
Abstract
Background:
Dermatophytes can mimic or possibly trigger mycosis fungoides (MF).
Objectives:
To present the case of a 55-year-old male referred for MF refractory to therapy who instead had extensive tinea pseudoimbricata (concentric, annular lesions secondary to Trichophyton rubrum).
Methods:
Case report with biopsy and cultures.
Results:
Oral antifungal therapy dramatically improved his lesions, and only a few MF lesions persisted after treatment.
Conclusions:
Concurrent tinea may confound the treatment and diagnosis of MF.
MYCOSIS FUNGOIDES (MF) is an indolent epidermotropic cutaneous T-cell lymphoma of helper/memory T cells that presents as heterogeneous, papulosquamous patches, plaques, and tumors. 1 Few cases of MF with superimposed fungal infection masking and/or exacerbating the disease have been reported.2–4 Tinea pseudoimbricata is a delayed hypersensitivity to the cytoplasmic antigen of the Trichophyton species and has not been reported with MF. 5 We present a patient with MF resistant to therapy who had extensive tinea pseudoimbricata secondary to Trichophyton rubrum.
Case Report
A 55-year-old African American male was referred for MF refractory to therapy. He had a 30-year history of a pruritic rash that began on his feet when he was in Vietnam. It gradually spread to involve his legs and trunk over years. Treatment for tinea pedis improved his rash on the feet, but he did not use antifungal therapy elsewhere. A histologic diagnosis of MF, including clonal T-cell receptor gene rearrangement, was made from a skin lesion biopsy in 2003, 1 year before presentation. Topical mechlorethamine had triggered an inflammatory reaction and was discontinued. Psoralen plus ultraviolet A (PUVA) was given three times per week beginning 1.5 years prior to presentation, but there was “progressive disease.” He received treatment with oral bexarotene, eight tablets (600 mg) daily, but he experienced disease progression, anemia, and dose-limiting hypertriglyceridemia.
At initial presentation in July 2004, there were large annular, erythematous concentric rings with scaly outer borders present on the trunk and extremities (Figures 1 and 2). Confluent papulosquamous plaques covered 60% of the body surface, including the abdomen, thighs, right arm, left flank, and lower groin, with keratoderma of his feet. The most indurated areas with superimposed pustules were present on the thighs. White superficial onychomycosis was present on nails. Skin scrapings from lesions on the thigh, feet, back, and abdomen were floridly positive for dermatophyte hyphae. A lesional skin biopsy taken from a ring lesion on his abdomen showed a perivascular lymphocytic infiltrate intermixed with a few plasma cells and eosinophils cuffing the dermal blood vessels. The lymphocytes were small, without atypia or epidermotropism (Figure 3), and the periodic acid–Schiff stain for fungus was negative. Fungal cultures taken from lesions on the back, thighs, and lower legs grew T. rubrum. Staphylococcus aureus was cultured from his thigh pustules. There was no adenopathy.
