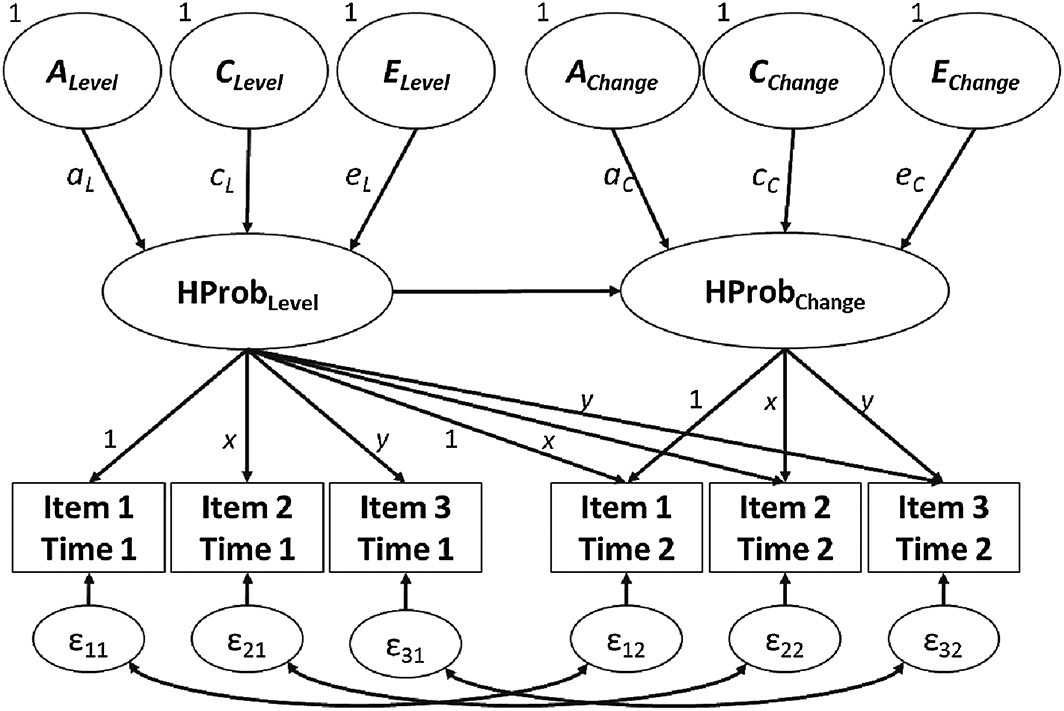
Latent change twin model of health problems (HProb): controlled for variance due to random error (ε) and stable non–random item–specific variance (correlations between error variables); this model disentangles individual differences in level and change into variance components due to additive genetic influences (ALevel and AChange), environmental influences shared by twins (CLevel and CChange) and environmental influences not shared by twins (ELevel and EChange). For simplicity, the model is shown for only one twin. Additive genetic factors are correlated at r A = 1 for monozygotic and r A = .5 for dizygotic twins. Shared environmental components are perfectly correlated within monozygotic and dizygotic twins, whereas nonshared environmental and error of measurement components are uncorrelated between twin siblings. All genetic and environmental variance components are fixed to one in order to estimate effects through path coefficients (a L and a C , additive genetic effects on level and change; c L and c C , shared environmental effects on level and change; e L and e C , nonshared environmental effects on level and change). See text for further model assumptions.
Bivariate latent change model analyses
To investigate the interrelation between personality traits and health problems over time, we ran bivariate latent change model analyses (McArdle, 2009; Soto, 2015). The bivariate latent change model approach allows estimations of initial correlations between personality traits and health problems at T1, correlations between personality trait change and true score change in health problems as well as effects from baseline levels of one variable on the degree of subsequent change in another variable (Figure 3). This bivariate latent change model approach provides information on the patterns of links between changing variables. It also allows estimations of prospective effects from personality trait levels and health status at an initial point of time on subsequent change in personality trait levels and health status controlled for correlations between the two variables at an initial point of time.
