
Abstract
The Darrach and Sauvé-Kapandji procedures are considered to be useful treatment options for distal radioulnar joint disorders. Postoperative instability of the proximal ulnar stump and radioulnar convergence, however, may cause further symptoms. From October 1999 to May 2002, a total of 19 wrists in 15 men and four women, with an average age of 48.3 years, were treated by stabilizing the proximal ulnar stump with a half-slip of the extensor carpi ulnaris tendon using modified Darrach and Sauvé-Kapandji procedures. The average follow-up period was 77 months (range, 62 to 91 months). No patient complained of symptoms due to instability of the proximal ulnar stump. Grip strength improved in all wrists after surgery. Postoperative X-rays, including loading X-rays, showed improved alignment in both coronal and lateral planes. We concluded that stabilization of the proximal ulnar stump with ECU tenodesis is an effective procedure for treating distal radioulnar joint disorder after the Darrach and Sauvé-Kapandji procedures.
Keywords
Introduction
Several procedures that have been proposed to manage distal radioulnar joint (DRUJ) disorders include the Darrach procedure, the Sauvé-Kapandji (S-K) procedure, hemiresection interposition arthroplasty (Bowers procedure), and matched distal ulna resection [3, 8, 16]. Although satisfactory clinical results were obtained in most reports [5, 8, 13, 14], instability of the proximal ulnar stump and radioulnar convergence resulting in pain over the ulnar stump have been noted [5, 8, 13, 14]. Minami et al. [12] developed a modified S-K procedure to treat osteoarthritis (OA) of the DRUJ; long-term follow-up was reported to have satisfactory functional outcome. The purpose of the study is to retrospectively review the clinical outcome of our study population having undergone such modified procedures. We report the results of a 5-year follow-up study of patients who underwent modified Darrach and Sauvé-Kapandji procedures with partial extensor carpi ulnaris tendon and new method of tenodesis to treat chronic derangement of the DRUJ.
Materials and Methods
From October 1999 to May 2002, a total of 19 wrists in 15 men and four women with chronic derangement of the DRUJ underwent either a modification of the Sauvé-Kapandji procedure or the Darrach procedure (S-K: 12; Darrach: seven) involving stabilizing the proximal ulnar stump with a half-slip of the extensor carpi ulnaris tendon. The average age of the patients was 48.3 years (range, 12 to 71 years). The patients complained of painful disabilities involving the wrist that hampered their daily activities, limitation of motion, and weakness of grip strength.
Primary osteoarthritis of the DRUJ was diagnosed in ten wrists. Secondary osteoarthritis due to distal radial fracture malunions was diagnosed in seven wrists. Congenital madelung syndrome was diagnosed in one wrist, and a giant cell tumor of the distal ulna was diagnosed in one wrist. The average follow-up was 77 months (range, 62 to 91 months). The pre- and postoperative wrist assessments were based on both subjective and objective criteria, including wrist pain, range of motion, grip strength, work status, and radiographic evaluations.
