
Abstract
Background
Emotional and social characteristics may influence rehabilitation and recovery after traumatic brachial plexus injury.
Purposes
We sought to investigate if traumatic brachial plexus injury patients have different levels of social support and employ distinct coping strategies from uninjured control subjects. In addition, we studied which coping strategies are more commonly used among traumatic brachial plexus injury patients.
Methods
Questionnaires for social support (Interpersonal Support Evaluation List and Social Support Questionnaire) and coping strategies (Brief-Coping Orientation to Problems Experienced) were administered to traumatic brachial plexus injury patients and an age- and sex-matched volunteer cohort (without brachial plexus injury).
Results
There were no differences in interpersonal support (mean [SD] = 26.0 [8.6], 26.5 [6.8]), number of persons available for emotional support, and satisfaction with support between traumatic brachial plexus injury patients (n = 36) and volunteers (n = 43). The following coping strategies were more common among traumatic brachial plexus injury patients: active coping, self-distraction, denial, behavioral disengagement, venting, planning, self-blame, and acceptance.
Conclusion
Patients with traumatic brachial plexus injury have similar levels of social support as healthy volunteers but are more likely to use an array of coping strategies. Surgeons and other clinicians should be aware of coping strategies favored by patients, particularly the potential for behaviors detrimental to recovery such as behavioral disengagement, self-blame, and denial. This work will inform future investigations into the influence of social support and coping strategies on clinical outcomes after traumatic brachial plexus injury.
Introduction
Traumatic brachial plexus injuries [tBPI] result in a sudden decrease or complete loss of upper extremity function. Due to the time-sensitive nature of the disease process, early efforts are traditionally focused on restoring upper extremity function through physical therapy and surgical reconstruction. However, recent qualitative studies have suggested that the profound emotional and psychological elements of these injuries may affect recovery after tBPI [7, 15]. Because social support and coping strategies are two key emotional components in recovery from trauma, a better understanding of these approaches within tBPI patients must be gained to maximize patient engagement in the recovery process [7, 15, 16]. Franzblau and Chung conducted a study involving 12 patient interviews and found that acceptance, active coping, and planning were three coping mechanisms often used within the tBPI population [6]. However, further investigation into the quantity and quality of social supports and comparison of these coping strategies with a healthy age- and sex-matched cohort will help increase the understanding of the unique psychosocial dynamics of this population.
The purpose of our study was to examine the levels of social support in tBPI patients and the coping strategies they employ. Comparison of tBPI patients with uninjured volunteer control participants will provide insight into how tBPI patients adjust to a new reality marked by some element of permanent disability, possible inability to return to work and lower earning potential, affected relationships, and higher rates of PTSD, depression, and anxiety [7, 8, 15]. Given the devastating nature of their injury, we hypothesized that tBPI patients have different levels of social support and distinct coping strategies compared with age- and sex-matched controls. A greater understanding of the social support and coping strategies for tBPI patients can facilitate comprehensive, interdisciplinary care during the recovery process.
Methods
This cross-sectional study was approved by our Institutional Review Board and all research subjects provided informed consent.
Over a 6-month period, we recruited all known tBPI patients over age 18 years either by telephone or during planned visits to our peripheral nerve clinic. Patients about to undergo surgical reconstruction (pre-operative) and those already treated surgically (post-operative) were included. All patterns/severities of brachial plexus injuries were included, but isolated peripheral nerve injuries (to the median, radial, ulnar, musculocutaneous, and axillary nerve) were excluded. Patients with significant comorbid neurologic, ipsilateral thoracic, or upper extremity injuries were excluded. Injury severity categorization was performed by the senior author, a fellowship-trained hand surgeon with additional training in peripheral nerve surgery. Recruitment was conducted by a research coordinator either in person (following clinic visits) or by telephone. A total of 36 subjects agreed to participate in the study and three patients declined. No additional follow-up was needed.
