
Abstract
Isolated compression of the recurrent motor branch (RMB) of the median nerve is not commonly reported. This report deals with a case of fascial band compression of the RMB of the median nerve with sparing of the sensory portion of the nerve in a single patient. The episode was precipitated by the subject was clearing fallen trees after an ice storm. Symptoms occurred only in the left, nondominant hand of the patient, a 43-year-old invasive cardiologist. He presented within weeks of symptom onset, but marked clinical and electrodiagnostic abnormalities of the branch were already present. Timely decompression after evaluation led to a successful clinical outcome, with restoration of full strength on manual muscle testing by 6 months postoperatively and marked electrodiagnostic improvements as well by 11 months after operation. Final clinical examination 16 months after operation showed thenar muscle bulk and strength well maintained.
Introduction
Carpal tunnel syndrome is a commonly diagnosed condition [7]. In contrast, isolated compression of the recurrent motor branch (RMB) of the median nerve is not commonly diagnosed and infrequently reported in the medical literature. A single report from 1982 documents fascial bands causing RMB compression in a set of three hands in two patients [1]. These patients had severe thenar atrophy preoperatively. Most other reports of RMB compression have been caused by nearby cystic masses, although other reports have documented RMB abnormalities from Shiatsu massage of the hand, anomalous vessels, or schwannoma formation [2–6, 9, 10].
This case report discusses a case of isolated recurrent motor branch compression with normal sensory findings. The compression was attributable to a fascial band. In this report, the patient sought care within weeks of symptom onset, and thenar muscle bulk was preserved at the time of presentation. Ultimately, this patient had a return of strong antiresistance contraction in the thenar muscles by 6 months after operation, along with a near normalization of electrical parameters as measured by serial electrodiagnostic studies by 11 months after operation. Final clinical evaluation was 16 months after operation. The patient is aware that his case is being presented.
Case Report
The patient in this study was a 43-year-old, right-hand-dominant invasive cardiologist. He had an abrupt onset of left hand weakness after clearing fallen trees in February 2004 following an ice storm. His hand felt “achy” and he noticed difficulty with fine thumb manipulation on the left. He did not have numbness in the left hand. The patient was otherwise healthy, with no medical illnesses, no regular medications, and no prior history of a hand problem. The patient sought a hand surgery evaluation within 2–3 weeks of the onset of his hand weakness.
Upon initial physical examination in March 2004, the patient had the ability to contract his left thenar muscles, but could not contract at all against resistance. Thenar eminence muscle bulk was symmetric on visual inspection, and of a grossly normal size in his hands. Moving two-point discrimination was 5 mm in all digits of both hands. The patient did not have an obvious ganglion or mass in the carpal tunnel or on the palmar aspect of the left wrist on physical examination.
MRI scan taken in April 2004 showed grossly normal carpal tunnel morphology with no mass present in the area of the median nerve. Also, in April 2004, median nerve conduction velocity (NCV) studies showed severe abnormality of thenarmotor input (latency >10.6 ms, amplitude 0.6 mV, velocity 35.4 m/s), and median sensory findings within normal range (latency 3.25 ms, amplitude 20.2 mV, velocity 54.9 m/s). Median electromyography (EMG) showed spontaneous insertional activity, 2+ fibrillations, 2+ sharp waves, and 1–3 units on testing of recruitment pattern.
The patient was offered nerve exploration and decompression in May 2004, 3 months after onset of symptoms. He underwent an extended carpal tunnel release via loupe magnification for RMB exploration in May 2004.
During operation, the median nerve was grossly normal morphologically. The RMB had a palmar–radial takeoff point in the distal carpal tunnel, with a transligamentous course into the thenar muscles. A stout fascial band was present at this site and appeared to kink and indent the RMB (Fig. 1). This area was painstakingly decompressed, allowing a more spacious path for the RMB. The nerve had an indention at the fascial compression site, and was pale distal to that site. No neuroma was noted on gross inspection (Fig. 2).