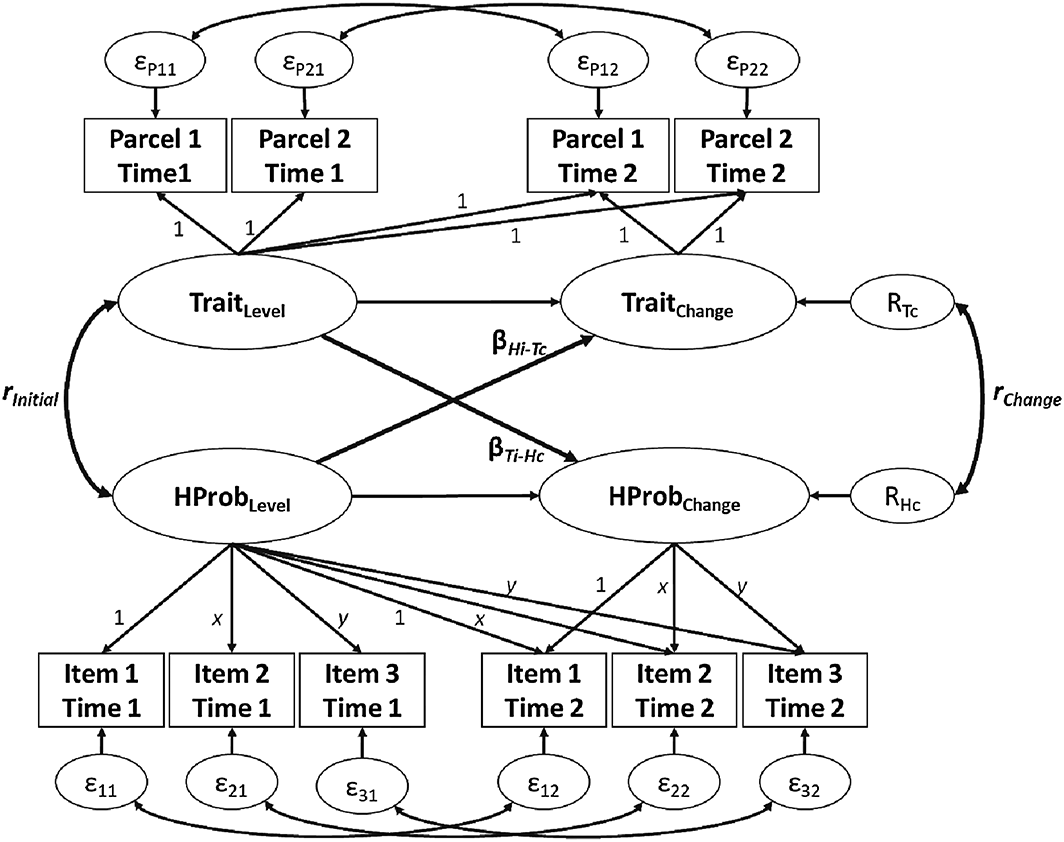
Bivariate latent change model: the means of parcels 1 and item 1 are fixed to zero, and the means of parcels 2, item 2 and item 3 are constrained to be equal across measurement occasions in order to estimate average level and change scores. The model allows estimations of initial correlations between latent personality trait levels and health problems (HProb) at time 1 (rInitial), correlations between latent personality trait change and change in health problems (rChange) as well as prospective trait effects on change in health problems (βTi → Hc) and prospective effects of health problems on trait change (βHi → Tc).
Results
Average and individual level and change in health problems
The univariate latent change model analyses yielded at least acceptable model fit as indicated by root mean square error of approximation (RMSEA) <.08 and comparative fit index (CFI) >.90 (Hu & Bentler, 1999; Steiger, 1990) for both latent variables of health conditions, FHP (χ2 = 40.81; df = 18; RMSEA = .055; CFI = .950) and SHP (χ2 = 54.76; df = 18; RMSEA = .069; CFI = .948). In line with and in addition to preliminary but less reliable composite–based and item–based mean–level change analyses (Tables 1 and S3), we found significant average change for FHP as well as for SHP, indicating that health problems increased from average age 71 to 76 years (Table 2). Furthermore, latent change model analyses revealed that individuals significantly differed in the intraindividual slope of FHP and SHP. Neither age nor sex was significantly associated (p < .05) with change in health conditions (Table 2). The findings were consistent across twin A and twin B subsamples, except for the average change in the FHP (Table S5).
Univariate latent change model fitting results: model parameter estimates
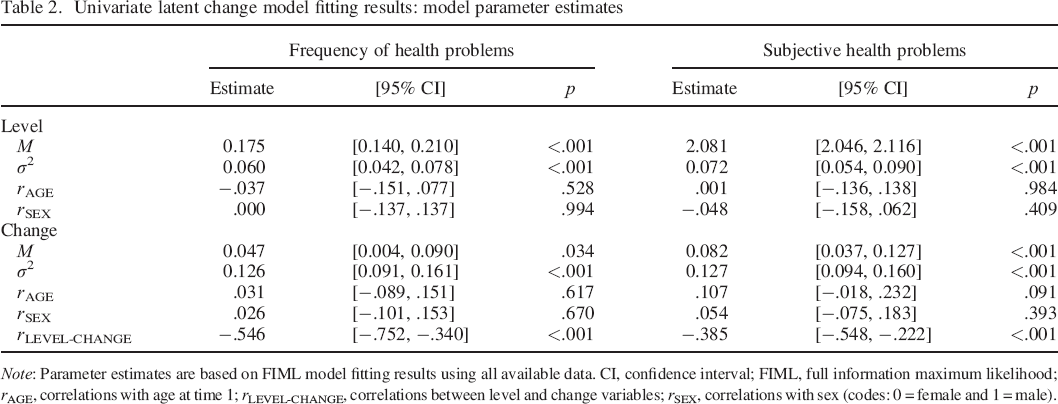
Note: Parameter estimates are based on FIML model fitting results using all available data. CI, confidence interval; FIML, full information maximum likelihood; rAGE, correlations with age at time 1; rLEVEL–CHANGE, correlations between level and change variables; rSEX, correlations with sex (codes: 0 = female and 1 = male).
