
Abstract
Leiomyoma is a rare benign tumor of nonstriated muscles. Its common elective localization is in uterus muscle, but it may involve the hand. Limb localization is rare, usually in the lower limbs. We report a case of a 70-year-old women who presents a leiomyoma of the right index finger. A surgical excision was performed. The result was good without recurrence. We report the diagnosis, prognosis, and therapeutic aspects of this tumor, with a literature review.
Introduction
Leiomyoma is a benign tumor of nonstriated muscles [2, 5, 12]. The hand is a very rare location [1, 13]. It is seen more frequently among women than men, most often in the third and fourth decade of life [11]. It should be included in the differential diagnosis of subcutaneous masses of extremities.
Clinical Case
A 70-year-old right-handed woman presented with a painful mass of the flexor surface of her right index finger. Physical examination revealed a painful 1.5 × 1 cm round, freely movable mass with firm consistency, associated with sensory impairment (Fig. 1). The x-ray examination of the right index finger was normal without bone involvement and without microclacification. Tumor excision was performed under brachial-plexus block anesthesia. Macroscopic description underlined a round and encapsulated grayish nodule with firm consistency near the neurovascular bundle (Fig. 2). The microscopic study demonstrated a capsulated lesion of elongated cells white monomorphic cigar-shaped nuclei and no atypia. The immunohistochemical phenotype was positive for smooth muscle actin but negative for S-100 protein and CD34 (Fig. 3). At 6 months follow-up, the incision was healed, motor and sensory function were intact, and there was full range of motion. Neither recurrence nor surgical morbidity was observed. There was no evidence of other masses elsewhere in the body.
Discussion
Leiomyoma is benign tumor of nonstriated muscle [2, 5, 12]. The uterus is considered the most common location for leiomyoma [1, 11, 14]. When it occurs in the extremities, it is more common in the leg, ankle, and foot [9, 13] than it is in the upper extremity. Hachisuga et al. [5] reported 562 cases of leiomyoma, among which there were 229 cases located in the calf and the ankle, 48 cases in the head, and 56 cases in the hand.
In the literature, we found 147 cases of leiomyoma of the hand [6, 13]. It is a rare pathology, but it is not exceptional. The mechanism of these tumors is still not clear, though many authors claim that this tumor arises from tunica media layer of veins [1, 2, 5]. Leiomyoma of the hand is associated with pain in more than 80% of cases. This pain may be a minor tingling or intense. It may appear spontaneously or be caused by contact and cold. All authors note progressive pain, although it was painless at the beginning. The main mechanisms that may explain the pain are still hypothetical. It may be due to peripheral nerve fibers in contact with the tumor [5, 8, 10] or attributed to active contracture of the tumor smooth muscle elements resulting in local ischemia [11, 14].

Subcutaneous nodule of the second phalange of the right index.
In the literature, the average diameter of the tumor is less than 2 cm. There was no case of spontaneous regression of the tumor [3, 5, 13]. The evolution of the tumor is classically benign. One case of bone erosion (proximal phalanx of the index) and one case of large tumor of hand measuring 7 cm are reported [4, 7].
The treatment of leiomyoma of the hand is surgical consisting of simple excision of the mass and ligation of feeding vessels [1, 10, 12, 14]. The tumor occasionally lies in close proximity to a nerve and vessel, especially when located in the volar surface of the hand. Complete excision is usually curative [2, 3].

Macroscopic aspect of a leiomyoma of the index note, its proximity to the medial pedicle.
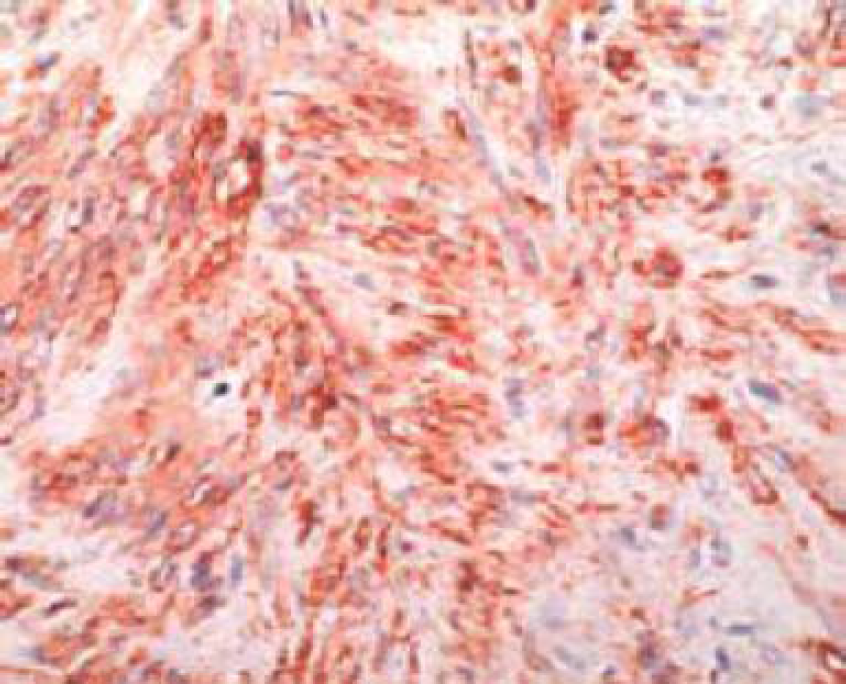
Immunohistochemical aspect of leiomyoma.
Conclusion
Leiomyoma is a rare tumor of the hand. Its diagnosis must be considered when a patient presents with an isolated painful nodule with a slow growth. The prognosis is good after surgical exeresis without risk of recurrence.