
Abstract
Purpose Fixed-angle devices have been a major advancement in orthopedic fracture care and have become an attractive option for fixation of distal radius fractures. Several volar locking plates exist, but there is insufficient literature comparing the strengths of these plates. This study compares the biomechanical strength of two popular volar locking plate systems (Synthes LCP and Hand Innovations DVR-A) along with a nonlocking volar T-plate (Synthes).
Methods Twenty-three formalin-fixed cadaveric forearms were divided into three groups with similar ages and bone densities. An unstable extra-articular fracture was created using a standardized osteotomy. Each group was fixed with one of the three plates. Each specimen was loaded in axial compression for 2000 cycles at a force of 400 N. Each specimen that completed cyclic testing was loaded to failure. Stiffness, yield point, and ultimate strength were recorded for each construct.
Results Each fixed-angle construct completed all 2000 cycles. The nonlocking plates failed at an average of 560 cycles. The mean stiffness of the DVR-A, LCP, and the volar T-plates were 277.00, 343.17, and 175.67 N/mm, respectively. There was a statistically significant difference between both fixed-angle plates and the nonlocking plate (p<0.05). The difference between each fixed-angle construct did not reach significance. Yield point and ultimate strength could only be determined for the two fixed-angle devices. There was no statistically significant difference between the constructs for both yield point (DVR-A=855.56 N, LCP=894.15 N) and ultimate strength (DVR-A=1,021.97 N, LCP=1,114.87 N).
Conclusions Given our data, fixed-angle constructs withstand cyclical loading representing normal physiologic forces encountered during post-operative rehabilitation. There was no significant biomechanical difference between the two fixed-angle constructs. Our results support that volar fixed-angle locking plates are an effective treatment for unstable extra-articular distal radius fractures, allowing early postoperative rehabilitation to safely be initiated.
Introduction
The incidence of orthopedic injuries is on the rise because of the advancing population age and increase in physical activity. Distal radius fractures are no exception to this increase and constitute up to 15% of all extremity fractures [6]. Furthermore, in the USA, the annual incidence of distal forearm fractures attributable to osteoporosis is 250,000 per year [7]. Osteoporotic bone can complicate the effectiveness of surgical repair and presents the surgeon with treatment dilemmas. The goals of surgical treatment of distal radius fractures are to provide articular congruity [13, 15], maintain alignment, and regain motion early in the postoperative period.
The advantages of volar locking plates over dorsal plates and external fixators have been described in recent literature [10, 13]. External fixators oblige immobility across the joint, which may result in potential muscle atrophy, disuse osteopenia, and tightening of the joint capsule. This complicates rehabilitation and functional outcome, especially for those patients with osteoporosis. Dorsal plates carry the risk of tenosynovitis and tendon rupture due to the proximity of the plate to the extensor tendons. These complications have been reported to necessitate the removal of the dorsal plate in 11 to 33% of cases [1, 4, 12]. Volar plates diminish the aforementioned risks and have improved the outcome in treating distal radius fractures. Furthermore, and critical to reaching the goal of safe, early postoperative range of motion, volar locking plates introduce improvement in the stability of the fracture repair compared to nonlocked volar plates.
At the time of preparation of this manuscript, there were seven different biomedical companies with volar locking plates for distal radius fractures. There are now almost 30. The stability of fixed-angle volar locking plates over dorsal plates has been documented in the literature, but there is minimal data comparing individual fixed-angle plates [8]. The purpose of this study was to evaluate and compare the biomechanical strength of two popular volar locking plates and one standard nonlocking volar plate in the treatment of an unstable extra-articular distal radius fracture.
Materials and Methods
Twenty-three formalin-fixed cadaveric forearm specimens were harvested at a level 1–2 cm distal to the radial head. All soft tissue except the wrist ligaments, capsule, and interosseous membrane were removed. The digits were disarticulated at the metacarpophalangeal joint.
