
Abstract

Keywords
Case report
A 42-year-old recreational cyclist presented with a 3-month history of right-sided neck pain. The patient experienced pain radiating to the right periscapular region and paresthesias in digits 1–3. The onset of the pain was sudden. She described the pain as intermittent and sharp, ranging from 8–10/10 on numeric pain rating scale. The pain was worse at nighttime, often so severe that it would wake her from sleep. She also noted severe headaches and right upper extremity numbness and weakness. She had visited the emergency room twice, both times being admitted to a neurology service because of the severe nature of the pain and what was described as atypical hemiplegia and migraines. A CT scan of the head and cervical spine and an MRI of the cervical spine were normal. The patient was discharged on pain medication, which included prednisone, depakote, zoloft, motrin, and topamax. There was no history of trauma, falls, or any inciting events. She had no history of bowel or bladder incontinence, recent travel, or fever and chills. Her medical history was significant for migraines, right carpal tunnel syndrome, and depression. She was taking lexapro and clonazepam for depression.
Physical examination revealed mild limited cervical range of motion with end range axial pain with flexion, extension, and lateral rotation. Spurling maneuver was positive on the right side eliciting pain in digits 1 and 2. Active and passive range of motion of the right shoulder was minimally limited compared to the left (asymptomatic) side. Additional findings included medial winging of the right scapula and mild weakness (4+/5) of the right triceps. Muscle strength throughout the rest of the upper extremities was 5/5. The rest of the physical examination revealed normal muscle bulk and tone, normal sensation, symmetric upper extremity reflexes, and negative Hawkins’, Neer's, Roos’, Wright's, and Adson's provocative tests.
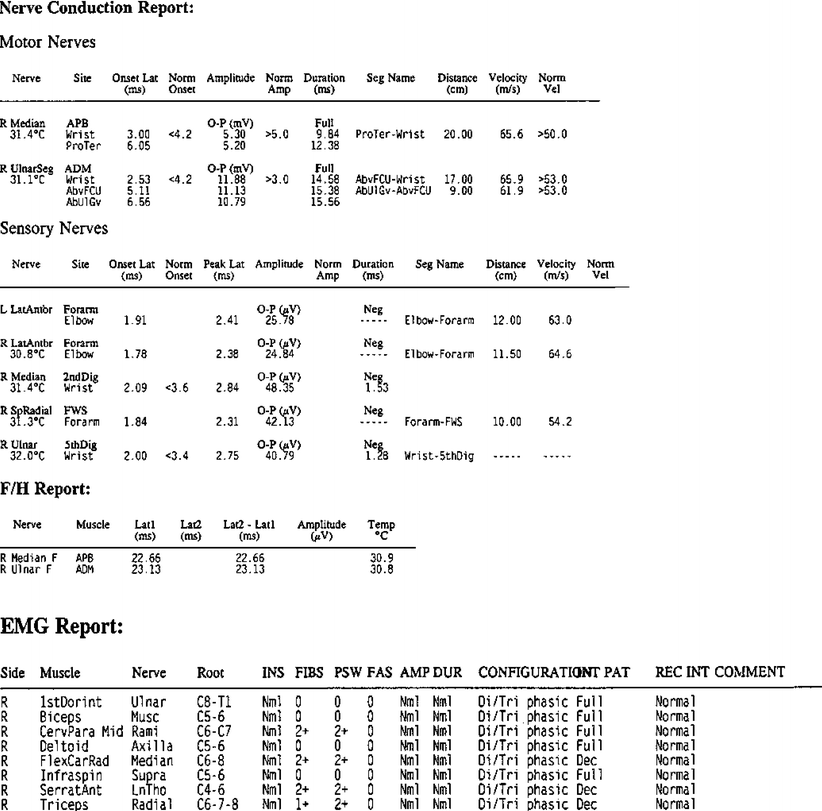
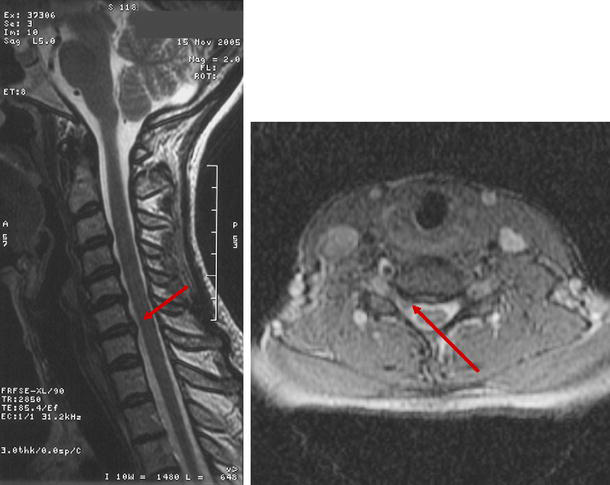
Clinical evaluation at this point was suggestive of Parsonage–Turner syndrome vs a cervical radiculopathy, although a broader differential diagnosis was considered (Fig. 1). Electrodiagnostic studies were performed and showed evidence of severe denervation (2+ positive sharp waves and fibs) corresponding to muscles of the right C7 myotome and including the paraspinal muscles, consistent with a right C7 radiculopathy (Fig. 2). Motor unit recruitment was reduced in the involved muscles and there were no polyphasic potentials. An MRI of the cervical spine was repeated and revealed mid to lower cervical spondylosis, moderate left-sided C5/6 foraminal stenosis, and mild right-sided C6/7 foraminal stenosis (Fig. 3). Because the MRI findings did not demonstrate significant nerve root compression, the patient was diagnosed with Parsonage–Turner syndrome and Lyrica was prescribed. Over the next 6 weeks the patient's symptoms improved but then suddenly worsened.
