
Abstract
Background
International volunteering missions are becoming an important focus of plastic surgeons in the United States. The purpose of this paper is to describe the teaching of pediatric hand surgery in Vietnam to share the lessons learned from this project.
Methods
Two medical education trips were conducted to the no. 1 Children's Hospital in Ho Chi Minh city (Saigon) to teach pediatric hand and burn reconstructive surgery to the surgeons and therapists. This is the main referral children's hospital for the country, and pediatric hand surgery expertise is not available.
Results
Structured education programs were conducted over two trips to introduce congenital hand surgery and burn reconstructive procedures using flap techniques. The education programs included lectures and surgical demonstrations of selected procedures. Their proficiency was verified by supervised conduct of these operations.
Conclusions
A well-conceived medical education program can introduce complex surgical discipline to a country. Through two trips, the surgeons at this referral center will have the capability to take care of many children requiring reconstructive hand surgery.
Introduction
Hand surgery is a specialty that began during World War II when Dr. Sterling Bunnell was commissioned by the United States Army to set up hand centers throughout the country to take care of the injured. As Hand Surgery has matured in the United States, many hand surgeons are introducing this specialty to other regions of the world. In developing countries, hand injuries are rampant, resulting from rapid industrialization and unsafe working conditions in factories. Children are also susceptible to hand trauma caused by burns from cooking over open fires. Congenital hand conditions are often untreated because hand surgery expertise is not available; rendering these children to lifelong deformity that hinders their integration to society.
The care of surgical problems in developing countries is markedly underdeveloped. For example, there are currently only 400 surgeons in eight East African countries to serve over 200 million people [2], and it can be assumed that plastic surgery is not well represented in the surgical community. In developing countries where social care systems are still in their infancy, the inability to work is a tremendous burden to the family, reducing the victim to helplessness that is beyond our understanding.
Plastic surgeons have the expertise and the obligation to teach hand surgery to the developing world in an effort to elevate the standards of hand and upper limb care in these countries. Children's health is a low priority in the developing world; the probability of a child in the United States born in 2003 dying before he/she reaches 5 years of age is 8 in 1,000 live births, while in Kenya, it is 123 in 1,000 [8]. A large segment of the population in developing countries is children. For the developing world to fully maximize the potential of her population, enhancing the health of children should be the highest priority because a healthy labor force is crucial to the economic growth of a nation.
The purpose of this paper is to describe the introduction of pediatric hand surgery to Vietnam at the major children's hospital in Ho Chi Minh (HCM) city, formerly known as Saigon. While serving in volunteer medical missions can be personally rewarding, understanding local culture and personal capabilities is crucial. Successful volunteering trips can have an important impact to our surgical colleagues and to the children in the countries served. In this paper, I will share my experience in two trips over a course of 6 months at the no. 1 Children's Hospital in HCM city.
Background
Vietnam has an important place in American history. The searing images of children running from the Napalm bombing of a Vietnamese village and the last helicopter evacuation from the top of an apartment building remain etched in our consciousness. After more than 30 years since the end of the Vietnam war or “the American war” that the Vietnamese government proclaimed, Vietnam is now beginning to open up her borders and invite greater economic and cultural interactions with the rest of the world.
Interplast, which has been working on children's health, has an active presence in Vietnam. It carries out several missions to treat facial clefts in remote regions of the country. More recently, Interplast initiated a Medical Educator program whereby a visiting educator will teach surgical principles to local surgeons. Because of the prevalence of hand problems in developing countries, Hand Surgery has become an important specialty program for Interplast to cultivate interest and expertise. When I was asked by Interplast to be the first Hand Surgery Medical Educator at the no. 1 Children's Hospital in HCM city, I was eager to participate in teaching pediatric hand surgery in Vietnam.
To assess the medical needs of Vietnam, one must understand changes in the demographic distribution of the country since the end of the war. The war ended in 1975, and in the 1979 census, Vietnam had a population of 52.7 million [1]. At the end of 1985, the population was almost 60 million [1]. Today, the population is 84 million and 27% of the population is less than 14 years old and have no recollection of the war [6]. The gross domestic product of Vietnam is $232.2 billion and the per capita income is $2,800. Most of the labor force (57%) is involved in agriculture, although industry (food processing, garments, machine-building, mining) contributes to the majority (41%) of the gross domestic product [6]. The number of physicians serving this nation is quite inadequate with 0.5 physicians per 1,000 people, compared to 2.3 physicians per 1,000 people in the United States [5]. As related to me by a junior surgeon at the no. 1 Children's Hospital, the medical school in HCM city graduates about 200 medical students a year. However, less than half of them are able to obtain additional training in a residency position. The rest of the graduating medical students have to find additional sources of work and often are employed as sales representatives for drug companies. Compounding the problem is the lack of surgical training positions in this country. In this premier children's hospital, there are only a few surgical trainees to assume the burden of taking care of a large segment of the population that consists of children. Therefore, an urgent issue for Vietnam is to overhaul the educational system by improving and increasing the number of residency positions for the growing health care needs of the country. Because the training of surgeons is an arduous and prolonged process, it is even more important that qualified surgeons are trained in various surgical disciplines to elevate the overall quality of surgical care.
