
Abstract

Keywords
The Centers for Disease Control and Prevention (CDC) reported in 2006 that arthritis affects 46 million adults in the United States and is our nation's most common cause of disability.1 While there are more than 100 different forms of arthritis, rheumatoid arthritis and osteoarthritis (OA) are the two most common forms that affect adults. Rheumatoid arthritis is an autoimmune disease resulting in inflammation of the joints, which leads to pain and destruction of joints and organs. OA is characterized by a breakdown of cartilage, the cushion between the ends of bones, and can also damage ligaments, menisci, and muscles.
OA is the most common form of arthritis; it represents an enormous public health burden in terms of health care costs, disability, lost earnings, and reduced quality of life. In 2005 the National Arthritis Data Workgroup estimated that 27 million U.S. adults—more than 10% of the adult population— had OA,2 and it has also been estimated that by 2030, 67 million U.S. adults will have arthritis.3 In 2009 almost 1 million people were hospitalized for OA; it is also the main underlying cause of joint replacement, for which the 2009 costs were $42.3 billion.4 In 2003 arthritis and other rheumatoid conditions resulted in $128 billion in total medical costs and lost earnings.5
In 2010 the CDC and the Arthritis Foundation published A National Public Health Agenda for Osteoarthritis (www.cdc.gov/arthritis/docs/oaagenda.pdf), a major call to action. It lays out how successfully employing novel approaches to the prevention, early detection, and treatment of OA can affect the financial, societal, and personal burden of this chronic disease. Though this groundbreaking report placed a spotlight on many clinical and advocacy groups, the largest group of health care providers—nurses—was notably absent. Nurses have ranked at the top of Gallup's annual “honesty and ethical standards” poll for many years,6 and as educators nurses can have great influence on public perceptions of disease processes and care. In the primary care setting, studies have shown, nurses’ assessment and coordination of care, as well as their education of patients about disease processes and prevention of complications, are invaluable.7–9
Symposium planning committee, left to right: Maureen Shawn Kennedy, Patricia Quinlan, Marjorie G. Kulesa, Laura Robbins, Basia Belza, and Elizabeth Schlenk.
Although articles about OA have been published in nursing journals, we question whether nurses are missing opportunities to teach patients about screening, prevention, complementary therapies, and pain management, perhaps because of the misperception that OA is part of the aging process and less important to treat than diabetes or cardiovascular disease.
This question led us to other questions. Are enough nurses being trained in OA management? Are assessment tools for monitoring both disease progression and complications widely available in all primary and acute care settings, physicians’ offices, clinics, and community health care centers? Do assessment and monitoring tools pay adequate attention to patients’ level of health literacy, language, age, gender, race, culture, ethnicity, and socioeconomic factors?
To answer these questions and determine the level of awareness and knowledge of OA among nurses, AJN, the Hospital for Special Surgery, and the National Association of Orthopaedic Nurses developed a collaborative project—the State of the Science in the Prevention and Management of Osteoarthritis. The objectives were to identify gaps in the science and barriers to the early identification of OA and the implementation of interventions that promote mobility, decrease pain, and slow progression. describe the state of the science of current interventions for preventing immobility and managing the effects of OA. achieve consensus on the priorities for developing the best nursing practices—in the clinical, educational, research, and policy arenas—in order to meet the needs of diverse populations with OA in a variety of settings. disseminate the analysis and recommendations to clinicians, nurse leaders, educators, researchers, specialty nursing organizations, other health care professionals, policymakers, consumer advocacy groups, and the general public.
The Symposium
The collaborators convened a symposium at the Hospital for Special Surgery in New York City in July 2011. The symposium brought together more than 40 leaders in nursing, physical therapy, medicine, complementary and alternative medicine, public health, pharmaceutical research, and others. All were practicing, teaching, and/or conducting research related to OA or were involved in OA advocacy initiatives. Organizations represented included the American Academy of Nurse Practitioners, the American Society for Pain Management Nursing, the Arthritis Foundation, the Association of Rehabilitation Nurses, the Association of Rheumatology Health Professionals, the CDC, the Rheumatology Nurses Society, and the U.S. Bone and Joint Initiative. Partial funding for the symposium was provided by the Division of Education and Academic Affairs at the Hospital for Special Surgery. Unrestricted educational grants were also received from Genzyme and Zimmer.
