
Abstract
Background:
Diagnosis of pyoderma gangrenosum can be difficult, leading to overdiagnosis or underdiagnosis.
Objective:
To identify clinical features helpful in establishing a diagnosis of pyoderma gangrenosum and to compare the characteristics of patients with pyoderma gangrenosum with those of patients with chronic venous ulcers.
Method:
A retrospective chart review was performed in 28 patients with typical pyoderma gangrenosum and compared with the clinical features in 28 patients with chronic venous ulcers.
Results:
(1) Even when other body sites are affected, pyoderma gangrenosum usually affects the upper and lower legs and feet or peristomal sites compared with chronic venous ulcers that are limited to the lower legs and feet. (2) Pyoderma gangrenosum can be associated with systemic diseases, especially inflammatory bowel disease. (3) Pustules and purulent discharge are features of pyoderma gangrenosum but not of chronic venous ulcers. (4) Crater-like holes or cribriform scarring is commonly seen in pyoderma gangrenosum but not in chronic venous ulcers. (5) Pathergy is a specific but not sensitive finding of pyoderma gangrenosum. It does not occur in patients with chronic venous ulcers.
Conclusions:
Diagnosis of pyoderma gangrenosum should be considered in patients with purulent ulcers affecting the legs or peristomal sites. To confirm the diagnosis, specific features should be sought, including pathergy, crater-like holes or cribriform scarring, and association with inflammatory bowel disease. Other causes of ulceration should be excluded.
DEFINITIVE DIAGNOSIS OF PYODERMA GANGRENOSUM can be extraordinarily challenging. Diagnostic criteria are not firmly established, and, as a result, the condition is incorrectly diagnosed by some and missed by others. Clinical features are described well in the original publications reporting pyoderma gangrenosum and should be used to diagnose this disease.1,2
We reviewed the charts of 28 patients with typical features of pyoderma gangrenosum in an attempt to identify diagnostic features that are sensitive or specific markers of this disorder, and the features were compared with those in 28 patients with chronic venous ulcers, also known as venous stasis ulcers.
Methods
A retrospective chart review was performed in 28 patients diagnosed with pyoderma gangrenosum and seen at The Mount Sinai Medical Center in New York City since 1992. Ulcers with other possible causes, including infection or venous stasis, were excluded. Clinical features were compared with those in 28 patients with chronic venous ulcers. Diagnostic features that were examined included site of involvement; associated diseases; the presence or absence of pathergy, pustules, purulent discharge, and undermined borders; and development of “crater-like” holes or cribriform scarring.
Results
Ulcer Site
Twenty-two of 28 patients with pyoderma gangrenosum had ulcers involving one or both legs; 7 patients had peristomal ulcers, including 1 patient who had concomitant leg ulcers. Other sites of involvement included the back (7 patients), abdomen (5 patients), buttocks (4 patients), arms (3 patients), face (3 patients), and chest (2 patients). Six of 28 patients had lesions limited to peristomal sites, 12 patients had lesions only on the legs, and 10 patients had lesions on more than one body site (Figure 1). In all 28 patients with chronic venous ulcers, ulcers were localized to the lower legs and feet.
Peristomal pyoderma gangrenosum. Note the ulcer that began with pustules and crater-like holes around the patient's stoma.
Associated Diseases
Eleven patients with pyoderma gangrenosum had Crohn's disease, four had ulcerative colitis, one had chronic myelogenous leukemia (CML), and one had autoimmune hepatitis. Inflammatory bowel disease did not occur in any patients with chronic venous ulceration. Venous varicosities and peripheral vascular disease were not seen in patients with pyoderma gangrenosum.
Pathergy
Three patients with pyoderma gangrenosum exhibited pathergy, that is, the formation of ulcers at sites of minor trauma or in surgical scars. Pathergy was not reported in any patients with chronic venous ulcers.
Pustules
Pustules were seen in 14 of 28 patients with pyoderma gangrenosum but not in any patients with chronic venous ulcers.
Purulent Discharge
A purulent discharge requiring dressing changes more than twice daily was reported in 17 of 28 patients with pyoderma gangrenosum but did not occur in any patients with chronic venous ulcers.
