
Abstract
Background
Early detection of surgical site infection (SSI) following spinal surgery would allow for prompt treatment and would improve overall outcome, yet early diagnosis is a challenge. Computed tomography (CT) guided aspiration of fluid collections may aid in diagnosis, as its diagnostic utility has previously been demonstrated in the setting of hip SSI, knee SSI, and spontaneous diskitis. There is no literature on its use in post-operative spinal SSIs.
Questions/Purposes
The current study aims to (1) determine the diagnostic value of CT-guided aspiration in evaluating suspected SSI; (2) identify the characteristics of the clinical presentation that are predictive of SSI; and (3) identify characteristics of the hematologic workup that are predictive of SSI.
Methods
Thirty patients who underwent CT-guided aspiration of paraspinal post-operative fluid collections and culture of aspirate fluid over the 6-year period from 2006 to 2011 were retrospectively reviewed. Aspirate fluid culture results were compared to intraoperative cultures, which were used as the “gold standard” for diagnosing SSI. The diagnostic value was evaluated by determining the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of aspirate fluid cultures. Clinical presentation, patient demographics, comorbidities, and laboratory values were reviewed for association with infection risk.
Results
Eleven of thirty patients undergoing CT-guided aspiration were subsequently confirmed to have SSI through positive cultures. Wound drainage, wound erythema, elevated ESR, and cloudiness of aspirate fluid were associated with SSI. The sensitivity and specificity of aspirate cultures were 36.4 and 89.5%, respectively, and the respective positive predictive value (PPV) and negative predictive value (NPV) were 66.7 and 70.8%.
Conclusions
Cloudy aspirate fluid was highly suggestive of infection, while wound erythema, drainage, and elevated ESR were also suggestive of SSI. CT-guided aspirations are a useful adjunct tool in evaluating for SSI but further studies are necessary before it can be considered a stand-alone diagnostic procedure.
Introduction
Post-operative surgical site infection (SSI) is a devastating problem following spinal surgery and is associated with a worse long-term patient outcome, a large financial burden to the health care system, significant morbidity and even mortality [5, 6, 13–15, 19, 23]. Infection rates range from 0.7% following minor surgical procedures to as high as 10–15% following complex instrumented spinal fusions and revision surgery [5, 6, 13–15, 19, 23]. Obesity, diabetes, smoking, age greater than 60, and history of surgical infection are reported risk factors for SSI [6, 13, 14, 20, 23, 24]. Clinical sequelae of SSI may include delayed post-operative recovery, sensory and/or motor neurological deficit, and the need for additional procedures [12]. However, detecting SSI early remains a clinical challenge and is critical for successful post-operative outcomes [13].
One diagnostic adjunct that can be useful in the post-operative setting in patients suspected of having a SSI is a computed tomography (CT) guided aspiration for percutaneous sampling of fluid collections. The fluid can then be further analyzed with microbiological culture and white blood cell (WBC) count with differential to aid in diagnosis of a SSI. The existing data on the diagnostic value of these tests has come from studies following hip and knee arthroplasty, with elevated WBC count, percentage of polymorphic neutrophils (PMN), and synovial fluid cultures being significant predictors of post-operative periprosthetic joint infections [2–4, 7–9, 11, 16, 18, 21]. A high sensitivity and specificity of CT-guided aspiration for infection has similarly been reported in the setting of spontaneous diskitis [3]. However, extrapolation of these results to SSI in patients having undergone spinal surgery may not be appropriate given the lack of a true joint synovium encompassing the entire post-operative fluid collection. There is no literature on the diagnostic value of CT-guided aspirations in the post-operative spine surgery patient.
The present study analyzes the utility of CT-guided aspiration, microbiologic and visual evaluation of the fluid aspirate, and serum measurements of acute phase reactants in suspected infections following spine surgery. Despite the difference in local environment between total joint arthroplasty and spine surgery, we hypothesize that the underlying infectious pathologies produce similar clinical presentations, and that analyzing these parameters for the diagnosis of SSI in the post-operative spine surgery patient has high sensitivity and specificity. Specifically, the current study aims to (1) assess the predictive value of CT guided aspiration in the confirmed diagnosis of SSI, (2) determine the predictive value of the wound appearance and clinical presentation, and (3) determine the predictive value of the serum tests with the actual occurrence of infection.