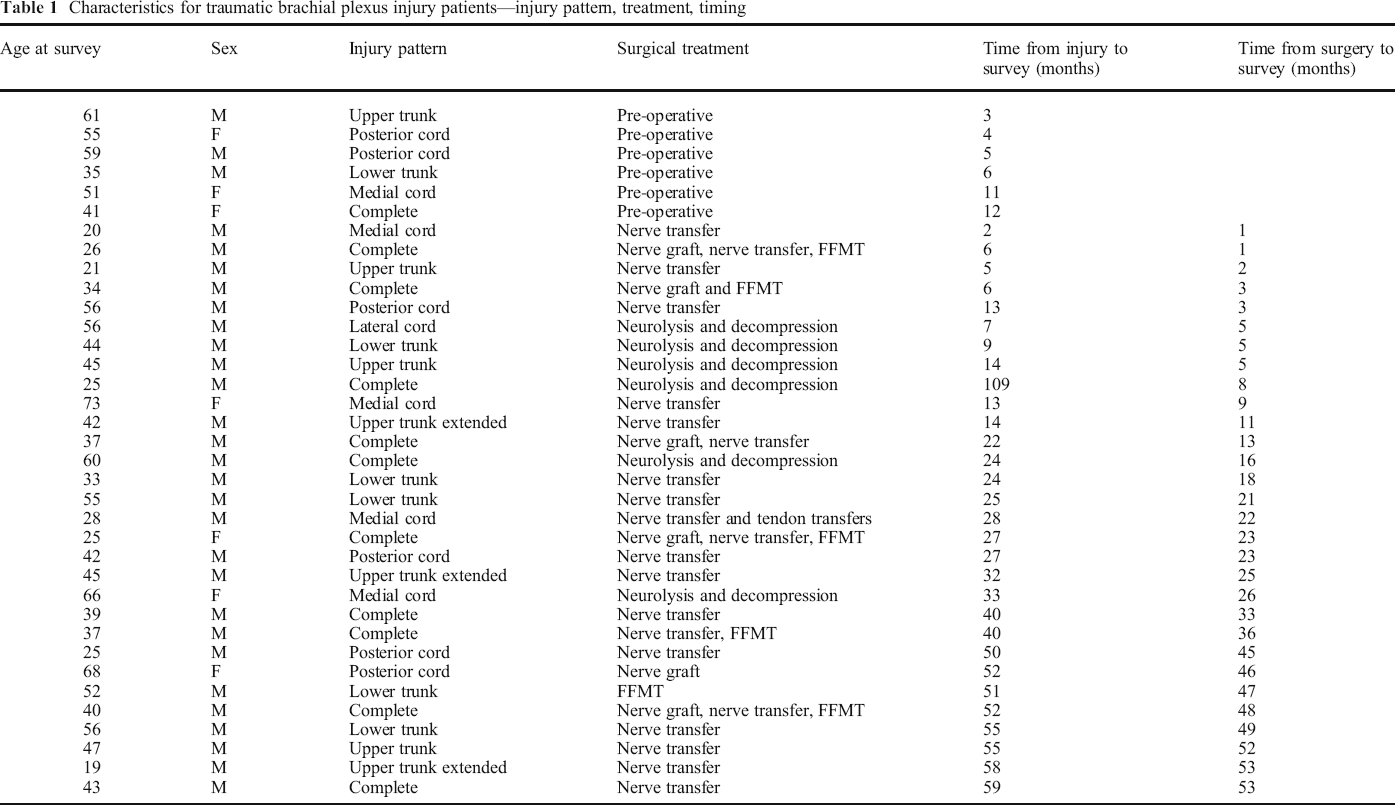
We enrolled 36 tBPI patients and 43 healthy volunteers. Data for all outcome measures followed a normal distribution when assessed with skewness and kurtosis. Among the 36 tBPI patients, 6 completed the surveys before surgery, 11 completed the surveys ≤ 12 months after surgery, and 19 completed the surveys > 12 months after surgery. Eleven patients had a complete/panplexus injury pattern, seven had an upper trunk or upper trunk extended pattern, six had a lower trunk pattern, and 12 had infraclavicular cord-level injuries (Table 1).
Characteristics for traumatic brachial plexus injury patients—injury pattern, treatment, timing
The enrolled tBPI patients were age- and sex-matched to adults in a healthy volunteer cohort. Age matching was performed within ranges: 18 to 34, 35 to 44, 45 to 54, 55 to 64, and > 65 years. Participants were recruited from an institution-managed repository of research volunteers. Healthy participants provided informed consent via telephone and were given $15 gift cards to a national retail store for their participation. All 43 contacted volunteers agreed to participate in the study and none declined.
