
Abstract
Background
There is little comparative long-term clinical data comparing Bankart repair alone to the addition of remplissage.
Questions/Purposes
Our purpose was to compare results of patients with significant humeral head lesions and who underwent either isolated arthroscopic Bankart repair or remplissage.
Methods
This is a retrospective cohort study of 14 isolated arthroscopic Bankart and 10 remplissage repairs all with large engaging Hill-Sachs (HS) lesions. Average follow-up was 40.72 months (26.3–51.1) in the Bankart group and 31.55 months (24.1–39.9) in the remplissage group. Surgical failure was defined as a dislocation or subluxation. Groups were matched on handedness, age within 3 years, and HS lesion size. Glenoid bone loss and HS size were measured on MRI. Additionally, WOSI and DASH scores were obtained.
Results
The average age at surgery was 26.0 years (17.8–41.1) of the isolated Bankart patient and 24.4 years (16.4–38.3) in the remplissage group. The average HS lesion volume was 310.22 mm3 in the Bankart group and 283.79 mm3 in the remplissage group. The failure rate for the Bankart group was 8 out of 14 patients (57.14%). For the remplissage group, the failure rate was 2 out of 10 patients (20.0%). Average WOSI scores were 73.72 in the Bankart group and 79.54 in the remplissage group. For DASH scores, the average Disability/Symptoms Scores were 16.23 for the Bankart group and 12.05 for the remplissage patients.
Conclusions
In comparison to isolated Bankart repair, remplissage was a superior option for recurrent instability patients with large Hill-Sachs lesions as seen by diminished failure rates and improved outcome scores.
Introduction
Traumatic anterior shoulder instability is a common diagnosis in orthopedics with important anatomic considerations for the treating surgeon. Of these, the Hill-Sachs lesion has been identified as a common pathology in 67–93% of cases of recurrent anterior dislocations [14, 16, 19]. One method of addressing this pathology is the remplissage technique. This procedure has gained popularity as it can be preformed arthroscopically and is reproducible. It involves a tenodesis of the infraspinatus after which an arthroscopic Bankart repair is performed [13]. In published reports of patients treated by remplissage with Bankart repair with moderate to large Hill Sachs lesions, the failure prevalence is 8–15% with only 1.9–5.8° of external rotation loss [6, 10, 12, 13, 20]. Though there has been acceptance of the remplissage with Bankart repair procedure, there is limited data comparing patients treated with arthroscopic Bankart alone or with an arthroscopic Bankart and concurrent remplissage for recurrent anterior shoulder instability and significant Hill Sachs lesions. The comparison is necessary to assess the clinical contribution of the remplissage to improving shoulder stability in these complex patients.
Only a few studies have attempted to isolate the effects of the tenodesis of the infraspinatus through comparative analysis. Recently, Nourissat et al. published a prospective Bankart-remplissage comparison study [9]. A limitation of this paper is that the size of each patient's Hill-Sachs lesion was not controlled for or accurately measured, precluding a true comparison of the two treatments. A second study by Franceshi et al. found significantly higher failure rates in patients with Hill Sachs lesions, treated with arthroscopic Bankart repair compared to remplissage with Bankart repair, but was limited as defects were quantified by plain radiographs and arthroscopic methods rather than volumetrically with cross-sectional imaging [5].
To that effect, the present study compares two cohorts of patients, all of whom had large, engaging humeral head lesions identified and measured on high-resolution MRI. In addition, these are all patients who underwent either isolated arthroscopic Bankart repair or remplissage with a Bankart repair based on two different surgeons’ operative techniques. Our primary hypothesis is that patients with large engaging Hill-Sachs lesions will have a lower prevalence of subsequent instability after undergoing a remplissage procedure with Bankart repair. Secondarily, we will look at subjective outcomes measures of patients undergoing either procedure and we anticipate the remplissage with Bankart repair procedure will yield better outcomes compared to Bankart repair alone.
