
Abstract

American Association for Hand Surgery Concurrent Scientific Paper Session A-1
The Use of Pyrolytic Carbon for the Treatment of Complex Post Traumatic Arthritis and Acute Joint Loss in the MCP and CMC Joint
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Furkan Erol Karabekmez, MD; Ahmet Duymaz, MD; Steven L. Moran; Mayo Clinic
Introduction
Preservation of joint motion in cases of acute joint destruction and post-traumatic arthritis are challenging problems for surgeon. Previous options for preserving joint motion have included silicone and soft tissue interpositional arthroplasty. Pyrocarbon arthroplasty has been recently introduced as another option. We wished to examine our intermediate outcomes with the use of pyrocarbon complete and hemi-arthroplasty for the treatment of acute traumatic joint loss and post-traumatic arthritis.
Material and Method
From May 2003 to August 2007, 6 MCP and 3 CMC joint pyrolytic carbon metacarpophalangeal implants were inserted in 6 patients. Two patients underwent complete MCP arthroplasty, 3 patients underwent CMC hemiarthroplasty, and 1 patient underwent acute hemiarthroplasty of the small finger. Charts were reviewed for final range of motion (ROM), pinch and grip strength. Post-operative complications were noted. Hand radiographs were reviewed for signs of implant loosening, migration and subsidence. Visual analog scale (VAS) scores were used to assess postoperatively pain.
Results
All patients were male manual laborers with an average age 47 years. Follow-up averaged 36 months. None of the joints required removal. There were no cases of post-operative subsidence, loosening or implant facture. Pre-operative motion in the two patients with post-traumatic MP arthritis was 15 degrees, post-operative MP ROM was 65.8 degree and this change was found to be significant (p<0.05). Mean CMC radial abduction angle and palmar abduction angle were 38.3 and 40 degree respectively in CMC arthroplasty cases. There was no statistical difference in radial or palmar abduction angles of CMC joints pre and post-operatively and no significant difference was seen when compared to the contra lateral normal hands. Statistically significant improvement was found between grip strength of the CMC joints pre and postoperatively (p<0. 05). Average postoperative VAS (scale 1–10) was 0 in cases of MCP arthroplasty and 1 in cases of CMC arthroplasty. All patients returned to previous employment.
Conclusion
Pyrocarbon arthroplasty provides an excellent option for joint preservation in cases of acute and post traumatic arthritis of the MCP and CMC joint. Joint replacement provided pain relief while maintaining adequate ROM for post-operative activities. All patients returned to previous employment. Further study is required to assess long-term outcome.
Biomechanical Comparison of Three Fixation Techniques of Four Corner Arthrodesis: K wires vs Circular plate (Spider Plate) vs Locked Circular plate (Xpode Plate)
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Alexander Y. Shin, MD1; Jirachart Kraisarin, MD2; Lawrence J. Berglund, BS1; David G. Dennison 1; Kai-Nan An, PhD1; (1)Mayo Clinic; (2)Chang Mai University
Introduction
Four-corner arthrodesis is a common technique for salvage of degenerative wrist problems as well as carpal instability. Advocates of plate fixation state that rigid fixation allows early motion, which improves outcome of surgery. Despite this claim, there have been no comparative studies the effect of early motion on fixation type. The purpose of this study is to compare biomechanical profile of Kwires versus locked and unlocked dorsal circular plate in four-corner arthrodesis in physiologic condition mimicking early active range of motion.
Materials and Methods
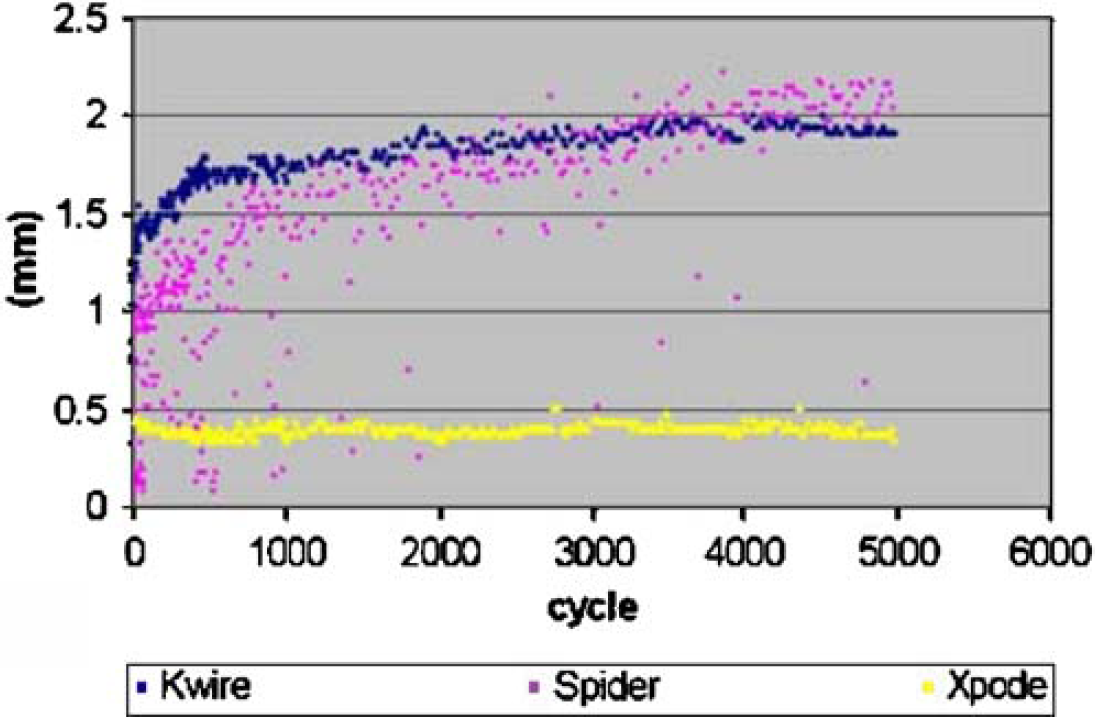
6 paired(12wrists) of fresh frozen cadaveric wrists underwent scaphoidectomy and four corner arthrodesis using K-wires (0.045″ × 4), unlocked stainless steel dorsal circular plates (Spider plate, Kinetikos Medical Inc.) or locked polyethlyethlyketone circular plate (Xpode, Trimed Inc.) An electromagnetic motion sensor was placed in the capitate and lunate. The specimens were placed in a cyclical flexion-extension wrist joint simulator. Repetitive cyclic wrist flexion and extension was applied using both displacement and force control. Hardware failure or motion > 2 mm was considered a failure of fixation.
Results
The biomechanical profiles for 5000 cycles and the initial 100 cycles are shown below(Figure). 67% in the K wire group catastrophically failed, and 67% of the Spider plate group failed. There were no failures of the Xpode plate fixation group. Mode of failure in K-wire group were including pin breakage, bending, and loosening. For the spider group failure mechanism involved loosening screws.
Discussion
This study determined the immediate stability of each fixation technique for cyclical loading mimicking early motion. Spider plate provide more rigid fixation in flexion and abruptly increase motion when more than 35 degree wrist extension occur. Xpode plate provided more stability in extension and was able to withstand cyclical loading in this experiment, and could tolerate simulated early range of motion without failure.
Outcome assessment of arthroscopic interpositional arthroplasty of the trapeziometacarpal joint
Institution where the work was prepared: Brown Hand Center, Phoenix, AZ, USA
Michael Fitzmaurice, MD; P. Stephen Mahoney, MD; Michael Brown, MD; Brown Hand Center
Osteoarthritis of the trapeziometacarpal joint is a common cause of pain in the upper extremity. Small joint arthroscopy allows performance of partial trapeziectomy with interposition arthroplasty without the morbidity of an open procedure. We describe the preliminary results of an outcome assessment of interposition arthroplasty with the artelon implant utilizing the DASH and Nelson scores. The DASH score is a general outcome assessment of function and symptoms in the upper extremity, however, the Nelson score is a new outcome tool designed specifically for trapeziometacarpal arthritis. The DASH is scored from 0–100 with the higher number indicating greater disability. The Nelson is also scored from 0–100; however the lower number indicated greater disability. 21 procedures on 19 patients (2 bilateral) have been performed. Evaluation was performed pre-operatively and at 13 weeks post-operatively. Nearly all patients had full range of motion and were able to touch the small finger to the 5th metacarpal head. Patients who were not retired were able to return to normal work activities. The average DASH score pre and post-operatively was 46 and 22. The average Nelson score pre and post-operatively was 49 and 75. There was a significant improvement in both scores, however, the Nelson score is a shorter survey, easier for patients to complete and appears to be more specific to trapeziometacarpal arthritis. The outcome assessments for the arthroscopic partial trapeziectomy with arthroplasty utilizing the artelon implant demonstrate a significant improvement in both function and symptoms without the morbidity associated with open techniques.
Short-Term Outcomes of Trapeziometacarpal Artelon Implant Compared with Abductor Pollicis Longus Tendon Interposition Arthroplasty - A Case-Control Study
Institution where the work was prepared: Department of Orthopedics, Hässleholm Hospital, Hässleholm, Sweden
Isam Atroshi, MD, PhD; Ingrid Isaxon, PT; Magnus Flondell, MD; Maria Jörheim, MD; Peter Kalén, MD, PhD; Hässleholm Hospital
Background
Several implants have recently been introduced for the treatment of trapeziometacarpal (TMC) osteoarthritis. The Artelon implant is a biodegradable T-shaped device designed to be placed in the TMC joint following minimal trapezial resection to provide joint reconstruction and stabilization. This study aimed to compare short-term efficacy of the Artelon implant with that of trapeziectomy and Abductor Pollicis Longus (APL) tendon suspension interposition arthroplasty.
Methods
A case-control study was designed to include at least 3 controls for each case. The inclusion criteria were primary TMC osteoarthritis that failed nonoperative treatment, surgery with the Artelon implant or trapeziectomy and APL tendon suspension interposition arthroplasty, and postoperative follow-up time of at least 6 months. The Artelon group comprised 13 consecutive patients (10 women), mean age 54 (range 44–75) years. The APL group comprised 40 patients (33 women), mean age 58 (43–76) years, randomly selected with computer among 88 consecutive eligible patients. The mean follow-up time for the Artelon group was 13 (SD 4) months and for the APL group 12 (SD 3) months. All patients completed the QuickDASH questionnaire and a scale measuring thumb pain and related activity limitation, both scored from 0 (best) to 100. Satisfaction with the results of surgery was recorded. The majority attended physical examination performed by a therapist who was blinded to the surgical procedure.
Results
No statistically significant differences between the groups were found but a tendency for better results after APL arthroplasty. The median QuickDASH score for the Artelon group was 25 and for the APL group 20 and the median pain score was 38 and 28, respectively. In the Artelon group 8 patients (61.5%) were satisfied and 5 (38.5%) were neutral or dissatisfied compared with 32 (76%) and 7 (18%), respectively, in the APL group. The mean grip strength as a percentage of the contralateral hand was 82% in the Artelon group and 95% in the APL group and the mean pinch strength was 61% in the Artelon and 86% in the APL group. No statistically significant differences were found between the groups with regard to thumb palmar or radial abduction. One patient in the Artelon group underwent revision to APL arthroplasty.
Conclusions
The short-term outcomes of Artelon implant arthroplasty are at best similar to those of APL tendon suspension interposition arthroplasty. Considering the higher cost of the Artelon implant, these results may not justify its use in the treatment of TMC osteoarthritis.
The Effect on Wrist Flexion Strength of Thumb Carmpometacarpal Joint Arthroplasty Using the Entire Flexor Carpi Radialis Tendon
Institution where the work was prepared: Curtis National Hand Center, Baltimore, MD, USA
Rebecca J. Saunders, PT/CHT; Michael S. Murphy, MD; Curtis National Hand Center at the Union Memorial Hospital
Introduction
Thumb carpometacarpal joint arthroplasty with ligament reconstruction and tendon interposition is a well established procedure for painful arthrosis of the thumb carpometacarpal joint. Many surgeons utilize the entire flexor carpi radialis (FCR) tendon for ligament reconstruction, while some prefer preserving part of the tendon's normal insertion onto the second metacarpal base.
Purpose
To determine if harvesting the full FCR tendon effects postoperative wrist flexion strength.
Methods
A prospective study of 17 patients who underwent thumb carpometacarpal joint arthroplasty with ligament reconstruction and tendon interposition was performed. All patients underwent isometric testing of wrist strength and motion preoperatively, at three months postop, and at six months postop utilizing the Dexter Hand Therapy System automated testing device for strength testing. Testing and ROM measurements were performed by one CHT.
Results
The data was analyzed using paired t tests. There was no statistically significant difference in the wrist flexion strength between preoperative and final postoperative values at 6 months. Average wrist flexion strength, measured in inch-pounds, was 36.7 preoperatively and 37.8 at six months postop (P=0.71). There was also no significant difference in final wrist flexion range of motion. Average wrist flexion preop was 78.9 degrees and at 6 months postop was 77.0 (p=0.51)
Conclusion
Utilizing the entire FCR tendon for thumb CMC arthroplasty with ligament reconstruction and tendon interposition does not adversely effect eventual wrist flexion strength or the range of wrist flexion.
Long-term Follow-up of Surface Replacement Arthroplasty of the PIP Joint
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Peter M. Murray, MD; William P Cooney; Ronald L Linscheid; The Mayo Clinic
Introduction
We propose that surface replacement arthroplasty is a durable alternative for the treatment for osteoarthritis (OA) and rheumatoid arthritis (RA) of the proximal interphalangeal (PIP) joint of the finger. The purpose of this study is to examine the long-term outcome of a surface replacement PIP joint prosthesis with a CrCo proximal component and an ultrahigh-molecular-weight polyethylene distal component.
Methods
51 prostheses were used in 36 patients (mean age, 58 years) over 32 years. There were 33 fingers with degenerative arthritis, 9 with post-traumatic osteoarthritis, and 9 with rheumatoid arthritis. The mean follow-up was 10.7 years (range, 2.6–31.8 years). 44 patients had a dorsal approach, 5 a volar approach and 2 had a lateral approach. 35 patients had cement and 16 had a press fit technique. At follow-up patients were evaluated by physical examination, radiography, DASH, and SF36 assessments.
Results
Average total arc of motion at follow-up was 42 degrees compared to 43.7 degrees pre-operative. 45 of 51 joints were in service at follow-up examination. The average postoperative visual analog pain score was 8/100. 26 of 36 patients had reported pain pre-operative with 6 being severe. The average follow-up DASH score was 46.5, many patients had multiple disabilities. There were 28 complications in 10 patients including 4 fusions and 2 amputations. Complications included extensor and flexor tenodesis, heterotopic bone formation, boutonnière deformity and swan-neck deformity. Additional radiographic complications of polyethylene wear and asymptomatic loosening occurred in 4 and 3 patients respectively. Infection did not occur.
Discussion
At long-term follow up, PIP arc of motion was less but similar to pre-operative motion. 90% of the prostheses were still in service at follow-up and pain relief was excellent. Infection did not occur. We conclude that PIP joint surface replacement arthroplasty is a durable and pain relieving alternative for the arthritic PIP joint of the finger.
Flexor Tendon Tissue Engineering: Bioreactor Cyclic Strain Increases Construct Strength
Institution where the work was prepared: Stanford University and Palo Alto VA, Palo Alto, CA, USA
Sepideh Saber, BS1; Andrew Y. Zhang, MD1; Sae H. Ki, MD1; Derek Lindsey, MS2; Hung M. Pham, BS1; James Chang, MD/FACS3; (1)Stanford University; (2)VA Palo Alto Health Care System; (3)Stanford University Medical Center
Purpose
Mutilating injuries of the hand and upper extremity result in tendon losses too great to be replaced by autologous grafts. Our goal is to use tissue engineering techniques to produce additional tendon material. In this study, we used a custom bioreactor to apply cyclic mechanical loading onto tissue engineered tendon constructs to study ultimate tensile stress, elastic modulus, construct architecture, and cell orientation.
Methods
A custom LigaGen tissue bioreactor providing uniaxial tendon strain was used for this study. Tendon constructs were subjected to a stretch force of 1.25 N over a 5 day course. Constructs used were acellularized tendons reseeded with tenocytes or left unseeded. Actual tendon strain was measured linearly by comparing resting tendon length to tendon length under applied tension. Ultimate tensile stress and elastic modulus of the tendon constructs were compared after different cycle parameters (1cycle/min vs. 2cycles/min in alternating 1 hour periods of loading and rest) using a materials testing system (MTS 858, MTS Inc). Histologic appearances were examined for tendon architecture with specific emphasis on collagen organization and cell orientation. Finally, pairwise comparison of means across groups was assessed using the two-tailed unpaired Student T-test with the significance level set at p<0.05.
Results
Seeded tendon constructs that were exposed to a 1 cycle/min load were found to have a significantly increased ultimate tensile stress and elastic modulus (UTS=84.73 N; ë=1054.77 MPa) compared to non-loaded controls (UTS= 38.90 N, p=0.002; ë=699.98 MPa, p=0.03). Seeded tendon constructs exposed a 2 cycle/min load also had a significant yet less remarkable increase (UTS=73.95 N; ë= 1045.21 MPa) compared to non-loaded controls (UTS= 38.90 N, p=0.01; ë=699.98 MPa, p=0.02). Histologically, stressed tendons showed better alignment of collagen fibrils. Cyclic strain further caused the cells and their actin cytoskeleton to reorient parallel to the direction of strain. This alignment was in stark contrast to the random cell orientation of unstressed constructs.
Relevance
This study shows that cyclic loading of tendon constructs increases the strength of seeded constructs and changes the constructs' collagen architecture and cell orientation. The use of the bioreactor may therefore accelerate the in vitro production of strong, non-immunogenic tendon material that can potentially be used clinically to reconstruct significant tendon losses. The ultimate goal of this project is to produce tissue engineered tendon for clinical use in hand and upper extremity reconstruction.
Barbed Suture Tenorrhaphy - An Ex-Vivo Biomechanical Analysis
Institution where the work was prepared: Curtis National Hand Center, Union Memorial Hospital, Baltimore, MD, USA
Pranay M. Parikh, MD1; James Patrick Higgins, MD2; Steven Paul Davison, MD, DDS1; (1)Georgetown University, (2)Union Memorial Hospital
Purpose
Use of a barbed suture for flexor tenorrhaphy could permit knotless repair with tendon barb adherence along the suture's entire length. The purpose of this study is to evaluate the tensile strength of a novel technique for flexor tendon repair employing barbed suture.
Methods
Forty cadaveric FDP tendons were lacerated in Zone II and randomized to a novel barbed 2–0 polypropylene repair in a knotless 3-core or 6-core configuration, or to a traditional 4-core cruciate repair with either 4–0 polypropylene, 4–0 braided polyester, or 4–0 fiberwire. For each repair, we recorded the cross-sectional area at the repair site before and after tenorrhaphy. Tendons were linearly distracted to failure, and load at failure and mode of failure recorded.
Results
The mean cross-sectional area ratio of 4 core cruciate control repairs was 1.5+/-0.3, whereas those of 3-core and 6-core barbed repairs were 1.2+/-0.2 (p=0.009) and 1.2+/-0.1 (p=0.005), respectively. The mean load to failure of control repairs was 29+/-7 N, whereas those of 3-core and 6-core barbed repairs were 36+/-7 N (p=0.32) and 88+/-4N (p<0.001), respectively. Cruciate repairs failed by knot rupture or pullout in 24/24 tendons whereas barbed repairs failed by suture breakage in 13/14 repairs (p<0.001).
Conclusions
In an ex-vivo model of flexor tendon repair, a 3-core barbed suture technique achieved tensile strength comparable to that of traditional 4-core cruciate repairs, while demonstrating significantly less repair site bunching. A 6-core barbed suture technique demonstrated markedly increased tensile strength compared to 4- core cruciate controls, as well as significantly less repair site bunching. Our data suggest that barbed suture repair may offer several advantages in flexor tenorrhaphy, and that further in-vivo testing is warranted.
Brunelli Pull-OutTechnique in Flexor Tendons Repair in Zones II and III: A Study on 65 Cases
Institution where the work was prepared: University of Medicine Cluj, Spitalul Clinic de Recuperare, Cluj-Napoca, Romania
Alexandru Georgescu, Prof, MD, PhD; Irina Capota, MD; Filip Ardelean, MD; Ileana Matei, MD; UMF Iuliu Hatieganu
Background and Aims
Reconstructing the continuity of long fingers flexor tendons in zones II and III still raises problems from operative point of view. One of the surgical methods with great success rate for zone II lesions is the pull-over technique described by Brunelli. In this paper we will present the modifications proposed by us for this technique, as well as the indication's expansion for lesions in zone III.