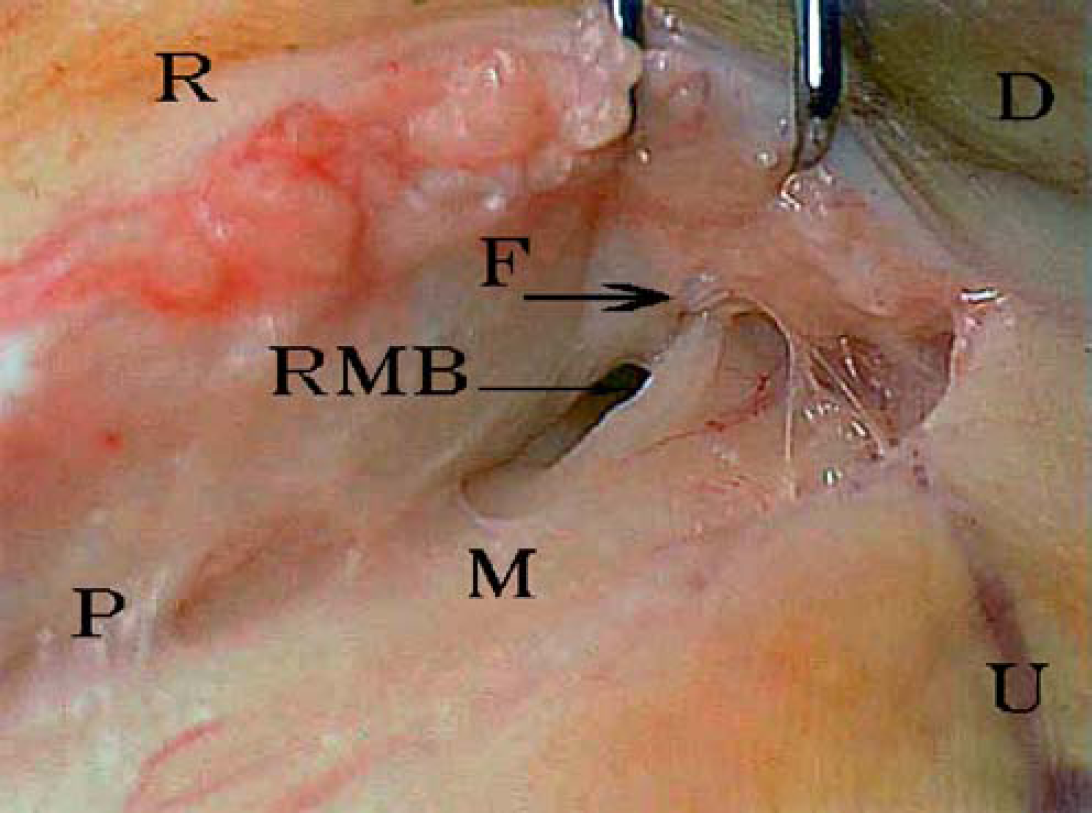
F = fascial band (thick arrow), RMB = recurrent motor branch of the median nerve (thin arrow), M = median nerve, R = radial, U = ulnar, P = proximal, D = distal.
