
Abstract
Background
Humeral head avascular necrosis (AVN) of differing etiologies may lead to shoulder arthroplasty due to subchondral bone collapse and deformity of the articular surface. There have been no large studies evaluating the complications for these patients after they undergo total shoulder arthroplasty (TSA).
Questions/Purposes
The first objective of this study is to evaluate the complication rate after TSA in patients with humeral head AVN. The secondary objective is to compare the complication rates among the different etiologies of the AVN.
Methods
Patients who underwent TSA were identified in the PearlDiver database using ICD-9 codes. Patients who underwent shoulder arthroplasty for humeral head AVN were identified using ICD-9 codes and were subclassified according to AVN etiology (posttraumatic, alcohol use, chronic steroid use, and idiopathic). Complications evaluated included postoperative infection within 6 months, dislocation within 1 year, revision shoulder arthroplasty up to 8 years postoperatively, shoulder stiffness within 1 year, and periprosthetic fracture within 1 year and systemic complications within 3 months. Postoperative complication rates were compared to controls.
Results
The study cohorts included 4129 TSA patients with AVN with 141, 778 control TSA patients. Patients with posttraumatic AVN were significantly more likely to have a postoperative infection (OR 2.47, P < 0.001), dislocation (OR 1.45, P = 0.029), revision surgery (OR 1.53, P = 0.001), stiffness (OR 1.24, P = 0.042), and systemic complication (OR 1.49, P < 0.001). Steroid-associated AVN was associated with a significantly increased risk for a postoperative infection (OR 1.72, P = 0.004), revision surgery (OR 1.33, P = 0.040), fracture (OR 2.76, P = 0.002), and systemic complication (OR 1.59, P < 0.001). Idiopathic and alcohol-associated AVN were not significantly associated with any of the postoperative evaluated complications.
Conclusions
TSA in patients with humeral head AVN is associated with significantly increased rates of numerous postoperative complications compared to patients without a diagnosis of AVN, including infection, dislocation, revision arthroplasty, stiffness, periprosthetic fracture, and medical complications. Specifically, AVN due to steroid use or from a posttraumatic cause appears to be associated with the statistically highest rates of postoperative TSA complications. Given these findings, orthopedic surgeons should be increasingly aware of this association, which should influence the shared decision-making process of undergoing TSA in patients with humeral head AVN.
Introduction
Humeral head avascular necrosis (AVN) can be a disabling condition causing significant pain, decreased range of motion, and loss of shoulder function. Approximately 7% of AVN in the body occurs in the humeral head, second only to the femoral head in terms of frequency of involvement, and most patients with humeral head AVN have concomitant femoral head involvement [6, 7, 24]. Approximately 5% of shoulder arthroplasties are performed for a primary diagnosis of humeral head AVN [9].
The AVN disease process is multifactorial, and, while some debate exists regarding the specific processes involved, the underlying common pathway is compromised blood flow to the humeral head eventually resulting in death of the subchondral bone [32]. The diminished blood flow can be caused directly by disrupted arterial inflow or indirectly as the result of either venous congestion or local alterations in fat metabolism and adipocyte size, both leading to increased intra-osseous pressure and microvascular compromise [7, 8]. As the disease progresses, loss of the subchondral support can lead to microfracture and collapse, jeopardizing the overlying chondral tissue and changing the geometry of the articular surface. This leads to altered biomechanics and areas of focally increased contact pressures both of which further contribute to cartilage degeneration [27].
Etiologies which initiate this process of altered blood flow include trauma, corticosteroid use, hemoglobinopathies such as sickle cell disease, alcohol use, systemic diseases such as systemic lupus erythematosus, and idiopathic causes [7, 16, 21, 24, 29, 31, 34]. Corticosteroid-associated AVN is the most common non-traumatic etiology [16, 17, 21].
Treatment of humeral head AVN varies depending on disease stage. Mainstay non-operative modalities for early-stage disease are aimed primarily at alleviating symptoms and include NSAIDs, risk factor modification, and physiotherapy. Other medications intended to target various pathophysiologic mechanisms of the disease such as vasodilators, lipid-lowering agents, anticoagulants, and bisphosphonates are largely theoretical, and limited evidence exists to support their use for humeral head AVN. Limited arthroscopic debridement and/or core decompression may be an option for select patients in early disease states. Resurfacing techniques have been described, but limited data exists regarding long-term outcomes [20, 31, 38]. In more advanced stages with humeral head collapse and significant bipolar arthritis, total shoulder arthroplasty (TSA) remains the mainstay treatment option.
