
Abstract
Background
Operative indications for supination-external rotation (SER) ankle fractures depend on the integrity of the medial structures. Despite the importance of assessing deep deltoid ligament injuries, the accuracy of common diagnostic tests has not been established.
Questions/Purposes
The objective of this study was to compare the ability of injury (non-stress) and stress radiographs and magnetic resonance imaging (MRI) to diagnose deep deltoid ligament ruptures in operative SER ankle fractures.
Methods
Patients were included who underwent surgical fixation of SER ankle fractures and had appropriate injury and manual stress test radiographs, pre-operative ankle MRI, and intra-operative assessment of deep deltoid integrity by direct visualization. The medial clear space (MCS) was considered positive for all values over 5 mm on the injury or stress mortise radiographs. MRI analysis of the deep deltoid ligament injury was performed by blinded fellowship-trained musculoskeletal radiologists. Intra-operative direct visualization and assessment of the deltoid was performed using a direct medial ankle approach at the time of operative fracture fixation.
Results
Using intra-operative visualization as the gold standard, MCS measurements and MRI had differing abilities to diagnose a deep deltoid rupture. In cases where the MCS was less than 5 mm on injury radiographs and stress tests were performed, MCS measurements were much less accurate than MRI in predicting deltoid ruptures (46% versus 79%, respectively) with a high false positive rate (80%). In contrast, an MCS measurement of greater than 5 mm on injury radiographs was a strong predictor of deep deltoid rupture (accuracy of 95%).
Conclusion
Compared with direct visualization of the deltoid ligament intra-operatively, these data support proceeding with surgery when the MCS on injury radiographs is greater than 5 mm without any additional stress tests or advanced imaging. When the MCS is less than 5 mm, we recommend MRI analysis because of its increased accuracy and decreased false positive rate. Improving our ability to diagnose deltoid ruptures will contribute to more effective management of patients with SER ankle fractures.
Keywords
Introduction
The supination-external rotation (SER) ankle fracture as described by Lauge-Hansen is the most frequent pattern of rotational ankle fracture [25, 32, 33, 51]. Surgical treatment of SER ankle fractures depends on the stability of the ankle mortise. SER stage II ankle fractures consist of a lateral malleolus fracture without a medial-sided injury and can be managed effectively with non-operative treatment [1, 2, 4, 24, 31, 32, 42, 52]. In contrast, SER stage IV injuries have a lateral malleolus fracture with either a medial malleolus fracture or deep deltoid rupture. The additional medial injury creates an unstable ankle mortise and warrants operative fixation to restore the congruency and stability of the ankle joint [1, 2, 9, 23, 40, 41, 44, 45, 49, 53]. Unfortunately, no consensus exists for objective criteria for diagnosing an unstable ankle mortise with these injuries [16, 27, 30, 47].
The deltoid ligament is composed of deep and superficial components, and the deep deltoid ligament functions as the primary medial stabilizer by limiting external rotation of the talus [3, 5, 12, 35, 37, 38, 43, 46]. In the absence of a medial malleolus fracture, determining whether an isolated lateral malleolus fracture is associated with a deep deltoid rupture dictates whether to pursue conservative or operative treatment. Because of this, much attention has been spent on methods for diagnosing deltoid ruptures [6–8, 10, 11, 14, 15, 17–21, 34, 36, 39, 47, 49, 50]. The most common method to assess for a deltoid rupture with a lateral malleolus fracture has been a mortise radiograph with an external rotation stress test [13, 20, 23, 29, 34, 36, 39, 47, 49]. Recently, magnetic resonance imaging (MRI) has also been used to determine the status of the deltoid ligament in ankle fractures [7, 8, 19, 36]. While several studies have compared these two methods for detecting deltoid ruptures [7, 19, 21, 36, 47], they lacked a non-radiographic gold standard for meaningful comparison. Using a prospective cohort of SER ankle fracture patients who underwent surgical exploration of the medial ankle for potential repair of the deep deltoid, we aimed to compare mortise radiographs and MRI for diagnosing a deep deltoid rupture.
