
Abstract
Background
Hip arthritis is one of the major causes of disability worldwide. Hip resurfacing arthroplasty (HRA) has emerged in recent years as an alternative to total hip arthroplasty (THA), but complications of HRA have limited the patient population to younger male patients with primary osteoarthritis and large hip anatomy. How the functional benefits of HRA in this population compare with those of THA is not entirely clear.
Questions/Purposes
The primary aim of this study was to determine whether there were differences in hip disability and patient satisfaction with surgery between these two groups at 2 years after surgery, using patient-reported outcome measures (PROMs) and subjective measures of patient satisfaction. Additionally, we sought to determine whether there were differences in post-operative discharge disposition, revision rates, or adverse events.
Methods
We searched an institutional database to identify patients undergoing unilateral HRA or THA between January 2007 and July 2011 who met today's recommended criteria for HRA: younger male patients with large-enough hip anatomy to make surgery viable (a femoral head of at least 48 mm in HRA patients and, in THA patients, an acetabular shell size of 54 mm, the minimum outer shell size that could accommodate a femoral head component of 48 mm; for matching purposes, acetabular shell size in THA was used as a surrogate for the femoral head size used in HRA). We used propensity score matching to control for potentially confounding pre-operative variables and administered the Hip Disability and Osteoarthritis Outcome Score (HOOS) survey, including its subdomains, at the 2-year mark. We also assessed differences between groups in Lower Extremity Activity Scale scores, 12-item Short Form Health Survey results, and answers regarding satisfaction with surgery. We calculated minimal detectable change, minimum clinically important change, and substantial clinical benefit using anchor-based techniques for multiple outcome measures.
Results
There were 251 patients in each group. HRA patients scored significantly higher than THA patients on the 2-year HOOS sports and recreation (92 versus 87, respectively) and on rates of overall satisfaction (94% versus 89%, respectively). The HRA group also had a greater chance of achieving minimum clinically important change (18.75 points) in the HOOS sports and recreation subdomains than the THA group (97% versus 91%). No significant difference was found in 6-month adverse event rates. HRA patients also had a significantly shorter mean hospital stay, a higher rate of discharge to home, and a lower incidence of a “significant” limp after surgery.
Conclusion
HRA may provide a functional benefit in sports and recreation and greater satisfaction in patients who meet the current criteria for HRA. Because these benefits may be small, pre-operative counseling should focus on balancing the possible functional benefits against the longer-term risks associated with metal-on-metal bearings.
Keywords
Introduction
Hip arthritis is one of the major causes of disability worldwide, with those affected showing diminished physical and mental health [26, 47]. The success of total hip arthroplasty (THA) in improving quality of life (QOL) is undeniable, but in younger patients who outlive the utility of their prostheses, hip resurfacing arthroplasty (HRA) has emerged as an alternative [12, 24]. The first HRA, developed in the early 1970s, used metal-on-polyethylene bearings and was unsatisfactory because of excessive wear, osteolysis, and bone loss [16]. Improvements in surgical technique, bearing materials, and fixation strategies made HRA a viable option, particularly in younger and more active patients [32].
The technique currently in use for HRA as treatment for end-stage hip arthritis was approved for use in the USA in 2006 [8, 32]. Proponents of HRA cite advantages, including preservation of bone stock, reduced bearing wear, restoration of more normal hip anatomy, return to impact activities, avoidance of proximal-femur stress shielding, and a lower risk of dislocation through a larger ball size [15, 28]. However, HRA also carries risks of unique complications, including extended surgical exposure, femoral neck fracture, osteonecrosis, and adverse reactions to metal ion debris, all of which have been associated with specific patient demographic variables [20, 21, 30, 37]. For this reason, HRA is currently recommended only in male patients less than 65 years of age with large anatomy and primary osteoarthritis [31], which is further supported by cost–utility analyses [16, 46]. A number of studies have compared HRA with THA [33, 38], including biomechanical and radiographic outcomes [25, 42]. However, the definitions of success used in these studies have been objective and surgeon dependent, not taking into account subjective patient outcomes.
Conflicting evidence exists regarding the functional advantages of HRA, as compared with THA, in terms of patient satisfaction and patient-reported outcome measures (PROMs). Short-term follow-up studies comparing functional outcomes after HRA and THA, including two prospective randomized, controlled trials, have generally found no differences in multiple outcome measures [5, 6, 11, 13, 41]. However, a long-term prospective comparative study by Haddad et al. found that at an average of 12 years after surgery, higher proportions of patients in the HRA group were running and involved in sports and heavy manual labor [15]. No studies have evaluated functional outcomes of HRA in patients meeting current criteria—male sex, age under 65 years, and hip anatomy that accommodates a femoral resurfacing component of 48 mm or larger—using a well-matched cohort of THA patients for comparison.
The primary aim of this study (Question 1 in Results) was to compare outcomes of hip arthroplasty in propensity score–matched cohorts of patients undergoing unilateral HRA or THA, with regard to the Hip Disability and Osteoarthritis Outcome Score (HOOS) and its subdomains at 2 years after surgery [36]. Our null hypothesis was that there would be no difference in the patient-reported HOOS score at 2 years between matched HRA and THA groups.