Patients and Methods
This study was a retrospective cohort study of 24 patients treated from 2006 to 2011. Two board-certified orthopedic surgeons with over 20 years of experience performed all surgical procedures. One surgeon performed all remplissage with Bankart repair procedures, which was the treatment in his practice at the time for recurrent instability patients with isolated large Hill-Sachs lesions. All isolated Bankart repairs were performed by a second surgeon, which was his predominate technique for recurrent instability patients with a Bankart lesion as well a Hill-Sachs defects. All patients within each surgeon's practice, with large Hills Sachs lesions, were treated with their preferred procedure. After IRB approval, the patients were identified based on ICD-9 and CPT codes, as well as examination of operative notes to verify proper procedure. Inclusion criteria involved either a remplissage and Bankart or arthroscopic Bankart repair, diagnosis of anterior instability, and engaging Hill-Sachs and identified large Hill-Sachs lesion on high-resolution MRI. Patients were excluded if there was no Hill-Sachs lesion identified on MRI; if the Hill-Sachs lesion did not meet the Rowe criteria for a large defect (4-cm width by 1-cm depth) [14], there was more than 20% anterior glenoid bone loss using the circle method of Sugaya et al [15] (verified by Huijsmans el al for MRI [7]) on T1-weighted axial views when the coracoid was present or the procedure was an open Bankart repair. Prior surgery was not an exclusion criterion. Pre-analysis, we identified 289 patients surgically treated by these two surgeons for anterior shoulder instability patient including patients undergoing Latarjet, open procedures, humeral bone grafting, and isolated Bankart repairs in the absence of large Hill Sachs lesions as defined by Rowe. In terms of breakdown by surgeons, instability case totals were 126 patients for JDK (over 70% of patients were anterior instability) and 163 patients for RGH (over 75% of patients included were anterior instability).
Preoperative MRI evaluation was performed utilizing a closed high-field 3.0-Tesla (3 T) scanner (Triotrim) with a shoulder coil. The MRI images were evaluated by a fellowship-trained musculoskeletal radiologist with the recording of the size of the humeral head defect. Also, the size of the Hill Sachs deformity in all patients was measured on axial, coronal, and sagittal cuts where the largest value was recorded on each axis. This MRI measurement is similar to previously published work by Park et al. [10].
Patient questionnaires were conducted by telephone by two orthopedic surgery residents, with training from the senior authors. Patient responses were compared to their charts to confirm accurate patient recall. Patients were offered the right to refuse on all voicemails and conversations. After informed consent was received, both a Western Ontario Shoulder Instability (WOSI) Score and Disability of the Arm, Shoulder and Hand (DASH) score were administered by questionnaire. Both questionnaires have been validated for assessment of instability patients as well as future predictors of dislocation [8]. Operative failure was defined as patient-reported subjective subluxation or shoulder dislocation at any point after surgery which was determined based on follow up questioning.
Independent Mann-Whitney tests were used to analyze differences between groups for continuous variables (i.e., Hill Sachs volume, outcome instrument scores). The chi-squared test and Fisher's exact test were used to determine differences between binary (i.e., failure) and ordinal or categorical variables (i.e., number of anchors). Linear regression analysis was used to determine if there was a difference in outcome between the remplissage with Bankart repair patients and isolated Bankart patients after controlling for potential confounders including age, sex, handedness, and follow-up. Binary logistic regression analysis was carried out to determine if any factor was predictive of future dislocation. Statistical significance level was set at p < 0.05. Post hoc power analysis was performed with an alpha error of 5% and beta error of 20%. Outcome proportion in each group was 20 and 51%, respectively. With relative group size 42 vs 58%, we needed a total of 88 patients. Statistical analysis was performed using SPSS version 16.0 (SPSS Inc., Chicago, IL).
