
Abstract
Arthritis of the first carpometacarpal (CMC) joint of the hand is a common and often debilitating disease. Diagnosis can be readily made with history, physical exam, and radiographic evaluation. Patients with advanced disease who have failed conservative treatment modalities have multiple surgical options including ligament reconstruction, resection arthroplasty, silicone implantation, tendon interposition, or total joint arthroplasty. This article will describe the variety of approaches to treatment as well as the author's preferred method.
Introduction
The carpometacarpal (CMC) joint of the first ray is a diarthrodial saddle joint comprised of two major articulations, the trapeziometacarpal articulation to the thumb and the scaphotrapezial articulation, as well as two lesser articulations, the trapeziotrapezoid and the trapeziometacarpal to the index finger, determined by the axis of thumb compression and function. Given the myriad of activities that an average human undertakes, the CMC joint can be stressed repeatedly in its three main planes of movement: abduction–adduction, flexion–extension, and opposition. An individual with laxity of the ligamentous stabilizers of the CMC joint, namely the anterior oblique (volar beak) ligament and the dorsoradial ligament, can develop synovitis and wear off the cartilage of the CMC joint, with eventual degenerative changes including joint space narrowing, osteophyte formation, ligament attenuation, and eventual dorsal radial subluxation of the joint [4, 5]. It was further demonstrated that during active pinch and release, there existed a dorsal enlargement of the hand indicative of a translation of the metacarpal on the trapezium. If the volar beak ligament was eliminated, the dorsal translation and articular contacts were similar to the values obtained on a patient with known osteoarthritis of the CMC joint [29]. With continued use of the hand, the patient can then develop metacarpophalangeal hyperextension, which further increases pain while decreasing pinch strength and range of motion.
Diagnosis
The typical presentation is a female between 50–70 years of age, complaining of an insidious radial thumb pain that originally worsened with use, has decreased her ability to perform activities of daily living, decreased strength, and decreased dexterity. Opposition requiring activities, such as writing, opening jars, or carrying heavy objects between the thumb and fingers, are instigators of the pain. There has been an increasing weakness of pinch, progressing to stiffness and cramping with increasing stage. As time progresses, the pain may exist at rest. However, there is also a younger group of patients, 20s–30s complaining of pain in the thenar eminence, or cramping in the first web space, resulting from joint laxity and synovitis of the trapeziometacarpal joint. This pain may radiate up the radial aspect of the forearm with activities such as writing. Regardless of the patient's age, the pain is often mitigated by rest and analgesics.
Physical examination often reveals a dorsoradial prominence of the thumb metacarpal base secondary to subluxation due to ligamentous laxity and the pull of the adductor pollicus longus muscle. There is tenderness to palpation at the trapeziometacarpal joint, as well as the scaphotrapezial joint in advanced stages of disease. Crepitus may often be felt, and the grind test of the trapeziometacarpal joint will often produce pain. One can check for translation and ligamentous laxity of the joint with stabilization of the metacarpophalangeal and the interphalangeal joints. Pain with distraction of the trapeziometacarpal joint can help differentiate synovitis.
Radiographs of the CMC joint in the standard AP, lateral, and oblique view can help confirm suspicion of the diagnosis. A stress view of the joint, obtained by a 30° PA view centered on the thumbs while the patient presses the thumb tips together, can help assess the degree of joint space loss and subluxation of the trapeziometacarpal joint [4, 14]. One must be careful to make a diagnosis, not only by radiographic evidence, but also by patient complaints and physical examination. Approximately 25% of women and 8% of men will develop radiographic evidence of degeneration of the CMC joint, yet most remain asymptomatic, and when questioned, only 28% of women with CMC, and 55% with CMC and scaphotrapezial arthritis will admit to pain [1].
The differential diagnosis of CMC arthritis is broad in spectrum. Arthritic diseases, such as rheumatoid arthritis, rheumatoid synovitis, tenosynovitis, osteoarthritis, and septic arthritis; autoimmune diseases, such as systemic lupus erythematosus, psoriatic arthritis, Reiter syndrome, or scleroderma; inflammatory arthridities, such as gout and pseudogout; as well as gamekeeper's thumb, carpal tunnel syndrome, de Quervain disease, and trigger thumb must all be remembered during the evaluation process [4, 9].
