
Abstract
A 1-year-old boy presented to us with congenital inability to flex his elbow. He had bilaterally absent biceps brachii and brachialis muscles, a rare condition. We performed pedicle latissimus dorsi musculocutaneous flaps to the left and right volar upper arm at 21 and 24 months of age, respectively, to create elbow flexors. By 4 years of age, he had excellent elbow flexion bilaterally with strength grade in excess of 4.5. In addition to discussing our patient's treatment options, we discuss other potential causes of weak elbow flexion when faced with this clinical dilemma.
We were presented with the clinical problem of an infant who had been unable to flex his elbows actively since birth, but in whom there was good passive range of elbow motion. Congenital or infantile inability to bilaterally flex the elbow has been previously reported. The list of potential causes includes arm trauma, isolated musculocutaneous neuropathy, brachial plexopathy, poliomyelitis, arthrogryposis, focal muscular atrophy, and congenital elbow flexor absence. The last is a rare condition.
Congenital muscle absence has been described for a variety of muscles. The most common deficiency is absence of the sternocostal portion of the pectoralis major muscle, which occurs in Poland syndrome (sequence) and is frequently unilateral [16]. Other shoulder girdle muscles may be absent either in isolation or in association with the Poland sequence such as pectoralis minor, serratus anterior, trapezius, and latissimus dorsi [29]. Congenital absence of the radius (radial dysplasia) has a variety of muscle anomalies in the forearm but may also include congenital absence of the biceps brachii muscle [49]. In a case of radial dysplasia with an absent biceps, wrist centralization of the ulna was performed in addition to a muscle transfer to restore elbow function (in this case, the triceps was used) [38]. In the forearm, isolated congenital absence of finger extensors has been described [37]. Ethans and Leahey [18] have described the only published report that we could find of congenital absence of bilateral elbow flexors. They made the diagnosis by magnetic resonance imaging (MRI) and found absence of both the biceps brachii and brachialis muscles.
The objective of our case report is first to describe our patient who was born with congenital bilateral absence of elbow flexors as well as his surgical treatment by means of pedicle latissimus dorsi transfers. Second, we discuss differential diagnoses to consider when faced with a young infant with inability to flex the elbows and, in addition, discuss an approach that aids in the determination of the etiology of this clinical presentation.
Case Report
Our patient presented to us at 1 year of age. He had bilaterally extended elbows, and his wrists were minimally flexed (although this wrist position corrected spontaneously with time). He was unable to flex the elbows actively. Passive elbow flexion was not entirely normal but easily ranged from full extension to at least 90° of flexion.
Review of the patient's birth history revealed that he had a clinically insignificant intracranial bleed and had been born at full term through an uncomplicated vaginal delivery. Subsequent studies included a normal electroencephalogram. A brain MRI performed 1 month after birth showed a resolving intracranial bleed. Magnetic resonance arteriography of the circle of Willis was normal with no evidence of aneurysms or vascular malformations. In a neurology consultation before our meeting, the patient concluded that he had only the observed upper limb restriction and no evidence of cerebral parenchyma insult or sequelae.
The patient was able to crawl at 10 months of age, and he could walk unassisted by the time of our initial consultation (12 months of age). He had developed some interesting adaptive maneuvers to accommodate his inability to actively flex the elbows. He would push up against an object (such as a table top) with his forearms to passively flex his elbows, or he would abduct his shoulder to enable gravity to bring his elbows into flexion. In this manner, he was able to bring food items to his mouth. He would lead with his thumb when picking up objects as the absence of biceps muscle function (also a strong supinator) kept his thumb in a pronated downward position.
Examination revealed bilateral upper extremities that were held in elbow extension and partial forearm pronation at rest. There was no active elbow flexion, and passive flexion was possible to only 90°. Wrist motion was normal. Antecubital creases were absent. Motor examinations of median, radial, and ulnar nerves were normal, and on sensory examination, there was a normal withdrawal response, and tactile sensation was normal in all areas. It was difficult to assess biceps muscle bulk, as this child had the usually anticipated baby fat that obscured direct muscle palpation. He was well nourished and on the 25th percentile for height and the 50th percentile for weight. Deltoid, pectoralis, and latissimus dorsi muscles were normal bilaterally. Hand and wrist function was normal.
Plain radiographs of both upper extremities were unremarkable. As best could be determined in a young child, electromyography studies showed some volar upper arm motor unit potentials but markedly decreased maximum recruitment pattern (which is dependent on voluntary effort).