Surgery
Both surgeons used similar techniques for isolated repair and concomitant repair of the Bankart lesions as well as postoperative protocols. The remplissage with Bankart repair procedure was preformed as described by Park et al [11]. Postoperatively for both surgeons, patients’ extremities are immobilized in a sling for 5 weeks, with gentle activities of daily living (bathing, writing, and so on) allowed out of the sling, with the shoulder in an adducted position at all times. Gentle active and active-assistive range of motion is allowed at 6 weeks postoperatively. At 3 months, progressive capsular stretching and strengthening of the shoulder are allowed. Patients are allowed to resume their preinjury level of activity at 6 months postoperatively or when shoulder strength is 90% of that of the unaffected limb.
Results
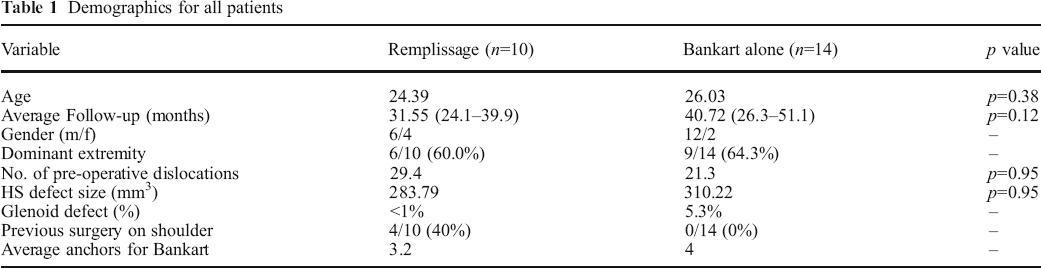
Out of 289 instability patients identified, only 14 arthroscopic Bankart repairs alone and 10 remplissage with Bankart repair patients met inclusion and exclusion criteria and were available for follow-up. In the remplissage with Bankart repair group, there were a total of 11 patients identified with only 1 patient lost to follow-up. As for the isolated Bankart repair group, a total of 18 patients were identified and 4 patients were lost to follow-up. The average follow-up was 40.72 months (26.3–51.1) in the isolated Bankart repair group and 31.55 months (24.1–39.9) in the remplissage with Bankart repair group. The average age at surgery was 26.0 years (17.8–41.1) in the isolated Bankart repair and 24.4 years (16.4–38.3) in the remplissage with Bankart repair group (see Table 1). Additionally, in comparison of the groups, the patient’s dominant extremity was involved in 60% of remplissage with Bankart repair patient and 64.3% in the Bankart group. The average numbers of preoperative dislocation was 29.4 in the remplissage with Bankart repair group and 21.3 in the isolated Bankart repair group. In terms of previous surgery, for the remplissage with Bankart repair group, 4 of the 10 (40%) had previous surgery (none were initially in the isolated Bankart group). All of these surgeries were Bankart repairs that eventually failed and were revised as a remplissage with Bankart repair. For the Bankart repair alone group, no patient had previous surgery on his or her affected shoulder. The average Hill-Sachs lesion volume (calculated by MRI) was 310.22 mm3 (SD 240.5 mm3) in the Bankart repair group and 283.79 mm3 (SD 192.6 mm3) in the remplissage with Bankart repair group (p = 0.95). For the Bankart group, the average glenoid deficiency was 5.3%, for the remplissage with Bankart repair group, the patient had <1% glenoid bone loss (p = 0.95). The average number of Hill-Sachs anchors was 1.5, and the average number of Bankart anchors in the remplissage with Bankart repair patients was 3.2. For the isolated Bankart repair group, the average number of anchors was 4. (Table 1)
Demographics for all patients
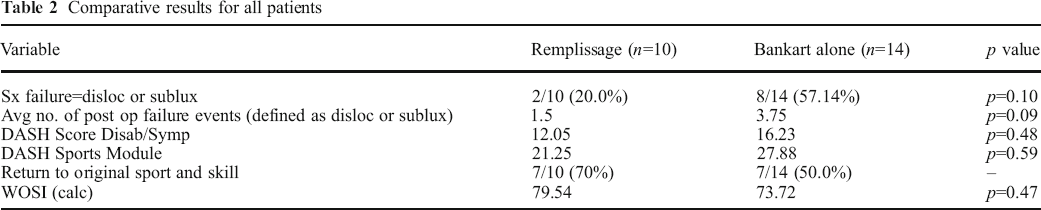