Anteroposterior and lateral radiographs, as well as bone mineral density (BMD) scores were obtained for each specimen. Radial inclination, BMD, and T scores were recorded for each wrist. Specimens were excluded if there was radiographic abnormality such as evidence of prior fracture or abnormal radial inclination. A total of 23 satisfactory specimens were separated into three test groups. Statistical evaluation of the three groups with an analysis of variance (ANOVA) test was performed to ensure similar samples in each group to limit variability.
Each group was assigned to be instrumented with one of three volar plates; group A, DVR-A plate (Hand Innovations, Miami, FL); group B, LCP distal radius plate (Synthes, Paoli, PA); and group C, Volar nonlocking T-plate (Synthes).
Proximal Fixation
Proximal plate fixation was completed first. The plate was placed onto the volar surface of the distal radius in anatomic position and secured with two proximal screws of appropriate bicortical length after drilling and tapping. The proximal screws were nonlocking, cortical screws in all three groups. Nonlocking screws were chosen to standardize proximal fixation in all three groups, as only nonlocking screws are available for the DVR-A plate (Fig. 1).
Distal Fixation
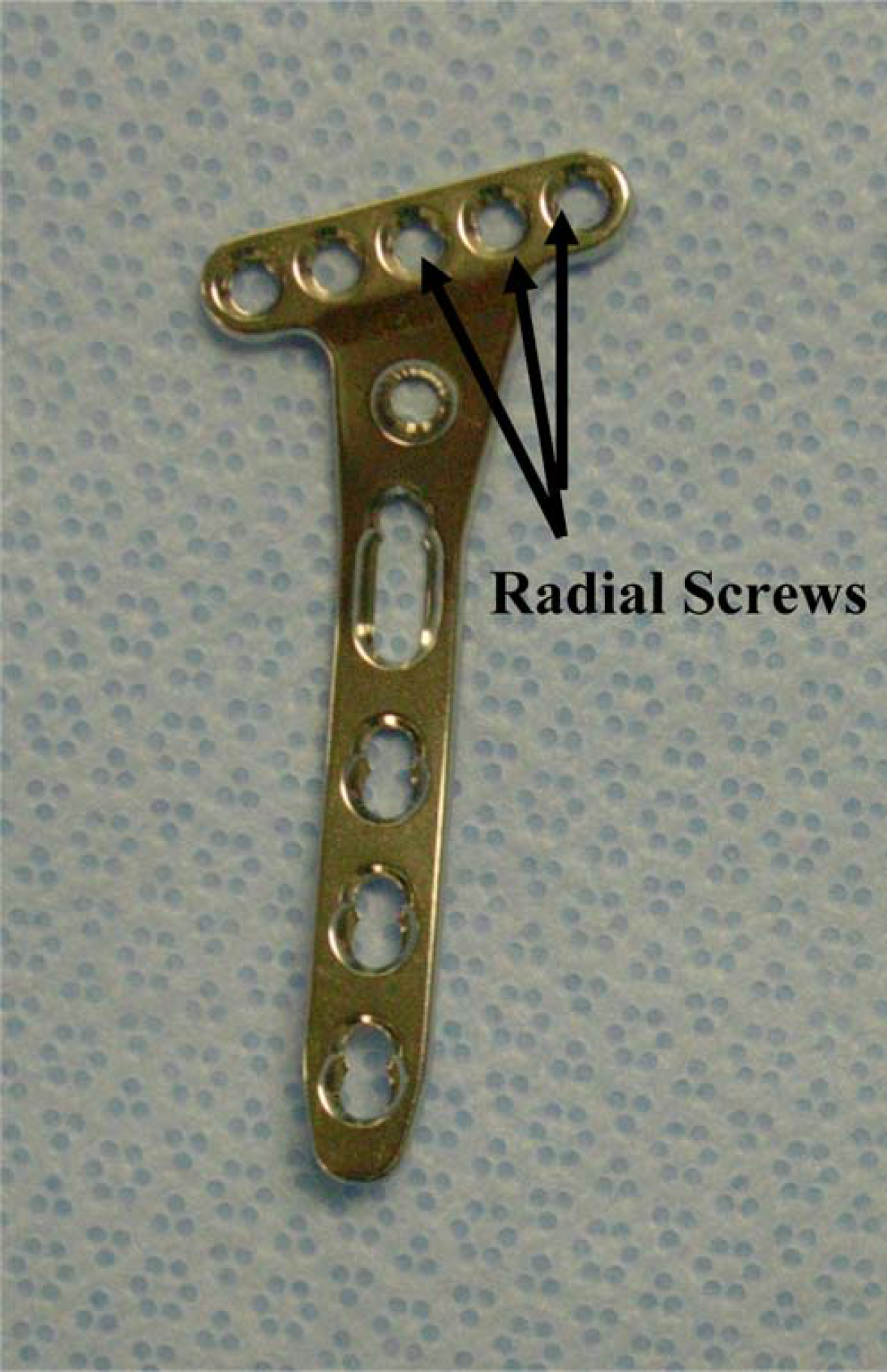
