
Abstract
A hand blast injury case causing a large through-and-through composite tissue loss is presented. This injury resulted in a dorsal and a palmar hand defect with segmental bone loss. Soft tissue coverage of both dorsal and palmar wounds was achieved by two separate pedicle flaps with pedicles closely arising from the femoral artery: a superficial inferior epigastric artery (SIEA) flap and a groin flap. Simultaneously, a large iliac corticocancellous bone graft was harvested from the same incision to be used for the wrist fusion procedure. This approach uses two separate pedicled flaps with robust independent blood supply to cover simultaneously a dorsal and a volar hand wound. A large through-and-through hand defect can be reconstructed readily with this approach, and it is associated with much less perioperative morbidity compared to free composite tissue transfer options. The dissection of both the groin flap and the SIEA flap is straightforward and can be easily performed by a single surgeon. The combined use of these two flaps allows stable coverage of sizable dorsal and palmar wounds of the hand.
A through-and-through defect of the hand is a difficult reconstructive problem. It often requires complex reconstruction of bone, tendon, nerve, and vascular injury within the hand. Subsequently, each wound needs to be reconstructed individually to protect the functional repair within.
We present a case featuring large palmar and dorsal hand defects with a concomitant segmental bony loss and wrist instability following a close-range gunshot wound. This problem was successfully reconstructed using two separate pedicled flaps, superficial inferior epigastric artery (SIEA) and superficial circumflex iliac artery (SCIA), and a simultaneous iliac crest corticocancellous bone graft for the wrist fusion procedure.
Case Report
A 24-year-old right-hand-dominant male sustained a shotgun wound to his left hand when the hand was resting over the muzzle of a shotgun. Initial examination showed a 2-cm diameter entry wound on the palm and a 6-cm diameter exit wound on the dorsum of the left hand (Fig. 1). Vascular examination showed that perfusion was intact to the thumb and all fingers. He had loss of sensation to the ulnar thumb and the entire index finger. He had no wrist extension, thumb extension, and flexion and extension of the index finger. X-ray showed destruction of the proximal index and long metacarpals and comminuted fractures of the trapezium, trapezoid, capitate, and distal scaphoid (Fig. 2).