For surgical failures, the prevalence for the arthroscopic Bankart repair group was 8 out of 14 patients (57.14%) with 3 dislocations and 5 subluxations postoperatively. For the remplissage with Bankart repair group, the failure prevalence was 2 out of 10 patients (20.0%) with 1 dislocation and 1 subluxation (p = 0.10). Subgroup analysis was preformed for patients without prior surgery and no further significance was found (p = 0.16). As for revision rates, no patients (0%) in the remplissage with Bankart repair group underwent revision surgery at the time of follow-up while 1 patient (7.1%) underwent a latarjet procedure in the Bankart repair group. Average WOSI scores were 73.72 (28.75–97.08) in the Bankart repair group and 79.54 (51.25–99.58) in the remplissage with Bankart repair group (p = 0.47). As for WOSI stiffness scores, averages were 1.70 for the remplissage with Bankart repair group compared to 1.71 in the Bankart repair group. For WOSI loss of ROM scores, averages were 2.90 for the remplissage with Bankart repair group compared to 2.79 for the Bankart repair group. With regard to DASH scores, the average Disability/Symptoms Scores were 16.23 (2.27–56.82) for the Bankart repair group and 12.05 (0–29.55) for the remplissage with Bankart repair patients. The scores of the DASH sports module were 27.88 (0–87.50) for the Bankart repair alone group and 21.25 (0–87.50) for the remplissage with Bankart repair group (p = 0.59). There was no correlation between the number of preoperative dislocations and the failure prevalence. For patients who eventually failed, there were 1.5 more dislocations or subluxations per patient after the initial failure event in the remplissage with Bankart repair group compared to 3.75 more dislocations or subluxations after the initial post operative failure in the isolated Bankart group (p = 0.09). (Table 2)
Comparative results for all patients
Ten out of 10 (100%) patients in the remplissage with Bankart repair group participated actively in sports as well as 13 out of 14 (92.9%) patients in the Bankart alone group. These activities included baseball, lifting weights, snowboarding, ice hockey, and swimming. Seven out of 10 (70%) of remplissage with Bankart repair patients reported return to playing their sports after 2 years of follow-up. For the Bankart repair group, 7 out of 14 (50%) patients reported being able to return to their sport.
Discussion
Recurrent shoulder instability from humeral defects can be a challenging problem, and this is especially true with reference to failed arthroscopic Bankart repairs. The presence of a significant Hill-Sach's lesions [14] can be as high as 93% in patients with recurrent, traumatic anterior shoulder instability. Therefore, the importance of addressing humeral defects is critical [19]. Recently, this has been addressed by the remplissage with Bankart repair procedure with good results [12, 20]. However, a clinical comparison of patients with similar-sized large Hill-Sachs lesions was needed to demonstrate the additional role of adding the remplissage procedure to an arthroscopic Bankart with respect to preventing recurrent instability.
Though the remplissage with Bankart repair procedure has had increasing acceptance, there are still concerns about postoperative stiffness and significant external rotation loss after surgery which has been reported by Deutsch and Kroll [4]. Despite this case report, most of these concerns have been addressed with further studies demonstrating external rotation loss of 1.9–8.9% with minimal reported stiffness of patients after the remplissage with Bankart repair procedure [9, 10, 13, 20]. Though studies have hypothesized mechanisms of failure for patients with large humeral head defects treated with isolated Bankart repair, there has not been full acceptance in the orthopedic community [3, 12, 13, 16]. Thus, a common question remaining unanswered in the literature [20], how much does the tenodesis in remplissage improve outcomes?
