
Abstract
Meniscal and parameniscal pathology is usually diagnosed through magnetic resonance imaging. The availability of high-frequency high-resolution linear transducers for sonographic detection of peripheral meniscal and parameniscal pathology has made not only the diagnosis but also the treatment of symptomatic parameniscal cysts a more accessible option. This case report illustrates the use of sonographically guided meniscal cyst aspiration and injection as an alternative to surgical treatment in the proper clinical scenario.
Introduction
Meniscal cysts are a fairly common entity encountered in the setting of meniscal tears. They often present as a palpable mass or focal pain along the joint line or may be found incidentally as an asymptomatic finding associated with a meniscal tear with communication of synovial fluid into the meniscocapsular complex [1, 2].
Typically, meniscal and parameniscal pathology is diagnosed through magnetic resonance imaging (MRI). However, the availability of high-frequency high-resolution linear transducers for sonographic detection of peripheral meniscal and parameniscal pathology has made not only the diagnosis but also the treatment of symptomatic parameniscal cysts a more accessible option. One study using high-resolution ultrasonography has shown a sensitivity of 97%, specificity of 86%, and accuracy of 94% with negative (NPV) and positive predictive values (PPV) 94% and 92%, respectively, in the sonographic detection of meniscal cysts [1]. Another study showed a sensitivity, specificity, PPV, and NPV of 94%, 100%, 100%, and 94%, respectively, in the sonographic detection of parameniscal cysts [3]. We present a case of a meniscal tear and parameniscal cyst diagnosed by magnetic resonance imaging and treated with ultrasound-guided aspiration and injection.
Case report
This is a 55-year-old male who had a MR examination for medial knee pain. MRI demonstrated a complex medial meniscal tear with intrasubstance meniscal cyst formation that was treated arthroscopically with debridement. After a period of almost 1 year, the patient was reimaged with MRI and noted to have a retear of the medial meniscal remnant and had developed a symptomatic meniscal cyst that ascended proximally to the meniscofemoral ligament (see Fig. 1a,b). The patient was sent for ultrasound-guided aspiration and drainage of the cyst. Preliminary scanning over the medial joint line utilizing a high-frequency linear 17–5-MHz transducer demonstrated a focal anechoic cyst extending medially from the periphery of the body segment of the medial meniscus (see Figs. 2 and 3). Under direct sonographic guidance, the cyst was aspirated and injected with a corticosteroid and anesthetic mixture (see Fig. 4). The steroid mixture was observed under real-time ultrasound to directly enter the cyst confirming accurate needle placement with real-time visualization of cyst decompression (see Fig. 5). Upon clinical follow-up, the patient reported mild improvement of symptoms at 6 months postprocedure without the need for further intervention.
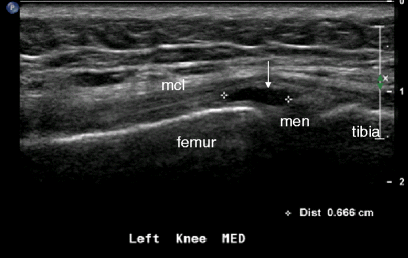
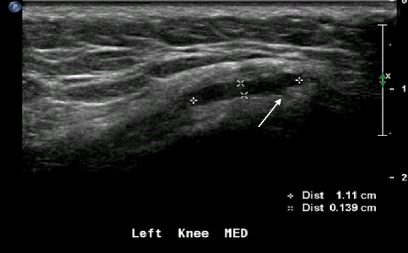
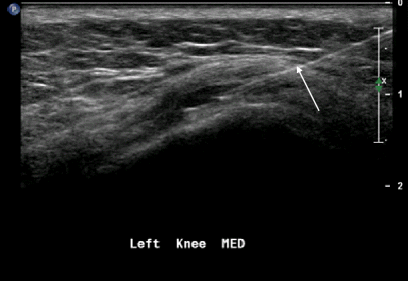
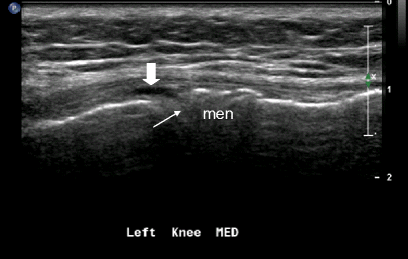
High-resolution ultrasonography in the coronal plane demonstrates an anechoic meniscal cyst (thin white arrow) superficial to the meniscus (men) and deep to the medial collateral ligament (mcl) High-resolution ultrasonography in the coronal plane demonstrates a small hypoechoic cleft (thin white arrow) extending from the cyst to the peripheral meniscal substance reflecting the tear High-resolution ultrasonography in the coronal plane demonstrates the linear echogenic needle (thin white arrow) extending into the cyst for aspiration High-resolution ultrasonography in the coronal plane demonstrates tiny hypoechoic cleft (thin arrow) representing the communication between the horizontal meniscal tear with the decompressed meniscal cyst (block arrow)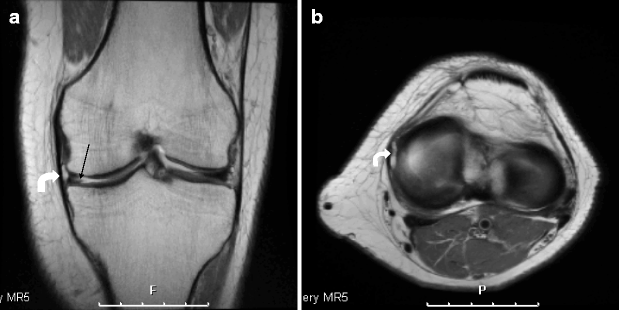