The progam started with participants hearing from a person living with OA, Kathy Geller. Her description of this debilitating disease and its treatments set the stage for the conference. Speakers then presented highlights of their papers on the current knowledge of OA, national initiatives, the nurse's role in assessing risk and progression, interventions to relieve symptoms and minimize progression and disability, and strategies for promoting self-management. Each presentation was followed by a question-and-answer period. A panel of three orthopedic nurses identified issues that typically arise when caring for adult patients with OA.
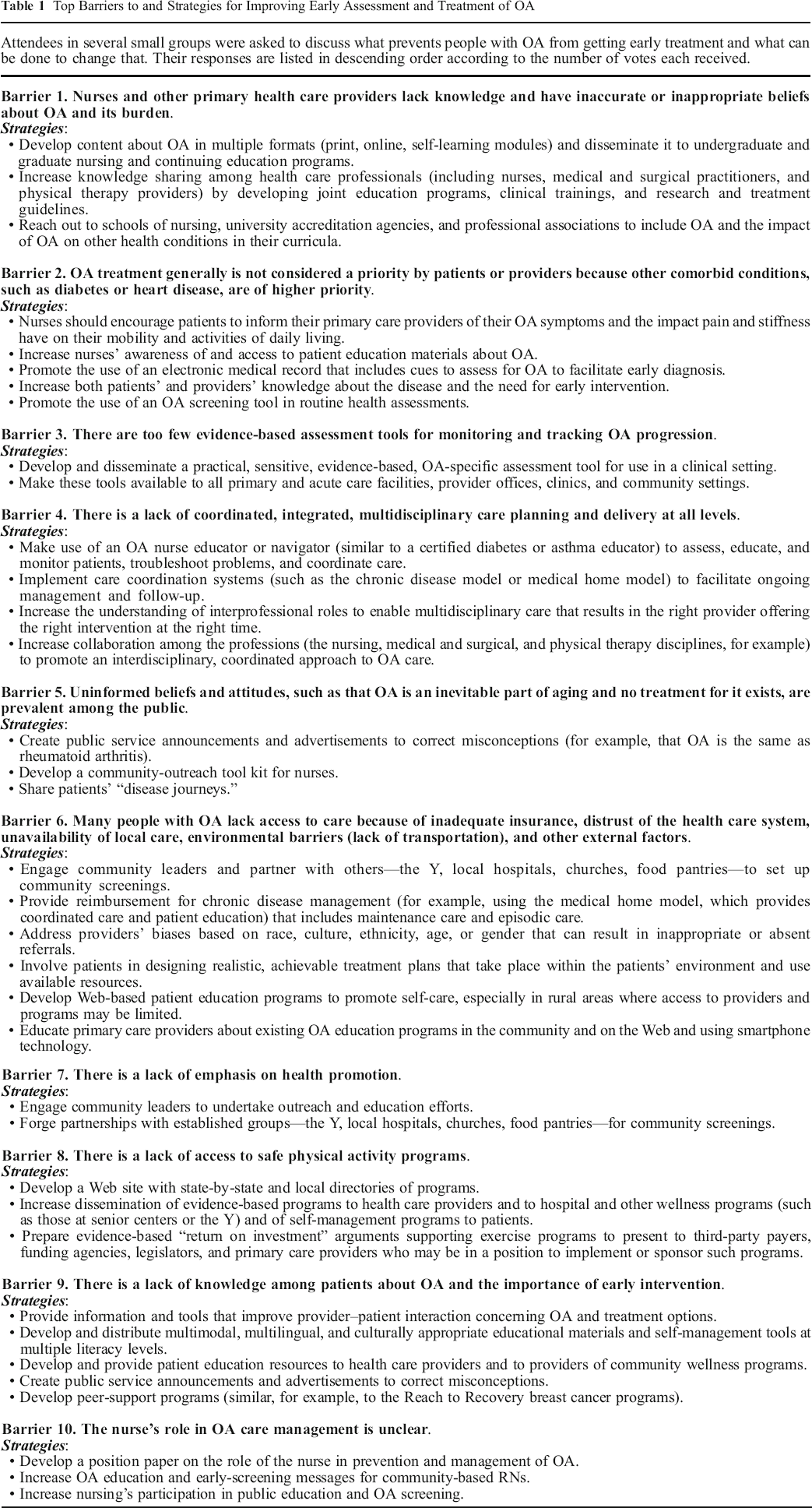
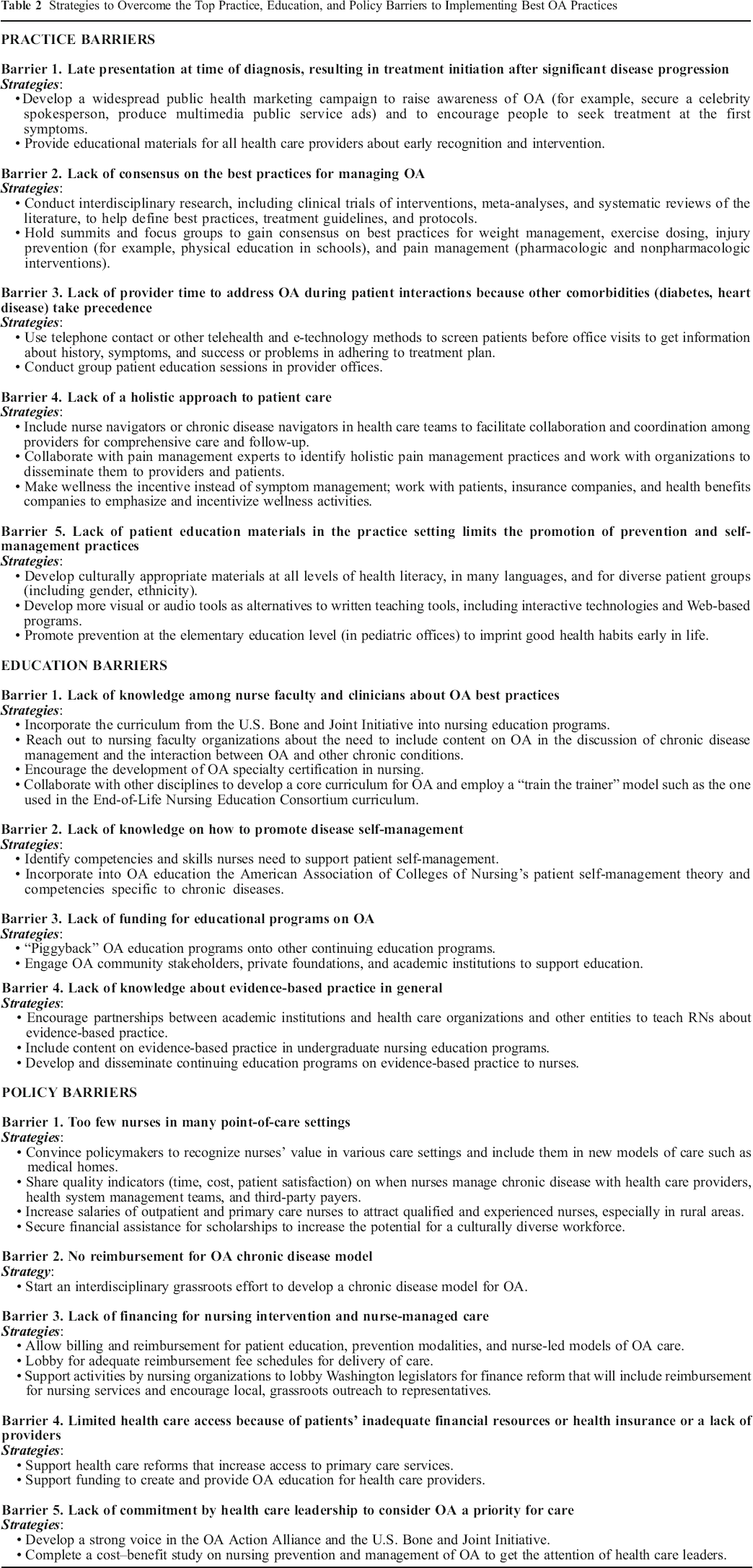
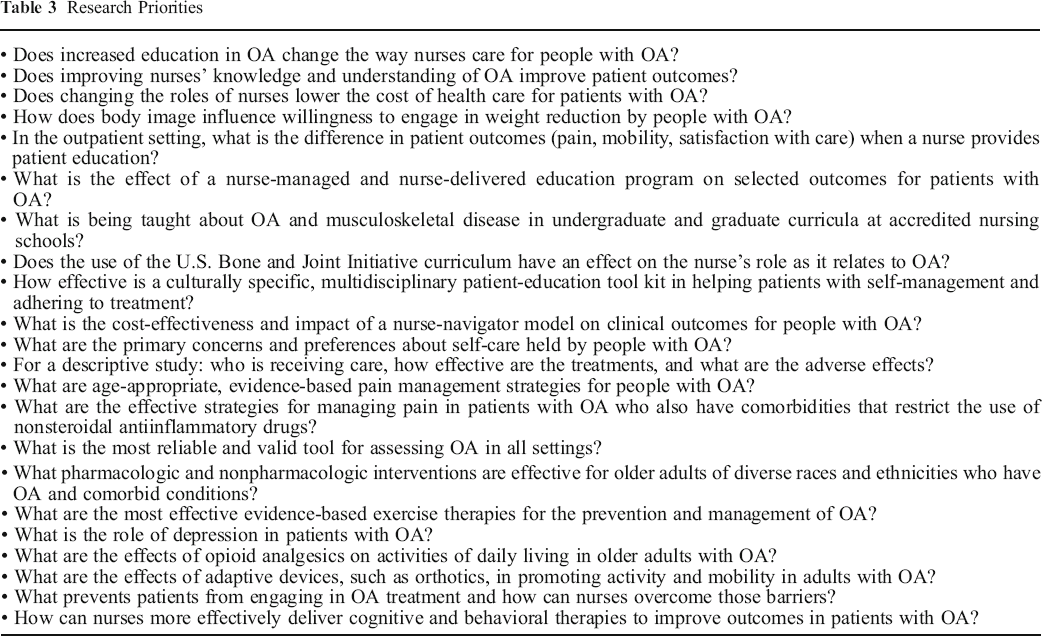