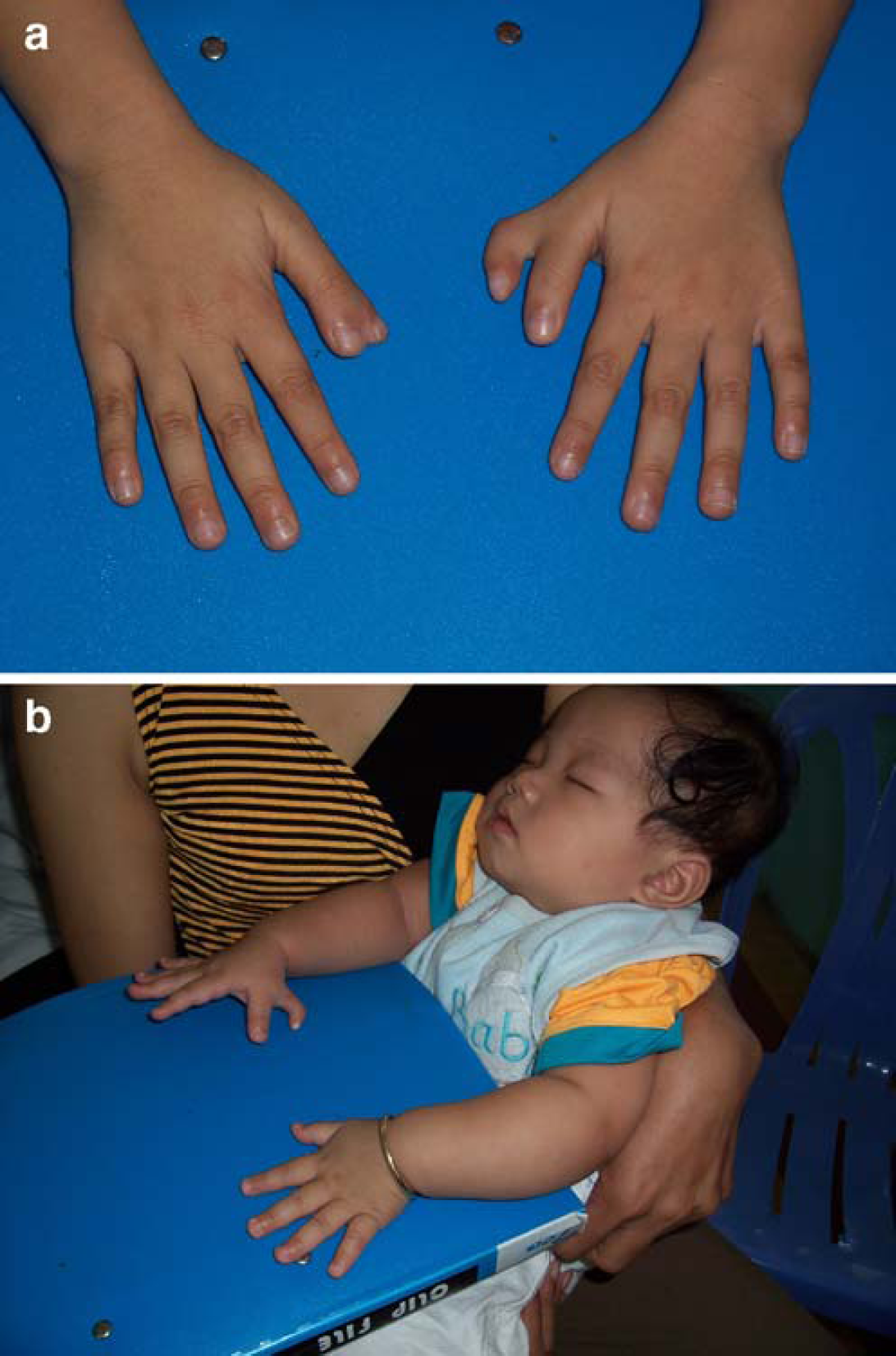
The no. 1 Children's Hospital is the main referral children's hospital in Vietnam (Fig. 1a and b). It serves a region stretching from Central to Southern Vietnam with a catchment area of over 40 million people. This hospital has an excellent burn unit and is expanding its surgical capabilities. In the near future, it will add a pediatric heart program that is complemented by a state-of-the-art intensive care unit. The Department of Burn and Plastic Surgery receives referrals for acute and secondary burn reconstruction problems. Although many children do survive from severe burns, the lack of expertise and equipment for secondary burn reconstruction hampers their rehabilitation. While burn contractures are treated routinely with skin grafting, the application of flaps—either local or distant—is not practiced in this facility. I introduced to them the pedicle groin flap to resurface the entire dorsum of the hand after burn scar excision (Fig. 2a–d). The use of flaps for burn reconstruction will be an important component of their overall burn care program in children. In addition, future introduction of microsurgical techniques will be crucial in addressing many of the difficult burn contracture problems and pediatric congenital conditions.