Our second aim (the “Question 2” section) was to determine whether there were differences between the two patient populations in other outcomes, using the Lower Extremity Activity Scale (LEAS) [40], the 12-item Short Form Health Survey (SF-12) [50], and the self-reported satisfaction. Our additional aims (the “Question 3” section) were to determine whether there were differences between the groups with regard to discharge disposition, post-operative complications, or revision rates.
Materials and Methods
We performed a retrospective analysis of an institutional arthroplasty database to identify all patients treated between January 1, 2007, and July 1, 2011, meeting present-day HRA criteria: male sex, age under age 65 years, primary osteoarthritis, and the ability to accommodate a femoral head resurfacing component of 48 mm or more. Patients were included if their records contained the necessary demographic and clinical follow-up information and data from completed PROMs. Patients were excluded if there was less than 2 years of follow-up data available for review or if baseline information necessary for matching was missing. In the THA cohort, an acetabular diameter of 54 mm or greater was used as a surrogate for HRA femoral head size (the minimum outer shell size needed for a femoral head component of 48 mm used in HRA).
All HRAs were performed using an extensile posterior approach, allowing for a 360° view of the acetabulum [7]. Of the 251 HRAs, 231 were performed using the Birmingham Hip Resurfacing™ (BHR) System (Smith & Nephew, Memphis, TN, USA), two using the ReCap® Femoral Resurfacing System (Zimmer Biomet, Warsaw, IN, USA), ten using the Conserve Plus system (Wright Medical, Memphis, TN, USA; no longer in use), and eight using the Cormet device (Stryker, Mahwah, NJ, USA; no longer in use). The acetabular component of the BHR System has a porous surface with a calcium hydroxyapatite coating to allow cementless implantation. Both components are manufactured from as-cast high-carbon cobalt–chrome alloy with 4-mm increments in the diameter of the femoral component, and 2-mm increments for the acetabular component. In 2008, 2-mm increments became available for the femoral component size and were used thereafter. The intended acetabular component inclination and anteversion targets were 40 and 15°, respectively, with the femoral component cemented in neutral or mild valgus relative to the femoral neck, using regular-viscosity Simplex bone cement (Stryker, Mahwah, NJ, USA) [8]. The acetabulum was under-reamed by 1 mm relative to the component to allow for press-fit fixation.
In the THA group, all surgery was performed using a standard posterior approach with removal of the femoral head and a portion of the femoral neck appropriate for femoral stem choice and leg length restoration. The femoral shaft was exposed to open the femoral canal, and the femoral component was inserted into the canal with the articulating femoral head placed onto the neck of the femoral component. The choice of femoral components and bearing surfaces was at the discretion of the operating surgeon and was recorded. The only differences in post-operative protocol between the groups were the implementation of posterior hip precautions for 6 weeks after surgery in the THA group and weight bearing as tolerated with crutches for the same length of time in the BHR System group.
All patients were asked to provide information on standard PROMs at their pre-operative visit and at the 2-year follow-up visit; the PROMs included the LEAS, the HOOS subdomains (pain, stiffness, activities of daily living, QOL, and sports and recreation), and the SF-12, which includes physical component and mental component summary scales.
Patients were also asked to rate their 2-year satisfaction with surgery using a 5-point Likert scale covering a number of areas: relief of pain, improvement in the ability to do housework or yard work, improvement in the ability to participate in recreational activities, and overall satisfaction with the results of hip surgery; a 6-point Likert-like scale was used to assess QOL.
The entire unmatched cohort was used to calculate the minimal detectable change (MDC), the minimum clinically important difference (MCID), and the substantial clinical benefit (SCB). MDC, defined as the minimum amount of change required to distinguish a true health change from variability resulting from measurement error, was calculated using previously described techniques [29]. Essentially, it was calculated as follows: MDC = z score × SEM ×
The MCID reflects the minimum change in PROM or satisfaction scores that a patient perceives as a change in his or her health [2, 4] and can be calculated using as many as 14 different methods [51]. We calculated the anchor-based receiver operating characteristic (ROC) curve and the anchor-based mean change score [3] without clinician consensus because estimates derived from surgeon opinion would seem to violate the intent of PROMs, which is to understand outcomes exclusively from the patient's perspective [29]. The anchor-based approach relies on an anchor question, asked at follow-up, and distinguishes patients who have experienced a change in their health from those who have not. We chose the 2-year post-operative satisfaction question regarding the improvement in QOL (using the 6-point Likert-like scale) as the anchor question. Logistic regression and the area under the ROC curve are used to find the delta score cut point that best identifies which patients experience a minimal improvement and those who do not according to anchor question responses. Finally, the SCB, defined as the lower bound for defining optimal patient benefit, was calculated using the anchor-based ROC approach [29].