Sources of individual differences in level and change in health problems
The proportions to which variance in intraindividual true score changes as well as level of health problems were due to genetic, shared environmental and nonshared environmental influences were estimated via latent change twin model analyses. MZ and DZ twin correlations based on composite scores of health problems were low and mostly not significant (Table S6), suggesting strong influences acting to make twin siblings different from one another (i.e. nonshared environmental influences). The results of the latent change twin model fitting are presented in Table 3.
Latent change twin model fitting results: model fit indices and model parameter estimates
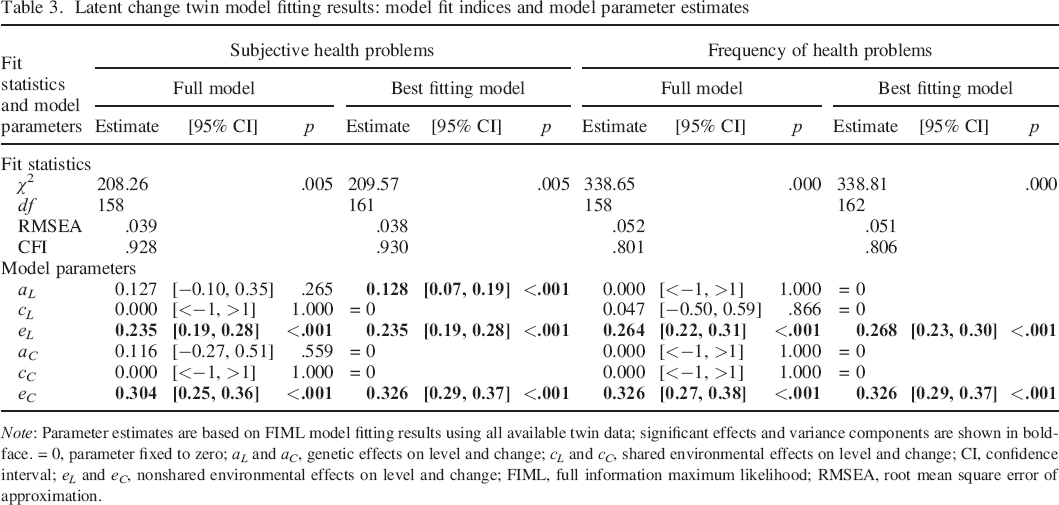
Note: Parameter estimates are based on FIML model fitting results using all available twin data; significant effects and variance components are shown in boldface. = 0, parameter fixed to zero; a L and a C , genetic effects on level and change; c L and c C , shared environmental effects on level and change; CI, confidence interval; e L and e C , nonshared environmental effects on level and change; FIML, full information maximum likelihood; RMSEA, root mean square error of approximation.
Model fitting analyses indicated that level variance in SHP was attributable to both significant genetic and nonshared environmental influences. Fixing the shared environmental variance components in level and change as well as the genetic variance component in change to zero did not lead to a significant decline in model fit (Δχ2 = 1.308; Δdf = 3; p = .727). However, fixing the genetic level component in SHP to zero yielded a significantly worse model fit (Δχ2 = 4.471; Δdf = 1; p = .034). Generally, genetic factors accounted for a relatively small component of subjective health status level (23%), whereas environmental factors contributing to the differential continuity in SHP were substantial (77%) and not shared by twins. Regarding individual differences in subjective health change, model fitting results suggested that nonshared environmental factors represented the primary source, whereas factors shared by twins showed negligible contributions.
For FHP, model fitting analyses yielded significant level and change components that were neither due to genetic factors nor attributable to shared environmental influences. Fixing the shared environmental and genetic components to zero did not lead to a significantly worse model fit (Δχ2 = 0.165; Δdf = 4; p = .997). That is, environmental influences unique to individuals represented the primary source of differential continuity and individual differences in slopes of the FHP. 4
In sum, interindividual differences in intraindividual true score changes were found to be due to individual–specific environmental influences not shared by twins. This is noteworthy, because in case of significant links between true change in personality traits and health problems, these change correlations would be environmentally mediated.