Literature evaluating shoulder arthroplasty for humeral head AVN is relatively sparse and is fraught with inconsistency, conflicting definitions, and wide variations in reported data. Satisfactory patient-reported outcomes following arthroplasty for humeral head AVN range from 25 to 94%, and complication rates range from 0 to 32% [15, 22, 27, 34]. Most series exclusively evaluating arthroplasty outcomes in patients with humeral head AVN involve a small number of subjects and often combine varying etiologies of AVN and arthroplasty types [22, 27, 29]. The purpose of the present study is to utilize a national database to evaluate and compare complications after TSA in patients with humeral head AVN and to contrast differences in complication rates based on the etiology of AVN.
Patients and Methods
Data for the present study was derived from a for-fee database of patients, the PearlDiver Patient Records Database (www.pearldiverinc.com; PearlDiver Inc., Fort Wayne, Indiana). The database contains procedure volumes and demographics for patients with International Classification of Diseases, 9th Revision (ICD-9) diagnoses and procedures or Current Procedural Terminology (CPT) codes. Data for the present study was derived from the 100% Standard Analytic Files Medicare database within the PearlDiver records, which has over 100 million individual patient records from 2005 to 2012. Access to the database was granted by PearlDiver Technologies for the purpose of academic research. The database was stored on a password-protected server maintained by PearlDiver.
Patients who underwent TSA from 2005 to 2012 were identified using ICD-9 procedure codes and CPT codes, including conventional and reverse total shoulder arthroplasty (ICD-9s 81.80, 81.88 and CPT 23472). Patients who underwent TSA for shoulder avascular necrosis (AVN) were identified using ICD-9 code 733.41 (aseptic necrosis of head of humerus). These patients who underwent TSA for AVN were then further subdivided into the following cohorts according to the etiology of the AVN using ICD-9 codes, including (1) posttraumatic (ICD-9s 812.00–03, 812.09); (2) alcohol use (ICD-9s 303, 303.90–93, 305.00–03); (3) chronic steroid use (ICD-9s V58.65, V87.45, E93.20); and other/idiopathic (patients without ICD-9 codes specified for groups 1–3). Control groups were also created, which included all patients with the aforementioned CPT/ICD-9 codes for TSA without a diagnosis of AVN.
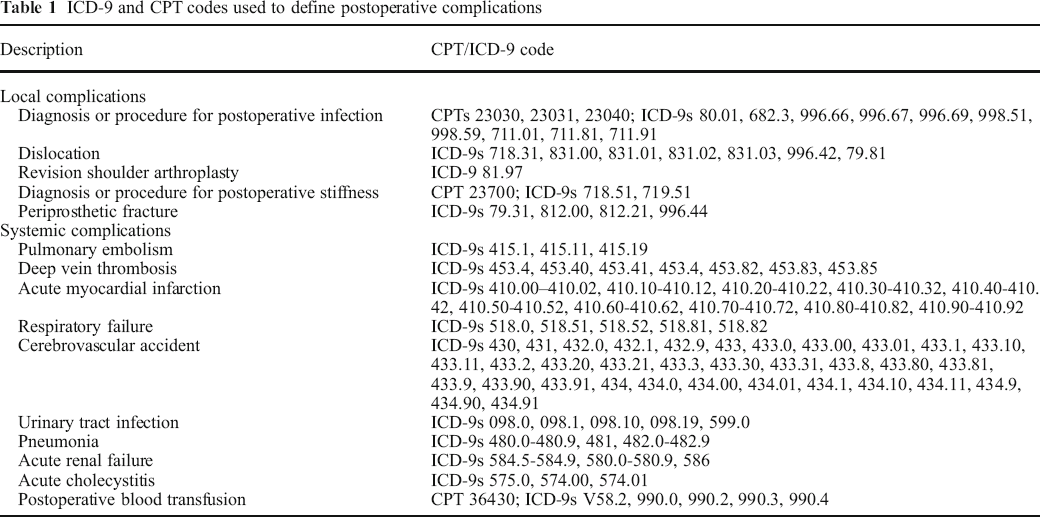
Patients in each cohort were queried for basic demographics and comorbidities including sex, age (<65, 65–80, >80 years), obesity, diabetes mellitus, and smoking status. Each cohort was then queried for postoperative complications following the surgical procedure utilizing ICD-9 and CPT codes for postoperative infection within 6 months, dislocation within 1 year, revision shoulder arthroplasty up to 8 years postoperatively, shoulder stiffness within 1 year, and periprosthetic fracture within 1 year and systemic complications within 3 months (Table 1).
