
Abstract
Traditional management of unstable fourth and fifth carpal–metacarpal (CMC) fracture–dislocations (fx–dislocs) of the hand includes closed reduction and percutaneous pinning (CRPP) versus open reduction internal fixation (ORIF). Traditional trajectory of pin placement is toward the base of the hook of the hamate. Our case series of CMC fx–dislocs treated with this trajectory led to the development of ulnar deep motor branch symptoms (sxs). We attempt to propose an alternative trajectory that could lower the chance of iatrogenic injury. Five fresh frozen cadaveric specimens underwent percutaneous pinning of the fifth CMC joint using fluoroscopic guidance. Each cadaver was dissected, and the proximity of the deep motor branch of the ulnar nerve was measured in relation to a pin that penetrated the volar cortex. Our results confirm the close proximity of the deep motor branch of the ulnar nerve to the volar cortex of the hamate and demonstrate the potential for iatrogenic injury during CRPP of the fifth CMC fx–dislocs, especially with penetration of the volar cortex. By demonstrating the close proximity of the deep motor branch to the volar cortex of the hamate in cadavers, we highlight the potential for iatrogenic injury with CRPP of CMC fx–dislocs as seen in our case series. We recommend a more midaxial starting point on the proximal metacarpal with a trajectory aimed at the midbody of the hamate to prevent penetration of the hamate volar cortex and limit the chances of iatrogenic injury.
Keywords
Introduction
Fracture–dislocations of the fourth and fifth carpal–metacarpal (CMC) joints are well-described in the literature. However, there is little commentary available with regards to ulnar nerve injury related to these fractures and their management. A handful of case reports exist describing various levels of neuropraxia of the ulnar deep motor branch and postulate several theories that include repetitive blunt trauma, initial fracture displacement, compression from hematoma, traction injury, and iatrogenic injury from operative intervention. Our senior orthopedic surgeon (JSR) had three cases of ulnar deep motor neuropathy after closed reduction and percutaneous pinning (CRPP) of fourth/fifth CMC fx–dislocs. The following case is our primary patient; the other two patients were referred to our institution after their index surgery.
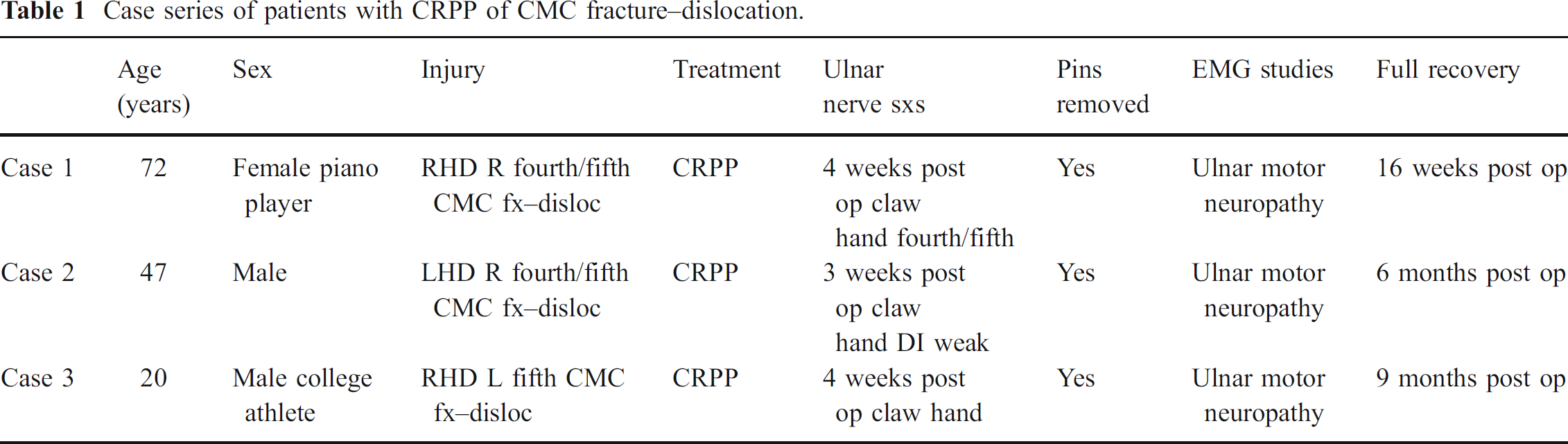
Case 1: A 71-year-old female, right-handed pianist sustained a fx–disloc of the fourth and fifth CMC joint of her left hand status post motor vehicle accident. No neurological deficits were noted on presentation. Three days post injury, she underwent CRPP. Four weeks post surgery, she developed a minor claw hand deformity of her ring and small finger consistent with complete palsy of the ulnar deep motor branch. The Kirshner wires were removed and she underwent urgent electromyography (EMG) and nerve conduction study (NCS) that was consistent with severe ulnar deep motor neuropathy. That same day, she was taken urgently to the operating theater for wound exploration that revealed an intact nerve with significant surrounding scar tissue. Four months after decompression, the patient fully recovered without residual pain or deficit.