Materials and Methods
Following approval by our institutional review board, patients with operatively treated ankle fractures by a single surgeon between 2010 and 2015 were prospectively included in the study. Inclusion criteria consisted of skeletally mature patients with an SER fracture pattern, injury (non-stress) ankle mortise radiographs, manual stress exam radiographs if the medial clear space (MCS) on injury radiographs was less than 5 mm, pre-operative ankle MRI within 1 week of the injury, and operative exploration of the medial ankle joint with documentation of the status of the deep deltoid ligament. Patients with medial malleolus fractures were excluded. An SER fracture pattern was defined as an oblique lateral malleolus fracture near the level of the tibiotalar joint extending from anterior–inferior to posterior–superior [26]. All patients with an MCS of 5 mm or less on injury mortise radiograph had a stress exam. External rotation manual stress radiographs were performed by on-call orthopedic residents trained in the technique. MCS measurements were performed by an independent orthopedic surgeon, blinded to the MRI and clinical findings, using Centricity™ Enterprise Web Picture Archiving and Communications System (GE Healthcare, Little Chalfont, Buckinghamshire, UK). The MCS was measured at the level of the talar dome using a horizontal line from the medial articular surface of the talus to the lateral articular surface of the medial malleolus [47].
Ankle MRI studies were performed on a 1.5 or 3.0 Tesla unit (Signa Horizon LX version HD23 or Discovery 750W version DV25, GE Medical Systems, Milwaukee, WI, USA) using a dedicated extremity coil. Two fellowship-trained attending musculoskeletal radiologists who were unaware of the clinical findings independently analyzed all ankle MRIs to determine the status of the deep deltoid ligament. Complete ligament tears were considered ruptured; partial tears were considered intact. Discrepancies in MRI readings were settled by a third attending radiologist to create a consensus outcome measurement.
Patients with SER ankle fractures were indicated for surgery if they had an MCS of 5 mm or more on the injury or stress mortise radiograph or a preliminary MRI demonstrating a complete deep deltoid rupture. All patients included in the study underwent a medial approach by a single surgeon (D.L.) with intent to repair a ruptured deep deltoid and restore medial ankle stability [22, 28, 48]. During this medial approach, the deep deltoid ligament was examined and its status documented in the operative report as either completely ruptured or intact. Ruptured deep deltoids underwent an anatomic repair using a 5-mm suture anchor (DePuy Mitek, Raynham, MA, USA).
Data was analyzed using SAS Software, version 9.3 (SAS Institute, Inc., Cary, NC, USA). Continuous variables were reported using means and standard deviations, and frequencies were used to describe count variables. Inter-rater reliability for MRI diagnosis was tested using the intra-class correlation coefficient version (2.1).
Results
Seventy-nine patients met the inclusion and exclusion criteria. Forty-five (57%) were male, and the average age was 44 years (range, 15 to 87 years).
Twenty-seven patients (34%) had an MCS measurement of less than 5 mm on injury (non-stress) radiographs and underwent manual stress exams. Of these patients, 10 had an MCS of less than 5 mm on the manual stress radiographs. The remaining 52 patients (66%) had an MCS of greater than 5 mm on the injury radiographs and did not require manual stress exams, giving a total of 69 patients (87%) diagnosed with a deltoid rupture based on injury or stress MCS measurements (Table 1). Fifty-eight patients (73%) were diagnosed with a deltoid rupture by the consensus MRI analysis. The agreement between the musculoskeletal attending radiologists was fair: 75% agreement, corresponding to a κ statistic of 0.36.