Classification
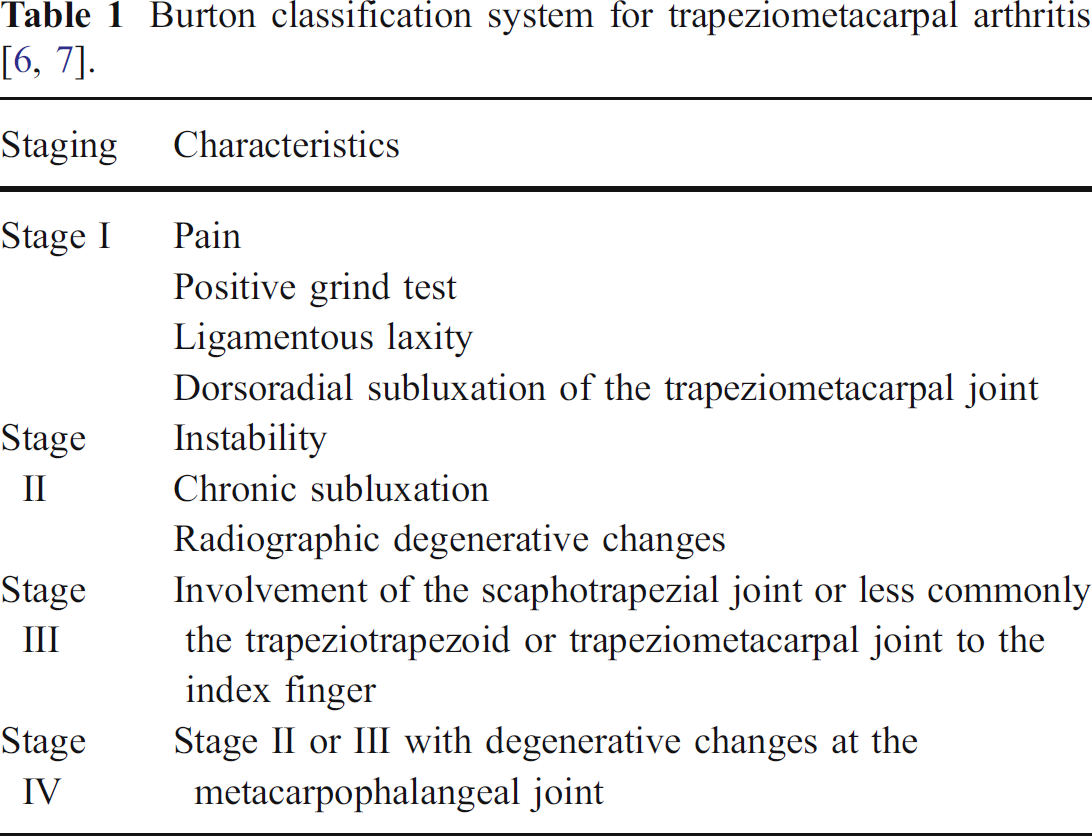
There are two major classification systems for CMC arthritis. The first system was developed by Burton and utilizes clinical signs, patient symptoms, and radiographs (Table 1). Stage I involves early degeneration of the trapeziometacarpal joint characterized by patient reported pain, a positive grind test, and ligamentous laxity, demonstrated by subluxation in a dorsoradial direction. Stage II demonstrates increased instability, chronic subluxation, and degenerative changes evidenced by radiograph. Stage III is a further progression of the degeneration to involve the scaphotrapezial joint, with stage IV as either stage II or III with metacarpophalangeal joint changes [9, 37]. This classification depends on subjective symptoms and objective signs rather than pure radiographic changes and makes large transitions from stage to stage in terms of degenerative changes on radiograph without subclassifying finer differences.
