
Abstract
Background
In total ankle replacement (TAR), correct positioning of the implant is crucial. Malposition of the components may increase contact pressures and diminish prosthesis survival. The effect of sagittal tibiotalar alignment on functional outcomes after fixed-bearing TAR remains unclear, however, and no studies have compared fixed-bearing implants with respect to the anteroposterior (AP) position of the talar component.
Questions/Purpose
The purposes of this study were (1) to evaluate the effect of sagittal tibiotalar alignment on functional outcomes in fixed-bearing TAR and (2) to compare post-operative sagittal tibiotalar alignment in two types of fixed-bearing implants.
Methods
In a retrospective analysis of 71 primary TARs performed at a single center, we studied the INBONE™ II Total Ankle System and the Salto Talaris® Ankle. Radiographic measurements of the tibial axis–talus (T-T) ratio and the AP offset ratio were performed before and after surgery, respectively, and we evaluated Foot and Ankle Outcome Scores (FAOSs) and the 12-item Short Form Health Survey (SF-12) mental component summary (MCS) and physical component summary (PCS) scales pre-operatively and at 2 years after surgery. The Pearson correlation and independent-samples t test were used to evaluate differences in FAOSs, SF-12 MCS scores, and SF-12 PCS scores regarding post-operative sagittal alignment.
Results
Post-operative sagittal tibiotalar alignment was neutral in 39 ankles and anterior in 32 ankles. We observed no significant between-group differences in clinical outcome scores. Patients with a Salto Talaris Ankle prosthesis had a greater AP offset ratio (0.12) than patients with an INBONE II implant (0.05). However, the greater translation did not correlate with outcome scores.
Conclusion
At the 2-year follow-up, no correlation between the post-operative AP offset ratio and functional outcome scores was observed between the two fixed-bearing-implant groups. Further studies with longer follow-up are needed to determine whether the difference in sagittal alignment has an effect on functional outcomes in the long term.
Keywords
Introduction
Total ankle replacement (TAR) has become an established option for the treatment of advanced ankle osteoarthritis, largely because of advances in prosthesis design and operative techniques over the past 2 decades. However, the risks of complications and implant failure remain higher in TAR than in hip or knee arthroplasty [12, 17, 19]. Previous studies have shown prosthesis misalignment to be a common reason for implant failure and revision surgery [1, 6]. Malposition of the prosthesis leads to high joint contact pressures, which can negatively affect implant survivorship [7, 8].
Establishment of neutral post-operative sagittal tibiotalar alignment (anteroposterior [AP] offset ratio) (Fig. 1) may be an important factor in TAR but has been studied primarily in mobile-bearing implants [1, 3, 4, 20]. In a study of the Scandinavian Total Ankle Replacement™ (STAR™) system by Tochigi et al., anterior translation of the talar component was associated with smaller range of motion and has been considered a cause of early prosthesis failure [20]. However, subsequent studies have failed to show a correlation between sagittal translation of the talar component in relation to the tibial axis (the AP offset ratio) and clinical outcomes [3, 4]. The effect of sagittal positioning of fixed-bearing implants on clinical outcomes in TAR is still unknown. In a study with 30 patients who underwent TAR using a fixed-bearing implant, Datir et al. found that the lateral talar component angle had significant correlation with post-operative outcomes [5]. However, the sagittal translation of the talar component was not evaluated.
The anteroposterior (AP) offset ratio. X is the distance between the longitudinal axis of the tibia and a parallel line intersecting the center of the talar component. Y is the length of the tibial tray. AP offset ratio = X/Y. This measurement represents the sagittal translation of the talar component in relation to the center of the tibia.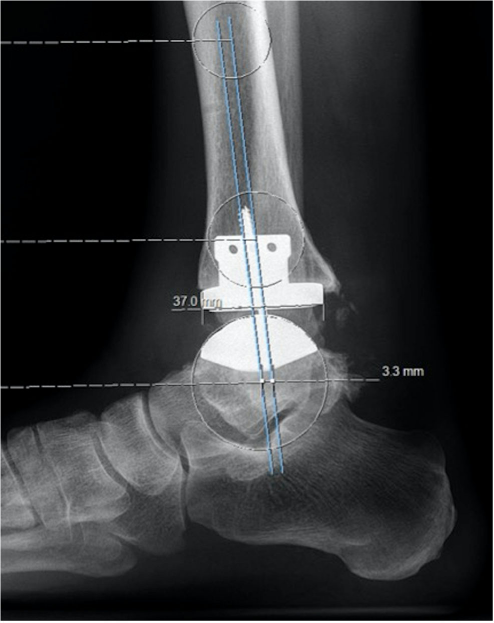
We hypothesized that sagittal tibiotalar alignment would be altered in fixed-bearing TAR according to implant design and degree of constraint and that patients with neutral sagittal alignment would have better post-operative clinical outcome scores than patients with sagittal malalignment. Our specific research questions were (1) Does post-operative sagittal tibiotalar alignment affect clinical outcomes in fixed-bearing TAR? (2) Considering the differences in TAR implant designs and degrees of constraint, are there differences in post-operative sagittal alignment between these two types of fixed-bearing TAR?