Summary of the deltoid ligament status based on intra-operative assessment, magnetic resonance imaging readings, and medial clear space analysis
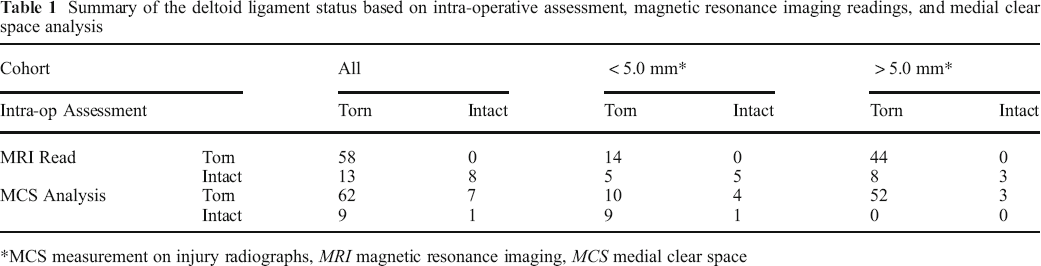
MCS measurement on injury radiographs, MRI magnetic resonance imaging, MCS medial clear space
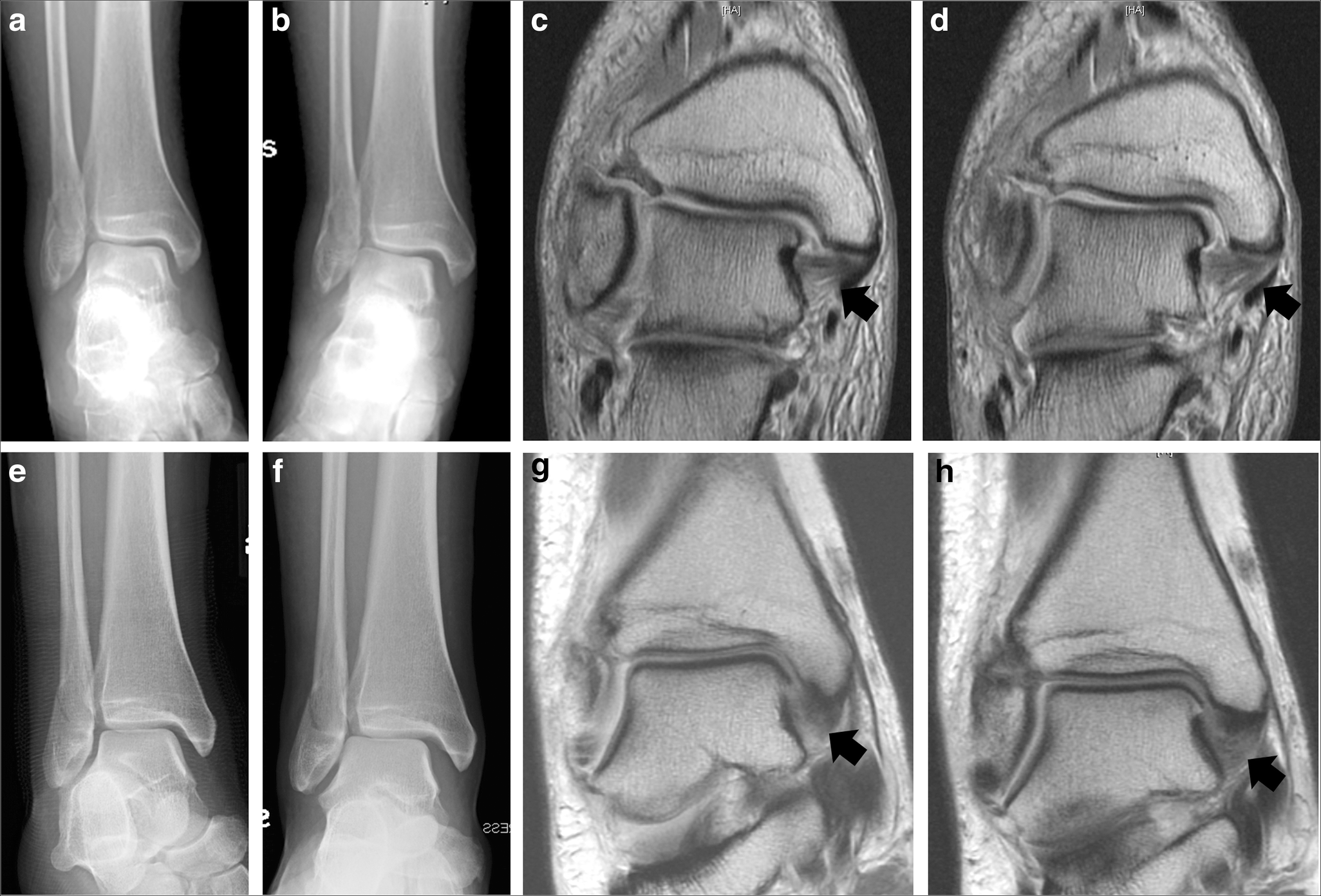
Using direct intra-operative observation through a medial ankle dissection as the gold standard in the current study, 71 patients (90%) had a ruptured deep deltoid and eight (10%) had an intact deep deltoid. Of the eight with an intact deep deltoid ligament intra-operatively, seven patients (88%) had an MCS of greater than 5 mm on injury mortise radiographs (three) or manual external rotation stress exams (four) (Table 1, Fig. 1). In contrast, none of these patients had a ruptured deep deltoid on MRI analysis.