After calculating candidate MDC, MCID, and SCB values for all domains of the PROMs and satisfaction scores, patients were propensity score matched. In the present study, the propensity score is the patient's conditional probability of receiving HRA, given the individual's pre-surgery characteristics; by adjusting for differences in baseline characteristics between the two cohorts, the covariates of each cohort become comparable. Variables used in the estimation of the propensity scores in each cohort included age, body mass index (BMI), Charlson Comorbidity Index, baseline activity level (LEAS), baseline PROM scores, Elixhauser comorbidity conditions, American Society of Anesthesiologists physical status classification system score, laterality, and year of surgery.
Every pre-operative covariate captured in the registry was used to create propensity scores, including baseline activity level and PROMs. Propensity score techniques have been shown to overcome many of the limitations of conventional observational studies while allowing them to mimic the randomization of randomized, controlled trials [9]. A propensity score addresses confounding by expressing the probability of having been treated with an intervention based on variables present at or before the time of treatment [39]. Because the propensity score was used by matching every pre-operative covariate available in the database, no risk-adjusted results were necessary. A total of 22 surgeons contributed patients to the THA group (one to 75 cases per surgeon), and a total of eight surgeons contributed patients to the HRA group (one to 189 cases per surgeon). (The 189 procedures representing the upper end of the range were performed by one surgeon [EPS].)
All data were collected using Excel software (Microsoft Corporation, Redmond, WA, USA). Means and SDs were calculated for continuous variables, and proportions were calculated for categorical variables. Length of hospital stay and patient discharge disposition (home, rehabilitation, or subacute nursing facility) were recorded and compared