First Trip
I served in Vietnam during Thanksgiving 2005. It is a special occasion to give thanks for what we have in the United States by providing a much needed service to Vietnam. These educational trips follow Dr. Bunnell's tireless effort to teach hand surgery to underserved regions. My goal was to introduce pediatric hand surgery to Vietnam.
Coordination of this trip to maximize the learning experience for the Vietnamese surgeons proved to be challenging. The relatively inaccessible internet system in Vietnam limited pre-trip communication about their needs. Despite difficulties with drafting an education agenda, all the teaching goals were accomplished, and hurdles were resolved by simply having a face-to-face planning meeting with my hosts upon my arrival. My first day was devoted to screening potential children to demonstrate surgical techniques. I was rather surprised to evaluate eight consecutive children with a variety of duplicated thumb conditions (Fig. 3a and b). Thumb duplication appears to be more common in Asian populations; one Japanese study reported 16% of upper limb congenital anomaly cases over a 16-year period to consist of thumb duplication [3]. Because this is a rather common condition in Vietnam, I was asked to demonstrate various surgical techniques for different duplicated thumb types (Table 1).
Descriptive information for the treated children during first visit*.
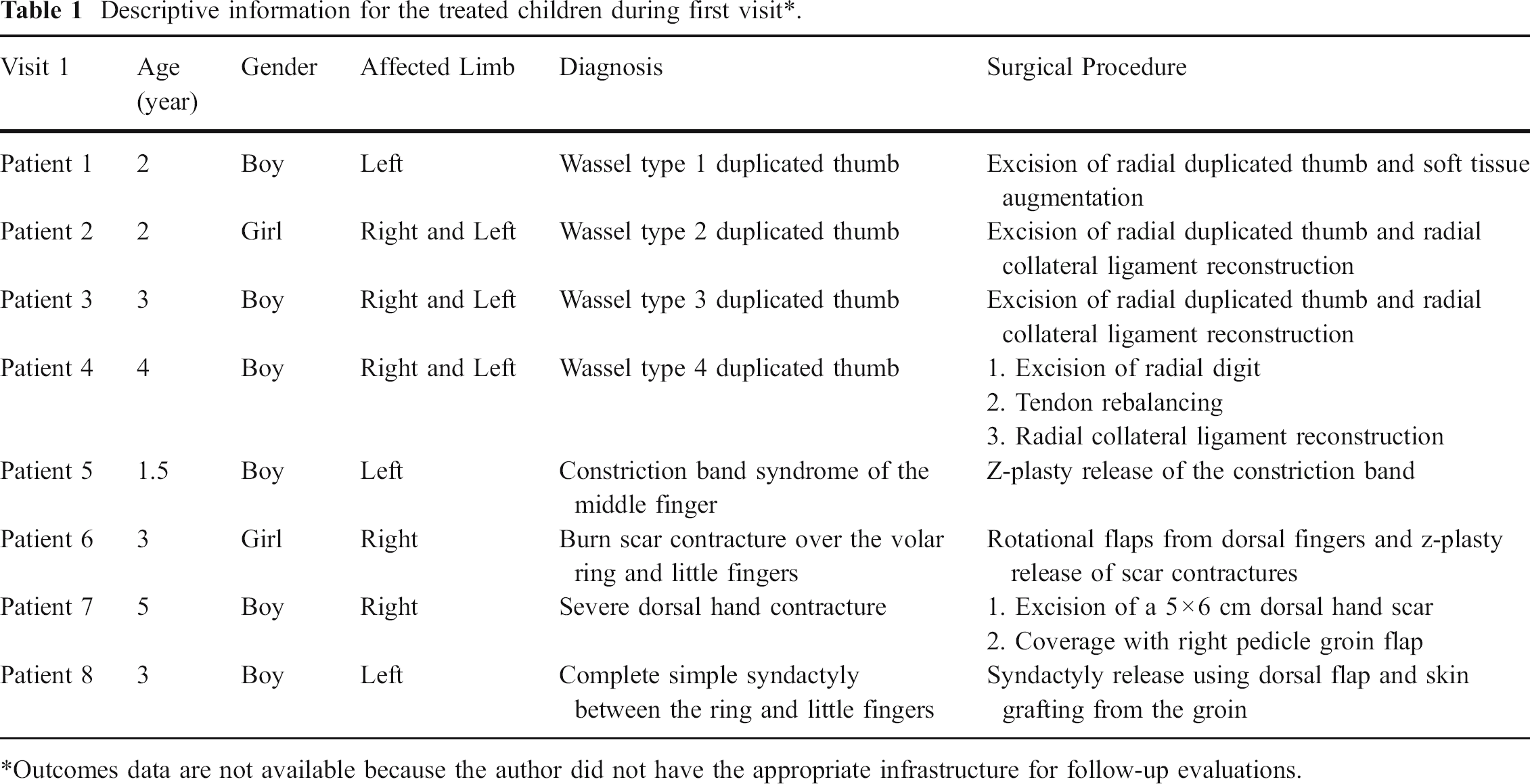
Outcomes data are not available because the author did not have the appropriate infrastructure for follow-up evaluations.
