
Abstract
Background
The incidence of hip replacements in the younger patient is ever increasing. With this in mind, improving the longevity of hip arthroplasties is paramount. Alumina ceramic is a promising bearing surface due to its low wear rate and biological inertness.
Purpose
This study aims to review our experience with ceramic-on-ceramic total hip arthroplasty, reporting on the need for revision as well as the cause of failure. Our secondary purpose is to review our experience with the phenomenon of squeaking analysing and its effect on clinical outcome with specific emphasis on component positioning. Also reported are the results of our retrieval analysis of explanted components documenting the wear rate and our analysis of strip wear.
Methods
A consecutive series of 301 primary cementless alumina-on-alumina total hip arthroplasties at a minimum of 10 years follow-up was reviewed. These arthroplasties all had third-generation ceramic-on-ceramic bearings performed through a posterior approach with repair of capsule and external rotators to bone. We analysed hips both clinically and radiographically. Analysis of wear in 62 ceramic bearings was performed using a Roundtest RA300 machine (Mitutoyo; Andover, UK), which has an accuracy of 0.01 μm.
Results
Overall, the survival rate of the implants was 98% at 10 years. No ceramic fractures were encountered in this study. Seventy-four patients reported squeaking hips, and two cases were revised due to squeaking (0.6%). No failures were related to bearing wear.
Conclusions
We believe that ceramic-on-ceramic is a safe bearing coupling with excellent survivorship at 10 years.
Introduction
Interest in ceramic-on-ceramic hip arthroplasty is increasing as a result of the realisation of osteolysis associated with wear debris generation in conventional metal-on-polyethylene bearings and the recent problems associated with metal-on-metal articulations. The first ceramic-on-ceramic hip arthroplasty was implanted in 1970 by the French surgeon Pierre Boutin. This was in the form of an all alumina cup and an alumina ceramic ball glued to a cemented metal stem. Alumina ceramic was attractive to Boutin because of “its hardness which renders it perhaps indestructible for the life of the patient, its perfect chemical inertia, its low coefficient of friction and its tolerance by the organism” [1]. After having initial concerns regarding the brittleness of ceramic components, he was encouraged with the early results of his first 200 cases, in which no fractures of components occurred. This early design (Ceraver-Osteal hip) was not used outside Europe, and not until the design by Mittlemeier and Walter in Germany that ceramic-on-ceramic bearings gained popularity worldwide. The Mittelemeier Autophor ceramic-on-ceramic hip was used extensively outside of Europe, including the USA, Australia and Japan. These early prosthesis designs had high failure rates as a result of poor acetabular component fixation [5, 22]. This problem was addressed with the use of a metal-backed cup design.
Not only has the design of ceramic implants evolved but also the composition. The release of third-generation ceramic, in 1994, saw the introduction of ceramic manufactured with use of a hot isostatic pressing to reduce grain size, limit grain boundaries and inclusions, ultimately providing better wear properties and resistance to fracture [20]. When zirconia particles are dispersed and incorporated into the ceramic alumina matrix, the fracture resistance of the matrix improves. This alumina matrix composite, Biolox delta is 82% alumina, 17% zirconium oxide, 0.3% chromium oxide and 0.6% strontium oxide [9]. Only sporadic reports of Biolox delta acetabular component fracture appear in the literature with no reported fracture of a Biolox delta femoral head since its introduction in 2004 [16].
Because of the increased brittleness of ceramic, some surgeons are reluctant to use it due to the risk of component fracture. A review of 25 years of ceramic hip replacements by Sedel and co-workers found 13 fractures in 5,500 cases, including eight head and five cup fractures [6]. Survivorship of ceramic-on-ceramic bearing-related failures is very encouraging with reports of 100% survivorship at 10 years [8] (Table 2). Lewis et al. [11] also reported excellent results at a median of 8 years.
Additionally, ceramic-on-ceramic hip arthroplasty carries a risk of the development of squeaking. Squeaking is defined as a high-pitched audible sound that occurs during movement of the hip joint. It is a forced vibration, which comprises a driving force and a dynamic response. The driving force is believed to be the frictional vibrating force that is generated between the hard bearing materials, and the dynamic response is resonance of a part of the hip joint—yet to be confirmed. It was first described in the 1950s, following Judet acrylic hemiarthroplasty. Charnley also noted squeaking during his friction analysis of alumina ceramic on ceramic. The incidence of squeaking range from <0.5 to 11% in reports [7, 14, 18, 19], with a lower rate of revision for squeaking (0.6%) [12]. Jarrett et al. believe that this phenomenon has been under-reported because the presentations are often transient and often not reproducible during follow-up consultations. The implication of squeaking is not known as yet, but it has been reported that the wear of squeaking hips is greater than retrieved silent hips, although wear rates are not great enough to produce bearing failure [17].