The interrelations between personality traits and health problems
For all 10 investigated associations based on bivariate latent change models, the model fit was at least acceptable (Table 4). The model fitting results yielded that there were no initial correlations between personality trait levels and health problems, except the positive association between neuroticism and subjective assessments of health problems, indicating that people with higher neuroticism baseline levels reported more health problems (Table 5). FHP (i.e. more days of illness/hospitalization) at T1 predicted an increase in extraversion over time, and increasing FHP was associated with decreasing agreeableness. Increasing SHP over time accompanied increasing neuroticism and declines in extraversion and conscientiousness.
Bivariate latent change model fitting results: model fit indices
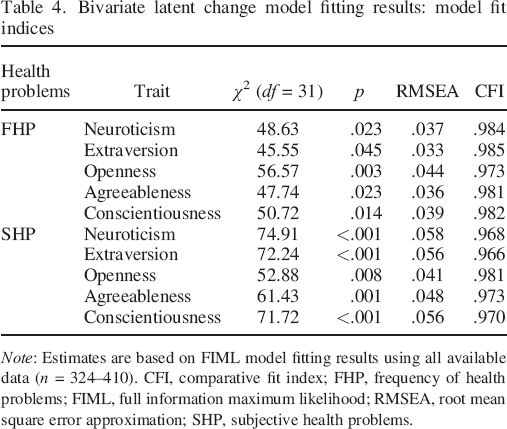
Note: Estimates are based on FIML model fitting results using all available data (n = 324–410). CFI, comparative fit index; FHP, frequency of health problems; FIML, full information maximum likelihood; RMSEA, root mean square error approximation; SHP, subjective health problems.
Bivariate latent change model fitting results: parameter estimates
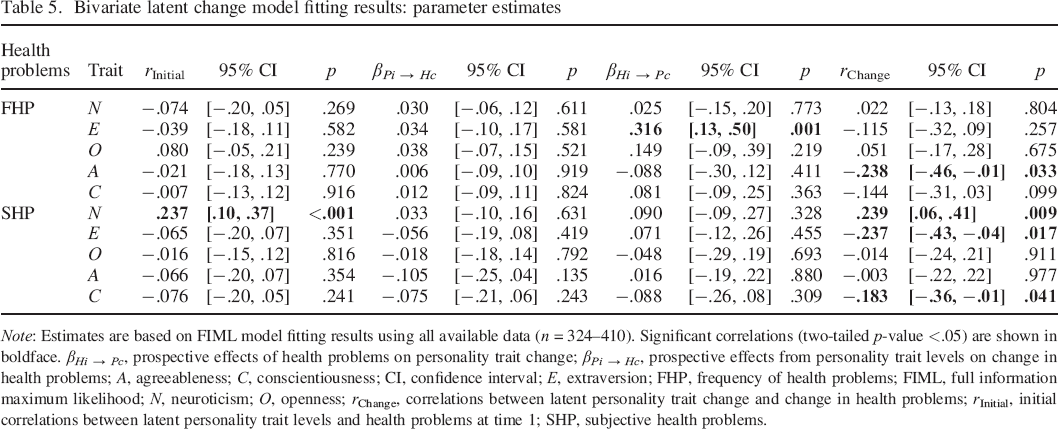
Note: Estimates are based on FIML model fitting results using all available data (n = 324–410). Significant correlations (two–tailed p–value <.05) are shown in boldface. βHi → Pc, prospective effects of health problems on personality trait change; βPi → Hc, prospective effects from personality trait levels on change in health problems; A, agreeableness; C, conscientiousness; CI, confidence interval; E, extraversion; FHP, frequency of health problems; FIML, full information maximum likelihood; N, neuroticism; O, openness; rChange, correlations between latent personality trait change and change in health problems; rInitial, initial correlations between latent personality trait levels and health problems at time 1; SHP, subjective health problems.
Only one significant initial correlation between personality traits and health problems was found (between neuroticism and SHP), but four significant correlated changes. This might be attributable to the fact that the association between health problems and personality traits becomes more important with increasing age. Therefore, we additionally (i.e. post hoc) computed true score correlations between personality traits and health problems within and between measurement occasions based on a latent variable modelling approach. At T1, we only found the significant positive correlation (r = .237; p < .001; 95% CI: .106, .368) between neuroticism and SHP (see also Table S8). FHP at T1 was associated with more extraversion at T2 (r = .189; p < .009; 95% CI: .046, .332) and SHP at T1 showed positive links to neuroticism at T2 (r = .230; p = .001; 95% CI: .093, .367), whereas no personality trait level at T1 showed significant associations with health problems at T2, indicating that health problems predict neuroticism and extraversion, but not vice versa. At T2, however, there were significant correlations between SHP and those personality traits that showed significant average declines over time (Table S8). That is, more SHP were associated with higher neuroticism (r = .223; p = .001; 95% CI: .088, .358), lower extraversion (r = −.193; p = .006; 95% CI: −.330, −.056) and lower conscientiousness (r = −.156; p = .023; 95% CI: −.291, −.021). In addition, FHP was negatively associated with agreeableness (r = −.154; p = .046; 95% CI: −.305, −.003).