After proximal screw fixation, the distal screw holes were drilled and measured before osteotomy. Each plate had different distal fixation options. The Synthes T-plate had a maximum of three distal screws (Fig. 2). Therefore, to standardize distal fixation between the groups, a total of three distal screws were used for all three plates. The radial three distal screw holes in the Synthes LCP plate were chosen (Fig. 3). The DVR-A plate had two rows of distal screw options. Here, the radial three holes of the proximal row were chosen to be filled (Fig. 1). Each screw hole was then drilled with the appropriate-sized drill bit and guide. Using a depth gauge, the distal screw-length measurements were recorded.
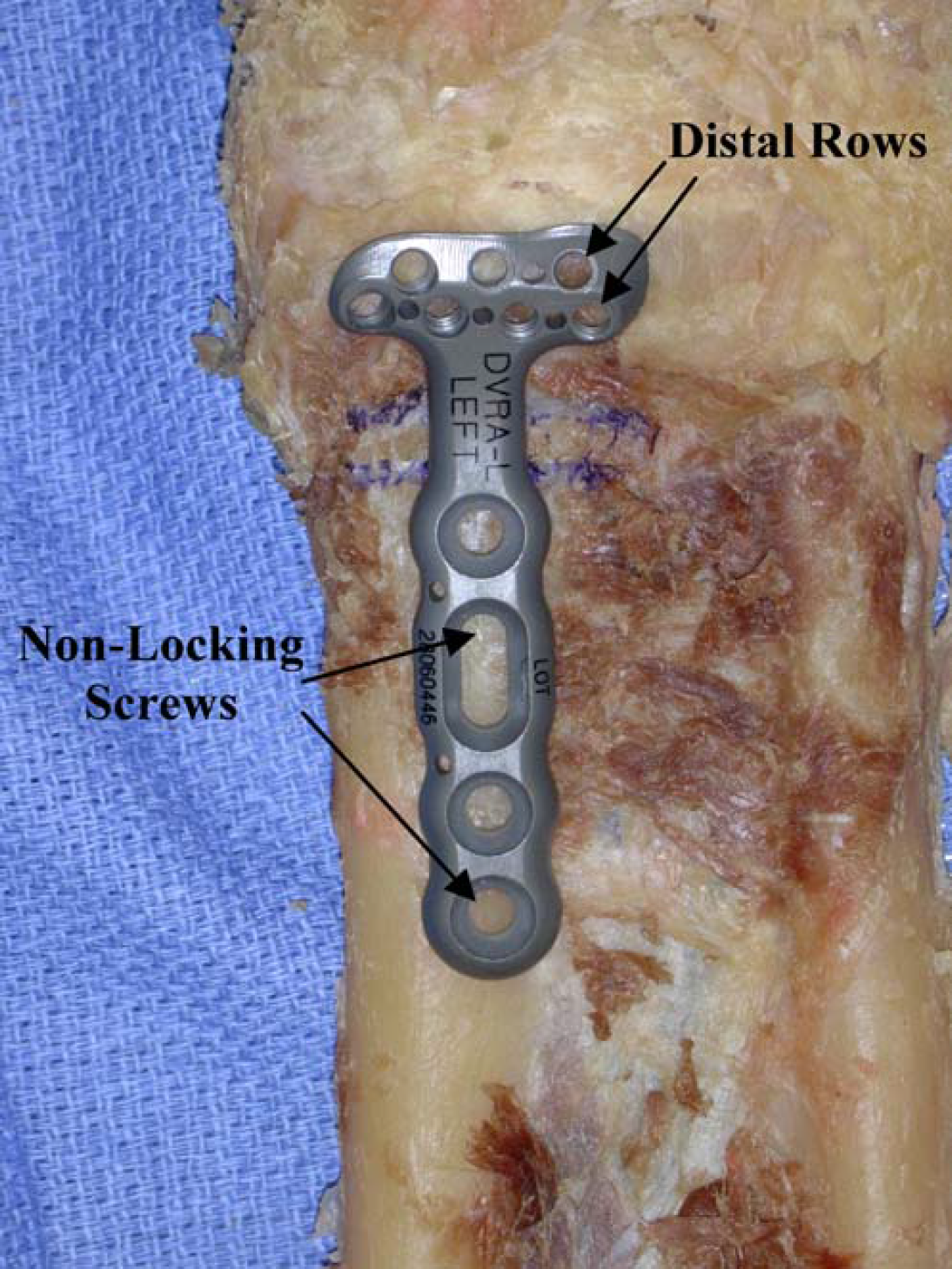
The DVR-A plate with planned osteotomy marked on the volar radius. The distal row of screws is marked as well as the nonlocking proximal screw holes.

Volar T-plate (nonlocking).
Osteotomy
After predrilling and measuring the distal screw holes, as described above, each plate was removed from the bone before distal screw placement. Using a sagittal saw, a 5-mm-wide transverse osteotomy was made in the radius. The distal cut of the osteotomy was made 20 mm proximal to the joint line as described by Osada et al. (Fig. 4)[7]. By removing a 5-mm segment of bone, an unstable fracture pattern with severe metaphyseal comminution was simulated. The plate was reapplied using the previously placed proximal screws. The distal screws were placed through the corresponding, previously drilled holes to ensure an anatomic relationship of the radius after osteotomy and instrumentation (Fig. 5).
A commercially available adhesive was used to pot each specimen both proximally and distally. Distal potting was done to the middle of the metacarpal bones (Fig. 6). Each specimen was placed into a vertical MTS uniaxial load frame (MTS 858 MiniBionix II uniaxial testing machine, MTS Corporation, Eden Prairie, MN). Figure 6 shows an example of a potted specimen in the MTS machine. The specimens were cyclically loaded with a compressive force of 400 N for 2,000 cycles. Putnam et al. described these forces within the range of normal physiologic forces generated through the wrist during a rehabilitation period [9]. The number of completed cycles, as well as implant failure or plate compromise, was documented and recorded. After cyclic loading, the specimens that were still intact were loaded to failure in compression. Yield point and ultimate strength for each construct were then recorded. Using a best-fit technique, stiffness for each specimen was determined.
A student t test to compare data sets was used for statistical evaluation of the biomechanical data. Statistical significance was set at a P value of less than 0.05.
LCP plate.