between groups. Implant variables, including size and bearing surface, were recorded. At up to 6 months after surgery, rates of complications, including deep venous thrombosis, infection, major bleeding, pneumonia, dislocation, additional hip surgery, and persistent pain, were recorded and compared between groups. Six-month outcomes were also recorded, including the need for an assistive device for ambulation, joint stiffness, muscle weakness, muscle paralysis, perceived inequality in leg length, significant limping, and change in superficial sensation. Outcome measures were compared between groups, including 2-year PROMs, satisfaction scores, revision rates, and adverse events. The mean change in outcome scores was compared between groups. The percentages of patients in each cohort who achieved relevant MCD, MCIC, and SCB values were calculated and compared between groups. Finally, we considered the face validity of the various MDC, MCID, and SCB values based on conceptual frameworks requiring that MDC be less than MCID and that MCID be less than or equal to SCB. We reasoned that an MCID or SCB that was smaller than an MDC, which represents the error of the scoring instrument, should not be considered a valid estimate [44]. All analyses were conducted using SAS for Windows 9.4 (SAS Institute Inc., Cary, NC, USA). A critical p value of 0.05 was set for all comparisons. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Results
Patient selection before and after application of inclusion and exclusion criteria
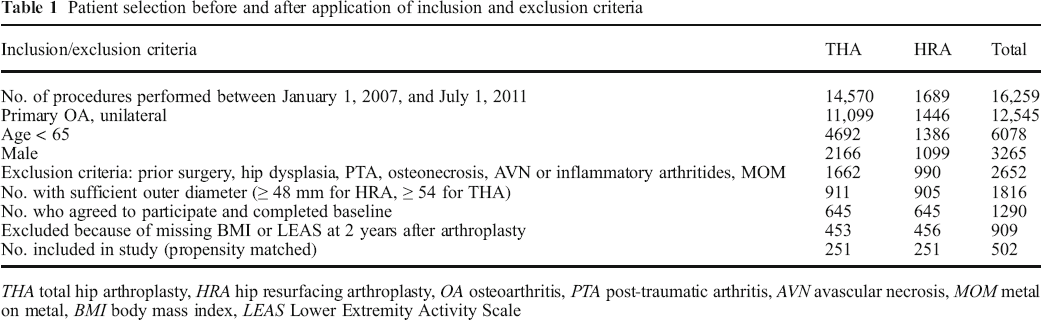
THA total hip arthroplasty, HRA hip resurfacing arthroplasty, OA osteoarthritis, PTA post-traumatic arthritis, AVN avascular necrosis, MOM metal on metal, BMI body mass index, LEAS Lower Extremity Activity Scale
Baseline characteristics of propensity score–matched patients
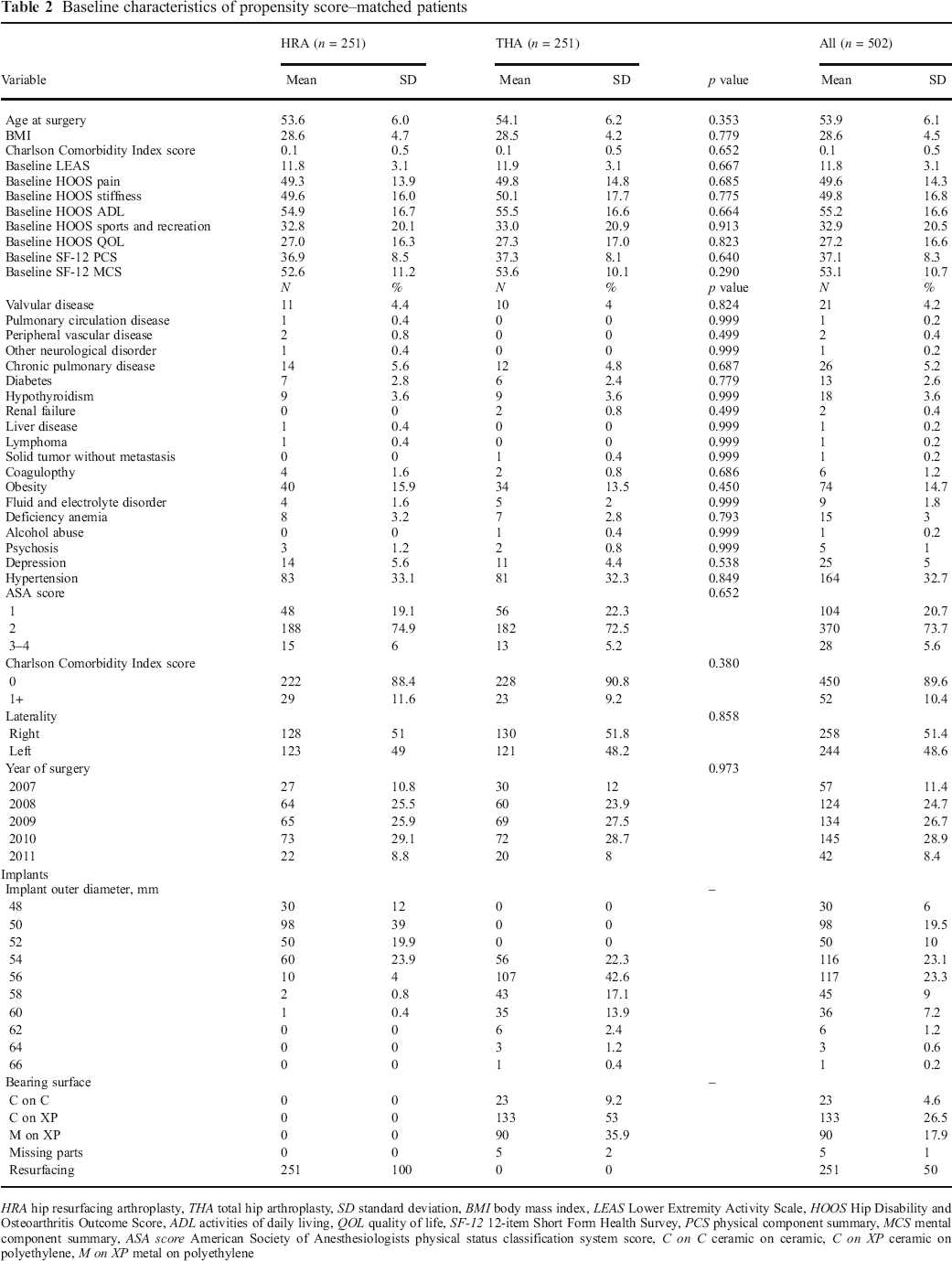