The other two patients' clinical courses were fairly similar and are demonstrated in Table 1. All patients demonstrated physical symptoms of ulnar deep motor neuropathy along with consistent EMG/NCS studies. All patients underwent pin removal and achieved full recovery without residual pain or deficit.
History
One of the earliest descriptions of ulnar nerve palsy in carpometacarpal fracture–dislocations is provided by Francis Howard from the Sahlgrenska Hospital of Hand Surgery in Gothenburg, Sweden [4]. He describes the susceptibility to injury of the deep motor branch with fractures of the pisiform, hamate, and fourth and fifth metacarpals.
Various occupations have been associated with ulnar nerve symptoms at the wrist that include gold polishers, oyster openers, and cutlery workers. It is their occupation-specific repetitive trauma to the ulnar aspect of the hand that is believed to cause irritation to the ulnar nerve in Guyon's canal, oftentimes from a ganglion cyst. Howard describes six cases of closed fractures to either pisiform, hamate, or fourth/fifth metacarpal with varying degrees of ulnar nerve symptoms. In his study, he utilizes “digital span” (the max abduction length between tips of index and small) and abduction strength (resistance against forced adduction). Howard recommended accurate assessment of ulnar nerve function with these injuries on presentation to afford better observation of progression. He recommended evacuation of a hematoma early to prevent ischemic necrosis of the nerve. He also advocated wound exploration and nerve decompression at 6–8 weeks if there was no documented improvement from initial presentation.
Anatomy and Ulnar Nerve Injury Classification
As described by Shea et al., anatomically, the ulnar nerve lies in the relatively narrow confines of Guyon's canal as it passes across the wrist into the hand [9]. In Guyon's canal, the ulnar nerve passes radial to the pisiform and ulnar to the hook of the hamate. Just beyond the pisiform, the ulnar nerve splits into a superficial and a deep branch. The superficial branch upon exit from the canal passes through a fat pad deep to the palmaris brevis muscle which it supplies before continuing subcutaneously to provide sensation to the ulnar aspect of the hypothenar eminence and the small and ulnar half of the ring fingers. The deep motor branch along with the ulnar artery make an abrupt turn around the hook of the hamate to enter the narrow interval between the abductor digiti minimi and flexor digiti minimi. It then penetrates the belly of the opponens minimi and follows along the deep palmar arch to innervate the interossei, lumbricals, and flexor pollicis brevis.
Case series of patients with CRPP of CMC fracture–dislocation.
Shea et al. described three types of syndromes [9]. The type I syndrome includes a complete motor palsy to ulnar innervated muscles and a sensory deficit in the palmar distribution of the hypothenar eminence and the ulnar two fingers. Normal sensation on the dorsum of the ulnar aspect of the hand locates the lesion distal to the origin of the dorsal cutaneous branch and hence distal to the elbow. This lesion is located proximal to Guyon's canal and as result compresses both sensory and motor portions of the nerve before its division.