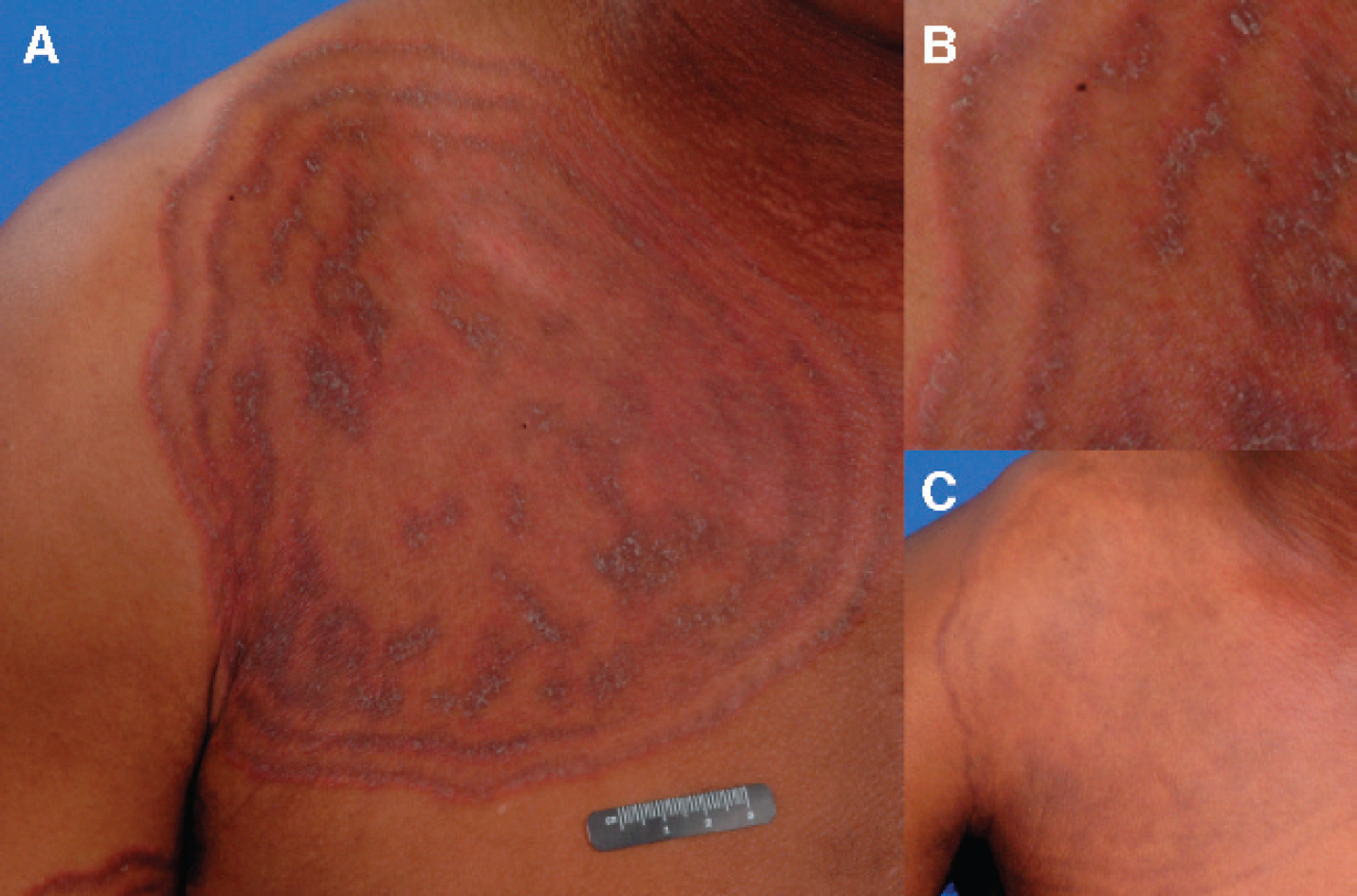
Clinical appearance of tinea pseudoimbricata A, Extensive involvement of the trunk with large, erythematous, annular concentric circles with scaly outer borders secondary to infection with Trichophyton rubrum. B, Close-up view of concentric circles with scaly outer borders. C, Post-treatment with mild postinflammatory hyperpigmentation.

Clinical appearance of tinea pseudoimbricata A, Extensive involvement of the legs with large annular and erythematous concentric circles with scaly outer borders secondary to infection with Trichophyton rubrum. B, Post-treatment with mild postinflammatory hyperpigmentation.