Material and Method
The study refers to 65 cases involving flexor tendon lesions in zone II and III, operated in our service since the year 2000 until now. From these, 58 were zone II lesions and 7 zone III lesions. Lacking the very long and highly curved needles used by Brunelli, we modified the initial technique by starting from the proximal towards the distal area and used 2 straight needles continuous threads. In addition and especially for the zone III lesions, we incised the digital skin until near the insertion area of flexor digitorum profundus and the suture thread was passed through the tendon in one or more steps to reach the distal end of the tendon. In 42 cases we used non-absorbable sutures that were removed after 21 days, and in 23 cases absorbable sutures, that were only cut after 21 days. In 57 cases the surgical procedure took place under regional anesthesia that allowed the reinforcement of patient's psychological motivation, seeing the favorable results during surgery. The recovery started from the first post-operative day with passive fingers mobilization, and 48 hours after the surgery we initiated the active against-resistance mobilization.
Results
The patients were followed for 3–24 months after the surgery. We obtained a complete flexion in 32 patients; in 7 patients we had a flexion deficit of 5–10 degrees, in 19 patients we had a 10–20 degrees flexion deficit and in 7 cases we had a 20–30 degrees flexion deficit (all of them having zone III lesions). All the patients were able to resume social life and work in the same place after maximum 45 days. We had no rupture cases and tenolysis was necessary in only 5 cases (patients with complex traumas).
In conclusion, we consider that the Brunelli's technique is a very good method for zone II lesions and that the modifications proposed by us allow a broadening of its indication's field.
Flexor Tendon Tissue Engineering: the Biomechanical Analysis of Explanted Acellularized Tendon Constructs
Institution where the work was prepared: Stanford Hospital and Clinics and the VA Palo Alto Healthy Care Palo Alto, CA, USA
Andrew Y. Zhang, MD1; Sae H. Ki, MD1; Sepideh Saber, BS1; Derek Lindsey 2; Hung M. Pham, BS1; James Chang, MD3; (1)Stanford University; (2)VA Palo Alto Health Care System; (3)Stanford University Medical Center
Purpose
The demand for tendon grafts may exceed supply in mutilating hand injuries. Our tissue engineering model uses the acellularized rabbit forepaw zone II flexor tendon as the scaffold. Cultured tenocytes and adipoderived stem cells (ASCs) are seeded onto acellularized tendon to create novel tendon constructs. Previous studies have established that these constructs are viable in vitro, and that the constructs along with acellularized scaffold maintain comparable tensile strength to fresh tendons in vitro. The purpose of this study is to investigate the in vivo integrity of our scaffold and tendon constructs.
Methods
The experimental cohort contains three groups including 1) acellularized tendon scaffolds, 2) constructs seeded with cultured tenocytes, 3) constructs seeded with ASCs. These constructs were grafted to span a 2 cm gap in rabbit zone II 3rd digit FDP tendons. Our controls included autologus tendon graft over the same area in the adjacent 4th digit and intact fresh tendon in the 2nd digit. Macroscopic and histological appearances along with mechanical testing for ultimate tensile stress (UTS) were determined at 2 and 4 weeks time points. Statistical analysis was performed using the paired two-tailed student t test.
Results & Conclusions
All cohort groups have macroscopic appearances indistinguishable from autologus graft and fresh tendon at all time points. There did not appear to be significant adhesion formation between the grafts and the tendon sheath. Histologically, collagen architecture was preserved in all experiments groups. Minimal cell penetration into the collagen architecture was noted, however it appears that there was more cell penetration as time elapsed.
The UTS was not statistically different between our three experimental cohorts and controls. At 2 weeks time point, the average UTS for intact tendon was 60(N/mm2) compare to 52(N/mm2) for autologus graft (n=12; P=0.2), 61.2(N/mm2) for acellularized tendon (n=3, P=0.46), 46(N/mm2) for Tenocyte seeded constructs (n=4, P=0.55), and 67(N/mm2) for ASC seeded constructs (n=7; P=0.12). At 4 weeks, the average UTS for intact tendon was 53(N/mm2) compare to 42(N/mm2) for autologus graft (n=7; P=0.13), 46(N/mm2) for acellularized tendon (n=3; P=0.5), 41(N/mm2) for Tenocyte seeded constructs (n=3; P=0.29), and 42(N/mm2) for ASC seeded constructs (n=3; P=0.3).
Relevance
Our study suggests that tissue engineered grafts remain viable in the short-term in vivo. Surprisingly, acellularized tendon alone retained strength and may be a suitable substitute for autologus grafting in the short term. Further work will include longer follow up and analysis of repair strength and construct gliding characteristic.
Biomechanical Comparison of Lasso Tendon Repair to Pulvertaft Weave and Side-to-Side Repairs
Institution where the work was prepared: University of Texas Southwestern Medical Center, Dallas, TX, USA
Sean Bidic; Anubodh Varshney, BS; Orenstein Harry; University of Texas Southwestern Medical Center
Introduction
Pulvertaft weaves, although reliable, require substantial tendon length for overlap. Side-to-side tendon repair are less reliable. A new technique for joining tendons, the lasso repair, has been developed. The hypothesis is that the lasso has similar biomechanical strength as the Pulvertaft weave, requires less tendon, and is simpler to perform.
Methods
Lasso repair involves making an axial stab incision 1.5 cm from the end of the passive tendon that allows the active tendon to be tightly weaved using a hemostat. A second longitudinal incision is made in the active tendon such that the active tendon can be weaved through itself. Horizontal mattress sutures are placed at both weave points; an additional suture is placed in between the incisions. Pulvertaft weave repairs had three weaves and sutures and side-to-side repairs had three sutures embedded in the 2.5 cm overlap. Repairs were conducted using porcine trotter flexor tendons obtained at animal sacrifice. Lasso and Pulvertaft weave repairs were standardized with the first incision 1.5 cm from the end of one tendon. Side-to-side repairs were standardized to a 2.5 cm overlap. 4–0 Mersilene suture with 5 knots per suture was used. Ten repairs of each type were performed. Tendon length used in each repair and width of the repair, and time to complete the repair were assessed. Repair failure for each repair was measured using a tensile testing machine with a 5 kN load cell was used to test repairs to failure at a crosshead speed of 20 mm/minute. Load and extension plots and maximum load were digitally recorded using data acquisition software.
Results
The mean maximum load in the side-to-side, Pulvertaft weave, and lasso repair specimens was 88.58N, 159.67N, and 155.78N respectively. Maximum load is found to be the same between lasso and Pulvertaft weave repair based on the Student's t-test (p<0.05). Lasso repair used 7.1 mm less tendon than the Pulvertaft weave and took less than half of the time to complete. Lasso repair is slightly thicker at its widest point than the Pulvertaft weave, but the thickness is concentrated to a small area, while in Pulvertaft weave repairs the thickness is spread out throughout the specimen.
Conclusions
Our study supports the hypothesis that lasso tendon repair is as strong as the Pulvertaft weave, takes less time to perform, and requires less tendon. Side-to-side repair is shown to be an inferior technique due to its characteristically low maximum load.

Flexor Tendon Repair using Modified Lim and Tsai Six Strand Suture Technique
Institution where the work was prepared: Department Of Surgery, Singapore General Hospital, Singapore, Singapore
Jayan Man Shrestha, MS; (General, Su; Shian Chao Tay, MD, MS; Singapore General Hospital
Introduction
Flexor tendon repair with 6 strand suture technique has resulted in improved strength and increased resistance to gapping. We used a modification of Lim and Tsai's technique for flexor tendon repair and assessed the clinical outcome.
Methods
A retrospective review of all complete flexor digitorum profundus (FDP) and flexor pollicis longus (FPL) tendon injuries in zones 1, 2 and 3, with or without flexor digitorum superficialis (FDS) tendon injuries, from May 2002 to May 2006 was conducted. Thirty-one patients with 38 fingers and thumbs were found. Functional outcome was assessed using Strickland and Glosovac's criteria for the finger, and White's method for the thumb.
Results
Out of a total of 38 digits, 22 were rated as excellent (58%), 9 good (24%), 7 fair (18%) ad 0 poor (0%). Twenty-five of these digits were injured in zone 2 and, 13 digits of these digits were rates as excellent (52%), 6 good (24%), 6 fair (24%) and 0 poor (0%). The rate of flexor tendon rupture was 2.6%.
Conclusion
The modified Lim and Tsai technique for flexor tendon repair is a useful 6-strand technique for flexor tendon repair with a satisfactory outcome rate.
Biomechanical Comparison of FiberLoop versus Looped Supramid Extra versus Ethibond Suture in Zone II Flexor Tendon Repair Using a Cyclic Protocol
Institution where the work was prepared: The Cleveland Clinic, Cleveland, OH, USA
Joy V. Sharma, MD, MS; Ryan Milks, BSE; Kathleen A. Derwin, PhD; Peter J. Evans, MD, PhD; Jeffery N. Lawton, MD; The Cleveland Clinic
The purpose of this study was to investigate differences in gap formation and failure load between FiberLoop, looped Supramid Extra (LSME), and Ethibond suture in Zone II flexor tendon repairs. In addition, the inherent properties of the sutures were tested in a simulated tendon construct.
Two sets of ten paired human cadaveric flexor digitorum profundus tendons were used. The tendons were transected in zone II, and randomly repaired with either 4–0 FiberLoop or 4–0 LSME in the first set of ten paired tendons. The second set of ten were randomly repaired with 4–0 Ethibond or 4–0 FiberLoop. All repairs where performed using an eight-strand cruciate repair technique followed by a running epitendinous 6–0 prolene suture. The repaired tendons were cycled 8000 times between 2N and 25N and then pulled to failure. Suture markers were placed on both sides of the repair site to analyze gap formation. In the second part of the study, an eight-strand cruciate repair was performed using a custom fixture simulating a tendon construct. Failure load, method of failure, and knot volumes were recorded and statistically analyzed for the aforementioned suture products.
In the first part of the study, no significant differences were found in gap formation between suture types at 8000 cycles. All mean gaps were less than 2 mm. FiberLoop repairs failed at significantly (p=0.002) higher loads (72.9± 6.6 N) when compared to LSME (64.3±8.8N). However, no significant difference in failure loads was found in the paired flexor tendons comparing FiberLoop and Ethibond. All repairs failed at the tendon suture interface. In the second part of the study, FiberLoop failed by knot slippage at low loads when four throws per knot were used. When six throws per knot were used FiberLoop (235±15.6 N) was significantly stronger than LSME (114.5±6.3 N) and Ethibond (123.9±12.6 N) and majority of repairs failed by suture breakage.
Our data suggests that all three suture products were able to withstand cyclical loading with less than 2 mm gap formation using an eight-strand cruciate repair technique. The second part of the study suggests that FiberLoop is inherently stronger than LSME and Ethibond but the increased strength is realized only when an increased number of throws is used to secure the knot. In the clinical setting, suture breakage may be irrelevant as all repair failures occurred at the suture tendon interface regardless of suture product.
Indications and Clinical Experience Using Adhesion Barrier Wrapping
Institution where the work was prepared: Miami Hand Center, Miami, FL, USA
Alejandro Badia, MD, FACS; Badia Hand to Shoulder Center
The development of postoperative adhesions has long caused clinical problems for hand surgeons in a variety of scenarios. Acute repairs of either tendons or nerves has often been associated with the development of exuberant scar tissue postoperatively that interferes with function. It has been a long sought after goal to try to minimize adhesions using a variety of techniques in order to improve clinical outcome after these types of surgical interventions. Recurrance of adhesions is also a common problem after either tenolysis or neurolysis. The use of a bioresorbable polylactide sheet to minimize adhesions to a protected viscera has demonstrated good clinical benefit in general surgery and gynecologic surgery applications. It is comprised of polylactic acid (PLA) which has a long clinical track record of having minimal tissue reaction with no known side effects. These same benefits have only recently been introduced in the musculoskeletal arena. Clinical indications will be outlined and a series of case examples presented in order to illustrate this concept as applied to hand surgery. Follow-up on these patients has demonstrated no adverse foreign body or inflammatory response, and the clinical goals have been achieved in all cases: namely that of minimizing adhesions as demonstrated by physical exam at the application site. While this physical barrier does not solve the elusive goal of reducing adhesions in zone II flexor repairs due to its mechanical nature, it seems promising for minimizing post-op adhesions in such critical areas as the dorsum of the hand, forearm flexor/extensor tendon applications, and a wide variety of peripheral nerve applications. A future prospective randomized study assessing one specific clinical scenario will shed further light on its efficacy.

American Association for Hand Surgery Concurrent Scientific Paper Session A-2
Intramedullary Fixation of Displaced Distal Radius Fractures
Institution where the work was prepared: Temple University Hospital, Philadelphia, PA, USA
Asif M. Ilyas, MD; Joseph J. Thoder, MD; Temple University Hospital
Purpose
Multiple treatment options exist for operative fixation of distal radius fractures. Recently, there has been increased interest in intramedullary fixation. We treated 10 displaced and unstable distal radius fractures with an intramedullary nail over a one year period. We present our results with an average follow-up of 21 months (minimum 12 months).
Methods
The implant use was limited to extra-articular and simple intra-articular distal radius fractures that displayed instability or persistent malreduction after attempted closed reduction and splinting. The patients were followed at set intervals for a minimum of 12 months.
Results
At an average follow-up of 21 months, the average volar tilt was 3.8° dorsally angulated, radial inclination was 22.9°, radial height was 12.1 mm, and ulnar variance was −0.6 mm. All cases maintained reduction of the fracture between immediate post-operative and final radiographs except for two cases that incurred a loss of volar tilt by 15° and 20°, respectively. Range of motion included wrist flexion of 67°, wrist extension of 71°, supination of 82°, pronation of 85°, radial deviation of 23°, and ulnar deviation of 38°. Grip strength of the operative limb relative to the uninjured limb was 91%. According to the DASH form there was 8 excellent, 1 good, and 1 poor result. The average DASH score was 8.12 (range, 0–57). There were two cases of transient superficial radial sensory neuritis and one case of late DRUJ arthrosis from implant penetration of the joint.
Conclusion
Our report finds that the use of the intramedullary nail in the treatment of displaced distal radius fractures is promising but not without complications. We found good overall maintenance of reduction except in two cases without any long-term soft tissue problems in any cases. The indication for its use should be limited to extra-articular and simple intra-articular distal radius fractures.

Comparison of AO Type B and Type C Volar Shearing Fractures of the Distal Radius
Institution where the work was prepared: Massachusetts General Hospital, Boston, MA, Tuvalu
Jesse Jupiter1; J. Sebastiaan Souer2; David Ring1; (1) Massachusetts General Hospital; (2)Mass General Hospital/Harvard Medical School
Purpose
Fractures of the volar articular margin of the distal radius with volar radiocarpal subluxation (volar shearing fractures) can be accompanied by fracture of the dorsal metaphyseal cortex. We hypothesized that, among volar shearing fractures, injuries with a dorsal cortical break (AO/OTA Type C fracture) are more common than isolated volar marginal articular fractures (partial articular or Type B fractures). We also compared wrist function and perceived disability after both types of fractures.
Methods
In a prospective cohort study of plate and screw fixation of the distal radius, 58 patients with a volar marginal shearing fracture of the distal radius and volar radiocarpal subluxation (volar Barton's fracture) were followed for at least one year. Thirty-eight patients that also had a dorsal metaphyseal cortical fracture (Type C fracture) were compared with 20 patients with a true (Type B) fractures in terms of demographics, injury circumstances, and outcomes according to motion, grip strength, pain, Gartland/Werley Score, DASH and SF-36 scores at 6, 12, and 24 months follow-up.
Results
There were no differences in baseline characteristics between Type B and C fractures. Patients with Type C fractures had significantly less motion forearm rotation (163 vs. 174 degrees; p=0.05), grip strength (72% vs. 85% of opposite arm; p=0.03), and significantly more pain (2.2 vs. 0.6; p=0.01) than patients with Type B fractures at the early (6 month) follow-up, but not at later (12 and 24 month follow-ups). There were no significant differences in Gartland and Werley, DASH, or SF-36 scores at any time point.
Conclusions
Type C volar shearing fractures take longer to recover, but ultimately do as well as true Type B volar shearing fractures.
Significance
Volar shearing fractures are usually complete articular, Type C fractures
Distal Radius Fractures Treated with Multiplanar Cross Pin Fixation and a Low Profile Non-Bridging External Fixator; the CPX System
Institution where the work was prepared: Ather Mirza, MD, Smithtown, NY, USA
Ather Mirza, MD; Ather Mirza, MD
Purpose
To present the findings of distal radius fractures (DRF) treated with the CPX System.
Methods
Forty-nine patients with 52 unstable DRF (40 intra-, 12 extra-articular) were treated with the CPX System. Mean age 54 years (range 17–87 y). Radiological measurements, grip and pinch strength, active wrist range of motion (AROM), and outcome instruments: The Patient-Rated Wrist Hand Evaluation (PRWHE) and the Disabilities of the Arm, Shoulder and Hand (DASH) was used to determined patient's outcome.
Results
Postoperatively, a removable orthosis was applied, mean 6 days (range 2–10 d) and formal wrist rehabilitation began, mean of 8 days (range 2–16 d). There were no pin tract infections, non-unions, tendon injuries or angular collapses. Radiographic parameters were not fully restored in four patients. Two patients had an increase in ulnar variance. K-wires and external fixation was removed, mean of 46 days (range, 39–61 d). At final follow-up (mean 14±10 months) grip and lateral pinch strength recovered 87% and 94% respectively; mean wrist AROM increased to a minimum of 83% of the non-injured side; mean DASH and PRWHE scores were 12.16±14.62 and, 13.8±14.8 respectively. One patient developed complex regional pain syndrome which revolved and one patient had mild transient superficial radial nerve sensitivity without functional compromise. All returned to their prior employment and/or activities.
Conclusion
The CPX System combines multiplanar internal cross pin fixation with a low profile external fixator, providing maintenance of fracture reduction while allowing rehabilitation of the wrist, and resumption of usual activities.
Treatment of Distal Radius Fractures Using a Radial Stabilization Locking Plate
Institution where the work was prepared: Texas Tech University Health Science Center, El Paso, TX, USA
Miguel Pirela-Cruz, MD; Texas Tech Medical Center; David Esquivel, ORT; Texas Tech University Health Science Center
Introduction
Volar plating of distal radius fractures (DRF's) is currently the treatment of choice for addressing unstable fractures of the distal radius. However, there some fractures that require operative intervention but with a less invasive approach. DRF's can now be treated with a radial locking plate that provides adequate stabilization of the fracture and allows for early range of motion (ROM).
Material and Methods
A retrospective review of 36 DRF's was performed. One surgeon in one institution using a newly developed anatomic distal radius plate carried out the surgeries on Type A (extra-articular) and some Type B (partial articular). Supplementary fixation such as a single 0.045 k-wire was required rarely. Range of motion exercises was started one week post-operatively.
Results
All fractures were healed at 6 months post-operatively. A few patients experienced transient paraesthesias in the distribution of the superficial branch of the radial nerve. By 6 months however, the paraesthesias were resolved. Range of motion, D.A.S.H. scores and SF-36 will be presented.
Conclusion
0.R.I.F. using a radial stabilization locking plate provides a simple alternative to traditional volar plating in selective fractures. This approach reduces the surgical dissection and facilitates post-operative recovery.
A Prospective Randomized Clinical Trial of Unstable Distal Radius Fractures treated with External Fixation, Radial Column Plating, or Volar Plating
Institution where the work was prepared: New York Orthopaedic Hospital, Columbia University Medical Ctr, New York City, NY, USA
David H. Wei, MSc1; Noah M. Raizman, MD2; Clement J. Bottino, MD1; Charles M. Jobin, MD1; Robert J. Strauch, MD1; Melvin P. Rosenwasser, MD1; (1)New York Orthopaedic Hospital, Columbia University Medical Center; (2)George Washington University School of Medicine
Background
Optimal surgical management of unstable distal radius fractures is controversial. External fixation and locked volar plating demonstrate excellent clinical results, but evidence from rigorous comparative trials is rare. Additionally, locked radial column plating as an independent method of fixation has not been examined. We compare functional outcomes following external fixation, locked volar plating, and locked radial column plating.
