
Abstract
Statement of Need
There is a lack of literature discussing the management of multisystem involvement in patients with inflammatory arthritis, such as ankylosing spondylitis. As a result, patients with ankylosing spondylitis may be overlooked in attention to their joint disease; therefore cardiac or pulmonary disease may not be assessed appropriately in these patients. The overall collaborative management of this complex disease, with teamwork involving orthopedists and rheumatologists, should facilitate rehabilitation and mobility which will improve patient outcomes.
Target Audience
This activity is targeted at primary care physicians, specialty physicians, orthopedic surgeons, general medicine, residents, and fellows.
Objectives
Hospital for Special Surgery professional education activities are intended to improve knowledge, competence and performance of our learners and to lead to better patient care. At the conclusion of the activity, the participant should be able to:
Describe the need for interdisciplinary collaboration and discussion in the treatment of complex multisystem disease such as ankylosing spondylitis (AS). Work collaboratively with interdisciplinary team members when treating patients with complex multisystem disease such as AS. Define the elements of a multisystem evaluation prior to surgical treatment in patients with AS. Implement a multisystem evaluation approach in AS patients prior to decision regarding surgery. Define appropriate alternate treatments for heterotropic ossification, including Indocin therapy or radiation post-arthroplasty, in patients with AS. Utilize alternate types of treatments for heterotropic ossification, such as Indocin therapy or radiation therapy, in patients with AS. Identify and be able to incorporate preferential operating sequencing (such as hip arthroplasty prior to knee arthroplasty) in treatment for patients with AS.
Accreditation
The Hospital for Special Surgery is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Hospital for Special Surgery designates this Journal-based CME activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Faculty Disclosure
In accordance with the Accreditation Council for Continuing Medical Education's Standards for Commercial Support, all CME providers are required to disclose to the activity audience the relevant financial relationships of the planners, teachers, and authors involved in the development of CME content. An individual has a relevant financial relationship if he or she has a financial relationship in any amount occurring in the last 12 months with a commercial interest whose products or services are discussed in the CME activity content over which the individual has control. It is the policy of Hospital for Special Surgery to disclose all financial relationships that planners, teachers, and authors have with commercial interests. Relationship information appears below.
Baxter Supported/Contracted Research Funding
Ethilon Supported/Contracted Research Funding
Exactech Salary, Royalty or Honoraria
Clinical Orthopedics and Related Research Senior Associate Editor
Other than those noted above, the Hospital for Special Surgery Office of CME staff and CME Committee members have no relevant financial relationships to disclose regarding this activity.
Instructions for Post-Test and CME Credit
In order to earn CME credit for this journal activity, you must read the article and successfully pass the post test. A passing grade of 70% is required to earn credit. For questions related to the post-test, contact Allison Goldberg, MPA, Director of Professional Education at 212-606-1834.
Option 1: Take the post-test on-line.
Go to the HSS Journal homepage at www.springer.com/hss
Click on CME articles Click on “Multidisciplinary Conferences At HSS Surgical Arthritis Service Weekly Rounds: \” to view the full-text pdf article After you have reviewed the article click on “Complete the Current CME Test Online” to register and complete the test.
Option 2: Take the post-test via hard copy printed in the Journal.