Surveys were subsequently administered to both groups via email using the secure Research Electronic Data Capture (REDCap) System. We used the following questionnaires: Interpersonal Support Evaluation List (ISEL-12), Social Support Questionnaire 6 (SSQ-6), and Brief Coping Orientation in Problems Experienced (Brief-COPE). These surveys were selected based on their validation in prior studies and on their applicability to answering our research questions.
The ISEL-12 is a previously validated questionnaire measuring respondents’ perceived social support [1, 4, 5, 12, 14, 18]. It is derived from the original 40-item ISEL and contains 12 items graded on a four-point Likert scale (“definitely false,” “probably false,” “probably true,” “definitely true”). The questionnaire contains three different subscales designed to measure three dimensions of perceived social support: appraisal support, belonging support, and tangible support. The survey is scored as a continuous variable after reverse coding for some items to yield a score between 0 and 36. Higher scores are associated with a higher perceived availability of social support [4, 12]. The ISEL-12 has been used to assess patients with rheumatoid arthritis, hypertension, and those requiring long-term care for spinal cord injury [1, 5, 14, 18].
The SSQ-6 is a previously validated six-item measure of social support [19]. For each of the six items, respondents indicate the number of people available to them for social support in different facets of their life. For example, “Who accepts you totally, including both your worst and your best points?” Or, “Who can you count on to console you when you are very upset?” Respondents then grade their satisfaction with that support on a six-point Likert scale (“very dissatisfied,” “fairly dissatisfied,” “a little dissatisfied,” “a little satisfied,” “fairly satisfied,” “very satisfied”). The SSQ-6 has been extensively used to study patients with human immunodeficiency virus [2, 14]. Whereas ISEL-12 assesses participant's perceived availability of social support, SSQ-6 assesses how many persons are available for support and how satisfied they are with this perceived social support [19].
The Brief-COPE is a 28-item questionnaire that assesses the frequency with which respondents use 14 different coping strategies [3]. Each coping mechanism is assessed by two questions. For instance, measurement of “religion” as a coping mechanism is assessed by respondents’ answers to “I've been trying to find comfort in my religion or spiritual beliefs,” and “I've been praying or meditating.” The respondents use a four-point Likert scale (“I haven't been doing this at all,” “I've been doing this a little bit,” “I've been doing this a medium amount,” “I've been doing this a lot”). The Brief-COPE results are not designed to be analyzed in aggregate; rather, each coping mechanism scale is analyzed separately. The Brief-COPE has been previously administered to patients with spinal cord injury and burns [9, 20]. Additionally, Franzblau and Chung also used the Brief COPE to examine coping strategies among tBPI patients [6].
Our primary outcome was the ISEL-12, which can be analyzed as a continuous variable [5]. We compared the tBPI and healthy volunteer control groups using a two-tailed Student's t test, with the null hypothesis that the ISEL-12 is equal between the two groups. Because a minimal clinically important difference has not been established for the ISEL-12, we selected a difference of four as having a clinically relevant impact. With the assistance of a biostatistician, to perform an a priori sample size calculation to detect a mean difference of four between groups, assuming a within-group standard deviation of 5.8, based on prior work by Cooper et al. [5]. A minimum of 34 patients in each group would be necessary to detect a mean difference of four on the ISEL-12 with a power of 80% and alpha = 0.05.