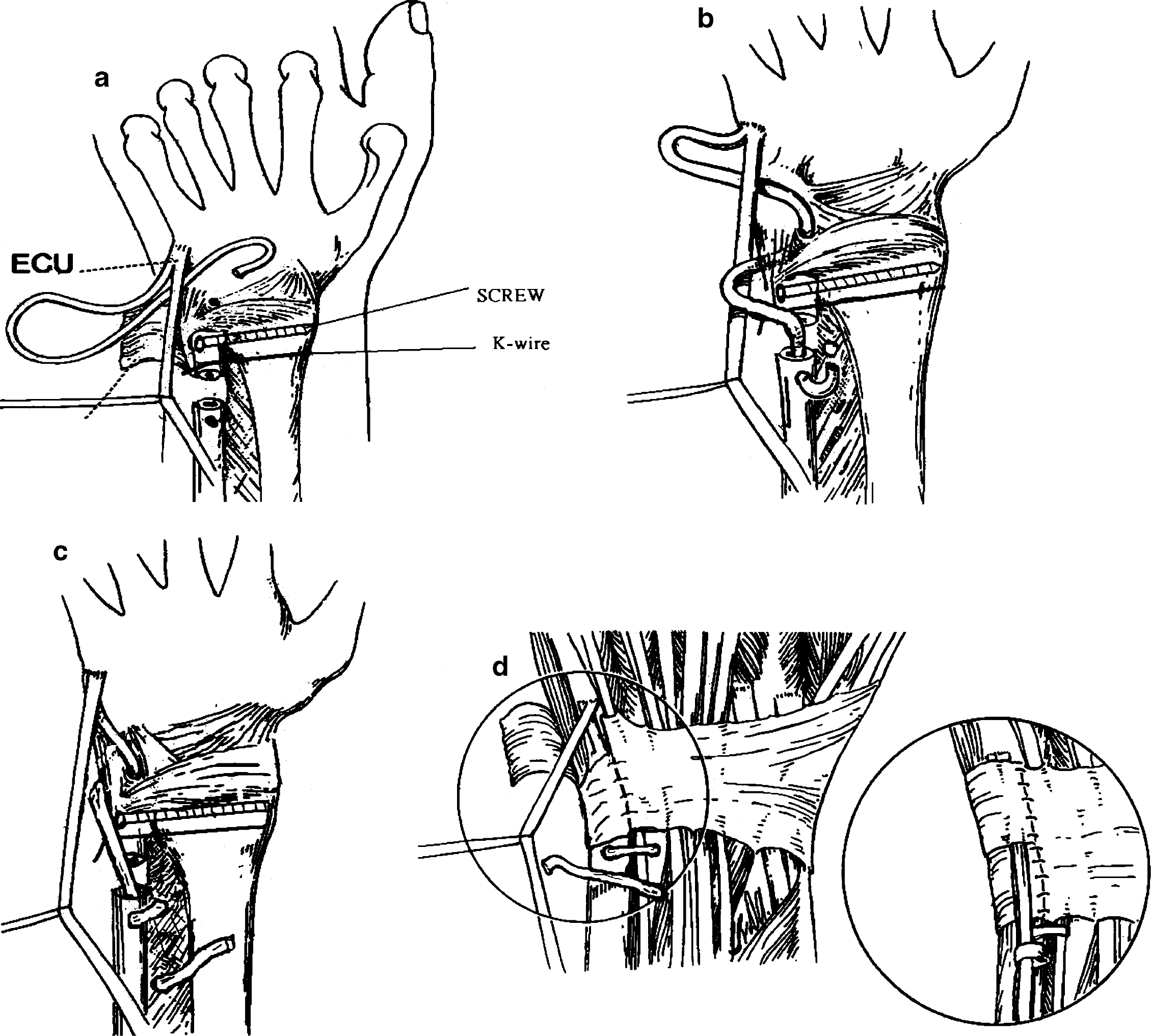
A drill hole is made in the dorsal cortex of the ulnar stump; a distally based slip of the ECU tendon was then created by longitudinal division.
Wrist pain was assessed based on patients' responses to a questionnaire. Wrist pain was graded as non-existent, mild (not impeding activity), moderate (impeding activity), or severe. All patients were specifically asked whether they were experiencing pain over the ulnar stump region or a sensation of movement of the ulnar stump. Work status was graded as regular work, restricted work, able to work but jobless, or unable to work owing to pain. The following ranges of wrist motion was recorded: flexion, extension, pronation, and supination. Additionally, wrist ranges of motion and grip strength (Jamar dynamometer setting III) were measured and reported in percentage using the uninvolved hand as a comparison.
Pre- and postoperative X-ray films were available for all patients. Ulna convergent instability was also checked radiologically [10]. The wrist is stress-loaded by asking the patient to hold a 5-lb lead cylinder with the shoulder adducted, the elbow flexed to 90°, and the forearm in the position of neutral rotation. The radiograph is then taken with the beam aligned in the coronal plane with respect to the anatomical position. During the maneuver, the patient is asked whether or not the action of lifting the weight recreates the pain. The patient's response is then correlated with the appearance of the radiograph.