You may complete the hard copy of the post test. Please mail the test to:
Office of Continuing Medical Education
Education Division
535 East 70th Street
New York, NY 10021
Journal CME Post-Test
CME Questions for Ankylosing Spondylitis/SAS Weekly Rounds
A 42 year old man with a 20 year history of neck and lower back pain that had been attributed to a motor vehicle accident presents to your office for a second opinion. He had been treated with muscle relaxants and oxycodone. Upon further evaluation, you suspect a diagnosis of ankylosing spondylitis (AS). Radiographic changes characteristic of ankylosing spondylitis in his axial skeleton might include:
Vertical syndesmophytes in the spine Bilateral symmetric sacroiliitis with erosions Squaring of the vertebral bodies Symmetric concentric hip joint space narrowing All of the above Diagnosis of ankylosing spondylitis requires x-ray evidence of sacroiliitis:
True False Osteoporosis in patients with ankylosing spondylitis is:
Present in fewer than ten percent of patients Present one third of patients Associated with low vitamin D levels Both a and c Both b and c A 37 year old man with a longstanding history of ankylosing spondylitis is admitted to the cardiac care unit after suffering from a myocardial infarction. Cardiac risk in ankylosing spondylitis may be related to:
Hypertension Hyperlipidemia Persistent inflammation All of the above Heterotopic bone formation (HO) after total hip arthroplasty (THA) is associated with:
Pre-operative ankylosis Advanced age Female gender Primary THA A 46 year old man with long standing AS is admitted for a revision total hip replacement (THR). Treatment options to prevent HO include:
Prednisone Indomethacin Low dose radiation therapy b and c A 50 year old man with AS presents with advanced arthritis of both hips and both knees with limited motion and pain requiring arthroplasty to treat pain and restore function. He should undergo THA first because:
THA will facilitate restoration of motion Correction of the hip contracture first prior to TKA improves the ability to perform ROM of the knees Referred pain from the hip to the knees will be eliminated All of the above (d) A 27 year-old man presents with 8 years of lower back pain and morning stiffness. Two months ago he noted pain and swelling in the left knee. Which of the following therapies may be useful in treating his back pain?
Sulfasalazine Anti-TNF-alpha inhibitors Methotrexate NSAIDS b and d a and c An individual diagnosed with ankylosing spondylitis at age 20 is less likely to require total hip arthroplasty than an individual diagnosed at age 35.
True False Which of the following may be useful in the preoperative assessment of patients with ankylosing spondylitis prior to arthroplasty?
Transthoracic echocardiogram Electrocardiogram Nuclear stress test a and c only All of the above
Case Report
A 51-year-old man presented to Rheumatology Clinic for evaluation of long-standing inflammatory arthritis. The patient complained of severe joint pain involving the left elbow, right wrist, ankles, hips, and most severely affecting both knees. His joint pain was present for over 10 years but was getting worse. He complained of 90 min of morning stiffness. He reported severe neck stiffness but denied pain. He was able to walk up to five blocks slowly before having to stop to adjust his posture. He had no systemic complaints such as fever, but reported a 25-lb weight loss over the past 30 years. He denied eye inflammation, oral or nasal ulcerations, chest pain, or exertional dyspnea, although his ability to exercise was reduced. He had no abdominal complaints, or history of psoriasis.
The patient first noted neck stiffness in the mid-1990s and subsequently developed knee pain. He underwent arthroscopic surgery of both knees at another hospital in 1999 for “damaged cartilage”. He was evaluated by a rheumatologist for joint inflammation following a motor vehicle accident in 2000 and at which time a diagnosis of psoriatic arthritis was made. He underwent repeat arthroscopic surgery of both knees in 2001 and 2002. Over the following 3 years, the patient noted the onset of swelling, pain, and warmth of the left elbow, right wrist, and ankles as well as pain and stiffness in the left hip. Over the course of his illness, he was seen by multiple rheumatologists and was treated with a variety of medications including sulfasalazine, methotrexate, and prednisone. These were discontinued due to intolerance or lack of efficacy. In 2007, he developed a rash over the lower extremities. A biopsy confirmed pyoderma gangrenosum and the patient was treated successfully with 3 months of cyclosporine and 2 weeks of intralesional steroid injections and 3 months of cyclosporine, which were then discontinued. At the time of presentation to the Hospital for Special Surgery, the patient was only taking Naprosyn 500 mg twice daily and omeprazole 40 mg daily.
The patient's medical history was additionally significant for GERD as well as “inflammation” seen on a routine colonoscopy in 2007. An HIV test was negative in 2006 and a PPD was negative in 2009. Medications included Naprosyn 500 mg twice daily and esomeprazole 40 mg daily. He was intolerant to medications and reported itching due to lidocaine and anaphylaxis due to shellfish. The patient lived with his mother and was unemployed. He smoked one pack of cigarettes daily for the last 35 years [5, 18]. Family history revealed his sister had “arthritis in the eye.”