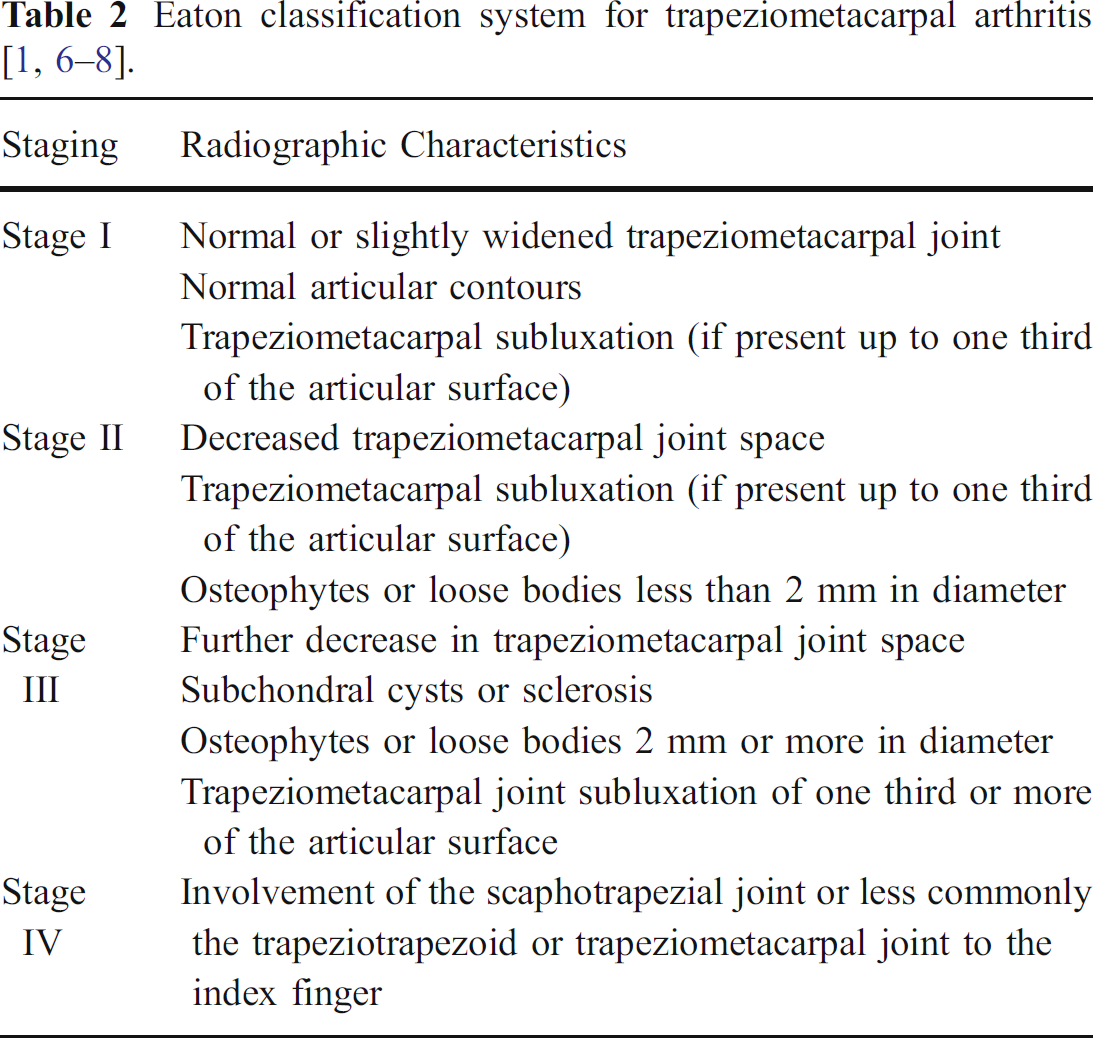
The Eaton classification (Table 2) relies on radiographic changes only, removing the patient's subjective complaints and objective findings from the staging protocol. This is the staging system that, in our experience, is most useful clinically and, therefore, will be the system utilized in the remainder of this paper. Stage I demonstrates a normal to slightly widened trapeziometacarpal joint secondary to ligamentous laxity or effusion, normal articular contours, and up to one-third subluxation. Stage II is progression to involve a narrowing of the trapeziometacarpal joint and osteophytes or loose bodies less than 2 mm in diameter. Stage III is marked by a further decrease in the trapeziometacarpal joint space, subchondral cysts, sclerosis, osteophytes, or loose bodies measuring 2 mm or more in diameter, and subluxation measuring greater than one third of the joint space. Once the degeneration involves the scaphotrapezial joint, stage IV is declared [4, 9, 13, 37].
