
Abstract

Introduction
“Osteochondral lesion” is an umbrella term used for an array of disorders related to the subchondral bone and overlying cartilage, including osteochondritis dissecans (OCD) and osteochondral fractures [8, 12, 26]. These injuries constitute an increasing health burden on the growing numbers of recreational and professional athletes of all ages [14]. Among surgical treatment options, the use of bioabsorbable-implant fixation has proven to be an effective alternative to metallic screws [5]. Despite having the advantage of obviating the need for additional surgery for implant removal, bioabsorbable implants are associated with a number of complications, including local tissue reaction, implant breakage, and fixation failure [9, 27, 30]. Prompt and accurate diagnosis of such complications improves clinical decision making and increases the effectiveness of restorative treatments.
The purpose of this article is to highlight how magnetic resonance imaging (MRI) can be employed to detect complications of bioabsorbable implants in patients treated surgically for osteochondral lesions. In particular, we highlight a three-dimensional spoiled gradient–recalled acquisition in steady state (3D-SPGR) protocol that has been shown to be effective. In doing so, we aim to provide orthopedic surgeons with a practical knowledge base for collaborating with radiologist colleagues to enhance MRI visualization of bioabsorbable implants.
Osteochondral Lesions
Osteochondritis dissecans (OCD) is itself a term commonly used to describe a subset of lesions that are thought to develop as a result of microtrauma or repetitive microtrauma to subchondral bone in a watershed area of bone at particular risk for such injury. This primary bone pathology may result in secondary injury to overlying cartilage. Conversely, an osteochondral fracture occurs when an acute trauma disrupts the subchondral bone as well as the overlying articular cartilage [12].
Although epidemiologic evidence that accounts for this broad category of disorders is lacking, OCD has an estimated prevalence of 9.5 to 29 per 100,000 population, with an increased predilection in male adolescents [8]. The lateral aspect of the medial femoral condyle is the classic location for osteochondral lesions, yet they also present frequently in the elbow and ankle and, less commonly, in the shoulder and hip [4, 11, 19]. Given that repetitive microtrauma, at least theoretically, plays a role in the pathogenesis of osteochondral lesions, social patterns of sport specialization and year-round competition may increase the incidence of osteochondral lesions in adolescents [3]. Surgical management of unstable OCD lesions has also demonstrated favorable treatment outcomes in older, skeletally mature patient populations [17].
The American Academy of Orthopaedic Surgeons has established clinical practice guidelines for the management of osteochondral lesions [6]. In many adolescent patients with open physes, osteochondral injuries can be treated with non-operative management consisting of activity modification and rest from high-impact sporting activities. In patients who fail 3 to 6 months of non-operative treatment, surgical management may be indicated. Arthroscopic drilling can be performed in patients with stable lesions, whereas in those with partially or fully detached lesions, surgical fixation is indicated [8].
Bioabsorbable-Screw Fixation
Metallic screws have traditionally been employed in surgical fixation of unstable osteochondral lesions to ensure a stable environment for subchondral bone healing [13, 14, 29]. Although this technique has resulted in favorable outcomes, metallic-screw fixation necessitates a second procedure for hardware removal. Metal screws also interfere with post-operative evaluation by introducing a metal artifact that distorts subsequent MRI [20]. In response, novel implant designs consisting of degradable polymers have emerged as alternative means of osteochondral lesion fixation. There is no need for hardware removal with biodegradable screws, and they enable post-operative monitoring of lesions with MRI [5]. Tissue harvesting from donor sites is also unnecessary. In biomechanical testing, the fixation strength of bioabsorbable screws is equal to that of metallic screws [28]. Clinical studies have demonstrated encouraging outcomes when bioabsorbable screws are used for unstable osteochondral lesions [2, 7, 16].
Currently available bioabsorbable implants are composed of a specific ratio of different polymers that ensures that they are sufficiently stable to promote fracture healing yet also retain the capacity for degradation. The rate of degradation, in turn, helps determine the host's immunological response to the implant, with faster degradation leading to increased local tissue reaction [31]. The earliest generations of bioabsorbable screws were plagued by significant adverse local tissue reaction. Implant design has evolved, with those made primarily of polyglycolic acid being replaced by those consisting primarily of polylactic acid, which prolongs degradation time and, consequently, reduces adverse local tissue reaction [24].
Despite such improvements, local tissue reaction still occurs, typically within the first 6 to 12 months after implantation [9, 27]. In addition, screw breakage is the leading source of surgical complications, occurring in up to 20% of patients in some reports and often causing mechanical symptoms that can necessitate revision surgery [5]. Camathias et al. [5] noted cartilage defects in patients requiring revision arthroscopy for removal of broken screws. It is unknown whether implant-induced cartilage injuries predispose patients to an accelerated progression of arthritis, although the potential for long-term sequelae from complications associated with bioabsorbable nails highlights the need for timely detection and accurate characterization of post-surgical pathoanatomy.