He underwent immediate exploration, radical debridement of the wrist and hand, open carpal tunnel release, and the placement of an external fixator. The distal carpal row was destroyed with fragmentation of the scaphoid. After the debridement, a portion of the hamate, triquetrum, and lunate remained. The thumb metacarpal base was freefloating due to destruction of trapezium and scaphoid. The bases of the index and long metacarpals were fractured with avulsion of extensor carpi radialis longus and extensor carpi radialis brevis from their respective insertions. Both superficialis and profundus flexor tendons to the index finger were ruptured. The thumb and index finger digital nerves were avulsed from the median nerve.
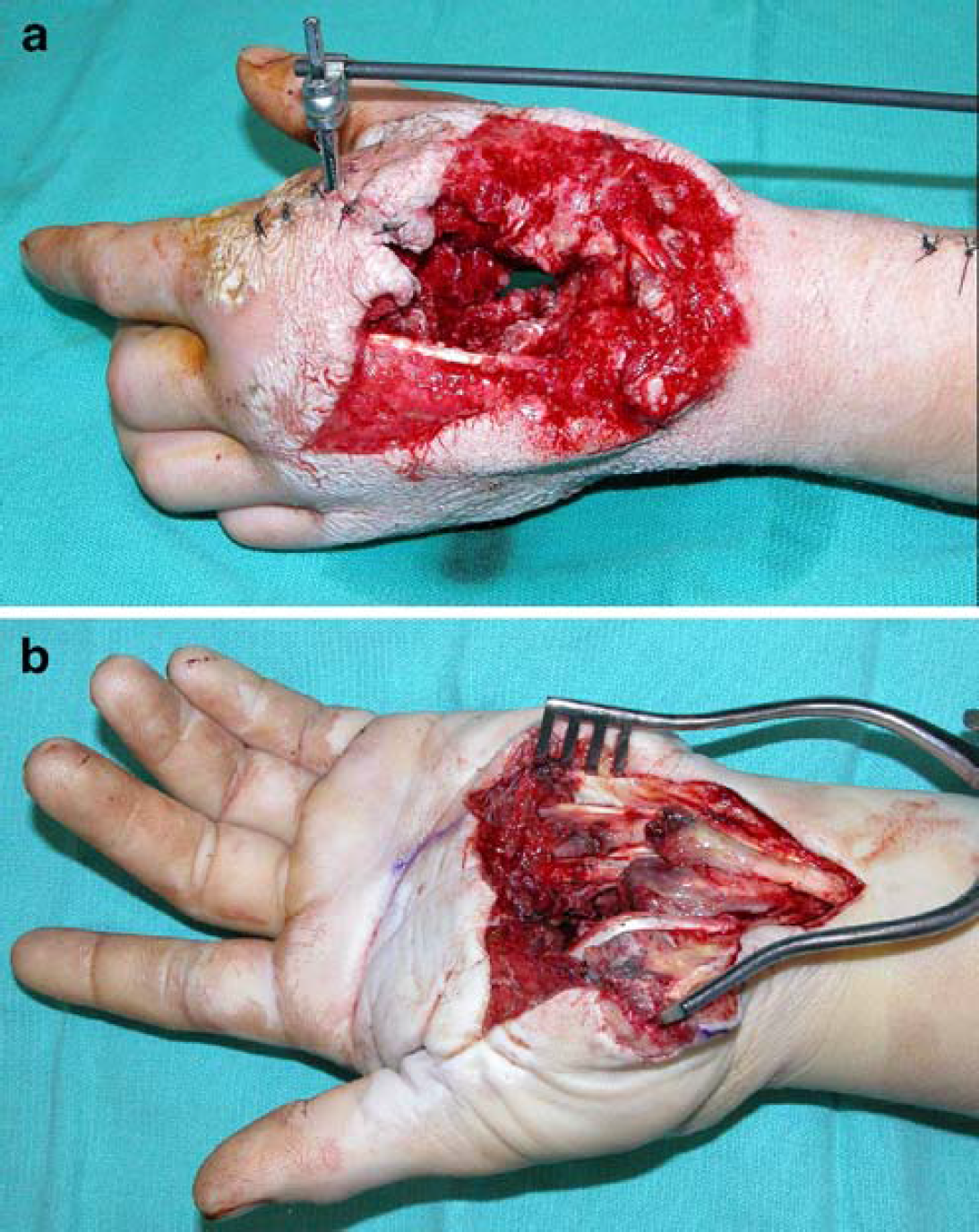
Preoperative examination showing a 2-cm-wide volar entry wound (
After serial debridements, he underwent a total wrist fusion using a 5×5-cm corticocancellous bone graft from the left iliac crest. The flexor digitorum superficialis of the middle finger was transferred to the flexor digitorum profundus of the index finger. The thumb was stabilized by pinning its metacarpal to the bone graft to allow fibrous nonunion. The soft tissue problems include a dorsal wound with exposed hardware and the bone graft and the volar wound with multiple exposed tendons.
For the simultaneous coverage of both dorsal and palmar hand defects, we designed two separate pedicle flaps: left groin flap and SIEA flap. Intraoperative Doppler exam showed the origin of the SCIA for the groin flap arising from the common femoral artery just below the inguinal ligament. The SIEA arose from the common trunk with the SCIA (Fig. 3).
The groin flap was dissected first by incorporating the bone graft harvest incision. The flap was lifted from the underlying fascia using the electrocautery from lateral to medial direction. At the level of the anterior superior iliac spine, blunt dissection under the sartorius fascia identified and preserved the lateral femoral cutaneous nerve. The SCIA was lifted with the sartorius fascia by dissecting the flap medially towards its origin.
The SIEA flap was then dissected from superior to inferior direction. After the skin incision, the dissection was carried down to the external oblique fascia. After gentle retraction of the flap using skin hooks, the dissection was carried inferiorly towards the pedicle. A slight back cut was made medially to allow for better lateral rotation and length.