Patients and Methods
Following institutional review board review and approval of our study protocol, patients who underwent spine surgery at a single institution over a 6-year period (January 1, 2006 to December 31, 2011) were retrospectively reviewed. An institutional database was queried for patients >18 years old who had CT-guided aspiration in the post-operative period after an index spinal operation. The gold standard used to define infection was positive bacterial growth from operative deep wound cultures obtained during incision and drainage procedures performed subsequent to the CT aspiration. The culture results from aspirate fluid were compared to the operative cultures to determine the diagnostic properties of aspiration fluid cultures. Patients who underwent aspirations but underwent no subsequent debridement surgery were evaluated based on their post-operative clinical history. Those who did not require subsequent operative intervention in the 12 months following their index procedures were deemed to be free of SSI. The decision to order the aspiration was determined by the surgeon's clinical judgment based on the patient presentation.
We identified 30 patients who met inclusion criteria. Demographic and surgical parameters are listed in Table 1. The mean patient age was 57.1 ± 12.2 years (range 39 to 80 years) and the mean BMI was 28.8 ± 7.0 kg/m2 (range 20.2 to 36.8 kg/m2). Although cervical spine surgery was not an exclusion criterion, no cervical spine patients were identified in our search.
Demographic patient data
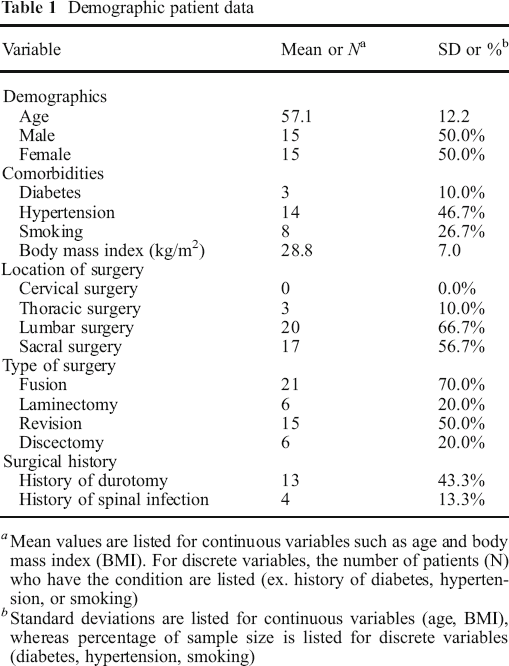
Mean values are listed for continuous variables such as age and body mass index (BMI). For discrete variables, the number of patients (N) who have the condition are listed (ex. history of diabetes, hypertension, or smoking)
Standard deviations are listed for continuous variables (age, BMI), whereas percentage of sample size is listed for discrete variables (diabetes, hypertension, smoking)
Electronic medical records were reviewed for demographic data including age, gender, body mass index (BMI), diabetes, hypertension, and smoking status, as well as additional risk factors, such as history of prior spinal wound infection and history of dural tear. Operative notes were reviewed for type of procedure, anatomic location of the surgery, and pre-operative antibiotic use. Post-operative data included notes on wound maintenance, history of fever, post-operative antibiotic use, as well as hematological data such as WBC count, PMN percentage, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Patients’ operative records following surgery were also reviewed to determine if they required revision or washout procedures.
At the time of index surgery, all patients received standard preoperative prophylactic antibiotic therapy consisting of 2 g of I.V cefazolin or 500 mg of I.V. vancomycin. The same antibiotics were continued in the immediate post-operative period until wound drains were removed for an average of 1.8 days.