It seemed then that this patient had a solitary bilateral biceps brachii problem (possibly also brachialis muscle as this is difficult to evaluate independently) given the isolated inability to flex the elbows and weakness of forearm supination. We elected to perform a muscle transfer to restore biceps function in the hope that this would not only provide functional improvement but also maintain congruity of the elbow joint. We used a latissimus dorsi muscle transfer as has been described by others for restoration of elbow flexion [27, 42, 50, 54, 62]. Surgical exploration of the upper arm to define the pathology was necessary to inset the musculocutaneous flap, and therefore, further diagnostic tests were felt to be unnecessary.
By age 21 months, the child had not shown functional improvement in the elbow, and a left latissimus dorsi musculocutaneous flap was performed (Fig. 1). The humeral tendon attachment was taken down and anchored to the coracoid process. The transferred muscle was tubed and inserted distally with bone anchor sutures to the proximal ulna (Fig. 2). The skin island accompanying the muscle transfer enabled tension-free wound coverage over the volar upper arm. Our intraoperative dissection revealed the absence of both biceps brachii and brachialis muscles. The only subfascial structures in the volar upper arm were the brachial artery and the ulnar and median nerves.
By 23 months of age, the child had developed active left elbow flexion against gravity, and at 2 years of age, a functional latissimus dorsi musculocutaneous transfer was performed to the contralateral side. The intraoperative finding of absent biceps brachii and brachialis was confirmed on the right side as well.
By 4 years of age, the child had excellent biceps function bilaterally with strength grade in excess of 4.5. He can bring the hands to his mouth and can reach behind his head (Fig. 3). He has normal development of hand prehensile grasp. Supination is good on the right but more difficult on the left. There appears to be normal skeletal development by radiographic evaluation.
Discussion
The main purpose of our manuscript is to provide an analysis of potential problems that need to be assessed when evaluating a young infant with absent elbow flexion including the clinical evaluation and tests pertinent to making an accurate diagnosis. An isolated congenital bilateral inability to flex the elbow in an infant is an uncommon presentation, and congenital absence of elbow flexors appears to be quite rare [18]. On clinical examination, it is important to be absolutely certain that this is truly an isolated functional problem. Inability to