Injury mortise radiographs (
Of the 71 patients with a ruptured deep deltoid observed intra-operatively, 62 (87%) had MCS measurements greater than 5 mm on injury mortise radiographs (52) or manual stress exams (10). MRI analyses predicted that 58 of these 71 patients (82%) had ruptured deep deltoid ligaments (Table 1). Overall, compared with intra-operative direct visualization, MCS measurements diagnosed a deep deltoid ligament rupture with 87% sensitivity, 13% specificity, and accuracy of 80%. MRI had a sensitivity of 82%, specificity of 100%, and accuracy of 84% to diagnose a deep deltoid rupture (Table 2), indicating more false positives using MCS measurements and more false negatives using MRI.
Summary of the ability of magnetic resonance imaging and medial clear space measurements to detect ruptures in the deep deltoid ligaments when using intra-operative observation as the gold standard
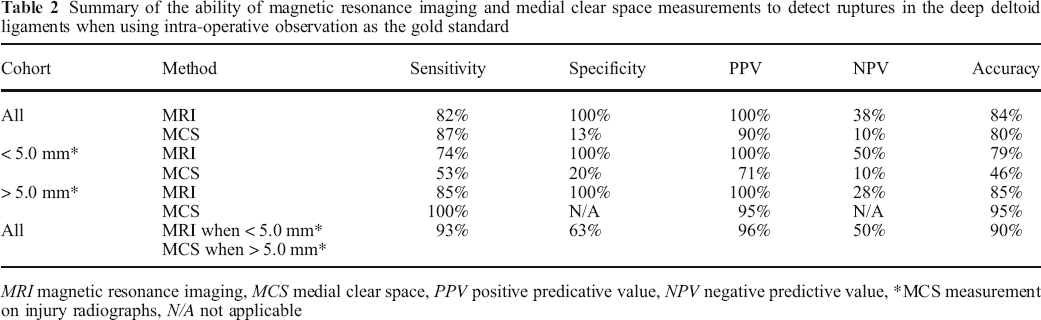
MRI magnetic resonance imaging, MCS medial clear space, PPV positive predicative value, NPV negative predictive value,
MCS measurement on injury radiographs, N/A not applicable
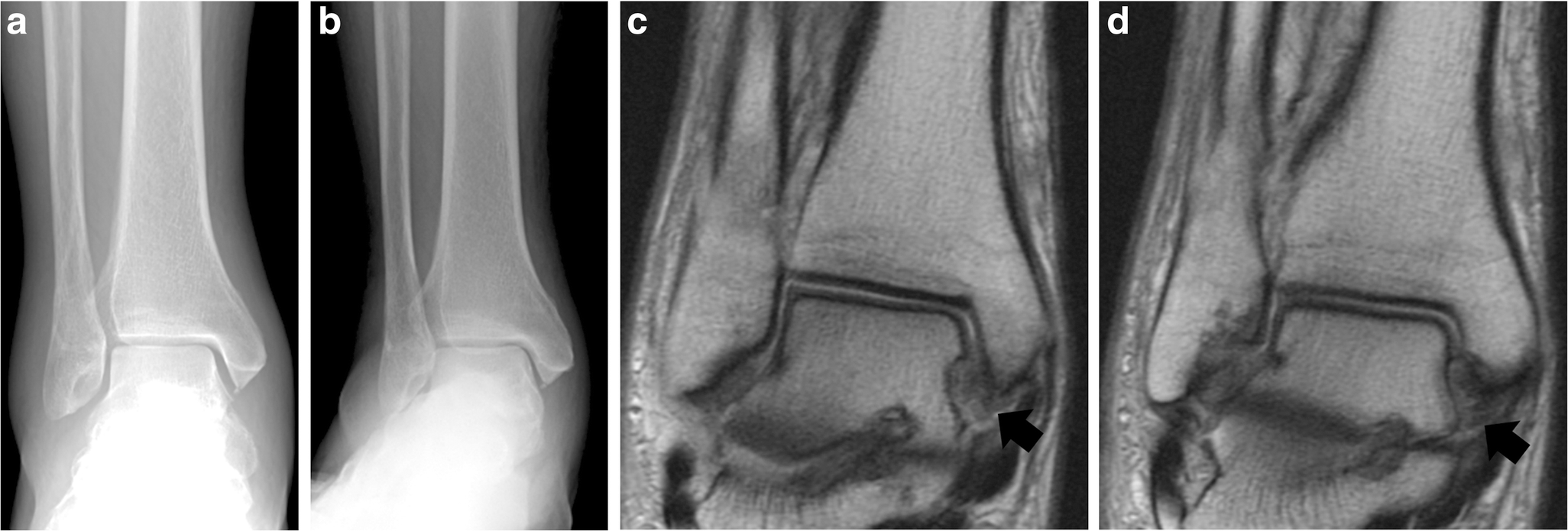
These initial results suggested that MRI analyses and MCS measurements may have different abilities to diagnose deep deltoid ruptures depending on MCS measurements from the injury radiographs. Because previous studies have indicated that MCS measurements of 5 mm may be optimal for differentiating between a stable and unstable ankle fracture [23, 36, 47], we subsequently determined the ability of MRI and MCS measurements to diagnose a deep deltoid rupture in patients with MCS measurements of less than 5 mm on injury radiographs and in patients with MCS measurements of greater than 5 mm. In patients with an MCS of less than 5 mm on injury radiographs, MRI had improved sensitivity (74% vs. 53%), specificity (100% vs. 20%), and accuracy (79% vs. 46%) over stress exams for predicting a ruptured deep deltoid ligament (Figs. 1, 2). In contrast, in patients with an MCS over 5 mm on injury radiographs, MCS measurements had improved sensitivity (100% vs. 85%) and accuracy (95% vs 85%) over MRI (Fig. 3).