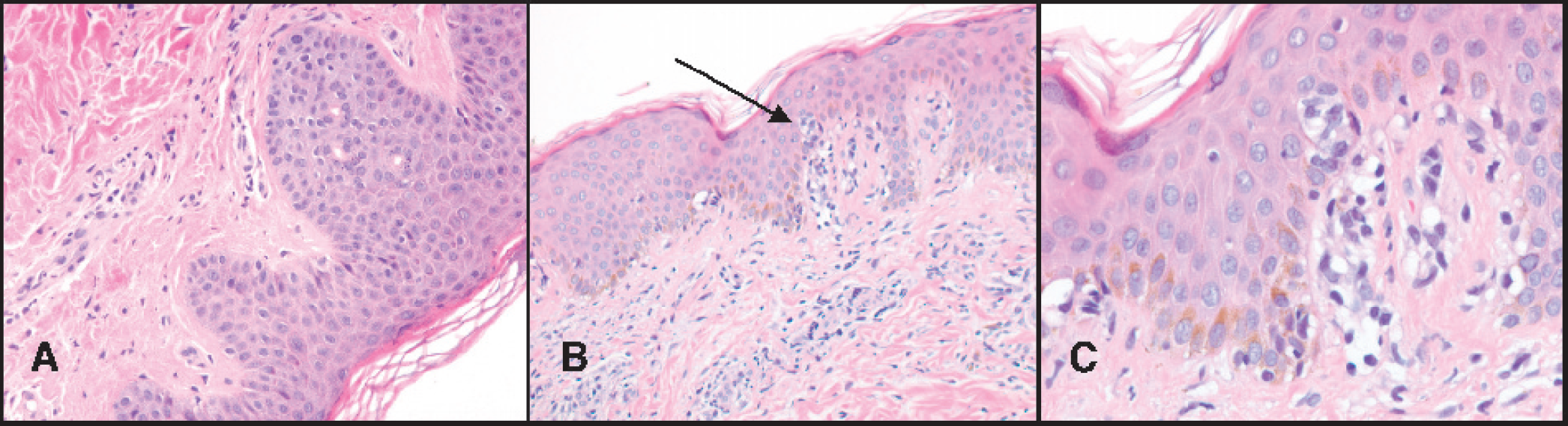
Histology of lesional skin biopsy specimens. A, There is mild perivascular lymphocytic infiltrates of morphologically unremarkable small lymphocytes intermixed with few plasma cells and eosinophils, suggesting erythema annulare centrifugum (40×). B, Low-power view of lymphocytic infiltrate with Pautrier's microabscesses. Arrow indicates Pautrier's microabscesses (40×). C, An atypical lymphocytic infiltrate of moderate density is present in the superficial dermis and epidermis with the presence of Pautrier's microabscesses. Most lymphocytes are of medium size, with some admixed large lymphocytes (100×). This morphologic change is characteristic of mycosis fungoides. Periodic acid-Schiff stain.
There was no evidence on flow cytometry of an aberrant clone of CD4(+)/CD26(–) T cells in the blood, skin, or bone marrow. The absolute CD4 count (164 IU) was lower than normal (202–1,453 IU). Serology for human immunodeficiency virus (HIV)-1 and −2, cytomegalovirus, and Epstein-Barr virus was negative, as was the rapid plasma regain test. Lactate dehydrogenase was elevated (695 IU/L, normal < 618 IU/L), and the soluble interleukin-2 receptor was at the lower limits of normal. He was therefore staged at IB, T2N0B0.
The patient was treated initially with oral terbinafine 250 mg daily and dicloxacillin 500 mg twice daily. He was told to apply naftifine cream twice daily to the affected areas and mupirocin to fissures, ulcers, and nares for Staphylococcus. One month later, the annular and concentric lesions had cleared, leaving only postinflammatory hyperpigmentation (see Figures 1C and 2B). After antifungal therapy, he had a few remaining pink papules and plaques on the trunk comprising less than 1% body surface area. New lesional biopsy specimens from the back and abdomen plaques were interpreted as MF based on the presence of markedly atypical lymphocytes in the superficial dermis and epidermis and in Pautrier's microabscesses (see Figure 3, B and C). Most of the lymphocytes present were medium in size, with some admixed large lymphocytes. Epidermal atypical lymphocytes were positive for CD4, negative for CD8, and 10% and 5% stained positive for CD25 and CD30, respectively. The dermal T cells stained positive for CD8. Monoclonal T-cell receptor gamma chain gene rearrangements using the V-gamma-2 primer were detected by polymerase chain reaction analysis.