flex the elbow may be the most obvious clinical problem, and other associated issues may be more subtle and need to be sought to arrive at the correct clinical diagnosis. In most cases of inability to flex the elbows, there will be other clues that will help arrive at the correct clinical diagnosis.
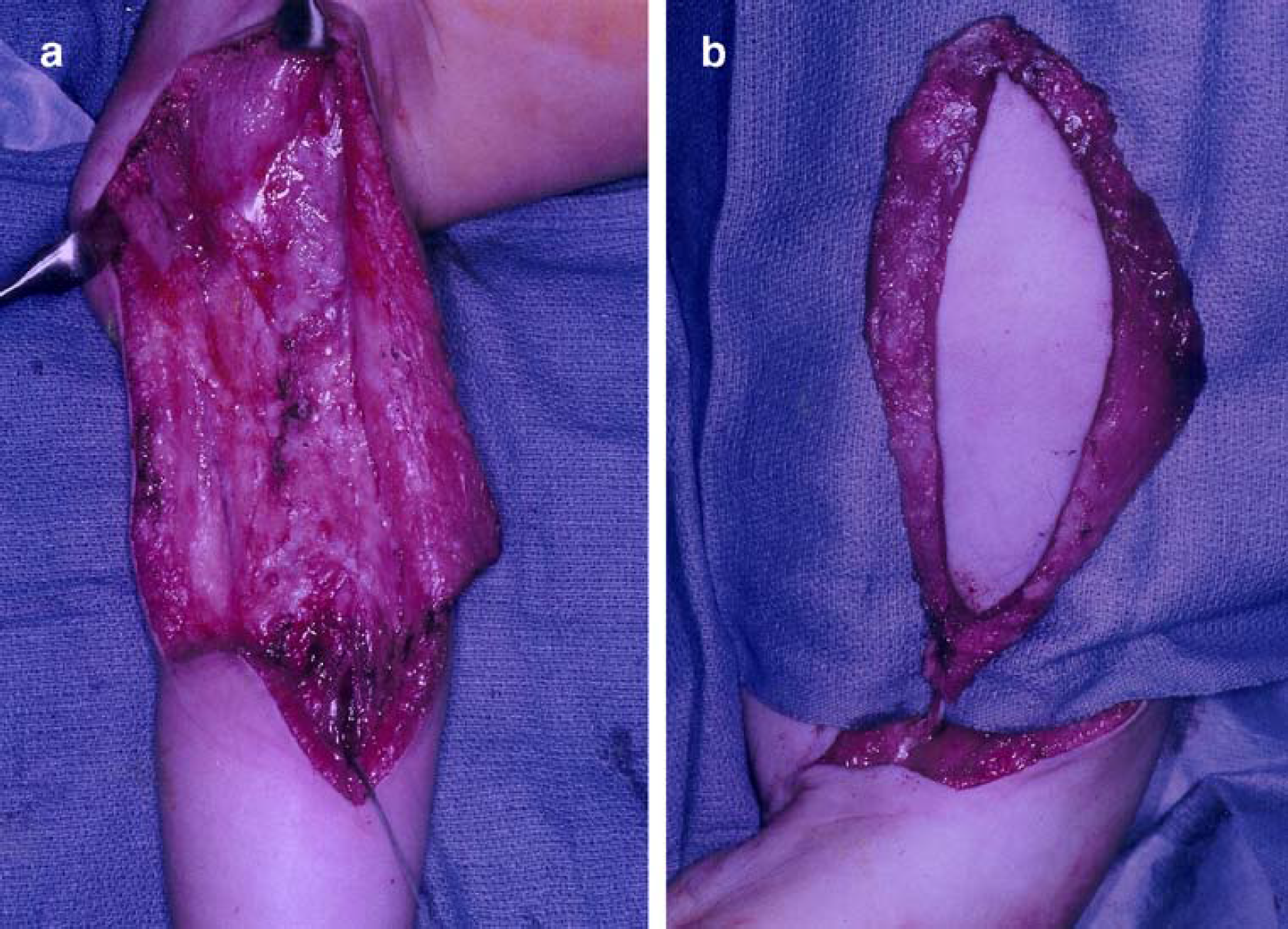
A Intraoperative view of the volar forearm compartment showing absence of biceps brachii and brachialis muscles. D shows deltoid insertion on the humerus. b Musculocutaneous latissimus dorsi muscle flap prior to tubing and insetting as a functional muscle transfer.
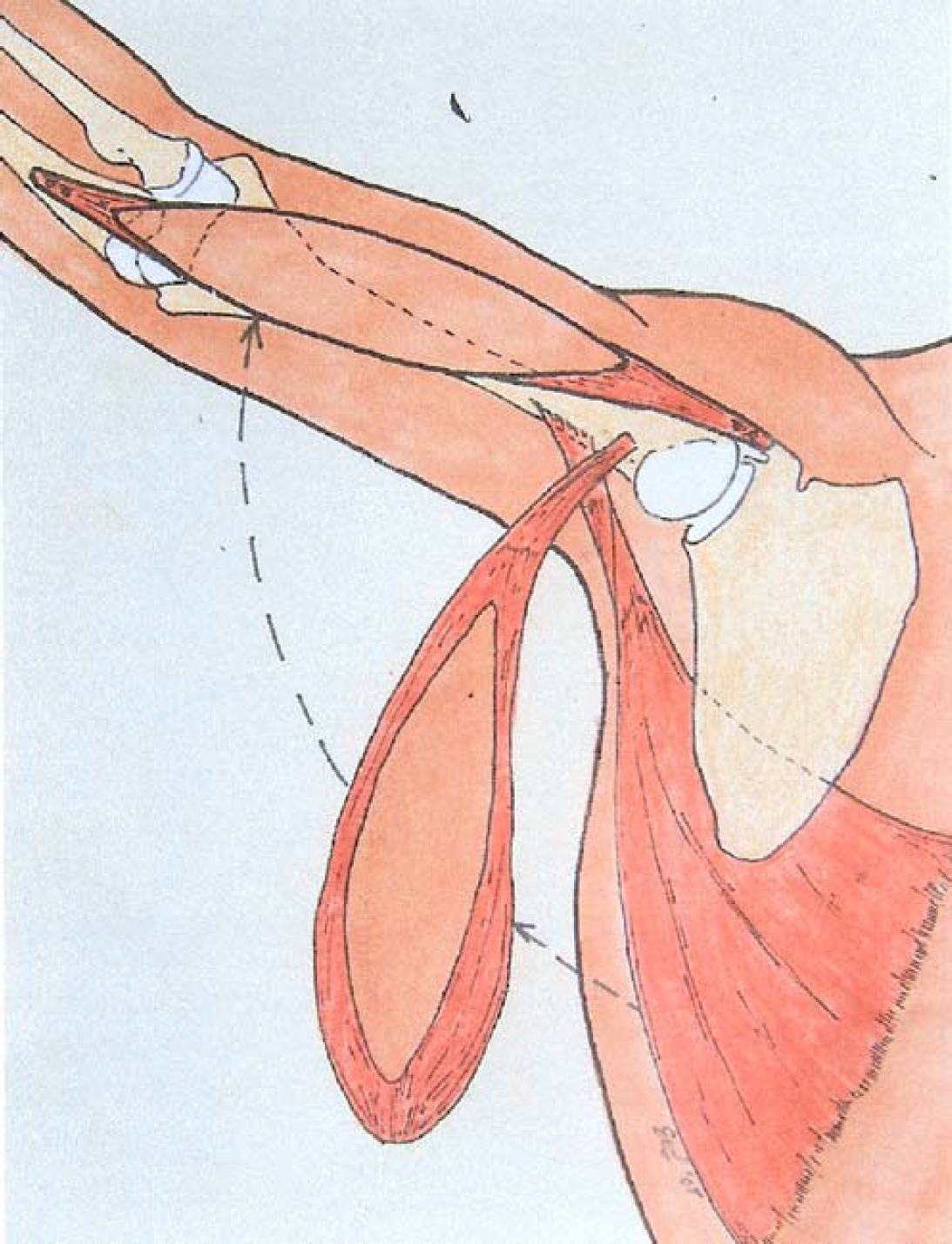
Pedicle transfer of the musculocutaneous latissimus dorsi flap. Bone anchors facilitate proximal and distal bone attachments to coracoid process and ulna, respectively.
Arthrogryposis and obstetrical brachial plexus palsy (OBPP) are among the more common problems to present with absent or weak elbow flexion. Others include a variety of central and peripheral nerve degenerations, muscle dystrophies, and myasthenic (affecting neuromuscular transmission) disorders.
The risk of OBPP is increased by high birth weight [43, 44] and by the presence of shoulder dystocia [45]. OBPP injury occurs more commonly to the upper roots C5 and C6 (Duchenne–Erbs's palsy), and Klumpke's palsy involving