Non-Surgical Treatment Options
All patients, regardless of their initial staging, require a trial of conservative therapy before any operative considerations. This management consists of activity modification, joint protection, thenar muscular strengthening, and non-steroidal anti-inflammatory drug (NSAID) use, and splinting with a long opponens, or thumb spica, for 3 to 4 weeks. If the patient must continue work, a short thumb-stabilizing splint can be utilized during work hours and switched for the thumb spica during off hours. If symptoms improve, the patient can be gradually weaned off the splint. If initial conservative management fails, physical therapy and corticosteroid injections into the CMC joint may be utilized for pain relief. Note, corticosteroid injections should be used with caution in patients with early-stage disease given their potential to accelerate arthritic degeneration. The goal of conservative management is not necessarily to eliminate all pain and discomfort, but rather to allow increased activities of daily living and an improved quality of life. Day et al. [12] reported success rates of 40% for subjective relief at greater than 12 weeks with a corticosteroid injection followed by 3 weeks of splinting. His outcomes were better for stages 1–3 compared with stage 4 in which no patients reported success or symptomatic relief. Our success rate with conservative management in achieving these goals is 60–70%. Once a trial of non-operative treatment has failed in a compliant patient, surgical intervention is the next step (Fig. 1).
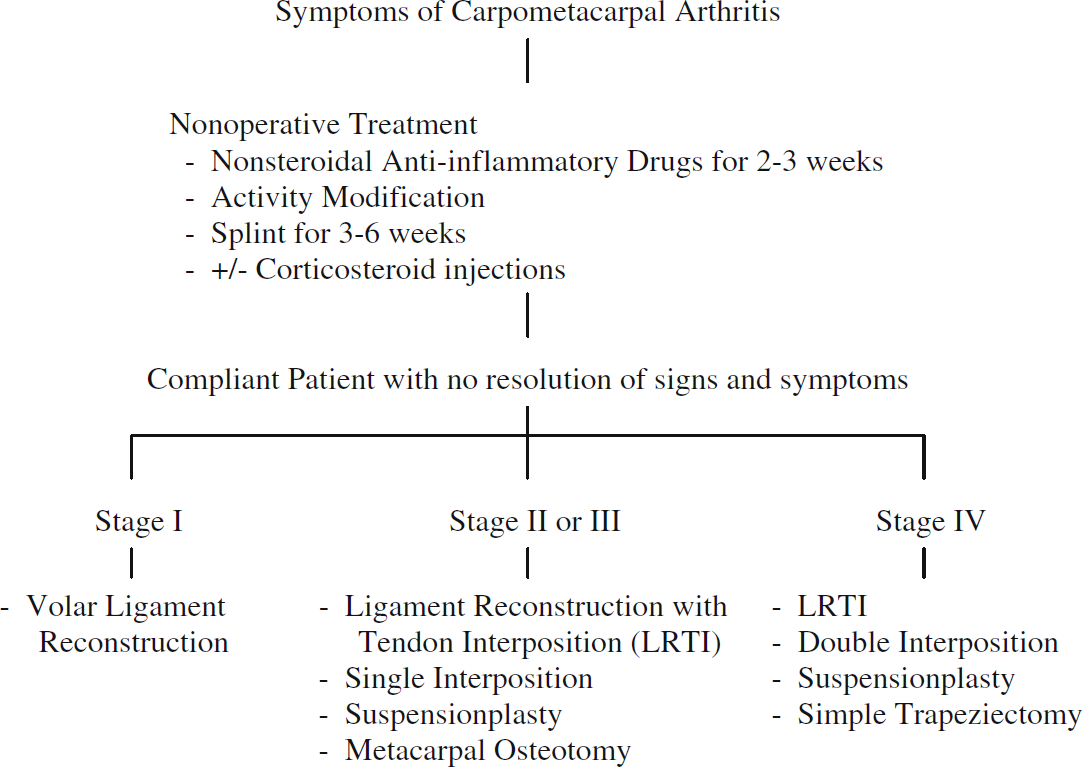
Flow diagram for treatment of carpometacarpal arthritis [1].
Surgical Options
Indications for surgical intervention in first CMC arthritis are similar to the indications for arthroplasty of most joints: persistent pain, decreased function, instability, and failure of conservative management. Since modern surgical intervention for first CMC arthritis began approximately five decades ago, multiple techniques have been introduced. Surgical options vary with the stage and nature of the disease. In early stages, trapeziometacarpal ligament reconstruction and/or arthroplasty have been shown to provide good symptomatic relief while also hindering further degenerative changes [15, 16]. For severe or late-stage disease, some have advocated arthrodesis of the first CMC joint, assuming that there is good mobility of the joints proximal and distal. In light of the success of the various arthroplasty techniques, arthrodesis has fallen out of favor and is generally reserved for post-traumatic or rheumatoid arthritis limited only to the first CMC joint of the hand.