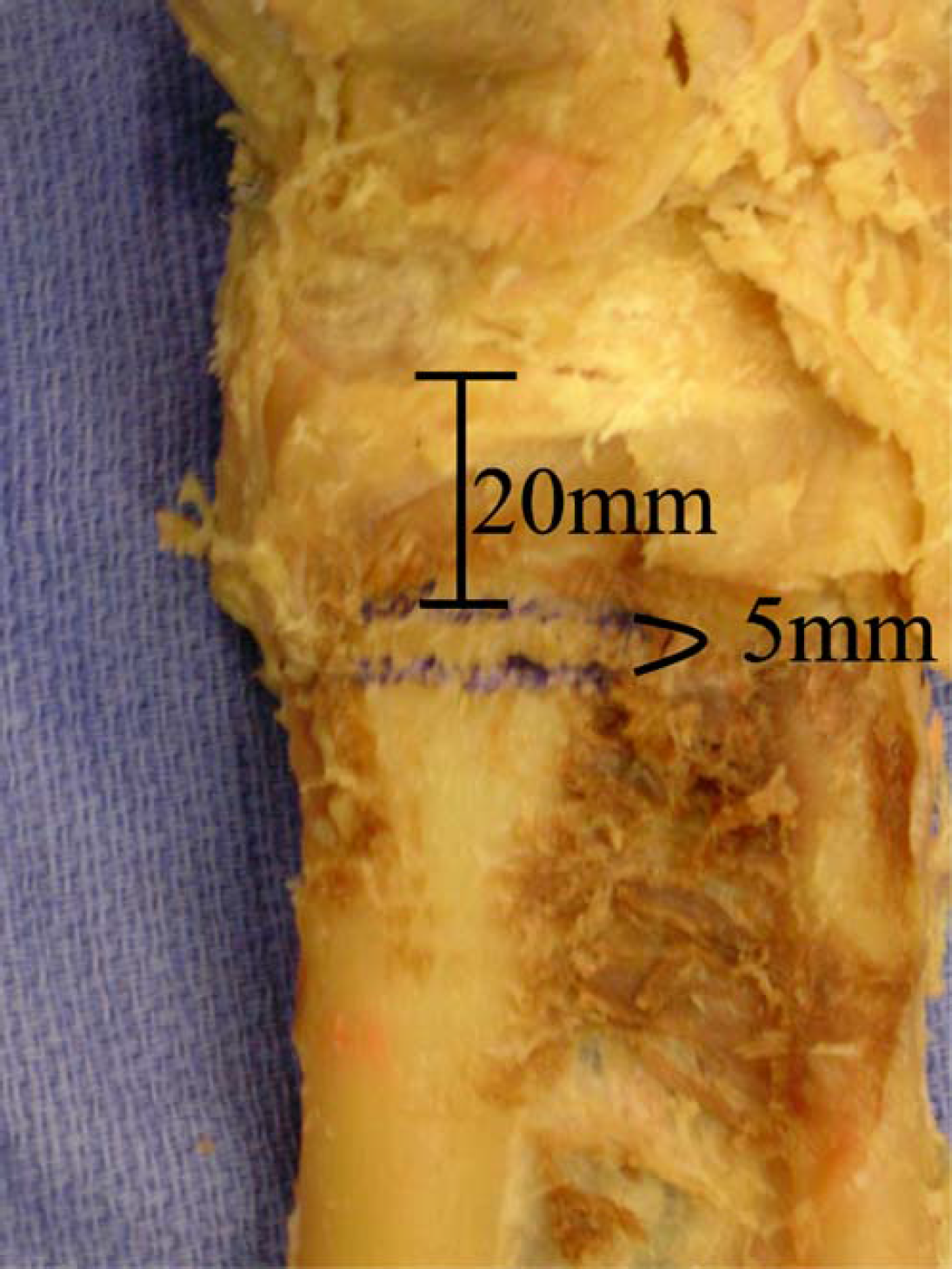
Planned osteotomy.