C8 and T1 roots is less common. These patterns of injury can be bilateral [31], and cases of bilateral involvement make up 5% of brachial plexus injuries [24]. When the upper roots are injured, the clinical presentation is similar to our patient's clinical picture, but a careful search will also reveal other muscular deficits (Table 1). Many cases of OBPP are transient and recover within the first 3 months of life.
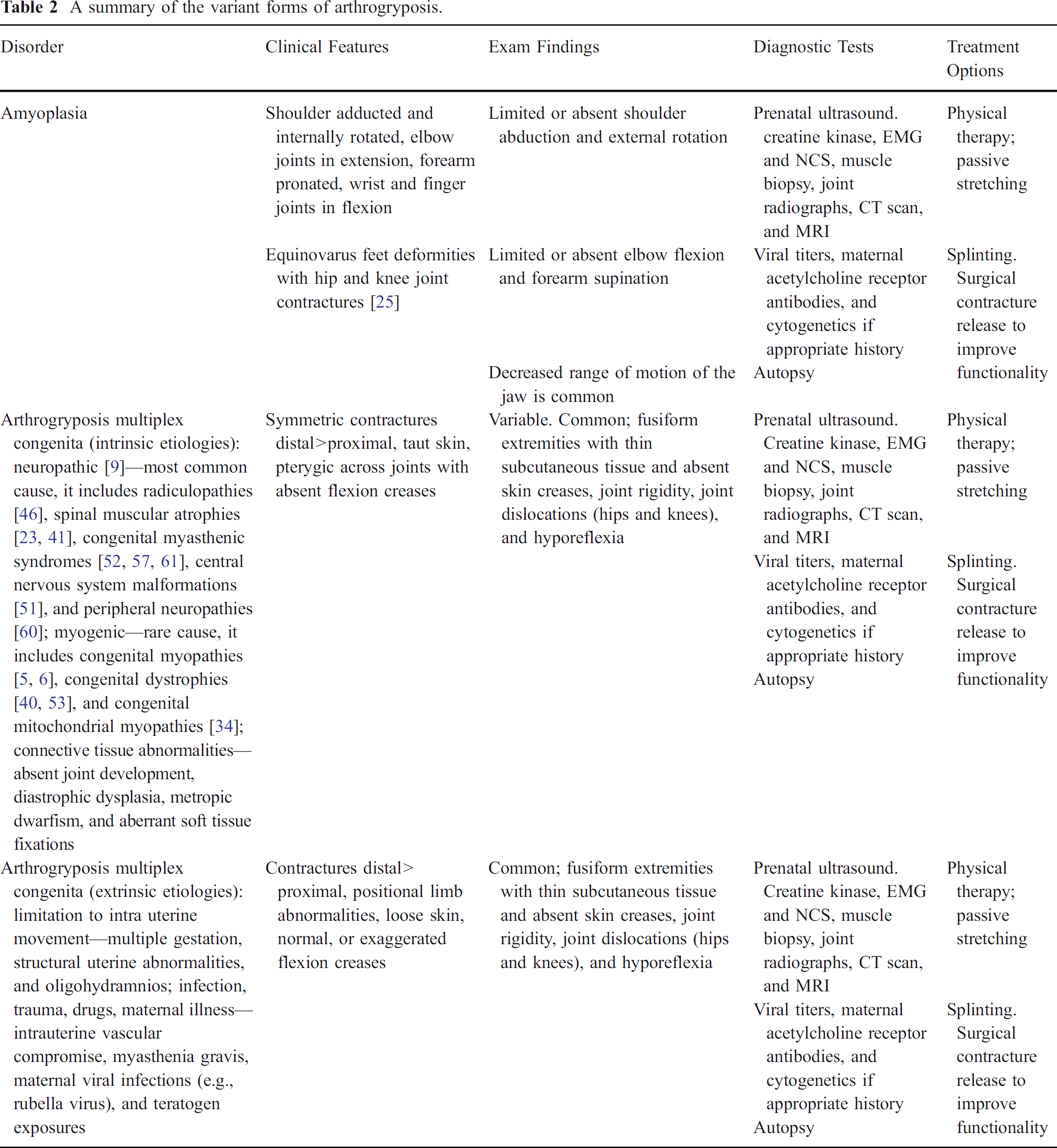
Arthrogryposis [32] or nonprogressive congenital joint contracture is a secondary manifestation of a heterogeneous group of disorders that cause fetal akinesia, which may be classified as intrinsic or extrinsic (Table 2). These disorders have stiff joints, and passive range of motion of the elbow might be expected to be more greatly restricted than was the case with our patient. The presence of arthrogryposis should be investigated to determine the primary abnormality. Amyoplasia (Table 1) is the most common form of arthrogryposis characterized by absence of limb muscles that are replaced by fibrous and fatty tissue.
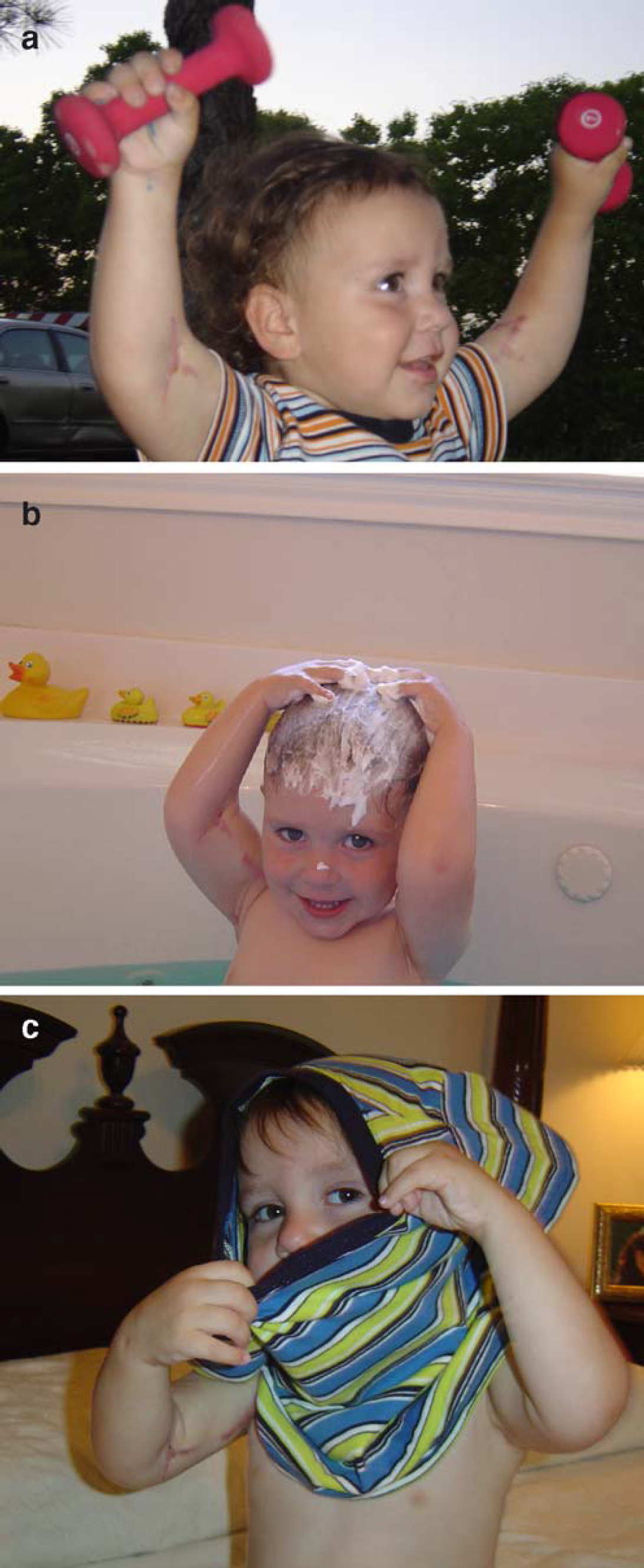
Postoperative pictures after bilateral neo-biceps reconstruction show a good strength, b ability to reach behind the head for personal hygiene, and c performance of daily activities such as donning a shirt.
