
Abstract
We present a rare case of persistent complete posterior interosseous nerve palsy associated with a chronic type I Monteggia elbow fracture-dislocation consisting of anterior dislocation of the radial head and malunion of the ulna in an 8-year-old child requiring surgical treatment. Posterior interosseous nerve neuropraxia following acute Monteggia injury patterns about the elbow has been described and is thought to be secondary to traction or direct trauma. The condition typically resolves following successful closed reduction of the radial head. This report describes combined treatment of the nerve and skeletal injury for the chronic type I Monteggia injury. The literature is reviewed, and diagnostic challenges with and treatment options for chronic Monteggia fracture-dislocations in children are discussed.
Keywords
Introduction
Chronic complete posterior interosseous nerve (PIN) palsy is a recognized but uncommon sequela of the type I Monteggia elbow fracture-dislocation in children. This report describes combined radial nerve exploration with PIN neurolysis and surgical reconstruction of a chronic type I Monteggia injury in a child. PIN subluxation followed by chronic compression at the proximal radioulnar joint (PRUJ), radiocapitellar joint (RCJ), and arcade of Froshe may be suspected in this rare clinical scenario.
Case Report
An 8-year-old right-hand-dominant boy presented to our institution approximately 3 months after sustaining an injury to his left elbow following a fall on ice. His elbow injury was initially treated at another institution with cast immobilization for 6 weeks. Following cast removal, the mother complained of persistent deformity of the left elbow and weakness of the hand. Radiographic evaluation revealed evidence of a chronic type I Monteggia fracture-dislocation with persistent anterior dislocation of the radial head and malunion of the ulna (Fig. 1). Clinical examination was consistent with a complete posterior interosseous nerve palsy. Digital and thumb extensions were graded 1/5, and there were no palpable contractions of