Discussion
Suspected meniscal tears are a common indication for MR examination of the knee. However, not infrequently, patients present specifically with a palpable mass or joint line pain attributable to a meniscal cyst. According to the Mayo Clinic, in a review of all meniscectomies performed over a period of 28 years, meniscal cysts occurred in 1% of meniscal tears [1]. Mass consistency can vary from fluctuant to solid [1]. Meniscal cysts are thought to be more common laterally although this may vary as noted in the literature [3, 4]. The more common consensus among authors is that meniscal cysts are far more frequently encountered laterally at an incidence of 75% to 90% [1]. This may be in part related to the relative weakness of the lateral meniscocapsular attachments when compared to the more tightly adherent medial meniscocapsular junction [3]. According to one study, lateral meniscal cysts tend to occur just anterior to the lateral collateral ligament, through a region of inherent weakness, and are more likely to reach a larger size [3]. In contrast, medial meniscal cysts are thought to be confined with limited expansion by firmer meniscocapsular tissue, only reaching larger sizes after violating the capsule and potentially extending for some distance from the meniscus [1].
Sonographic evaluation of the meniscus has been established for some time and has improved with the advent of high-frequency linear transducers. The availability of both color and power Doppler has played an important role in differentiating soft tissue masses that typically exhibit vascularity as manifested by intrasubstance power or color flow as opposed to the avascular parameniscal cyst.
The ability to perform a dynamic examination with sonography is also of use in the evaluation of parameniscal cysts with a characteristic feature described as the “disappearing sign” [1]. With active knee flexion, observing decreasing size of the periarticular mass is reported to be suggestive of a meniscal cyst [1]. The disappearance of the cyst is most likely related to decompression of the cyst back into the joint as a result of increasing periarticular pressure in the surrounding soft tissues. In some cases, meniscal cysts can be directly compressed by the transducer resulting in decompression of synovial fluid through the meniscal tear back into the joint differentiating meniscal cysts from soft tissue ganglion cysts [1].
The traditional treatment for parameniscal cysts is usually performed through open surgical removal or arthroscopic meniscal repair and cyst drainage. The role of percutaneous drainage is especially pertinent in patients with clear contraindications to operative management or in those patients who prefer more conservative treatment. Ultrasound-guided aspiration and injection is a useful alternative for nonsurgical treatment of symptomatic parameniscal cysts. As a conservative alternative to surgical treatment or as a temporizing measure for patients who present with discomfort related to parameniscal cyst formation, the utility of percutaneous drainage is well documented with little to no associated morbidity [4]. In addition, the use of power Doppler aids in the direct visualization and subsequent avoidance of vascular structures that may present as obstacles to aspiration.
As this case demonstrates, symptomatic parameniscal cysts can be accurately diagnosed and safely treated with sonographically guided percutaneous aspiration and injection. While most commonly considered a temporizing measure in the absence of primary repair or debridement of the underlying meniscal tear, many patients are afforded long-term relief including those for whom high surgical risks make them poor candidates for operative treatment.