Materials and Methods
In this retrospective cohort study, we identified 71 patients treated at a single center between 2009 and 2014 who underwent TAR with either the Salto Talaris® Ankle (Integra LifeSciences, Plainsboro, NJ, USA) or the INBONE™ II Total Ankle System (Wright Medical Technology, Memphis, TN, USA). Three fellowship-trained foot and ankle orthopedic surgeons performed the procedures using a standard anterior approach. Inclusion criteria were primary TAR, adequate weight-bearing imaging before surgery and at 1 year after surgery, and Foot and Ankle Outcome Score (FAOS) survey results at 2 years.
Patient demographics were collected. There were 36 male (51%) and 35 female (49%) patients. The average age at the time of surgery was 69.8 years (range, 44 to 87 years). The Salto Talaris Ankle prosthesis was used in 42 procedures (59%), and the INBONE II system was used in 29 procedures (41%).
Standard weight-bearing lateral ankle radiographs were assessed pre-operatively and at the 1-year post-operative visit. Images were digitized and stored within Sectra Workstation IDS7 (Sectra AB, Linköping, Sweden). Measurements were independently performed by a musculoskeletal radiologist and a foot and ankle fellow using the Sectra Workstation IDS7 software. Radiographic measurements were calculated to one decimal point. The tibial axis–talus (T-T) ratio (± standard deviation) was used as a measure of pre-operative sagittal alignment, as previously described [21]. The T-T ratio is measured from the intersection point of the tibial axis with the talar reference line, which spans the AP dimension of the talus. The ratio is expressed as a percentage of the AP length of the talus (Fig. 2). Sagittal tibiotalar alignment was assessed post-operatively using the AP offset ratio, as described by Barg et al. [2]. The AP offset ratio is the ratio between the distance from the tibial axis to the center of the talar component and the length of the tibial prosthesis component, as seen in lateral radiographs (Fig. 1). This method was initially described for measurement of sagittal alignment in mobile-bearing components. Post-operative sagittal alignment was categorized as neutral (an AP offset ratio < 0.1) or anterior (an AP offset ratio > 0.1). There were no patients with posterior alignment (a negative AP offset ratio).
The tibial axis–talus (T-T) ratio. B to D (BD) is the distance between the posterior talar point and the distal tibial axis. A to B (AB) is the talar length. T-T ratio = BD/AB × 100.
Results of the FAOS survey and 12-item Short Form Health Survey (SF-12) mental component summary (MCS) and physical component summary (PCS) were obtained pre-operatively and 2 years after surgery. The FAOS is a region-specific questionnaire that contains 42 questions divided into five subscales. It has been validated for assessment of ankle arthritis [14] and has been used in previous TAR studies [3, 9, 15, 16, 24]. The SF-12 questionnaire is used to assess general health. A longer, 36-item version of the questionnaire has been validated for use in the orthopedic population and as the standard score against other instruments in validation studies [10, 23]. The FAOS and SF-12 are well established worldwide and were the standard instruments used in the assessment of foot and ankle pathologies at our institution during the study period.
Statistical Analysis
Inter-observer reliability was assessed using two-way random, absolute agreement, single-measure intra-class correlation coefficient (ICC), and the Pearson correlation. Pre-operative and post-operative sagittal alignments were assessed using an independent-samples t test to detect differences between the two implant groups. The Pearson correlation and t tests were used to evaluate differences in FAOSs, SF-12 MCS, and SF-12 PCS between neutral and anterior alignment groups.