Methods
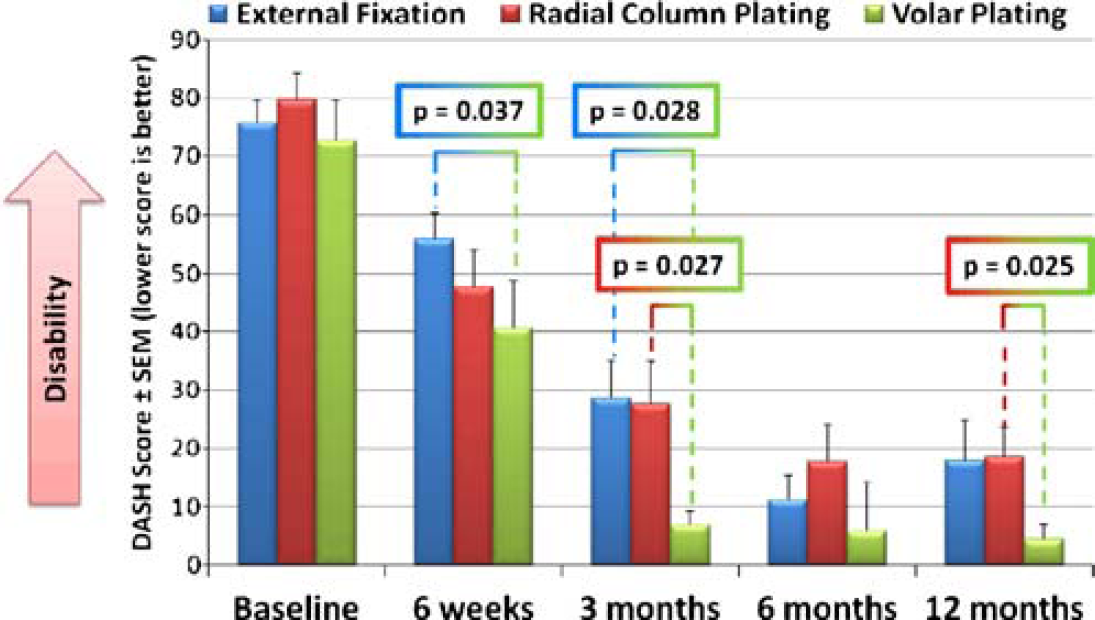
Forty-six patients with single limb injuries were randomized as follows: twenty-two to external fixation, twelve to locked volar plating, and twelve to locked radial column plating. Fractures included OTA types A3 and C1-C3. At two, six, twelve, twenty-four, and fifty-two weeks after surgery, patients completed the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire. Grip and lateral pinch strength, range of motion (ROM), and radiographic parameters were also evaluated.
Results
At six weeks, volar plating demonstrated a significantly better mean DASH score compared to external fixation (p=0.037), but was not significantly different from radial column plating (p=0.33). At three months, volar plating demonstrated the best DASH score, significantly better than external fixation (p=0.028) and radial column plating (p=0.027). By six months and one year, all three groups reached DASH scores comparable to the normal population. External fixation showed significantly better grip strength compared to radial column plating (p=0.042) at six months, but at one year no significant differences were observed. Volar plating showed significantly better lateral pinch strength compared to radial column plating at three months (p=0.042) and one year (p=0.036), but no significant differences were found when compared to external fixation. ROM did not significantly differ between groups at any time beginning twelve weeks after surgery. Radial column plating maintained the best radial inclination and radial length at one year, significantly better than both external fixation and volar plating (all p<0.05).
Conclusions
Early rehabilitation of locked volar plating predictably leads to better patient reported outcomes in the first three months after fixation. However, by one year all three techniques provide excellent outcomes despite minimal differences in strength, motion, and radiographic alignment.
Minimally Invasive Osteosynthesis (MIO) for Asian Osteoporotic Distal Radius Fractures with Small Intramedullary Nail
Institution where the work was prepared: Komaki City Hospital, Komaki, Japan
Naoya Takada; Komaki City Hospital
Purpose
Distal radius fracture is one of common injuries in Asian elderly population. Since 2006 we have used MIO technique with a small intramedullary nail for osteoporotic distal radius fractures. The purpose of this study is to evaluate the clinical outcome of 20 osteoporotic distal radius fractures treated with this method retrospectively.
Methods
Twenty female patients who had sustained distal radius fracture were treated with MIO technique using small intramedullary nail. Their average age at the time of surgery was 67 (range 55–85). According to the AO/OTA classification system, 9 patients were type 23-A2, 3 type 23-A3, 6 type 23-C1, 2 type 23-C2. Two small skin incisions (1.5–2 cm) were used for this procedure. The small intramedullary nail was inserted from a cortical window between the 1st and 2nd dorsal extensor compartments. Three distal buttress screws were inserted into distal fragment and 2 locking screws were inserted into proximal fragment. No patient required post operative immobilization. The average follow-up period was 8.2 months (range 3–18). The range of motion of the wrist, Green and O'Brien score, Quick DASH score and radiographic outcomes were assessed at the latest follow-up and post operative complications were evaluated.
Results
The average range of flexion and extension were 61 (range 50–90) and 62 (range 45–90) degrees. The average Green and O'Brien score was 88 (range 75–100) points. The average Quick DASH score was 3.7 (range 0–13.6) points. Palmar tilt, ulnar variance, radial inclination and radial height at the final follow-up X-ray were 10 degrees, 0.5 mm, 20 degrees and 9 mm respectively. Loss of reduction, implant failure, deep infection and tendon or nerve problems were not found postoperatively.
Conclusion and Significance
No postoperative complications were observed and the clinical outcome was good in this study. This angular stable implant maintained reduction position even in osteoporotic bone. Small skin incisions are advantageous to cosmetic effect. Using this MIO technique, pain and swelling can be little and patients can quickly return to activities of daily; living. The small intramedullary nail was found to be very useful for the treatment of osteoporotic distal radius fractures, although a long-term follow-up is still necessary.
The Effect of an Unrepaired Ulnar Styloid Base Fracture on Outcome after Operative Treatment of a Distal Radius Fracture
Institution where the work was prepared: Massachusetts General Hospital, Boston, MA, USA
Jesse Jupiter; David Ring; J Sebastiaan Souer; Massachusetts General Hospital
Purpose
The indications for ORIF of an ulnar styloid base fracture in association with fracture of the distal radius are debated. We tested the hypothesis that there is no difference in motion or function in patients with untreated ulnar styloid base fractures compared to patients with no ulnar fracture.
Methods
Seventy-four matched pairs of patients, one with an ulnar styloid base fracture and the other with no ulna fracture, were culled from a prospective cohort study of plate and screw fixation of the distal radius. Patient pairs were matched for age, gender, AO fracture type, and injury mechanism. The two cohorts were analyzed for differences in motion, grip strength, pain, Gartland and Werley Score, DASH and SF-36 at 6, 12, and 24 months follow-up.
Results
Patients with an ulnar styloid base fracture had slightly but significantly less motion (styloid fracture vs. no styloid fracture) in the arc of forearm rotation at two-year follow up (164 vs. 171 degrees; p=0.03), pronation at six months follow up (80 vs. 84 degrees; p=0.05), supination at six months (77 vs. 82 degrees; p=0.03), and radio-ulnar deviation at six months (75.9% vs. 84.3% of opposite arm; p=0,04), but had less pain at one-year follow-up (0.5 vs. 1.0; p=0.04). All other comparisons at all other time points showed no significant differences.
Conclusion
Patients with distal radius fractures treated with open reduction and internal fixation that have an unrepaired base of ulnar styloid fracture are nearly identical to patients with no ulnar fracture. The small differences in motion and pain were inconsistent across time, small enough to be of questionable clinical relevance, did not correlate with self-rated disability or physician rated outcome scores.
Significance
Routine internal fixation of an ulnar styloid base fracture is not recommended.
Corrective Osteotomy for Intra-Articular Malunion of the Distal Part of the Radius
Institution where the work was prepared: Ootawara Red Cross Hospital, 2-7-3 Sumiyoshi-cho Ootawara-city Tochigi pref, Japan
Hirokazu Tochigi, MD1; Kazuki Satou, MD, PhD2; Hirofumi Yoshida, MD1; Toshiyasu Nakamura, MD, PhD2; Hiroyasu Ikegami, MD, PhD3; Yoshiaki Toyama, MD, PhD3; (1)Ohtawara Red Cross Hospital; (2)keio University, (3)Keio University
Corrective osteotomy is an appealing treatment for malunited articular fractures of the distal part of the radius since articular incongruity may be the factor most strongly associated with arthrosis and diminished function after such fractures. However, malunion cases of distal radial intra-articular fractures treated with wrist fusion or total wrist arthroplasty were often observed. Enthusiasm for osteotomy has been limited by concerns regarding the difficulty of the technique and the potential for additional injury, osteonecrosis, and nonunion. The purpose of this report was to present the experience of surgeons with intra-articular osteotomies for these injuries, with an emphasis on the techniques and outcomes.
Material and Methods
Seven skeletally mature patients were evaluated at an average of eleven months after corrective osteotomy for intra-articular malunion of the distal part of the radius. The indication for the osteotomy included articular incongruity of >2 mm as measured on a posteroanterior radiograph. According to AO classification, there were two B2, one B3, two C1, two C2. The average interval from the injury to the osteotomy was six months. Preoperative range of motion averaged 38° of wrist extension, 35° of wrist flexion, 50° of supination, 69° of pronation. Preoperative grip strength averaged 15% of that the contralateral side. As a general rule, osteotomy was performed at the original fracture site. The articular reduction was carefully monitored with image intensification. The osteotomy was secured with screws alone in one patient (with the addition of external fixator), plate and screws in six patients. Autogenous bone graft was applied in all patients.
Results
All of the osteotomy sites had healed without evidence of osteonecrosis. One patient had a rupture of the extensor pollicis longus, which was treated with a tendon transfer. The final range of motion averaged 63° of wrist extention, 53° of wrist flexion, 72° of pronation, 81° of supination. The final grip strength averaged 77% of that on the contralateral side. The rate of good results was 43% according to a modification of the rating system of Green and O'Brien.
Conclusions
The results of corrective osteotomy for the treatment of intra-articular malunion are comparable with those of osteotomy for the treatment of the extra-articular malunion. Intra-articular osteotomy can be performed with acceptable safety and efficacy, it improves wrist function, and it may help to limit the need for salvage procedures such as partial or total wrist arthrodesis.
Three-dimensional Corrective Osteotomy of Malunited Fractures of the Upper Extremity Using a Novel Computer Simulation System and a Custom-designed Surgical Device
Institution where the work was prepared: Osaka University, Suita, Japan
Tsuyoshi Murase, MD1; Kunihiro Oka, MD1; Hisao Moritomo1; Akira Goto, MD1; Sayuri Arimitsu1; Yukari Takeyasu1; Junichi Miyake1; Kazuomi Sugamoto, MD1; Hideki Yoshikawa, MD1; Kozo Shimada, MD2; (1)Osaka University; (2)Osaka Koseinenkin Hospital
Background
Three-dimensional (3D) anatomical correction is desirable for treatment of long bone deformity of upper extremity. We developed an original system including a 3D computer simulation program and a custom-made surgical device designed on the basis of simulation to achieve accurate results. In this study, we have investigated the clinical application of this system and preliminary results for corrective osteotomy of malunited fractures of the upper extremity.
Methods
Twenty-two patients with long bone deformities of the upper extremities (four cubitus varus deformities, ten malunited forearm fractures, and eight malunited distal radial fractures) participated in this study. 3D computer models of the affected and contralateral normal bones were constructed using data from computed tomography. The 3D deformity axis and accurate amount of deformity around it were quantified by comparing these models, and a 3D deformity correction was simulated. A custom-made osteotomy template was designed and manufactured to reproduce the preoperative simulation during actual surgery. When we performed surgeries, we placed the template on the bone surface, cut the bone through a slit on the template, and corrected the deformity as preoperatively simulated, which was followed by internal fixation. All patients underwent radiographic and clinical evaluations before surgery and at the most recent follow-up.
Results
Corrective osteotomy was achieved as simulated in all the cases. Bony union occurred in all the patients within 6 months. Regarding cubitus varus deformity, the average humeral-elbow-wrist and tilting angles (i.e., the anterior tilt of the articular condyle of the distal humerus) were 2° and 28°, respectively, after surgery. Radiographic examination showed that the angular deformities of malunited forearm fractures were nearly nonexistent after surgery. All radiographic parameters for malunited distal radius fractures were normalized. The range of forearm rotation in cases of forearm malunion and that of wrist flexion-extension in cases of malunited distal radius improved after surgery.
Conclusions
Corrective osteotomy for bone deformities of the upper extremity using a computer simulation and custom-designed osteotomy template accurately corrects the deformity and consequently improves the clinical symptoms.
Does Delayed Fixation of Non-Displaced Scaphoid Fractures Affect Union Rate
Institution where the work was prepared: Naval Medical Center San Diego, San Diego, CA, USA
Nathan Hammel, MD; Leo Kroonen, MD; Eric Venn-Watson, MD; Edton Ganal, MD; Brian Fitzgerald, MD; Eric Hofmeister, MD; Michael Thompson, MD, PhD; NMCSD
Background
Scaphoid fractures are common upper extremity fractures which can lead to painful non-union. Surgical treatment of non-displaced fractures has led to equivalent union rates as cast treatment although many studies have examined the beneficial effects of surgical fixation on the time to union and return to sport or work. Delayed union of both operative and non-operative treatment can be a difficult problem usually requiring additional surgery. This IRB approved, retrospective study attempts to address a difference in union rates for acute, non-displaced fractures treated operatively within 3 weeks of injury or greater than 3 weeks after injury.
Material and Methods
28 operatively treated non-displaced scaphoid fractures with adequate follow up were identified from our records of operatively treated acute scaphoid fractures by the 3 senior authors over a two year period. Of these patients, 17 were treated within 21 days, at an average of 8 days after injury. Eleven were treated more than 21 days from injury at an average of 47 days. These groups were similar demographically. There were more associated injuries in the early treatment group (5 of 17). The fractures were of the scaphoid waist in 14 of 17 in the early treatment group and in 5 of 11 in the delayed treatment group. In the delayed treatment group there were 5 proximal pole fractures. Fixation was carried out through an appropriately placed percutaneous or open approach. Headless, variable pitch compression screws were used. The outcome of development of non-union was established by clinical and radiographic data analyzed by a senior author.
Results
One of seventeen patients treated early went on to a non-union for a rate of 6%. One of 11 patients in the delayed treatment group developed a non-union for a rate of 9%.
Discussion
Our study evidences an expected union rate for non-displaced fractures despite a delay in treatment and an unfavorable fracture location mix.
Patterns of Upper Extremity Injury in Operation Iraqi Freedom
Institution where the work was prepared: Naval Medical Center, San Diego, CA, USA
Leo T. Kroonen, MD; Kevin Kuhn; Anatoly Hernandez; Naval Medical Center San Diego
Introduction
While there has been some literature documenting general demographics of injuries from the current conflict in Iraq, to our knowledge there has been no study specifically quantifying and describing the patterns of injury to the upper extremity. The purpose of our study was to evaluate wounding patterns to upper extremity in active duty service members evacuated to a major tertiary care medical facility after sustaining injuries in Operation Iraqi Freedom.
Methods
After obtaining approval by the Institutional Review Board, data was retrospectively collected for all casualties returning to our tertiary care facility between April 2003 and July 2006. All patients with an injury to the upper extremity were analyzed. We used simple descriptive statistics to quantify the portion of the upper extremity affected, mechanism of injury, open or closed injury, bony involvement, associated neurologic injury to the extremity, presence of infection, total number of days hospitalized at our facility, and presence of deep vein thrombosis.
Results
Data were recorded for total of 365 casualties received at our facility. Of these casuaties, 134 had sustained injuries to the upper extremity. Injuries involving the shoulder (21/15.7%), brachium (26/19.4%), elbow (19/14.2%), forearm (37/27.6%), wrist (18/13.4%) and hand (53/39.6%). The mechanism of injury involved blunt trauma (34 patients/ 25.4%), blast injuries (68/50.1%) and burn injuries (9/ 6.7%). Positive wound cultures were found in 22 cases (16.4%). 90 cases (67.2%) involved a bony injury, with 52 open fractures (57.8%) and 43 closed fractures (47.8%). Injuries to neurovascular structures were present in 29 patients (21.6%). Deep vein thrombosis was found in three patients (2.2%).
Discussion
Advances in body armor, trauma care and evacuation systems have resulted in the survival of more casualties in the current conflicts than any other previous wars. A critical analysis of the patterns of injury to upper extremity is useful in order to identify potential areas for prevention, and to familiarize the upper extremity surgeon with the nature of these combat injuries. Our study indicates that, at least at the tertiary care level, upper extremity injuries represent the majority of orthopedic injuries. They often result from blunt trauma and blast injuries. A high index of suspicion should exist for concomitant infection and/or nerve injury. Familiarity with the nature of these injuries will assist the upper extremity surgeon in rendering appropriate treatment.
Wrist and DRUJ Arthroscopy findings in Distal Radius Fractures: Treatment and Frequency of Ulnar Styloid Process Fractures and Triangular Fibrocartilage Complex (TFCC) Injuries
Institution where the work was prepared: Yukihiko Obara, Tokyo, Japan
Yukihiko Obara; Saitama Social insurance hospital; Eiko Yamabe, MD; Hiratsuka City Hospital; Astuo Kawakita; Nerima General Hospital
TFCC injury often accompanies distal radius fracture. As part of the treatment of distal radius fractures, arthroscopy was performed to assess TFCC injury, and the incidence of ulnar styloid process fractures and TFCC injuries was ascertained.
Subjects and Methods
The subjects included 49 patients who underwent surgery for distal radius fractures. The patients' average age was 57.3 years. For treatment of the distal radius fracture, a locking plate was used. For ulnar styloid process fracture with DRUJ instability, pinning was performed, and for TFCC fovea detachment without ulnar styloid process; fracture, direct-vision TFCC was also performed in 9 hands. The clinical results were assessed using Mayo modified wrist scores. The type and frequency of ulnar styloid process fracture, the type and frequency of TFCC injury, and the clinical results were investigated.
Results
An ulnar styloid process fracture was seen in 27 hands. A TFCC injury was seen in 35 hands, involving the: disc proper in 19 hands, radial edge in 10 hands, and fovea in 11 hands. DRUJ arthroscopy showed TFCC ulnar facet detachment in 11 hands. The 14 patients with distal radius fractures without TFCC injury were young (average age: 45.3 years), while the 35 patients with distal radius fractures and TFCC injury were elderly (average age: 62.1 years). Ulnar styloid fracture was observed in 27 hands (average age: 58.0 years) and absent in 22 hands (average age: 56.7 years). DRUJ arthroscopy was performed in 35 patients, and TFCC fovea detachment was first seen by arthroscopy in 13 hands (average age: 70.8 years), but TFCC detachment was not seen in 21 hands (average age: 54.1 years). The occurrence of TFCC fovea detachment was not related to ulnar styloid process fracture. The average clinical score was 87.3 points.
Discussion
The present study confirmed that the incidence of TFCC injury in distal radius fractures is high (71.4%). Furthermore, DRUJ arthroscopy confirmed TFCC fovea detachment in 38%. The average age of these patients was high, and the incidence of degenerative injury was believed to be high. However, the incidence of untreated TFCC fovea detachment was unexpectedly high, and favorable results were obtained by performing TFCC suturing in addition. In the future, when treating distal radius fractures, arthroscopy should be performed to accurately assess the site of injury, following which appropriate treatment should be administered.
Biomechanical analysis of an air-cell equipped plastic splint (Aircast) versus conventional plaster splint in a distal radius fracture model
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Shian Chao Tay, MD, MS1; Kristin Zhao2; Kai-Nan An2; William P. Cooney2; (1)Singapore General Hospital; (2) Mayo Clinic
Background
Despite the plethora of surgical treatment options available for definitive treatment of distal radius fractures, acute treatment, and in some cases, definitive treatment is still based on splint immobilization.
Aim
The aim of this biomechanical study is to determine the efficacy of fracture stabilization that is afforded by a polyethylene forearm-based wrist splint, StabilAir Wrist Fracture Brace or Aircast, equipped with inflatable air-cells, as compared to a conventional plaster splint. The hypothesis is that distal radius fracture stabilization provided by Aircast wrist brace is equivalent to conventional plaster splints.