ICD-9 and CPT codes used to define postoperative complications
A binomial multivariate logistic regression analysis was employed to evaluate the independent effect of AVN on postoperative complications. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each comparison between study cohorts and controls. This regression controlled for patient demographics (age, sex, BMI, tobacco use, alcohol abuse) and comorbidities (inflammatory arthritis, depression, hypercoagulable state, diabetes mellitus, hyperlipidemia, hypertension, peripheral vascular disease, congestive heart failure, coronary heart disease, chronic kidney disease, current dialysis use, chronic lung disease, chronic liver disease, and hypothyroidism). Forest plots were constructed from the regression data. P < 0.05 was considered statistically significant.
Results
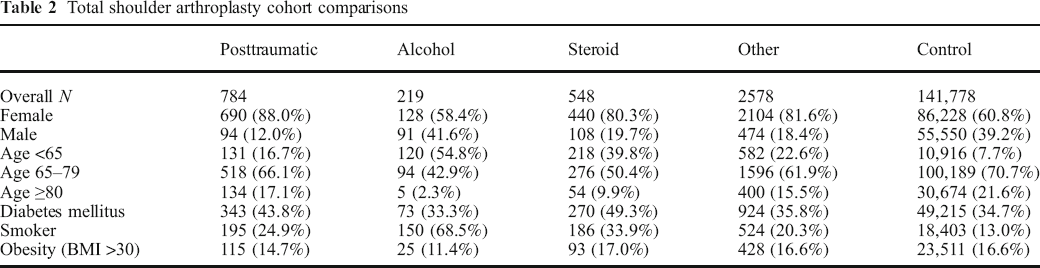
The final study cohort included 4129 TSA patients with shoulder AVN and 141, 778 controls. A comparison of demographics and medical comorbidities is provided in Table 2. While there were differences noted in demographics and comorbidities, these were controlled for in the logistic regression analysis.
Total shoulder arthroplasty cohort comparisons
Complications after TSA in patients with AVN were more common than in controls (Table 3 with statistical comparisons presented in Fig. 1a–f). Infection was significantly more common in patients with posttraumatic AVN (OR 2.5, P < 0.0001) and steroid-related AVN (OR 1.7, P = 0.004) compared to controls (Fig. 1a). Dislocation was more common in patients with posttraumatic AVN compared to controls (OR 1.5, P = 0.03) (Fig. 1b).