The purpose of this report is to review our experience with ceramic-on-ceramic total hip arthroplasty (THA). Specifically, we aim to report on the need for revision as well as the cause of failure. Our secondary purpose is to review our experience with the phenomenon of squeaking analysing and its effect on clinical outcome with specific emphasis on component postioning and the incidence of this phenomenon. We also wish to report the results of our retrevial analysis of explanted components documenting the wear rate and our analysis of strip wear.
Methods
In our experience, we have performed 5,500 primary hip arthroplasties, and over 4,000 of which were ceramic-on-ceramic bearings. To document the mid-term clinical success as well as the causes and rate of failure of ceramic-on-ceramic THA, we reported a consecutive series of 301 primary cementless alumina-on-alumina total hip arthroplasties at a minimum of 10 years follow-up [21]. These arthroplasties all had third-generation ceramic-on-ceramic bearings performed through a posterior approach with repair of capsule and external rotators to bone. We analysed hips both clinically and radiographically.
We separately analysed this population of ceramic-on-ceramic THAs for the development of squeaking. When squeaking developed, we recorded the time to onset from the date of the arthroplasty. We recorded the demographics and body characteristics of those who developed squeaking. We specifically noted the activities that most typically resulted in audible squeaking. The effect of squeaking on the clinical outcome was assessed using the Harris hip score, which was compared to those without squeaking. The effect of squeaking on patient satisfaction was also assessed and compared to those without squeaking. Radiographic analysis of the squeaking hips, assessing component positioning, was performed and compared to the non-squeaking hips.
Seven ceramic bearings have been retrieved more than 6 months after implantation. Analysis of wear in these bearings was achieved using a Roundtest RA300 machine (Mitutoyo; Andover, UK) which has an accuracy of 0.01 μm.
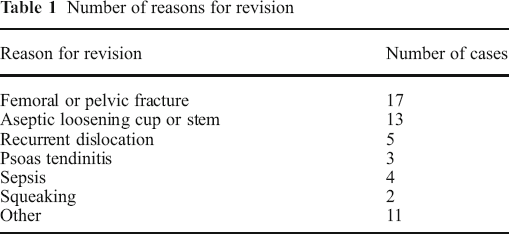
We have carried out further analysis on 55 ceramic heads retrieved from ceramic-on-ceramic arthroplasties in our unit. These were revised for a number of reasons, including aseptic loosening, infection and recurrent dislocation, but bearing failure, resulting in squeaking, occurred in only two hips (Table 1). We mapped the femoral head surface of these retrieved implants using an artificial hip profiler (Redlux Ltd., Southampton, UK). This machine uses a white light sensor to collect 40,000 points on the surface of the head in approximately 1 min. The data collected were then imported into software to match a best-fit sphere. The colour scale shows you wear depth in microns.
Number of reasons for revision
Results
At 10 years, 10% of the patients had died of unrelated cause, and 5% were revised. The average Harris hip score was 95 points at the last follow-up, and 97% of the patients scored an excellent or good result, with less than 5% have moderate residual pain. Radiographically, all patients assessed had evidence of stable bony ingrowth, and no evidence of any osteolysis was present. There were eight revisions in all, four stem revisions due to periprosthetic fracture, one secondary to aseptic loosening and one to facilitate a femoral shortening osteotomy. There were one cup revision for psoas tendonitis and one for anterior impingement. Overall, the survival rate of the implants was 98% at 10 years [21]. No ceramic fractures were encountered in this study.