Starting point for traditional K-wire placement (left). Dissection demonstrating the extreme proximity of deep motor branch (arrow) with K-wire penetration through volar cortex of hamate (right).
The type II syndrome has normal sensation but motor nerve palsy. The superficial sensory branch is preserved whereas only the deep motor branch is injured. This injury is located at the start of the division of the motor and sensory branches as the motor branch hooks around the hook of hamate. This is purely a motor deficit.
The type III syndrome involves sensory deficits to the volar surface of the hypothenar eminence and fourth and fifth fingers from compression to only the superficial sensory branch. There is no associated motor deficit or atrophy. This is purely a sensory deficit.
Pathophysiology
In a novel cadaver study by Yoshida et al., the anatomy and pathomechanics of ring and small finger carpometacarpal injuries are elegantly defined [10]. Using a custom made jig that was created to hold fresh frozen cadaver upper extremities, Yoshida et al. were able to reproduce to a certain degree a pattern of injury after axial loading of the fourth and fifth carpometacarpal joints with the fingers held at 20° flexion at the ring metacarpal phalangeal joint and 30° flexion at the small metacarpal phalangeal joint, forearm neutral, 90° elbow flexion, and 20° wrist extension [10]. After loading the cadaver extremities with simulated axial trauma, they were then dissected to examine the anatomy of the injury. The study showed that the mode of failure follows either a ring or small metacarpal neck/shaft fracture or a ring/small fracture–dislocation pattern. None of the specimens failed with a combination of both. The particular pattern of injury is dependent upon whether the load was transmitted at the distal dorsal aspect of the fourth/fifth metacarpal neck or axially transmitted through the shaft. Yoshida et al. also found a strong contribution from the intermetacarpal ligaments and metacarpal–carpal ligaments in certain injury patterns [10].
Methods and Materials
A series of fresh frozen cadaver dissections was performed after percutaneous pinning of the fifth CMC joint. Four cadavers were male, one was female. Three cadaveric specimens were right hands, two were left hands. The age range for the cadaver limbs was 61 to 89 years old. All cadavers were obtained from Life Legacy Foundation, Tuscon, AZ, USA.
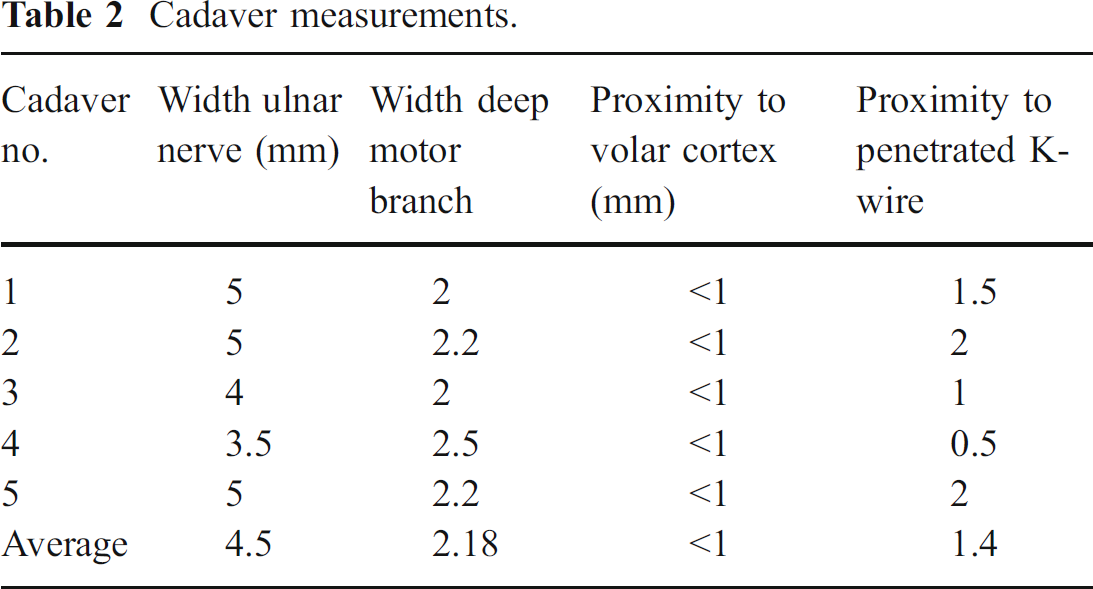
Cadaver measurements.
