
Abstract
There are several references in the hip and knee literature that mention converting fusions to a prosthetic total arthroplasty, but similar reports of total shoulder arthroplasty after glenohumeral fusion are lacking. The indication for conversion of a glenohumeral arthrodesis to a total shoulder arthroplasty is persistent periscapular pain refractory to conservative treatment. The purpose of the following article is to describe the preoperative plan and surgical technique in the conversion of a glenohumeral fusion to a total shoulder arthroplasty in single case of protracted scapulothoracic pain.
Introduction
Humeroscapular arthrodesis, also known as shoulder arthrodesis, is performed for a number of different indications. These can include severe instability, posttraumatic brachial plexus injuries, paralysis of the rotator cuff and deltoid, infection, failed arthroplasty, and iatrogenic bone deficiency [1]. Shoulder arthrodesis can consist of an extra-articular (acromiohumeral) fusion, an intra-articular (glenohumeral) fusion, or a combination of the two. Ideally, a well-positioned shoulder arthrodesis allows the patient to reach his back pocket, groin, mouth, and have slight external and internal rotations [1, 8]. The most common goal of fusion is pain reduction, although very few patients report being completely pain free [1, 8]. Clare et al. [1] reports pain relief and satisfaction in 35–83% of patients in the literature. Dissatisfaction rates were reported at 18–52%, with the most common complaint being continued moderate to severe pain. Safran and Iannotti [8] report that, of the 26% of patients who still complained of moderate to severe pain, most (59%) had pain over the surgical area. Twenty-nine percent had pain in the periscapular region, and 12% had diffuse pain [8]. From this literature, it is evident that pain, including scapulothoracic pain, is a relatively common complication of shoulder arthrodesis [1, 8].
There are several references in the hip and knee literature that mention converting fusions to a prosthetic total arthroplasty, but similar reports of total shoulder arthroplasty after glenohumeral fusion are lacking. In a case series of three patients that underwent conversion to total shoulder arthroplasty (TSA), two cases were non-unions after attempted arthrodesis, and only one case was a successful glenohumeral arthrodesis [9]. The indication for surgery was persistent pain, and two patients were described to have periscapular pain. All patients reported diminished but persistent pain to varying degree, and the authors suggested that conversion of a glenohumeral arthrodesis to TSA may be a viable option in cases of periscapular pain with a relatively preserved cuff and deltoid [9]. The purpose of this report is to describe the preoperative plan and surgical technique in the conversion of a glenohumeral fusion to a TSA in a single case of protracted scapulothoracic pain.
Case report
The patient was a 32-year-old man who initially sustained a work-related injury to his left shoulder in September of 2004. The patient developed recurrent posterior instability with multidirectional laxity, and he failed two arthroscopic stabilizations and one open stabilization. After multiple stabilizations, he continued to have significant instability, along with glenohumeral pain and crepitation. The patient was offered another open stabilization, but he refused secondary to the three previous failed attempts at stabilization. Glenohumeral arthrodesis provided as an alternative treatment option to address shoulder instability, and the patient was counseled on possible complications and long-term sequelae [1, 8]. He was made aware of the significant decrease in range of motion associated with the arthrodesis and the reliance on scapulothoracic motion to perform his activities of daily living. He also understood he would not be able to return to his baseline level of work. In September 2006, he underwent a glenohumeral arthrodesis using three 7.3-mm cannulated screws for intra-articular fixation and a pelvic recon plate for extra-articular fixation. The procedure was performed without complications. He was fused in 20° of abduction, 20° of flexion, and 40° of internal rotation (Fig. 1a, b).
Plain radiographs were obtained after combined intra-articular and extra-articular glenohumeral arthrodesis. 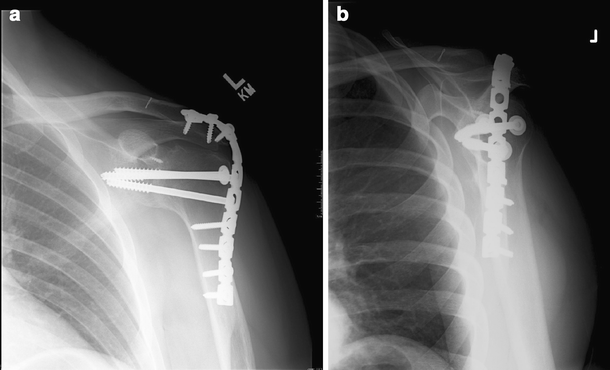
Although the shoulder was stable, the patient continued to complain of vague and persistent pain. One year after arthrodesis, he underwent a removal of the pelvic recon plate without significant pain relief. He appeared to have a solid fusion on serial radiographs, and during the removal of the extra-articular recon plate, his cuff musculature appeared to be intact. His complaints of pain had spread into his neck, his shoulder blade, and his surrounding periscapular musculature. The patient continued to have persistent scapulothoracic pain refractory to conservative treatment and pain management. His range of motion at the shoulder was minimal, if any, and most activities even at waist level caused him significant pain. After extensive discussion, the patient was given the option of conversion of the glenohumeral arthrodesis to TSA.