Complication rates after total shoulder arthroplasty for avascular necrosis
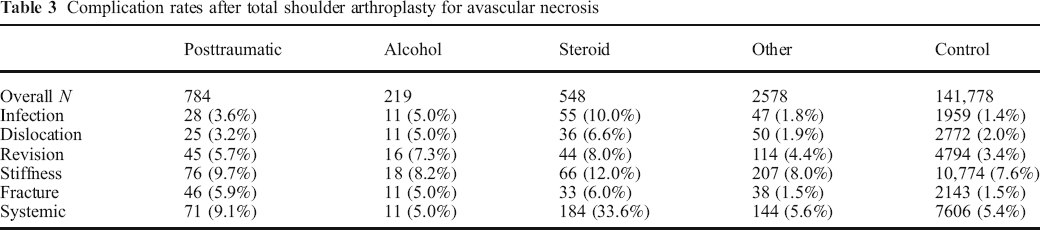
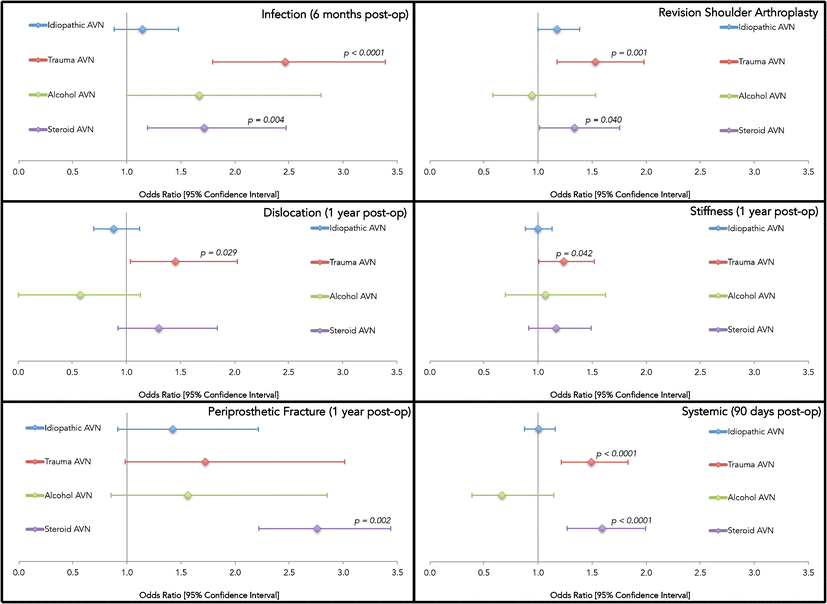
Revision shoulder arthroplasty was significantly more common in patients with posttraumatic AVN (OR 1.5, P = 0.001) and steroid AVN (OR 1.3, P = 0.04) compared to controls (Fig. 1c). A diagnosis of postoperative stiffness was significantly more common in patients with posttraumatic AVN (OR 1.2, P = 0.04) compared to controls (Fig. 1d). Postoperative fracture was more common in patients with steroid AVN (OR 2.8, P = 0.002) and approached statistical significance for patients with idiopathic and posttraumatic AVN (Fig. 1e). Systemic complications were significantly more common in patients with posttraumatic AVN (OR 1.5, P = 0.0001) and steroid AVN (OR 1.6, P < 0.0001) compared to controls (Fig. 1f).
Discussion
The present study demonstrates significantly increased rates of complications after total shoulder arthroplasty in patients with AVN of the humeral head compared to patients without a diagnosis of humeral head AVN. The rate of complications varied based on etiology of the AVN, with the highest rates of complications noted in patients with steroid-associated and posttraumatic AVN. Patients with AVN related to alcohol use and from idiopathic causes had statistically similar rates of complications compared to controls.
This study has several limitations that require mention. Many of the limitations of our study are inherent to all studies utilizing large administrative databases such as PearlDiver. The power of the analysis is dependent on the quality of the available data, which includes accuracy of billing codes and miscoding or non-coding by physicians all as potential sources of error. While we attempted to accurately represent a large population of interest by using this database, we cannot assure that the database represents a true cross section of the USA, as only Medicare data was included in the analysis. Another limitation is that no additional information is available regarding the details of the etiology of the avascular necrosis (e.g., duration of steroid usage or details of the trauma to the humeral head). However, due to the rarity of shoulder arthroplasty after humeral head AVN, utilization of a database like PearlDiver provides a powerful method for evaluating complications despite the limitations of such a method.
Numerous studies have demonstrated the reliability and efficacy of total shoulder arthroplasty for osteoarthritis, rheumatoid arthritis, rotator cuff arthropathy, and posttraumatic arthritis [26, 39]. AVN of the humeral head remains a relatively uncommon cause of shoulder arthritis and accounts for approximately 5% of all shoulder arthroplasties performed [15]. The most common causes of humeral head AVN are chronic corticosteroid use and trauma [16, 17]. Studies investigating the results and complications of TSA specifically in the osteonecrotic shoulder are limited to small, retrospective case series that often group TSA, hemiarthroplasty, and the various etiologies of AVN [17, 19, 22, 27, 29]. While many of these studies have demonstrated the ability of arthroplasty to improve pain, function, and range of motion in patients with AVN, postoperative complication rates have varied among the many etiologies of humeral head AVN [17, 19, 27, 29].