Operative Technique
The cadavers were thawed for 24 h before the procedure. Using a mini c-arm fluoroscope for guidance, a 0.045-in. K-wire was introduced percutaneously from the dorsal medial aspect of the base of the fifth metacarpal (Fig. 1) and directed in a palmar and radial trajectory across the carpometacarpal joint toward the base of the hook of the hamate. It was not unusual to reposition the K-wire with a second or third pass for adequate placement. An additional K-wire is often used in clinical practice to aid in stability and increase rotational control. K-wire placement was confirmed with fluoroscopy.
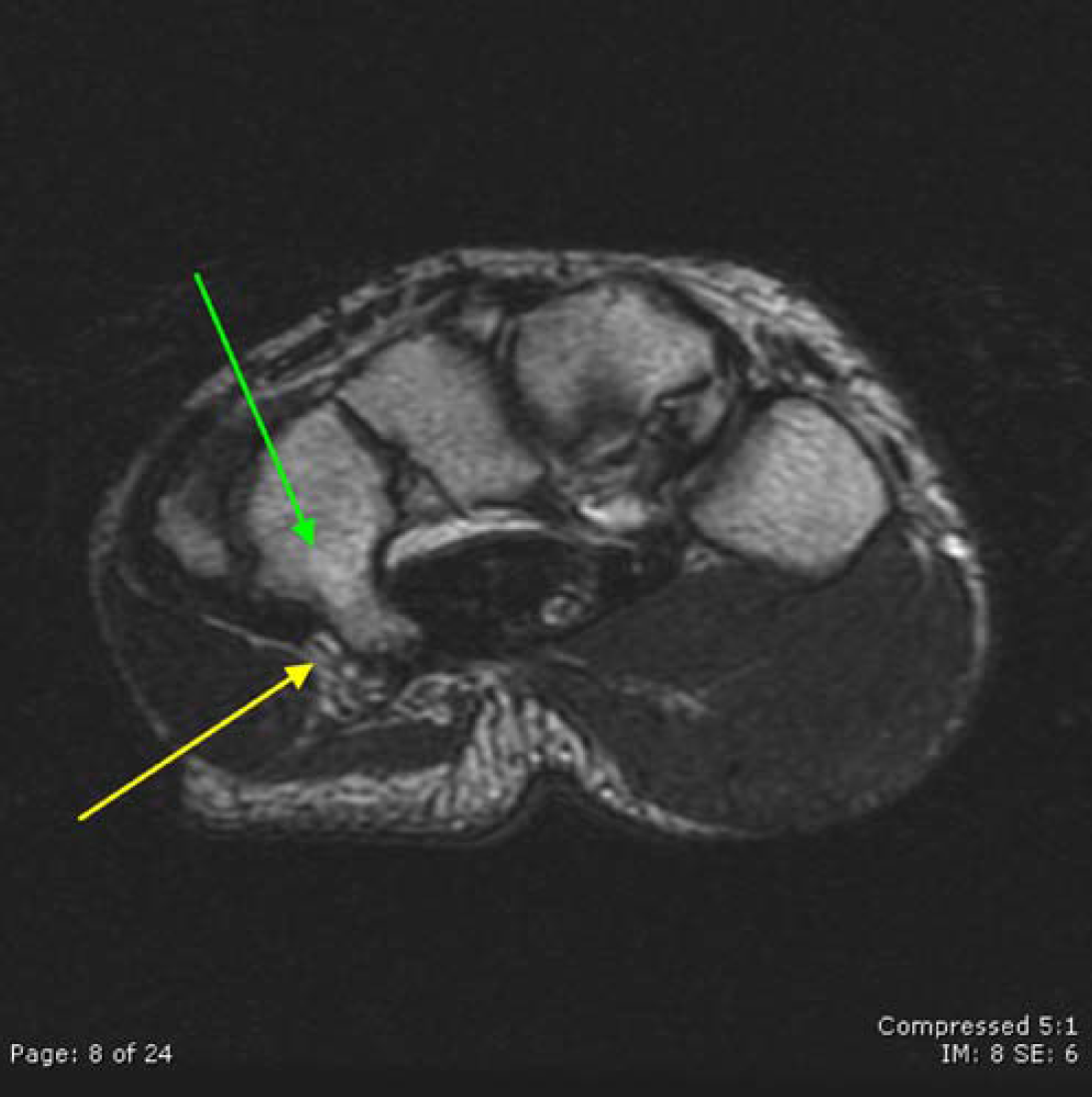
