
Abstract
Brachymetatarsia is a congenital or developmental condition that results in a short metatarsal. Problems that arise from this condition can include pain, difficulty with shoe wear, and cosmetic concerns. Multiple techniques have been described that successfully correct the deformity, including both acute and gradual distraction. We describe a modification of the technique of gradual lengthening by way of distraction osteogenesis in which an axial transarticular K-wire is incorporated into a monolateral frame, thereby increasing the stability of the construct and potentially minimizing complications.
Introduction
Brachymetatarsia is a rare condition of the foot characterized by shortening of the metatarsal bones. The reported incidence is 0.02% to 0.05% and female patients exceed males by a ratio of approximately 25:1 [1, 2]. It is thought to be the consequence of retarded growth or premature closure of the epiphyseal plate. The digit dorsal to the shortened metatarsal may be consequently displaced over the adjacent metatarsal [3–10]. Brachymetatarsia may be congenital and idiopathic in etiology and may be associated with systemic diseases such as pseudohyperparathyroidism, Turner's syndrome, Down's syndrome, Apert syndrome, enchondromatosis, multiple epiphyseal dysplasia, sickle cell anemia, and poliomyelitis [3–7, 11, 13].
Brachymetatarsia may affect one or more metatarsals and may be unilateral or bilateral [1–10]. The incidence of bilateralism has been reported to be more than 50%. [11, 14
Patients seeking treatment commonly have cosmetic concerns. However, many may also complain of pain in the forefoot or toes, callosities, or problems with shoe wear due to toe alignment [10, 12]. Multiple surgical techniques have been reported for the management of brachymetatarsia. These include acute lengthening with internal fixation and gradual lengthening by the manner of distraction osteogenesis. All of the previously described techniques have recommended pinning of the metarsophalangeal joint in order to prevent subluxation during the lengthening process, although no specific technique for doing this has been described. In this report, we describe an adaptation of the distraction osteogenesis method in which an axial wire is incorporated into the device to prevent metatarsophalangeal (MTP) joint subluxation. The advantage of this method is the increased stability of the construct which may theoretically reduce the risk of pin infections and the discomfort during the lengthening process.
Case report
The patient was a 16-year-old female that was diagnosed with a congenitally short fourth metatarsal (Figs. 1a, b and 2). At the time of diagnosis, the patient was otherwise healthy. She was a dancer who often performed barefoot and requested correction of the deformity for cosmetic purposes. There was a callous on the dorsum of the fourth toe as well as an extension deformity at the MTP joint. The patient was indicated for distraction osteogenesis to correct the brachymetatarsia and create a symmetric cascade to the toes, thereby improving the appearance of the foot.
AP radiograph of the left foot demonstrating brachymetatarsia of the 4th metatarsal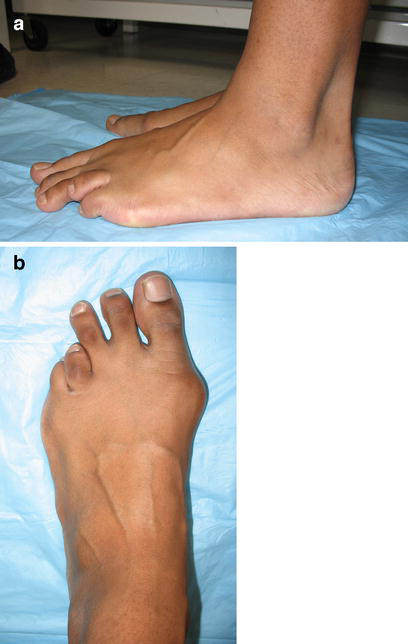

The planned surgical procedure included a fourth metatarsal osteotomy with the application of a uniplanar external fixator to perform distraction osteogenesis of approximately 2 cm. A longitudinal incision was made along the axis of the fourth metatarsal, and two tapered half pins were inserted at the distal and proximal ends in the center of the metatarsal. A frame was attached, and another half pin was inserted into the proximal and distal ends of the bone. The frame was then removed, and using multiple drill holes and an osteotome, the osteotomy was performed closer to the proximal pin cluster. The frame was then reattached, and an axial transarticular K-wire was inserted through the distal end of the toe across the MTP joint. The K-wire was bent and fastened to the EBI mini-rail External Fixator (Biomet/EBI Inc, Parsippany, NJ) by means of the screw clamp attachment creating a unified distal segment (Figs. 3a, b and 4). The distal segment, comprised of the distal metacarpal metaphysis and toe, was then moved as a unit during the lengthening. Distraction was started 1 week post-operatively at a rate of 0.25 mm three times per day for 14 days, then switched to 0.25 mm two times per day for the final 3 weeks of lengthening. An electrical bone stimulator (Biomet/EBI Parsippany, NJ) was applied 3 weeks post-operatively to enhance bone healing. The patient reported taking no pain medications or antibiotics during the 6-week lengthening period. A total lengthening of 2 cm was performed.