Our secondary outcomes were the SSQ-6 and the individual coping strategies reported in the Brief-COPE. Both components of the SSQ-6 were analyzed as continuous variables using a two-tailed t test to maintain consistency with prior studies [10, 13, 17]. The possible score range for the number of supports in the SSQ-6 is 0 to 54. The possible score range for the satisfaction with supports in the SSQ-6 is 6 to 36. Individual coping strategies of the Brief-COPE are each assessed with two questions, with a possible maximum score of eight for each coping strategy. The Brief-COPE is not designed to be analyzed as an aggregate measure. We compared use of each coping strategy between groups using a two-tailed t test. Effect size was calculated using Cohen's d. For all outcomes, we planned to assess normality of data distribution and use non-parametric tests if the data did not follow a normal distribution. All statistical analysis was preformed using the IBM SPSS Version 26.0 (Armonk, NY, USA
Results
Patients with tBPI (mean [SD] = 26.0 [8.6]) and healthy volunteers (mean [SD] = 26.5 [6.8]) scored similarly (p = 0.73, d = 0.07, CI = 23.9, 27.4) on the ISEL-12 assessment of interpersonal support. On the SSQ-6, there was no difference in the number of persons listed as available for emotional support (p = 0.59, d = 0.1, CI = 2.8, 3.9) (Table 2). Traumatic BPI patients and healthy volunteers reported similar levels of satisfaction with these relationships (p = 0.30, d = 0.2, CI = 4.3, 4.8)
Assessment of social support using the Interpersonal Support Evaluation List-12 (ISEL-12) and Social Support Questionnaire-6 (SSQ-6)

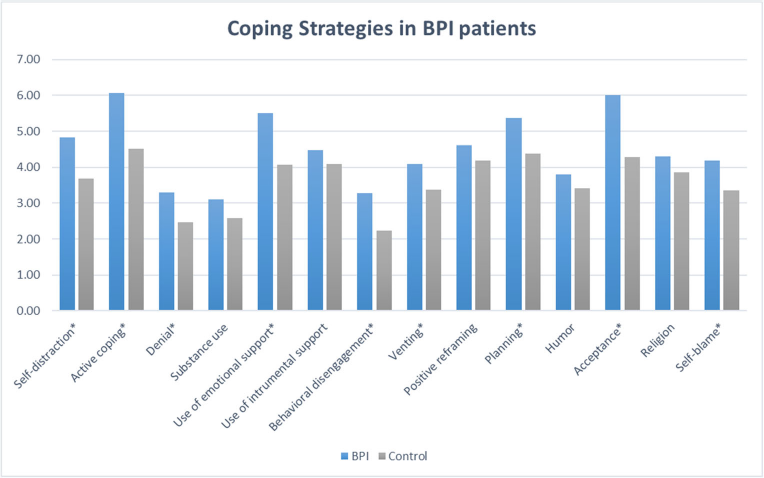
Coping strategies employed by tBPI patients and healthy volunteers. Asterisks indicate signficant difference (p < 0.05) between the two groups.
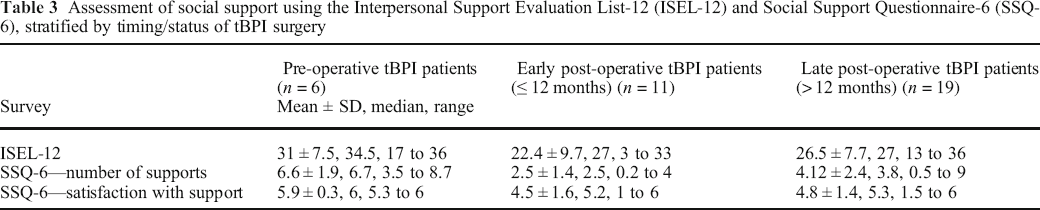
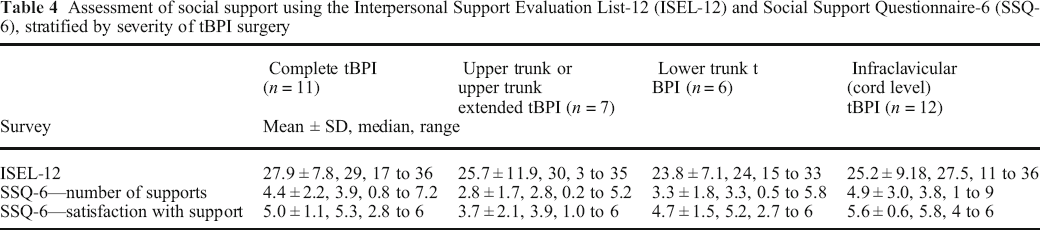
We separately tabulated the ISEL-12 and SSQ-6 based on injury severity and timing of survey administration (using 12 months as an arbitrary designation between “early” and “late” after surgery). These tabulations for social support measures (ISEL-12 and SSQ-6) are presented in Tables 3 and 4 and Figs. 2 and 3. We did not perform any comparative statistical analyses based on timing of survey administration or severity of injury, as we were not powered adequately for those comparisons. A small number of surveys were missing one or more answers; in this case, the entire survey data was excluded from the analysis.