T2-weighted axial wrist MRI. The deep motor branch of ulnar nerve can be visualized abutting the hook of the hamate. Green arrow hamate, yellow arrow deep motor branch ulnar nerve with hypointense central signal surrounded by hyperintense rim of signal consistent with fat.
Dissection was then performed by a single investigator. The following were measured using a standard millimeter rule:
The distance between the deep motor branch and the volar cortex.
The width of the deep motor branch and its proximity to the volar cortex of the hamate.
The distance between the K-wire that had penetrated the volar cortex to the deep motor branch.
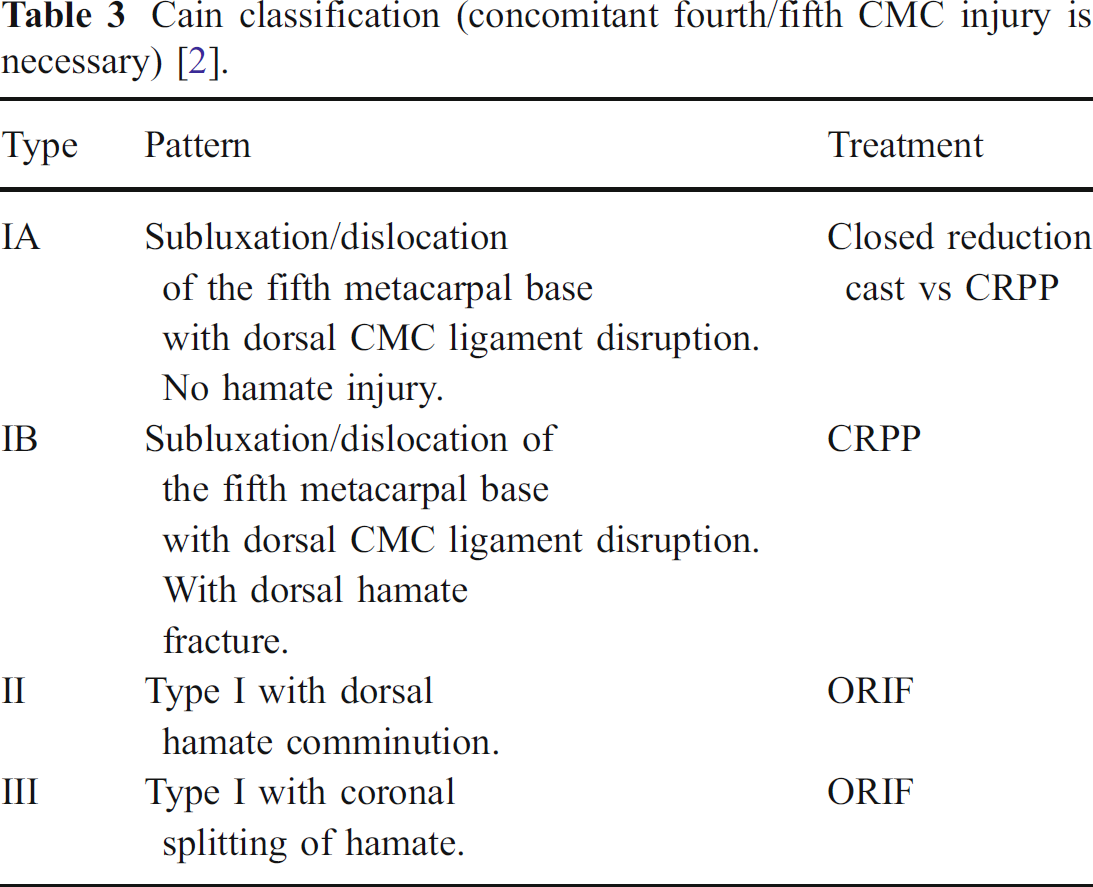
Cain classification (concomitant fourth/fifth CMC injury is necessary) [2].