Our data suggests that arthroscopic Bankart repair alone did not provide the stabilization necessary to prevent further instability in patients with large Hill-Sachs lesions in the absence of glenoid defects. A failure rate of 57% in patients with isolated arthroscopic Bankart repair is similar to the literature for patients with these defects [1, 3]. The failure rate of 20% for patients undergoing a remplissage in addition to an arthroscopic Bankart is marginally higher than the reported average of 0–15% [5, 12, 13, 20] but is much lower in comparison to our isolated Bankart repair group. Our remplissage with Bankart repair failure prevalence may have been slightly higher because we included subluxations as failures as well. Another interesting result is that among patients who had instability postoperatively, the Bankart repair group had two times as many dislocations and subluxations after the initial failure. This may be due to the fact that the infraspinatus after failure with the remplissage with Bankart repair technique is still partially filling the defect preventing even further dislocations. In a previous study by Park et al., one of the patients who dislocated after remplissage with Bankart repair still showed 75–100% filling of the humeral defect by the infraspinatus despite a previous dislocation, without an intact Bankart repair [10]. Additionally, in patients who failed after isolated arthroscopic Bankart repair, the labral repair may have completely detached once the Hill-Sachs lesion engaged on the anterior glenoid rim making these patients inherently more unstable than the remplissage with Bankart repair failure patients with an intact infraspinatus. While not statistically significant, our remplissage with Bankart repair patients’ postoperative WOSI and DASH scores were 7.9 and 34.7% better than in the group of patients treated with isolated arthroscopic Bankart repair.
We believe we selected a good cohort of recurrent dislocators to assess the clinical role of the remplissage's addition to the Bankart procedure as our patient population had significant humeral head defects with an average volume of 310.22 mm3 in the Bankart repair group and 283.79 mm3 in the remplissage with Bankart repair group. These lesions were measured on high-resolution MRI, verified to be engaging intraoperatively, and were not associated with significant glenoid bone loss. Also, since these patients had an average of over 20 prior dislocations, we can assure ourselves that these cohorts represent a complicated patient group and that their Hill-Sachs lesions played an important role in their preoperative as well as postoperative instability. Finally, by all patients having anterior glenoid defects of less than 20% and an average of 5% or less, the potential for glenoid bone loss to play a confounding role in our interpretation is minimized [18].
In review of the literature, two studies have attempted to control for the infraspinatus tenodesis by studying patients who received arthroscopic Bankart repair or the remplissage with Bankart repair procedure. The first study by Nourissat et al. was a prospective study that examined 15 patients with the remplissage with Bankart repair procedure and 17 with an isolated Bankart repair [9]. They found no difference in dislocation rates between the two groups (6.25%, respectively) nor did they find any difference in postoperative range of motion. Their attempt was not to directly compare the procedures as they did not control for the size of Hill-Sachs lesion and the lesions were not precisely measured on CT or MRI. In addition, they used Instability Severity Index Score (ISIS) to categorize patients for surgery and only did Bankart repair alone on ISIS of less than 4 and for ISIS of greater than 4 they performed a remplissage with Bankart repair procedure. This is not much different from common practice, and they stated the additional two ISIS points ascribed were typically for patients with the presence of a Hill-Sachs lesion on AP radiographs. In doing this, they eliminated a true comparison by having the more stable patients receive Bankart repair alone and patients more prone to dislocate receive the remplissage with Bankart repair procedure.
Another recent article that compared the two procedures was by Franceschi et al., in which the authors retrospectively studied 50 patients with engaging Hill-Sachs lesions, comparing 25 patients receiving isolated arthroscopic Bankart repair and 25 patients who underwent remplissage with Bankart repair [5]. They found 20% of Bankart repair patients had postoperative dislocations or subluxations with no patients from the remplissage with Bankart repair group reporting surgical failure at postoperative follow-up periods of 25.4 and 24.8 months, respectively. While they stated all Hill-Sachs were engaging, the size measurements were done on plain radiographs and by arthroscopy, which offers poor correlation and no quantification of the Hill-Sachs lesion's volume. Workman et al. documented that plain radiographs and arthroscopy offer significantly worse detection and measurement outcomes compared to MRI with regard to humeral head defect measurements [17]. For the arthroscopic scoring, they reported 35 out of 50 patients (70%) had grade II or medium-size lesions; however, Burkhart et al. suggests that the presence of engaging lesion is important but the large engaging Hill-Sachs lesions are the main cause of recurrence [3]. In addition, despite their strong preoperative data, there was no mention of the number of preoperative dislocations, which could have given more insight into the instability of the patients. With such impressively low dislocation rates for both procedures in comparison to the literature, one conclusion is that the patients in that study represented patients with small and less significantly engaging humeral head defects.