Individual patient data.
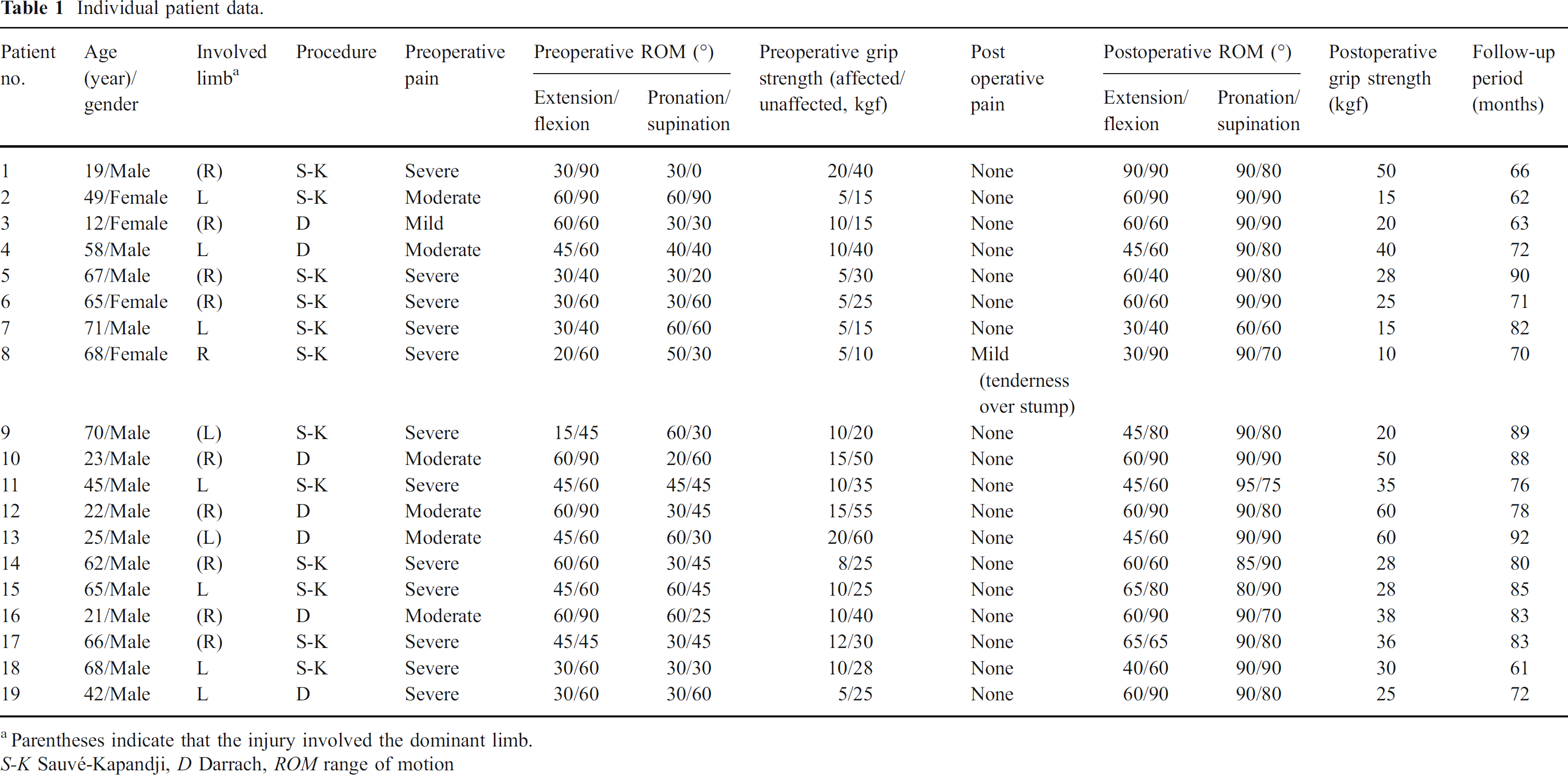
Parentheses indicate that the injury involved the dominant limb.