The patient was started on a 10 mg percentage of mechlorethamine ointment to the body and topical clobetasol 0.05% ointment to MF lesions and was to continue terbinafine 250 mg daily for 1 week per month for tinea. At the 3-month follow-up, the tinea rings had resolved, but new patches and plaques were present on the trunk. Interferon-α with PUVA three times a week was recommended, but the patient continued to use topical mechlorethamine. As of March 2005, he had stable single patches and plaques over 3.5% of his body surface, with a negative potassium hydroxide examination.
Discussion
This is a unique patient who presented with biopsy-proven MF but with extensive concentric, gyrate, wood-grain, annular lesions not typical of MF. His MF had been very resistant to topical mechlorethamine, PUVA, and oral bexarotene. He also had a history of fungal disease beginning many years previously, with a positive response to antifungal therapy used on his lower legs and feet, but he had not tried it elsewhere.
On presentation to our clinic, the patient had positive scrapings for hyphae from the foot, thigh, and trunk lesions, and cultures from these areas grew T. rubrum. Biopsy of the lesions displayed a nonspecific perivascular infiltrate (see Figure 3A) without evidence of MF, raising the question of the lesions being a reactive process. The fact that the patient's lesions began at 60% involvement of his body surface area and decreased to less than 1% after institution of oral and topical antifungal therapy suggests that his skin lesions were predominantly due to a reaction induced directly or indirectly by tinea rather than to MF. The history of gradual onset from feet to trunk over many years suggests that the presence of widespread dermatophytosis may also have been a factor leading to development of MF, that is, the “persistent antigen.”
A number of diseases “mimic” MF clinically and histologically, but they generally resolve with appropriate treatment. 6 The staging of MF is basically built on clinical examination, and each lesion is implicitly assumed to be MF as it is included toward staging. If there is a real mimicker on hand, this assumption is not valid. MF has been previously described with extensive tinea (Table 1). A comprehensive review by Zackheim and McCalmont listed 25 different clinical diagnoses, histologically diagnosed as MF, and included one case of MF masquerading as erythema annulare centrifugum (EAC). 7 We considered EAC, a delayed-type hypersensitivity to dermatophytes,8–10 because his trunk lesional biopsy contained perivascular lymphohistiocytic infiltrates with characteristic “cuffing” or “coat sleeve” of lymphocytes.11–13 The histology of EAC, however, is nonspecific. EAC is described with a trailing edge of scale, whereas the patient's lesions had a leading edge of scale. EAC lesions are most often single annular rings rather than concentric rings within rings.