Method
Five right sawbone forearm models and one cadaveric wrist with distal radius fractures (Universal Type IIA) were tested. A custom testing apparatus was built to hold the forearm and a pneumatic force was applied across the metacarpal heads. Fracture displacement was monitored with an optoelectric tracking device synchronized with the load data. The models were tested from 0 to 1.7 kg of load in three conditions: unsplinted control; modified sugar-tong plaster splint treatment; Aircast wrist brace treatment.
Results
There was no significant difference in mean fracture displacements between modified sugar-tong plaster splint treatment and Aircast wrist brace treatment in both sawbone and cadaveric models.
Conclusion
Our study validates the efficacy of the Aircast wrist brace in a biomechanical model. Clinical assessment of the brace is currently in progress for acute, undisplaced and reduced, stable distal radius fractures, and for the post operative support of open reduction internal fixation of distal radius fractures.
Does Vacuum Assisted Wound Closure Affect Tissue Pressures Following Forearm Fasciotomy for Compartment Syndrome? A Cadaver Model
Institution where the work was prepared: William Beaumont Hospital, Royal Oak, MI, USA
Rachel S. Rohde, MD; Nicholas J. Cook, MD; Gregory V. Sobol, MD; William Beaumont Hospital
Introduction
Compartment syndrome occurs when pressures within tissue compartments increase enough to compromise perfusion of structures within the confined spaces. Surgical decompression via fasciotomy lowers these pressures allowing reperfusion, however, edematous tissues often preclude primary wound closure. Temporary wound coverage following fasciotomy traditionally has involved application of sterile non-adherent dressings until definitive wound coverage is feasible. Recently, vacuum assisted wound closure devices (VAC) have gained popularity for wound coverage following fasciotomy. However, the effect of applying a negative pressure environment to tissues recently challenged by increased pressures is unknown. The purpose of this study was to determine the effect of VAC dressing placement on post-fasciotomy compartment pressures.
Materials & Methods
Fourteen fresh-frozen cadaveric upper extremities were obtained. Ten were transhumeral amputations, while four remained attached to the cadaver torso. Simulated forearm compartment syndromes were induced by infusion of Hespan. Pressures at defined proximal, middle, and distal locations in each forearm were recorded prior to and following fasciotomy and after placement of the vacuum assisted closure device. Statistical analysis was performed using Randomized Complete Block Design (RCBD).
Results
There was no statistically significant difference in average pressure with regard to side (right versus left arm) or location of pressure catheter within the arm (proximal, middle, distal). There was no significant difference in the average pressure immediately following fasciotomy compared to that after VAC placement among specimens within each amputation group; however, there was a statistically significant difference in the pressure change following VAC application between the two types of amputations (p<0.05).
Conclusion
Placement of a vacuum assisted wound closure device following fasciotomy for forearm compartment syndrome in a cadaver model does not significantly change compartment pressures. Whether similar pressure consistency is observed clinically in patients treated with VAC following fasciotomy for compartment syndrome currently is being investigated.
A New Test for Evaluating Acute Ulnar Collateral Ligament Injuries of the Thumb
Institution where the work was prepared: University of New Mexico Medical School, Albuquerque, NM, USA
Deana Mercer, MD; John Veitch, MD; Keikhosrow Firoozbakhsh, PhD; Amanda Medoro, MS; Alicia Lacovara, BS; University of New Mexico
Purpose
Traumatic dislocation of the thumb metacarpal phalangeal (MCP) joint can cause a spectrum of injuries to the ulnar collateral ligament complex. Evaluation of the extent of injury to the ulnar collateral ligament complex of the thumb MCP joint is difficult to determine. Radiologic testing is expensive and may delay treatment. It has been alluded to by Smith that the extent of dorsal-volar stability at the thumb MCP joint may provide insight into the structures that have been compromised due to injury. This biomechanical study explores the amount of dorsal-volar instability at the thumb MCP joint with sequential sectioning of the structures that provide ulnar stability at the thumb MCP joint.
Methods
Fifteen fresh frozen cadaver hands (8 male and 7 female, ages 38 to 59) were used in this study. The thumb MCP joint in all specimens were disease free. A specially designed jig was used to secure the specimens in place and to uniformly measure the thumb MCP joint anterior-posterior translation. Load was applied dorsally and volarly and displacement measured. A fixed force of 10N was applied to the proximal phalanx. The moment arm was kept constant throughout the experiment at 1 cm, measured distal to the thumb MCP joint. The displacement was consistently measured at 2 cm distal to the joint. There were three groups tested (1) thumb MCP joint ulnar structures intact prior to sectioning (intact group), (2) thumb MCP joint with ulnar collateral ligament sectioned (MC group) (3) and thumb MCP joint with ulnar collateral ligament and accessory collateral ligament sectioned (MC + group). Load was applied to the intact group, MC group and MC+ group. Sequence of loading was randomized.
Results
The mean and standard deviation were 7.13±4.62 mm for the intact, 12.06±4.96 mm for the MC, and 19.86± 5.00 mm for the MC+ groups. The differences between the groups were statistically significant (p<0.05) using a 2-tailed paired student t-test. This analysis showed that the measured displacements in the MC and MC+ groups were, respectively, 1.69 times and 2.78 times higher than those of the intact group (p<0.001).
Discussion
This biomechanical cadaveric study demonstrates a statistically significant difference in dorsal-volar translation of the thumb MCP joint with increasing disruption of the ulnar collateral ligament complex. The dorsal-volar translation test may help determine the extent of thumb MCP ulnar complex injury and help guide appropriate treatment.

American Association for Hand Surgery Concurrent Scientific Paper Session B-1
Treatment of Symptomatic Neuromas of the Dorsal Radial Sensory Nerve using a Resorbable Nerve Conduit
Institution where the work was prepared: Thomas Jefferson, Philadelphia, PA, USA
A. Lee Osterman, MD; Sergio Rodriguez; John Taras; Thomas Jefferson University
Established symptomatic neuromas of the dorsal radial sensory nerve are difficult problems for which no ideal treatment exists. This paper studied the role of neurolysis and wrapping of the neuroma in a resorbable collagen conduit.
21 patients, 7M, 14F; average age of 33 years (20–52) met the entry criteria: intractable DRSN pain; failure of time, desensitization, and neuroleptic medication; positive electrical studies or a surgically documented DRSN injury. All had DRSN neurolysis and wrapping of the neuroma segment with a NeuraGen® Nerve Guide. Results were evaluated clinically, by visual analog scale, and by DASH questionnaire.
The dominant hand in 52%. 11 had previous surgery to the radial wrist including 4 direct injuries and repair to the DRSN; 7 cases of indirect injury including Dequervain's release, CMC arthroplasty, lipoma resection, ORIF distal radius fracture, and dog bite. The 10 closed injuries related to crush injury, percutaneous needles, radial fracture, and casting. 17/21 has preop electrical studies. All had preop pain management including desensitization and neuroleptics, 17/21 had lidocaine, 12/21 had steroid injection. 2 patients on narcotic medication. The median time from original injury to surgery was 8 months (4–37). The condition was work related in 5; litigation active in 4.
Mean FU 2.8 years (1.2–4.5). No patient was lost to FU. 90% (19/21) were improved and 95% would repeat the surgery. In 19/ 21 hypersensitivity was improved and patients were postoperatively able to tolerate watchbands, bracelets and sleeves. Pre and postop 2PD and Semmes monofilament measurements were variable and not significantly different but all sensory maps identified the DRSN distribution and tended to improve. Subjectively preop numbness decreased in 66%.
Preop TInels decreased from 100% to 38%. Visual analog scales(0–10) improved both at rest and in activity: rest 5 to 0.7; activity 7 to 1.8. Dash improved 71+/-22 to 29+/-18. Wrist ROM Improved in flexIon, radial and ulnar deviation. Grip strength improved 61% to 92%. Key and Tip pinch showed similar data: 55% to 84%, 62% to 88%. Work return: 6 not working rtw usual job; 2 not working rtw modified;; 7 working stayed working;. 4 high level athletes were able to return to their sport.
In summary, neurolysis and wrapping with a resorbable collagen tube is effective in significantly improving the symptomatic neuroma of the DRSN. It is simple to perform, avoids ablation of the nerve and the harvesting of other tissues. One drawback is the expense of the conduit.
Intra- and Inter-Examiner Variability in Performing Tinel's Test
Institution where the work was prepared: Union Memorial Hospital, Baltimore, MD, USA
Kenneth R. Means, MD; Curtis National Hand Center; Eric H. Williams, MD; Dellon Institute for Peripheral Nerve Surgery: Baltimore. Clinical Instructor; Johns Hopkins University School of Medicine; Scott Lifchez, MD; Johns Hopkins University School of Medicine; Reg Dunn; Union Memorial Hospital; A. Lee Dellon, MD, PhD; Dellon Institute for Peripheral Nerve Surgery
Though initially used to detect nerve regeneration, the Hoffman-Tinel sign was adopted in the early 1950's to also detect sites of nerve compression. There have been few attempts to standardize Tinel's test. The goal of this study was to evaluate the intra- and inter-examiner variability in the range of forces created using different Tinel's test techniques.
Methods
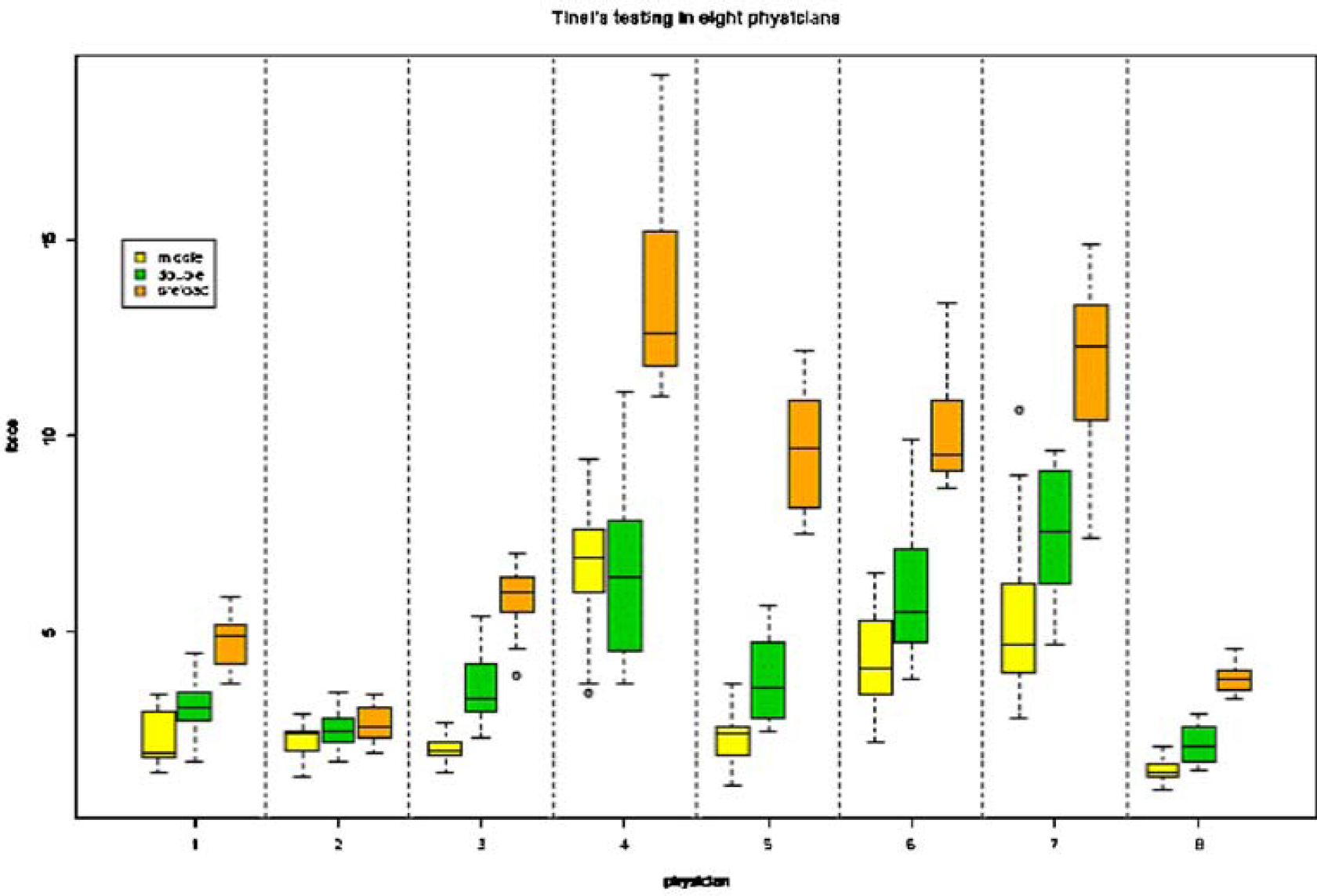
Eight clinicians, consisting of two experienced hand and peripheral nerve surgeons (>10 years in practice), three junior hand and peripheral nerve attending surgeons (1-3 years in practice), and three surgeons in training (plastic or orthopedic surgery residents or hand fellows) were included in the study. A Sensotec load cell with a detection range of 0–100 lbs was used to record the forces generated during the testing. Three different Tinel-type maneuvers were evaluated: 1) striking the load cell using the middle finger only, 2) using the index and middle finger together as a “double finger” strike, and 3) preloading with the opposite thumb and then striking the thumb. Examiners were instructed to use their customary range of force during the testing. Each participant performed three sets of five strikes per technique. Participants were blinded from the load cell recordings. Data was recorded using Labview (National Instruments, Austin, TX) software. Graphic and statistical analysis was performed with the R-Project software.
Results
Intra-examiner: There was a significant difference within nearly all examiners between the range of force they generated with the middle or double finger technique and that which they generated using the pre-load technique (see graph). There was also a difference within nearly all examiners when comparing the range of forces using the middle finger and double finger techniques. Inter-examiner: There were large differences in the range of forces produced by the various examiners for each technique.
Conclusion
There has been no standardization for eliciting the Hoffman-Tinel sign. This study demonstrates that there are considerable intra- and inter-examiner differences in the range of forces generated during a lab simulation for multiple Tinel's techniques that are used in clinical practice. This variability may be responsible for clinical differences in the ability to obtain a Hoffman-Tinel sign in a patient between examiners and may partially explain the inconsistency in sensitivity and specificity reported for Tinel's test in the literature. Further research on standardization is needed and should be used for any studies that employ Tinel's test as part of the study protocol.
Outcomes of Single Versus Double Nerve Transfers for Elbow Flexion
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Brian T. Carlsen, MD; Michelle Kircher; Robert J. Spinner; Allen T. Bishop; Alexander Y. Shin; Mayo Clinic
Background
Restoration of elbow flexion after upper brachial plexus injury can be restored with a single nerve transfer to the biceps branch of the musculocutaneous nerve (MCN) from an ulnar nerve fascicle or a double nerve transfer with an additional nerve transfer to the brachialis branch of the MCN from a median nerve fascicle.
Purpose
Compare the outcomes of single and double nerve transfers for elbow flexion.
Methods
A retrospective review was performed of all patients with paralytic loss of elbow flexion receiving nerve transfer to restore elbow flexion. Single and double nerve transfers were compared in regard to injury level, elbow flexion, supination, and grip strengths, and DASH scores. Elbow flexion and supination torque strength were measured quantitatively in six single and thirteen double nerve transfer patients.
Results
Fifty-five patients (23 single, 32 double) underwent nerve transfer to restore elbow flexion. The mean time from injury to operation was similar (178 days, single vs. 181 days, double). Double nerve transfer patients trended toward improved elbow flexion strength (21% vs. 16%, single) when compared to the contralateral side (p = NS). MRC grade improved to 4 or better in 14/21 single and 24/30 double nerve transfer patients. Supination strength tended to be greater in double nerve transfer patients (37% of contralateral side) compared to single nerve transfer patients (22% of contralateral side) (p = NS). Grip strength was greater in the double nerve transfer patients (42%, single vs. 63% double, p<0.05) compared to the contralateral side. Pre-operative DASH scores were significantly greater in single (51.3) vs. double (37.3) nerve transfer patients. Single nerve transfer patients had a greater improvement in DASH scores (20.2 vs. 8.3, p<0.05). Final mean DASH scores were similar in the 2 groups (29.5, single vs. 28.6, double). The injury level was different between the two groups with 19/23 single nerve transfer patients having injury beyond the C5–6 level and only 16/32 of double nerve transfer patients with >C5–6 injury (Chi probability, 0.041).
Conclusions
Outcomes are similar for single and double nerve transfers for elbow flexion. Double nerve transfer patients have greater grip strength and tend toward improved elbow flexion and supination strength. Patients appropriate for double nerve transfer tend to have less severe injury and lower pre-operative DASH scores than single nerve transfer patients. Single nerve transfer patients had a greater improvement in DASH scores to a level similar to double nerve transfer patients.
Mirza Single-Portal Endoscopic Carpal Tunnel Release. A Prospective, Randomized Study
Institution where the work was prepared: Beth Israel Deaconess Medical Center, Boston, MA, USA
Abigail Zamora, BA; Charles S Day, MD; Albert Yeh, BA; Miguel Ramirez, MD; Beth Israel Deaconess Medical Center/Harvard Medical School
Hypothesis
The Mirza palmar uniportal carpal tunnel release technique involves a small longitudinal incision in the palm that allows identification of the superficial palmar arch and associated branches of the median nerve. This should reduce risk for complications that occasionally arise in traditional endoscopic release techniques.
Methods
All patients were enrolled at a single tertiary care academic medical center. Patients were randomized to either the open or Mirza endoscopic limbs. Exclusionary criteria included other surgical procedures on the affected limb. Follow up visits were performed blindly at 2, 4, 8, and 12 weeks post-operatively. Outcome measurements included the standardized Disabilities of the Arm, Shoulder, and Hand (DASH) survey, grip and pinch strength, sensory tests (2-pt. discrimination, monofilament), and a patient satisfaction questionnaire. Statistical analysis was performed with repeated measures ANOVA.
Results
A total of 48 patients (mean age 54, range 26–81; 36 women) have been enrolled so far. A total of 50 hands underwent surgery (23 endoscopic, 27 open), with the average incision size being 1.67 cm and 2.87 cm. respectively. There was no significant difference between the two procedures with respect to improvement of sensation, DASH scores, grip strength, pinch strength, return to work, overall patient satisfaction, scar tenderness, or return to daily functions throughout follow-up (p>0.05). However, patients who underwent the open procedure reported significantly better pain relief at the 2, 4, and 12 week visits than those who underwent the endoscopic procedure. There were no surgical complications in either group. When asked before surgery, 24 patients preferred the smaller incision, 21 had no preference, and 1 preferred the larger incision.
Conclusions
Contrary to previous studies, there was no difference in the complication rate between the Mirza endoscopic release and open release. Patients preferred the smaller incision despite there being minimal difference in functional outcome. Patients with the open release reported greater pain relief.
Summary Sentence
Patients preferred the endoscopic incision over the open incision despite minimal difference in functional outcome. Patients who underwent the open procedure experience greater pain relief. There was no difference in the complication rate between the Mirza and open procedures.
The 6-item CTS Symptoms Scale - A Brief Outcomes Measure for Carpal Tunnel Syndrome
Institution where the work was prepared: Department of Orthopedics Hässleholm-Kristianstad, Hässleholm, Sweden
Isam Atroshi, MD, PhD; Hässleholm and Kristianstad Hospitals; Per-Erik Lyrén, MSc; Umeå University; Christina Gummesson, PT, PhD; Lund University
Purpose
We used item response theory (IRT) to derive a brief carpal tunnel syndrome (CTS) symptoms scale from a previously validated scale.
Methods
Preoperative questionnaires, including the CTS 11-item symptom severity and 8-item functional status scales, from 693 patients (71% women) undergoing carpal tunnel release were analyzed. The scales were examined using reliability and factor analyses and IRT including differential item functioning (DIF) concerning gender.
Results
Factor analysis of the two scales combined showed presence of a dominant factor related to function including all functional status and two symptom severity items, and three other factors with symptom severity items. The IRT Partial Credit Model (PCM) fit the data well. Four items were removed from the symptom severity scale and two items were merged creating the new 6-item CTS symptoms scale. Factor analysis showed one dominant factor explaining 60% of the variance. Reliability was high (alpha=0.86). The PCM properly fit the new scale and IRT person separation reliability was 0.85. One item displayed significant but very small DIF.