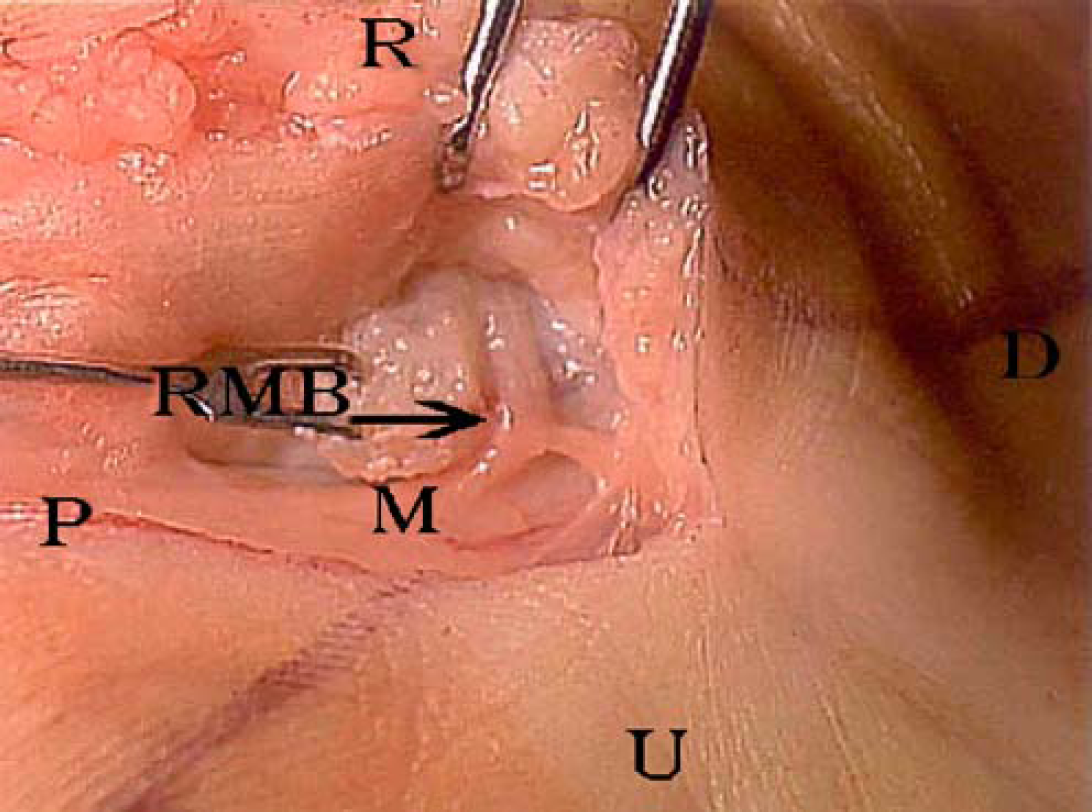
RMB = recurrent motor branch of the median nerve (thin arrow), M = median nerve, R = radial, U = ulnar, P = proximal, D = distal.
The surgical wound was closed in layers over silastic wound strips; a soft bandage was used. Postoperative occupational therapy took place in six visits over the first 8 weeks postoperatively. The first visit was postoperative day 4. The patient combined therapy visits with a home program of dry dressings, tendon gliding, digit blocking, and general hand and wrist active and active assisted range of movement. Sutures were removed on postoperative day 14. Scar massage, retrograde massage for edema, and a nighttime elastomere scar mold were also used. The so-called Russian electrical stimulation (pulsed alternating current stimulation) for the thenar muscles was used 8 min per session twice daily for 8 weeks postoperatively. At the time of suture removal, grip strength was 35 1b in the left, operative extremity and 95 lb in the unaffected extremity, with key pinch 2 lb on the left, 10 lb on the right. At discharge from therapy 8 weeks after operation, left-hand grip strength was 75 lb and key pinch was 4 lb.
The patient reported back for work within 3 weeks. He noted slow, but steady improvement in opposition strength of his thumb over the following months. Manual muscle testing revealed a strong contraction against resistance by 6 months postoperatively. Electrodiagnostic testing (all tests from same doctor and facility) around 6 months after decompression showed thenar motor latency improved to 5.8 ms, amplitude of about 0.6 mV, with resolution of fibrillations and sharp waves, normal insertional activity, and a decreased recruitment pattern.
A final electrodiagnostic test was performed in April 2005, 11 months after operation. The examination showed a motor latency of 4.6 ms and motor amplitude of 4.6 mV. Insertional activity was normal, fibrillations and sharp waves were not present, and recruitment pattern was now normal/full. A physical examination took place in September 2005, 16 months after operation. The thenar muscles on the left side had a strong antiresistance contraction, thenar muscle bulk was approximately equal to the right hand, opposition of the left thumb tip was present to the level of the small finger metacarpal head, and the patient was at work full-time, full-duty in his cardiology practice.
A 2-year postoperative occupational therapy assessment took place in May 2006. Grip strength on a three-trial average was 110 1b on the right and 130 1b on the left. Key pinch averaged 12 1b on both right and left sides.
Discussion
Isolated compression of the recurrent motor branch of the median nerve is not commonly reported. Bennett and Crouch [1] documented fascial compression in 1982. While most other authors have documented compression by cysts, other mechanisms such as vigorous Shiatsu massage and vascular compression are also reported [2–6, 9, 10].