Results
There was no significant difference in pre-operative T-T ratio between the groups receiving the Salto Talaris Ankle or the INBONE II implant (p = 0.143). Pre-operatively, the average T-T ratio in patients receiving a Salto Talaris Ankle implant was 34.38 ± 12.28 (95% confidence interval [CI], 13.58 to 62.94), and in recipients of the INBONE II implant, it was 30.26 ± 10.24 (95% CI, 10.75 to 49.75). Inter-observer reliability for the pre-operative sagittal alignment using the T-T ratio had an ICC of 0.999, indicating very good agreement, whereas the post-operative AP offset ratio measurement demonstrated an ICC of 0.479, indicating fair or moderate agreement.
AP offset ratio correlated with FAOS and SF-12 scores
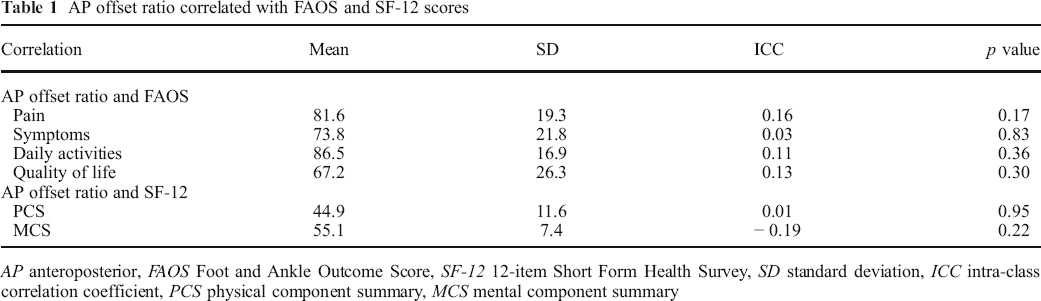
AP anteroposterior, FAOS Foot and Ankle Outcome Score, SF-12 12-item Short Form Health Survey, SD standard deviation, ICC intra-class correlation coefficient, PCS physical component summary, MCS mental component summary
Correlation of FAOS scores with post-operative AP offset ratio neutral and anterior groups
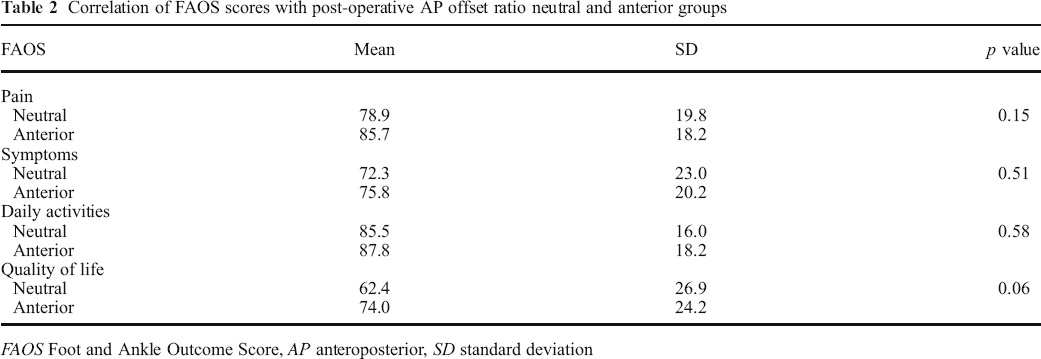
FAOS Foot and Ankle Outcome Score, AP anteroposterior, SD standard deviation
Comparison of pre-operative T-T ratio and post-operative AP offset ratio between prosthesis types
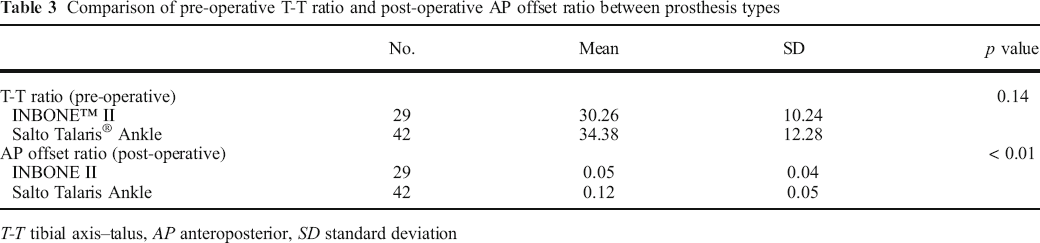
T-T tibial axis–talus, AP anteroposterior, SD standard deviation
Discussion
We found no correlation between post-operative sagittal tibiotalar alignment (AP offset ratio) and FAOSs or SF-12 MCS and PCS scores. Post-operatively, the patients with INBONE II implants had a significantly lower AP offset ratio than patients with a Salto Talaris Ankle prosthesis, indicating a more neutral sagittal alignment. However, the mild anterior translation of the talus in the Salto Talaris Ankle group had no significant effect on patient FAOS results or SF-12 scores. Differences in operative technique and prosthesis design likely contribute to the difference in post-operative sagittal alignment. Despite both prostheses being fixed-bearing implants, the INBONE II has a more constrained design, which could explain the more stable AP positioning. In addition, the Salto Talaris Ankle implant often does not provide full coverage of the tibia in the anterior-to-posterior dimension [11]. In such cases, the tibial component is placed flush with the anterior cortex of the distal tibia, leaving some bony overhang posteriorly. Given that the implant employs a fixed bearing, the talar component will conform to the tibial component. Therefore, in these cases, the talar component will also be anterior to the tibial axis, as our study demonstrated.