Conclusions
The 6-item CTS symptoms scale has good measurement properties and can be used for outcome evaluation in CTS.
Early Clinical Outcomes with the Use of Decellularized Nerve Allograft for Repair of Sensory Defects within the Upper Extremity
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Furkan Erol Karabekmez, MD; Ahmet Duymaz, MD; Samir Mardini; Steven L. Moran; Mayo Clinic
Introduction
Nerve conduits have become an established option for repair of sensory deficits of up to 2 cm. More recently, decellularized nerve allograft has also been advocated as an option for nerve repair, however no clinical studies have examined its efficacy for sensory nerve defects. The aim of this study was to examine our early experience with the use of decellularized nerve allograft for repair of segmental nerve defects within the hand and fingers.
Material and Method
From July 2007 to March 2008, 9 patients who had 10 nerve gaps were treated surgically using Axogen® nerve allograft. They were 8 digital and 2 ulnar nerve defects. The etiologies of the nerve defects were traumatic nerve transection in 6 defects and neuroma resection and reconstruction in 4 defects. Eight of the affected nerves were sensory and two were mixed, containing motor and sensory fibers. The outcomes were evaluated with moving and static two point discrimination tests. Implantation sites were also evaluated for any signs of infection, rejection or graft extrusion.
Result
There were 8 men and 2 women with a mean age of 42 years (23–65). Mean nerve graft length was 2.3 cm with a range of 0.5–3. Mean follow up time was 4 months (2–5). Average two point discriminations were 7.2 mm moving and 7.5 mm static at last recorded follow-up. No rejection or infection sign were seen around the graft material and sensory improvement was observed in all of the patients despite this short term follow up. Re-exploration of 2 fingers was required for flexor tendon rupture in one and flexor tendon tenolysis in the other. In both cases the nerve allograft was visualized and appeared well incorporated in the repair site.
Conclusion
Decellularized nerve allografts were capable of returning adequate sensation in nerve defects ranging from 0.5–3 cm. There were no cases of infection or rejection and material handling properties were excellent. Decellularized nerve allograft may provide an option for segmental nerve gaps beyond 2 cm. Randomized comparative studies will be required to determine efficacy in comparison to collagen conduits or nerve autograft.
Effect of Profession on Duration of Symptoms Prior to Carpal Tunnel Release Surgery
Institution where the work was prepared: Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
Eric Makhni; Harvard Medical School/Beth Israel Deaconness Medical Center; Charles S. Day; Harvard Medical School
Introduction
The effect of patient career/profession on the duration of symptoms prior to carpal tunnel release has not been investigated. This study sought to determine if such a correlation exists.
Methods
All records of patients seen and examined in our clinic between January 2005-January 2007 were reviewed. Those patients with the diagnosis of carpal tunnel syndrome were included in this review. Records were reviewed for demographic data (including patient profession, such as “serice,” “retired,” “medical,” “laborer,” “clerical,” or “other,”) as well as data pertaining to timing of symptom onset, disease diagnosis, and operative repair (if applicable).
Results
A total of 245 patients carried the diagnosis of carpal tunnel syndrome among all records reviewed. 122 of these patients ultimately had corrective surgery, while the remaining 123 underwent only conservative management. The average age of those patients who received operative management was significantly higher than those who underwent only conservative management (56.3 years vs. 50.3 years; p<0.001). When considering patient profession, there were no significant difference among any of the above-mentioned groups when considering fraction undergoing surgery (p=0.55), duration of symptoms (p=0.61), or number of visits prior to diagnosis (p=0.8). However, there was a trend towards an increasing number of visits before surgery for those in the medical profession (p=0.1).
Conclusions
Those undergoing operative repair for carpal tunnel syndrome are older than those undergoing conservative management only. Because the two treatment groups were similar with respect to duration of symptoms prior to surgery, age may play an important role when considering operative repair. Further, those in the medical profession had more clinic visits pre-operatively than other counterparts, signifying an poentially increased threshold for conservative management.
Comparison of Anterior Transposition and In Situ Decompression for Ulnar Nerve Compression at the Elbow: One Surgeon's Experience
Institution where the work was prepared: Johns Hopkins University School of Medicine, Baltimore, MD, USA; Johns Hopkins University School of Medicine
Ron Gutmark, BA; Elizabeth N. Le, BS; E. Gene Deune, MD
Objective
The most optimal surgical technique for treatment of cubital tunnel syndrome (CTS) has not been conclusively determined. This study examined 38 operations for the treatment of CTS using in-situ decompression (IS) (n=16) or anterior submuscular transposition (ASM) (n=22).
Methods
A retrospective chart review on consecutive operations from 2/2000 to 9/2007 was undertaken on 34 patients, 18 males and 16 females with an average age of 44.7. These patients underwent either IS (n=20) or ASM (n=22). 42.1% of patients had operations on their dominant hands. Severity of ulnar nerve compression prior to and after surgery was determined by objective measures including pinch and grip strength, two point discrimination, and electromyographical (EMG) data, and by subjective measures including the Dellon scoring system and patients' questionnaire (average time to survey was 54 months).
Results
The reoperation rate for the IS group was 0% (0/16) and 18.2% (4/22) for the ASM group. In the IS group, average Dellon scores decreased after surgery by 1.09 points compared with a decrease of 0.18 points for the ASM group. For patients in the IS group, two point discrimination decreased by 2.11 mm after surgery compared to a decrease of 1.94 mm in the ASM group. Grip and pinch strength for the IS group increased by 39.71 and 3.35 lbs, respectively, compared to an increase of 10.18 and 3.53 lbs, respectively, for the ASM group. There were no clear differences between males and females using the various criteria, except with grip and pinch strength, which showed greater improvement with ASM in males vs. females. Those in the younger group (<49) who underwent ASM showed greater improvement in all criteria over the older group. EMG showed greater improvement in the ASM group compared to the IS group with regard to latency and velocity, but the IS group showed greater improvement in amplitude (Table 1).
Conclusion
This study illustrates a superior improvement in several key indicators of efficacy in the IS group when compared to the ASM group. However, EMG latency and velocity and sensory conduction velocity showed better performance than the IS group, but this apparently did not correlate with subjective symptoms. This is likely due to the more invasive nature of ASM and the choice of bed in which the nerve is placed.
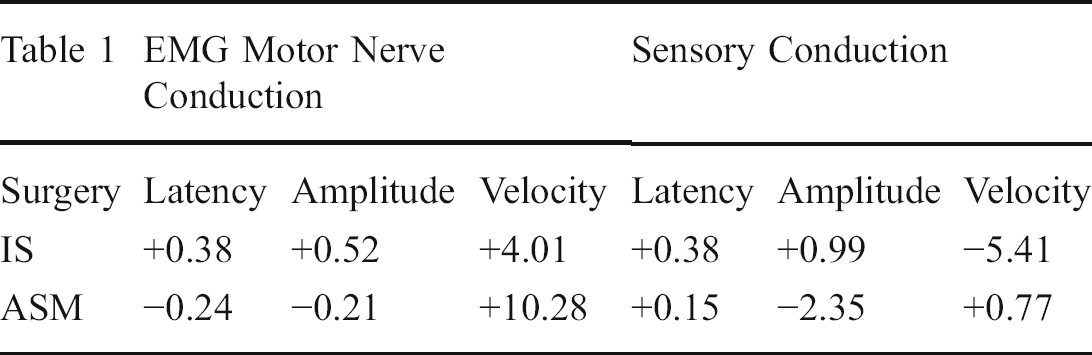
Revision Surgery after Carpal Tunnel Release Using Fascio-Cutaneous Island Flaps
Institution where the work was prepared: University Hospital Bern, Bern, Switzerland
Matthias Traub, MD; Esther Voegelin; University Hospital Bern
Hypothesis
The use of fascio-cutaneous island flaps in the treatment of recurrent or persistent carpal tunnel compression syndrome (CTS) reduces painful symptoms by providing a tension-free gliding tissue cover.
Methods
From 1997–2007, 16 patients (9 women, 7 men, aged 26 to 77 years with a mean of 56.8 years) had 18 operations for either recurrent or persistent CTS, or neuropathic pain syndrome. All patients were treated with neurolysis of the scarred median nerve followed by either a reversed posterior interosseous (n=12) or an ulnar artery perforator flap (n=6) depending on extension and localisation of scarring. The patients were evaluated pre- and postoperatively using a pain visual analogue scale and the DASH score. Sensibility, motor dysfunction, pain and success of the treatment were classified as good, improved or bad. Postoperative ENMG examinations were performed.
Results
Patient mean follow-up was 23.8 months (1.7 to 93.5). The pain evaluation showed a statistically significant improvement (p<0.005) decreasing from a mean value of 6.7 to 1.5. The DASH score was significantly improved postoperatively (p<0.005). The best results were observed in patients without extensive preliminary median nerve damage. The duration of symptoms before re-operation did not influence the outcome. Eight patients demonstrated good, six improved and two patients maintained poor results. The two patients with poor results suffered from extremely scarred and injured median nerves following previous surgery.
Summary
Protective coverage of the median nerve by use of a fascio-cutaneous island flap after failure of carpal tunnel release provides a tension-free gliding tissue cover and reduces the risk of adhesions It reduces painful symptoms effectively, however does not guarantee total pain relief in all patients Pain relief and functional recovery strongly depend on the pre-existing condition of the median nerve Postoperative ENMG show release of compression but no recovery of axonal damage
Application of Fibrin Glue in Microvascular Anastomoses: Comparative Analysis with the Conventional Suture Technique Using a Free Flap Model
Institution where the work was prepared: Instituto de Ortopedia e Traumatologia da USP, Såo Paulo, Brazil
Alvaro B. Cho, MD; Mattar Júnior Rames; Faculdade de Medicina da USP
Background
Several studies have already reported the utilization of fibrin glue in microvascular anastomoses to minimize the number of sutures and to decrease the operative time. Despite the good results obtained in most of these experiments, its clinical application has not launched. The aim of this study was to clarify the controversies around the safeness of fibrin glue application in microvascular anastomoses and also to demonstrate the potential benefits of fibrin glue application in a realistic free flap model.
Methods
Twenty-seven rabbits were used in this study. The experimental model consisted of a free groin flap transfer to the anterior cervical region. The flap's circulation was restored by means of an end-to-side anastomosis between the femoral and carotid arteries, and an end-to-end anastomosis between the femoral and external jugular veins. The first seven animals were used in a pilot study to test the experimental model and train the surgical procedure. The remaining 20 rabbits were divided into two groups according to the anastomosis technique: Group I (conventional suture) and Group II (fibrin glue). The animals were kept alive for at least of two weeks when the anastomoses were re-explored. We used the Student's “t” test to compare the quantitative parametric data and the Mann Whitney “u” test to compare the quantitative non-parametric data.
Results
The number of sutures required to complete the arterial and venous anastomoses was reduced in 39% and 37% in group II, respectively. The mean arterial anastomosis time was 4,5 minutes shorter in the fibrin glue anastomosis group (p=0,00004). The mean venous anastomosis time was 6,4 minutes shorter in group II (p=0,0001). The ischemic time of the flaps was 11,2 minutes shorter in the fibrin glue anastomosis group (p=0,001). The total operative time was also shortened by 15,6 minutes in group II (p=0,0395).
Conclusions
Both arterial and venous anastomoses were benefited from fibrin glue application, which made them easier and faster to perform. Despite the significant amount of suture reduction, the anastomoses maintained adequate patency rates and mechanical strength and the flaps'survival rate was not negatively affected. In this study, the application of fibrin glue in microvascular anastomoses was safe and reliable. The risk-benefit ratio of fibrin glue application in microvascular anastomoses is favorable for its use.
Pedicled Descending Branch Muscle-sparing Latissimus Dorsi Flap for Trunk and Upper Extremity Reconstruction
Institution where the work was prepared: UT Southwestern Medical Center, Dallas, TX, USA
Corrine Wong, MBBS, MRCS; Michel Saint-Cyr, MD; UT Southwestern Medical Center, Dallas
Background
The major blood supply of the latissimus dorsi muscle flap is based on the descending and transverse branches of the thoracodorsal artery. This segmental blood supply allows the muscle to be split and harvested based solely on vascularization from the descending branch, thus sparing the latissimus dorsi muscle function. This article reports the use of the descending branch muscle-sparing latissimus dorsi myocutaneous flap in reconstructing defects on the trunk and upper extremities.
Methods
Five patients with defects on the trunk or upper extremities had soft tissue reconstruction with a pedicled descending branch muscle-sparing latissimus dorsi myocutaneous flap. A transverse skin paddle design was used in all cases. All flaps were performed by the senior author. Complications were recorded, and range of motion analysis was performed comparing operated and non-operated sides during follow-up appointments.
Results
The descending branch muscle-sparing latissimus dorsi flap was used for reconstruction of the: chest wall (2), axilla (2) and upper extremity (1). The skin paddles harvested ranged from 15×7 cm to 24×9 cm. All donor sites were closed primarily. There was one case of minor wound dehiscence on the donor site and one case of wound infection (reconstruction was for chronic, severe axillary hidradenitis suppuritiva). There were no incidences of seroma. In all cases, there was no difference in strength or range of motion around the shoulder joint when comparing the operated to the non-operated side.
Conclusions
The pedicled descending branch muscle-sparing latissimus dorsi myocutaneous flap with a transversely orientated skin paddle results in minimal functional deficit of the donor site, absence of seroma, low rate of flap complications and an aesthetically acceptable scar.
Forearm Osseous Reconstruction with Vascularized Free Fibula Grafts
Institution where the work was prepared: Mayo Clinic, Rochester, MN, USA
Brian T. Carlsen, MD; Scott Thompson, BA; Steven L. Moran, MD; Allen T. Bishop, MD; Alexander Y. Shin, MD; Mayo Clinic
Background
Vascularized osseous reconstruction is indicated for large skeletal defects. Studies reporting the outcome of vascularized fibula for forearm reconstruction are sparse and most include other anatomic locations.
Purpose
Report the outcomes of forearm reconstruction with vascularized fibula grafts.
Methods
A retrospective review was performed of 21 consecutive patients receiving vascularized fibula grafts for forearm reconstruction from 1980 through 2007 at a large academic institution. Patients were analyzed in regard to the etiology and location of the defect. Endpoints included time to skeletal union, post-operative complications, range of motion, and DASH scores.
Results
Twenty-one patients (15 male, 6 female) with an average age of 26.7 (6–59) were identified. The etiologies of the defect included trauma (5), infection (4), tumor (11), and congenital pseudoarthrosis (1). The average defect size was 8.0 cm with a range from 4–13 cm. Eight patients had reconstruction of a single bone (radius or ulna), six patients had construction of a single-bone forearm with the graft, ten patients had fusion of the wrist with the graft, and three patients had a combination of wrist fusion and one-bone forearm construction. At the time of the study, sixteen patients were available for fusion analysis. Primary union was achieved in 10/16 (62.5%) patients at an average of 5.7 months. Six of sixteen (37.5%) patients required additional procedures to achieve union at one of the osteosynthesis sites with union achieved at an average of 28 months after the initial operation in this group. One patient had an additional vascularized corticoperiosteal bone graft from the medial femoral condyle. Seven of 10 patients with reconstruction of tumor defects achieved primary union, vs. two of four patients following reconstruction of infection and trauma related defects. DASH surveys were able to be completed on nine patients at an average of 12 years after injury. DASH scores averaged 15.2 for this group. Postoperative complications were common, occurring in 13/21 (62%) patients. There was one early microvascular failure with conversion to non-vascularized bone graft. Other complications included nonunion (7), infection (3), tendon adhesion (2), radioulnar synostosis (1), delayed microvascular thrombosis (1), fracture of the fibula graft (1), plate fracture/hardware failure (1), median nerve neurapraxia with delayed recovery (1), and superficial radial nerve neuroma (1).
Conclusion
Osseous reconstruction of the forearm with a vascularized fibula graft is a complex procedure associated with major complications. It can provide satisfactory outcomes in patients with limited reconstructive options.
Intravascular Stenting Method for Fingertip Replantation
Institution where the work was prepared: Narushima Mitsunaga, tokyo, Japan
Jun Araki; Narushima Narushima, MD; Tokyo university
Remarkable progress has been made in microsurgery. However, fingertip replantation following amputation has not gained much popularity because of its technical difficulty. We have developed the intravascular stenting (IVaS) method, in which a nylon monofilament is placed inside the vessel lumen to act as a temporary stent, facilitating anastomosis completion. We performed 9 fingertip replantations using the IVaS method. Intravascular stent size varied from 4–0 to 6–0 (0.199–0.07 mm diameter). There were no cases in which the back wall of a vessel became inadvertently caught in the anastomosis. The overall survival rate for distal digital replants was 88% (8/9 replants). It is very difficult to evenly anastomose vessels of differing diameter, especially on a supermicrosurgical scale. In this respect, the IVaS method plays a role in stably anchoring the two vessel ends, allowing for the even spacing of suture knots, even in vessels of different caliber. Because of its ease of use and exactitude, many surgeons may be able to use the IVaS method to reliably complete small anastomoses in fingertip replantations.
Triangular Flaps: a Modified Technique for the Correction of Congenital Constriction Ring Syndrome
Institution where the work was prepared: Chang Gung Memorial Hospital, Kaohsiong, Taiwan
Lynn PL Tan, MBBS, MRCS, MMed; Singapore General Hospital; Yuan-Cheng Chiang MD; Chang Gung University and Chang Gung Memorial Hospital
Background
Congenital constriction ring syndrome (CCRS) is a congenital anomaly with a wide spectrum of clinical presentation. The accepted method of correcting a circular constriction is to excise the deep part of the constriction, and break the line of the circular scar with multiple Z- or W-plasties. Specific correction of soft tissue is recommended concurrently, to better correct the “sandglass” deformity.
Materials and Methods
Here we describe a technique using triangular flaps to correct the deformity in 7 patients with constriction ring syndrome, involving either the upper or lower limbs. In this technique, triangular flaps can be introduced either proximal or distal to the ring, depending on the limb circumference, to better correct the contour deformity.
Results
In all 7 patients, a normal extremity contour was obtained, with complete elimination of the deformity caused by the constriction ring. A mean follow-up of 34 months revealed an aesthetically acceptable scar, with no case of recurrence.
Conclusion
Triangular flaps designed either proximal or distal to the constriction ring is able to correct the contour deformity of the limbs with better versatility and aesthetic results.
Patient Reported Outcome Following a Traumatic Peripheral Nerve Injury
Institution where the work was prepared: University of Toronto and York University, Toronto, ON, Canada
Christine B. Novak, PT, MS, PhD(c)1; Dimitri J. Anastakis, MD1; Dorcas E. Beaton, PhD1; Joel Katz, PhD2; (1) University of Toronto; (2)York University, University of Toronto
Outcome following traumatic peripheral nerve injury (PNI) is variable and the degree of disability depends on multiple factors related to the injury and to the patient.
Purpose
The purpose of this study was to evaluate patient reported outcome and the presence of pain and disability following an upper extremity PNI.
Methods
Following Research Ethics Board approval, the medical charts were reviewed of patients who met the following inclusion criteria: adult patients who at the initial consult were at least 6 months from an upper extremity traumatic PNI and had completed a DASH questionnaire and the SF-36. For the SF-36, comparisons were made between the Canadian norms and the nerve injured patients. Patients were classified as having high pain if they exceeded 2 standard deviations from the normative data. Comparisons of the DASH scores was performed using t-tests or a oneway ANOVA between the following independent variables; pain, workers' compensation or litigation involvement, gender, time since injury, nerve injured. Multiple linear regression was used to evaluate the variables (gender, workers' compensation or litigation involvement, dominant hand injured, time since injury, age, nerve injured, bodily pain) that predicted outcome (DASH).
Results
There were 84 patients (19 women, 65 men) with a mean age 38 years (sd 14 yrs). The mean time following injury was 4 years and the most frequent injury was to the brachial plexus (n=27). For all 8 domains of the SF-36 and the physical and mental component scale, the mean values of the nerve injured patients indicated significantly more impairment than the normative values (p<0.001). The mean DASH score was 52, which indicated an elevated level of disability. Patients with more bodily pain (p<0.001) and brachial plexus injuries (p=0.023) had significantly more disability. Using manual backward elimination and 0.1 level of significance for removal, the final model contained the predictor variables bodily pain (beta=-.481, p<0.001), age (beta=.424, p=0.002) and nerve injured (beta=-4.683, p=0.024) and 45% of the variance was explained with this model.