Previously Reported Cases of Mycosis Fungoides and Tinea Corporis
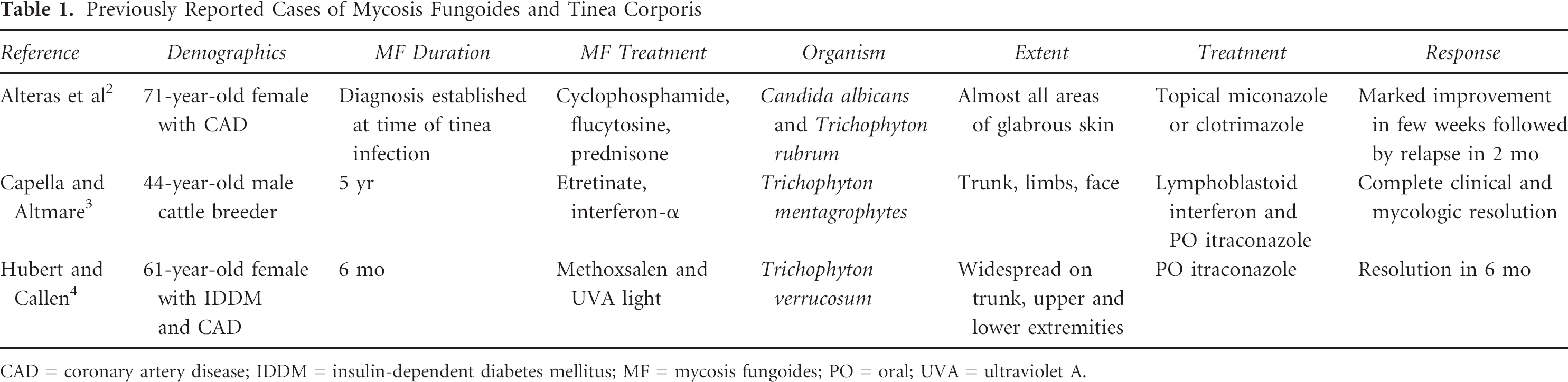
CAD = coronary artery disease; IDDM = insulin-dependent diabetes mellitus; MF = mycosis fungoides; PO = oral; UVA = ultraviolet A.
This latter clinical feature caused us to also consider erythema gyratum repens (EGR) or tinea imbricata in the differential diagnosis. EGR is a rare paraneoplastic syndrome associated with lung, breast, or esophageal cancer.12,13 It has not been reported with MF. Because his annular lesions cleared with antifungal therapy and MF lesions remained, EGR is an unlikely diagnosis.
Tinea corporis does not manifest clinically with concentric rings, except for tinea imbricata in association with Trichophyton concentricum on glabrous skin. 14 Since this patient's cultures grew T. rubrum from trunk, leg, and thigh lesions, it does not fit the existing definition of tinea imbricata, a delayed hypersensitivity confined to T. concentricum cytoplasmic antigen. T-lymphocyte hyporeactivity is thought to allow sequential waves of scaling and infection to occur, forming the widespread, annular, erythematous concentric rings. 5 Our patient had a low absolute CD4 count (with negative serology for HIV), which may have increased his susceptibility to extensive tinea corporis with a tinea pseudoimbricata–like reaction. Also, MF patients have increased susceptibility to infections that involve cutaneous T cells in addition to tinea, such as herpes, Kaposi's varicelliform eruption, 15 and other cutaneous malignancies. 16 Three cases of so-called tinea pseudoimbricata or “tinea indecisiva” with Trichophyton tonsurans and Trichophyton mentagrophytes have been reported to mimic tinea imbricata's widespread, annular, erythematous, scaling concentric rings.17,18 Tinea pseudoimbricata and coexisting MF best fit the clinical presentation of this patient. We suspect that the tinea pseudoimbricata is essentially a rare clinical presentation of EAC, the more common delayed hypersensitivity reaction to the dermatophyte antigen.
This patient illustrates Tan and colleagues' hypothesis that “MF may arise in the setting of a persistent cutaneous antigen,” in this case supplied by T. rubrum. 19 A T cell-mediated contact hypersensitivity reaction to dermatophyte antigens caused the clinical appearance of erythema, scaling, and even bullae characteristic of tinea and, in this case, concentric rings. Although we suspect that longstanding tinea triggered the onset of MF in this patient, he continued to develop new lesions after antifungal therapy that were confirmed as MF by biopsy features, including epidermotropism and positive T-cell receptor gamma gene rearrangements. The remaining lesions did not contain fungal hyphae, indicating that MF persisted despite the resolution of the initial fungal infection. T-cell lymphocytes from MF lesions demonstrate loss of activation-induced cell death. 20 Successful treatment of extensive MF in a refractory patient using oral and topical antifungal therapy underscores the importance of excluding coexisting dermatophytosis in patients with MF. As the legendary Dr. Lamar Callaway would have said, “If it scales, scrape it!”