the extensor carpi radialis brevis or extensor carpi ulnaris. Sensory examination in the radial nerve distribution was unremarkable. Electrodiagnostic studies confirmed a left PIN neuropathy. Motor nerve conduction studies failed to record compound muscle action potentials in the left radial nerve forearm–elbow segment, and electromyography of PIN-innervated muscles demonstrated membrane instability and no motor units. Sensory nerve action potentials of the left radial nerve revealed normal amplitudes and conduction velocities. A physical therapy program was initiated, and the patient was followed at monthly intervals. Repeat clinical and electrodiagnostic evaluations at 3 months following the initial study revealed no interval change.
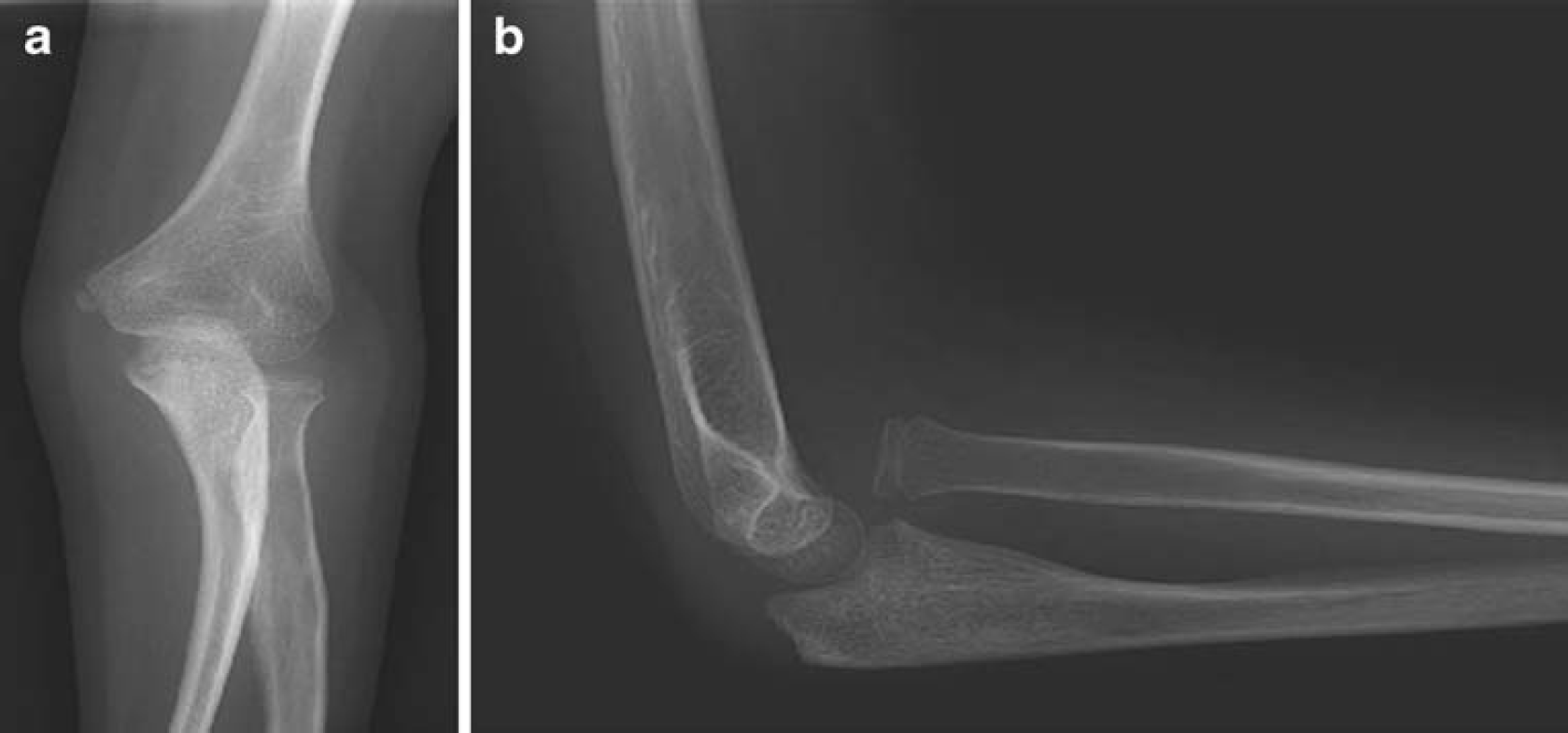
Preoperative anteroposterior (
At 9 months following the original injury, the patient underwent exploration of the left PIN and reconstruction of the chronic Monteggia fracture-dislocation. An anterolateral approach was utilized. The radial nerve was first identified between the brachialis and brachioradialis at its emergence from the lateral intermuscular septum. Distally, the bifurcation was identified, and the PIN was explored to the level of the arcade of Froshe. The radial head was found anteriorly dislocated between the superficial radial nerve and PIN. The PIN was subluxed posterior to the radial head and encased in thick scar adherent to the capsules of the proximal radioulnar and radiocapitellar joints (Fig. 2). Chronic compressive changes of the nerve and epineural fibrosis were visualized at these sites of capsular cicatrix and at the arcade of Froshe. Intraoperative neurophysiologic recordings were attempted, but given the time elapsed since the initial injury, recordable distal responses from the PIN-innervated muscles were not obtained, and the anatomy in this case did not allow studying the neuroma in continuity. A complete microsurgical neurolysis was performed (Fig. 2).
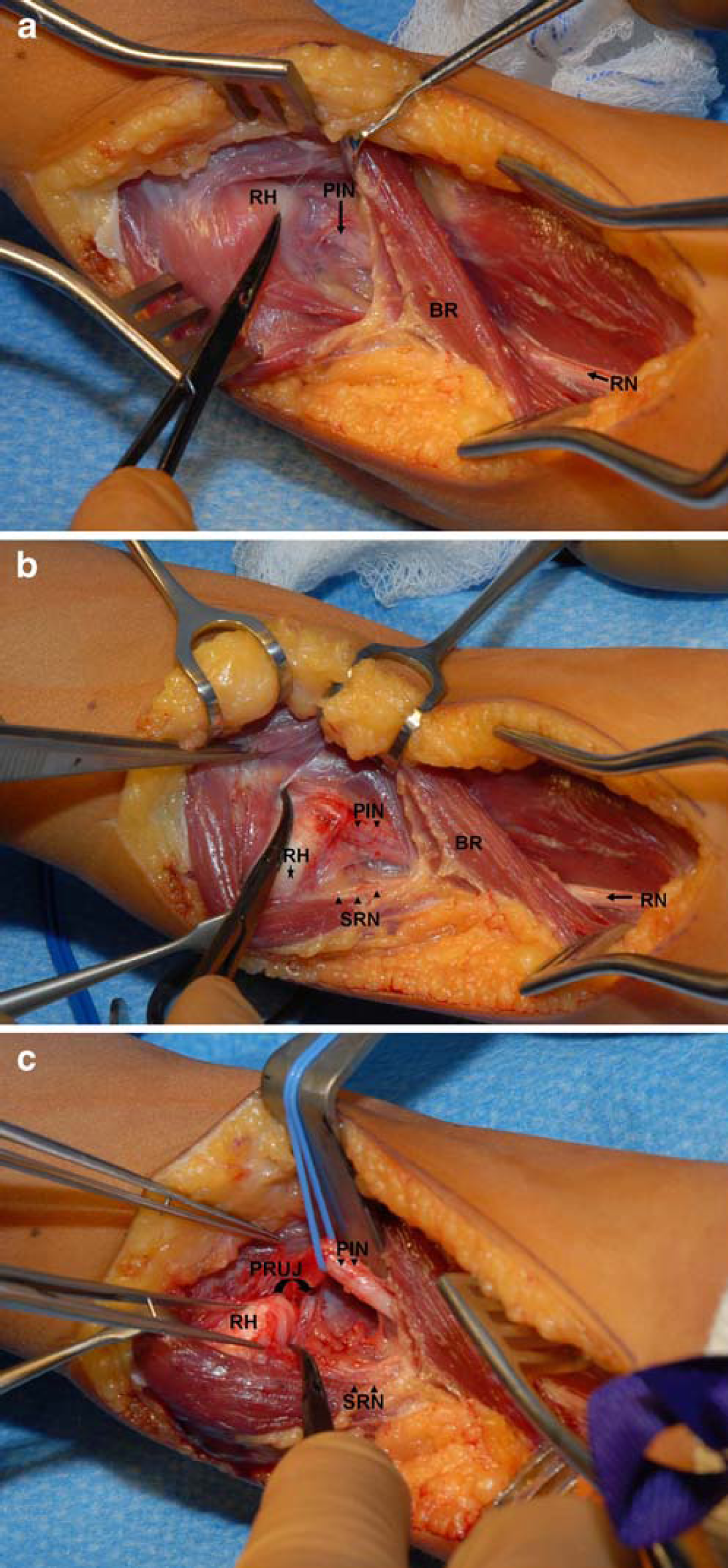
Intraoperative step-wise radial nerve exploration and neurolysis.
