
Abstract
Introduction
Our current understanding of osteoarthritis (OA) is as an illness (the clinical manifestations of the disease) and a disease (the structural joint changes) [19]. To date, relatively little attention has been paid to understanding the illness relative to the disease. Better characterization of our patients’ symptoms is likely to improve our ability to target the right treatment to the right patient, resulting in improved outcomes.
Patient Perceptions of Pain from OA
Pain has been identified as the top concern for people living with OA; pain drives health care use [18]. The traditional biomedical view of OA pain is as nociceptive, resulting from joint tissue injury [13]. However, this perspective fails to recognize that pain and other OA symptoms may be strongly influenced by psychological and physical health [40, 42], social support [16], gender [43], coping behaviors [27, 30, 36], and self-efficacy [28]. This explains, in part, why people with similar OA severity radiographically may experience markedly different levels of pain or other symptoms [5, 32]. Thus, evaluation of the illness OA, and pain in particular, warrants a biopsychosocial perspective that incorporates not only biological and physiological factors, but also social, cultural, and personal factors [5, 8].
Qualitative work in the UK [1, 45] and Canada [14] found that the OA pain experience is not adequately captured by existing measures. Further, scores on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale [4] are confounded by physical functioning (the scale asks about pain experienced with specific activities). Thus, WOMAC pain and physical function scores are highly correlated [41]. Together, these studies suggested the need for a new OA pain measure. To address this gap, focus groups were conducted in 143 individuals aged 47 to 92 years with painful hip or knee OA to obtain detailed descriptions of OA pain from early to late disease, including the features of OA pain that participants found most distressing. Two distinct types of pain were identified: a dull, aching pain that became more constant over time, punctuated increasingly with short episodes of a more intense, often unpredictable, emotionally draining pain that often led to avoidance of social and recreational activities. Distressing pain features were the pain itself (its intensity, quality, and predictability) and the pain's impact on mobility, mood, and sleep [23]. Using these data, a new hip/knee OA pain measure was developed, the OARSI-OMERACT Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP) [9, 20, 23]. Psychometric testing of the ICOAP to date indicates its reliability, validity, and responsiveness to changes in OA pain following both pharmacological and surgical intervention [20].
In addition to supporting the development of a new pain measure, this qualitative research highlighted the importance to patients of the quality or characteristics of their pain and its impact on sleep and mood—all features that were previously poorly understood and evaluated both in OA research and clinical practice. Almost one quarter of the focus group participants characterized their OA pain using descriptors typically used for neuropathic-type pain [25]. Indeed, mounting evidence exists to suggest that people with chronic, painful OA may experience sensitization of the central pain pathways or central sensitization [3, 7, 10, 15, 17, 26, 39], which may lead to neuropathic-type pain in a subset of people with painful OA [6, 24, 31, 37]. Research evaluating the discriminatory symptom profile suggesting central sensitization in OA is ongoing; predominance of symptoms suggesting sensitization may assist in mechanism-based selection of OA pain therapies, which may ultimately improve patient response and outcomes [25].
To elucidate the relationships among pain, fatigue, disability, and depressed mood over time, these factors were assessed in an established cohort with moderately severe hip/knee OA at three time points over 2 years. Controlling for contextual factors, we found that OA pain caused depressed mood through its effect on fatigue and disability (Fig. 1). These effects led, in turn, to worsening of pain and disability over time. Contextual factors that negatively influenced these relationships included poor coping and lower social support [22]. These findings support the need for improved OA pain management, including contextual factors like coping, to prevent or attenuate the negative downstream effects of pain.
The relative strengths of the longitudinal relationships after controlling for contextual factors [22] based on regression coefficients. Reprinted from Hawker GA, Gignac MA, Badley E et al. A longitudinal study to explain the pain-depression link in older adults with osteoarthritis, Arthritis Care Res (Hoboken), 63(10):1382–1390, copyright 2011 with permission from John Wiley & Sons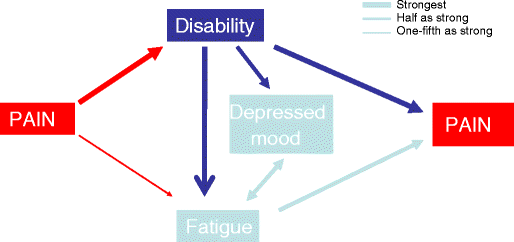
Sleep was not explicitly examined in the above-noted longitudinal study but likely mediates, in part, the relationship between OA pain and fatigue. Indeed, Lavigne et al. [33] have shown that chronic pain leads to disruption of sleep architecture and sleep deprivation, reducing pain threshold and increasing perceived discomfort. In people with chronic, painful OA, self-reported poor sleep quality is common [2, 34, 35] but is rarely assessed or treated [21]. Depressed mood is also highly prevalent in people with painful OA [22], which is concerning as comorbid depression has been linked to reduced adherence to self-management and pharmacologic interventions and reduced effectiveness of these strategies [11, 44]. Identifying and treating sleep and mood disorders among people with painful OA may help to reduce the downstream effects of OA pain. One intervention that is likely to have the greatest overall impact is physical activity, which has been associated with reductions in pain [12], reductions in symptoms of anxiety and depression [38], and improvements in sleep quality [29].
Summary
Research to date supports a comprehensive approach to the evaluation of the OA illness experience, incorporating the quality, intensity, and predictability of the pain as well as its impact on fatigue, mood, sleep, and disability. A greater understanding of the relative efficacy and effectiveness of OA treatment options on each of these symptoms has potential to improve selection of the best therapies for an individual patient. Recognition of, and attention to, the influence of contextual factors on the OA illness experience, in particular coping skills and social support, may further reduce the impact of the disease. Finally, disordered sleep and mood and the presence of pain sensitization should be considered as alternative treatment targets, particularly among patients for whom first-line OA pain medications, e.g., NSAIDs, cannot be safely used.
Footnotes
Disclosures
The author certifies that she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.