On physical examination, the patient appeared cachectic but was not in distress. His temperature was 35.0 C, blood pressure 109/64 mmHg, pulse 66 bpm, and the patient was breathing comfortably on room air. The sclerae were not injected, mucous membranes were moist without ulcerations. Auscultation of the heart was unremarkable. His chest was clear with limited chest wall expansion. The abdomen was soft and nontender and the liver and spleen were not palpable. Examination of the lower extremities revealed multiple hyperpigmented scars of 1 to 2 cm in diameter with one 10-cm lesion on the right inner leg.
When standing, his overall sagittal balance was positive (anterior) with a notable kyphosis centered in his upper thoracic spine. He had a compensatory cervical lordosis, which allowed him to keep his brow level, but could not extend beyond level. He could flex his cervical spine to the chin-on-chest position. Cervical rotation was limited to approximately 30° in both right and left gaze. There was no pain to palpation about the spine. He had limited flexion of the lumbar spine. The patient walked with a crouched gait keeping both hips and knees flexed throughout his gait to maintain balance.
Examination of his upper extremities revealed symmetric, painless, shoulder motion with forward flexion and abduction to 130°, internal rotation to the lower lumbar spine, and external rotation (with arm adducted) to 10°. His right elbow had painless range of motion from full extension to 130° of flexion. The left elbow had palpable boggy synovitis and significant pain with motion, which was limited to −30° of extension and 100° of flexion. His right wrist had pain at terminal motion, which was limited to 60° of flexion, 45° of extension, 5° of radial deviation, and 10° of ulnar deviation. His right hand was unremarkable, as was his left wrist and hand.
Examination of his lower extremities revealed substantial muscle atrophy, most significantly involving the quadriceps, hamstrings, and gastrocnemius/soleus complex. His right hip had decreased motion with a 10° flexion contracture, flexion to 100°, external rotation to 30°, and internal rotation to 10°. His left hip was more limited with a 20° flexion contracture, 80° of flexion, external rotation to 40°, and internal rotation to -10°. Both hips were painful throughout range of motion, but most pronounced on flexion and internal rotation. His right knee alignment was neutral and the ligaments were intact. The right knee had a palpable