Post-Operative MRI
Although radiographs remain the first-line imaging modality for the diagnosis and ongoing evaluation of osteochondral lesions, MRI provides the clinician with unmatched high-resolution three-dimensional visualization of soft tissue structures [25]. The treating surgeon may elect to obtain an MRI scan in patients who report mechanical symptoms of the joint, a persistent loss in range of motion, or refractory pain and swelling.
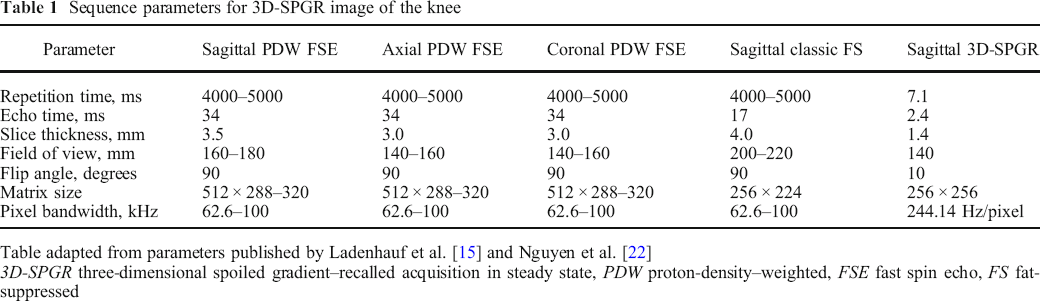
In the evaluation of skeletally immature patients, our institution routinely acquires a 3D-SPGR image using a surface coil. Multiplanar 3D-SPGR is performed using a previously described institutional set of MRI parameters (Table 1) [15, 22]. 3D-SPGR is a readily available, non-proprietary pulse sequence that can be easily integrated into existing clinical practices of both radiologists and orthopedic surgeons. This protocol demonstrates superior physeal cartilage characterization and can be performed using a 1.5-Tesla or 3.0-Tesla magnet (GE Healthcare, Waukesha, WI, USA) [22, 25]. 3D-SPGR has the advantage of faster image acquisition, thereby limiting motion artifact, which can be particularly problematic in younger patients undergoing MRI [23].
Sequence parameters for 3D-SPGR image of the knee
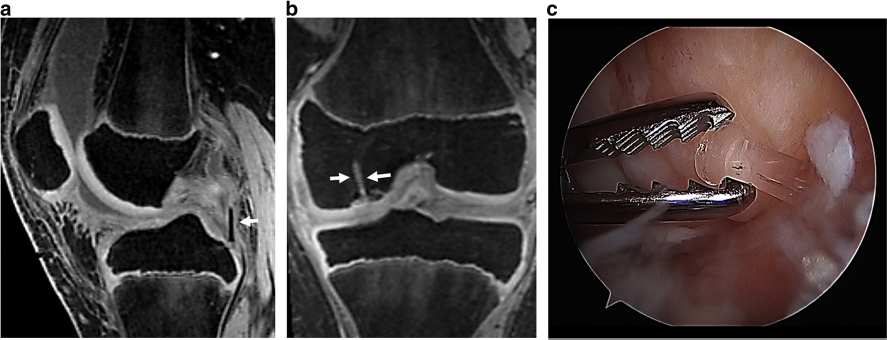
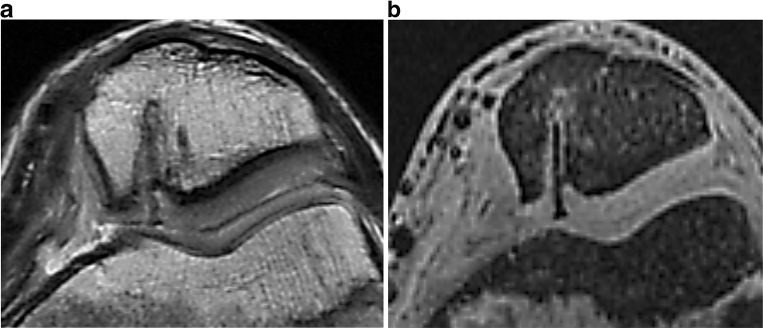
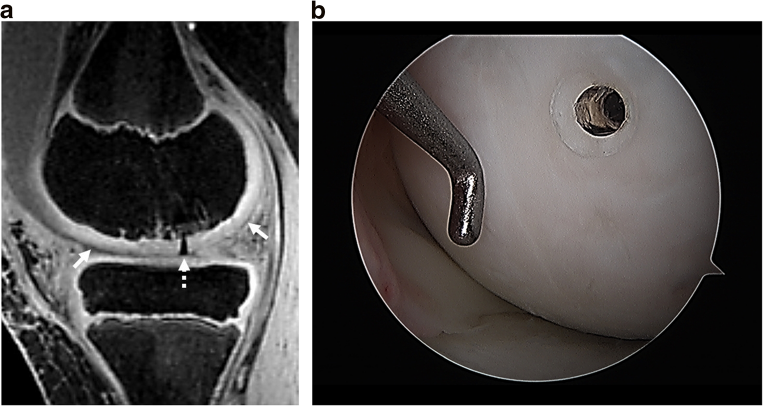
We have discovered a secondary use for this sequence: detecting fractured and dislodged bioabsorbable nails. 3D-SPGR is extremely sensitive to inhomogeneity in the magnetic field, making such problems particularly conspicuous (Fig. 1). Conventional MRI sequences such as T1, T2, and proton-density techniques are much less sensitive to the magnetic perturbations caused by these nails (Fig. 2). 3D-SPGR has high spatial resolution and shows hyaline cartilage with higher signal intensity [10, 18]. The sequence confers a high contrast-to-noise ratio, facilitating its ability to visualize cartilage amid the surrounding structures within the knee. Fat suppression further improves the image contrast by dampening the signal of adjacent bone marrow [32]. Additionally, this enables the treating surgeon to see the progression of healing between parent and progeny bone after fixation. Because use of a physeal-sensitive gradient sequence is not routine in musculoskeletal MRI, it is recommended that the treating surgeon communicate with the consulting radiologist regarding its use for post-operative evaluation. Early identification of complications related to bioabsorbable nails facilitates prompt treatment (Fig. 3).
The timeline for nail degradation is an important consideration for clinicians interpreting post-operative MRI. Edema is identified by regions of high signal intensity surrounding implants on fluid-sensitive sequences. In an analysis by Camathias et al. of 24 patients who were treated with biodegradable screws and underwent MRI at 6-month intervals for a minimum of 2 years, edema was present around 56% of screws at the 6-month evaluation [5]. However, no edema was seen around any screws at