The presence of a post-operative fluid collection was confirmed with pre-aspiration imaging in 25/30 patients. Of these, 17 underwent contrast-enhanced magnetic resonance imaging (MRI) and eight underwent CT imaging. The remaining five patients did not have pre-aspiration imaging, but the decision to proceed with aspiration was made based on clinical findings such as wound drainage or localized fluctuance.
Patients underwent CT-guided aspiration at a mean of 45.7 ± 45.5 days (range 6 to 179 days) following their index surgery. All aspirations were performed on lumbosacral post-operative fluid collections in the decompression and/or fusion bed. The volume of fluid obtained ranged from 1–500 cm3. When inadequate volume was obtained for culture, a saline lavage was performed to obtain sufficient fluid. Aspirated fluid was sent for cell count and culture, and the physical properties were assessed for cloudiness and characterized as serous, serosanguinous, or bloody.
Radiographic reports of the CT-guided aspiration were reviewed for volume and appearance of fluid aspirated as well as anatomic location of the fluid collection. Microbiological analysis of aspirate fluid included culture, gram stain, acid-fast stain, and fungal stain. Automated cell count was performed but cytopathology was not. The aspirate workup was compared to operative wound cultures and post-operative clinical history to determine the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the aspiration cultures in diagnosing SSI. Statistical analysis was performed by independent sample t tests and chi-squared tests comparing clinical parameters between patients with confirmed SSI and those without SSI.
Results
The sensitivity and specificity of aspirate cultures in detecting SSI were 36.4% (95% CI 11.2–69.1%) and 89.5% (95% CI 66.8–98.4%), respectively, and the respective PPV and NPV were 66.7 and 70.8% (Table 2). Of the 30 patients identified as having CT-guided aspiration following spinal surgery, 11 had SSI confirmed by the operative cultures (36.7% six male and five female). Of these 11 confirmed infections, eight (73%) were diagnosed approximately 2 to 6 weeks post-operatively. Aspiration cultures correctly diagnosed four (50%) of these infections. Of the remaining three infections that occurred beyond this timeframe, aspirate cultures were falsely negative. The other 19 patients with negative cultures or who did not require post-operative surgical intervention were deemed to be free of infection. Six patients had positive culture of aspirate fluid, and of these patients four were deemed to have confirmed SSI based on the above criteria. Twenty-four patients had negative culture of aspirate fluid, of which seven were deemed to have confirmed SSI. At the time of aspiration, 11 patients were receiving additional intravenous and/or oral antibiotic therapy due to high suspicion of SSI (n = 9) or concurrent urinary tract infection (n = 2). Five of these 11 went on to be diagnosed with SSI as confirmed by operative cultures, and two of these five also had positive aspiration cultures. A strong trend was observed with fluid WBC (17, 215 ± 32, 513 cells/μL SSI vs. 728 ± 962 cells/μL non-SSI; p = 0.06), but no statistically significant difference was noted due to wide data variance. Fluid cloudiness was significantly associated with SSI (p < 0.001): clarity of fluid was 100% (0/19) predictive of lack of infection (Table 3). The most common pathogen found in operative wound cultures was Staphylococcus aureus (Table 4).
