
Abstract

Introduction
Qualification is defined as the “graded, ‘fit-for-purpose’ evidentiary process linking a biomarker with biology and clinical endpoints” [5]. As recently defined by the Federal Drug Administration (FDA), “qualification is a conclusion that within the stated context (manner and purpose) of use, the results of assessment with a drug development tool (DDT) can be relied upon to have a specific interpretation and application in drug development and regulatory decision making” [3].
Biomarkers of OA
However, currently there are no FDA-qualified osteoarthritis (OA) biomarkers. All OA biomarkers in current use are for research use only. There are two biomarkers, NTX1 and CTX1, used in osteoporosis research and clinical monitoring that are in fact in vitro diagnostics for osteoporosis. These, along with the advent, in 1979, of dual-energy photon absorptiometry as an FDA-approved method for quantifying bone mass of the spine, led to the rapid development of effective osteoporosis drugs [1]. OA currently is analogous to osteoporosis approximately 30 years ago—a disease in need of robust FDA-approved outcome measures to overcome the lack of appropriate tools for sensitively quantifying the state of the OA joint. Some of the current critical knowledge gaps related to OA biomarkers are listed in Table 1.
Some of the current critical knowledge gaps related to OA biomarkers

The FDA recently issued guidance describing the qualification process for DDTs intended for potential use, over time, in multiple drug development programs [3]. As noted by the FDA, in the past, the qualification of DDTs was on a case-by-case basis, benefiting only the submitter of the application. The increasing complexity and cost related to development of DDTs are more likely to succeed in a collaborative setting that benefits all stakeholders and encourages participation in advance of being certain it will be of immediate value. It is believed that this approach will likely speed the process of DDT development [3]. Moreover, the new guidance is intended to provide some degree of generalizability for use of the tools such as use across multiple clinical disorders, multiple drugs, or drug classes. The pathway for DDT qualification defined by the FDA/Center for Drug Evaluation and Research (CDER) is summarized in Table 2. These particular procedures pertain to the pathway related to qualification for use by any interested party when needed for drug development.
Pathway for drug development tool (DDT) qualification
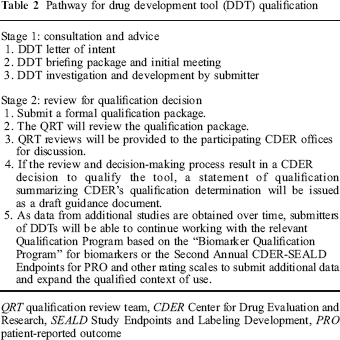
QRT qualification review team, CDER Center for Drug Evaluation and Research, SEALD Study Endpoints and Labeling Development, PRO patient-reported outcome
Growing out of the OARSI/FDA Initiative biomarkers projects [2, 4] has become a major project termed the OARSI/Foundation for NIH biomarkers project to address the critical need for FDA-qualified OA biomarkers. The project will utilize already acquired images and samples from the Osteoarthritis Initiative study.
The study will encompass three main aims. To examine the relationship between efficacy markers and clinical outcomes [change in radiographic, magnetic resonance imaging (MRI), and biochemical markers over 1–2 years will predict progression to clinical outcome at 4 years] To identify the most responsive biomarkers of progression To develop a risk score based on baseline values of several biomarkers including JSN, quantitative and semiquantitative MRI measures, and biochemical biomarkers that would determine those individuals who progress to end-stage disease faster
In addition to radiographic and MRI outcomes, the study will evaluate 11 commercially available OA-related biomarkers poised to be used by any interested parties if the data justify their use in the contexts encompassed by the specific aims.
Summary and Future Initiatives
As milestones from the OARSI/Foundation for NIH biomarkers project, we expect to have a well-identified DDT concept and evidence indicating a potential to have one or more uses in drug development. We anticipate subsequent waves of qualification will involve additional biomarker candidates, e.g., based on unbiased discovery methods (such as proteomics) and additional types of biomarkers (such as RNA) and their probable combinatorial use.
In the subsequent phases, we hope to help develop and commercialize useful custom multiplex OA biomarker panels, advance investigational and new biomarkers, tackle the difficult problem of developing means of diagnosing very early OA including susceptibility to posttraumatic OA shortly after acute injury, promote effective utilization of existing resources such as the Brandt sample repository, and encourage ongoing collection and analysis of samples from clinical studies and trials. Thus, the process will be an iterative one but hopefully one well informed by the paradigm of the OARSI/Foundation for the NIH OA Biomarker study that will rapidly lead to the first available FDA-qualified biomarkers as drug development tools.
Footnotes
Acknowledgments
The author wishes to acknowledge NIH NIAMS PO1 AR050245, NIA Claude D. Pepper Older Americans Independence Centers 5P30 AG028716, and NIA R21 AG039782-01 for funding support.
Disclosures
The author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.