HRA hip resurfacing arthroplasty, THA total hip arthroplasty, SD standard deviation, BMI body mass index, LEAS Lower Extremity Activity Scale, HOOS Hip Disability and Osteoarthritis Outcome Score, ADL activities of daily living, QOL quality of life, SF-12 12-item Short Form Health Survey, PCS physical component summary, MCS mental component summary, ASA score American Society of Anesthesiologists physical status classification system score, C on C ceramic on ceramic, C on XP ceramic on polyethylene, M on XP metal on polyethylene
MCIC and SCB for the satisfaction measures and QOL, recorded at 2 years after surgery a
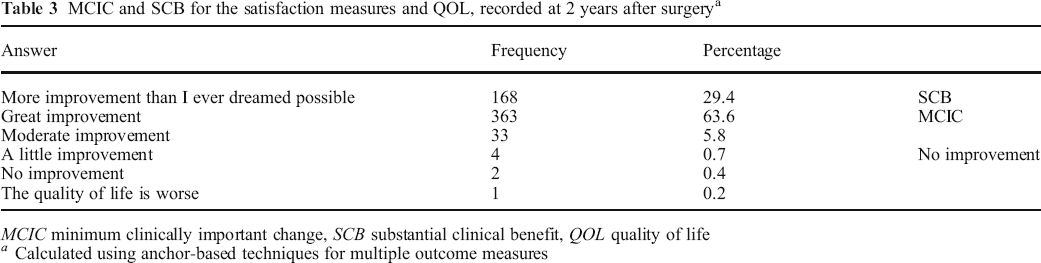
MCIC minimum clinically important change, SCB substantial clinical benefit, QOL quality of life
Calculated using anchor-based techniques for multiple outcome measures
Question 1
MDC, MCIC, and SCB for HOOS subdomain outcome measure, as well as percentages of patients achieving relevant values at 2 years
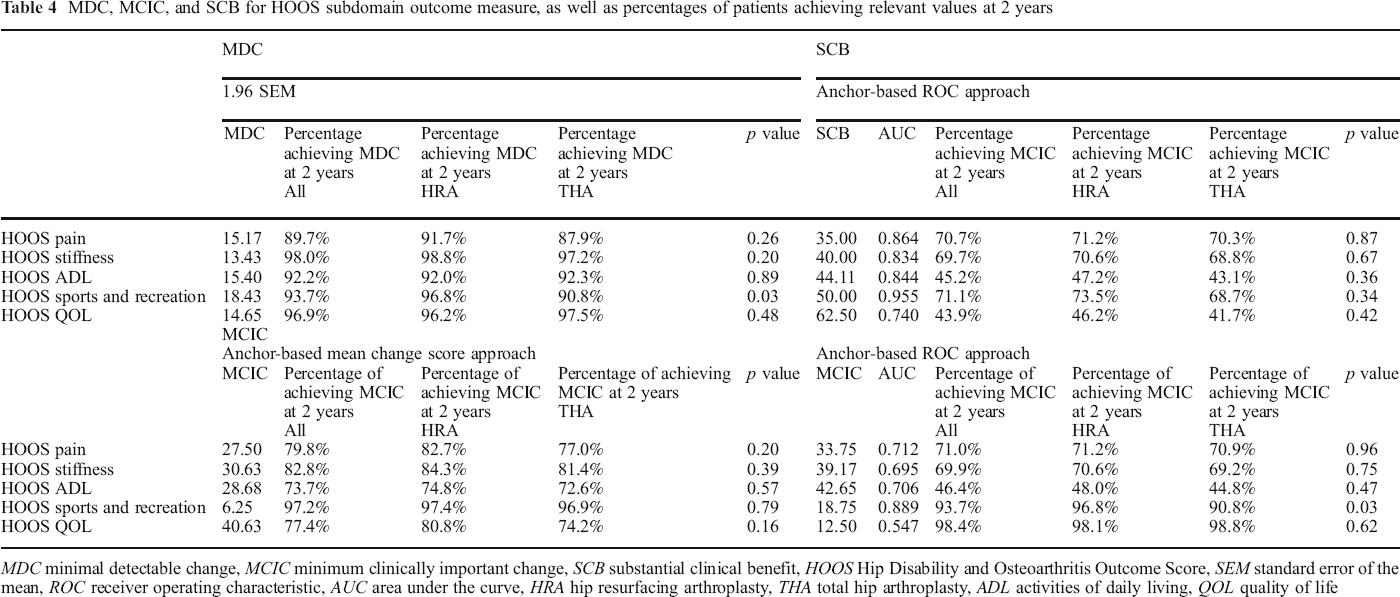
MDC minimal detectable change, MCIC minimum clinically important change, SCB substantial clinical benefit, HOOS Hip Disability and Osteoarthritis Outcome Score, SEM standard error of the mean, ROC receiver operating characteristic, AUC area under the curve, HRA hip resurfacing arthroplasty, THA total hip arthroplasty, ADL activities of daily living, QOL quality of life
Two-year satisfaction scores and 2-year changes from baseline patient-reported outcomes
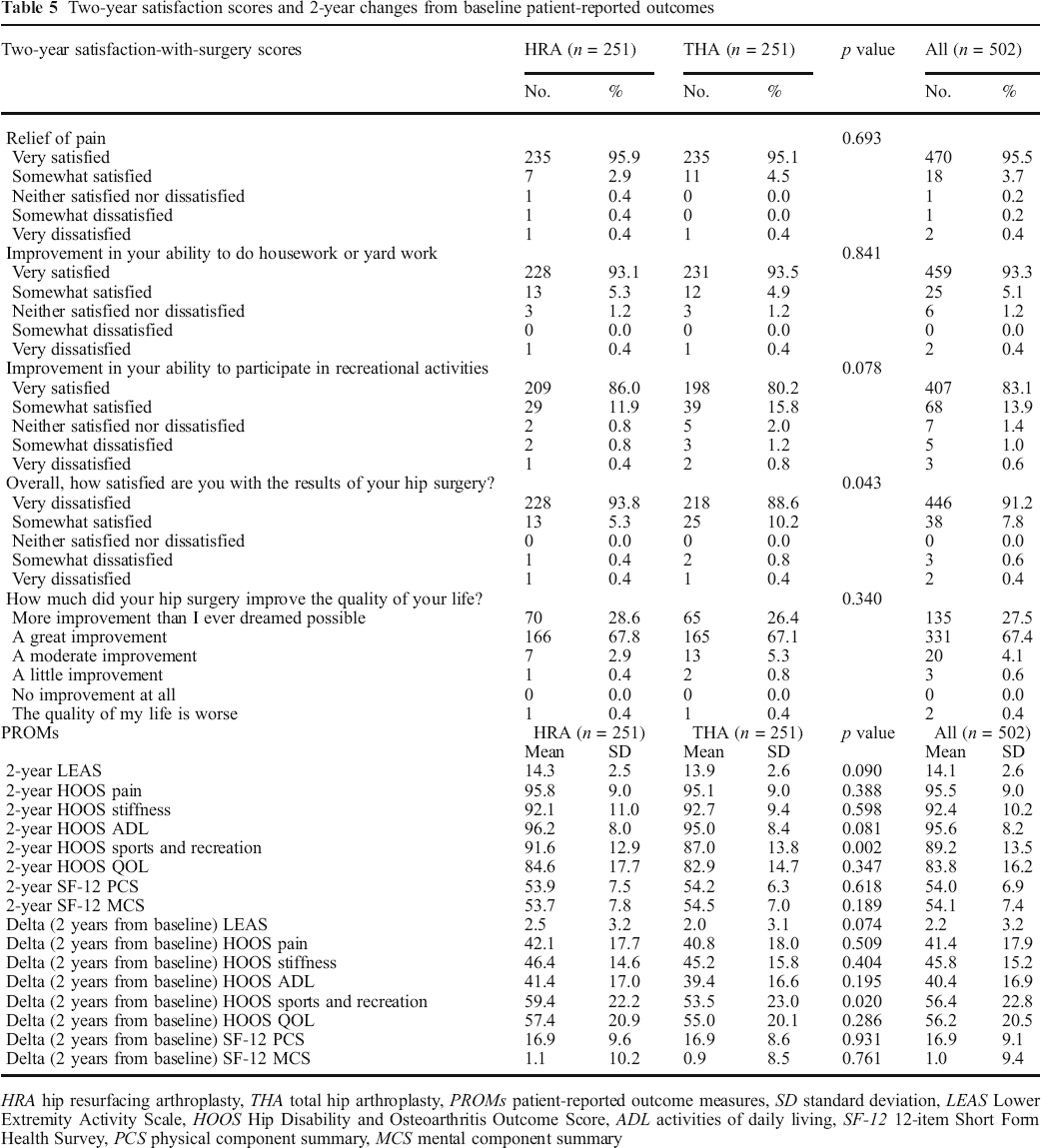
HRA hip resurfacing arthroplasty, THA total hip arthroplasty, PROMs patient-reported outcome measures, SD standard deviation, LEAS Lower Extremity Activity Scale, HOOS Hip Disability and Osteoarthritis Outcome Score, ADL activities of daily living, SF-12 12-item Short Form Health Survey, PCS physical component summary, MCS mental component summary
Question 2
When comparing the HRA and THA groups, the 2-year and improvement-from-baseline PROMs were not significantly different with regard to the LEAS or SF-12 subscores (Table 5). The 2-year satisfaction ratings were not significantly different between the HRA and THA groups with regard to pain relief (p = 0.69), improvement in the ability to do housework or yard work (p = 0.84), improvement ability to perform recreational activities (p = 0.08), or improvement in QOL (p = 0.34). However, the overall satisfaction with surgery was greater in the HRA group. The HRA group more frequently reported being “very satisfied” with surgery (94% versus 89%, p = 0.04).