Assessment of social support using the Interpersonal Support Evaluation List-12 (ISEL-12) and Social Support Questionnaire-6 (SSQ-6), stratified by timing/status of tBPI surgery
Assessment of social support using the Interpersonal Support Evaluation List-12 (ISEL-12) and Social Support Questionnaire-6 (SSQ-6), stratified by severity of tBPI surgery
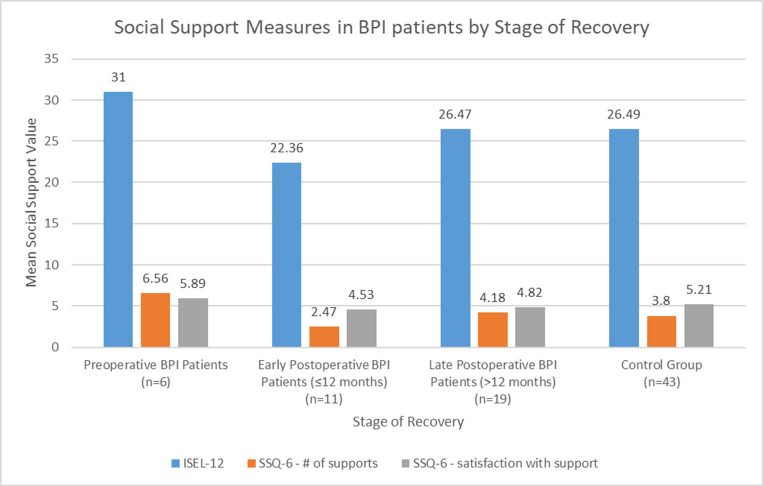
Mean value of social support measures among pre-operative tBPI patients, early post-operative tBPI patients (≤ 12 months from surgery), late post-operative tBPI patients (> 12 months from surgery), and healthy volunteers (tBPI = traumatic brachial plexus injury; ISEL-12 = Interpersonal Support Evaluation List-12; SSQ-6 = Social Support Questionnaire-Short Form).
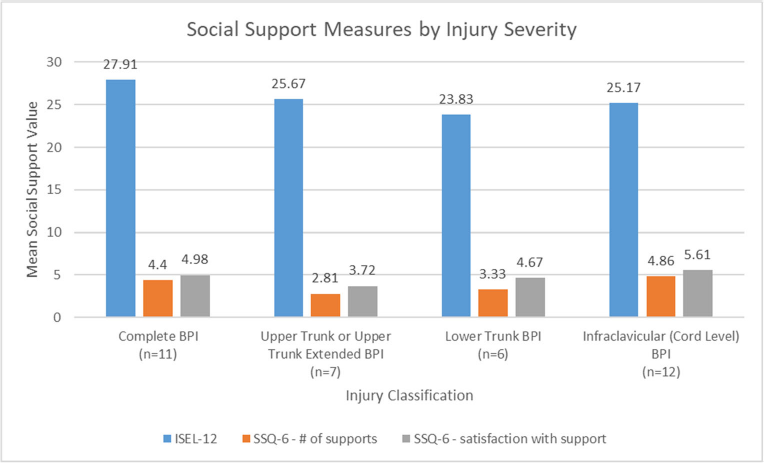
Mean value of social support measures stratified by injury severity (tBPI = traumatic brachial plexus injury; ISEL-12 = Interpersonal Support Evaluation List-12; SSQ-6 = Social Support Questionnaire-Short Form 6).
Discussion
We demonstrated nine specific coping mechanisms that were more significantly used in the tBPI population, including active coping, self-distraction, denial, use of emotional support, behavioral disengagement, venting, planning, self-blame, and acceptance. Increased use of coping mechanisms among the tBPI cohort demonstrates the traumatic nature of injury and potential need for supplemental psychosocial support during the disease process. Our data support the findings of Franzblau and Chung, who found that acceptance, active coping, and planning were three coping mechanisms often used within the tBPI population [6]. We built on their findings by demonstrating the coping mechanisms present in tBPI patients compared with a healthy, age-, and sex-matched cohort. In addition to acceptance, active coping, and planning, traumatic BPI patients were more likely to use self-distraction, denial, emotional support, behavioral disengagement, venting, and self-blame. Additionally, patients who have at least 12-month post-surgical treatment were more likely to employ acceptance and self-blame than those earlier in their recovery, while timing did not seem to affect the use of other coping strategies. Identification of this array of coping strategies can guide care providers from multiple disciplines as they interact with tBPI patients, emphasizing the importance of referral to resources such as mental health professionals and social workers during the recovery process. While provider discretion should be exercised when focusing on a singular aspect of a patient's array of coping strategies, special consideration should be paid to the potential for behaviors detrimental to the recovery process such as behavioral disengagement, self-blame, and denial.