Arthroplasty techniques have ranged from simple partial or complete trapeziectomy to various implant and ligament interposition and reconstructions. These techniques have been generally indicated for stage II or greater disease once the patient failed conservative management.
Excisional arthroplasty involves the removal of the trapezium and a substitution of the flexor carpi radialis (FCR) tendon into the empty space to help decrease the loss of joint space resulting from the surgically induced bone loss. The incision is made from the dorsal base of the thumb to the scaphoid tuberosity on the volar aspect of the wrist and continued proximally along the FCR tendon. The superficial radial nerve branches are protected, the volar capsule around the trapeziometacarpal joint is incised, and the abductor pollicis longus (AbPL) and extensor pollicis brevis (EBP) tendons are retracted dorsally after release of the first dorsal compartment. The radial artery is identified and protected. The trapezium is then excised from dorsal to volar. Attention is turned to the FCR tendon; a 5-cm strip is harvested, being careful to preserve its distal attachment. The tendon is rolled into a ball and inserted into the space created from the excised trapezium [5]. Results indicated an average relief of pain for 6 years, with a reduction of pinch strength and joint height of 30 and 50%, respectively. This technique was later modified to excision of only one half of the trapezium to try to maintain joint height [17, 18]. While this technique removes the trapezium (in entirety or just partially) in an attempt to reduce the pain associated with the disease, complications include a reduction of pinch strength, a loss of joint height with full trapezial excision, and a technique that does not correct pantrapezial involvement with partial excision. This technique addresses the pain from osteoarthritic bony contact, but does not address the main pathology—volar beak ligament laxity.
Tendon interposition arthroplasty with ligament reconstruction was described by Burton and Pellegrini, utilizing an incision extending from the base of the thumb to the interval between the AbPL and EPB. The trapezium is excised completely in stage IV disease or limited to the distal portion in stages II or III. The incision is then extended over the thumb metacarpal to expose the base and proximal shaft, which is debrided of all diseased articular cartilage. A small drill hole is created in the radial base of the thumb shaft. A segment of the FCR tendon approximately 10–12 cm in length is harvested and split distally to its insertion site. This tendon is passed through the drill holes at the metacarpal base. The tendon is tensioned with the thumb in traction and abduction, and then secured to the lateral periostium and itself. The remainder of the tendon is inserted into the defect from the excised trapezium and secured to itself and the deep palmar capsule. The incision is closed in layers, and the thumb is immobilized for 4 weeks, followed by 4 weeks of protected range of motion [5, 8]. Short and long-term follow-up demonstrates favorable results with regards to pain, function, and satisfaction. There is an increase in grip and pinch strength from baseline, an increase in the ease of performing activities of daily living, and a subjective decrease in pain with a majority reporting no pain, or pain with exertional activities only [8, 28, 34].
Brunelli and Brunelli [7] described the utilization of the AbPL to recreate the volar beak ligament, thereby, removing one of the prime deforming forces of the base of the first metacarpal while reconstructing the pathologic laxity of the volar beak ligament. Roberts et al. [31] reported results on 15 thumbs in 14 patients after an average of 21 months of follow-up. Subjectively, 13 of the 14 patients were very satisfied with the results of the operation and were graded objectively as good or excellent in 11 of 15 thumbs. The average pain score postoperatively on a visual analogue scale was 1.2 out of 10.
Complete harvest of the FCR tendon was reported by Naidu et al. [27]. Thirty-nine patients were studied prospectively with disabilities of the arm, shoulder, and hand (DASH) scores, grip strength measurements, pinch strength measurements, and flexion/extension torque recordings. Postoperatively, the patients were followed for a minimum of 24 months. In this study, DASH scores improved from 43 to 12, and both grip and pinch strength improved. However, the contralateral extremity had 2.5 times more fatigue resistance with flexion resistance, and the flexion/extension torque ratio decreased on the operative side.
The technique of ligament reconstruction with tendon interposition removes the pain-generating bone on bone surfaces, recreates the pathologically lax volar beak ligament, and fills the void created by the trapeziectomy in an attempt to decrease subsidence. In our institution, this procedure is the operation of choice for operative candidates. In effort to reconstruct the anatomy without creating decreased fatigue strength, the ulnar half of the FCR tendon is harvested at the muscle-tendon junction, whereas the radial half is allowed to remain. Given the rotation that the tendon makes within the carpal canal, the ulnar half is more suitable for ligament reconstruction.