Sensitivity, specificity, positive predictive value and negative predictive value of CT-guided aspiration culture
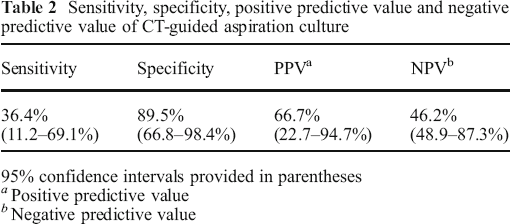
95% confidence intervals provided in parentheses
Positive predictive value
Negative predictive value
Aspirate characteristics
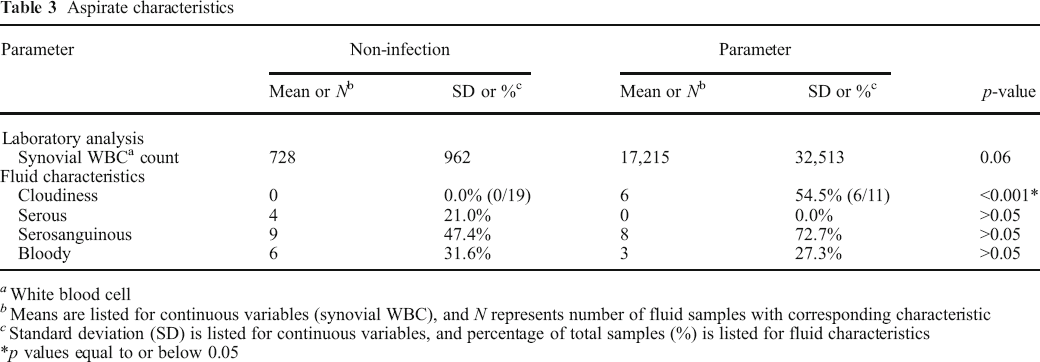
White blood cell
Means are listed for continuous variables (synovial WBC), and N represents number of fluid samples with corresponding characteristic
Standard deviation (SD) is listed for continuous variables, and percentage of total samples (%) is listed for fluid characteristics
*p values equal to or below 0.05
Microbial pathogens detected by deep wound culture
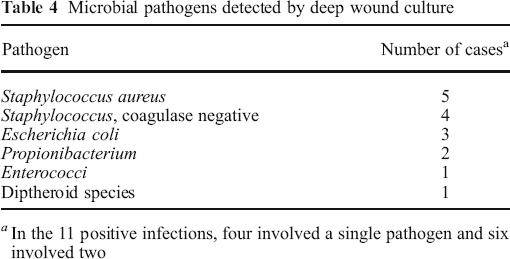
In the 11 positive infections, four involved a single pathogen and six involved two
Wound drainage, erythema, and fever were the most common presenting symptoms raising suspicion for SSI, respectively, seen in 46.7% (14/30), 26.7% (8/30), and 30.0% (9/30) of patients. Two patients presented with all three of these symptoms, nine presented with two, and 12 presented with none. Erythema (p < 0.001) and drainage (p = 0.03) were significantly associated with SSI (Table 5).
Clinical presentation and hematological workup
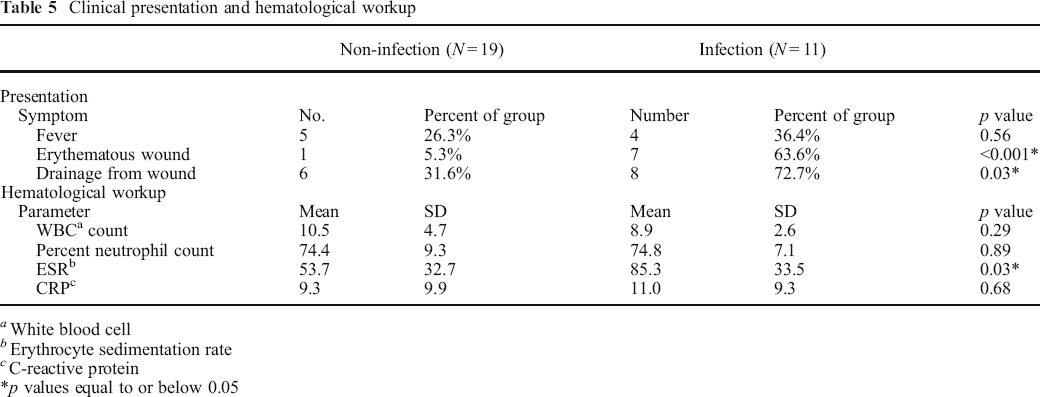
White blood cell
Erythrocyte sedimentation rate
C-reactive protein
p values equal to or below 0.05
The mean WBC count in patients with SSI was 8.9 × 103 cells/μL (σ = 2.6 × 103, range 5.7 × 103–14.2 × 103) compared to 10.5 × 103 cells/μL (σ = 4.7 × 103, range 6.0 × 103–23.3 × 103) in patients without SSI. ESR and CRP levels were obtained at a mean of 35.5 days after index surgery (range 8–167). Patients with SSI had mean ESR and CRP of 85.3 mm/h (σ = 33.5, range 13–123) and 11.3 mg/dL (σ = 9.3, range 0.7–31.8) compared to 53.7 mm/h (σ = 32.7, range 15–117) and 9.3 ± 9.9 mg/dL (0.7 to 30.3) in non-SSI patients. ESR was significantly elevated in patients with SSI compared to those without (p = 0.03), and multivariate regression analysis showed each one-point increase in ESR increased the likelihood of infection by 3%. No significant differences were found with respect to WBC or CRP (Table 5).