This study is not without limitations. The AP offset ratio ICC was 0.479, indicating only fair or moderate agreement. This highlights the difficulty in making precise measurements on post-operative radiographs after TAR. In addition, differences in sagittal alignment could influence functional outcomes that could not be detected because of the short follow-up period or the small sample size. Finally, only mild variations in sagittal tibiotalar alignment are expected in fixed-bearing TAR, which makes a significant difference in clinical outcomes less likely to be detected.
Studies of mobile-bearing implants have yielded mixed results in sagittal alignment and patient outcomes. In a study of 317 patients, Barg et al. demonstrated that neutral sagittal alignment of the implant was correlated with greater pain relief and better functional outcomes [1]. In a study of 119 patients, Cho et al. failed to confirm those results, showing similar functional outcomes regardless of post-operative sagittal alignment [4]. Braito et al. also found no significant differences in functional outcomes according to post-operative sagittal translation of the talar component [3]. However, fixed-bearing implants, such as the INBONE II and the Salto Talaris Ankle, conceivably do not engage the peri-ankle ligaments the same way that mobile-bearing implants do [18]. Furthermore, studies of mobile-bearing implants have shown that significant anteroposterior relocation of the talus occurs within the first 6 months, which is not likely to occur with fixed-bearing implants [13, 22]. To our knowledge, this is the first study to evaluate the effect of sagittal tibiotalar alignment on functional outcomes in fixed-bearing TAR.
The results of this study suggest that post-operative sagittal tibiotalar alignment does not influence short-term functional outcomes in fixed-bearing TAR. Furthermore, we noted a difference in the post-operative sagittal alignment between two types of fixed-bearing implants. This difference may be attributed to the difference in the implant design and in the articular constraint inherent in the two implants. Further studies are needed to determine whether sagittal alignment plays a role in long-term clinical outcomes and implant survivorship after fixed-bearing TAR.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM1_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM1_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM2_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM2_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM3_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM3_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM4_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM4_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM5_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM5_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9728_MOESM6_ESM - Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study
Electronic supplementary material, 11420_2019_9728_MOESM6_ESM for Sagittal Tibiotalar Alignment May Not Affect Functional Outcomes in Fixed-Bearing Total Ankle Replacement: A Retrospective Cohort Study by, Natalie M. Nielsen, MD, Guilherme H. Saito, MD, Austin E. Sanders, BA, Scott J. Ellis, MD, Carolyn M. Sofka, MD, Constantine A. Demetracopoulos, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
Compliance with Ethical Standards
Conflict of Interest:
Natalie M. Nielsen, MD, Austin E. Sanders, BA, and Carolyn M. Sofka, MD, declare that they have no conflicts of interest. Guilherme H. Saito, MD, reports fees as a consultant from Wright Medical Technology, outside the submitted work. Scott J. Ellis, MD, reports fees as a consultant from Wright Medical Technology. Constantine A. Demetracopoulos, MD, reports fees as a consultant from Integra LifeSciences and Wright Medical Technology.
Human/Animal Rights:
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent:
Informed consent was waived from all patients for being included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.