effusion and synovitis. His motion was painful and limited to −40° of extension and 90° of flexion. The alignment of his left knee was in approximately 5° of varus. The ligaments were intact, but the deformity was correctable. The left knee also had an effusion and synovitis. This knee had limited, painful motion to −35° of extension and 90° of flexion. His bilateral ankles and feet were unremarkable and in neutral alignment.
Neurovascular examination of both upper and lower extremities was intact bilaterally.
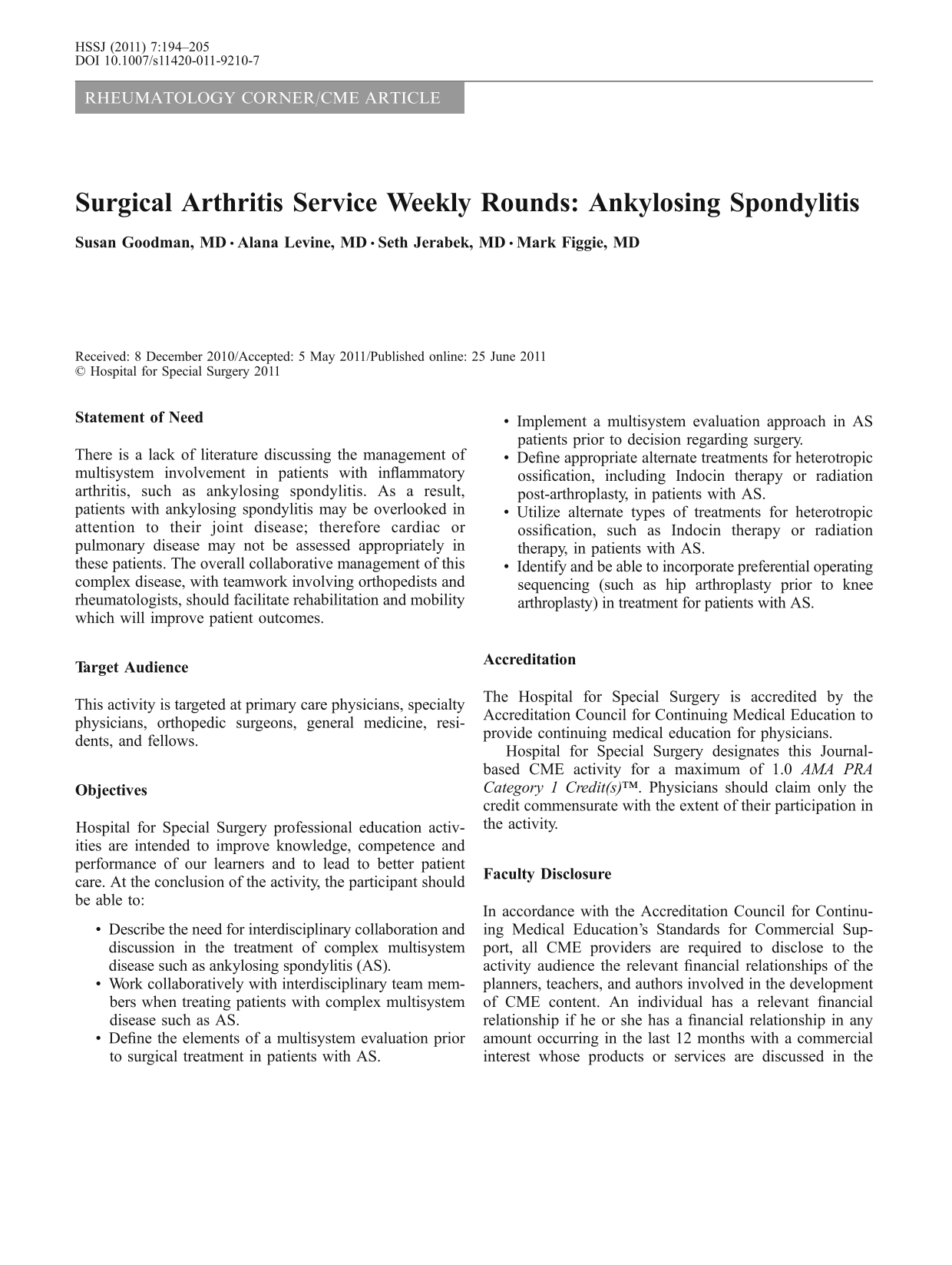
Laboratory evaluation of the patients
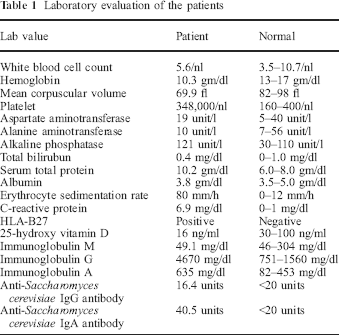
Radiographs of the spine and pelvis revealed fusion of the sacroiliac joints bilaterally as well as moderate axial joint space narrowing of the right hip and severe axial joint space narrowing of the left hip (Fig. 1) Radiographs of the knees demonstrate tricompartmental narrowing of both knees and small effusions with small osteophytes (Fig. 2). There were segmental, non-contiguous syndesmophytes at multiple levels throughout the thoracic and lumbar spine (Fig. 3). A radiograph of the right hand was negative for joint space narrowing or erosions. His chest film was unremarkable for lung pathology.
CME Registration Form
CME Registration Form
The ACCME requires that each accredited CME provider evaluate and assess the effectiveness of all CME accredited activities and to show evidence of this process at the time of an accreditation survey.This activity evaluation will assist us to document our efforts to address physician gaps in knowledge and scope of practice, in a way that will improve physician competence, performance and care outcomes.Should you have any questions, please contact the Activity Director, or staff of the Office of Continuing Medical Education. Thank you.
TEST EXPIRES JUNE 30, 2012
Please complete the following contact information:
Last Name
First Name
Title (ie MD, PhD, NP)
Email Address
Specialty (ie Orthopaedics, Rheumatology, Pediatrics)
Please indicate your profession:
◯ Attending Physician
◯ Athletic Trainer
◯ Resident/Fellow
◯ Research/Scientist
◯ PA, NP or Nurse
◯ Other
◯ Therapist
EVALUATION (must be completed for you to receive credit)
How likely are you to implement the following strategies in your practice:
(Scale: 1= Not At All Certain; 7= Very Certain)
Describe the need for interdisciplinary collaboration and discussion in the treatment of complex multisystem disease such as Ankylosing Spondylitis (AS) patients.