Care was taken to maintain a moist environment using saline mist. Guyons' canal was dissected from proximal to distal, and the three branches of the nerve and the hook of hamate were identified (Fig. 1). If the K-wire had not yet penetrated the volar cortex, it was then advanced through the cortex at the time of dissection. Measurements were then taken to demonstrate the proximity of the K-wire to the deep motor branch. To confirm the cadaver results, digital magnetic resonance imaging (MRI; performed at our institution) of the wrist of five anonymous patients were reviewed with the assistance of a musculoskeletal radiologist. The images were able to demonstrate a close correlation with our cadaver dissections. Using T2-weighted axial cuts, it is possible to visualize the deep motor branch of the ulnar nerve as it courses over and around the hook of the hamate.
Results
The results confirmed our hypothesis that the deep motor branch is in extreme proximity to the base of the hook of the hamate. The measurements are presented in Table 2. Based on our cadaver dissection, the average distance between the deep motor branch and a penetrated Kirshner wire was 1.4 mm. The deep motor branch appears to lie on the volar cortex of the hamate. The deep motor branch was effectively touching the volar cortex of the hamate and was within 1 mm of the cortex. The cadaver measurements were also very close to the measurements obtained from the MRI images. Using the MRI images, the average distance between the deep motor branch and the volar cortex of the hamate was measured to be 1.53 mm (Fig. 2).
Discussion
Sacks and Peterson described injury to the deep motor branch of the ulnar nerve after conservative management [8]. In their case report, a 61-year-old man injured his right hand after a fall, complaining of throbbing and swelling pain. X-rays showed an intraarticular fracture of the base of the fifth metacarpal with dorsal and ulnar displacement of the metacarpal shaft. Under general anesthesia, closed reduction was successfully performed and maintained in a well-molded short arm cast that incorporated the fifth metacarpophalangeal joint in 60° flexion with the wrist in neutral. Four weeks post cast, there was radiographic evidence of healing. The fracture site was nontender and stable. Two weeks after removal of the cast, he had difficulty writing with wasting of first dorsal interosseus and intrinsics. At 4 months, full recovery was obtained. Marck et al. also described failure of conservative management with cast therapy (loss of reduction) that resulted in open reduction and internal fixation using plates and cancellous screws [6]. Bora and Didizian also described satisfactory treatment of this injury with minimal ulnar displacement with molded cast therapy [1]. Patients with dislocations in their series were treated with open reduction and percutaneous pinning because of the inherent instability of the fracture. The deforming forces from the extensor carpi ulnaris and hypothenar muscles result in proximal migration of the metacarpal shaft.

The x-rays demonstrating the lateral projection post CRPP using the new trajectory. It is clearly shown that the K-wire enters into the body of the hamate with no chance for penetration of the volar cortex. The image on the right shows the outline of the hamate and the new trajectory of the K-wire.