Crater-like Holes
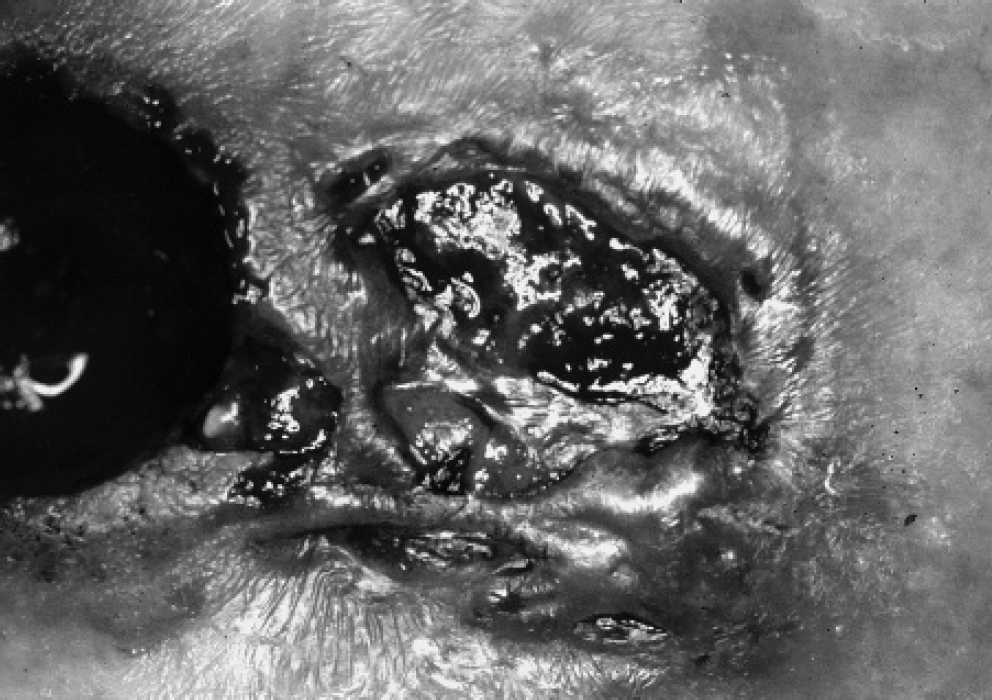
Crater-like holes or cribriform scarring was seen in 15 of 28 patients with pyoderma gangrenosum (Figure 2) but not in any patients with chronic venous ulcers.

Pyoderma gangrenosum. Note multiple crater-like holes.
Undermined Borders
Thirteen of 28 patients with pyoderma gangrenosum were reported to have sharply demarcated, deep ulcers compared with no patients with chronic venous ulcers.
Discussion
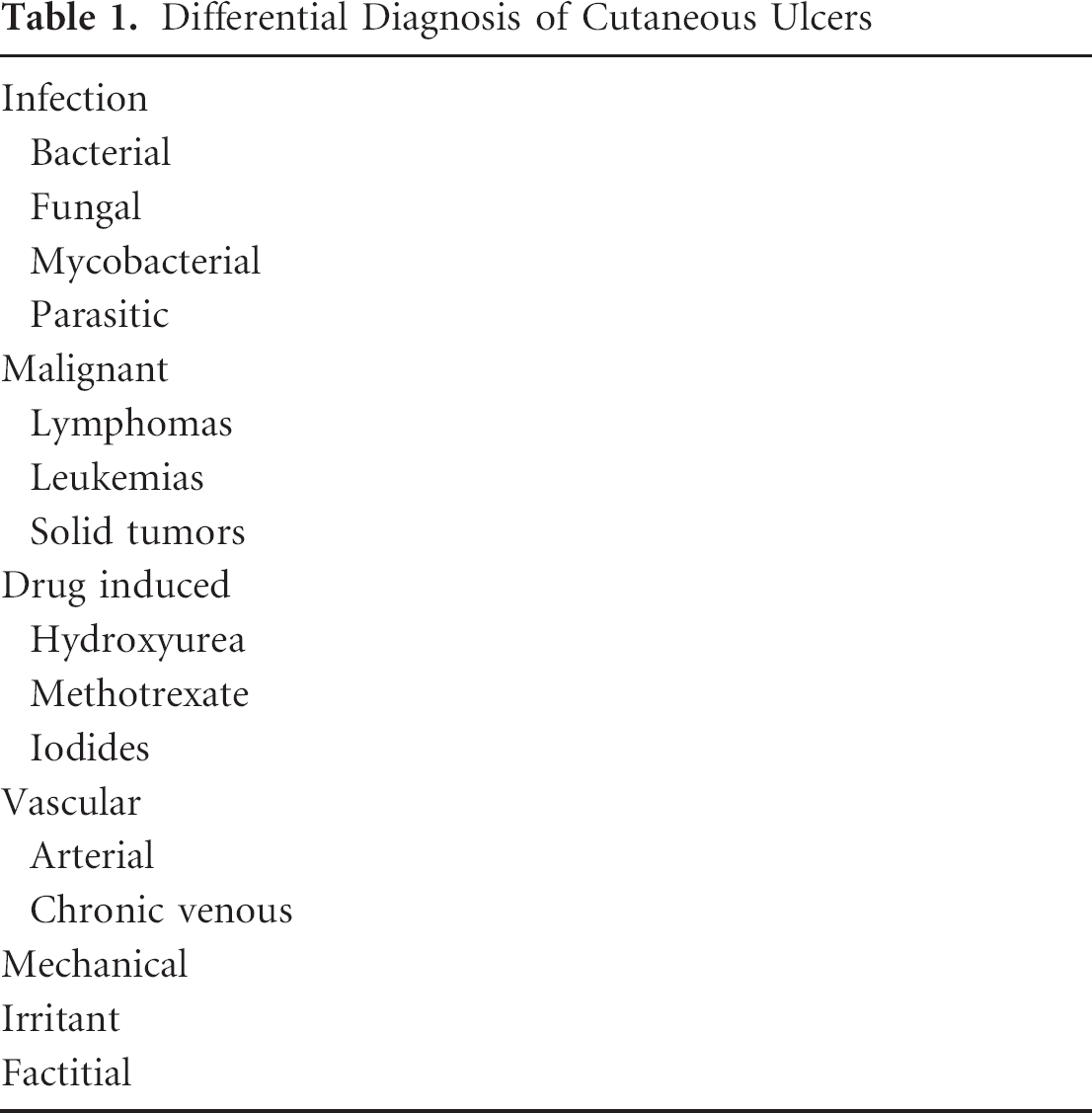
The differential diagnosis of cutaneous ulcers can be quite lengthy, including infectious, malignant, drug-induced, and factitial ulcers (Table 1). It is therefore useful to have clinical features that distinguish pyoderma gangrenosum from other causes of cutaneous ulceration. It is well known that chronic venous ulcers can occur anywhere in the lower extremities below the knee, where perforating veins connect the deep and superficial system. 3
Differential Diagnosis of Cutaneous Ulcers
We have identified several features that are helpful in distinguishing pyoderma gangrenosum from other cutaneous ulcerating disorders and specifically from the most common cause of leg ulcers, venous stasis:
Even when pyoderma gangrenosum involves other body sites, all patients have lesions on the legs or peristomal areas. 4 Chronic venous ulcers always affect the lower legs and occasionally the feet. There were no instances of venous stasis causing ulceration on other body sites.
The association between pyoderma gangrenosum and systemic disease has been known since the original description of this skin disorder. 1 Traditionally, inflammatory bowel diseases have been linked with pyoderma gangrenosum, but more recently, rheumatoid arthritis, myelodysplastic syndrome, acute myelogenous leukemia, CML, Takayasu's arteritis, hepatitis C, and the anticardiolipin antibody syndrome have been associated.
In our series, 11 of 28 patients with pyoderma gangrenosum had Crohn's disease and 4 of 28 had ulcerative colitis; only 1 patient had CML and 1 had autoimmune hepatitis. Our series may be skewed because of the large inflammatory bowel disease population treated at The Mount Sinai Medical Center. Alternatively, our criteria for the diagnosis of pyoderma gangrenosum may select patients with typical lesions that are more commonly seen in patients with inflammatory bowel disease. As reported by Bennett and colleagues, atypical pyoderma gangrenosum is associated with hematologic disease or malignancy compared with the typical lesions in patients with inflammatory bowel disease. 5 Inflammatory bowel disease was not found in any of the 28 patients with chronic venous ulcers.