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Work collaboratively with interdisciplinary team members when treating patients with complex multisystem disease such as Ankylosing Spondylitis (AS) patients.
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Define the elements of a multisystem evaluation prior to surgical treatment in patients with Ankylosing Spondylitis (AS).
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Implement a multisystem evaluation approach in Ankylosing Spondylitis (AS) patients prior to decision regarding surgery.
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Define appropriate alternate treatments for heterotropic ossification, including Indocin therapy or radiation post-arthroplasty, in patients with Ankylosing Spondylitis (AS).
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Utilize alternate types of treatments for heterotropic ossification, such as Indocin therapy or radiation therapy, in patients with Ankylosing Spondylitis (AS).
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Identify and be able to incorporate preferential operating sequencing (such as hip arthroplasty prior to knee arthroplasty) in treatment for patients with Ankylosing Spondylitis (AS).
1 2 3 4 5 6 7
□ □ □ □ □ □ □
Overall, the content covered in this journal article to date has been useful and relevant to my scope of practice.
◯ Strongly ◯ Disagree ◯ Disagree ◯ Agree ◯ Strongly Agree
Do you feel a commercial product, device, or service was inappropriately promoted in the educational content?
◯ Yes ◯ No
If no, please comment
Was the learning format(s) for this activity appropriate for the content being presented?
◯ Yes ◯ No
What new information do you feel that this CME activity should have provided in order to improve your:
Competence
Performance
This AP view of the pelvis reveals apparent fusion of the sacroiliac joints bilaterally (arrows) and predominant axial joint space narrowing of both hips (upwards arrow) Radiographs of both knees reveal symmetric tricompartmental joint space narrowing with juxta-articular osteopenia and minimal proliferative change Bridging syndesmophytes are noted focally at L2–3 on the right and T9–10 on the left in a segmental, non-contiguous fashion (see arrows)


The patient's case was discussed at the interdisciplinary Comprehensive Arthritis Program conference. Left hip replacement surgery followed by bilateral knee replacement surgery was recommended but the patient declined hip surgery. A decision was made to go forward with an ultrasound-guided left hip steroid injection 2 weeks prior to bilateral knee replacement surgery. As part of a pre-operative assessment, a transthoracic echocardiogram was performed given the patient's long smoking history and limited exercise capacity. The echocardiogram revealed wall motion abnormalities suggestive of coronary artery disease, so the patient was referred to Cardiology for further evaluation. He underwent a nuclear stress test that showed fixed defects, indicating prior ischemia, but no reversibility. No medical contraindications to surgery were identified.
Surgical evaluation acknowledged a patient presenting challenging orthopedic problem. The kyphotic deformity of the thoracic spine was assumed to contribute to the loss of motion of the hips and knees. Kyphosis can lead to compensatory contractures in the hips and knees. The spine service was consulted and surgical deformity correction was discussed with the patient. However, after considering the risks of spine surgery and the fact that his spine did not cause him discomfort, the patient elected to forego spinal deformity correction and preferred to focus on his painful extremities. In pre-operative planning for this case, all of the contractures had to be evaluated simultaneously as correcting one contracted joint would be ineffective due to the predictable reversion to the pre-operative contracture status in both operated and non-operated joints. Correction of the knees alone would cause imbalance of the trunk with the likelihood that the knee contractures would return. When patients have loss of motion at the hip as well as arthritis of the knees, we usually recommend that the hip be replaced first. Addressing the hip first allows for restoration of motion and correction of the hip flexion contracture, thus making it easier to rehabilitate the knee when total knee arthroplasty is performed. Replacing the hip first also eliminates any referred pain from the hip to the knee. However, in this situation, the patient continued to refuse hip surgery, in spite of careful counseling and education. He claimed to have understood the risk that hip contractures might not improve but his priority was pain relief at the knees. Our compromise given his refusal to entertain hip surgery was to inject his hip pre-operatively in order to give him pain relief at the hip and improve his rehabilitation post-operatively. In addition, we planned to use shoe lifts on his left side to compensate for the hip flexion contracture.