Conclusion
In patients with traumatic peripheral nerve injuries, disability as measured by the DASH is associated with more bodily pain, older age and brachial plexus involvement. Assessment of chronic pain following PNI and further investigation into the associated factors may provide an opportunity for efficacious treatment and better health related quality of life.
American Association for Hand Surgery Concurrent Scientific Paper Session B-2
Arthroscopic Transosseous Repair of the Ulnar Disruption of the TFCC to the Ulnar Fovea
Institution where the work was prepared: Department of Orthopaedic Surgery, Keio University, Tokyo, Japan
Toshiyasu Nakamura, MD, PhD; Kazuki Sato, MD, PhD; Masato Okazaki, MD; Yoshiaki Toyama, MD, PhD; Hiroyasu Ikegami, MD, PhD; Keio University
Treatment of the DRUJ instability due to ulnar disruption of the TFCC is a challenging issue. We described here an arthroscopic outside-in suturing (trans-ulnar suturing) of the ulnar disruption of the TFCC to the ulnar fovea.
Technique
When the disrupted TFCC from the fovea was diagnosed through the radiocarpal or DRUJ arthroscopy, the TFCC was tightly reattached to the fovea through two tunnels made from the outer cortex of the ulna to the center of the fovea using outside-in pullout technique with double 3–0 polyester sutures (Ticron or Etibond). Before suturing, the fovea area was refreshed by arthroscopic shaver via DRUJ portal.
Patients
We underwent the arthroscopic repair of the TFCC in 21 wrists. Age ranged 14–53 (average 27), 8 male and 13 female were included. There were 10 right and 11 left wrists. TFCC tears were ulnar peripheral + horizontal in 6, fovea avulsion in 14, and proximal slit in 1. Periods from initial injury to the surgery were 6–48 months (average 30). Pain, range of rotation and DRUJ instability were evaluated.
Results
All patients complained pain preoperatively. Pain disappeared in 14 wrists, remained in 3 and recurred in 4. There were no loss of forearm rotation pre- and postoperatively. Preoperative DRUJ instability was noted as „b in 2, + in 6,++ in 13 and postoperatively, 16 wrists indicated no instability. We obtained excellent results in 13, good in 2, fair in 3 and poor in 3.
Conclusion
Arthroscopic trans-ulnar suturing technique is promising procedure in ulnar disruption of the TFCC with DRUJ instability.
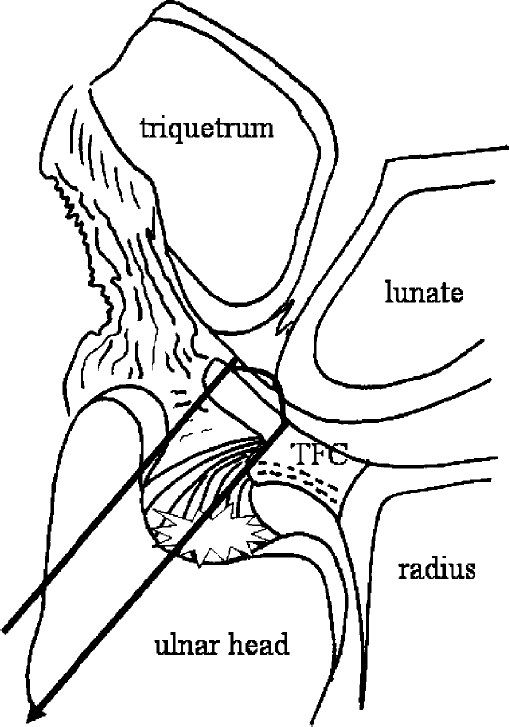
Efficacy and Safety of Clostridial Collagenase for Injection in Patients with Dupuytren's Contracture: Results of a Phase III Trial
Institution where the work was prepared: Indiana Hand Center, Indianapolis, IN, USA
F. Thomas D. Kaplan, MD1; Bronier L. Costas, MD1; Vincent R. Hentz, MD2; Lawrence C. Hurst3; John Lubahn4; (1)Indiana Hand Center; (2)Stanford University Medical Center; (3)SUNY-Stony Brook; (4)Hamot Medical Center
Purpose
Injectable Clostridial collagenase (AA4500) is an investigational, minimally invasive, nonsurgical treatment for Dupuytren's contracture (DC). Single-center trials demonstrated that injection of AA4500 into Dupuytren's cords corrected metacarpophalangeal (MP) and proximal interphalangeal (PIP) joint contracture to 0°Æ-5°Æ of normal in most cases; no placebo-injected cords achieved this response. Two phase III studies (Collagenase Option for Reduction of Dupuytren's [CORD] I and CORD II) are evaluating the efficacy and safety of AA4500 in a larger patient population. Results of the double-blind phase of CORD I are presented here.
Methods
CORD I is being conducted at 16 US sites: an open-label extension is ongoing for patients who require additional therapy for failure of placebo or involvement of other joints. Enrollment required MP and/or PIP flexion deformities °Ã20°Æ. Patients received °Â3 0.58-mg collagenase injections in the cord affecting a primary joint at 4 week intervals. Follow-up occurred 1 day, 1 week, and 1 month after each injection. Primary efficacy variable was primary joint correction to 0°Æ–5°Æ of normal after the last injection. Cords affecting subsequent joints could be injected. Flexion contracture, range of motion, grip strength, and adverse events were evaluated.
Results
In the randomized, double-blind, placebo-controlled phase of CORD I, 306 adults (80% male; mean age 63±9.5 years) who had a mean duration of symptoms of 61±77 months and a mean baseline contracture of 50¨¬ ±20¨¬ were evaluable for efficacy. 62% had one hand affected; 38% had bilateral disease. 58% of patients had no prior treatment; 38% had surgery; and 14% had physical therapy. Patients receiving AA4500 achieved a 79.3% reduction (from 50.2¨¬ to 12.2¨¬) in joint contracture vs 8.6% (from 49.1¨¬ to 45.7¨¬) on placebo (P<0.001). Post-treatment joint contracture was °Â25¨¬ in 82.2% of patients and within 0°Æ-5¨¬ of normal (the primary end-point) in 64% of patients. In contrast, only 6.8% of patients on placebo achieved joint contracture to within 0°Æ-5¨¬ of normal (P<0.001). The most common adverse events included pain, swelling, bruising, and pruritis at the injection site, and transient lymph node swelling and pain. No systemic allergic reactions were noted. Three SAEs possibly related to drug occurred (2 tendon ruptures and 1 complex regional pain syndrome).
Conclusions
The results of this phase III study confirm previous clinical trials (J Hand Surg 2007;32A:767), which showed that injectable Clostridial collagenase effectively and safely corrected or significantly improved MP and PIP contractures in most patients with 1 or more DC-affected joints.
Treatment of Scaphoid Nonunions Using Vascularized Bone Grafts Transplanted Through a Dorsal Approach
Institution where the work was prepared: Kyoto University Hospital, Kyoto, Japan
Ryosuke Kakinoki, MD, PhD1; Ryosuke Ikeguch1; Takashi Nakamura1; Taiichi Matsumoto, MD2; (1)Kyoto University; (2)Kurashiki Central Hospital
Purpose
To report surgical outcomes of 17 patients with scaphoid nonunions using vascularized bone grafts transplanted dorsally.
Patients and methods
17 scaphoid nonunions in 17 patients (16 males and a female) underwent surgery using vascularized bone grafts supplied by the 1–2 intercompartmental supraretinacular arteries. All vascularized bone grafts were transplanted through the dorsal capsule, leaving the palmar radiocarpal ligament intact. The mean age of the patients at the time of the surgery was 27 years (range, 13–59). The mean interval between the injury and surgery was 4.3 years (range, 8 weeks to 42 years). Four patients had had surgery for the scaphoid before the present operations. Arcs of the dorsiflexion, palmar flexion, radial deviation and ulnar deviation and the grip strength of the bilateral wrists were measured before surgery and at the time of the final follow-up in each patient. The arc angles and grip strength of the affected hands were expressed as percentages of those of the contralateral hand. The radiolunate angles of the affected wrists were measured on the postoperative and preoperative plain X-ray films. The postoperative status of the affected wrists was assessed using a modified Mayo Wrist Scores.
Results
Bone union was obtained in all patients except a patient. The average interval between the surgery and bone union was 11.9 weeks (range, 8–30 weeks) in the remaining 13 patients. The DISI deformity was corrected after the operations in all patients having shown DISI deformity before the surgery. The respective preoperative and postoperative average arcs of the affected wrists were 80±12% and 74±14% in the dorsiflexion, 76±17% and 62±18% in the palmar flexion, 55±21% and 53±26 in the radial deviation, 94±23% and 75±12% in the ulnar deviation. The preoperative and postoperative grip strength were 71±17% and 84±17%, respectively. The palmar flexion and ulnar deviation significantly decreased postoperatively. The radiolunate angles significantly decreased from −10.2±9.7% preoperatively to 1.2±9.4% post-operatively in the patients having had the DISI deformity before surgery. The mean modified Mayo Wrist Score was 74 (range, 60–90). There were no patients who developed avascular necrosis of the proximal scaphoid.
Conclusion
Vascualrized bone grafts transplanted to scaphoid nonunions dorsally corrected the DISI deformity and prevented the development of the avascular necrosis of the proximal scaphoid.
Underutilization of Upper Extremity Reconstruction for Persons with Tetraplegia: The Patient Perspective
Institution where the work was prepared: Rehabilitation Institute of Chicago, Chicago, IL, USA
Michael S. Bednar, MD1; Rebecca Ozzelie, OTR/L2; Elizabeth Jordan, OTR/L, CHT1; (1)Loyola University -Chicago; (2)Rehab Institute of Chicago
While it is estimated that 65% of persons with tetraplegia would benefit from upper extremity reconstruction, fewer than 10% actually have the procedure performed. Recent studies suggest barriers to these procedures include an inadequate referral network between physiatrists and surgeons and the hestitancy of physiatrists to recommend these procedures to their patients. At our institution, tetraplegic patients are seen in a multidisciplinary clinic, including both physiatry and hand surgery. The physiatrists encourage all patients to be evaluated. Despite this, only 18% of patients who are candidates for upper extremity reconstruction choose to have the procedures. The goal of this study is to survey the patients who chose not to have surgery to determine reasons for their choice.
Over 5 years, 113 patients were evaluated. Twenty eight patients were ineligible for surgery. Fifteen had surgery. Of the remaining 85, 70 were contacted to participate in this study and 30 agreed. Of the participants, the mean age was 36 years old, 90% were male. An IRB approved telephone survey, based on the instrument designed by Curtin, was administered by one of two occupational therapists. Questions included those derived from the disability dimension of the Standford Health Assessment Questionnaire to determine functional status. All questions were answered on a 4 point scale. Data was analyzed using a cluster analysis.
Four clusters of patient attitudes were identified. The first, named “conflicted” had the lowest time since injury (6.4 years). Their concerns centered on having to rely on others, waiting for recovery, and not wanting more surgery. The second cluster, named “waiting for the cure”, stated this was their only concern. They had the highest level of function. They had the smallest increase in interest in having surgery after attending clinic of any of the clusters. The third cluster, named “too costly”, cited cost, relying on others, and business of life as barriers. This group had the lowest ADL scores and the longest time since injury. The last cluster, named “questioning”, stated they still didn't understand the benefit of the surgery. This group had the largest increase in interest in surgery after attending clinic.
Each of the four groups presented with unique issues and concerns regarding their decision to not have upper extremity reconstruction. Each of the groups requires differing degrees of education about the procedures and rehabilitation, insurance issues, and social support.
The Point Prevalence of the DRUJ Injuries Complicating Perilunate Injuries
Institution where the work was prepared: Kleinert Institute for Hand and Microsurgery, Louisville, KY, USA
Tuna Ozyurekoglu, MD; Paolo Sassu; Sandy Hanlin; Christine M. Kleinert; Institute for Hand and Microsurgery
Purpose
To find out the prevalence of the distal radioulnar joint related injuries associated with Perilunate dislocations at their initial presentation to the hand surgeon.
Methods
Twenty-two perilunate dislocations in 21 consecutive patients were evaluated and treated at our Level 1 Trauma Center between November 2003 and July 2006. Two female and 19 male patients with a mean age of 37 (range 19–59) formed the group. Nine patients were involved in motor vehicle accidents, 12 patients fell from height. There were 8 perilunate dislocations and 14 transscaphoid fracture dislocations in the group. Five had contralateral wrist injuries. Pathologic findings were analyzed for each wrist by reviewing the patient charts, operative notes and digital images. The distal radioulnar joint (DRUJ) related injuries were defined by the presence of a fracture at the base of the ulna styloid, widening or subluxation of the DRUJ, distal radioulnar instability noted or treated at the time of initial surgery.
Results
Eleven wrists (50%) showed DRUJ related injuries. Eight of these had a displaced fracture at the base of the ulna styloid, one had a flake of bone at the prestyloid area, one had a fracture of the ulnar shaft with DRUJ instability, and one had widening of the DRUJ. Three non-displaced ulna styloid fractures were not included. Of the eleven DRUJ related injuries only eight received initial treatment. Four wrists showed ulnar translocation of the lunate, four had associated fracture of the radius; eight had a fracture line through the triquetrum.
Conclusion
The point prevalence of the DRUJ injuries complicating Perilunate injuries at their initial presentation was estimated as 0.50, with a confidence interval of 28.8–71.2. Because the initial appraisal of both the osseous and ligamentous pathology is important in the management of perilunate dislocations DRUJ related injuries should also be addressed at their initial presentation.
Endoscopic Cubital Tunnel Recurrence Rates
Institution where the work was prepared: Orthopaedic Specialists, Davenport, IA, USA
Tyson Cobb, MD; Orthopaedic Specialists, PC; Patrick T. Sterbank, PA-C; ORTHOPAEDIC SPECIALISTS, P.C; Jon Lemke, PhD; Genesis Medical Center
Hypothesis
Endoscopic Cubital Tunnel release has a recurrence rate no greater than open cubital tunnel release.
Methods
After approval of our institutional review board we reviewed 134 consecutive cases of endoscopic cubital tunnel release in 117 patients. Post operative outcome was measured by the Modified Bishop classification. A recurrence was identified if the patient was symptom free immediately following surgery but had symptoms reappear after a minimum 3 month post operative period as described by Seradge et al in 1998. Two literature control groups were used from published reports of recurrence rate following open cubital tunnel release. Seradge, et al reported recurrence in 21 of 160 patients under going cubital tunnel release with medial epicondylectomy at 3 or more months. Lankester and Giddins reported 1 of 20 patients with recurrence after 10 months with simple decompression.
Results
Of the 134 cases of Endoscopic Cubital tunnel releases there were 104 cases for 94 patients with 3 month post operative follow-up. There were no exclusions and included concomitant surgeries and co morbidities. The mean follow up time for the 104 cases was 736 days ranging from 92 to 1,766 days. The 94 patients consisted of 58 males (61.70%), 36 females (38.3%), age range from 21–89 and the mean was 49 for males and 47 for females. One case (0.96%) met the criteria for recurrence at 4 months post procedure. Of the 104 cases, 92.31% had more than 4 months follow-up.
Data was then compared to the literature control groups used from published reports of recurrence rates following open cubital tunnel release. Pooled the combined controls had 22 of 180 cases (12.22%) with recurrences. The procedure recurrence percents varied significantly with p-value=0.0004. The data was analyzed using STATXACT for an exact test comparing the two recurrence percents.
Summary
We are 95% confident our true recurrence rate is between 0.02% and 5.24%. Recurrence after Endoscopic Cubital Tunnel release is not greater than recurrence following open cubital tunnel release.
Outcome Following Acute Primary Darrach Resection for Comminuted Fractures of the Distal Ulna at the time of Operative Fixation of Unstable Fractures of the Distal Radius
Institution where the work was prepared: New York University Hospital for Joint Diseases, New York, NY, USA
David E. Ruchelsman, MD; Keith B. Raskin, MD; Michael E. Rettig, MD; NYU Hospital for Joint Diseases
Background
Optimal acute management of the highly-comminuted distal ulna head/neck fracture sustained in conjunction with an unstable distal radius fracture requiring operative fixation is not well-established.
Purpose
To determine the clinical, radiographic and functional outcomes following acute primary Darrach resection for comminuted distal ulna fractures performed in conjunction with the operative fixation of unstable distal radius fractures.
Methods
Between 2000–2007, eleven consecutive patients, mean age 63 years (range, 45–75) were treated for concomitant closed, comminuted, unstable fractures of the distal radius and ulna metaphysis. All eleven patients underwent acute primary Darrach distal ulna resection through a separate dorsal ulnar incision with ECU tenodesis for irreparable distal ulna head/neck fractures at the time of operative fixation of the distal radius fracture. According to the Q modifier of the Comprehensive Classification of Fractures, there were six comminuted fractures of the ulnar neck (Q3), and five fractures of the head/neck (Q5). Operative fixation of the distal radius fracture included volar plate fixation followed by 6 weeks of cast immobilization in four patients, and standard spanning external fixation with supplemental percutaneous Kirschner wires in seven patients. At a mean of 3.5 years postoperatively, clinical, radiographic, and wrist-specific functional outcome with the modified Gartland and Werley wrist score were evaluated.
Results
At latest follow-up, mean wrist range of motion measured 55° flexion, 50° extension, 85° pronation, and 75° supination. Mean grip strength measured 90% of the contralateral, uninjured extremity (range, 55–120). No patient had clinical evidence of ulnar stump instability or symptoms related to the dorsal ulnar sensory nerve. Final radiographic assessment demonstrated restoration of distal radius articular parameters without ulnar stump instability or ulnar carpal translocation. According to the system of Gartland and Werley as modified by Sarmiento, there were seven excellent and four good results. No patient required a secondary surgical procedure at latest follow-up.
Conclusion
Acute primary Darrach resection yields satisfactory clinical, radiographic, and functional results in appropriately selected patients and represents a reliable alternative when anatomic restoration of the distal ulna/sigmoid notch cannot be achieved. Distal ulna resection concomitant with distal radius fixation may help avoid early or late secondary procedures related to distal ulna fixation or symptomatic post-traumatic distal radioulnar joint arthrosis.
Low Calcaneal Bone Mineral Density is Associated with a High Risk to Sustain a Distal Radius Fracture – a Population-Based Study
Institution where the work was prepared: Department of Orthopedics Hässleholm-Kristianstad, Hässleholm, Sweden
Isam Atroshi, MD, PhD1; Fredrik Åhlander, MD1; Mats Billsten1; Henrik G. Ahlborg, MD, PhD2; Dan Mellström, MD, PhD3; Claes Ohlsson, MD, PhD3; Östen Ljunggren, MD, PhD4; Magnus K. Karlsson, MD, PhD2; (1)Hässleholm and Kristianstad Hospitals; (2)Lund University; (3)Gothenburg University; (4)Uppsala University
Introduction
Osteoporosis is defined by the World Health Organization as a bone mineral density (BMD) T-score below −2.5 measured with a dual-energy X-ray absorptiometry (DXA) total body scanner. Portable heel scanners have gained increasing interest but their fracture predictive ability is less evaluated. We used a DXA heel scanner to estimate the prevalence of osteoporosis in a population with distal radius fracture and evaluate calcaneal BMD's predictive ability.
Material and Methods
Patients aged 20 to 80 years with distal radius fracture treated at one emergency hospital during two consecutive years were invited to calcaneal BMD measurement. Of 421 eligible patients, 333 (79%) participated; 270 women, mean age 63 (SD 12) years, and 64 men, mean age 54 (15) years. A Calscan DXL heel scanner estimated BMD (g/cm2) and T-score values. A population-based cohort including 153 women, mean age 58 (13) years, and 305 men, mean age 74 (5) years, served as controls. The comparison between the fracture and control populations involved women 40 to 80 and men 60 to 80 years. The age-specific prevalence of osteoporosis (T-score below −2.5 SD) was determined and the ability of calcaneal BMD to discriminate between the fracture and normative cohorts was assessed by receiver operating characteristic (ROC) analysis.