Differential diagnosis of unilateral upper extremity weakness, pain, and sensory loss Nerve conduction study demonstrating normal amplitudes, distal latencies and nerve conduction velocities. EMG demonstrating positive sharp waves and fibrillations in the right cervical mid paraspinals, right flexor carpi radialis, right serratus anterior, and right triceps, consistent with moderate to severe right C7 radiculopathy Sagittal T2 and axial T2 weighted images demonstrating a small right posterolateral disc protrusion at C6-7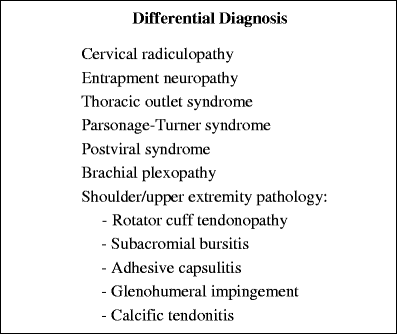
The patient returned for follow-up with complaints of recurrent right neck pain and right upper extremity weakness. Neck range of motion was now normal and Spurling's maneuver was now negative. There was greater upper right extremity weakness, with motor strength of right triceps 4+/5, right wrist extension 4−/5, and right wrist flexion 4/5. Reflexes were normal and sensation was intact. Parsonage–Turner syndrome was still the working diagnosis and the patient was referred to physical therapy to treat a superimposed cervical radicular component.
Over the next 2 months, the patient continued to have symptoms and developed a shingles-like rash on her buttock. She was treated by her primary care physician with Valtrex and within a few days the patient's neck and right arm pain completely resolved. One month later, she had recurrence of the buttock rash along with return of the neck and arm pain. She again received a course of Valtrex and her symptoms completely resolved. To date, 1 year later, she has been pain-free with almost full strength and able to return to all previous activities, including recreational cycling.
Discussion
Evaluation of the patient with neck and unilateral arm pain can present a diagnostic and treatment challenge. Anatomic localization is important but does not always guarantee a proper diagnosis. Radiating neck pain into the upper limb with numbness, tingling, and weakness is a typical presentation for a cervical radiculopathy. Anatomic localization to the root level can be done with electrodiagnostics when there is muscle denervation but cannot determine the anatomic cause [15, 44]. Correlation with imaging studies can help identify the anatomic etiology such as a disc herniations or foraminal stenosis. The degree of nerve root compression on imaging studies and clinical symptoms does not always correlate well, leaving some uncertainty to the cause of nerve root dysfunction.
Brachial plexopathies can cause similar symptoms but are usually associated with trauma. Parsonage–Turner syndrome is one of the more common atraumatic causes of a brachial plexopathy and was described by Parsonage and Turner [29] in 1948 but a patient with a similar clinical presentation was first reported in 1897 [13]. There are similar reports in the literature before Parsonage and Turner's classic paper [1, 7, 11, 39]. Also called brachial plexitis, acute brachial plexus neuropathy, neuralgic amyotrophy, and brachial neuritis, this condition continues to be idiopathic. Patients present with sudden and severe shoulder girdle pain. Pain can also involve the trapezius ridge, arm, forearm, and hand [5]. The symptoms often appear to be radicular-like but many of its hallmark features are atypical for a cervical radiculopathy. Pain is rarely positional, Spurling's maneuver is usually negative, and sensory changes are not in a dermatomal fashion. Pain lasts from hours to weeks and then gradually subsides but it is not always the predominating feature [29, 34, 38]. Rapid and severe atrophy follows weakness approximately 3–4 weeks after the initial onset of symptoms. As the pain subsides, 75% of patients are left with severe weakness in muscles innervated by the upper trunk of the brachial plexus [29, 38]. There is full motor recovery in approximately 36% of patients at 1 year, 75% of patients at 2 years, and in 89% of patients at 3 years [38]. Sensory changes are often not a significant complaint or finding [43] but sensory deficits were observed in 66% of patients in one study [6] and in a minority of patients in another [43].