In another case report by Murphy and Parkhill, they described an ulnar motor nerve lesion 8 weeks after a nondiagnosed fracture–dislocation of the base of the fifth metacarpal with volar dislocation of the metacarpal shaft [7]. The injury was treated with open reduction and internal fixation with K-wires in addition to an exploration of Guyon's canal and ulnar neurolysis. At 4 months follow-up, the patient continued to have mild weakness.
The study of Dahlin et al. is one of few to report a likely iatrogenic injury to the deep motor branch of the ulnar nerve after primary treatment of two cases (one second–fifth CMC fx–disloc, one third–fourth CMC fx–disloc) with plate and screws and screws alone, respectively [3]. Both patients on follow-up demonstrated partial ulnar neuropathy that resulted in reoperation, removal of hardware, and neurolysis at a later date that led to eventual functional recovery. Dahlin et al. stressed the need for accurate documentation of ulnar nerve function pre and post treatment to better elucidate a cause for the ulnar nerve palsy. He postulated that reposition, drilling, or application of screws could be a cause for injury.
Finally, percutaneous pinning using smooth transarticular K-wires was described by Cain et al. in the management of these injuries [2]. Cain advocated treatment options based on the injury pattern (Table 3). He proposed that stable type I injuries be treated with closed reduction and cast immobilization for 4 weeks. In unstable type IA injuries, he recommended percutaneous pinning. For type IB lesions, because of their unstable nature, open reduction with pinning was performed. Type II injuries were inherently unstable, requiring minimal flexion of the fifth metacarpal to dislocate. Open reduction was performed, the goal of which was to reconstitute the hamate buttress and dorsal carpometacarpal ligament. All type III injuries require open reduction and internal fixation to reconstitute a congruent articular surface.
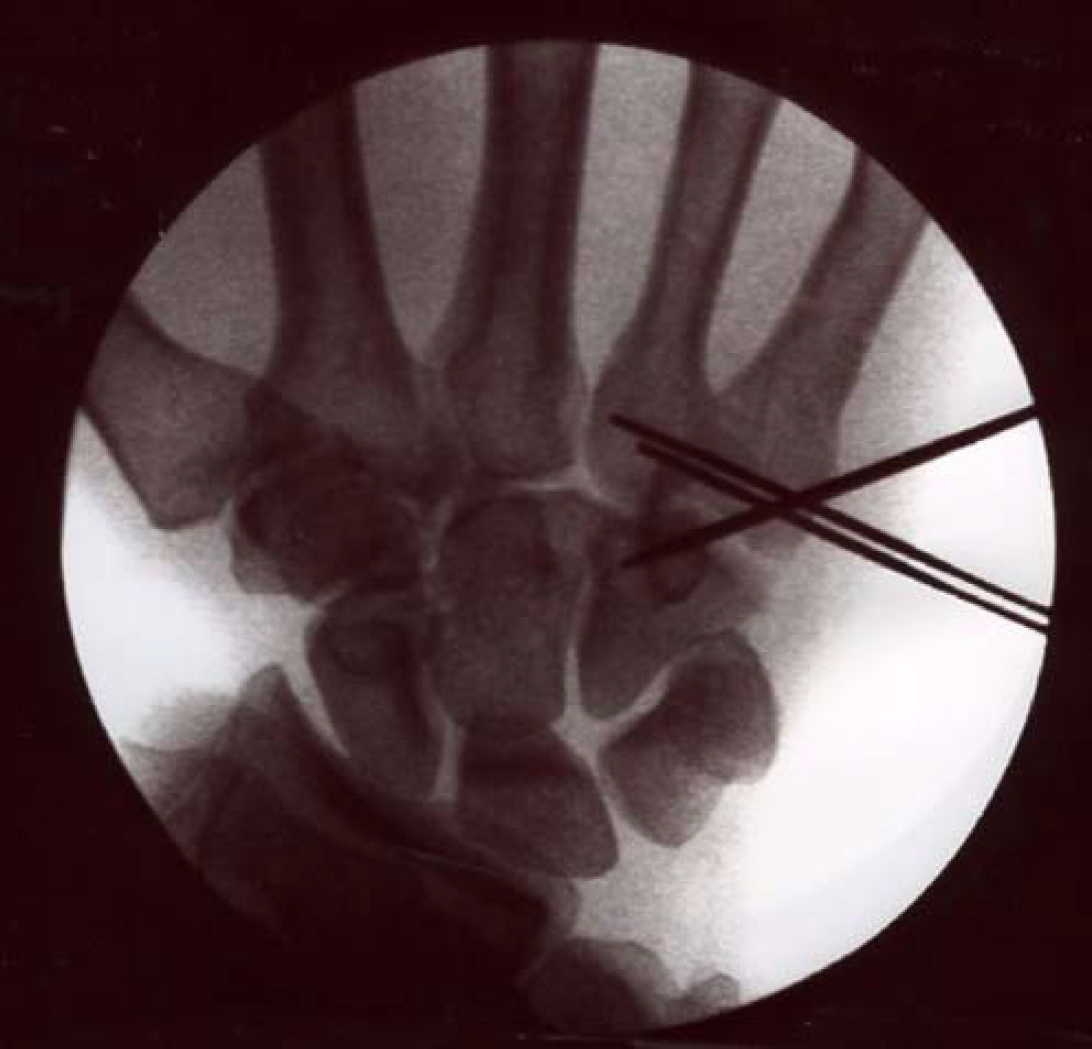
Posterior–anterior fluoroscopy image showing the K-wire from the base of the fifth metacarpal to hamate and transmetacarpal wire.
In terms of outcomes, there are few studies that evaluate the long-term effects of these injuries and their management. Lawlis et al. investigated the outcome status of 20 patients with carpometacarpal dislocations that were followed-up for an average of 6.5 years [5]. Of the 20 patients, 15 were treated with open reduction and internal fixation within 3 weeks of injury with excellent long-term results in 13 of 15. Three of the four unsatisfactory results involved injuries to the second and third carpometacarpal joints or had a concomitant ulnar nerve injury.