Presentations were followed by small-group discussion and identification by consensus of the top barriers and strategies. The groups identified strategies for addressing both barriers to early assessment and treatment and barriers in practice, education, and policy that prevent the implementation of best practices, as well as future research priorities. The small groups then presented their ideas to the entire group so that consensus could be achieved (see Tables 1, 2, and 3).
Top Barriers to and Strategies for Improving Early Assessment and Treatment of OA
Strategies to Overcome the Top Practice, Education, and Policy Barriers to Implementing Best OA Practices
Research Priorities
Main Themes
OA causes changes in joint structure, including osteophyte formation and joint capsule thickening, that lead to stiffness, aching, and pain. Pain increases with age and is greater among African Americans and women.12 Primary risk factors include genetic propensity, female sex, and older age; obesity, injury, and occupations that produce repetitive stress are the three greatest secondary risk factors.
Other groups that have developed initiatives are the CDC, the American College of Rheumatology (ACR), and the National Committee for Quality Assurance. This increased attention to the burdens of OA represents a movement, one that has been sparked by such coalitions’ policymakers and public health advocates.
A number of screening tools have been developed for OA, one of which is the evidence-based Risk Assessment Tool for those with knee pain (available at www.fightarthritispain.org). The primary goal is to identify those at risk in order to prevent disease onset, and the secondary aim is to prevent progression. If the degree of risk is determined to be high, the person can choose to have a comprehensive evaluation early in the disease process in order to learn how to prevent OA or slow disease progression.