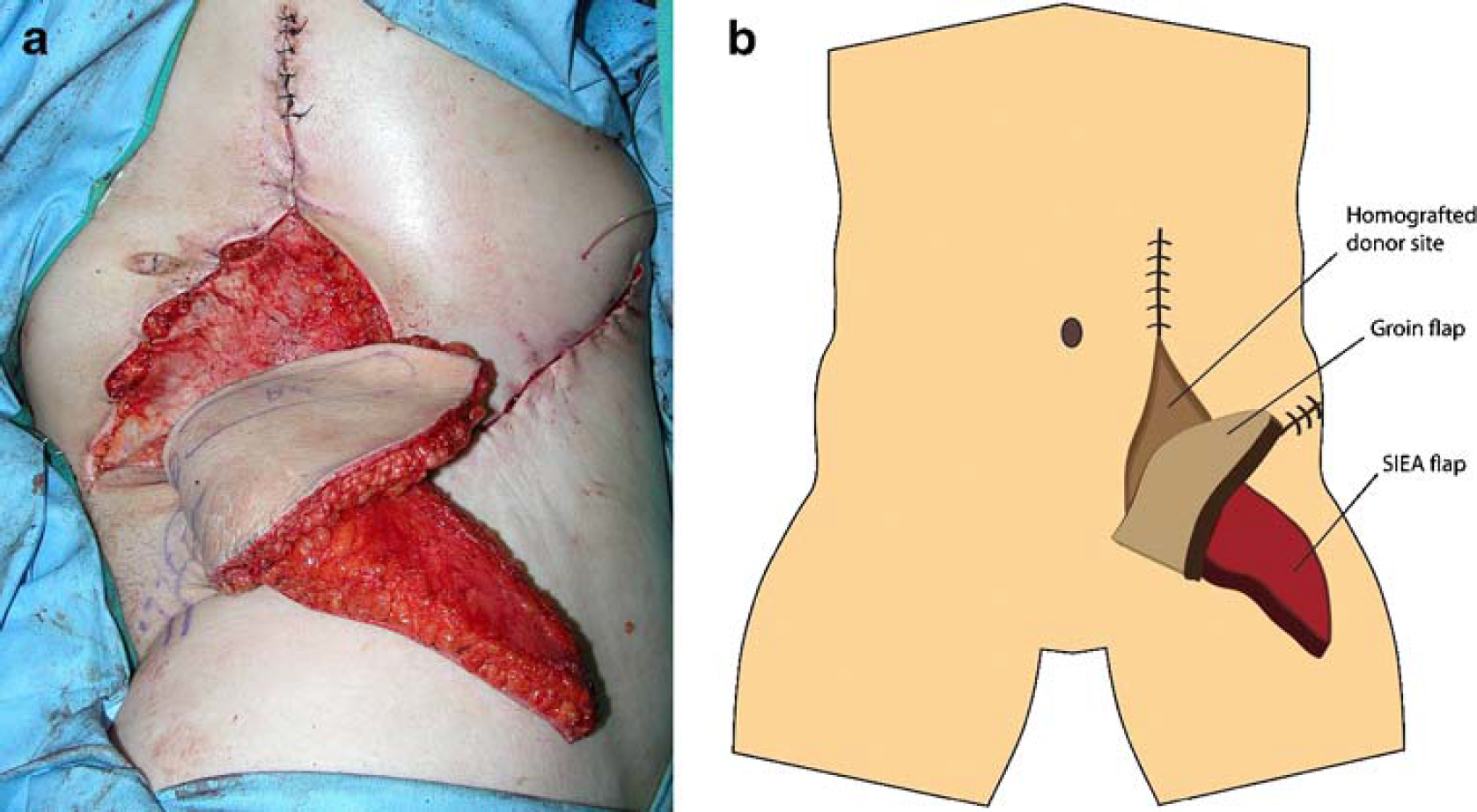
The palm of the left hand was placed on top of the overturned SIEA flap, and the SIEA was sutured onto the volar hand defect. The groin flap was then reflected back laterally to cover the dorsal defect (Fig. 4). The exposed undersurfaces of both flaps and donor sites were covered with homograft to prevent tissue desiccation and minimize drainage (Figs. 4 and 5), and the donor sites were closed primarily. His postoperative course was uneventful, and he was discharged home on postoperative day 5. Three weeks later, the flaps were divided. All the homografts were removed, and the remaining flaps after the division were returned to cover their respective donor sites.