Injury mortise radiograph (
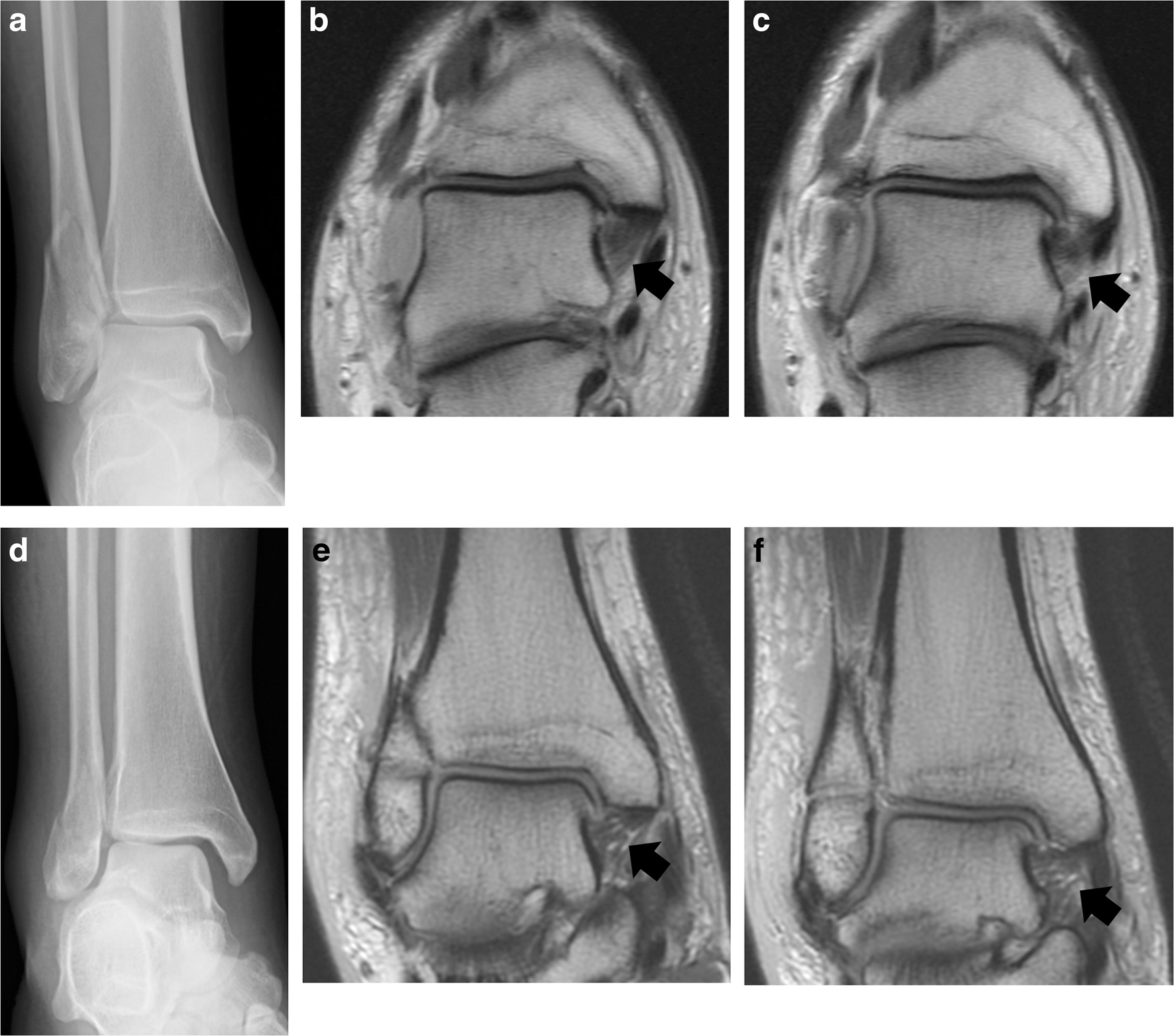
Injury mortise radiographs (
With a combined algorithm of only using injury radiograph if the MCS is at least 5 mm and adding MRI for those with MCS of less than 5 mm rather than external rotation stress radiography, sensitivity of 93%, specificity of 63%, and accuracy of 90% for deep deltoid rupture were noted (Table 2).
Discussion
Ankle mortise stability in the setting of an isolated lateral malleolus fracture depends on the status of the deep deltoid ligament. However, the diagnostic ability of tests such as MCS measurements and MRI to identify deep deltoid ruptures in ankle fractures has been unknown. In our prospective cohort of SER ankle fractures, we determined the accuracy of MCS measurements on injury and stress radiographs and MRI analysis to determine a deltoid rupture based on intra-operative direct observation as the gold standard. Our results suggest that MCS measurements on injury (non-stress) radiographs are most accurate when the MCS is greater than 5 mm. However, when the MCS measurements are less than 5 mm, MRI is a better diagnostic tool than manual stress examination. More specifically, MCS measurements have higher rates of false positives when the MCS is less than 5 mm, and MRI has higher rates of false negatives when the MCS is greater than 5 mm.
A limitation of this study is the high prevalence of deltoid ruptures in the cohort. However, this is difficult to avoid given the study methodology in which only surgical patients were included and a non-radiographic gold standard was used for comparison. Despite the possibility for selection bias, the increased prevalence of deep deltoid ruptures in the study cohort should not change the observed sensitivity and specificity, which are inherent to the test performed rather than the prevalence of a condition. Second, manual stress exams were performed by several different orthopedic residents, which may have been non-uniform. However, such