Question 3
Comparison between HRA and THA regarding length of stay, discharge disposition, six-month postoperative outcome measures and two-year revision rates.
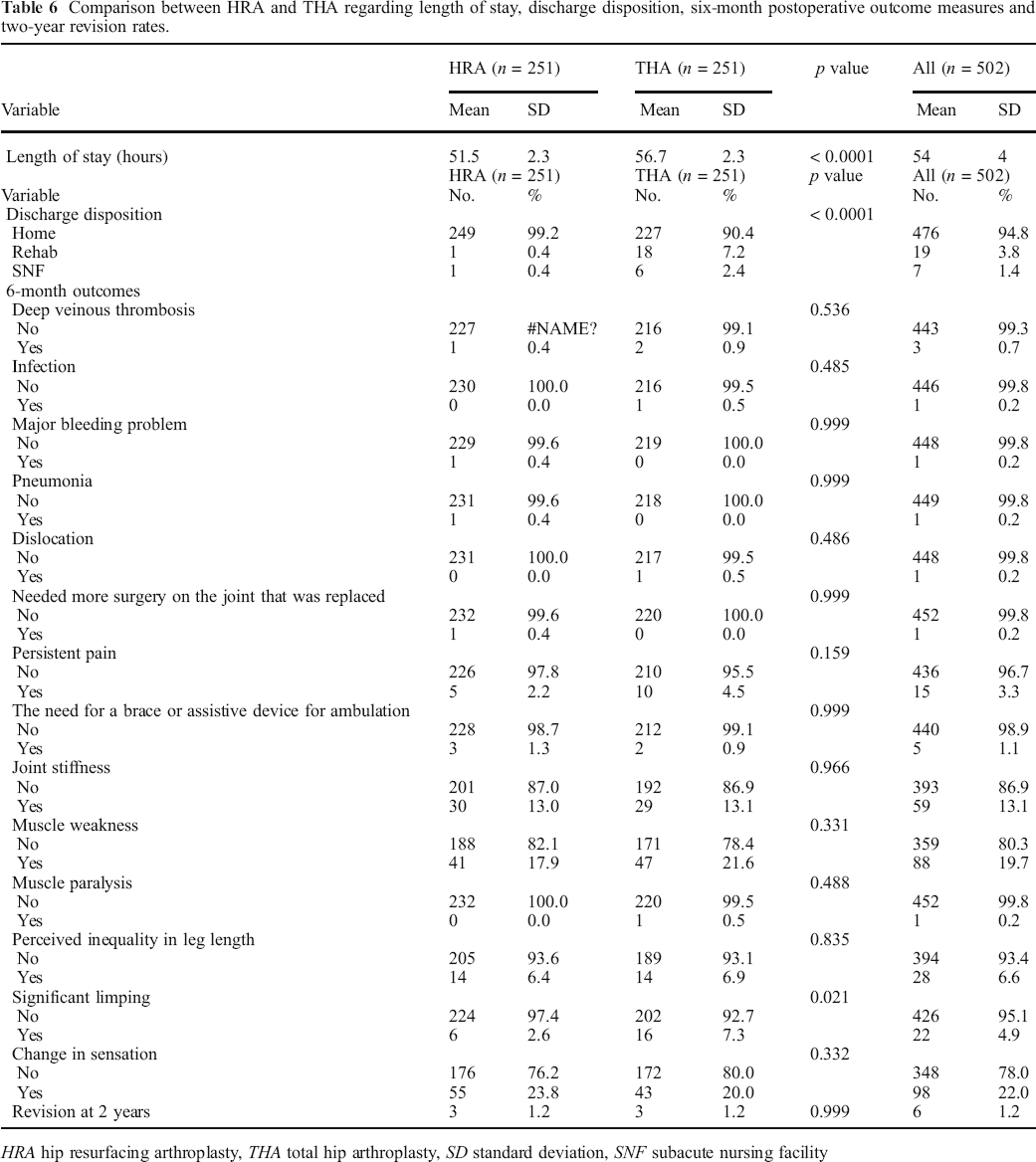
HRA hip resurfacing arthroplasty, THA total hip arthroplasty, SD standard deviation, SNF subacute nursing facility
Discussion
There is controversy over whether THA and HRA provide comparable improvements in PROMs and satisfaction among patients in whom the procedures are indicated. This study is unique because we sought to compare patient cohorts with similar pre-operative characteristics who met current surgical criteria for HRA: male patients under 65 years of age with relatively large femoroacetabular anatomy. This study sought to compare propensity score–matched cohorts of patients undergoing unilateral HRA or THA, looking at HOOS scores and HOOS subdomains at 2 years after surgery. We demonstrated some statistically significant differences between the HRA and THA groups in the HOOS subdomains, but the differences detected were small and have limited clinical relevance. Our second aim was to determine whether there were differences between the two patient populations with regard to the LEAS, SF-12 scores, or patient satisfaction. We demonstrated a difference in patient satisfaction but no differences in LEAS or SF-12 scores. Our final aims were to determine whether there were differences between the groups with regard to discharge disposition, post-operative complications, or revision rates. We found the HRA group had a shorter average hospital stay, a higher proportion of patients discharged home, less self-reported limping, and no differences in measured post-operative complications.