Surgical technique
Prior to the operation, we used standard radiographs and TSA templates in order to anticipate the osteotomy of the glenohumeral fusion mass as well as the component size. Using the humeral head templates, the precise proximal humerus osteotomy could be planned as well as the osteotomy at the level of the glenoid so that only the fusion mass and humeral head was removed (Fig. 2).
This demonstrates our preoperative plan with total shoulder arthroplasty templates. 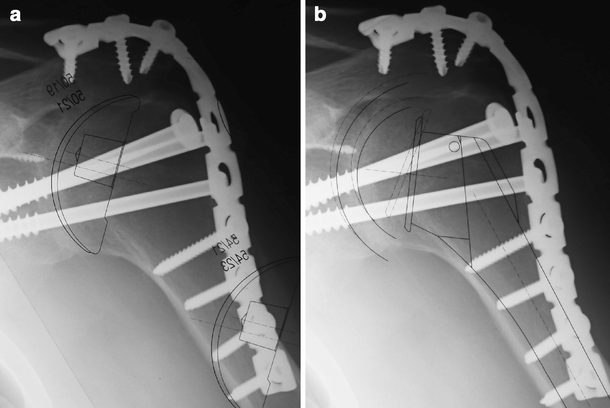
The patient had an interscalene block initiated in the preoperative holding area. He was brought to the operating room, placed under general anesthesia, and positioned in the beach chair position. The patient had a previous standard deltopectoral incision from his arthrodesis, and the same incision was used for this procedure. The area was anesthetized with local anesthetic and incised along the old scar. The deltopectoral interval was identified with the cephalic vein. The cephalic vein was ligated due to difficulty mobilizing it secondary to the surrounding scar tissue. The clavipectoral fascia was incised. The overlying deltoid and the underlying rotator cuff were then adequately exposed so that a retractor could be placed around the lateral and posterior aspects of the humerus. The subscapularis was identified and was then elevated directly off the anterior fusion mass, again confirming a complete glenohumeral joint fusion, as was seen on preoperative radiographs. The subscapularis was thin and atrophic and was tagged with number 2 Ethibond sutures.
Before performing the osteotomy, several factors were taken into consideration, including the retroversion of the humerus, the insertion of the rotator cuff tendons on the greater tuberosity, and the angle of the anatomic neck. All of these factors taken together as well as the preoperative template would guide the initial osteotomy into the fusion mass. A 1-in. osteotome was directed at approximately 30° retroversion with respect to the humerus (an oscillating saw can alternately be used as well). This was done by identifying the supraspinatus tendon as it attached to the greater tuberosity, identifying the posterior aspect where the bare area was initiated (approximately 5 mm medial to insertion). This point was used to mark the cephalad extent of the neck osteotomy. The initial humeral osteotomy was performed at a 135° inclination to simulate the average 45° anatomic neck of the humerus. A second cut was made perpendicular to the plane of the scapula with the triangular removal of a section of the fusion mass. The humerus was dislocated, and the remaining bone and bone fragments were removed from around the humerus. The humeral canal was prepared using standard reamers and broaches. A head cut protector was placed.
Attention was directed toward the glenoid side. There was bone remaining from the fusion mass on the glenoid, and the combination of an osteotome and rongeur was used to resect this back to the native glenoid. Despite the fact that this was a revision setting, it was possible to visualize the borders of the native glenoid once the triangular piece of fusion bone had been removed. The fusion bone did have a different appearance than the native bone of the glenoid, At this point, the standard total shoulder arthroplasty was performed according to the manufacturer's specifications.
Postoperatively, the patient was placed in a shoulder sling and abduction pillow per our normal protocol. Due to his history to instability, his physical therapy was delayed to allow the soft tissues to completely heal. He was allowed to come out of the sling after 4 weeks for pendulum exercises. Formal physical therapy was started at 10 weeks with limits of forward elevation to 90° and external rotation limit to 20°.
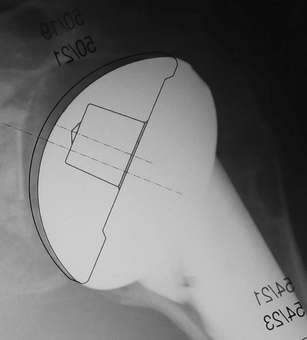
Three months after the surgical procedure, the patient reported a drastic decrease in periscapular pain, but he still requires narcotic oral analgesics under the supervision of pain management. Nine months after the procedure, he still complains of pain. He is not able to return back to his job of being an assembly mechanic but has been able to perform some more activities at waist level than before the arthroplasty. Figure 3 shows the prosthesis in good position, with good alignment of the humeral head in the glenoid. Figure 4 shows the template overlaid on the postoperative films, which is consistent with the preoperative plan as seen in Fig. 2.