Results
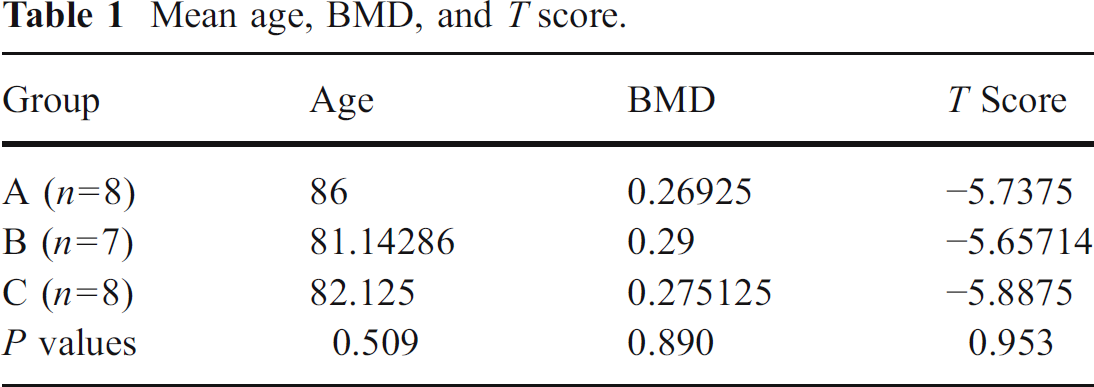
Table 1 shows the ANOVA results between the three tested groups. There was no statistically significant difference between the groups with respect to the average age, BMD, and T scores.
When comparing the biomechanical strength of the respective plates, both the DVR-A plate and LCP plate withstood cyclic loading significantly better than the standard nonlocking T plate (Fig. 7). The standard nonlocking T plate failed at an average completion of 560 cycles, whereas both the DVR-A plate and LCP plate withstood all 2,000 cycles. Only two of the T plate specimens completed cyclic loading.

Volar (left) and lateral (right) views of completed DVR-A plate and osteotomy.

Potted specimen in uniaxial MTS machine.
Both the DVR-A plate (277.0±79.4 N/mm) and LCP plate (343.2±115.3 N/mm) demonstrated a significantly increased stiffness compared with the nonlocking T-plate (175.7±28.0 N/mm; Fig. 8).
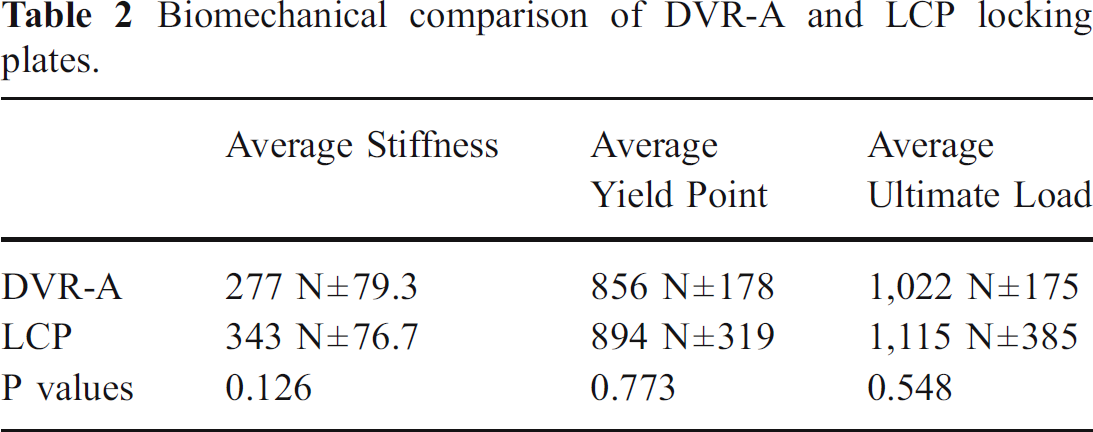
Table 2 summarizes the biomechanical properties of the two locking plates. The LCP plate was found to have greater stiffness, yield point, and ultimate strength when compared to the DVR-A plate. These differences were not statistically significant.