Bennett and Crouch's study reported on three affected hands in two patients. Their 24-year-old patient had had 4 years of atrophy in his left, dominant thenar eminence, and 8 months of atrophy in the right thenar eminence. Electrodiagnostic studies showed normal sensory parameters, but increased motor latency. At operation, the median nerve was grossly normal, but a fascial band compressed the RMB as it traversed the transverse carpal ligament. They reported similar findings on the right-carpal tunnel release and opponensplasty were performed at a second operative session. At 2 years follow-up examination, no thenar motor recovery was noted.
Their second patient was a 64-year-old female. She experienced numbness, tingling and loss of thenar muscle bulk bilaterally, with the right side more severely affected. Electrodiagnostic testing showed a “…severe right median nerve lesion at the wrist with complete denervation of the right APB muscle.” She also had a milder lesion on the left, mostly sensory. At operation, this patient's right RMB was sharply angled at its entry to the transverse carpal ligament, and a neuroma was present proximal to the entry point. This area was decompressed and treated with external neurolysis. Postoperative status was not documented on this particular patient [1].
The two patients reported by Bennett and Crouch had pronounced thenar wasting at initial presentation. In contrast, the patient in this report sought care within 2–3 weeks of symptom onset, so his thenar muscles were well preserved. In the reports of Kato et al. [5] and of Kobayashi et al. [6], timely resection of carpal tunnel ganglion cysts compressing the RMB also led to good recovery. Resection of anomalous muscle causing RMB compression in the report by Yamanaka and coworkers [10] did not lead to clinical improvement in their patient; he presented to his doctors with thenar atrophy already present. Widder and Shons [9] documented clinical and EMG improvement 2 months postoperatively after resection of an anomalous radial artery branch compressing the RMB; their patient had 2 years of preoperative symptoms and had thenar atrophy on initial presentation. Josty and Sykes [4] reported “…full function with no clinically demonstrable motor or sensory deficit…” 6 weeks after enucleation of a schwannoma of the RMB. The patient had noted a thenar mass for 20 years with increased symptoms in the 18 months prior to presentation.
Bennett and Crouch postulated two injury mechanisms in their report: transligamentous fascial compression or distal extraligamentous kinking [1]. The patient in this report had a thickened band present at the entry of the RMB to the transverse carpal ligament, corresponding to the first patient in the Bennett and Crouch report.
In comparing this patient with the patient discussed by Herskovitz and coworkers [2] (transient RMB palsy after a vigorous massage of the hand), the injury mechanism appears similar. In certain patients, it is possible that vigorous stimulation of the palm may cause translation of the motor branch back and forth over the fascial entry point to the transverse carpal ligament. In turn, this may induce an edematous reaction in the nerve, fascia or both, with subsequent swelling and nerve compression. While the patient in the present study exhibited no recovery by 3 months postinjury, the patient in Herskovitz et al. 's report [2] was clinically improving within 4 weeks of onset of symptoms.
While some might argue for observation of this patient, his presentation was abrupt, with severe clinical symptoms. Additionally, severe electrodiagnostic abnormalities consistent with a highly compromised nerve were also present. In light of the paucity of literature for guidance and documented poor outcomes in chronic cases, operative care was undertaken after a 3-month period of observation and evaluation. A supportive postoperative program of occupational therapy helped guide his recovery, including electrical stimulation for thenar muscle contraction during the early recovery period [8]. Serial physical and electrodiagnostic examinations documented subjective and objective recovery from this problem, with grip strength now about 20% greater in the affected hand 2 years after operation.
While highly uncommon, isolated median nerve motor branch compression with sensory preservation can occur. In this case, early decompression after initial observation and evaluation led to an impressive clinical and electrodiagnostic recovery. Clinicians should keep this entity in mind as a possible source of hand dysfunction.
Footnotes
Acknowledgments
The author would like to thank M. David Redmond, MD, Cindy Arnot, R. NCST, and Lynn Williams, R. EDT, for the superb electrodiagnostic care the patient received. The author would like to thank Joe Crisler, OTRL for the superb occupational therapy care the patient received. Todd Hoover, PT of Sumter Physical Therapy for superb care of this patient.