In sum, our analyses did indicate systematic change correlations. The latter results were in line with our directed hypotheses, namely, that reversed trends in personality traits in old age (i.e. increasing neuroticism and decreasing extraversion and conscientiousness) are significantly associated with declines in health. Interestingly, we found somewhat contradictory results for extraversion, with FHP predicting an increase (or better, less decline) in extraversion over time and higher SHP at T2 related to lower extraversion at the same time point. Because change in health problems was not significantly attributable to genetic sources or environmental factors shared by twin siblings, the linked change in personality and health might well be attributable to environmental sources, which individually affect one twin sibling but not the other.
Discussion
This study built on previous research showing personality changes and their relationship to health in old age (e.g. Müller et al., 2016; Wagner et al., 2016) and answering the call for more research on the sources of individual differences in health change and personality change across life (Allemand & Martin, 2016). Based on data from a longitudinal study of older adult twins, we investigated to what extent genetic and environmental sources contributed to individual differences in health changes, whether changes in health status over time, measured by more objective and more subjective indicators, were accompanied by reversed personality trait changes in old age and whether levels of one variable predicted change in the other variable.
Summary of results and first implications
In line with our expectations, we found that decreasing health in old age was associated with significant declines in emotional stability, agreeableness, extraversion and conscientiousness. This is also in line with previous studies that found comparable results for those traits. Our results thus replicate and add to the growing body of research on the link between personality changes and health changes in older age. Despite this evidence for correlated changes, we found little evidence for correlations between baseline levels of health problems and personality traits (except the positive link between neuroticism and SHP). In other words, stable differences in personality traits are not accompanied by stable differences in health conditions. This is in line with findings from a recent study by Mõttus, Marioni, and Deary (2017). Regarding health, it might be plausible to assume that not health level per se but rather health changes represent stereotypic markers of the aging process that go hand in hand with role–consistent personality changes.
When investigating prospective effects of personality trait levels and health status at an initial point of time on subsequent change in personality trait levels and health status, we did not find strong directional effects in either direction (except for the somewhat unexpected relation between more FHP and less decline in extraversion over time). This is not in line with our expectations and contradicts previous research, which has provided evidence for both directions of influence. Maybe our relatively small sample size and the time interval of 4.5 years precluded the detection of a bidirectional causation. However, some results of our analyses still allow for interesting insights that go beyond previous research. The combination of a lack of correlations between health and personality at the first measurement occasion (except between neuroticism and SHP) with significant change correlations points to the emergence of systematic links only at a later point in time. This led us to investigate latent variable correlations at both time points. We indeed found that significant associations emerged at the second measurement wave, when even the youngest participants were around 70 years old. Furthermore, this relation was visible for those personality traits that showed significant average declines over time (Kandler et al., 2015). One might thus speculate that the occurrence of personality changes might be expected when health declines become more prevalent and pronounced and thus related to the actual onset of disease and physical deterioration (Wettstein et al., 2017).
Even though we unexpectedly did not find significant linear and non–linear age effects on baseline levels of health and health change in our study, a recent study reported varying effects of neuroticism on functional health and vice versa across different age groups (Müller, Wagner, Smith, Voelkle, & Gerstorf, in press): effects of neuroticism on functional health were found to be stronger in a group aged between 70 and 84 years, whereas health decrements showed stronger effects on change in neuroticism in the oldest old (aged 85+ years). Of course, those different interrelations between personality traits and health for different age periods have to be further addressed in future research, preferably with larger samples and multiple measurement time points, in order to not only detect small effects but also to investigate the onset of directional and concurrent changes and also the bidirectional causality of effects (Luhmann, Orth, Specht, Kandler, & Lucas, 2014).
We also investigated the sources of individual differences in health levels and changes with the help of genetically informative (or rather environmentally sensitive) latent change twin models. We found that individual differences in the level of SHP (i.e. stability or recurrence) were largely attributable to environmental factors but to some degree also to genetic factors. The finding of genetic effects on individual differences in SHP is largely in line with previous studies (e.g. Christensen et al., 2003, 1999; Harris et al., 1992). Conversely, we found that variance in FHP was solely due to environmental factors not shared by twins. This lack of genetic effects for FHP seems surprising, because Christensen et al. (1999) found genetic effects on the rate of hospitalization. Harris et al. (1992), on the contrary, found no significant genetic effects on objective indicators of health in an older age group of their sample. Evidence for genetic influences on health may be sensitive to the choice of health measure, with better evidence for more subjective as opposed to more objective indicators.