We found a median wear rate of 0.2 mm3 in the ceramic bearings associated with a low incidence of osteolysis with only one case recorded out of 301 hips. We have actively found 74 patients with squeaking hips [15]. The average time to onset of squeaking was 40 months after surgery. Of the 74 patients, 11 hips had stopped squeaking spontaneously. Sixty-three percent of squeaking hips squeaked less than once per day; 32% reported once per day, and 5%, every step. Bending over caused the squeaking in 77% of cases, walking in 16%, stairs in 4% and sports in 3%. Those who squeaked were found to be younger (<60 years, p = 0.0002), heavier (p = 0.04%) and taller (p = 0.003). Squeaking hips had a significantly higher range of post-operative internal (p = 0.001) and external (p = 0.003) compared with silent hips. Patients with squeaking hips had significantly higher activity levels (p = 0.009). A squeaking hip was not associated with a significant difference in patient satisfaction (p = 0.24) or Harris hip score (p = 0.34). Four implant position factors enabled good prediction of squeaking, namely, high acetabular component inclination, high femoral offset, lateralisation of the hip centre and either high or low acetabular component anteversion.
Forty-six of the retrieved 55 heads showed stripe wear in two distinct patterns, an anterosuperior wear stripe and a posterior wear stripe. The anterosuperior wear occurs in walking, and the posterior wear occurs when the hip is flexed—sitting, climbing stairs or rising from a seated position when edge loading occurs. Analysis of these two distinct patterns of stripe wear showed a median volumetric femoral head wear rate of 1.9 mm3/year for anterosuperior edge loading and 0.2 mm3/year for posterior edge loading, although posterior wear was more commonly found (32/46). It was noted that there were no failures related to bearing wear. There were two cases revised due to squeaking in this group (0.6%).
Discussion
We report our experience of ceramic-on-ceramic hip arthroplasty at a minimum of 10 years and compare this with mid-term analysis in the literature. We report our experience of squeaking hips and relate these to patient factors and component placement. We also report our retrieval analysis, looking at wear rate and patterns of wear seen.
There are a number of limitations to this study. Although we actively sought out any and all patients with squeaking hips, we cannot be sure all were captured as squeaking may not be noticeable or bothersome to some of the patients and may, therefore, be under-reported. In our 10-year follow-up study, we were unable to totally eliminate lost to follow-up; however, this is similar to other series reporting mid-term survival results.
In our consecutive series of 301 primary cementless alumina-on-alumina total hip arthroplasty, we found a survivorship of 98% at 10 years. This is comparable with other published mid-term analysis of ceramic-on-ceramic hip arthroplasty with survivals ranging from 95 to 99% (Table 2).
Survivorship of ceramic-on-ceramic bearing related failures

As part of a three-arm study
We found a squeaking rate of approximately 1.9% (74/4,000) in our cohort of ceramic-on ceramic hip arthroplasties. Analysing patient factors and component placement in squeaking hips suggests that factors that increase the mechanical forces across the hip joint or increase the risk of neck-to-rim impingement and, therefore, edge-loading are those that predispose to squeaking [17]. This is confirmed by our finding of stripe wear on retrievals. Only two cases (0.05%) were revised for squeaking in our series, which we believe is due to the benign nature of this phenomenon, with patient satisfaction and functional outcomes, having no difference from non-squeakers.
Analysis of wear in retrieved ceramic heads showed two distinct patterns with rates of 1.9 mm3/year for anterosuperior edge loading and 0.2 mm3/year for posterior edge loading. These findings compare very favourably with the threshold wear rate of 38 mm3/year for polyethylene below in which osteolysis is not expected to occur [4].
In conclusion, alumina ceramic-on-ceramic bearings in cementless primary total hip arthroplasty has been shown to have good survival rate at 10 years with good functions, low wear rate and no adverse radiographic changes. Biolox delta ceramic appears to be a welcome improvement to an already durable bearing surface with good long-term results expected.
Footnotes
Disclosures
One or more of the authors (DM, CJ and WKW) has received research funding from Depuy, Stryker. Dr. Walter is a member of a speakers’ bureau or has made paid presentations on behalf of Stryker and Finsbury, serves as a paid consultant to or is an employee of Finsbury and has received research or institutional support from Stryker, DePuy Finsbury, CeramTec and global Orthopaedics. Dr. Molloy or an immediate family member has received research or institutional support from Stryker, DePuy. Dr. Jack or an immediate family member has received research or institutional support from Stryker, DePuy. C. Esposito or an immediate family member has received research or institutional support from Finsbury. Dr. Walter or an immediate family member has received royalties from Stryker and DePuy, is a member of a speakers’ bureau or has made paid presentations on behalf of Stryker and Finsbury, serves as a paid consultant to or is an employee of Finsbury and has received research or institutional support from Stryker, DePuy Finsbury, CeramTec and global Orthopaedics.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.