Double arthroplasty is an extension of the previous ligament reconstruction and tendon interposition (LRTI) and involves resurfacing of both the trapeziometacarpal and the scaphotrapezial joint. The thumb is approached from a volar curvilinear Wagner incision extending from midmetacarpal to the proximal pole of the scaphoid. The thenar muscles are elevated from their origins to gain exposure to the trapeziometacarpal and scaphotrapezial joint, the first metacarpal base, and the FCR tendon. After inspection of the scaphotrapezial joint through a radial arthrotomy, if the joint requires resurfacing, a long strip of FCR is obtained to its insertion. The proximal two thirds is detached and set aside. The distal one third of the FCR is passed through the first metacarpal shaft to perform the trapeziometacarpal joint interposition as mentioned above. The detached tendon is folded to create a double layer and inserted into the space created by the distally resected portion of the trapezium in the trapeziometacarpal joint. The remainder of the tendon is layered and secured to the scaphotrapezial joint creating a biologic resurfacing. If additional tendon is necessary, the flexor carpi ulnaris (FCU) is utilized. The results demonstrated a stable joint with near normal range of motion (90%), an increase of grip strength of 30%, and a slight increase of pinch strength of 12%. Patients graded their results as excellent or good in 96% of the procedures [3]. Livesey et al. reported similar results with restoration of a more dynamic hand, increased strength, and better preservation of joint space as compared to reconstruction with a single palmaris longus tendon alone [24]. This procedure has the theoretical advantage of decreasing subsidence of the first metacarpal by partial trapezial excision, resurfacing the remaining scaphotrapezial joint, and recreating the volar beak ligament. The disadvantage is that, if the resurfacing was to fail, there would remain arthritic bone on bone contact and a potential for continued pain. We feel that the subsidence resulting from complete trapeziectomy with LRTI is not significant enough to warrant such a procedure at our institution.
Mennon introduced an arthroscopic interpositional procedure in 1996 in which the patient's thumb is hung from finger traps in slight pronation and flexion with 5 lb of traction. Two portals are made along the trapeziometacarpal joint line, one dorsal and one volar to the AbPL, separated by 1 cm. The base of the metacarpal, trapezium, volar ligament, and the dorsal ligament are examined, and following inspection, the articular surface of the trapezium is debrided using a round burr until cancellous subchondral bone is visualized. FCR, palmaris longus tendon, fascia lata allograft, or a Gortex patch can be used as interpositional material; the capsule is closed and the patient is placed in a thumb spica splint [25]. Results from the procedure revealed no loss in range of motion, an average increase in pinch strength in 20 of 31 patients, no loss of preoperative range of motion, and subjective reports of no pain, or pain with exertional activities in 88% of patients. [25] Benefits of this technique involve a smaller incision, less extensive dissection, and ability to examine the articular cartilage under surgical magnification. However, at this time, there is no reported technique to allow for volar beak ligament reconstruction arthroscopically.
Meals et al. [19, 22, 23] described hematoma and distraction arthroplasty to aid in basal joint arthritis pain. With this technique, there is piecemeal excision of the entire trapezium followed by K-wire fixation of the thumb in a position of opposition and distraction. Seventeen out of 22 patients were pain-free at 6 months, and 18 of 22 were pain-free at an average of 88 months postoperatively. There was increase in grip strength and key pinch of 21 and 11%, respectively, compared to preoperative values, and 21 out of 22 thumbs were able to adduct to the palm of the hand and oppose to the little finger.
Silicone implant arthroplasty showed initial promising results in terms of improved function and decreased subjective pain. The technique was described by Swanson as involving a straight incision parallel to the extensor pollicis longus (EPL) over the trapezium, with identification and protection of the superficial radial nerve branches. The capsule over the trapeziometacarpal joint is opened with careful attention not to damage the radial artery. The trapezium is removed, and the base of the first metacarpal is squared. A hole is made in the intramedullary canal to receive the prosthesis, which is secured with a tight capsular closure [5, 9, 33]. Original results from the procedure demonstrated an increase in grip and pinch strength, range of motion, and decrease in subjective pain [33].