Discussion
The goal of this study was to determine the diagnostic utility of CT-guided fluid aspiration characteristics, clinical exam findings, and serum workup in the diagnosis of SSI following spine surgery. Among our 30 patients, aspiration culture results were limited indicators of underlying infection, but cloudy aspirate fluid was highly suggestive of infection. Other clinical parameters such as wound erythema, wound drainage, and elevated ESR were also suggestive of SSI. This is the first report of a consecutive series of post-operative spine surgical patients with a suspected infection to examine the diagnostic utility of post-operative CT-guided fluid aspiration.
Limitations of the present study include the small population of infected patients, which is a limitation to many similar studies. Also, the absence of confirmatory operative cultures for all patients is another limitation. However, patients who did not have post-operative surgical intervention were categorized as non-SSI as it is unlikely that any patient with persistent concern for SSI after aspiration workup would not undergo definitive irrigation and debridement. Losing patients to follow-up in the immediate timeframe following aspiration is less likely given the acuity of the workup but is an inherent limitation to the retrospective design. The temporal variability at which the laboratory tests were obtained further limits the analysis, as post-operative elevations in ESR and CRP have been shown to decline in a time-dependent manner following surgery [20]. The concurrent use of antibiotics in 11 patients may have altered the trend in ESR and CRP as well as the rate of culture-positivity in aspirate samples and surgical specimens. The generalizability of our results to post-operative patients with a low-index of suspicion for infection is limited, given that all patients in the present cohort had a clinical suspicion of an SSI and therefore a higher pre-test probability of infection. For example, patients with a seroma in the operative bed visualized on post-operative MRI obtained for other clinical indications are often not selected for further workup with CT-guided aspiration. Furthermore, since patients with more significant and definitive infections are more likely to return to the OR for prompt treatment rather than undergo a diagnostic test, they could not be included in the study.
Prior data on the diagnostic yield for CT-guided aspiration in detecting infection from hip and knee arthroplasty studies has consistently shown specificity greater than 94% [2–4, 7, 9, 16, 18, 21]. Sensitivity reports have been more controversial, ranging from 55–93%, which suggests a clinical uncertainty in the ability of aspiration cultures to detect post-operative infections [2–4, 7, 9, 16, 18, 21]. The post-operative spine surgical bed with the adjacent paraspinal muscle, bone, ligamentous and facet capsular tissue, dura, and neural elements creates a biochemical and structural milieu that is quite distinct from the diarthrodial knee and hip joints, which makes these previous results unlikely to extrapolate to the spine.
In a study specific to the spine, Chew and Kline evaluated the role of CT-guided aspiration in diagnosing spontaneous spinal infections. They found an overall high diagnostic yield, reporting a sensitivity of 91%, specificity of 100%, PPV of 100%, and NPV of 94% [3]. Although their study examined patients who were not in the post-operative setting, the high diagnostic values demonstrate the potential for aspirate fluid cultures to evaluate spinal infections. However, these results cannot be extrapolated to diagnosing SSI because a normal healing inflammatory response and the potential for sterile seromas creates distinct clinical environment.