Three weeks prior to surgery, the patient received bilateral hip injections with 40 mg of triamcinolone (Kenalog). This completely relieved the pain in his hips. He then underwent bilateral knee replacements under the same anesthetic, consisting of bilateral femoral nerve blocks and combined spinal/epidural anesthesia. The left knee was completed first. A standard medial parapatellar arthrotomy was performed. The superficial MCL was carefully dissected off the proximal tibia subperiosteally around to the posteromedial corner. The extramedullary tibial guide was placed resecting approximately 2 mm off the medial plateau and 10 mm off the lateral plateau. The intramedullary femoral guide set in 5° of valgus relative to the anatomic axis. A standard 10 mm cut from the distal medial condyle was performed; however, the knee would not come out into full extension. The semimembranosous was released as well at the posterior joint capsule, from both the femur and tibia. Ultimately, an additional 17 mm of distal femoral bone and 2 mm of tibial bone needed to be resected in order to get full extension with a 10-mm spacer block; however, the flexion gap was balanced with a 14-mm block. The femoral component could not be upsized secondary to the width of the distal femur. The distal femoral resection had been taken to the epicondyles at the level of the medial (MCL)- and lateral collateral ligaments (LCL) origins. The MCL and LCL were still intact; however, given the slight mismatch between the flexion and extension gaps and proximity of the distal femoral cut to the ligamentous origins, the femoral component was changed from a standard Biomet Vanguard PS design to a Biomet condylar constrained design using an 80-mm stem. It was cemented into place using the cobalt Biomet cement without antibiotics. The standard Biomet tibial baseplate was cemented without a stem. The polyethylene insert was 10 mm thick and constrained. The patella was resurfaced in standard fashion using a three-hole on-lay button. The left knee was well balanced in extension and slightly looser in flexion, but acceptable. Intraoperatively, the left knee came out to full extension and flexed to 100°. The right knee surgery was then performed in a similar fashion using the same soft tissue releases, similar bone cuts, and the identical components (Fig. 4 and 5).
Portable x-ray of the right knee taken in the recovery room Portable x-ray of the left knee taken in the recovery room

He stayed in the hospital 5 days post-operatively. Overall, he did well medically. Given his CAD, he had a cardiac rule out in the PACU post-operatively, which was negative. Warfarin and sequential compressive devices were used for DVT prophylaxis. He received a total of three doses of cefazolin for antibiotic prophylaxis. He was placed on indomethacin 75 mg daily for 14 days for heterotopic ossification prophylaxis. His pre-operative hemoglobin was 13.1. On POD 1, his hemoglobin was 7.9, thus he was transfused two units of pack red blood cells, increasing his hemoglobin to 10. His hemoglobin remained stable (>8.5) throughout the remainder of his hospital stay. On POD 5 he was discharged to a rehabilitation facility.
His rehabilitation while in the hospital consisted of formal physical therapy sessions twice daily as well as CPM use between therapy sessions. He wore knee immobilizers in to maintain extension at night. His motion upon discharge was equal bilaterally, extension to −10° and flexion to 90°. At his 6 week follow-up, he was very pleased with his pain control. His right knee extended to −10° and flexed to 90°, while his left knee extended to −15° and flexed to 95°. He continues to walk with a crouched gait secondary to his sagittal balance and hip flexion contractures.