S-K Sauvé-Kapandji, D Darrach, ROM range of motion

Postoperative X-ray film of a 45-year-old man with fracture.
Surgical Technique
After the standard S-K and Darrach procedures had been completed (S-K:12 wrists; D: seven wrists), a 3.5-mm drill hole was made in the dorsal cortex of the distal ulnar stump, 0.5 cm proximal to the osteotomy. A distally based slip of ECU tendon, 10 cm in length, was then created by splitting the tendon longitudinally (Fig. 1a). This strip was first passed through the ulnar collateral ligament and triangular fibrocartilage complex in a dorsal palmar direction and then passed through the distal ulnar medullary canal (Fig. 1b), exiting through the dorsal hole and then the interosseous membrane (Fig. 1c). The ECU was tightened and sutured to adjacent tissue, and the forearm was supinated to relocate the proximal ulnar stump to prevent dorsal subluxation. The distal ulna was covered with the joint capsule in a periosteal flap. The remaining ECU strip was placed in a dorsoulnar position, and the extensor retinaculum was used to stabilize the tendon over the dorsal aspect of the distal ulna (Fig. 1d).
Postoperative Management
Postoperatively, the wrist was held in a supinated position in a long arm splint for 3 weeks, then in a short arm splint for a further 3 weeks. Full range of motion of the wrist and forearm was started at 6-week follow-up.
Statistical Analysis
Data were analyzed using the Wilcoxon signed-rank test and the Friedman test. Statistical significance was defined as a p value less than or equal to 0.01.
Results
Follow-up data from an average of 77 months (range, 62–91 months) were obtained for all wrists (Table 1).
Pain
Wrist and ulna stump pain were evaluated at the most recent follow-up examination for each patient. None of the patients complained of pain, and all of the stumps were stable.
Range of Motion
Table 1 lists the preoperative average range of wrist motion in all patients. The preoperative range of motion of the affected wrist averaged 42.1° extension and 64.2° flexion. After surgery, the average range of motion improved to 54.7° extension and 71.3° flexion. Forearm motion averaged 41.3° pronation and 41.6° supination preoperatively. Forearm motion averaged 87.9° pronation and 81.8° supination postoperatively at last follow-up. Pronation/supination and extension significantly improved in all patients (p<0.01). Flexion did not significantly improve (p=0.041).
Grip Strength
The mean grip strength, measured with a Jamar dynamometer (Therapeutic Equipment. Clifton, NJ, USA), averaged 10 kgf (32.6% of the contralateral side) preoperatively. After surgery, the average grip strength increased to an average of 32.3 kgf. Grip strength improved significantly in all patients (p<0.01).
Return to Work
After an average of 77 months follow-up, 18 patients returned to their previous work status before surgery. One patient returned to light work but had no difficulty with functions of daily living.
Radiographic Evaluations
Pre- and postoperative X-ray films were checked in all wrists. No ulnar stump instability of the dorsal side was present in the lateral view, either without a weight or while gripping a 5-lb weight (Fig. 2a and b). Good range of motion of the wrist and forearm and no radiographic evidence of impingement between the ulnar stump and the radius were seen.
Postoperative Complication
There were no infections or immediate complications recorded in any of the patients who received the procedure.