Our study carries limitations due to its cross-sectional nature. As mentioned above, our tBPI cohort has patients who completed the surveys before surgery and at various times after surgeries. This limits the generalizability of our findings, as these emotional elements of recovery likely change over time. Many of the injuries among our tBPI cohort injuries occurred within the last 3 years and may not account for further loss of social support over an extended period of time after injury (> 3 years). However, by combining patients from multiple time points we were able to examine characteristics that distinguish tBPI patients from healthy, age-, and sex-matched controls with adequate statistical power. While we included patients with all levels of severity of traumatic brachial plexus injuries, we did not have a large enough sample size to compare the influence of injury severity on social support measures. It is expected that a complete/panplexus injury or lower trunk injury will have a more profound effect on patients than an isolated upper trunk injury, and we are incorporating these assessments into future prospective, long-term follow-up studies.
Social support measures, including availability, quality, and quantity of personal relationships, were similar between tBPI patients and healthy volunteers. It is encouraging that the tBPI cohort has similar support systems compared with healthy volunteers, but it remains unknown whether tBPI patients need higher and more consistent levels of support given the nature of disability, duration of recovery, and impact on mental, physical, financial, and social aspects of life. We did not design our study to empirically evaluate the evolution of social support after surgery, but the tabulations presented in Table 3 and Fig. 2 support prior assertions that the availability and quantity of social support evolve during recovery [6, 11]. While we were not statistically powered to analyze the impact of survey timing, we agree with prior investigators that fewer and better quality relationships may emerge post-operatively and evolve with time [6, 11]. For this reason, longitudinal assessment of the robustness of social support for tBPI patients should be included in future prospective studies.
Surgeons, hand therapists, and other healthcare professionals caring for patients with tBPI should be aware of the emotional and social characteristics that may influence patients’ engagement in the recovery process. While this may be true of all disease and traumatic injuries to some degree, we believe it is especially important in this population given the comprehensive negative implications of the injury. These include permanent physical dysfunction; mental, social, relational, financial, employment, and recreational repercussions; and subsequent loss of support and perceived personal value resulting from these effects. Surgeons and hand therapists caring for tBPI patients should be aware of the patient's social and emotional state, as well as how this evolves during the recovery process. There may be points in which referral to other disciplines, such as psychosocial therapy, pain therapy, or vocational rehabilitation, will be needed to help patients navigate the adjustment to their new reality.
Based on the results of this study and our anecdotal experience in clinical practice, we routinely assess the psychosocial condition of each patient, including their living situation, social supports, as well as their physical and emotional states. Understanding potential issues with social support and coping strategies common to this patient population helps us better identify and address them early. In our multidisciplinary complex nerve clinic, tBPI patients are assessed by peripheral nerve surgeons, hand therapists, pain psychologists, and pain management specialists. Referrals to social work are offered. We have regular multidisciplinary rounds prior to each complex nerve clinic with representatives from each discipline, during which we discuss individual patient needs and concerns for patients before or after BPI reconstruction. This allows us to take advantage of multidisciplinary expertise and provide a proactive and comprehensive strategy for each tBPI patient.
Electronic supplementary material
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM1_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM1_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM2_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM2_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM3_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM3_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM4_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM4_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM5_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM5_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Electronic supplementary material
Electronic supplementary material, 11420_2020_9814_MOESM6_ESM - Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury
Electronic supplementary material, 11420_2020_9814_MOESM6_ESM for Social Support and Coping Strategies in Patients with Traumatic Brachial Plexus Injury by, Ryan Sachar, BA, Andrew J. Landau, MD, Wilson Z. Ray, MD, David M. Brogan, MD MSc, Christopher J. Dy, MD MPH, in HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Electronic supplementary material
Compliance with Ethical Standards
Conflict of Interest:
Ryan Sachar, BA; Andrew J. Landau, MD; Wilson Z. Ray, MD; and David M. Brogan, MD MSc, declare that they have no conflicts of interest. Christopher J. Dy, MD, MPH, reports grants from National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health, outside the submitted work.
Human/Animal Rights:
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent:
Informed consent was waived from all patients included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.