Furthermore, and in line with our expectation, the longitudinal twin model analyses indicate that individual differences in change in both indicators of health problems are exclusively attributable to individual environmental influences not shared by twins. This is especially important, because we can infer from these results the common underlying sources of the correlated changes we found in our bivariate latent change models.
Implications for the interrelation between health and personality in old age
Because previous studies (e.g. Kandler et al., 2015; Read, Vogler, Pedersen, & Johansson, 2006) found that changes in personality traits in old age are also mainly attributable to environmental influences that act individually, the association between personality trait change and health change must be due to individual environmental circumstances and not to genetically driven deterioration in old age. This knowledge suggests that environmental factors individually affect changes in health problems that accompany reverse personality trends in old age. Even though this finding has to be replicated by future studies before drawing definitive conclusions, it highlights the power of the environment that acts to increase dissimilarity between genetically identical individuals (i.e. monozygotic twins) regarding health as well as personality in old age. It further provides evidence that concurrent changes in health and personality are not due to genetic deterioration processes affecting both variables. Our results provide a first empirical basis for further research on potential environmental risk factors of health problems and (or) environmental protective factors of health in old age. From a developmental viewpoint, the results from our study could also be used to more specifically investigate the timing and duration of environmental factors affecting health and personality in later life.
The fact that concurrent changes in health and personality traits are due to environmental factors also gives some indication on the directionality of effects. Because personality differences are rather stable and substantially genetically influenced, at least partial genetic mediation would be plausible if personality traits would affect health problems. A reasonable case can be made for SHP that showed stable associations with neuroticism, and stability in both neuroticism and SHP is at least moderately genetically influenced. However, our results indicate that correlated changes in both variables are not driven by genetic factors and most likely environmental, or are at least due to person × environment interactions in terms of interactions between genetic factors and environmental resources not shared by twins. The latter would act as nonshared environmental factors, if present but not taken into account in the model (Kandler & Zapko–Willmes, 2017). Thus, personality traits may account for the stability and genetic variance in health assessments (Kandler, Zimmermann, & McAdams, 2014) but less likely account for health change. This knowledge might facilitate the search for such environmentally triggered third variables in future research and thus a starting point for possible interventions related to both personality but also health change. For example, decreasing possibilities to interact with the physical and social environment (e.g. loss of partner and reduced mobility), as well as limited (e.g. financial) resources, might be promising candidates (Müller et al., 2017).
A strength of our study was that we included measures of different facets of health: SHP, indicative of one's current personal evaluation of health problems, and FHP, which although also self–reported (and thus susceptible to the related reporting biases), is less dependent on the persons’ subjective feeling. Furthermore, both constructs were measured with more than just one item and could thus be modelled as latent variables controlled for random error of measurement. In line with previous findings on subjective and more objective health (e.g. Wettstein et al., 2017), results for SHP and FHP differed. Increases in FHP were related to declines in agreeableness, possibly indicating reduced resources to invest in social relationships, which might also be linked to health changes.
Furthermore, the only prospective effect that emerged was the positive effect of FHP at T1 on change in extraversion. Given the significant decline in extraversion over time (Kandler et al., 2015), this indicates that more frequent health problems predict less decline in extraversion. This is intriguing, because we also found significant correlations between declines in extraversion and increases in SHP. Extraversion might be especially prone to changes in health problems. On the one hand, a plausible reaction to a perceived decline in health status might be to narrow down social and outgoing activities as well as energy, which are key facets of extraversion. But on the other hand, more frequent health problems may increase the probability to seek for more support from others. Thus, specific facets or nuances of extraversion may show different trends due to different mechanisms.
Subjective ratings of health problems were also related to changes in neuroticism and conscientiousness. The association between changes in health and changes in conscientiousness is in line with previous research that has connected conscientiousness with a variety of health variables throughout life (e.g. Friedman & Kern, 2014). The positive association between SHP and neuroticism, visible in moderate initial and change correlations, is also not surprising because more neurotic (i.e. more depressive and anxious) people see the world, their lives and their experiences in a more negative light (Kandler & Ostendorf, 2016). Moreover, previous research suggests that neuroticism is more strongly related to subjective health measures and symptom reporting, whereas its relation to objective health is less clear (Israel et al., 2014; Jokela et al., 2014, but see Wettstein et al., 2017). In contrast to FHP, levels of subjective health were also influenced by genetic sources. These genetic influences may in part be accounted for (or mediated) by neuroticism (Weiss et al., 2008).