Next, the Kocher interval between the extensor carpi ulnaris and anconeus was utilized to expose the radiocapitellar joint. Reduction of the radiocapitellar joint was initially prevented by the interposed capsule, torn annular ligament, and scar tissue, and these soft tissues were resected. A corrective ulnar osteotomy was then performed in order to obtain anatomic reduction of the radial head. Annular ligament reconstruction was performed utilizing a proximally based strip of periosteum harvested from the proximal ulna. The annular ligament reconstruction was tensioned to allow for smooth pronation and supination without any dislocation of the radial head throughout a full range of motion. Transcapitellar fixation of the reduced radial head was performed with a 3/32″ smooth Steinman pin to maintain the radial head reduced against the capitellum and reduce stress on the soft tissue reconstruction. The lateral capsule was repaired and the incision closed in layers. A long arm cast with the forearm in full supination and the elbow maintained in 90° of flexion was applied. Electrical muscle stimulation to the wrist and extrinsic thumb and digital extensors was immediately initiated through a window in the cast. The postoperative course was uneventful.
Serial postoperative radiographs demonstrated maintenance of reduction of the radiocapitellar relationship, and at 6 weeks postoperatively the long arm cast and Steinman pin were removed. Radiographic evidence of delayed union was seen at 6 months postoperatively, and the patient underwent revision surgery with plate fixation. At 6 months following the revision surgery, radiographs revealed three cortices of osseous healing at the ulnar osteotomy site with maintenance of the radiocapitellar relationship (Fig. 3). The patient is currently pain free at the elbow, forearm, and wrist, and abundant callus is palpable along the subcutaneous border of the ulna. At 12 months following neurolysis of the radial nerve, the patient demonstrates excellent clinical evidence of return of function of the posterior interosseous nerve. There is full active wrist extension without deviation and full active digital metacarpal–phalangeal joint extension with mild residual weakness of the extensor pollicus longus and abductor pollicus longus (Medical Research Council [MRC] 4/5). Clinical examination further demonstrated full active ulnohumeral flexion and extension. Active forearm rotation consisted of full supination and 30° of pronation.

Progressive bridging callus following plate fixation is seen at the prior delayed union osteotomy site. The radiocapitellar relationship remains reduced at 12 months following open reduction of the radial head and annular ligament reconstruction on orthogonal anteroposterior (
Discussion
In 1814, Monteggia first described the association of radial head dislocation with a concomitant fracture of the ulna [
In the presented case, it is unclear if the radial head dislocation was appreciated and closed reduction achieved at the initial treating institution. Orthogonal radiographs obtained 3 months following the initial injury revealed chronic anterior dislocation of the radial head and malunion of the ulna. The high incidence of redislocation of the radial head after either spontaneous [
Operative treatment of Monteggia fracture-dislocations is necessary when closed reduction is unsuccessful in patients seen more than a month after the injury (i.e., chronic radial head dislocation). Chronic disruption of the PRUJ continues to represent a challenging clinical scenario for the pediatric upper extremity surgeon. Outcomes following surgical reconstruction of chronic pediatric Monteggia injuries vary [
Though limited to retrospective series with small cohort sizes, several groups have reported satisfactory clinical and radiographic outcomes following various combinations of annular ligament repair or reconstruction [
Acute [
Persistent, chronic PIN palsy in the setting of a chronically dislocated radial head is an exceedingly rare entity and is reported only twice in the literature [
Based on these reports [
Footnotes
Acknowledgement
Herbert Valencia, RN/CFA for production of figures.