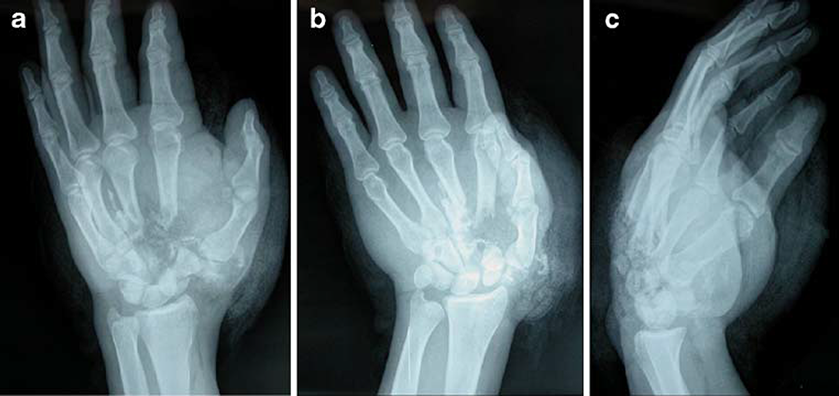
Preoperative x-ray showing destruction of the proximal third of index and long metacarpals and comminuted fractures of trapezium, trapezoid, capitate, and distal scaphoid.
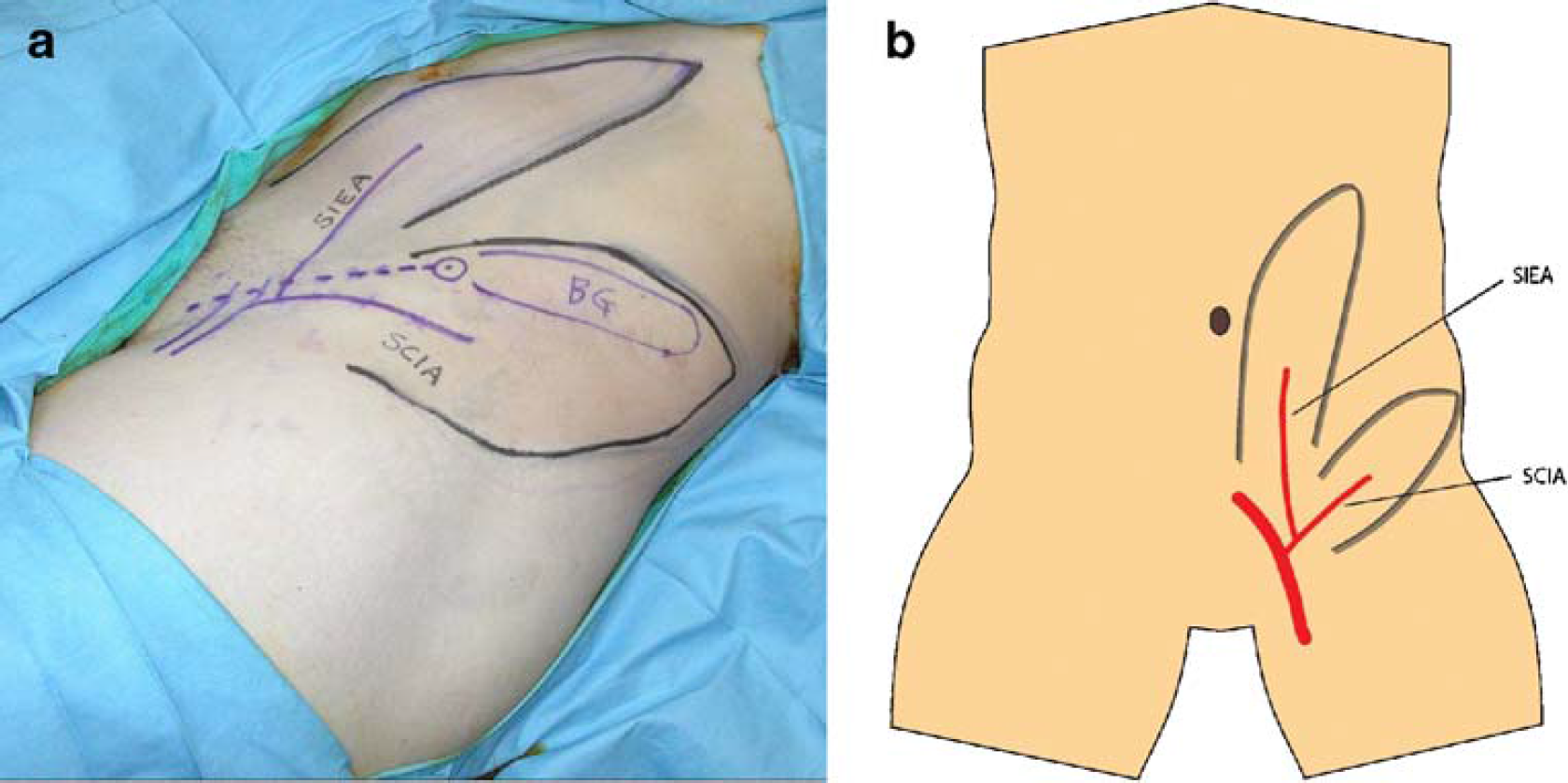
Markings of both groin and SIEA flaps with respective vascular pedicles: SCIA and SIEA. Note the bone graft harvest site at the superiolateral margin of the groin flap.
He had reasonable function of his hand after surgery and declined additional reconstructions (Fig. 6). The donor site scar is hypertrophic and immature at this time, but is not a concern for this patient (Fig. 7).
Postoperative hand function testing shows the following measurements at 3 months. The grip strength measurements showed 133 lbs on the right versus 11 lbs on the left, which continues to improve. From the sensibility standpoint, he continued to show absent sensation over his left index finger and the radial half of the middle finger. Total active arcs of motion were 103° for the index finger, 153° for the middle, 226° for the ring, and 254° for the small finger when metacarpophalangeal (MCP), proximal interphalangeal, and distal interphalangeal joint motion were added together for each finger. MCP joints showed 55°, 72°, 84°, and 93° of active flexion for the respective fingers. The Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) or the Michigan Hand Outcomes Questionnaire (MHQ) scores were not obtained because he was not a part of an outcomes study.
Orientation of the groin flap and the SIEA flap before insetting.
Discussion