Spinal muscular atrophies are a clinically heterogeneous group of inherited disorders with a common feature of motor neuron loss from the spinal cord and cranial nerve nuclei [7]. Classification of these disorders is based mostly on the age of onset [12]. The form most likely to present with a congenital muscular disability is the Werdnig–Hoffman syndrome [39]. It is also called acute infantile spinal muscular atrophy because the age of onset ranges from birth to 6 months of age. Indeed, as many as 30% of cases are said to have prenatal onset [12]. About 50% of these cases manifest symptoms at birth [2, 13] (Table 1).
More recently, three cases have been described of so-called “nonfamilial congenital cervical spinal atrophy” (Table 1) as a result of intrauterine hypoxic events [3, 20]. These patients share many features with our case. Other authors have previously described similar cases and are of the opinion that this condition should be described as arthrogryposis, neurogenic type with anterior horn cell degeneration limited to the cervical region [15, 28]. Hypoxic-ischemic changes in the anterior horn cells have been described in a patient with congenital cervical spinal atrophy [59], and a proneness to injury of anterior horn cells to hypotension has also been demonstrated [1]. Finally, with evidence from histologic specimens, it has been proposed that intrauterine hypotension can be a cause of arthrogryposis leading to anterior horn cell destruction [10, 11].
Disorders of the muscle such as central core disease [25], nemaline rod myopathy [25], and congenital muscular dystrophies [9, 40] represent an array of disorders with a wide range of clinical presentations with a few features similar to our patient's presentation (Table 1).
In addition, affecting muscles are congenital myasthenic syndromes (Table 1), which constitute a group of disorders that affect transmission at the neuromuscular junction with a clinical spectrum ranging from mild muscle weakness to severe disability [23, 48]. An association between maternal antibodies against acetylcholine receptors and arthrogryposis has been described, in which fetal movement is arrested or limited by disruption of myoneural interaction in utero [52]. These disorders result from pathologic transmission at the neuromuscular junction of all muscles with acetylcholine as the transmitter molecule.
Bilateral injury to the musculocutaneous nerve (Table 1) would be expected to be very rare, and it would be hard to imagine such a situation occurring as a congenital problem. The musculocutaneous nerve innervates elbow flexors (biceps brachii and brachialis) and also provides sensation to the radial aspect of the forearm. Musculocutaneous nerve palsies have been described. The mechanisms of injury to this nerve result from stretching of the nerve with the upper limbs in hyperextension, rapid isometric contraction of the coracobrachialis muscle (a muscle which the nerve crosses) [6], excessive strenuous activity [5, 6], prolonged positioning with the shoulder abducted and externally rotated [34, 53], violent forearm extension [58], and direct trauma to the anterior aspect of the shoulder [21].