subsequent visits. In a study of bioabsorbable pins placed in osteochondral lesions of the ankle, Nakasa et al. [21] theorized that bone marrow edema visible on MRI that persists beyond 6 months may signal the development of osteolytic changes surrounding the implant. Ongoing processes of polymer degradation and bony ingrowth lead to heterogenous signal intensities that become increasingly difficult to interpret. By 2 years after surgery, the signal intensity at the implant site cannot be distinguished from that in the surrounding native tissue [1, 22]. Further research is needed to guide our understanding of the signal intensity patterns that emerge over the course of polymer degradation.
In conclusion, osteochondral lesions are increasingly prevalent and can affect the cartilage and subchondral bone in a variety of joints, most commonly the knee, elbow, and ankle. Bioabsorbable implants offer a means of treating unstable lesions without the morbidity associated with follow-up surgery to remove metallic screws. Heterogenous polymer degradation patterns pose a challenge with respect to post-operative MRI. Accurate interpretation of MRI scans of bioabsorbable implants requires collaboration between the treating surgeon and radiologists. Based on our institutional experience, we recommend that post-operative 3D-SPGR be requested to improve detection of bioabsorbable implants in order for complications to be expeditiously diagnosed and treated. Bone marrow edema surrounding bioabsorbable implants is expected to be visible on MRI for approximately 6 months after surgery, although further study is needed to understand how persistent peri-implant edema affects clinical outcomes.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2020_9771_MOESM1_ESM - Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide
Electronic supplementary material, 11420_2020_9771_MOESM1_ESM for Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide by, Christopher M. Brusalis, MD, Harry G. Greditzer IV, MD, Peter D. Fabricant, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9771_MOESM2_ESM - Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide
Electronic supplementary material, 11420_2020_9771_MOESM2_ESM for Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide by, Christopher M. Brusalis, MD, Harry G. Greditzer IV, MD, Peter D. Fabricant, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9771_MOESM3_ESM - Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide
Electronic supplementary material, 11420_2020_9771_MOESM3_ESM for Using Magnetic Resonance Imaging to Identify Complications Associated with Bioabsorbable Implant Fixation of Osteochondral Lesions: A Practical Guide by, Christopher M. Brusalis, MD, Harry G. Greditzer IV, MD, Peter D. Fabricant, MD, MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
Compliance with Ethical Standards
Conflict of Interest:
Christopher M. Brusalis, MD, Harry G. Greditzer IV, MD, and Peter D. Fabricant, MD, MPH, declare that they have no conflicts of interest.
Human/Animal Rights:
N/A
Informed Consent:
N/A
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.