Results
The prevalence of osteoporosis in women aged 40 to 80 years with a distal radius fracture was 32% compared with 16% in the control group (age-adjusted prevalence ratio (PR) 1.46, 95% CI 1.01–2.11, p=0.046), and in men aged 60 to 80 years were 44% and 6%, respectively (PR 10.5, 95% CI 5.9–18.7, p<0.001). Age-adjusted BMD was lower in the fracture cohort than the normative cohort; mean difference (95% CI) in women 0.11 (0.10–0.13) and in men 0.13 (0.09–0.18) g/cm2 (p<0.001). One SD lower BMD was associated with an increased odds ratio (95% CI) for having a distal radius fracture of 1.8 (1.4–2.3) in women and 2.3 (1.6–3.3) in men. The area under ROC curve (95% CI) was in women 0.63 (0.57–0.69, p<0.001) and in men 0.77 (0.67–0.87, p<0.001).
Conclusions
The prevalence of osteoporosis based on DXA-measured calcaneal BMD is significantly higher in individuals with a distal radius fracture than in a normative cohort. Impairment in calcaneal BMD by one SD is associated with approximately doubled risk of a distal radius fracture.
Clinical and Radiographic Outcomes Following Utilization of Purpose-Designed Threaded Pins for the Treatment of Extraarticular Distal Radius Fractures
Institution where the work was prepared: The Philadelphia Hand Center, PC, Philadelphia, PA, USA
John S. Taras, MD; The Philadelphia Hand Center, PC; Joshua Abzug, MD; Hahnemann University Hospital
Hypothesis
Purpose-designed threaded pins are effective for the treatment of extraarticular distal radius fractures (T-Pin®, Union Surgical, Philadelphia, Pennsylvania).
Methods
A prospective study was undertaken to evaluate patients with extraarticular distal radius fractures who underwent fixation with threaded pins. Flexion, extension, pronation, supination, and JAMAR grip strength values were recorded. Data from the uninjured extremity provided a baseline by which to compare the patient's range of motion and strength. Pre- and postoperative radiographs were performed to assess volar angulation and ulnar variance. Statistical analysis was performed utilizing Signed Ranks test on SPSS.
Results
67 patients underwent fixation of their extraarticular distal radius fracture with purpose-designed threaded pins. The flexion-extension arc returned to 66% (87 degrees: 42 degrees flexion; 45 degrees extension) of the patients' normal arc by the 3 month period, and was 83% (119 degrees: flexion 54 degrees; extension 65 degrees) of normal by 1 year postoperatively. The pronation-supination arc was 83% (142 degrees: 77 pronation; 65 degrees supination) of the contralateral side by 3 months postoperatively and 94% of normal (159 degrees: 83 degrees pronation; 76 degrees supination) by 1 year. JAMAR grip strength at position 3 returned to 72% of normal at an average of 7 months. Preoperative radiographs demonstrated an average of 11.85 degrees of dorsal angulation and ulnar variance of minus 1 millimeter. The postoperative radiographs showed improvement to an average of 5.22 degrees of volar tilt and ulnar variance of 0.7 millimeters (p<0.05). There were 3 complications reported with 1 loss of reduction in a patient who was weight bearing in that upper extremity.
Summary
Purpose-designed threaded pins are safe and effective implants for the treatment of extraarticular distal radius fractures. Patients regain 90% of their range of motion by 1 year postoperatively and 72% of their strength by approximately 6 months postoperatively. Radiographic reduction is improved significantly with regard to radial length and volar tilt.
Outcome of Nonoperative Treatment of Ulnar-Sided Wrist Pain
Institution where the work was prepared: University of Pittsburgh Medical Center, Pittsburgh, PA, USA
Robert Joseph Goitz, MD; Ali Razfar; John M. Duffy, PAC; Robert Alexander Kaufmann, MD; Deborah Kowalchuk; James Irrgang; Camilo D. Borrero; Jeffrey D. Towers; University of Pittsburgh Medical Center
Hypothesis
Patients with acute ulnar-sided wrist pain can be effectively treated with a splint and steroid injection. Physical examination and MRI findings will predict failure of nonoperative treatment.
Methods
Forty-five patients with less than a three month history of ulnar-sided wrist pain were followed prospectively. All patients underwent a physical examination, radiographs and MRI. Patients were provided a custom fabricated Muenster splint. If pain continued after 1 month, patients received a steroid injection and continued splint wear for an additional month. If they continued to have pain, then surgery was offered. Univariate logistic regression was performed to estimate the effect of potential predictors on the odds of failing non-operative treatment.
Results
The mean age was 37.5 (range, 12–76 years) and the median duration of symptoms was 1.5 months. Thirty-three patients (75%) associated their pain with a traumatic event. 40.0% of patients were successfully treated with a splint alone. Nineteen patients received an injection at an average of 34 days following initial presentation. 58% of injected patients had successful relief of symptoms. 16 patients ultimately underwent surgery and 2 patients that failed splinting and injection deferred surgery for an overall success rate of 60% of this non-operative regiment. The TFCC stress test was the only finding that had a significant effect on the odds (OR 13.6, 95% CI 2.57, 71.86) of failing non-operative treatment. The likelihood ratio for a positive TFCC stress test was 2.40, which increased the post-test probability of failing non-operative treatment from 40% to 62%. The negative likelihood ratio was 0.18, which decreased the probability of failing non-operative treatment from 40% to 11%.
Summary
Patients with acute ulnar-sided wrist pain have a 60% chance of successful treatment with a splint and injection. Patients with a positive TFCC stress test have a higher chance of failing nonoperative treatment and may be better treated with immediate surgery.
Baseline Characteristics of Patients Enrolled in Two Phase III Studies of Injectable Clostridial Collagenase for Dupuytren's Contracture
Institution where the work was prepared: The Indiana Hand Center, Indianapolis, IN, USA
F. Thomas D. Kaplan, MD; Indiana Hand Center; Marie Badalamente, PhD; SUNY-Stony Brook; Robert N. Hotchkiss, MD; Hospital for Special Surgery; John D. Lubahn, MD; Hand, Microsurgery and Reconstructive Orthopaedics; Stephen Coleman, MD; Rivercity Hospital; Stephen Hall, MD; Emeritus Research
Purpose
Prior studies have shown that intralesional injections of Clostridial collagenase (AA4500)—an investigational, minimally invasive, nonsurgical treatment for Dupuytren's Contracture (DC)—reduce the degree of contracture in metacarpophalangeal (MP) and proximal interphalangeal (PIP) joints to within 5° of normal in most patients; placebo injections did not produce this response. The demographics of subjects participating in 2 multicenter, phase III studies comprising randomized, double-blind, placebo-controlled and open-label extension phases investigating the efficacy and safety of Clostridial collagenase are representative of a larger number of patients than previously studied.
Methods
Studies designated Collagenase Option for Reduction of Dupuytren's (CORD) I with 16 US sites and CORD II with 5 Australian sites are ongoing. Enrollment required flexion deformities of ≥20° of the MP and/or PIP joints. Patients in the double-blind phase receive up to 3 injections of 0.58 mg of collagenase in the primary joint, at 4–6 week intervals. In the open-label phase, patients receive up to 5 additional injections (up to 3 injections/joint). Patients are to be followed for up to 12 months post first injection.
Results
Baseline characteristics for the 374 patients enrolled in both studies (Table) are available. Mean age was 63±9.4 years. At time of diagnosis, 21% of patients were <45 years old (mean age, 53±13 years), 45% of patients had a family history of DC. Comorbidities included collagen diseases (knuckle pads [4%,] Ledderhose's disease [5%,] Peyronie's disease [5%]), diabetes (7%), and epilepsy (2%.) Disease was unilateral and bilateral in 60% and 40% of patients, respectively and mean number of affected joints per patient was 3±2. Mean duration of symptoms was 62± 78 months. Mean contracture was 50°±20°, and mean range of motion was 44±20. Overall, 56% of patients had no treatment prior to study entry. The topline efficacy and safety data for the double-blind phase of CORD I became publicly available in June 2008. Results from this analysis will be presented.
Conclusions
Baseline characteristics of this large population of patients with DC are similar to those from previously reported trials investigating Clostridial collagenase. Exceptions include bilateral disease, which was twice as common in the CORD studies, and frequency of comorbid fibrotic disorders such as Peyronie's Disease, which were lower among patients in the CORD studies.
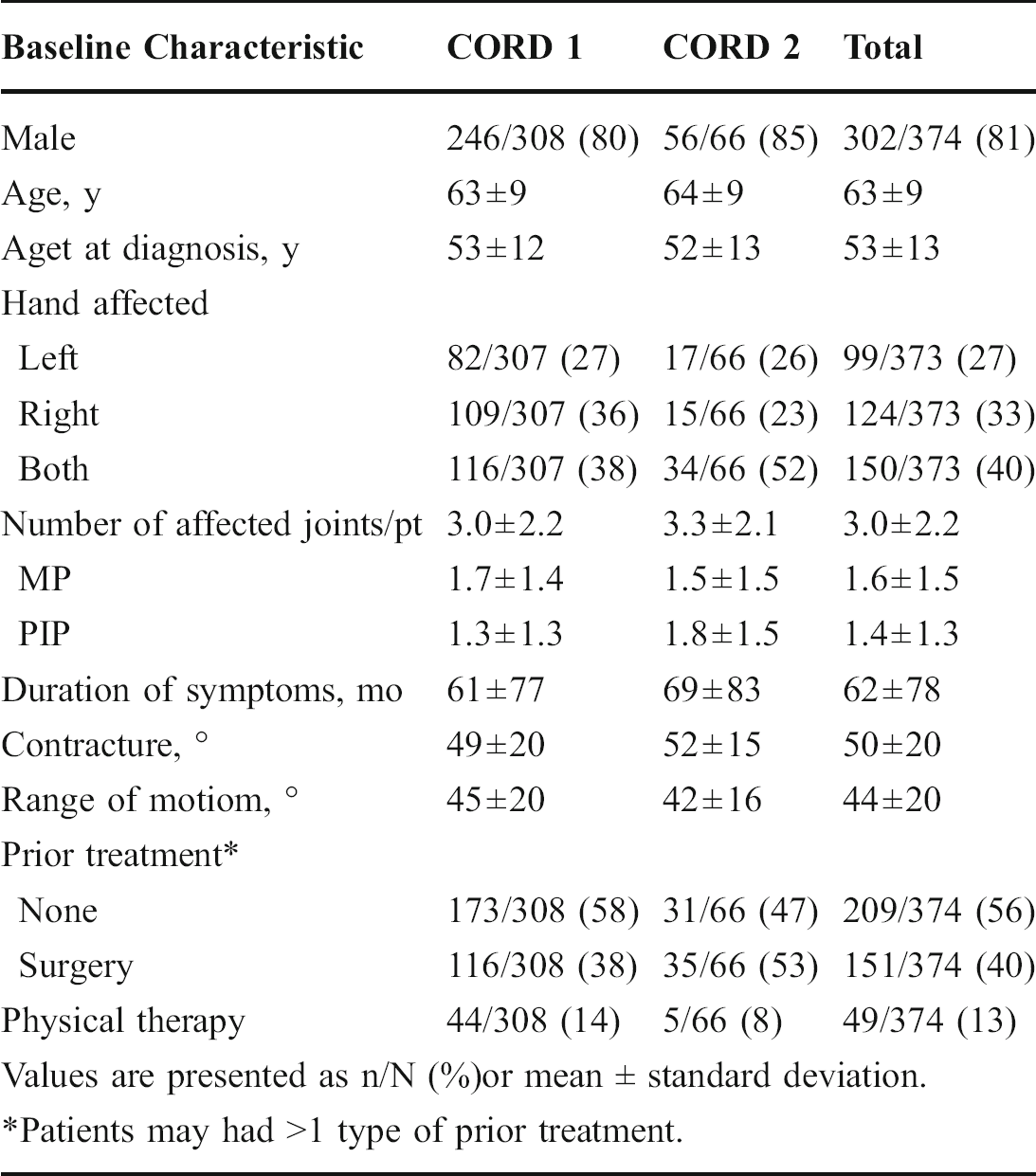
Patients may had >1 type of prior treatment.
Line Scan Diffusion Spectrum of Rat Denervated Skeletal Muscle
Institution where the work was prepared: HIratsuka City Hospital, HIratsuka City, kanagawa, Japan
Eiko Yamabe, MD1; Toshiyasu Nakamura, MD, PhD2; Yukihiko Obara, MD2; Koji Abe, MD2; (1)Hiratsuka City Hospital; (2)Keio University
Introduction
In case of peripheral nerve palsy such as radial, ulnar, and median nerve injury, denervated skeletal muscle shows increased T2 in the MR images. However, it takes certain amount of time, typically up to a week, before this change becomes visible. Since the mechanism behind this change is considered to be increased extracellular fluid (ECF), we hypothesized that the same change can be detected earlier by measuring diffusion. We measured both T2 and apparent diffusion coefficient (ADC) using peripheral nerve injury model of rats.
Materials and Methods
Total of 12 male rats were used, weighing approximately 200 g each. We made the nerve injury model by cutting the left posterior tibial nerve. At 1, 3, 5, 7, 14, 28 days after the surgery, T2 and ADC of gastrocnemius muscle, which was the target muscle of posterior tibial nerve, were measured using line scan diffusion method on a 1.5T clinical imager
Results
In the T2 weighted images, it was difficult to recognize the change until 7 days after injury. After two weeks, it became obvious in the T2 weighted images. T2 value increases gradually over two weeks, while ADC value increases right after injury, and decreases 5 days after injury. Four weeks after injury, ADC returned to normal, but T2 value stayed at high value (Fig. 1).
Discussion
Although both T2 and ADC are considered to reflect the state of extracellular fluid, our results show the clear difference between the time courses of T2 and ADC values after injury. Although clear mechanism behind these phenomena is not clear, diffusion MRI seems to be a better clinical tool for early diagnosis of peripheral nerve injury.
Conclusions
ADC increased quickly after injury, and was detectable one day after injury. Diffusion MRI can be a useful tool for early detection of peripheral nerve injury.
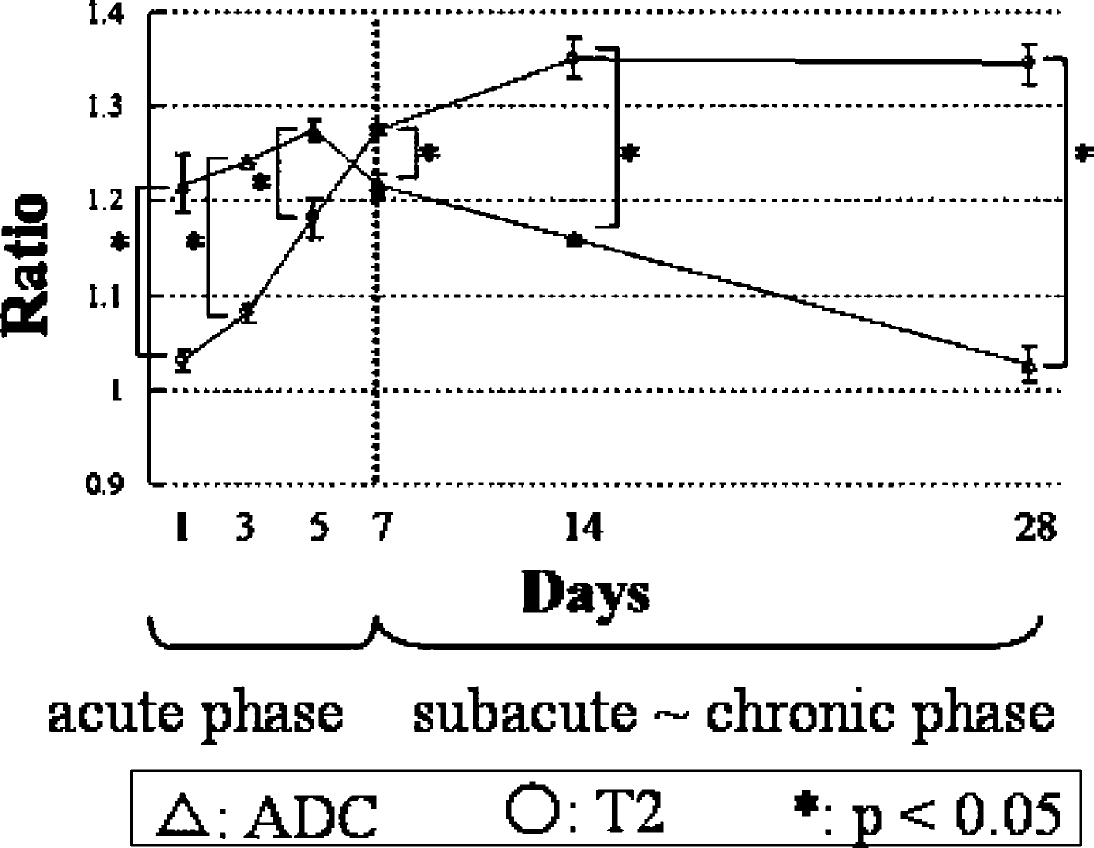
Time Courses of ADC and T2 ratios
Anatomical Features of the Pronator Quadratus muscle for the treatment of Distal Radius Fractures with a Palmar Locking Plate - Cadaveric Study
Institution where the work was prepared: Komaki City Hospital, Komaki, Japan
Naoya Takada; Komaki City Hospital
Purpose
Minimally invasive osteosynthesis (MIO) with a palmar locking plate is one of the beneficial treatments for distal radius fractures. Since 2004 we have been using this technique through 2 small skin incisions (1.5–2 cm) without dividing the pronator quadratus (PQ) muscle. However, there has been no report of the cadaveric study for this procedure. The purpose of this study is to understand the anatomical features of the PQ muscle for reduction of the fracture, plating and inserting screws.
Methods
Ten forearms of 5 fresh cadaveric specimens were used for this study. A skin incision was made on each of the volar sides of the forearms and the PQ muscle was exposed. The width (PQW) from the proximal edge of the PQ to the distal edge of it, and the distance (PRD) from the distal edge of the PQ to the joint surface of the distal radius were measured. After inserting the plate (length 86 mm) under the PQ, the distal part of the plate was held on the distal part of the radius and the proximal part of the plate was pulled off with a fixed locking sleeve from the radius. When the muscle fiber of the QP starts to tear, the distance from the volar cortex of the radius to the proximal edge of the plate was measured.
Result and Conclusion
The average PQW, PRD and PD were 34.5 mm (range 25–40 mm), 16.5 mm (range 15–20 mm) and 11.9 mm (range 25–40 mm). The length of the plate should be more than 51 mm (PQW + PRD) for this procedure to prevent damage to the PQ. For controlling the plate under the PQ it should be performed in the 12 mm area between the PQ and the volar cortex of the radius. It is important to understand the anatomical features of the Pronator Quadratus muscle and the data given above for the successful MIO and prevention of soft tissue damage.
Profit Margins for Inpatient and Outpatient Orthopedic Procedures: a Comparative Study
Institution where the work was prepared: Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
Eric Makhni; Harvard Medical School/Beth Israel Deaconness Medical Center; Charles S. Day; Harvard Medical School
Introduction
In an era of decreasing reimbursement in the health care system, cost-control becomes elevated in importance. This study sought to determine profit margins for different orthopedic procedures.
Methods
We reviewed the costs and revenues of all surgeries in the Department of Orthopedic Surgery over a one year period from July 2004–2005. All procedures were classified as one fo the following: back, foot/ankle, hand, joints, spine, sports, trauma, or “other.” Further, each surgery was designated as “inpatient” or “outpatient.” Within each subgroup, the revenue, cost (direct and indirect), and average-length-of-stay (for inpatient procedures) were noted.
Results
A total of 4117 orthopedic surgeries were performed from July 2004–2005. There were 1933 inpatient procedures and 2184 outpatient procedures. For inpatient cases, the overall average-length-of-stay was 4.6 days. This length of stay was 5.3 for spine and 4.8 each for trauma and joints cases. Hand and back cases were 2.3 and 2.7, respectively. Profit margins were highest for hand ($2,420) and lowst for joints and trauma (−$464 and −$1,244, respectively).
For outpatient procedures, the most profitable cases were those of hand/wrist ($266). Sports and foot/ankle cases were substantially less profitable ($128 and $158, respectively), and trauma cases were profitable by only $19. Spine procedures, however, had a profit margin of −$217.
Conclusions
Even though surgeon reimbursements for different orthopedic sub-specialties are pre-determined, many orthopedic procedures, when taking expenses into consideration, are not profitable for the governing hospital. Of all sub-groups, hand/wrist procedures were the most profitable in both the inpatient and outpatient setting. In the inpatient setting, increasing length-of-stay may be associated with decreased profits, but serial annual analysis is required to further elucidate this correlation.