Discussion
This patient illustrates the clinical overlap frequently seen in spondyloarthropathy patients, presenting here for a surgical evaluation at an advanced stage after decades of minimally treated disease. Inflammatory arthritis that predominantly affects the axial skeleton, spine, and the sacroiliac joints, is typical of ankylosing spondylitis (AS), psoriatic arthritis, and reactive arthritis as well as the arthritis associated with inflammatory bowel disease. The spine involvement in AS, which is present in 0.1–1.2% of the population, is characterized by the formation of vertical syndesmophytes, which results in boney fusion of the spine and profound loss of motion. Peripheral arthritis typically affects the axial skeleton. The hip is most commonly affected, in 40–50% of AS patients, followed by knee and shoulder involvement [1, 2, 5, 18]. Our patient illustrates this pattern. Extra-articular features include anterior uveitis, present in up to 30% of patients, as well as less frequent manifestations such as pulmonary disease and aortitis. Traditionally, the diagnosis of AS was based on the combination of inflammatory back pain, impaired spinal mobility, and radiographic evidence of sacroiliitis, but newer radiographic diagnostic criteria incorporate MRI findings of sacroiliitis such as bone marrow edema and erosions which appear prior to changes on plain radiographs. Additionally, consideration of clinical features such as uveitis, dactylitis, elevations in the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP), as well as recognition of HLA-B27, the genetic marker present in 90% of AS patients, have been emphasized in the desire to shorten the time required to make this diagnosis [15–17] .This patient demonstrates the overlap of spondyloarthropathy features; he has both spinal and peripheral arthritis, pyoderma gangrenosum, “inflammation” on colonoscopy, and positive anti-S. cerevisiae antibody which are associated with inflammatory bowel disease, as well as a family history suggestive of uveitis. Some have suggested that reactive arthritis and AS are identical diseases at different points in time, with HLA B 27 positivity predicting chronicity and evolution from typical reactive arthritis to AS [7]. Additionally, these patients present with a high likelihood of osteoporosis. The incidence is reported to be as high as 34% in AS patients, especially those who have active inflammatory disease reflected in elevations of ESR and CRP, as well as low vitamin D levels. This should be addressed pre-operatively to optimize bone health and possibly improve surgical outcome [2, 4].
A recent European Consensus report [22] provides guidelines for the medical management of AS including medications as well as physical therapy modalities. Exercise improves function in AS patients, and can be performed as structured physical therapy or as home exercise. NSAIDS are critical in the therapy of AS, as they improve pain and function both of the spine as well as peripheral arthritis. Continuous use of NSAIDS may also slow X-ray progression. Traditional DMARDS such as sulfasalazine and methotrexate have no role in the treatment of axial disease, but may be useful in managing symptoms of peripheral arthritis. Biologic DMARDS such as anti-TNF (tumor necrosis factor) agents are beneficial in treating pain and improving function in AS patients with peripheral and spinal disease. Syndesmophyte formation at inflamed vertebral edges, mediated by osteoblast differentiation, may not be prevented by TNF inhibition. New bone formation may be driven by small molecules other than TNF which contribute to molecular signaling, such as wingless type, prostaglandins, and bone morphogenic protein, which may explain this apparent decoupling of symptomatic benefits from radiographic response [18].
Orthopedic surgery is considered in AS patients to improve function and relieve pain, as well as to correct spinal deformities, when medical management has failed to prevented joint damage. Marked spinal kyphosis can result in impairment of forward gaze, as well as an inability to lie flat in bed. Compensatory hip and knee flexion can ensue, resulting in a painful, awkward flexed knee and flexed hip gait such as seen in our patient. The flexion contractures of the hip and knee also magnify pain and further impair function [9]. Hip arthroplasty is the most common orthopedic procedure performed in AS, as 40–50% of AS patients have hip involvement, which is usually bilateral. Patients with severe spine disease and a diagnosis of AS made at an earlier age are more likely to undergo total hip arthroplasty (THA) than patients diagnosed at an older age [20]. AS patients derive significant benefit from THA. Multiple series demonstrate significant improvement in pain, function, and range of motion in the operated hip. Implant survival, a concern given the average age at the time of THA of 40, is also good. One series reports a 73% 20-year implant survival, and 70% 30-year implant survival. However, global function in patients who have undergone THA is worse than those AS patients who did not undergo THA. Only 42% of AS patients undergoing THA who were under the age of 60 were employed, compared to 64% of AS patients who did not undergo THA. This is reflected in scores of disease activity; THA patients had BASDAI scores (1–10 scale, zero is normal) of 4.6 compared to 4.3 in the control AS patients. Function, measured by BASFI, was 6.9 in the THA patients compared to 4.7 in the control AS patients [3, 21].
Heterotopic bone (HO) formation, which can limit motion, may be increased in AS patients after THA. AS patients at high risk for HO are young, have pre-operative ankylosis, or are undergoing revision surgeries. Prophylaxis to prevent HO with indomethacin or low-dose irradiation should be considered in these patients [6].