Although initial results were excellent, long-term results yielded high incidences of subluxation, cold creep, silicone wear, synovitis, and bony erosion. Creighton et al. reported on 151 implants in 1991 and found a 56% incidence of scaphoid cysts as well as 74% metacarpal lucencies or cysts with evaluation, suggesting silicone synovitis; however, the results did not correlate with clinical signs as 84% of patients reported satisfaction with the surgery [11]. Other long-term studies demonstrated similar results with complications including prosthetic wear, radiographic evidence of loosening, and even prosthetic fracture [20, 21].
Titanium arthroplasty arose as an alternative bearing surface to silicone. Naidu et al. [26] utilized finite element analysis, DASH scores, and strength measurements in a 7-year study utilizing 50 thumbs. In this group, pistoning was noted with the finite elemental analysis, and 10 thumbs failed before 9 months. It was reported that, in the remainder of the thumbs, there existed continued swelling in activity, and continued weakness at a 2-year follow-up. Naidu et al. reported that this operation may be used in lower demand patients with good bone stock.
Currently, the idea of total joint arthroplasty is in the new and experimental stages. In the past, there have been implants, such as the Ledoux, Niebauer, and de la Caffiniere, that were tried and have limitations: either silicone in the prosthesis leading to potential silicone synovitis, or high rates of loosening, subluxation, and revision with other materials [2, 10, 32, 35, 36]. Hemiarthroplasty with the Swanson titanium implant and total arthroplasty with the Braun titanium and polyethylene prosthesis are still being investigated with reasonable results to date [6, 30].
Authors' Preferred Technique
Our proposed technique utilizes a more limited incision, with a unique approach to the trapezium, which not only allows easier identification and excision, but also protects the radial artery and the superficial branches of the radial sensory nerve.
The hand is prepped and draped in the usual sterile fashion, utilizing a tourniquet preset to 250 mmHg and an extremity drape. A 2-cm V-incision, apex dorsal, is marked over the first CMC joint. One percent Marcaine is injected, the hand is exanguinated, the tourniquet is inflated, and the incision is created (Fig. 2) with a 15-blade through the skin to the underlying fascia. Dissecting scissors are used to expose the APL and EPB tendons; the APL is retracted volarly, whereas the EPB is retracted dorsally. The tendons are held in this position with a self-retaining retractor. This position also moves and protects the lateral branch of the superficial radial nerve volarly, as well as the radial artery and dorsal branches of the superficial radial nerve dorsally, allowing full access to the joint without fear of injury to neurovascular structures.

Apex dorsal incision overlying the first extensor compartment.
The CMC capsule is capsulotomized with a 64-blade and dissected off volarly and dorsally for later repair. The full extent of the trapezium is identified and morsilized with a small osteotome and mallet. Care is taken not to extend too ulnarly and damage the FCR tendon. The trapezium is then completely resected with a rongeur and confirmed with palpation. The FCR tendon should now be visible at the base of the surgical field.
Attention is then turned to preparing the first metacarpal for reception of the FCR tendon by drilling two tunnels, one through the metacarpal shaft and the second through the dorsal aspect of the base (perpendicular to the nail bed) with a 3-mm drill bit (Fig. 3). The two tunnels should create a 90° angle, and they are cleared of remaining debris with a small courette with care to avoid destruction of the bone bridge just created.

Drill holes for the passing of the tendon graft. The first hole is centered on the articular surface and aimed straight down the medullary canal; the second is on the dorsal side of the thumb, perpendicular to the first drill hole as well as the plane of the thumb nail.
The FCR tendon is now ready for harvest. The distal aspect of the tendon sheath is opened, utilizing dissecting scissors, and a tendon passer is inserted and passed proximally. The volar aspect of the forearm is incised (approximately 1 cm) over the tip of the tendon passer, and dissection is carried out to identify the FCR tendon sheath and tendon. The FCR proximal to the tendon passer is secured completely with a hemostat to prevent splitting of the tendon proximally. The ulnar half of the FCR tendon just distal to the hemostat, at the end of the tendon passer, is incised and split distally. This ulnar half is inserted into the tendon passer and pulled distally with slow, constant pressure until it is split completely to its insertion at the base of the second metacarpal.