Parsonage–Turner syndrome primarily affects the upper trunk of the brachial plexus or one of the shoulder girdle's peripheral nerves, although rare involvement of the middle and lower trunks has also been reported [38]. The suprascapular, long thoracic, and axillary nerves are the most commonly involved peripheral nerves [21, 27, 30, 38]. The musculocutaneous, anterior interosseous, ulnar, median, and phrenic nerves were also reported [6, 19, 23, 28]. There are also reports of lumbosacral plexus involvement but most of these patients have complicated medical histories, suggesting there may be other contributing factors [4, 12, 23, 33]. Because the paraspinal muscles are usually spared, root level involvement is felt to be rare [23].
Electrodiagnostic studies have demonstrated it be an axonal process with the presence of positive sharp waves and fibrillation potentials in muscles involved. There is also often a reduction in motor unit recruitment. Nerve conduction velocities are usually normal but sensory amplitudes are reduced in the lateral antebrachial cutaneous sensory nerve in 32% of patients [10]. Although the predominant electrodiagnostic finding is axonal degeneration of affected muscles, the denervation pattern is not myotomal and selective denervation of muscles of different root levels can occur.
Gender differences exist in Parsonage–Turner syndrome. There is a higher incidence in men than women. Magee and DeJong [21] reported a male to female ratio of 11.5 to 1, Tsaires et al. [38] a ratio of 2 to 1, and Parsonage and Turner [29] a ratio of 2 to 1. But Martin and Kraft [24] found a much closer ratio of 11 to 9.
Etiology of the disorder is disputed, with 25% occurring after viral infection and 15% after immunization [14]. Other risk factors include patients who have had injury at a remote area, at postexercise, and at postsurgical [14, 24, 43]. Thirty-three percent of cases have bilateral involvement, but one side may be subclinical and only detected by evidence of axonal degeneration on EMG. The clinical course is usually self-limiting, and strength gradually returns, but this may be incomplete [35]. Treatment is symptomatic with nonsteroidal anti-inflammatory drugs, narcotics, anticonvalescents, and physical therapy [22, 27]. Steroids and antiviral medication were used but there is no consensus whether these medications are indicated [24]. The early use of steroids when they are given has a more favorable prognosis. Other causes of brachial plexopathy should be considered, such as stretch injury, cancer, postradiation, and idiopathy. There is also a hereditary form of brachial neuritis [37].
Postherpetic neuralgia is a viral syndrome that can cause symptoms similar to Parsonage–Turner syndrome or a cervical radiculopathy. Patients will usually develop a painful vesicular rash (shingles) with a dermatomal distribution. They may then experience a deep, burning, or aching electric-like pain that is often associated with paresthesias, dysesthesia, and hypesthesia. The neuropathic pain lasts from 1 to 6 months after resolution of rash and occurs with an incidence of 10 to 15% of those patients with zoster [8, 20]. The persistent pain is felt to be caused by local involvement of peripheral nerves and altered CNS signal processing [8, 17, 20]. Varicella zoster resides in the dorsal root ganglia and although symptoms are predominantly sensory, patients with postherpetic neuralgia can also have motor involvement resulting in motor deficits. Some patients may develop the neurological manifestations of postherpetic neuralgia without a rash, making the diagnosis in these patients more difficult to make. The clinical presentation of these patients may be very similar to patients with Parsonage–Turner syndrome but the anatomic distribution of their symptoms has a more radicular pattern.
Medical management consists of a combination of antivirals, analgesics, lidocaine patches, and neuropathic pain drugs such as Gabapentin, Lyrica, and Amitriptyline [3]. Antiviral therapy reduces risk of postherpetic neuralgia but 20% of patients greater than 50 years of age continue to have pain 6 months postantiviral therapy. Some patients can experience fairly acute symptomatic relief but 40 to 50% of those with herpetic neuralgia do not respond to any treatment [32]. One meta-analysis of four trials of acyclovir demonstrated a 42% reduction in the likelihood of postherpetic neuralgia [5]. Studies have demonstrated effective reduction of acute zoster pain with early treatment (within 72 h after rash appearance), but have not shown a conclusive effect on postherpetic neuralgic pain [40]. Various studies have shown efficacy of tricyclic antidepressants, opioids, pregabalin, and topical lidocaine in lessening the pain of postherpetic neuralgia [3, 8, 9, 31, 42] as has meta-analysis [20].