Mean age, BMD, and T score.
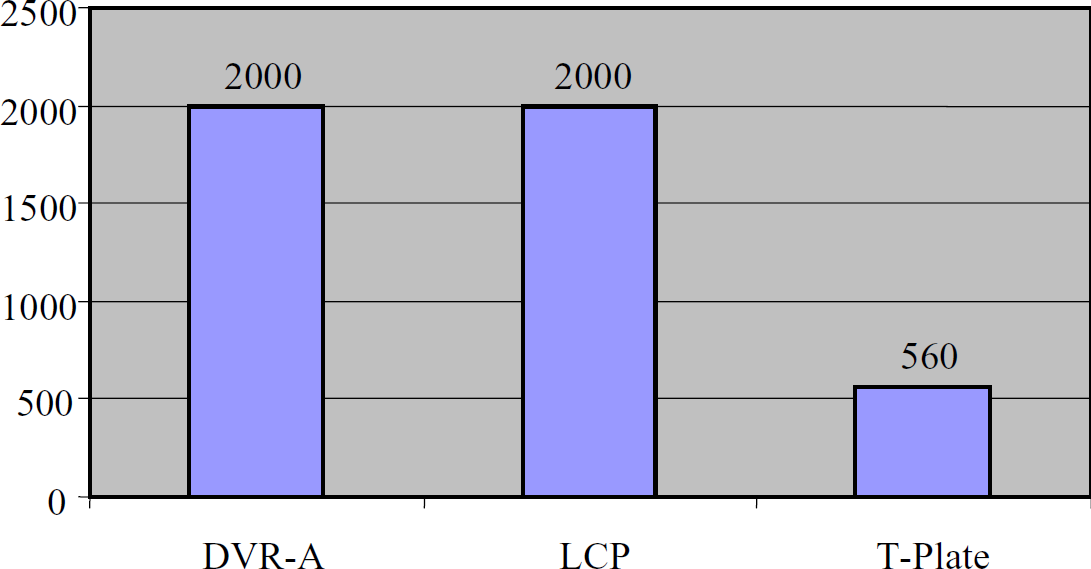
Average number of completed cycles.
Discussion
The advent of fixed-angle locking plates has improved fracture healing and addressed the inadequacies of nonlocked plates. Formerly, a rigid fixation construct with a nonlocked plate was achieved only if there was minimal motion at the joint or if the bone density was sufficient to withstand applied physiologic load. In other words, the stability of the screws in the bone and at the screw–plate interface was possible if the load was kept to a minimum. These are limiting factors that require prolonged cast immobilization even after surgical fixation. In osteoporotic bone, minimal axial stress may permit toggling of the screws and become loose. The locking plate introduced tines at the screw plate interface creating a “single beam construct,” which has been reported to be four times stronger than constructs that allow motion between the screws and plate [2]. Locked plates are ideal for osteoporotic, extra-articular fractures because they decrease the potential for toggling of the screws in the cortex. Furthermore, a fixed-angle device transfers the load from the intact subchondral bone across the compromised metaphysis to the intact diaphysis, which would theoretically permit early range of motion postoperatively, as the construct can withstand physiologic loading.
It is generally agreed that early range of motion postoperatively leads to improved functional outcome. In 1996, Rikli and Regazzoni [11] described a dual plating technique that allowed early active assisted range of motion with satisfactory results in all 20 patients. Fixed-angle devices apply this concept, but allow for a less extensile surgical exposure along with early rehabilitation.