TSA for AVN has been the subject of several studies primarily focusing on functional outcomes and implant longevity. In the largest published series, Hattrup and Cofield reviewed 127 shoulders, 56 TSA, and 71 humeral head replacements, treated with arthroplasty for AVN of the humeral head [17]. Postoperatively, they reported seven (5.5%) cases of instability, two (1.6%) fractures, and one (0.8%) infection. Two shoulders (1.6%) required revision surgery, and two others required a manipulation under anesthesia due to stiffness. The authors found an overall higher complication rate in the posttraumatic AVN group as compared to steroid use and other causes [17]. The present study evaluated almost 4000 TSA performed for AVN and found that patients with posttraumatic AVN had the highest odds ratios for infection, dislocation, revision shoulder arthroplasty, and stiffness. Steroid-associated AVN had the highest odds ratios for postoperative fracture and systemic complications.
Modern published rates of infection following TSA are reported to be between 0 and 4% [5, 10, 28, 35, 36]. While rare, this devastating complication exposes the patient to the increased morbidity of subsequent surgery in addition to the high failure rate and poor outcomes following revision surgery [4]. While most infections occur in the setting of immunosuppression secondary to host factors, systemic corticosteroid therapy has been demonstrated to increase infection risk following TSA [3]. Little data is available on the incidence of postoperative infection following TSA in patients with humeral head AVN. Hattrup and Cofield reported a 0.8% rate of postoperative infection in their series of 127 TSAs and shoulder HAs [17]. Only one other case of postoperative infection was reported in four other studies reviewed that included more than 60 shoulder arthroplasties for AVN [15, 27, 29]. We found that TSA for AVN due to trauma was associated with an odds ratio of 2.47 of experiencing a postoperative infection compared to controls. Patients with alcohol-associated AVN had a threefold increase (5.0%), and steroid-associated AVN had a sevenfold increase (10.0%) in rates of postoperative infection compared to controls. Control TSA in the present study had a postoperative infection rate of 1.4%, similar to values reported in prior studies.
TSA alters the complex dynamic stabilizers of the native shoulder, making soft tissue tensioning and implant placement essential in preventing dislocation. One review indicated that instability is the second leading complication associated with TSA, with a prevalence of 4% in 3081 TSA, which accounted for 30% of all complications [3]. A recent database study reported a 0.3% dislocation rate within 90 days following TSA, which accounted for more than 5% of 90-day readmissions [33]. Hattrup and Cofield reported 7 (5.5%) cases of instability in 127 patients who underwent arthroplasty for AVN; however, they did not specify whether these occurred in patients who had undergone TSA or hemiarthroplasty [17]. In the current study, a similar rate of dislocation was noted in the steroid and alcohol cohorts (6.6 and 5.0%, respectively). These were both more than double the incidence of instability in the idiopathic and control groups.
Modern revision arthroplasty rates following TSA have been reported to be between 0 and 5.6% [2, 12]. Risk factors such as poor glenoid bone stock, rotator cuff deficiency, and sex have been shown to decrease implant longevity [23, 30]. While AVN has been cited as a risk factor for revision surgery in the total hip arthroplasty literature, the association with TSA has not been evaluated [37]. Hattrup and Cofield reported that 2 of 127 shoulders (1.5%) required revision surgery following arthroplasty for AVN [17]. Parsch et al. prospectively evaluated 13 shoulders treated with arthroplasty for humeral head AVN with one (7.7%) requiring revision surgery for aseptic loosening [29]. The highest revision rate following arthroplasty for AVN has been reported by Feeley et al. who retrospectively compared 37 hemiarthroplasties and 27 TSA for AVN of the humeral head from various etiologies [15]. Two (5%) revisions occurred in the hemiarthroplasty group for excessive glenoid wear and five (18.5%) revisions in the TSA group for aseptic loosening. At 8 years postoperatively, this data demonstrated that the steroid-associated cohort experienced a revision rate of 8.0%. This is more than double that seen in the control group, and higher than the incidence of revision in all other AVN groups. In addition, the incidence of revision for posttraumatic and alcohol-related causes of AVN was significantly higher than both the idiopathic AVN and control TSA groups.