High energy penetrating injuries through the hand still continue to challenge us, as they often create a large through-and-through defect and damage multiple tissues. After a series of debridement procedures, the surgeon needs to provide skeletal fixation and stable coverage. Form, function, and safety of each reconstructive option should be carefully considered and weighed against each other before the most suitable reconstructive plan can be selected. Furthermore, each reconstructive plan should be tailored to the individual patient based on the history, examination, and patient preference [9].

First stage reconstruction with combined use of the groin flap and the SIEA flap.
This patient is a young, healthy non-smoker who required coverage of both dorsal and palmar hand wounds. He was uninsured and unemployed at the time of injury, but he had worked as a manual laborer occasionally. He expressed a concern about the cost of the reconstruction as well as the possibility of potential complications from extensive operations. He also wanted to avoid a prolonged rehabilitation and considered wrist strength and stability more important than mobility for his line of work.
Preoperative discussion with the patient presented the free versus pedicled flap options in the requirement to cover two large wounds on both sides of his hand. The patient opted for a shorter and simpler operation. We proposed two pedicled flaps based on a single vascular axis, a groin flap and an SIEA flap, to cover each wound separately. We also considered feasibility of limited arthrodesis to preserve motion, but the patient favored strength and stability over the wrist mobility. Therefore, we also planned to obtain a large piece of iliac crest bone graft for the wrist fusion through the groin flap incision.