Discussion
Dysfunction of the DRUJ is commonly encountered by patients with primary or secondary osteoarthritis following malunion of distal radius fracture. Both the Darrach procedure and the Sauvé-Kapandji procedure are reliable and effective methods of treating distal radioulnar joint disorders [5, 7, 8, 11–14]. The Darrach procedure is considered to be the traditional approach to excising the arthritic surface of the DRUJ. There are several variations of the Darrach procedure, some of which call for the complete excision of the distal ulna. Other variations call for a limited excision, leaving a partial interposition of the connective soft tissues to the remaining distal ulna. The Sauvé-Kapandji procedure involves the resection of several centimeters of ulnar bone mass proximal to the DRUJ; however, the ulnar head itself remains intact. The ulnar head is then fused to the distal radius. The presence of the distal ulnar stabilizes the joint.
However, complications following the Darrach's procedure and the Sauvé-Kapandji procedure have been described, such as instability of the distal ulna, abutment of the distal radius against the ulna, and attrition rupture of the ulnar extensor tendons [5, 7, 8, 13, 14]; these complications can result in pain at the ulnar stump. The mechanism of ulnar stump instability may involve actions of the pronator quadratus, pronator teres, extensor pollicis brevis, and abductor pollicis longus, as well as the effect of the interosseous membrane [1, 2]. Following the Sauvé-Kapandji procedure, the ulnar shaft is stabilized using the interosseous membrane, which provides some static stabilization, as well as the extensor carpi ulnaris and flexor carpi ulnaris tendons and a portion of the pronator quadratus, which provide dynamic stabilization [6] The relative importance of the various soft-tissue and osseous constrains that maintain the stability of the distal radioulnar joint remains controversial, although most authors have agreed that the dorsal and volar radioulnar ligaments at the periphery of the triangular fibrocartilage complex provide the primary constrains to the distal radioulnar joint. After the Darrach's procedure and the Sauvé-Kapandji procedure, the remaining structures that stabilize the ulnar shaft are the interosseous membrane, which provides some static stabilization, as well as the extensor carpi ulnaris and flexor carpi ulnaris tendons and a portion of the pronator quadratus, which provide dynamic stabilization. This study shows that ECU tenodesis in which the ulnar stump is tethered to the carpus provides static and dynamic stabilization.
Minami et al. [12] developed a modification of the S-K procedure to use in the treatment of OA of the DRUJ; they reported that the procedure had a satisfactory functional outcome at an average of 95 months of follow-up. In our 5-year follow-up of patients that were treated with either the modified Darrach or Sauvé-Kapandji procedures, postoperative pain relief was good in all wrists. Postoperative range of motion improved significantly in the flexion–extension arc and the pronation–supination arc. No radiographic evidence of impingement between the ulnar stump and the radius was noted.
Several procedures for stabilizing the distal radioulnar joint have been reported, such as tenodesis of the proximal ulnar stump using the extensor carpi ulnaris tendon, the flexor carpi ulnaris tendon, or both [4, 9, 12, 15]. Lamey and Fernandez [9] reported the technique of tenodesis of the flexor carpi ulnaris following the Sauvé-Kapandji procedure to stabilize the ulnar stump. All of the patients in their series exhibited postoperative dorsal instability of the ulnar stump. The authors believe that the operation is an excellent salvage procedure for the treatment of chronic posttraumatic derangement of the distal radioulnar joint. Breen and Jupiter [4] reported that combined tenodesis of the ECU and flexor carpi ulnaris was a reliable procedure for stabilizing the ulnar stump following resection of the distal ulna.
We used a slip of the ECU tendon as a dynamic tether to the proximal ulnar stump. In the present series, ECU tenodesis was used to control ulnar stump stability, and none of the patients exhibited postoperative volar or dorsal instability of the ulnar stump. The ECU is an important stabilizer of the ulnar head as it is constrained within the sixth dorsal compartment. Tendon constrain is lost after ulnar head resection or resection of the distal part of ulna shaft. Tenodesis reestablishes the constraint forces—dorsal displacement and radial convergence.
Our clinical results suggest that stabilization of the proximal ulnar stump with ECU tenodesis following either the Darrach or Sauvé-Kapandji procedures is a reliable method for preventing an unstable ulnar stump in patients with dysfunctional distal radioulnar joints.