Knee arthroplasty has been successful in AS patients, but there are fewer reports in the literature to asses benefit. One series of 30 total knee arthroplasties in 20 patients demonstrated a significant improvement in pain, with an improvement in Knee Society score from 14 pre-operatively to 87 post-operatively. A modest improvement in function was seen, with an average pre-operative Knee Society score of 16 which increased to 80 after surgery. Range of motion increased from 84′ prior to surgery to 94′ at 2 years, but had returned to the pre-operative range of motion at the time of the last follow-up. Patients with heterotopic ossification had worse motion than patients who did not have HO [13]. Patients such as ours raise serious challenges in regard to planning surgical intervention to optimize functional outcome. Performing knee replacement surgery in this patient prior to hip replacement is concerning in this regard.
Perioperative medical considerations in the AS patient undertaking arthroplasty include assessment of cardiopulmonary risk. Arthroplasty is considered an intermediate risk procedure according to the American College of Cardiology/American Heart Association, signifying a 1–5% risk of cardiac events such as myocardial infarction [10] Patients who can perform vigorous exercise do not need formal cardiac testing. However, patients such as this with severe spine disease and poor global function, which is characteristic of AS patients undergoing arthroplasty, are unlikely to exercise. Our patient had no cardiac symptoms, but was predictably very limited in his ability to exercise. Echocardiography revealed regional wall motion abnormalities suggestive of ischemic cardiac disease, and perfusion abnormalities were seen on stress testing. There were no reversible defects, however, to suggest ongoing ischemia. Cardiac imaging and stress testing can be useful in cardiac risk stratification prior to arthroplasty in patients who have severe functional limitations. The increase in cardiac risk in AS patients may reflect an increase in traditional risk factors such as hypertension and dyslipidemia, as AS is not as strong an independent risk factor for cardiac disease as RA. Cardiac valve abnormalities such as mitral and aortic regurgitation are well defined extra-articular features of AS, and will also be identified in pre-operative echocardiography. The addition of beta blocking agents to control heart rate and blood pressure may be desirable and cardioprotective, when blood pressure permits, and will be prescribed in this patient [11, 12].
Pulmonary disease occurs in AS patients and can contribute to perioperative risk. The risk of perioperative pulmonary complications is most highly linked to the surgical site—specifically, proximity to the diaphragm—as well as anesthetic technique [14, 19]. In hip or knee arthroplasty performed under regional anesthesia, the risk of pulmonary complications is generally low, but specific exceptions exist. Pulmonary involvement in AS includes apical fibrobullous disease, in which cavities may coalesce and become superinfected with pathogens such as Aspergillus fumigatus. Early mobilization, nebulizer therapy, and chest percussion may help prevent post-operative pulmonary infections. More commonly, chest wall restriction occurs because of ankylosis, of thoracic costovertebral joints. When chest wall excursion is less than 2.5 cm, the patient is an obligate diaphragmatic breather [8]. This is significant when post-operative ileus or narcotic induced constipation leads to abdominal distention and results in elevation of the diaphragm. As a result attention to perioperative bowel function is important. Additionally, when upper extremity surgery is performed under scalene block, ipsilateral diaphragm paralysis usually occurs. This technique is relatively contraindicated in patients with severe AS. Patients such as ours need aggressive early mobilization and careful attention to bowel function post-operatively to minimize pulmonary complications such as atelectasis.
Patients such as this present difficult management for the anesthesiologist. Intubation can be difficult and may require fiber-optic guidance because of the fixed neck flexion, as well as the possibility of temporomandibular and cricoarytenoid joint involvements which can further compromise the oral aperture. Our custom is to consult with anesthesia in advance of surgery [1].
In summary, patients with AS clearly benefit from arthroplasty, but require collaborative care to optimize outcome. This patient underwent successful bilateral knee arthroplasty under one anesthesia via combined spinal epidural technique, without complication. He was discharged on the fifth post-operative day on coumadin for DVT prophylaxis, with nearly 90° of flexion and hip extension to near neutral, to complete rehabilitation at an inpatient facility.