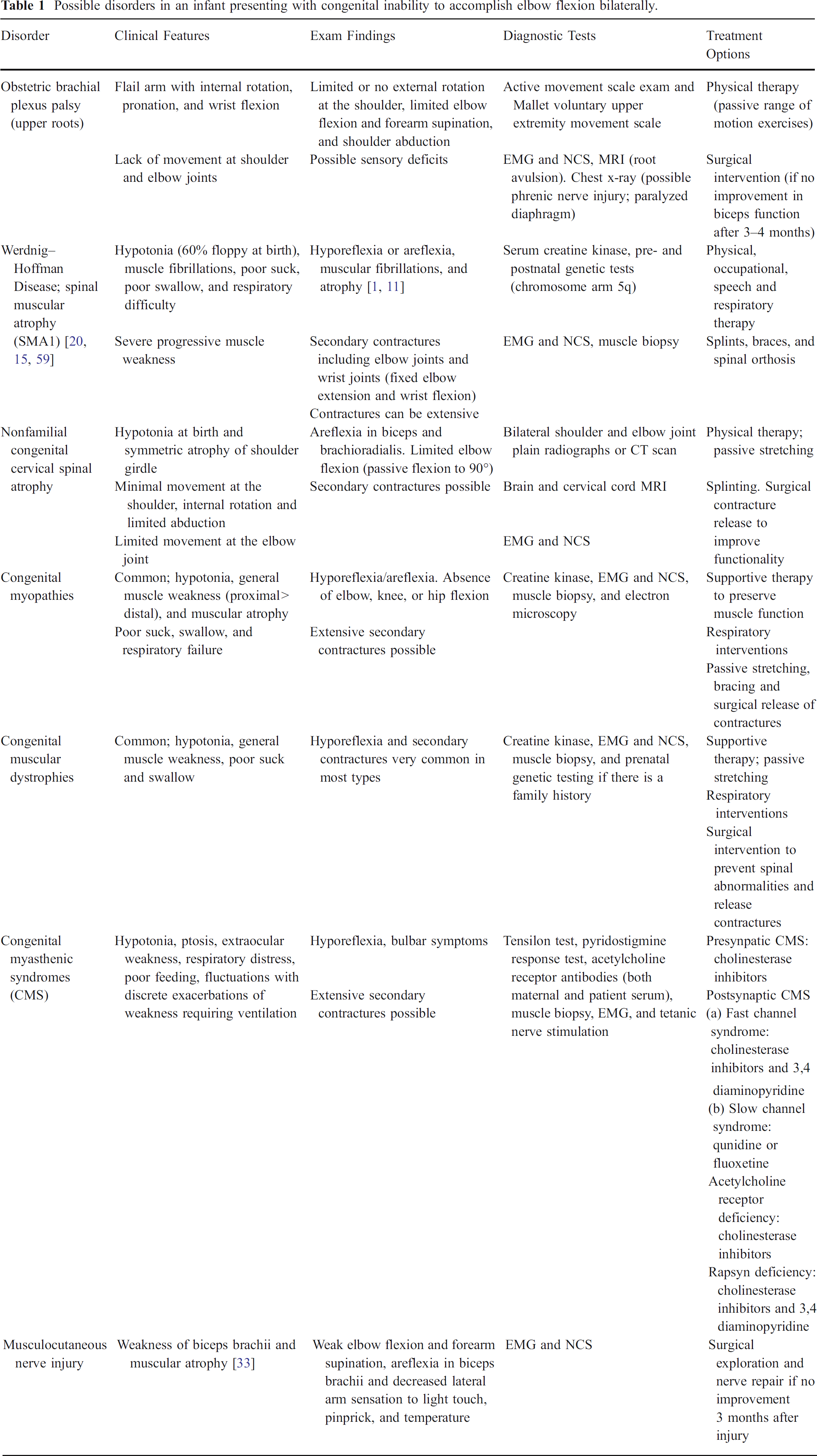
Possible disorders in an infant presenting with congenital inability to accomplish elbow flexion bilaterally.
In general, careful clinical evaluation will enable one to distinguish one type of disorder from the next. Special diagnostic studies are usually unnecessary. A thorough history that includes a pregnancy, birth, and family history would, for instance, reveal factors such as the presence of oligohydramnios, multiple gestations, maternal infections, macrosomia, or shoulder dystocia (risk factors for fetal akinesia and OBPP) that serve as a good foundation to direct judgment on appropriate and focused evaluations. Associated presenting clinical features can clarify the etiology. Generalized hypotonia associated with inability to flex the elbow would suggest a congenital myopathy, spinal muscular atrophy, or a myasthenic syndrome. Some common features of disorders other than isolated absence of elbow flexors that would present with weak or absent elbow flexion include poor suck or swallow, respiratory difficulties, associated congenital malformations, and secondary contractures.
