
Abstract
Total knee arthroplasty (TKA) has become the predominant treatment modality for severe degenerative joint disease. With recent advancements in surgical and anesthetic technique, patients with severe comorbidities are able to have this procedure; they would have been precluded from TKA only a matter of years ago. Although many studies have investigated risk factors and the causes of perioperative morbidity and mortality in the arthroplasty patient, few have linked risk factors with specific outcomes. We present a case report that illustrates the link between the use of angiotensin-converting enzyme inhibitors and the development of postoperative acute kidney injury. While this relationship has been extensively studied in cardiac and gastric bypass patient populations, it has never been examined in the setting of joint replacement.
Keywords
Introduction
Total knee arthroplasty (TKA), in the setting of advanced arthritis, has led to greater than 95% of patients experiencing significant pain relief, even up to 10 years postoperatively [18]. Recent improvements in surgical and anesthetic technique have led to decreased morbidity and mortality in this patient population [12, 14].
Many studies have examined the morbidity and mortality associated with joint arthroplasty and the factors placing patients at greatest risk [3, 7, 10, 13, 14, 16]. Although the presence of acute kidney injury (AKI) has been noted in many articles, exploration into its specific causes has not been investigated. Perioperative AKI is associated with an increased morbidity and mortality in hospitalized patients, with some studies showing greater than 50% postoperative mortality in severe cases [21, 23]. Epidemiologic data clearly depict the inverse relationship between perioperative survival rates and renal injury with a 0.3–0.4 mg/dl rise in serum creatinine increasing hospital-based mortality by 70% [4, 20]. Limited treatment options make it even more essential to identify the high-risk patients within the joint arthroplasty population. One risk factor for the development of AKI, which has been researched in cardiac and gastric surgery, is the preoperative use of angiotensin-converting enzyme inhibitors (ACE-I). Despite its documented adverse impact on postoperative outcomes in these procedures, it has not been studied in the setting of joint replacement [1, 2, 5, 6, 8, 20].
We present a case of AKI following an elective bilateral TKA in which the patient's use of an ACE-I cannot be overlooked. The common pre-, post-, and intrinsic renal causes of AKI in this patient are analyzed, and findings are described.
Case Report
A 65-year-old Caucasian female, with a history of osteoarthritis, presented to her orthopedic surgeon with a complaint of chronic bilateral knee pain. She denied any recent trauma or procedures to the affected joints. Physical exam and X-ray confirmed advanced bilateral degenerative joint disease. After consultation with her orthopedic surgeon, the patient selected bilateral total knee arthroplasty.
The patient had a history of hypertension for 10 years, which was treated with an ACE-I (lisinopril) in addition to a beta-blocker. Other comorbidities included obesity (BMI > 30), hypercholesterolemia, and coronary artery disease. For these conditions, the patient took a statin as well as aspirin. No other medications were taken during the perioperative period. Her only surgical history was an appendectomy when she was 10 years old. The patient's social and family histories were non-contributory.
Selected data from the patient's BMPs
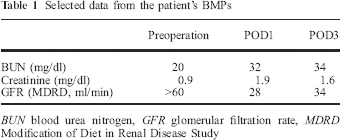
BUN blood urea nitrogen, GFR glomerular filtration rate, MDRD Modification of Diet in Renal Disease Study
Under spinal anesthesia, the patient received bilateral knee prostheses without any reported surgical or anesthetic complications. Prior to incision, 2 g of cefazolin was administered IV. The tourniquets were applied sequentially, not simultaneously, during the operation. The patient received 1,200 mL of lactated Ringer's solution intraoperatively. The patient's estimated blood loss, as determined by the attending surgeon and anesthesiologist, was 100 mL, and urine output was 255 mL over the 2-h and 5-min case. Mean arterial pressure (MAP) remained >60 mmHg throughout the procedure, indicative of adequate intravascular volume [22]. The patient's initial postoperative course was uncomplicated. Urine output was greater than 0.5 mL/kg/h up until 0600 hours on postoperative day 1 (POD1); the time at which the Foley catheter was removed, intravenous fluids stopped and urine output no longer measured. MAP was >60 mmHg throughout the patient's entire hospital stay. The patient also had adequate urine output during her entire postoperative course, as described in the nursing progress reports. The patient had no drains placed.
RIFLE classification for acute renal injury
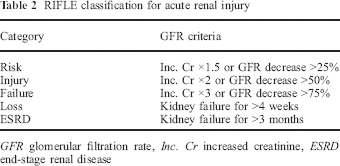
GFR glomerular filtration rate, Inc. Cr increased creatinine, ESRD end-stage renal disease
No complications were noted at the surgical site, and postoperative imaging showed satisfactory appearance of bilateral prosthesis insertion within the knees.