Implications for developmental regulation in old age
Our results linking personality and health change in older age warrant further replication to prove robust, and the possible underlying reasons and mechanisms, such as general deterioration of functioning in old age or environmentally induced wear–and–tear processes, need to be investigated. However, and even though our data do not speak directly to this issue, another speculation might come to mind. Personality development is inherently linked to the changing developmental tasks across the lifespan (Hutteman et al., 2014), and coping with health changes constitutes one central developmental task in older age. It thus stands to reason that personality changes after midlife might be functionally linked to these challenges and changes that are prevalent in old age. Analogously to what is assumed to be one of the functions of the maturity principle of personality development in younger years (Bleidorn & Schwaba, 2017; Roberts et al., 2006; see also Müller et al., 2017), personality change in older age might be instrumental in mastering these transitions. This perspective also provides a theoretical link to theories of adaptive lifespan development, such as the theory of selection, optimization and compensation (Baltes, 1987). When individuals are faced with an increasingly negative ratio of developmental gains and losses (such as health deterioration), their personality might be subject to changes that are differently functional or adaptive compared with younger ages. Resources have to be invested differently to maintain one's well–being in older age, and goals might shift. For example, becoming more neurotic might be due to a higher investment of resources into a heightened awareness to identify and avoid problems, challenges and dangers of everyday life (which might be considered compensation of reduced resources to tackle those problems and challenges). Becoming less extraverted might be the consequence or at least the reflection of the investment of scarce resources rather in close friendships instead of maintaining an extensive social circle (i.e. loss–based selection). The execution of these principles and the concurrent personality changes might thus help to master transitions in old age.
In order to follow up on our results and to explicitly test this idea, future research should continue along these lines in order to investigate to what extent the reported changes in personality are indeed functional and thus in line with theories of developmental regulation in older age. This could be achieved by directly showing that the proposed changes in personality are related to indicators of successful aging, such as social participation and independence, as well as the ongoing maintenance of health (i.e. fewer additional conditions) and well–being in late life (Kandler et al., 2015; Müller et al., 2017). Furthermore, people whose personality and health changes in orchestration (i.e. a high change correlation in the assumed direction) might show improved functioning in old age compared with those with lower correlated change.
Furthermore, it will be necessary to understand the exact mechanisms and processes underlying concurrent health and personality changes. Recent propositions regarding the mechanisms of personality development, such as the Triggering situations, Expectancy, States/State expressions, and Reactions framework (TESSERA) might be useful to understand these underlying processes (Wrzus & Roberts, 2017). Repeated experiences of challenging everyday situations due to health restrictions might lead to a gradual change in perceptions and behaviour, manifesting in long–lasting personality change according to the refined formulation of the maturity principle for old age: ‘Opposite trends in old age can be explained by different developmental and adaptive strategies … compared to younger adults’ (Kandler et al., 2015, p. 188).
Limitations and further directions for future research
Even though our study exhibits a number of strengths, such as the longitudinal twin design and the differentiated measures of health, a number of limitations have to be kept in mind that also point to directions for future research. We found concurrent changes in health and personality only for some traits. Previous studies have been heterogeneous in the way that they sometimes did find significant effects for all Big Five traits (e.g. Müller et al., 2016; Stephan et al., 2017), whereas other studies only found effects for some of the traits (e.g. Wagner et al., 2016). It has to be noted though that if significant mean–level changes are found, they are in the direction of increased neuroticism, and decreases in the four other factors, which is in line with the theoretical idea of a refined formulation of the maturity principle for old age (Kandler et al., 2015).
Our sample was comparatively small in size at least for genetically informative analyses and the interval between T1 and T2 spanned about five years, which might prevent the detection of small effects over a shorter or even longer time period (Luhmann et al., 2014). Because we performed a number of statistical tests, our alpha level might also be considered rather liberal. Still, we had directed hypotheses, and the different analyses were not all run to test the same hypotheses; thus, we retained our alpha level at p < .05 in order not to inflate beta errors (i.e. the type II error rate). Nevertheless, replications of our results with larger samples are strongly warranted. Variance restrictions due to dropout of less healthy people might also play a role, limiting the magnitude of the observable correlations. Even though the differences were not significant, health problems for the cross–time dropout subsample at T1 tended to be larger compared with the subsample that also participated at T2 for both FHP (M = 0.49 vs. M = 0.29) and SHP (M = 5.65 vs. M = 5.44).