Careful physical examination will not only reveal the primary presenting deficit but also any other associated but less obvious deficits. Physical examination in our patient showed elbows in extension and partial forearm pronation at rest, no active elbow flexion, and slightly reduced passive elbow flexion (to 90°). Our patient's deficits were isolated to the elbow joint and muscles of elbow flexion and forearm supination. Musculocuteneous nerve palsy findings are most similar to our patient's presentation as the muscle groups affected are identical to the absent muscles in our patient. However, even in this instance, special diagnostic tests are unnecessary as presenting features and physical evaluation are sufficient to delineate both disorders. We could not find any published reports of isolated bilateral congenital injury to the musculocutaneous nerve. There are some described mechanisms of bilateral injury to the musculocutaneous nerve in older patients [5, 6, 8, 10, 19, 21, 34, 35, 53, 58], but it is difficult to conceptualize a clinical scenario of congenital palsy isolated to the nerve, bilaterally. Musculocutaneous palsy would furthermore present with sensory deficits of the lateral upper arm, which admittedly will be challenging to document in infants [56].
Electrodiagnostic studies, whereas more difficult to perform and interpret in infants, may be helpful. Ethans and Leahey [18] confirmed the diagnosis of bilaterally absent musculotendinous units of the biceps brachii with MRI, and this may be a reasonable approach to confirm the diagnosis. However, in the course of narrowing the list of clinical disorders in an infant that could present with inability to flex the elbow joint bilaterally, a thorough clinical evaluation is sufficient to identify congenital absence of elbow flexors.
A summary of the variant forms of arthrogryposis.
There are a variety of surgical options to restore elbow flexion, and these choices depend largely on the best available muscles for transfer. Restoration of biceps function has been described by a number of pedicle muscle transfers to include pectoralis [47], triceps [30], latissimus dorsi [27, 42, 50, 54, 62], and also microvascular muscle transfers using either gracilis or latissimus dorsi muscles [4, 22, 26] and by advancing the flexor/pronator muscle mass up onto the humerus (Steindler transfer) [36]. Microvascular transfers are necessitated when there are no available pedicle muscle transfers. The Steindler transfer results in comparatively weaker elbow flexion, and triceps transfers leave the patient with deficits in elbow joint extension. Elbow joint flexion/extension cocontractions occur if a split triceps transfer is used and may be problematic. The pectoralis muscle is often preferred in patients with arthrogryposis as the latissimus dorsi muscle is frequently not available in those cases [26]. The gracilis muscle has been used as a microneurovascular transfer for biceps functional restoration in patients with arthrogryposis and is revascularized on the brachial vessels and reinnervated by the intercostal nerves [26]. The latissimus dorsi muscle is more frequently used for paralytic disorders. In severe brachial plexus problems, local pedicle muscle transfers may be unavailable, necessitating microvascular muscle transfers.
The goal of our report is not to discuss the relative merits of these available muscle transfers nor to debate the methods and locations of proximal attachment or distal insertion of the latissimus muscle transfer, as these have all been discussed adequately elsewhere [27, 42, 50, 54, 62]. Suffice it to say that, in our patient, the latissimus dorsi muscle was selected over the pectoralis major out of concern for potential anterior chest wall deformity when utilizing the pectoralis muscle for transfer. When the latissimus muscle is used as a pedicle transfer to restore biceps function, it is best to detach the humeral tendon and reattach it to the coracoid process [50].
The coracoid and lateral acromion have been used interchangeably for the proximal origin without any significant differences in the overall function of the transfer. Using the coracoid as the origin allows for the insertion to be further distal and thus potentially increasing the flexion moment arm and providing greater mechanical advantage [14]. Historically, the latissimus has been woven into the remnant of the biceps tendon [21, 55, 58]. The current patient obviously had no biceps tendon available for insertion. The distal insertion has generally been into the bone further distally to gain a greater moment arm than would ordinarily be achieved by inserting into the biceps tendon. This insertion may be either to the ulna or to the radius with the latter having the potential advantage of enhancing forearm supination as well but at the possible risk of causing radial head dislocation. Our aim was to provide the best possible elbow flexion for this child, and so, we utilized the latissimus dorsi musculocutaneous flap with the technique described. We elected to make the distal insertion as far distal on the ulna without overstretching and maintaining the resting length potential of the muscle to maximize elbow flexion and to avoid the risk of radial head dislocation. The ulna also provides easier accessibility for muscle insertion than does the radius. The skin island of a musculocutaneous latissimus flap additionally aids in closing the incision at the recipient site. Good results have generally been reported with pedicle muscle transfers using one of these larger shoulder girdle muscles.