Pathergy is a specific—but not sensitive—finding in pyoderma gangrenosum, occurring in only 3 of 28 patients in our series. The only other condition in which pathergy regularly occurs is Behçet's disease. We do not include the development of peristomal pyoderma gangrenosum as a manifestation of pathergy, although it is entirely possible that peristomal trauma or irritation contributes to the development of pyoderma gangrenosum at those sites. Of the three patients with typical pathergy, one patient had peristomal ulcers and developed lesions of pyoderma gangrenosum in a midline abdominal incision remote from the site of the stoma.
When patients with pyoderma gangrenosum are examined early in the course of their skin lesions, the primary lesion appears to be a pustule that enlarges and breaks down, forming the ulcers that we identify as pyoderma gangrenosum. In our series, 14 of 28 patients had identifiable pustules.
A purulent discharge is readily apparent in active, untreated pyoderma gangrenosum. Seventeen of 28 patients were found to have a purulent discharge, with many of the patients reporting the need to change dressings several times daily because of the volume of discharge. Many of the other patients with pyoderma gangrenosum were treated at the time they were examined, so the purulent discharge was not seen. Substantial purulent discharge was not found in any of the patients with chronic venous ulcers.
“Crater-like holes” are very characteristic signs of pyoderma gangrenosum. These holes represent the openings to fistulous tracks underneath the skin. On pressure, pus can be pushed out of the fistulous tracks (Figure 3). The tracks can be demonstrated by injecting medication in one side of a lesion of pyoderma gangrenosum, only to see it exit another side through one of the crater-like holes. When the crater-like holes reepithelialize, cribriform scarring results. The presence of crater-like holes or cribriform scarring is one of the most specific clinical features of pyoderma gangrenosum and does not occur in chronic venous ulcers (Figure 4).
Borders that are undermined—sharply demarcated and deep—are characteristic of pyoderma gangrenosum. The latter finding is not specific but does help distinguish pyoderma gangrenosum from chronic venous ulcers. Other ulcers, such as diabetic ulcers and pressure ulcers, may also have undermined borders. Even less specific, and certainly less sensitive, is the presence of a violaceous border.

Early lesion of pyoderma gangrenosum. Crater-like holes represent the openings of pus-filled fistulous tracks. Pus can be expressed by applying pressure to adjacent skin.

Chronic venous ulcer. Crater-like holes and cribriform scaring are not characteristics of chronic venous ulcers.
The role of skin biopsy in the diagnosis of pyoderma gangrenosum has been controversial. Microscopic findings are not specific, ranging from a mild perivascular lymphocytic infiltrate to a full lymphocytic vasculitis or neutrophilic vasculitis. 2 Skin biopsy is most useful in excluding malignant or infectious diseases that can mimic pyoderma gangrenosum.
Undoubtedly, there are other patients with pyoderma gangrenosum who differ from the patients presented here. Nevertheless, the clinical features reported in our patients should be helpful in accurately establishing the diagnosis of pyoderma gangrenosum. For example, the presence of crater-like holes, cribriform scarring, or pathergy should suggest a diagnosis of pyoderma gangrenosum. Likewise, the association with inflammatory bowel disease supports a diagnosis of pyoderma gangrenosum. The absence of pustules, purulent discharge, or ulcerations on the legs or peristomal sites makes a diagnosis of pyoderma gangrenosum less likely.
Conclusion
Criteria for the diagnosis of pyoderma gangrenosum should include the presence of ulcers on the legs or in peristomal sites for more than 4 weeks. Other helpful diagnostic criteria include the association with inflammatory bowel disease and the presence of crater-like holes or cribriform scarring. When it occurs, pathergy is a specific sign of pyoderma gangrenosum. Early in the course of lesions, pustules develop and a purulent discharge is common. Because other diseases can mimic pyoderma gangrenosum, infectious, neoplastic, or other causes of ulcers should be excluded. In patients with peristomal ulcers, mechanical, irritant, infectious, and disease-related factors, such as fistulae, must be excluded.
There are many treatments for pyoderma gangrenosum, and new therapies with tumor necrosis factor α blockers, such as infliximab 6 and thalidomide, 7 have recently been added to our therapeutic armamentarium. To ensure that each of these reports describes the same disease, it is essential that we use consistent criteria to diagnose pyoderma gangrenosum.