The goal of a medical educator trip is different from a large surgical trip. While surgical trips are conducted at underserved areas and typically require transporting large amounts of surgical equipment and personnel to take care of as many children as possible, the medical educator trips are tailored to established medical centers, using supplies that are available at the local facility to perform the teaching cases. Bringing sophisticated equipment may open up more possibilities for reconstructive options, but the medical educator should adapt to the local working environment by adopting the local working condition in the demonstrations. Importing sophisticated equipment may not be practical because of insufficient expertise in servicing the equipment. In many countries, the lack of a reliable supply of electricity limits the usefulness of the equipment.
The emphasis of the medical educator trip is not to perform a large number of surgical procedures, but to be selective in choosing procedures that have unique educational value. The goal is to introduce new procedures within the limitations imposed by a shortage of equipment or materials. The challenge for the medical educator is to use rather rudimentary equipment that he/she may not have seen before. For example, I used a hand drill to insert a wire to stabilize a thumb after duplicated thumb reconstruction. My Vietnamese colleagues were rather impressed that I had a perfect fixation on my first attempt, even without the availability of a fluoroscopy machine.
Many of the local surgeons are quite skillful because of the enormous amount of surgical problems they encounter. Creativity and malleability are mandatory to surgeons working in developing countries. The resourcefulness of our surgical colleagues in developing countries is in stark contrast to our rather sheltered environment in the United States.
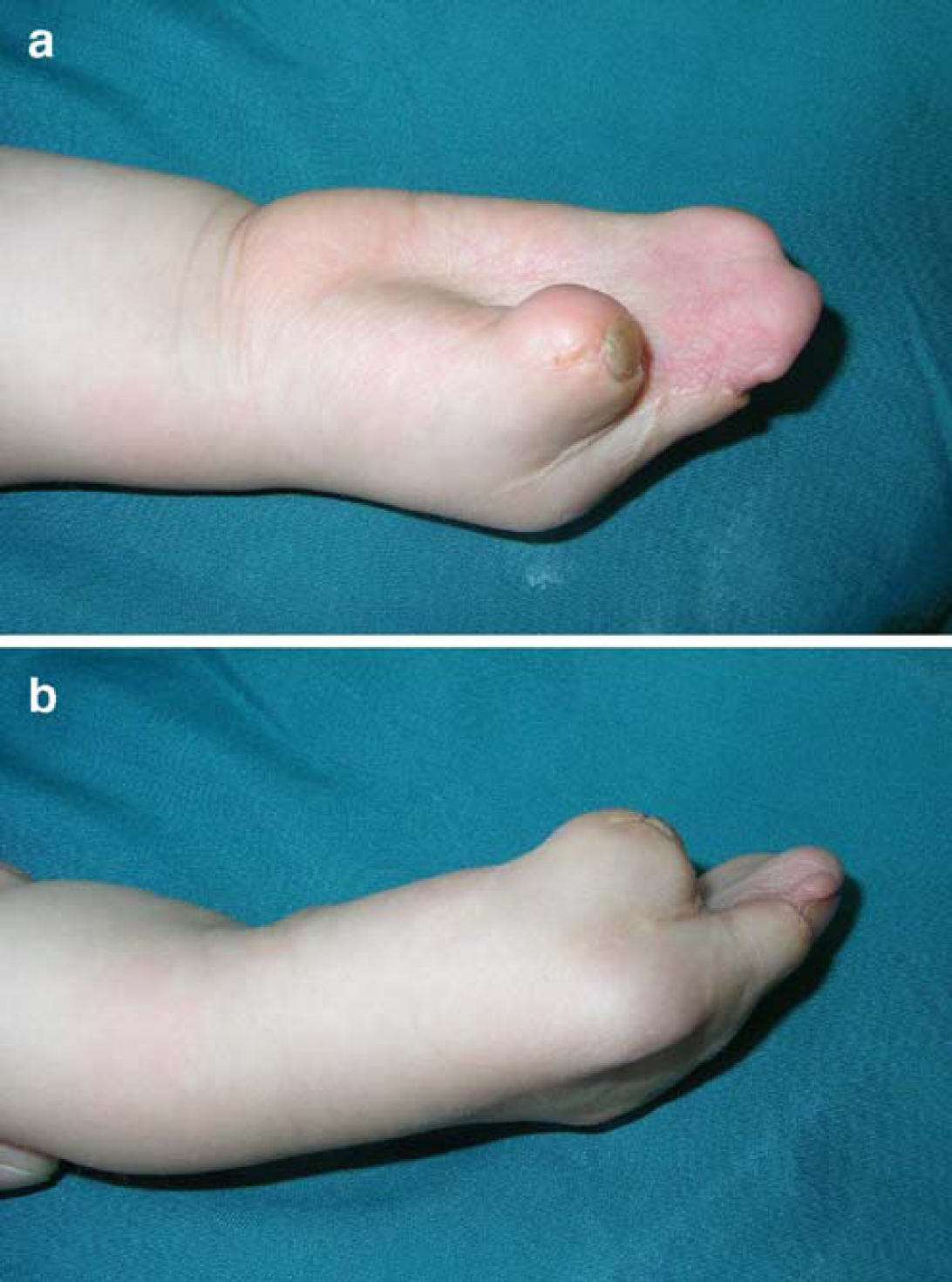
In treating duplicated thumbs, the Vietnamese surgeons simply excise one of the thumbs without considering ligament rebalancing to prevent future zig-zag deformity. I demonstrated to them the principles of ligament rebalancing and skin closure technique using Z-plasty to avoid secondary scar contracture. They were extremely fast learners and by the end of this 1-week trip, they were able to demonstrate their proficiency by applying these newly acquired skills. Other techniques that I demonstrated were flap reconstructive procedures after burn scar contracture releases. Because of cooking over open fires, many children are victims of accidental burns to the upper limb. The majority of these burns were treated conservatively at regional hospitals, and the treatment of choice is allowing the wounds to contract and heal. Predictably, marked burn contractures develop and were referred to the no. 1 Children's Hospital months or even several years later with severely deformed hand and upper extremity (Fig. 4). Surgeons at the no. 1 Children's Hospital treat these burns by scar releases and skin grafting only. They are unfamiliar with local tissue rearrangement or flap techniques to add more durable tissue for coverage. While skin grafting can solve the immediate problem, the skin grafts do not stretch sufficiently when the children grow, and recurrent contractures are common.