The groin flap is commonly used to cover large dorsal hand wounds, and, if feasible, it can be designed as a double-leaf (Y) pattern or other shapes to fit specific defects [11, 12]. Due to the relatively large defects in this patient, we opted for two separate pedicled flaps to cover each defect separately. Others have described using separate flaps from the groin area for coverage of separate hand defects. Koncilia et al. [8] described the combined use of a groin flap and a pedicled Scarpa's flap (SIEA) for circumferential finger burn defects. Watson and McGregor [14] used a groin flap and a tensor fascia lata myocutaneous flap to cover a completely degloved hand.
The dissection of the groin flap and the SIEA flap is relatively easy and straightforward, allowing a single surgeon to retract and cut the flaps with no need for an assistant. By using two separate flaps, each flap can be contoured specifically for the corresponding defect. Furthermore, the two separate pedicles provide excellent perfusion to the underlying tissues to support the large non-vascularized iliac bone graft used for the wrist fusion in this case.
There is a caveat to the use of an SIEA flap, however. Its pedicle of the superficial inferior epigastric artery may be absent. Taylor and Daniel [13] in 1975 reported in their dissection of 100 cadavers and found absence of SIEA in 35% of dissections. A more recent anatomic study by Reardon et al. [10] in 2004 showed that the SIEA was consistently found in 20 out of 22 cadavers. Therefore, pre- and intraoperative Doppler examination is required to confirm the presence and location of the SIEA.
Morbidity of the pedicled groin flap has been studied, and through 30 consecutive patients, Graf and Biemer [5] showed that the restriction in the shoulder mobility appears to be the most aggravating complication. The risk of postoperative shoulder stiffness increased with the age of the patient. Young patients are less likely to suffer from postoperative shoulder stiffness, and no one less than 50 years of age had any permanent stiffness in shoulder mobility after groin flap transfer in this study.

Left hand at 3 months.
Our patient in this case had full recovery of shoulder mobility almost immediately after the flap division without a need for formal physical therapy. Another advantage of this approach is minimal donor site morbidity. Both flap harvest sites were primarily closed with no need for skin grafting. The donor site scars seen in Fig. 8 are hypertrophic, but still immature at 3 months postoperatively. It is important to note that no skin grafting was required to close the defect. Donor site skin grafting causes significant morbidity in many otherwise excellent pedicled or free fasciocutaneous flap transfer techniques by disrupting the natural texture, color, and contour of the donor site. The groin flap donor site also provided a full access to the iliac crest for the bone graft harvest without creating another scar. Short operative time is another advantage. Dissection and elevation of both flaps was quick and easy, and the secondary division and insetting procedures were done in a short outpatient procedure.