Rehabilitation interventions aim to decrease pain and disability and improve function. They include exercise, physical techniques (such as applying heat, ice, and ultrasonography), manual mobilization and manipulation, assistive devices, gait training, and self-management education. Most of the primary professional orthopedic groups have publicly recognized the value of exercise and rehabilitation, and many of them have issued rehabilitation guidelines (for example, the ACR).14 Studies evaluating rehabilitation (summarized in two recent Cochrane reviews15, 16) have focused mainly on land-based exercise for knee OA and have shown small to moderate benefits for pain and function. A Cochrane analysis of six short-term studies of moderate or low quality found that aquatic exercise provided small to moderate improvements in function and only minor pain relief.17 Physical modalities are numerous and include thermotherapy, electrotherapy, light therapy, and pressure. Another analysis of three moderate-to-low-quality randomized clinical trials involving a total of 179 patients with knee OA showed that thermotherapy (heat or cold) improved range of motion, knee muscle strength, and function.18 Cold did not seem to affect pain but did reduce swelling.
Further study is needed on the appropriate dose of exercise, as are rigorous, longer-term studies on other interventions.
Pharmacologic agents are a primary form of treatment for OA because there are no approved disease-modifying therapies. Nonpharmacologic methods—patient education, weight loss, exercise, and physical therapy—are underused.14 Pain is the most often cited disability-causing symptom among women in later life and can be so severe that it threatens cognition, mobility, and independence.19
Only a few studies have attempted to explore pain management in OA in different populations (grouped by race, culture, ethnicity, age, or gender). Most of the pharmacologic agents have been shown to decrease pain mildly to moderately, with relief being moderate for acetaminophen and better for opioids and hyaluronan. Oral acetaminophen (used with caution) and topical agents have the best safety profiles. Adverse effects can be serious and include hepatotoxicity caused by acetaminophen overdose and the gastrointestinal, renal, or cardiovascular toxicity caused by nonsteroidal antiinflammatory drugs. Opioids are associated with serious adverse events and are usually used as a last resort.
Complementary and alternative medicine (CAM) is often used by patients to relieve symptoms and by many others to prevent OA. Traditional Chinese medicine and Ayurveda have been used for centuries, and thousands of other therapies and products are available. The National Center for Complementary and Alternative Medicine, part of the National Institutes of Health, has described CAM therapies at http://nccam.nih.gov/health/whatiscam. Unfortunately, because of limited funding (most CAM agents are not patentable), few large randomized, controlled trials have been conducted. However, numerous smaller trials have indicated that some CAM therapies are useful, particularly yoga, t'ai chi ch'uan, acupuncture, glucosamine sulfate supplementation, and others.
Middle-aged, well-educated white women as well as those with chronic illness and troublesome symptoms use CAM the most,20 and patients with all types of arthritis (data for OA alone are not available) use CAM significantly more than others do.21 Estimates of use by arthritis patients range from 59% to 90%.22
Behavior-changing and skill-building interventions work toward exercise performance and weight loss. Physical activity interventions can be delivered in a number of ways—in the home or in health care, community, or workplace settings. No single format has been found to be superior, but programs of longer duration (12 or more supervised sessions) give better results.15 A recent meta-analysis of exercise delivered in a community setting found clinically significant improvements in pain and function.25 There are few weight loss programs targeted specifically at OA.
Ideally, the provider should recommend educational or behavioral-change programs: arthritis patients whose physicians recommended a program were 18 times more likely to attend.26 Practitioners should be trained to build collaborative relationships with their patients in order to best support them. Other needed system changes include group health care visits and links to community services.
Nurses are in a unique position to inform and support their patients’ self-management, and there are many strategies that can help them better encourage it. Multimodal, multilingual, and racially and culturally appropriate patient education materials can be developed at multiple literacy levels, as can online programs, especially for use in rural areas. Peer-to-peer support programs can be developed for patients and summits can be held to gain consensus on the best weight management practices. Patient and community tool kits can be developed, and community leaders can be encouraged to participate in OA education.
Footnotes
Acknowledgements
Laura Robbins is a senior vice president for education and academic affairs at the Hospital for Special Surgery, New York City. Marjorie G. Kulesa is a past president of the National Association of Orthopaedic Nurses and the nurse coordinator for the Department of Orthopaedic Surgery at Winthrop-University Hospital, Mineola, NY. Contact authors: Laura Robbins (robbinsl@ hss.edu) and Marjorie G. Kulesa (mkulesa@ winthrop.org). The authors acknowledge Phyllis Tower for her help in searching the literature and writing. The authors have disclosed no potential conflicts of interest, financial or otherwise.