Stiffness following TSA can lead to significant patient dissatisfaction and require additional surgery to regain range of motion [11]. The reported incidence of stiffness following TSA has varied greatly. Neer first described stiffness as one of the most common causes of failure following TSA [25]. In a study that included 51 TSA for OA, Hasan et al. reported stiffness as the leading cause of failure in 69% of patients [16]. However, more recent studies have reported significantly lower rates ranging between 0 and 0.8% [11, 14]. Very little published data exists describing stiffness after TSA for humeral head AVN, with only one study reporting two (1.6%) cases of postoperative stiffness [17]. A 12% rate of postoperative stiffness in patients undergoing TSA for steroid-associated AVN was noted from the study; however, only the rate of stiffness related to trauma (9.7%) reached statistical significance.
The reported incidence of periprosthetic fracture following TSA ranges between 1.5 and 3%, which is in agreement with the control TSA cohort in this study [3, 18]. Established risk factors include osteopenia, osteolysis, and eccentric reaming during arthroplasty [13]. While Hattrup reported 2 (1.6%) fractures in 127 shoulder arthroplasties for AVN, several other studies have reported no periprosthetic fractures following TSA for AVN [17, 22, 27, 29]. From this study, the periprosthetic fracture incidence in the steroid-associated AVN group was four times that of both the idiopathic AVN and control groups, which may not be surprising due to the well-known association between corticosteroid use and subsequent osteopenia [1]. In addition, the periprosthetic fracture rates in the posttraumatic and alcohol AVN groups were also more than three times that of the idiopathic and control groups.
TSA is generally regarded as a low-risk, elective procedure associated with low systemic postoperative complication rates [33]. A recent database studied reported an overall 90-day readmission rate of 6% following TSA, which was significantly lower than both reverse TSA and hemiarthroplasty [33]. Eighty-two percent of all readmissions were due to medical complications such as deep vein thrombosis, pulmonary embolism, and pneumonia [33]. In the broader arthroplasty literature, a recent study demonstrated that patients undergoing total hip arthroplasty for AVN of the femoral head had significantly increased rates of certain medical complications than those who underwent the same procedure without AVN [40]. Any association between AVN and systemic complications following TSA has not previously been evaluated. The systemic complication rate in the current study is more than six times greater for patients undergoing TSA for steroid-associated AVN as compared to the idiopathic AVN and control TSA. The posttraumatic AVN group demonstrated a complication rate nearly double the idiopathic and control groups while the alcohol-associated AVN group did not differ from the idiopathic and control groups.
Total shoulder arthroplasty in patients with AVN of the humeral head is associated with significantly increased rates of numerous postoperative complications compared to patients without a diagnosis of humeral head AVN, including infection, dislocation, revision arthroplasty, stiffness, periprosthetic fracture, and medical complications. The rate of complications varied based on etiology of the AVN, with the highest rates of complications noted in patients with steroid-associated and posttraumatic AVN. Patients with AVN from etiologies other than steroids, trauma, or alcohol had statistically similar rates of complications compared to controls.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM1_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis is Associated with Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM1_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM2_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM2_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM3_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM3_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM4_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM4_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM5_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM5_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2017_9562_MOESM6_ESM - Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications
Electronic supplementary material, 11420_2017_9562_MOESM6_ESM for Shoulder Arthroplasty for Humeral Head Avascular Necrosis Is Associated With Increased Postoperative Complications by, Tyrrell Burrus M., MD, Cancienne Jourdan M., MD, Boatright Jeffrey D., MD, MS, Yang Scott, MD, Brockmeier Stephen F., MD, Werner Brian C., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1007/s11420-017-9562-8) contains supplementary material, which is available to authorized users.
Compliance with Ethical Standards
Conflict of Interest
M. Tyrrell Burrus, MD, Jourdan M. Cancienne, MD, Jeffrey D. Boatright, MD, MS, Scott Yang, MD, Stephen F. Brockmeier, MD, and Brian C. Werner, MD, have declared that they have no conflict of interest.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed Consent
Informed consent was waived from all patients for being included in the study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.