By design our study focused on the post-operative spine and the utility of aspiration cultures in diagnosing SSI among a group of patients with a post-operative fluid collection and concern for infection. We found cultures to have high specificity (89.5%) and moderate PPV (66.7%) with low sensitivity (36.4%) and NPV (46.2%). These findings are consistent with data from arthroplasty studies and suggest that the procedure may be used as a confirmatory tool in diagnosing SSI and guiding patient management. The low sensitivity and NPV, however, suggest that CT-guided aspiration culture results on their own may be inadequate to effectively rule out a post-operative SSI, especially in patients already on antibiotics.
The diagnostic value of CT aspirations may vary depending on the timeframe in which they are performed. The majority of the 11 infections (73%) occurred within 6 weeks of index surgery. When analyzing only the 15 aspirations occurring within the 6-week postoperative timeframe, the sensitivity was 50% (4/8) and specificity was 71% (5/7). Aspiration cultures were unable to detect any of the three infections occurring beyond 6 weeks, which may suggest that CT-guided aspirations have the highest clinical utility in the acute to sub-acute setting. When there is concern for infection beyond 2 months, the test may have limited diagnostic value. When infection delayed infection is suspected, the patient may benefit instead from proceeding directly towards surgery.
Beyond aspiration culture results, our study evaluated supplementary clinical data in diagnosing SSI. The physical exam yielded valuable clinical information, as both wound erythema and drainage were associated with infection (p < 0.001, p = 0.03, respectively). Furthermore, the appearance of the fluid aspirate itself was a useful indicator of SSI, with cloudy fluid being significantly associated with SSI (p < 0.001). Evaluating the aspiration results in addition to considering the clinical signs and evaluating the fluid properties itself increase the diagnostic value of CT-guided aspiration.
Other clinical parameters used to detect infection include hematologic markers such as ESR and CRP, which increase in states of inflammation and tissue injury. ESR and CRP are often elevated in the immediate post-operative period, but marked or persistent elevation may also be indicative of a post-operative infection [1, 10, 12, 17]. In our study, ESR levels were significantly higher in patients with SSI compared to those without (p = 0.03). Multivariate analysis also showed a 3% increased likelihood of infection with each one-point rise in ESR, which suggests that extreme elevations are highly suspicious of infectious processes. No statistical difference was seen with CRP, which may be attributed to the small sample size or the wide post-operative timeframe during which the tests were performed (mean 35.5 days after index surgery; range 8–167 days). Nonetheless, hematologic markers, particularly ESR, aid in the diagnosis of SSI.
In patients with moderately elevated pretest probabilities of having SSI, aspirations may be a useful tool to “rule-in” infection. Fluid clarity may be an intriguing way to exclude infection, particularly in the setting of negative cultures when obtained in the immediate post-operative timeframe, and may prevent the need for unnecessary surgical exploration. However, these findings alone do not clearly “rule-out” infection, and the diagnostic yield may decrease over time. Other biologic testing for infection status, such as assays for alpha-defensin or bacterial DNA, may substantially increase the future value of fluid analysis from the post-operative spine patient [22]. Currently, CT-guided aspirations are a useful adjunct tool in evaluating for SSI but further studies are warranted before it can be considered a stand-alone diagnostic procedure.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM1_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM1_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM2_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM2_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM3_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM3_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM4_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM4_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM5_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM5_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2016_9490_MOESM6_ESM - Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections
Electronic supplementary material, 11420_2016_9490_MOESM6_ESM for Evaluating the Diagnostic Yield of Computed Tomography-Guided Aspirations in Suspected Post-operative Spine Infections by, Jo Jonathan E., MD, Miller Andy O., MD, Cohn Matthew R., BS, Nemani Venu M., MD, Schneider Robert, MD, Lebl Darren R., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1007/s11420-016-9490-z) contains supplementary material, which is available to authorized users.
Compliance with Ethical Standards
Conflict of Interest
Jonathan E. Jo, MD, Andy O. Miller MD, Matthew R. Cohn, BS, Venu M. Nemani MD and Robert Schneider, MD have declared that they have no conflict of interest. Darren R. Lebl, MD reports other from Medtronic, K2M and Cohen and Company, outside the work.
Human/Animal Rights
Informed Consent
Informed consent was obtained from all patients for being included in the study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.