Burn scar contracture of the volar fingers limiting finger extension.
In a series of demonstrations, I performed simple Z-plasty, five-flap jumping-man Z-plasties, and cross-finger flaps to demonstrate tissue rearrangement techniques for the hand. As the surgeons advanced in their skill level, I demonstrated distant flaps such as a groin flap to resurface the entire dorsal hand. The use of the groin flap is an important advance for this hospital in expanding their capability to treat even more complex upper limb injuries.
Every afternoon, I gave a 2-h lecture to the surgeons and the therapists. The lectures varied from congenital and burn hand reconstruction to the care of traumatic hand injuries in children. Many of the complex conditions shown in my presentations were encountered at this hospital, but they do not have sufficient expertise to take care of these problems. At the end of this visit, they brought many of the complex conditions I showed in my lectures for my evaluation. These congenital problems vary from Apert's hand to congenital absence of the thumb. With great regret, I was unable to take care of these children at the end of this trip. However, I made a promise to my Vietnamese colleagues and the parents that I would return again to take care of these children.
Second Trip
Four months later, I returned to the no. 1 Children's Hospital again under the Interplast medical educator program. This visit had a different theme, unlike the more exploratory mission of the first visit. I went on a second trip in an effort to evaluate the progress in applying the techniques taught during the first visit. I was pleased to observe that many of the techniques I demonstrated have been used effectively by the surgical staff. Because of their competence in learning techniques from the first visit, the second visit was concentrated on demonstrating even more difficult reconstructive procedures. The main limiting factor hindering the introduction of more complex reconstructive hand surgery is the lack of adequate equipment in this hospital. For intricate pediatric hand surgery work, they use adult-sized instruments and sutures. Fixation of fractures and pinning of joints rely on a limited selection of K-wires driven