Discussion
Increasing life expectancies and better survival outcomes have resulted in more patients requesting TKA. Many of these patients have comorbidities that would have precluded them from such a procedure only a matter of years ago. It is thus crucial to identify and understand all of the factors that place patients at risk for major postoperative complications. The knowledge gained will lead to more appropriate preoperative evaluation and postoperative diagnostic work-up and management.
AKI is a serious and prevalent complication of lower extremity joint arthroplasty, comprising 14% of the major complications in patients undergoing primary unilateral elective lower extremity total joint arthroplasty [13]. The etiology of our patient's AKI includes the various causes of pre-renal, renal, and post-renal causes (Fig. 1). Post-renal AKI can be caused by urinary tract obstruction. However, our patient, even after Foley catheter removal, had adequate urine production, making this an unlikely cause of AKI. The patient did receive prophylactic cefazolin, a recognized nephrotoxic antibiotic [11]. Despite this, intrinsic renal causes of AKI are unlikely. The POD2 urinalysis did not show the presence of casts or epithelial cells and had a specific gravity of 1.011. Such findings argue against an intrinsic renal pathology. Pre-renal etiologies are the most common postoperative causes of AKI, occurring secondary to decreased renal perfusion due to reduced cardiac output, hypovolemia, or fluid sequestration [19]. The patient's intraoperative blood loss of approximately 100 mL was lower than expected for a bilateral TKA [15]. Further, the patient received more fluid (1,200 mL) than was lost during the procedure (355 mL). The patient had a history of CAD, and she received preoperative clearance from her cardiologist. Postoperative physical examinations did not show any signs of heart failure, EKG changes, or edema, suggesting that decreased cardiac output contributed to the AKI.
Main causes of AKI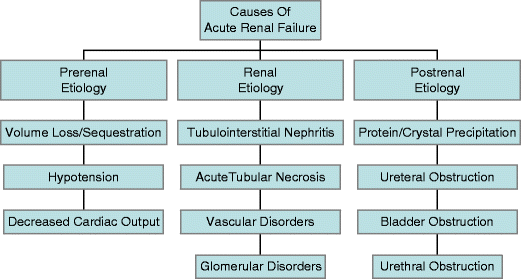
Ritter et al. [9, 17] and Lynch et al. [9, 17] theorized the diminished intravascular volume, secondary to an inability of certain patients to manage the fluid shifts that occur during bilateral total knee arthroplasty, as a cause of hemoconcentration and subsequent elevation in serum creatinine. While it is possible that our patient did experience fluid shifts, it is an unlikely cause of her AKI. Our patient experienced a dramatic rise in her serum creatinine without any alteration in vital signs indicating a hypovolemic state. The MAP was never less than 60 mmHg, there was always adequate urine output, and although on a beta-blocker, there was no documented tachycardia or position dependent change in heart rate; volume depletion is suspected when such findings are present. It is therefore reasonable to assume that other factors were involved in her development of AKI.
Preoperative use of ACE-I has been thought to contribute to the development of postoperative AKI [1, 2, 5, 6, 8, 20]. The connection between the two has been observed in both cardiac and gastric bypass patient populations but has never been reported in patients undergoing joint arthroplasty. Our patient was chronically treated with lisinopril, an ACE inhibitor, pre- and postoperatively for hypertension. The mechanism by which preoperative ACE-I use compromises renal function is not completely understood, but is thought to be associated with impaired autoregulation of renal blood flow, which may diminish the threshold at which renal injury can occur, allowing for the development of a pre-renal AKI at MAPs that are normally associated with adequate perfusion. In the presence of additional risk factors for AKI, the patient using an ACE-I is at an increased risk for kidney injury [20].
In this case report, we attempt to depict the possible correlation between the use of ACE-I and the development of AKI in a joint arthroplasty patient. Although our patient experienced spontaneous resolution of her AKI, patients often require significant medical intervention, including fluid resuscitation and dialysis. Not only does perioperative AKI adversely impact patient mortality, its treatment carries a large cost. We believe that future larger studies in patient populations with traits similar to the patient described in this case will report results similar to those seen in the cardiac and gastric bypass ACE-I studies. It is imperative that more research be conducted to further investigate this connection and determine if cessation of ACE-I prior to joint arthroplasty would be of benefit in reducing postoperative complications. This case will hopefully serve as a sentinel work, alerting the orthopedic community of this possibility.