An immediate post-operative photograph with external fixator and K-wire attachment in place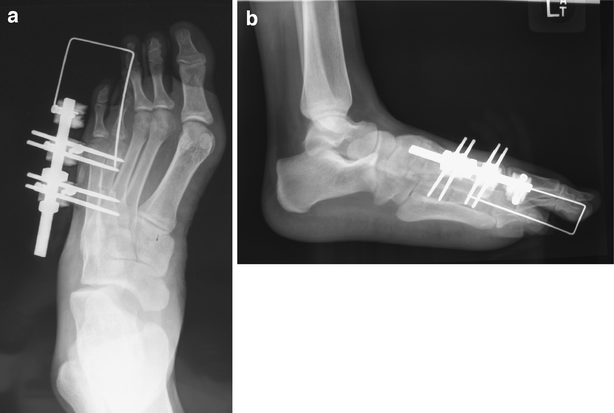

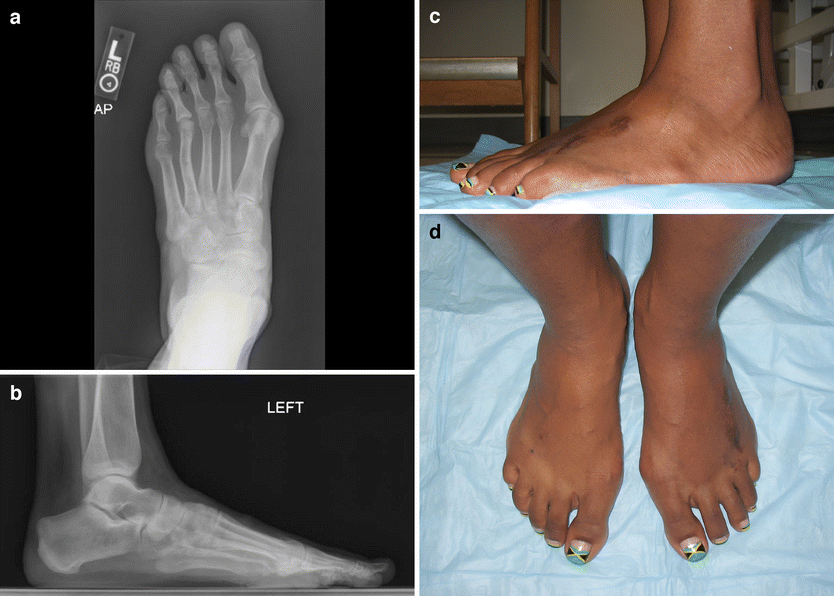
Following the period of gradual distraction, the transarticular K-wire was removed, and the external fixator was left in place during a consolidation period of 3 months (Fig. 5). During the consolidation period, an extension contracture of 20 degrees developed necessitating an MTP joint capsulotomy and extensor tendon lengthening which was performed at the time the fixator was removed. At the end of treatment, the normal cascade of the metatarsal heads had been restored as well as the proper sagittal alignment of the 4th toe (Fig. 6).
An AP radiograph of the foot during the consolidation phase of lengthening
Discussion
The pathology of brachymetatarsia may result in abnormal pressure distribution of the forefoot causing excessive load and pain at adjacent metatarsals. In addition, the digit of the shortened metatarsal may be dorsally displaced, resulting in callous and shoe wear problems [15]. Lastly, some patients may be concerned exclusively with the appearance of the foot. While many patients will desire treatment of brachymetarsia for cosmetic concerns, surgical reconstruction must also result in proper forefoot alignment and function. Since first described by McGlamry and Cooper in 1969, several studies have reported the effectiveness of one-stage lengthening with bone graft for surgical management of brachymetatarsia [1, 17–20, 23, 24]. The advantages of this method include a short treatment period and ease of post-operative care. However, one-stage lengthening without distraction osteogenesis typically does not allow as much lengthening. In addition, there may be an increased risk for ischemia of toe and delayed or non-union of the graft [9, 11, 13, 16, 25, 26].
Distraction osteogenesis is a commonly used and powerful technique for correcting limb deformities, and there are several reports in the literature of the successful application of this technique to treatment of brachymetatarsia [6, 21, 25, 27]. The technique that we describe is a modification of the ones previously described that promotes a more mechanically stable construct. In theory, motion of pins and bone segments during lengthening can create more discomfort for the patient and increase the risk for pin infections because of increased motion at the soft tissue–pin interface. By connecting the distal segment, including the toe and the transarticular pin, to the fixator, we hope to minimize these complications. The major advantages of gradual distraction over acute lengthening are the limited risk for neurovascular complications, the ability to lengthening with the need for bone graft, the ability to allow early weight bearing, and lastly, the ability to achieve greater magnitudes of lengthening [7, 11]. The principal disadvantages of callus distraction include longer time to bony union, pin–track infection, premature fusion, metatarsal angulation, subluxation or axial deviation of the MTP joint, and joint stiffness [6, 22, 28, 29].
Several authors recommended K-wire fixation of the MTP joint during distraction to prevent deformity of the joint [6, 10, 22]. We agree with this recommendation and have modified it by incorporating the axial transarticular K-wire into the frame so that it prevents subluxation of the MTP joint, remains stable, and advances during distraction.
Conclusion
This modification of the technique of metatarsal lengthening, using an axial K-wire incorporated into the frame, allows safe correction of brachymetatarsia while helping to minimize complications of joint subluxation and pin infection.