an exam more closely represents the practice in an academic trauma center, thereby conferring generalizability to the current study. While the measurements were performed using calibration by the Picture Archiving and Communications System, similar to previous studies, no further calibration of the measurements was performed. Further, other methods of assessing medial structures could not be tested, including gravity and weight-bearing stress examinations, as these techniques are not routinely obtained at our institution. Finally, the inter-observer reliability of MRI analyses was fair, although our observed reliability was consistent with those of previous studies [36, 47]. As with many diagnostic radiology tests, MRI can be dependent on the reader and imaging protocol, which may have implications for centers without designated musculoskeletal radiologists.
Several others have assessed methods to effectively diagnose deep deltoid ruptures in SER-type ankle fractures [6–8, 11, 17, 18, 36, 47, 49]. However, none of those studies have been able to determine the true diagnostic value of these tests due to a lack of gold-standard evaluation. Recently, Nortunen et al. performed comparisons between MRI analyses and MCS measurements from external-rotation stress tests in patients with SER-type ankle fractures [36]. They concluded that MRI analyses revealed deep deltoid injuries in all patients regardless of MCS measurement and that MRI did not have a role in the treatment algorithm for these patients. Given that their study did not have a non-radiographic comparison, it is difficult to determine the significance of these results other than the finding that the grade of deep deltoid injury on MRI correlated with MCS measurements. Schottel et al. performed similar comparisons of MCS measurements and MRI analyses and determined that non-stress and stress MCS measurements alone were inadequate to diagnose a deep deltoid rupture and advocated for additional diagnostic testing in patients with MCS measurements of 4 to 5.5 mm on stress radiographs [47].