The free FCR tendon is now passed through the shaft and out the dorsal aspect of the first metacarpal, utilizing the previously drilled passage. The tendon is tensioned, allowing the metacarpal to assume an abducted and slightly flexed position and secured in place with 3-0 Ethibond. The remainder of the tendon is wrapped around the intact FCR tendon and secured again with 3-0 Ethibond, creating a type of “anchovy” (Fig. 4). The site is irrigated, the capsule and subcutaneous tissue is closed with 2-0 Vicryl, and the skin is approximated with 5-0 Nylon. A thumb spica splint is applied for 2 weeks.
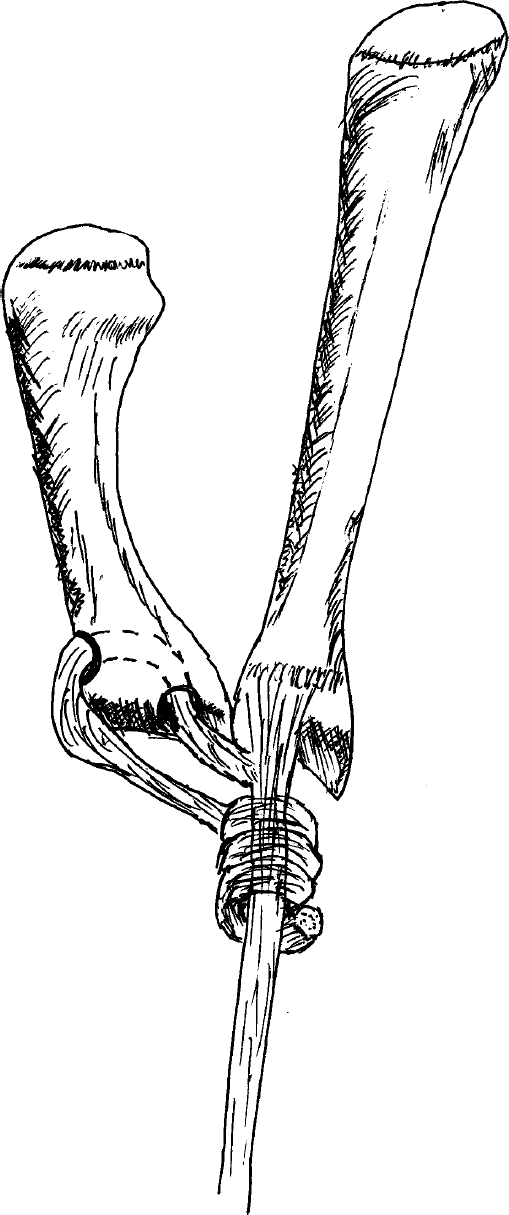
Artists rendition of the FCR tendon weave (compliments of Ian Duncan, MD).
Conclusion
Numerous techniques have been described in the literature to correct the common problem of basal joint arthritis. Multiple options, therefore, exist depending on the surgeon's education, comfort level, and frequency of correction. The main contributor to the pathologic process is the attenuation of the volar beak ligament and resultant subluxation of the joint surface. Abnormal force transmission occurs, resulting in osteophyte formation, stiffness, pain, and decreased function. The surgical option that is chosen should address the pain generated by bone on bone contact, but also restore the normal tension of the volar beak ligament. This restoration helps to reposition the thumb metacarpal in its anatomic position, yielding increased mechanics of the thumb. Operative techniques that address these criteria include the LRTI and double LRTI. Our senior author (J.T.) prefers to remove the entire trapezium and surrounding osteophytes to help eliminate the postoperative complication of recurrent bone on bone contact and resultant pain. The ulnar half of the FCR is utilized to reconstruct the volar beak ligament, and the remainder of the tendon acts as a spacer to decrease subsidence and fill the void created by the excised trapezium.
Our variation on the classic LRTI repair utilizes the theory of previously proven techniques of volar beak ligament reconstruction and tendon interposition. Our approach gives direct access through the first dorsal compartment to the trapezium while separating the overlying EPB and APL tendons to protect the radial artery and superficial radial nerve branches, respectively. This protection allows the surgeon to work unhindered and without fear of damage to these structures. While the technique is utilized in our institute for management of most operative cases of CMC arthritis, it is not the only repair that is effective. Our approach has yielded results that are comparable in short-term follow-up (5 years), in terms of function and subjective pain relief compared to the more traditional approaches and studies (unpublished data). The ligament reconstruction and tendon interpositon is a tool for a general orthopaedic surgeon, as well as a hand specialist, to help the management of a fairly common arthritic complaint.