by hand drills. No fluoroscopy is available and confirmation of reduction is assessed visually. During a syndactyly release in a 1-year-old child, I was given a pair of Mayo scissors that were the length of the child's forearm.
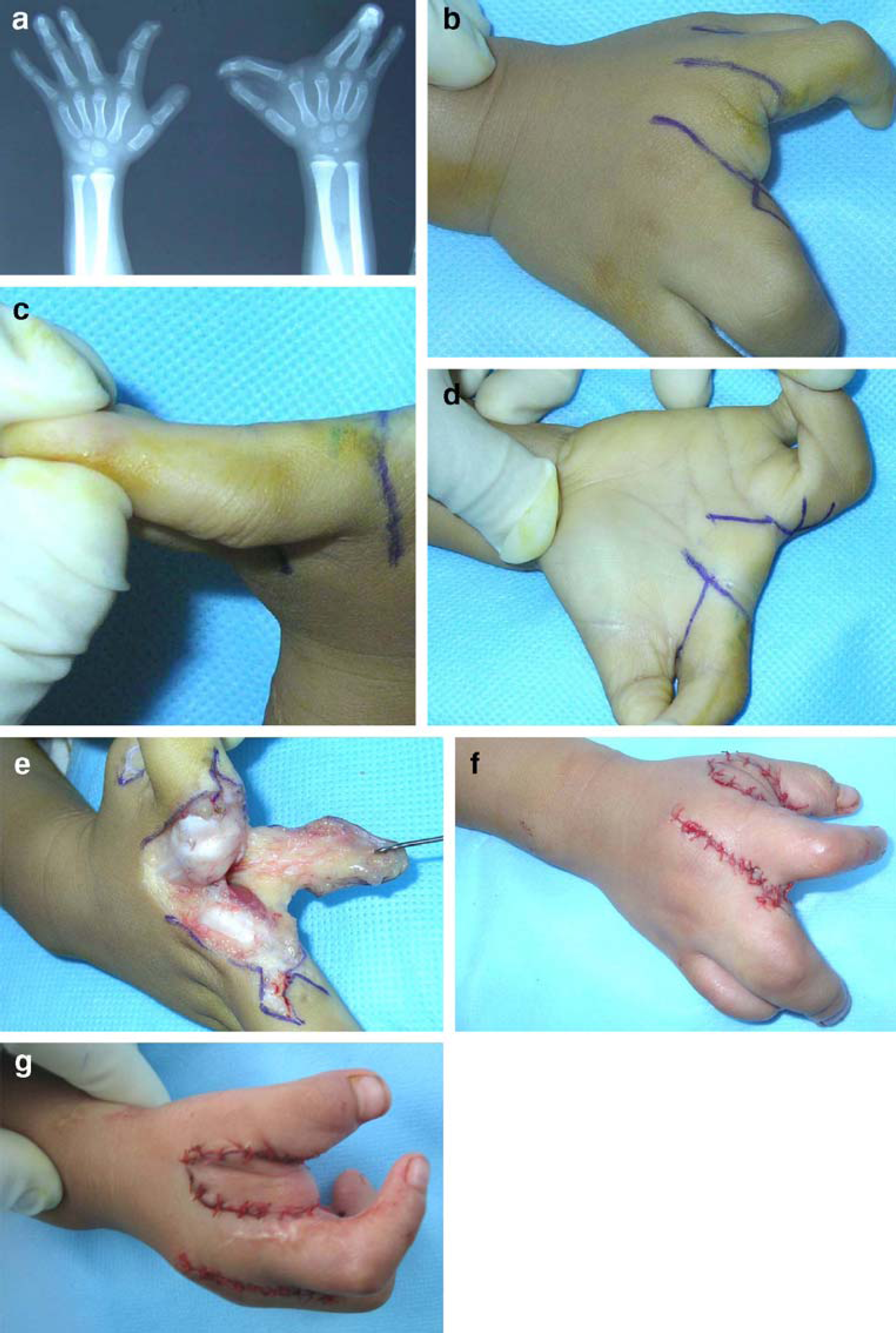
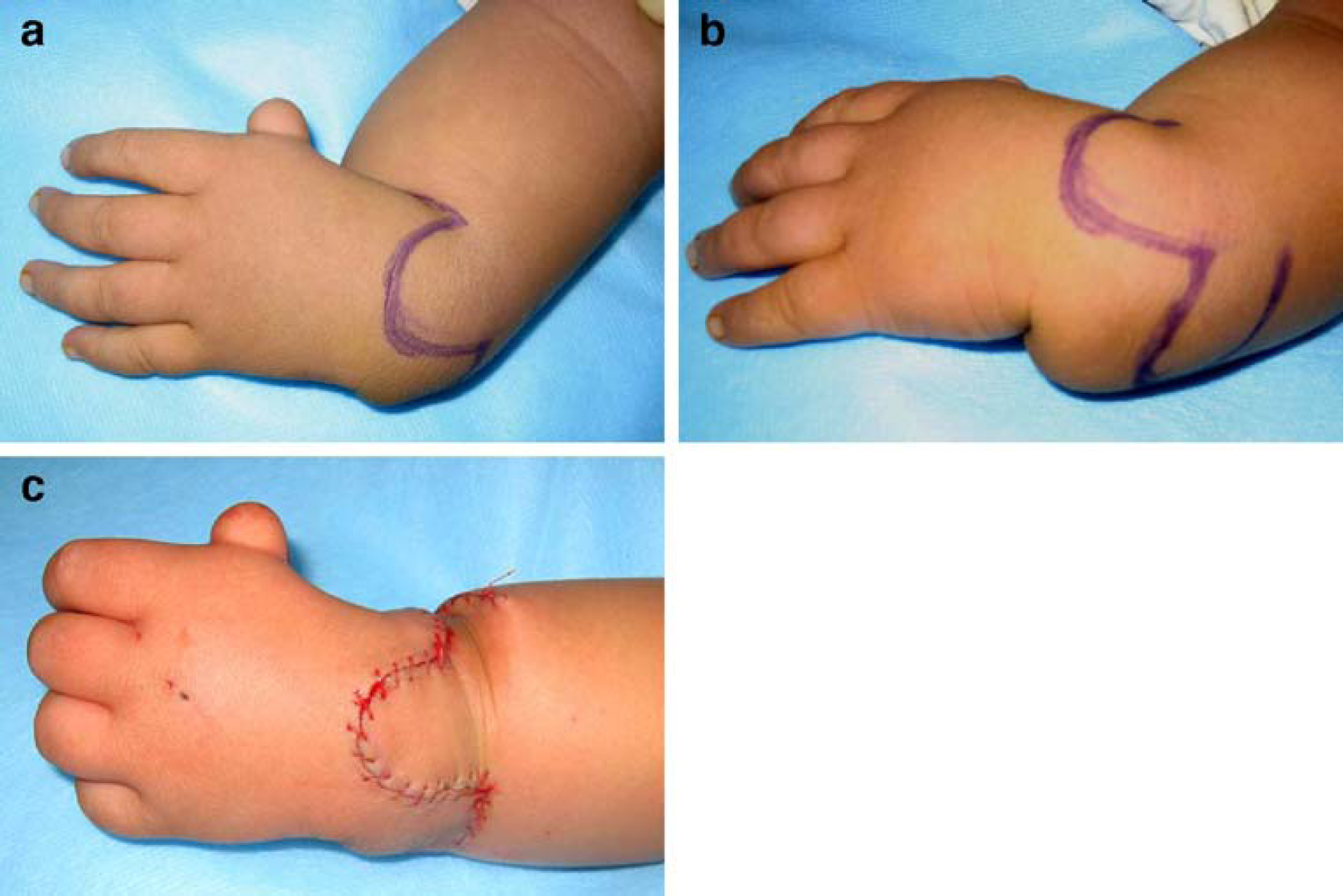
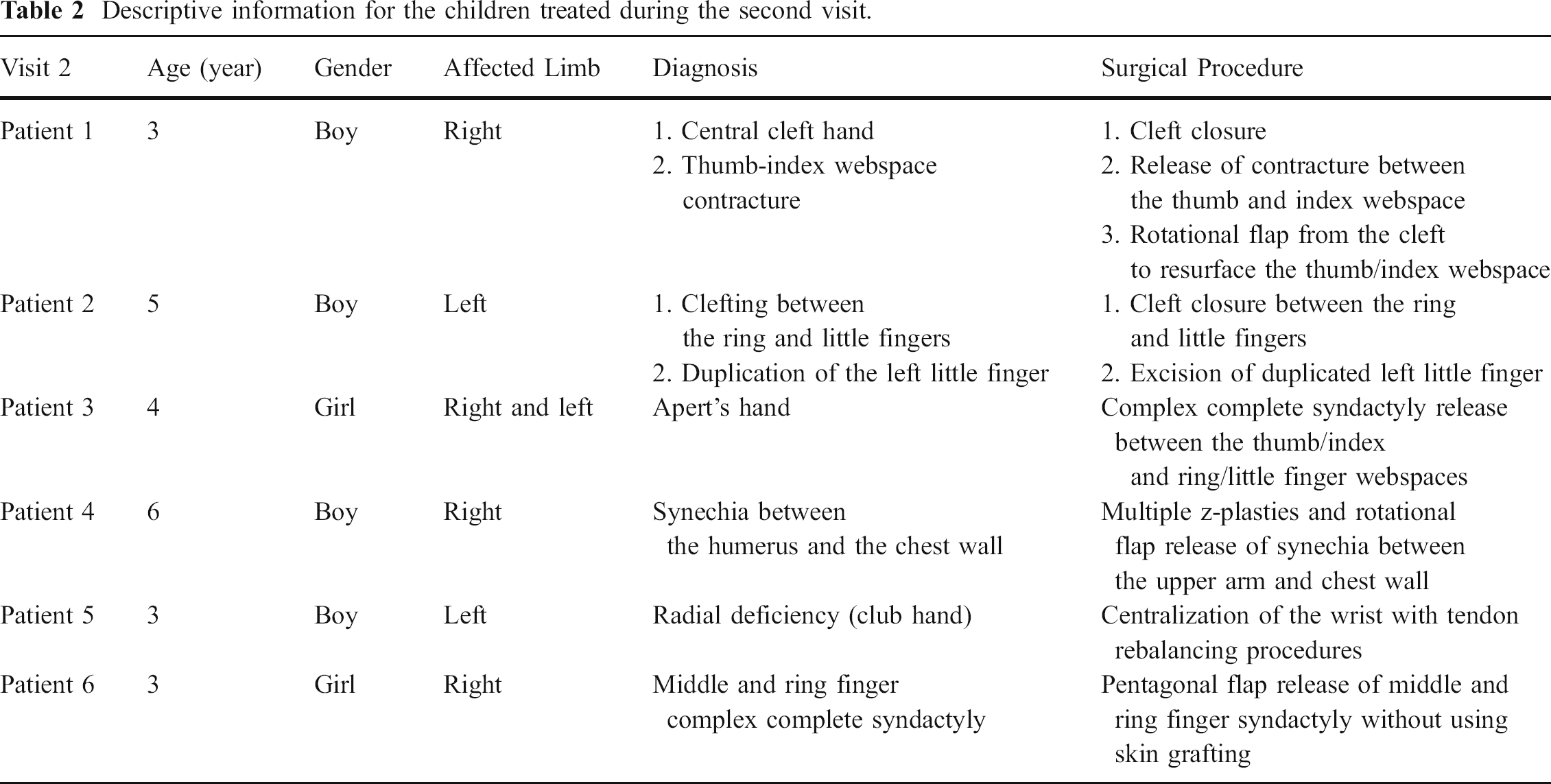
It is gratifying to see that the flap procedures that were taught previously were being incorporated routinely in their surgical plans. During this visit, complex congenital hand surgery procedures were performed, including complex syndactyly reconstruction in an Apert's hand (Fig. 5a and b), cleft hand reconstruction (Fig. 6a–g), and centralization procedure (Fig. 7a–c). Simultaneous procedures were performed for patients with bilateral hand problems so that the Vietnamese surgeons could observe me performing the procedure on one hand (Fig. 8), while I monitored them doing the procedure on the other hand. The active interchange during the surgical procedures fosters interactive learning that is efficient and productive during these relatively short trips (Table 2).