Immediate postoperative radiographs after conversion of total shoulder arthroplasty show the prosthesis in place with good alignment. Placing the humeral head template over the postoperative radiographs demonstrates the reproducibility of preoperative template plan in conjunction with intraoperative landmarks to restore normal glenohumeral anatomical relationships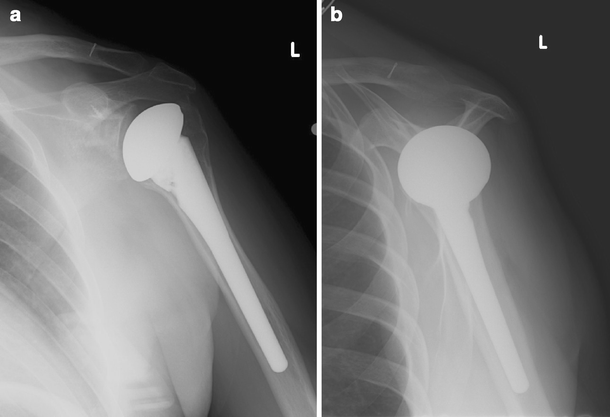
Discussion
From the literature, it is evident that pain, including scapulothoracic pain, is a relatively common complication of a shoulder arthrodesis [1, 8]. In patients without fusions, complaints of scapulothoracic pain and shoulder girdle weakness are most commonly attributed to osseous lesions such as an osteochondroma, bone abnormalities, or bursitis due to overuse or trauma [3]. While physical therapy protocols aimed at strengthening and improving posture as well as corticosteroid injections, nonsteroidal anti-inflammatory medications, and rest might improve bursitis, these techniques do little to improve the pain and weakness caused by skeletal distortion similar to a shoulder fusion [3, 4, 6, 7]. In the surgical treatment of scapulothoracic pain in the non-fused shoulder, open and arthroscopic techniques have been used to release and decompress the scapulothoracic articulation in response to bursitis, and open techniques have been reported for resecting boney abnormalities of the superomedial angle of the scapula [3–6]. Overall, there is an 81% satisfaction rate in pain relief and return to normal functioning for these surgeries [4, 5].
However, the literature does not report any of these techniques being used to alleviate scapulothoracic pain in patients with a fused shoulder. Although scapulothoracic fusions are used to relieve pain in this area, there is also no literature supporting this technique in the case of pain related to a fusion [2]. Sperling and Cofield [9] report a conversion of a shoulder arthrodesis to a total shoulder arthroplasty in three patients as an attempt to relieve severe pain in the scapulothoracic region. In these cases of a conversion of shoulder arthrodesis to a TSA, the patients involved had arthrodesis performed to address brachial plexus and massive rotator cuff injuries. There was no specific information to address functional outcome, but the improvements seen in this group of patients was reported as minimal. Of the three patients, only one had a fully fused shoulder, and he reported a decrease in pain from severe to mild and was satisfied with the procedure.
Due to the lack of evidence that other techniques would relieve scapulothoracic pain in a patient with a glenohumeral fusion, our current patient underwent a conversion of a glenohumeral fusion to a TSA in the hopes of relieving his severe and constant periscapular pain. In the present case, the patient failed multiple surgeries for instability, leading to the decision for a glenohumeral fusion to provide shoulder stability. In spite of the fusion, the patient did have an intact, albeit significantly atrophied, rotator cuff and deltoid muscle. If the patient did not have an intact cuff, we could postulate that the outcome could be similar to a total shoulder arthroplasty in the setting of cuff tear arthropathy, which has been shown to provide pain relief but not necessarily an increase in function. We were optimistic that our conversion to a total shoulder arthroplasty created the potential for improved pain as well as functional outcome.
Although there are numerous reports in the hip and knee arthroplasty literature on the conversion of arthrodesis to arthroplasty, there is only one other case reported in the shoulder literature. The present paper describes the preoperative and intraoperative methods of planning the humeral and glenoid osteotomy sites through the fusion mass with preservation of the normal anatomical relationships. In this case, our patient did have a slight increase in function at 9 months. Evaluation of the rotator cuff and deltoid prior to this procedure can help guide which patients would be good candidates for the procedure. Taking careful patient selection into consideration, conversion of glenohumeral arthrodesis to TSA is a reasonable alternative in patients with protracted scapulothoracic pain unresponsive to conservative treatment and pain management.