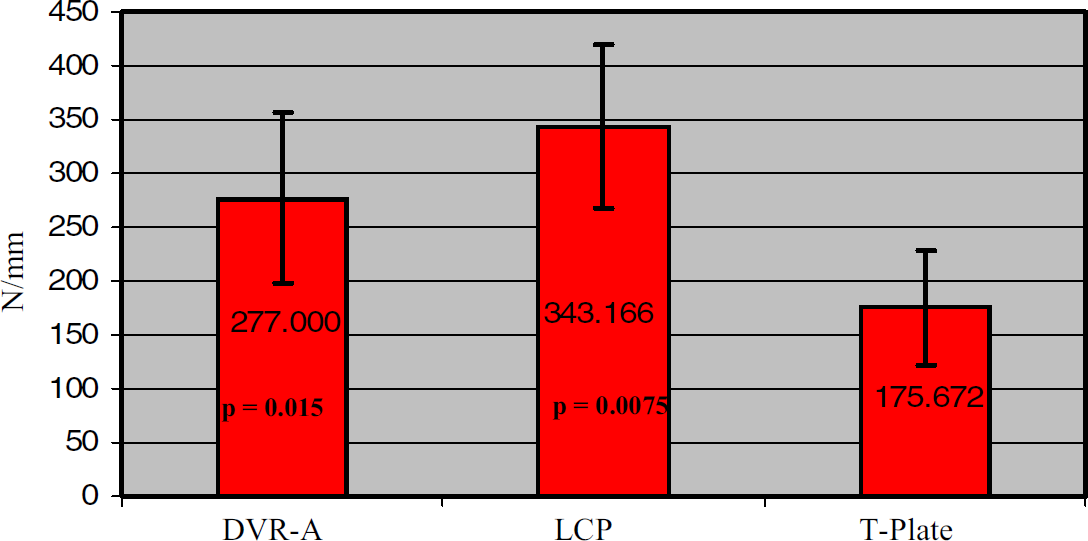
Average stiffness.
Biomechanical comparison of DVR-A and LCP locking plates.
There is little biomechanical data published comparing different locking plates for distal radius fractures. Trease et al. [14] reported no significant differences in stiffness or failure strength between volar locked and nonlocked plates. Similarly, Koh et al. [5] reported that in a wedge osteotomy trial comparing volar locked and nonlocked plates, the nonlocked plates had an average higher value of stiffness, but with a higher standard deviation than the other groups tested. In that same study, however, the nonlocked plates also showed signs of toggling at the screw hole interface. Our work compared three volar plates including two locking and one nonlocking volar plate. Our results strongly indicate that the two locking plates had increased stability in cyclic loading at physiologic loads when compared to a standard nonlocking volar plate. Thus, increased stiffness and maintenance of alignment seen with the two locking plates may permit early range of motion and postoperative rehabilitation. This may not be the case for nonlocking volar plates, dorsal plates, or external fixators. In fact, only two of the nonlocked plates were able to complete all of the cycles during simulated physiologic loading. In addition, our results indicate that there is no statistically significant difference in stiffness, yield point, and ultimate strength between the two locking plates tested.
Limitations of this paper include the use of embalmed cadavers. In one experiment, formalin-treated cadaver bones showed an increase in brittleness and a decrease in energy absorption when compared with frozen cadaver specimens [3]. We did ensure that all three testing groups had similar bone qualities. Nevertheless, one must use caution when extrapolating the data to live subjects. Another potential limitation of our study is the extra-articular fracture model tested. The majority of extra-articular distal radius fractures can be treated closed, and surgical fixation is warranted mostly for intra-articular displacement. However, creating an unstable, comminuted extra-articular fracture pattern ensured a reproducible pattern that would be difficult to simulate using an intra-articular model. Further studies will address intra-articular fractures with fixed-angle devices.
We have shown volar locking plates to have superior biomechanical properties at physiologic loads and can withstand significantly more force before implant failure when compared to standard nonlocking plates for fixation of unstable extra-articular distal radius fractures. These fixed-angle plates are an effective treatment for distal radius fractures to accomplish the surgical goals of stability, maintenance of alignment, and the ability to initiate early motion, all of which may lead to improved clinical outcomes after distal radius fixation.