Attentive Vietnamese surgeons observing a pediatric hand surgery procedure.
Descriptive information for the children treated during the second visit.
Unfortunately, because of time and logistic constrains, I was unable to follow the children I have operated on. However, during the second visit, I had the opportunity to see some of the children who came to see me after they heard that I was returning for another visit. All the patients I have seen have healed wounds and have quite acceptable results from the operations. This is not to indicate that all the children have done well. But because of the relatively high quality of care at the no. 1 Children's Hospital, I am satisfied that the children are well attended to after the operation.
Lessons Learned
One important consideration when operating in developing countries is to resist the urge to do an operation when the condition is not optimal. Safety for the patient is a crucial consideration because when a complication occurs, the volunteer surgeon may have left the country, leaving a complex management problem to others who may not be capable to treat the complication. In addition, one may be pushed by the local surgeons into performing complex operations that the volunteer surgeon may not be comfortable in undertaking, perhaps because of the limited capability of the facility. It is preferable to be honest and defer treating the patient at the expense of “losing face.” A mishap in a surgical case can create lingering problems that hinder future constructive relationships at these sites.
One must also respect the local culture by being adaptable to the practicing environment. Many of the surgeons in developing countries are masterful surgeons, working under difficult conditions. The purpose of these educational trips is not to satisfy one's ego by showing how much one knows, but rather, to develop a collaborative relationship between the visiting educator and the local surgeons to elevate the standard of surgical care and to provide much needed help to the children.
In teaching hand surgery to the local surgeons, the medical educator should share in great detail the indications of the operations and the postoperative management plans. Many of the local surgeons are more interested in the technical allure of the operations, without acquiring an understanding of when to or when not to perform the operations. In addition, they may be unprepared to supervise the postoperative therapy requirements or manage the complications after the operations. Technical instructions should be supported with a thoughtful background discussion of these important surgical principles.
Because of language problems, the medical educator may have difficulty in fully conveying the concepts of the surgical procedures to the local surgeons. It is not uncommon for local surgeons to nod politely during the explanation or discussion when they may not fully understand the instructions. Because Vietnam is a multilingual culture, many of the surgeons are more fluent in French than English. During the lectures, they may have to translate an English presentation in their minds into French and then into Vietnamese. It is important to speak slowly and continue to ask questions during the surgical demonstration to gauge their level of understanding. One must be sensitive to certain cultural issues as well during the lectures. For example, one should not pose a technical question to senior surgeons in a group setting because their inability to answer the questions may be quite embarrassing to them in the hierarchical system. I was provided with translators in these two trips. They were quite helpful in bridging the language issues and also alerting me of potential cultural breaches.
As surgical volunteering efforts increase from the United States, there are more national discussions about the proper conduct of these trips. Some are questioning whether the large expense in the surgical trips, including personnel, equipment, transportation, and lodging costs, is justified [7]. Often, there are local surgeons who are capable of performing these operations, but the lack of reimbursement for these cases dissuades many from undertaking these additional responsibilities when the surgeon's pay is rather meager already. Paying local surgeons to perform these operations, some argue, may be a more effective strategy. This may be a sensible discussion because an experienced orthopedic surgeon in Vietnam makes about $10 per day working in a government hospital. To commission trained local surgeons to go to outreaching hospitals to perform necessary procedures may be reasonable if service for patients is a consideration. A well-organized medical educator trip may have a greater impact in elevating the overall level of expertise in a country.
The opportunity to have residents accompanying the educator on these trips is appealing but may lead to conflict with local culture. The purpose of these visits is to interact directly with the local surgeons to benefit the local staff. Concerns have been shared from other trips that the local surgeons may feel alienated when their patients were being used as teaching cases when residents worked with the senior surgeons. Therefore, we must be sensitive to this issue and make all effort to prevent the perception that patients are used for teaching purposes by American surgeons. The medical educator must perform the operations and teach the residents and the local staff in a similar fashion without differentiating between the two groups.
Some surgical trips are criticized because surgeons who were not trained in a particular procedure or who have not performed in an area of surgical discipline are performing these operations. Furthermore, some volunteer groups do not involve the local medical authorities in the treatment of patients [4]. Complications and suboptimal results can create mistrust for all parties that will deleteriously affect future volunteering trips. While these unscrupulous events are uncommon, occasional lack of oversight can be magnified and ruin the reputation of many of the well-organized missions.
Overall, medical volunteering efforts within and outside of our borders are highly satisfying and will reinforce why we chose to be physicians and surgeons in the first place. While the accomplishment of individual physicians may be modest, the collective effort by all surgeons to engage in volunteering effort can be an imposing force that will advance the efforts of many of the surgery pioneers in introducing surgical principles to far reaching areas of our world.