Limitations of this retrospective study include the use of propensity score matching, which can only be performed with measured covariates. Although unmeasured covariates should be balanced, residual confounding is still possible. Previous studies have demonstrated that analyses using propensity scoring methods cannot adjust for unmeasured confounding [17, 27]. Moreover, the matching process necessarily resulted in a selected cohort of THA patients that is not representative of all patients undergoing THA at our institution, and bias may have been introduced in favor of HRA because patients choosing HRA may have a belief that it is superior to conventional THA [35]. This could have resulted in better self-reported outcomes. Similarly, only patients with at least 2 years of clinical follow-up and complete PROM data were eligible for propensity matching. This represents a possible detection bias, although it should be similar in both groups. Another limitation is the possibility that the outcome instruments we used are not discriminating enough in such high-level patients and that the results reflect the ceiling effects of the outcomes [19]. More sensitive scoring systems should be used to study young patients with hip disease to better evaluate and differentiate the results of modern surgical techniques. The follow-up of the cohorts in our study was relatively short, and longer-term follow-up should improve the validity of our findings. Although all procedures were performed using a posterior–posterolateral approach, surgeons may use different techniques (for either procedure) and differences in individual surgical technique were not controlled for. Additionally, it is possible that the clinical differences detected in this study represent, in part, differences in activity restrictions imposed by the surgeon. Specifically, HRA patients generally have fewer post-operative restrictions placed on them than THA patients and may therefore recover faster and be more satisfied. Finally, the majority of the HRAs included in the study were performed by a single surgeon (EPS), which may decrease the generalizability of the results.