Limitations
We understand there are limitations and our study is no exception. Firstly, our retrospective data has its own inherent drawbacks. An additional concern is the comparison of two surgeons and the introduction of performance bias. It is possible there were inherent differences between the two surgeons. As such, this may explain why the outcomes were worse with isolated Bankart repair, rather than a true difference in the surgical procedures. While this is one consideration, it is unlikely as our results are similar to previous studies [2, 5, 9]. Further limitation is the lack of significance in the study, which may be a result of a small sample size. As our power analysis recommended 88 patients, but the study had only 24 patients, we may have improved our results with additional patients. Also, one might assume differences in Hill-Sachs lesion size (p = 0.95) and follow-up (p = 0.12) may have reached statistical significance with a larger population. Despite these concerns, we did select for the largest Hill-Sachs lesions out of 289 patients treated for shoulder instability. With such specific parameters, it limited our ability to obtain a large cohort. Even with this, we demonstrated a increased prevalence of surgical failure with Bankart repair alone and a trend toward improved failure rates with the remplissage procedure (p = 0.10 and p = 0.09, respectively). We believe our results demonstrate the remplissage tenodesis plays a crucial role in stability of the large Hill-Sachs lesions.
In our cohort of patients, in comparison to isolated Bankart repair, arthroscopic Bankart repair with remplissage was a superior option for recurrent instability patients with Hill-Sachs lesions as seen by diminished failure rates and improved outcome scores.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2015_9438_MOESM1_ESM - Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage
Electronic supplementary material, 11420_2015_9438_MOESM1_ESM for Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage by, Garcia Grant H., MD, Park Min Jung, MD, MMSc., Zhang Clare, MD, Kelly John D. IV, MD, Huffman G. Russell, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2015_9438_MOESM2_ESM - Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage
Electronic supplementary material, 11420_2015_9438_MOESM2_ESM for Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage by, Garcia Grant H., MD, Park Min Jung, MD, MMSc., Zhang Clare, MD, Kelly John D. IV, MD, Huffman G. Russell, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2015_9438_MOESM3_ESM - Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage
Electronic supplementary material, 11420_2015_9438_MOESM3_ESM for Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage by, Garcia Grant H., MD, Park Min Jung, MD, MMSc., Zhang Clare, MD, Kelly John D. IV, MD, Huffman G. Russell, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2015_9438_MOESM4_ESM - Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage
Electronic supplementary material, 11420_2015_9438_MOESM4_ESM for Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage by, Garcia Grant H., MD, Park Min Jung, MD, MMSc., Zhang Clare, MD, Kelly John D. IV, MD, Huffman G. Russell, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2015_9438_MOESM5_ESM - Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage
Electronic supplementary material, 11420_2015_9438_MOESM5_ESM for Large Hill-Sachs Lesion: A Comparative Study of Patients Treated with Arthroscopic Bankart Repair with or without Remplissage by, Garcia Grant H., MD, Park Min Jung, MD, MMSc., Zhang Clare, MD, Kelly John D. IV, MD, Huffman G. Russell, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1007/s11420-015-9438-8) contains supplementary material, which is available to authorized users.
Disclosures
Conflict of Interest
Grant H. Garcia, MD, Min Jung Park, MD, MMSc., Clare Zhang, MD, John D. Kelly IV, MD and G. Russell Huffman, MD, MPH, have declared that they have no conflict of interest.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed Consent
Informed consent was obtained from all patients for being included in the study.
Required Author Forms
Disclosure forms provided by the authors are available with online version of the article.
Level of Evidence
Therapeutic Level III