Entrapment neuropathies can also cause pain with impairment in motor and sensory dysfunction. Peripheral nerves can be injured from excessive traction from faulty mechanics or compressed by fibrous tissue, ganglions, tumors, or bone [25]. These patients rarely have pain in the neck or in a radicular pattern, as with our patient. Pain will usually be localized at the site of entrapment and will be accompanied with the motor and/or sensory symptoms. Pain in the periscapular region might be the result of entrapment of the suprascapular nerve in the suprascapular notch or the axillary nerve in the quadrilateral space. Numbness or paresthesias in digits 1–3 of the hand could be secondary to a radial nerve entrapment in the arm or elbow or a median nerve entrapment at the wrist (carpal tunnel syndrome) [36]. Symptoms from entrapment neuropathies are usually positional or worse with use of the affected limb. Electrodiagnostic studies are usually very diagnostic in these conditions.
Thoracic outlet syndrome (TOS) is another source of unilateral upper extremity pain and sensory changes; the true or “classic” type is caused by compression of the lower trunk of the brachial plexus by a cervical rib or fibrous band from an elongated C7 transverse process [25, 26]. Clinical presentation is not of neck pain, but of mild, deep, aching upper extremity pain, hand weakness and clumsiness, and atrophy of thenar eminence (abductor pollicis brevis) called the “guttering sign” [16]. Thoracic outlet syndrome predominantly affects the lower trunk or medial cord of the brachial plexus. Physical examination is significant for Tinel's sign in the supraclavicular fossa, sensory deficits on the medial forearm and ulnar side of hand (without ring finger splitting), weakness of hand intrinsics, and atrophy of thenar and hypothenar eminences [16, 18]. EMG studies on these patient will usually demonstrate abnormalities in muscles innervated by the lower brachial plexus, such as the abductor pollicis brevis and flexor digitorum indicis. Another form of TOS, also known as “common TOS,” has more widespread nature of symptoms, causing arm and shoulder pain that is worse with prolonged arm elevation. The pain is poorly localized, associated with sensory deficits in the hand and weakness/clumsiness without nerve conduction study or EMG findings [41].
Other shoulder and upper extremity musculoskeletal disorders may also cause unilateral upper extremity pain and decreased range of motion, including rotator cuff calcific tendonitis, subacromial bursitis, and adhesive capsulitis, but none of these have neurological deficits [26].
Summary
This patient's clinical presentation of right-sided neck pain, periscapular pain, numbness, and weakness along with positive EMG findings were suggestive of a cervical radiculopathy [25]. An MRI study revealed some cervical disc disease but only mild foraminal stenosis. Previous reports have demonstrated that patients older than 65 years of age commonly have some abnormality of the cervical disc space, and 28% of asymptomatic adults over the age of 40 years have herniated discs or spurs on MRI so that subtle abnormal findings on MRIs may not be clinically significant [2].
The distribution of EMG findings in this case made a C7 radiculopathy difficult to rule out but the degree of muscle denervation with no significant nerve root compression on MRI was nevertheless surprising. Furthermore, our patient had a classic positive Spurling maneuver [35], which is diagnostic for a cervical radiculopathy and atypical for Parsonage–Turner syndrome. This is not an infrequent diagnostic dilemma in patients with clinical evidence of a cervical radiculopathy, often leading the clinician to consider alternative diagnoses. This is especially true when imaging studies demonstrate an equivocal result, which commonly occurs. The clinical course and the response to the antiviral medication Valtrex for treatment of shingles-type buttocks rash raises the possibility of postherpetic neuralgia or an atypical form of Parsonage–Turner syndrome.
A literature review reveals such a wide variety of clinical presentations and courses with Parsonage–Turner syndrome that multiple etiologies should be considered. The positive response of some patients to steroids, some to antiviral medication, and some only to pain medication suggests that Parsonage–Turner syndrome may be more than one disorder. We have also seen many patients who were diagnosed with cervical radiculopathies but without significant nerve root compression on MRI. We believe that some of these patients may have Parsonage–Turner syndrome, postherpetic neuralgia (without the rash), or some other viral or autoimmune etiology.
The true etiology of our patient's symptoms still remains unclear. We suggest the diagnosis of Parsonage–Turner syndrome or a variant should be considered in patients who present with similar radicular type of symptoms when there is poor anatomic correlation on imaging correlation. A short course of antiviral medication may play a role in their treatment.