The results of this propensity score–matched retrospective study detected a significantly greater improvement in the HOOS sports and recreation subdomain outcomes among patients undergoing HRA, as compared with those undergoing THA. The detection of an improvement in some of the HOOS subdomains at 2 years after surgery stands in contrast to some previous studies comparing functional outcomes between HRA and THA. For instance, one randomized, controlled trial demonstrated no difference in QOL between metal-on-metal hip resurfacing and uncemented metal-on-metal THR after 1.1 years or in gait at 3 months [13, 23]. Additionally, Lavigne et al. compared functional outcomes between large-head THA with HRA and found similar results in gait speed, postural balance, functional testing, and clinical data up to 12 months after surgery [23]. However, our findings are supported by the results of other studies that demonstrated higher activity scores after metal-on-metal hip resurfacing when compared with either metal-on-metal hip replacement or metal- or ceramic-on-polyethylene THA [22, 34, 45, 48]. For instance, in a case series reported by Lingard et al. comparing THA and HRA patients, at 1 year, there were significantly better Western Ontario and McMaster Universities Osteoarthritis Index pain scores and all SF-36 domains, as well as greater improvement in general health in the HRA group [26]. Similarly, Pollard et al. reported higher University of California at Los Angeles (UCLA) activity scores and EuroQol QOL scores when comparing 54 patients undergoing HRA with 54 patients undergoing hybrid THA at 5 to 7 years after surgery [38]. These comparative studies were limited, however, by the use of hybrid fixation for the THAs, which has been shown to fail prematurely in patients under the age of 50 with osteoarthritis and may not be generalizable to the current indications for hip resurfacing [1, 43]. The present study reflects the results of modern indications for HRA, and readers should keep in mind that female patients undergoing HRA have poorer Harris hip scores and higher complication rates than male patients [10, 18]. Additionally, it should be noted that even though the patient populations in our study were closely matched, the higher satisfaction rate and higher HOOS activity score shown in our results, though statistically and clinically significant, are relatively small.
The present study did not detect a difference between the two groups with regard to most of the post-operative complications, the exception being self-reported limping. This may be explained by the findings of Ghomrawi et al., who noted patients undergoing HRA had expectations of higher post-operative activity and a greater expectation of “getting rid of limp” and may therefore have been less likely to report post-operative limping [14]. The present study failed to detect a difference in revision rates, although it was not sufficiently powered to detect such a difference. Interestingly, our study detected a significantly shorter hospital stay in the HRA group than in the THA group. This is similar to the findings of an unmatched retrospective cohort comparison by Ward et al., which noted shorter stays in an HRA group, as compared with a THA group [49]. Finally, the dislocation rate was not different between the two groups. Despite a nearly circumferential capsulotomy and lower head-to-neck ratio in the HRA group, our study did not find an increased risk of instability events between the two groups.
In conclusion, despite its limitations, the present study demonstrated that HRA provided modest functional benefit with regard to a single HOOS subscore and greater satisfaction in those patients who met currently recommended criteria, without increases in short-term adverse events or revision. This study did not detect significant differences across all domains. Concerns regarding metal ion levels, pseudotumors, femoral neck fractures, and other complications are not resolved by the current study, and in this limited population of hip arthroplasty patients, pre-operative counseling should focus on balancing the possible functional benefits against the longer-term risks associated with metal-on-metal bearings. Given the known risks of metal-on-metal bearings, and the fact that the differences in PROMs appear to be modest, further studies should attempt to clarify the subsets of the population who may benefit most from HRA. Finally, our results may support identifying alternative bearings for HRA, so that its functional benefits could be achieved without the elevated risks seen with metal-on-metal bearings.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2019_9729_MOESM1_ESM - What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis
Electronic supplementary material, 11420_2019_9729_MOESM1_ESM for What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis by, Alexander S. McLawhorn, MD, MBA, Leonard T. Buller, MD, Jason L. Blevins, MD, Yuo Yu Lee, MS, Edwin P. Su, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9729_MOESM2_ESM - What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis
Electronic supplementary material, 11420_2019_9729_MOESM2_ESM for What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis by, Alexander S. McLawhorn, MD, MBA, Leonard T. Buller, MD, Jason L. Blevins, MD, Yuo Yu Lee, MS, Edwin P. Su, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9729_MOESM3_ESM - What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis
Electronic supplementary material, 11420_2019_9729_MOESM3_ESM for What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis by, Alexander S. McLawhorn, MD, MBA, Leonard T. Buller, MD, Jason L. Blevins, MD, Yuo Yu Lee, MS, Edwin P. Su, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9729_MOESM4_ESM - What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis
Electronic supplementary material, 11420_2019_9729_MOESM4_ESM for What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis by, Alexander S. McLawhorn, MD, MBA, Leonard T. Buller, MD, Jason L. Blevins, MD, Yuo Yu Lee, MS, Edwin P. Su, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2019_9729_MOESM5_ESM - What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis
Electronic supplementary material, 11420_2019_9729_MOESM5_ESM for What Are the Benefits of Hip Resurfacing in Appropriate Patients? A Retrospective, Propensity Score-Matched Analysis by, Alexander S. McLawhorn, MD, MBA, Leonard T. Buller, MD, Jason L. Blevins, MD, Yuo Yu Lee, MS, Edwin P. Su, MD, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
Compliance with Ethical Standards
Conflict of Interest:
Alexander S. McLawhorn, MD, MBA; Leonard T. Buller, MD; Jason L. Blevins, MD; and Yuo-Yu Lee, MS, declare that they have no conflicts of interest. Edwin P. Su, MD, reports receiving grants, personal fees as a consultant, and non-financial support from Smith & Nephew; personal fees as a consultant and non-financial support from United Orthopedic Corp.; non-financial support from OrthAlign Inc.; and ownership and investment interest in Insight Medical Systems.
Human/Animal Rights:
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent:
Informed consent was waived from all patients for being included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.