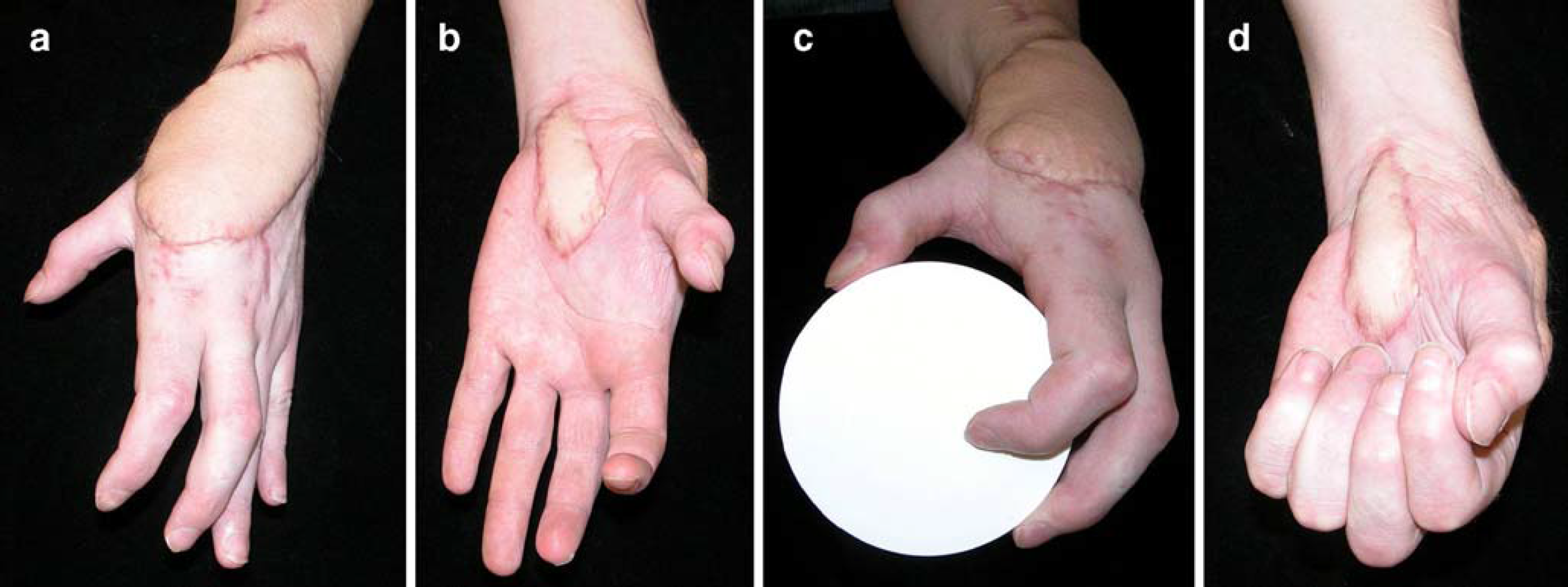
Hand function at 3 months.

The donor site scars are immature at 3 months postoperatively.
The use of a fillet flap along with its phalanges is another reconstructive option utilizing the spare part concept to reconstruct both bone and soft tissue defect in the hand either as a pedicled or free tissue transfer. The index finger fillet flap would have been a potential option in this case, as its sensibility and motor function was loss by the injury. However, in a high energy injury such as this case, we opted to recruit the tissue from well beyond the zone of injury. Furthermore, our assessment of the wound suggested that we needed a large (5×5 cm) bone graft and a large, stable soft tissue cover for both dorsal and volar wounds. Therefore, the fillet flap was not chosen for this case.
Free tissue transfer is another option for coverage of hand wounds, and many thin flaps have been reported. Notable ones include a free temporoparietal fascial flap [2, 3, 7] and a dorsalis pedis free fasciocutaneous flap [1, 4]. These flaps are thin and can provide excellent contour to hand wounds. The temporoparietal fascial flap, if endoscopically harvested, can also have excellent donor site appearance with minimal alopecia and scars [3]. However, there is a steep learning curve to harvest the flap endoscopically. The dorsalis pedis artery is quite a versatile axis because it can support multiple island flaps as a conjoint or chimeric flap on a single pedicle [6]. Substantial donor site morbidity is a big disadvantage of this flap because the foot does not have sufficient donor soft tissue. The subscapular system is another versatile pedicle for free tissue transfer because it can support the scapular flap, parascapular flap, latissimus dorsi flap, serratus anterior flap, and rib in different combinations. Although the free tissue transfer can provide excellent coverage for hand wounds, the long operative time with increased risks of perioperative morbidity as well as the need for special equipments and well-trained surgical teams makes it unattractive and difficult in many centers.
This case illustrated the use of the combined SIEA and groin flap for effective reconstruction of both dorsal and volar defects of the hand. This approach is straightforward, quick, and easily performed by a single surgeon with no need for assistants or specially trained teams of support personnel who are required for successful free flap reconstruction. Furthermore, it also provides an exposure for a large source of autologous bone graft if composite tissue reconstruction is needed at the same time.
Footnotes
Acknowledgment
The study was supported in part by a Midcareer Investigator Award in Patient-Oriented Research (K24 AR053120) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (to Dr. Kevin C. Chung).