We used a medial ankle dissection to provide a non-radiographic, direct visual assessment of the deep deltoid ligament integrity. This surgical approach is an effective method to repair the deep deltoid when ruptured [28]. While the objective of our study was not to determine the effectiveness of a deltoid repair in this injury, a recent biomechanical study demonstrated the efficacy of a deep deltoid ligament repair in combination with repair of the posterior inferior tibiofibular ligament in restoring syndesmotic rotational stability [48]. In addition, a clinical study supports repair of the deltoid ligament in bimalleolar equivalent ankle fractures in place of using trans-syndesmotic screws [22]. One limitation of this method of direct visualization to determine deep deltoid ligament integrity is a lack of further objective criteria for diagnosing a ruptured ligament, as is common with many diagnostic tests.
We used MCS measurements on mortise radiographs from manual stress tests for radiographic determination of a deep deltoid rupture. This method has been demonstrated to have high inter-observer reliability when compared with alternative measurement techniques [36, 47]. In addition, other measurements on mortise radiographs such as MCS increase, MCS percentage of increase, or MCS/superior clear space ratio were not found to be superior to absolute MCS measurements for predicting a medial sided injury in SER ankle fractures [47].
One patient included in this study had MCS measurements and a consensus MRI read that were both negative for a deep deltoid rupture. The pre-surgical MRI analysis indicated a ruptured deep deltoid; however, the MRI was subsequently read as having an intact deltoid by two other radiologists to create the consensus reading of an intact deltoid. This patient had an SER stage III injury and underwent fixation of the lateral and posterior malleoli. Unlike the generally accepted indications of conservative treatment for SER II injuries [32, 52] and operative treatment for SER stage IV injuries [1, 2, 53], the ideal management for SER stage III injuries is less clear.
Despite these limitations, this study provides insight on properly diagnosing deep deltoid ruptures in ankle fracture patients. We recommend that patients with an MCS of greater than 5 mm on injury mortise radiographs need no further diagnostic testing of deep deltoid competency and may be considered for surgical fixation and stabilization of an unstable ankle fracture. In patients with an MCS of less than 5 mm on injury mortise radiographs, MRI analysis is a better diagnostic test than manual stress exams for diagnosing deep deltoid ruptures. The increased specificity (100%) of MRIs in this subset compared to manual stress exams (20%) could decrease unindicated surgeries and likely offset the higher costs of MRI.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2018_9655_MOESM1_ESM - The Diagnostic Accuracy of Radiographs and Magnetic Resonance Imaging in Predicting Deltoid Ligament Ruptures in Ankle Fractures
Electronic supplementary material, 11420_2018_9655_MOESM1_ESM for The Diagnostic Accuracy of Radiographs and Magnetic Resonance Imaging in Predicting Deltoid Ligament Ruptures in Ankle Fractures by, http://orcid.org/0000-0001-7093-8836 Warner Stephen J., MD, PhD, Garner Matthew R., MD, Fabricant Peter D., MD, MPH, Schottel Patrick C., MD, Loftus Michael L., MD, MBA, Hentel Keith D., MD, Helfet David L., MD, Lorich Dean G., MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
The online version of this article (10.1007/s11420-018-09655-x) contains supplementary material, which is available to authorized users.
Compliance with Ethical Standards
Conflict of Interest
Stephen J. Warner, MD, PhD, Matthew R. Garner, MD, Peter D. Fabricant, MD, MPH, Patrick C. Schottel, MD, Michael L. Loftus, MD, MBA, and Keith D. Hentel, MD, declare that they have no conflicts of interest. David L. Helfet, MD, reports owning stock in FxDevices and OHK Medical Devices and being an unpaid consultant to OHK Medical Devices, Healthpoint Capital, and TriMedics, outside the submitted work. Dean G. Lorich, MD, reported personal fees from DePuy Synthes, outside the submitted work.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients for being included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.