Authors' Perspective
It was our initial perspective that the patients in our case series experienced ulnar deep motor symptoms from iatrogenic injury from management of their CMC fx–dislocs by CRPP. All patients had EMG/NCS consistent with ulnar deep motor symptoms and all had resolution of their symptoms after pin removal. It was postulated that perhaps inadvertent penetration of the volar cortex of the hamate during multiple passes of the K-wire could potentially injure the nerve. Our cadaver studies demonstrated the extreme proximity of the ulnar deep motor branch to the volar cortex of the hamate. We suggest an alternative trajectory for percutaneous pinning. Instead of aiming toward the base of the hook of the hamate, by starting at a more midaxial position on the fifth metacarpal base, one should be able to direct the pin into the midbody of the hamate. By doing so, we can perhaps eliminate the potential for penetration of the volar cortex. As long as the volar cortex is not violated, the deep motor branch is protected. A patient was treated with this new technique and the x-ray images demonstrating the new trajectory is shown in Figs. 3 and 4.
Weaknesses in our study include a small sample size of cadavers and patients. In addition, it can be postulated that in live specimens, perhaps the relationship between the hook of the hamate and the ulnar deep motor branch is not as close as appreciated as tissue turgor and fullness are altered between live tissue and cadaveric specimens. MRI comparison did show a slightly greater distance between the deep motor branch and the hamate when compared to our cadaver dissections. Further studies are needed to elucidate the exact course of the deep motor branch and to accurately determine its true relationship to the hook of the hamate.
Conclusions
We believe that penetration of the volar cortex of the hamate poses a risk for iatrogenic injury to the ulnar deep motor branch. Although our study is limited by size, we do believe that we can eliminate iatrogenic injury to the ulnar deep motor branch by avoiding penetration of the volar cortex of the hamate during CRPP of the fifth CMC fx–dislocs. We plan to continue to treat our patients using this new trajectory and perhaps establish a case series that can demonstrate the benefits of this new trajectory.