Our measures of health, even though including different facets, only cover some aspects, whereas other potentially relevant facets of health that have been investigated in previous studies (e.g. objective physician–rated health, measures of fitness and strength such as grip strength and measures of sensory impairment) were left out. The kind of health assessments might play a role with regard to the association between personality and health. This is also relevant considering the comparison standards (i.e. intraindividual change, comparison with younger people or people of one's age) that are used as anchor when evaluating one's health, which might influence the ratings and their developmental trajectories (e.g. Sargent–Cox, Anstey, & Luszcz, 2010). Further studies should thus aim at an even more differentiated and structured assessment of different objective and subjective health restrictions in order to obtain a full picture.
Even though we did not find any substantial effects of participant age on health status and change nor on personality trait change (Kandler et al., 2015), we did find that relations between health and personality emerged only at the second measurement occasion. Relatedly, our sample had a rather large age range, spanning from participants in ‘young old age’ to those already well into the fourth age. Given the larger restrictions of health and reduced autonomy in latest life, effects might differ for younger and older participants (Gerstorf et al., 2010; Müller et al., in press). Our sample size precluded the investigation of such age effects in more detail. Therefore, as mentioned above, those questions should be investigated in future research, with more statistical power and designs better suited for detecting the onset and interrelatedness of changes in later life.
Even though we used a latent variable modelling approach to control for measurement error, a limitation is that all our measures relied on participants’ self–reports. Thus, the correlations between variables and the estimates derived from the twin models might be biased by shared method variance and non–random rater biases (e.g. due to response styles). Accordingly, the sole reliance on self–reports has been frequently criticized (Kandler, Riemann, & Angleitner, 2013). It is thus strongly warranted for further research to include additional variables such as physician ratings of health status, official accounts of sick leave days and peer reports or observer ratings of personality traits in order to disentangle substantive effects from those that are due to shared method or other artificial sources of variance and also to get to the core of more specific associations between these variables.
It might also be interesting to disentangle the Big Five traits further into personality facets, or even personality nuances (Mõttus, 2016; Mõttus, Kandler, Bleidorn, Riemann, & McCrae, 2017). This may reveal a more rigorous and differentiated picture that helps to understand where and when correlated change between health and personality is most prevalent. Chopik (2016) could show that the relationship between conscientiousness and health in later life was dependent on the facet of conscientiousness employed: orderliness, industriousness and responsibility predicted chronic illnesses and self–rated health, whereas virtue did not; self–control only predicted illnesses but not self–rated health. This might be true for other personality traits as well (cf. Sutin et al., 2013). In addition, the investigation of moderator variables (i.e. the perception of one's own age, Stephan, Sutin, & Terracciano, 2014; sensory impairment, Wettstein, Kuźma, Wahl, & Heyl, 2016) and differences in changes (i.e. is the association between health changes and personality changes uniform across individuals, and if not, which variables predict individual differences in the strength of these relations?) are required in order to be able to integrate the results found in previous research.
Despite these limitations and open questions, our study offers new insights regarding health and personality development in later life, and the interrelation between personality traits and one central aspect of aging, namely, increases in physical health problems. The investigation of correlated changes and the sources of individual differences in health changes allow for a better understanding of the linkage between personality and health in old age: reverse personality trends go hand in hand with increasing health problems, and this association is environmental. The findings are in line with the theoretical idea that adaptive personality development in later life might differ from what has been established for young and middle adulthood.
Acknowledgements
The present research used data from the Genetic Oriented Lifespan Study on Differential Development (GOLD), which was conducted at the former Max Planck Institute for Psychological Research in Munich, Germany. GOLD was directed by Franz E. Weinert and funded by the Max Planck Society. Members of the GOLD research team were Ulrich Geppert, Frank Halisch, Ernst Hany, Franz J. Neyer, Gertrud Nunner–Winkler and Michael R. Waldmann. We thank the team as well as the GOLD participants for spending part of their lifetime with the GOLD study.
Supporting info item
Supporting info item, per2135-sup-0001-PER2135_supplement - Sound Body, Sound Mind? The Interrelation between Health Change and Personality Change in Old Age
Supporting info item, per2135-sup-0001-PER2135_supplement for Sound Body, Sound Mind? The Interrelation between Health Change and Personality Change in Old Age by Kornadt Anna E., Hagemeyer Birk, Neyer Franz J., Kandler Christian and Back Mitja in European Journal of Personality
Supporting info item
Supporting info item, per2112-Sup-0001-PER_Open_Practices_Disclosure_Form_PER 2135 - Sound Body, Sound Mind? The Interrelation between Health Change and Personality Change in Old Age
Supporting info item, per2112-Sup-0001-PER_Open_Practices_Disclosure_Form_PER 2135 for Sound Body, Sound Mind? The Interrelation between Health Change and Personality Change in Old Age by Kornadt Anna E., Hagemeyer Birk, Neyer Franz J., Kandler Christian and Back Mitja in European Journal of Personality
Open Practices Disclosure
Footnotes
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.