Modeling of Upper Extremity Problems
Institution where the work was prepared: University of Louisville, Louisville, KY, USA
Steven J. McCabe, MD, MSc; Stephanie Tapp; University of Louisville
Due to the complexity and expense of randomized trials they have not been commonly applied to answer research questions in upper extremity disorders. Decision analysis can be used to model the management of medical disorders and provides an alternative when randomized trials are not possible or practical. The similarity in the general management principles of many upper extremity inflammatory disorders opens the possibility of creating a generic decision model that can be easily adapted to a large number of upper extremity conditions providing efficient analysis of management decisions. For example, trigger digit, DeQuervain's tenosynovitis, carpal tunnel syndrome, and tennis elbow can all be treated with splinting, oral medication, injection, and surgery.
Markov modeling is a commonly used technique for decision analysis that has features that make it attractive for upper extremity problems. Markov models are especially suited to evaluate recurring events that are commonly seen in upper extremity care, and the time in a state of health that is also an important feature of upper extremity care.
Our purpose was to develop a Markov Model that is comprehensive yet flexible enough to evaluate the management of upper extremity inflammatory conditions. One major objective was that the model must be easily adapted to answer multiple questions for a variety of conditions.
We created a Markov model that has the capability to consider treatments such as splinting, injection, and surgery applied in a sequential fashion, each for a variable amount of time or number of applications. The evaluation of diagnostic tests and cost-effectiveness evaluation are also possible. The model accurately portrays clinical care and can be easily adapted to represent a variety of upper extremity problems by changing the treatments available, the number of applications or time each treatment is applied, the cost, potential complications, disutility of any treatment, and the efficacy of each treatment.
Using adaptation of this basic decision analysis model, researchers can answer many questions about management of upper extremity disorders.
The Determination of Finger Laterality Dominance during Routine Activities
Institution where the work was prepared: University of Missouri, Columbia, MO, USA
Dustin Christiansen, MD; Rukmini Rednam, MD; Steven L. Henry, MD; Stephen H. Colbert, MD; Bradley A. Hubbard; University of Missouri
Background
Finger injuries and some reconstructive procedures require incisions on, or sacrifice of, a fingertip pulp. We find no objective basis for the dogma regarding the relative importance of radial and ulnar sensory surfaces of the digits. This study attempts to quantify the use (value) of each half of each digit tip during various activities.
Materials & Methods
Seventeen volunteers participated in twenty-two routine activities using paint-covered items. Standardized photographs were taken, and the degree of involvement of the radial and ulnar halves of each fingertip was calculated using a template that allowed measurement of the percentage of the half of the fingertip (hemi-pulp) that was covered in paint. Intra- and inter-digital comparisons were made to determine hemi-pulp and finger dominance.
Results
One hundred forty-five fingertip uses, or instances, were analyzed, 110 from the dominant hand (22 activities x 5 fingers), and 35 from the non-dominant (7 activities x 5 fingers). A statistically significant preference of the radial or ulnar hemi-pulp was noted in 75 instances, 51.7% of all instances examined. Rates of laterality dominance were similar between the dominant and non-dominant hands. The thumb accounted for 14 of the 75 significant instances of laterality dominance (18.67%), with 10 (71.4%) instances of ulnar predominance and 4 (28.6%) favoring the radial. Among the fingertips, the radial hemi-pulp was favored 53 (86.9%) times, and the ulnar 8 (13.1%) times. Comparison of the entire fingertip of the index, long, and ring fingers revealed a predilection for use of the more radial finger, except in the case of gripping activities, in which the more ulnar digit was consistently favored. Finally, the ten sensory surfaces of the dominant hand were ranked based on the means of the percent of the hemi-pulp used across all activities. In decreasing order, they were ulnar thumb, radial index, radial thumb, radial long, ulnar index, radial ring, radial small, ulnar long, ulnar ring, and ulnar small.
Conclusion
A significant difference in the side of the fingertip used in the activities examined occurs more than half the time. For the thumb, this is usually the ulnar surface, for the fingers, the radial. Activities requiring finer hand movements favor use of more radial digits, while strength activities favor the ulnar. The ten sensory surfaces of the digit tips can be placed in a rank order based on use, which may represent their relative importance for sensory input during the activities examined
A Case Study of the RSD Or Psudo-Gout Hand and Extremity
Institution where the work was prepared: Mayo Foundation„ Rochester, MN, USA
Celoa Sue Robinsom, BS, in, ED, Cert; Life and Leisure Hand and Physical Therapy
This is a case study of an actual experience of mine when I developed a very painful right wrist after a bump on the dorsum of the right wrist, leaving a bruise, I am on coumadin due to atrial fibulation and my INR was 3.7. The blood from the bruise intered the right wrist joint producing a great deal of pain and restriction of motion. Being I am a Hand Physical Therapist I thought I was having Reflex Sympathetic Dystrophy. This presentation is how I rehabed my right wrist, hand and upper extremity emphasizing that a therapist has to be very gentle with the resultant hand, wrist and upper exctremity in order to obtain a fully functional hand, wrist and upper extremity. I saught help from my Ambulatory Phramist, Marcel D Bizien. Pharm D, PhD at the Kasson Mayo Family Clinic, Kasson, MN, my General Practioner, Dr. Michael W. Justice MD and a physician that was a Hand Physical Medicine Specialist, Dr Keith Bengtson. MD. With their guidence and input I have been able to, so far obtain a functional right hand and upper extremity. Throught this presentation my objectives are to empower Hand Occupation and Physical Therapist with the skills to produce a funtional Hand when the hand, wrist and upper extremity are involved with RSD and /or pseudo-gout.
American Association for Hand Surgery Posters
Omental Free Tissue Transfer for Coverage of Complex Upper Extremity and Hand Defects - The Forgotten Flap
Institution where the work was prepared: Lutheran Genaral Hospital, Chicago, IL, USA
Iris A. Seitz, MD; University of Chicago; Craig S. Williams, MD; Clinical Orthopedic Surgery Northwestern University Feinberg School of Medicine; Thomas A. Wiedrich, MD; Northwestern University Medical School; Loren Schechter, MD; Lutheran General Hospital
Background
Free omental tissue transfer is one of the oldest and most versatile reconstructive options for trunk, head and neck, and extremity defect coverage. Its usefulness is due to the flap's long vascular pedicle, large vessel size, relatively thin contour, tissue flexibility and large surface area. Most series have focused on use of this tissue for trunk and head and neck reconstruction. We report our experience with omental free flap coverage of complex upper extremity defects.
Material and Methods
A retrospective analysis of 3 cases of omental free flaps for upper extremity reconstruction between 1999 and 2008 was performed. Indication, operative technique and outcome were evaluated.
Results
All patients were male; age range was 20–38 years. Indications included tissue defects due to severe trauma or infection. One patient sustained a crush injury resulting in near complete amputation of both hands requiring revascularisation. The second patient had a crush, degloving injury of the dorsal hand. The third patient had massive tissue loss of the forearm and arm due to necrotizing fasciitis and compartment syndrome. All patients had several operations including revascularisation, wound debridement and fixation of associated fractures. The mean defect size was 280 cm2 with all patients achieving complete wound coverage with omental free flap and split thickness skin graft. No flap loss or major complications were noted. One patient required additional surgery secondary to osteomyelitis 4 months after the initial injury, and a subsequent debulking procedure 9 months later. The second patient had a superficial wound infection at the abdominal donor site that healed with local care. Laparoscopic assisted omental free flap harvest was performed in all cases in conjunction with the general surgery team. Mean follow-up was 3 years.
Conclusion
The omental free flap is a valuable, often overlooked reconstructive option. The long vascular pedicle and large amount of pliable, well vascularized tissue allow the flap to be aggressively contoured to meet the needs of complex three dimensional defects. In addition, laparoscopic assisted harvest may aid with flap dissection and result in reduced donor site morbidity.
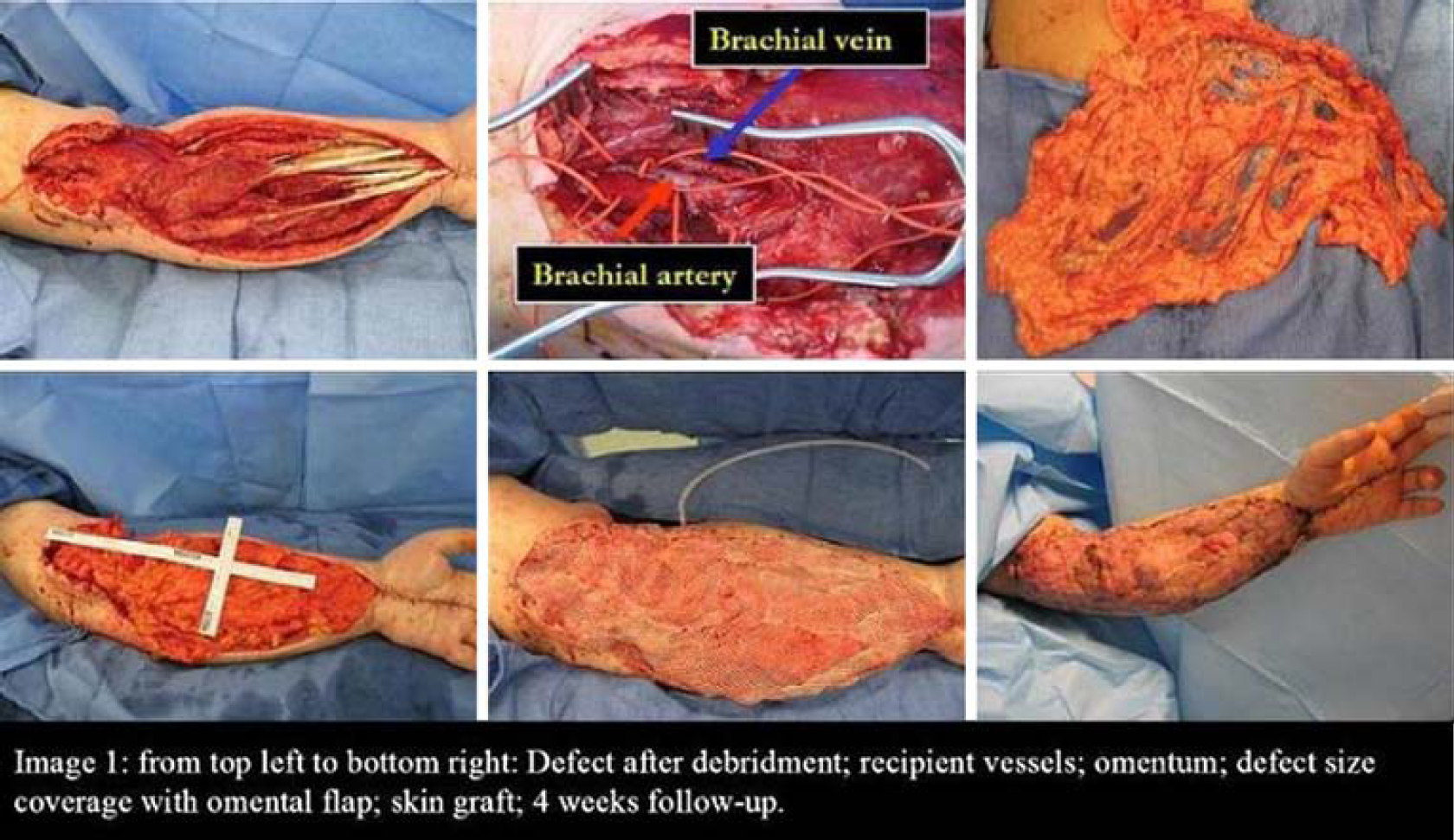
Surgical Outcome of Middle Phalanx Fractures
Institution where the work was prepared: Department of Hand Surgery, Singapore General Hospital, Singapore, Singapore
Hui Ling Chia, MRCS, MBBS; Shian Chao Tay; Beng Hoi Tan; Singapore General Hospital
Aim
There are many excellent reports on the outcome of middle phalangeal base fractures. However, there is a paucity of reports on surgical outcomes specific to fractures of the shaft and/or condyles of the middle phalanx (MP). A retrospective review was thus performed to evaluate the outcome of surgically treated middle phalangeal shaft and condylar fractures.
Method
All patients with surgery performed in 2005 and 2006 for MP fractures involving the shaft or condyles were included. Main outcome measures included clinical, functional and radiographic assessments. Using the modified Al-Qattan's classification, fracture displacement was graded before and after surgical fixation. Outcomes were classified into excellent, good and fair (modified from Barton, 1979). Patients with open or multiple fractures (on the same finger) were excluded.
Result
A total of 76 MP fractures were operated on 65 consecutive patients. Of these, 20 (26.3%) were MP fractures involving the shaft and/or condyles (3 condylar, 8 subcondylar, and 9 shaft). Moderately displaced (Type IIB) fractures were the commonest. Methods of fixation ranged from mini-plate and screws (25%), interfragmentary screw (45%), interosseous wire with kirschner wire (20%) or a combination (10%). Except for one lateral approach, all fractures were approached dorsally. Based on the modified Al-Qattan's classification, 15 of 20 fractures had excellent reduction after fixation. Mean follow-up time was 196.8 days. Seventeen of 20 fractures were followed to union with three fractures lost to follow-up before union. The average time to union was 113.5 days. The mean distal interphalangeal joint (DIPJ) motion was 40 degrees. One-third of patients were found to have an extensor lag of the DIPJ (range 15–40 degrees). All patients with extensor lag had undergone either plate or interosseous wire fixation and most of them (83.3%) of them occurred in patients with condylar and subcondylar fractures. 30% of patients had good outcomes, and 70% fair outcomes according to the modified Barton's criteria. The single patient with lateral approach with lateral plating had a fair outcome. Mean return to work was 45.9 days in our series.
Conclusion
Surgical outcome of MP fractures of the shaft or condyles was complicated by a high rate of DIPJ stiffness and extensor lag. This is despite early rehabilitation. Poor prognostic factors include condylar and subcondylar fractures, and the severity of initial fracture displacement. Fractures which were amenable to interfragmentary screw fixations alone, tended to have better outcomes.
Nerve Grafting in Upper Extremity
Institution where the work was prepared: Boston University School of Medicine, Boston, MA, USA
Harilaos T. Sakellarides, MD; Boston University School of Medicine
Purpose
To demonstrate that severe injuries of the hand can be treated by nerve grafting with very satisfactory end results.
Methods
Previously applied methods of nerve grafting had disappointing results. Over a span of 15 years, new techniques have been used, namely microscope, microsurgical techniques, and fine suture material. Evaluation of nerve repairs was according to the British method. Experimental work proved: 1) The detrimental role of tension at the suture line. 2) The deleterios effect of postoperative stretching on successful functonal recovery. 3) Regeneration axons advanced more easily through nerve grafts of 2 cm with two tension free anastomoses compared with a single suture under tension. The epineurium was the primary source of connective tissue proliferation.
Results
Motor recovery for Meidan nerve: Excellent 40%; Good 40%; Fair 20%. Ulnar nerve: Excellent 38%; Good 40%; Fair 22%. Radial nerve: Excellent 42%; Good 38%; Fair 20%.
Conclusions
Encouraging results were obtained providing certain details of the method are strectly followed.
Latissimus Dorsi Transfer for Massive Rotator Cuff Tears via an axillary approach
Institution where the work was prepared: Allegheny General Hospital, Pittsburgh, PA, USA
Bradley Palmer, MD; Mark Baratz; Allegheny General Hospital
Massive tears of the rotator cuff are a challenge for both the patient and surgeon. Treatment options include debridement (1) and repair with or without tendon graft (2, 4). When repair is not feasible the latissimus dorsi can be transferred in those patients who have good passive motion and minimal wear of the glenohumeral joint (6, 7,8,12). This article describes a technique borrowed from the plastic surgery literature to harvest the tendon using lighted retractors through a small transverse incision beneath the axilla. This technique gave adequate visualilzation to release the tendon, mobilize the muscle and pass the tendon to anterolateral incision. The comestic result is superior to previously described approaches.
Complication of Hand Extensor Tendon Lacerations in Emergency Caesarean Section
Institution where the work was prepared: Advocate Lutheran General Hospital, Park Ridge, IL, USA
Taizoon Baxamusa, MD, FACS1;; Preetha Prazad, MD2;; Henry Mangurten, MD2; (1)University of Illinois at Chicago, (2)Advocate Lutheran General Children's Hospital
Accidental fetal injury is a serious but underreported complication during caesarean delivery, particularly after one that is emergent. The most commonly documented injury is skin laceration. Though the majority of reported lacerations are superficial, a few are deep and require surgical intervention. We report a case of severe multiple extensor tendon lacerations with open metacarpophalangeal joint injuries sustained at the time of an emergency caesarean delivery that resulted in excellent functional outcome following surgical repair.
Community-acquired Methacillin-resistant Staphylococcus Aureus in the Suburban Plastic Surgery Hand Patient Population
Institution where the work was prepared: Lehigh Valley Hospital, Allentown, PA, USA
Marshall Miles, DO; Terry-Lynn Burger, RN, BSN; Robert X. Murphy Jr, MD, MS; Lehigh Valley Hospital
Introduction
Methacillin-resistant staphylococcus aureus (MRSA) is a frequent cause of infection in the postoperative patient. We observed increasing numbers of community-acquired MRSA infections in patients presenting to the hand surgery service at our suburban academic center. It is an important issue, as unsuspected community-acquired MRSA hand infections can too easily be admitted to the hospital, inadequately treated, and allow for nosocomial spread. The objective of this study was to examine the trend in the incidence of community-acquired MRSA hand infections in the plastic surgery patient, in order to sensitize practitioners to have a high index of suspicion for this entity and promote early recognition and treatment of this organism.
Methods
A multi-hospital retrospective chart review was undertaken to compare the incidence of community-acquired infections in plastic surgery hand patients from 2000 through 2007.
Results
Only two community hand MRSA infections were treated in 2000, as compared to three in 2001 and 2002, four in 2003, five in 2004, six cases in 2005, 14 in 2006, and 13 in 2007.
Conclusion
This retrospective review of infections at our institution clearly delineates an increasing number of community-acquired MRSA hand infections. The plastic/hand surgeon must be aware of the increased prevalence of this entity to adequately combat this organism and prevent prolonged hospital stays, expanded morbidity, and inflated treatment costs.
Radiographical Diagnosis of the Carpal Bone Fractures
Institution where the work was prepared: Showa University School of Medicine, Tokyo, Japan
Hirotsune Hirahara, MD; Souichirou Takigawa, MD; Katsunori Inagaki, MD; Kazutoshi Kubo, MD; Hideyo Miyaoka, MD; Showa University School of Medicine
Carpal bone fractures are common, in the majority of cases this involves scaphoid, triquetrum or hamate. Sometimes fractures can be difficult to identify due to complicated anatomical shape of the bones. Statistical analysis was performed on 252 retrospectively identified carpal bone fractures, that occurred in the past 16 years. 159 cases (63.1%) involved the scaphoid, 39 cases (15.5%) were triquetral fractures and 28 cases (11.1%) were hamate fractures. No trapezoid fractures were seen and the other carpal bones were only involved in less than 11% of cases. The authors feel that this is possibly due to the difficulty in diagnosing these fractures. However, it is possible that these fractured were misdiagnosed more often. Tomography and CT scanning are often needed. Unfortunately these constitute a greater radiation dose the patient of up to 10 times for tomography and even 250 times for CT. The cost of these techniques are also 2–3 times more and are usually added to the cost of initial plain radiographs. The authors newly developed special radiographic techniques to better identify capitate and trapezoid fractures, using conventional radiographic equipment. When compared to the technique that is currently used we saw a great improvement in idetifying the normal anatomy of these bones. This technique can easily be incorporated in standard clinical practice and should be used when there is a clinical suspicion for a capitate or trapezoid fracture. This will result in an easier diagnosis of fractures that otherwise may have remained occult and will decrease the need for other, more expensive, imaging techniques. This will have to be proven in further clinical research.
Sagittal Band Rupture in a Patient with an Anomalous Extensor Medii Proprius Tendon
Institution where the work was prepared: Geisinger Medical Center, Danville, PA, USA
John Thomas Riehl, MD; Joel Christian Klena, MD; Geisinger Medical Center
A cadaveric study of extensor medii proprius tendon incidence is presented along with a case report of sagittal band rupture involving an extensor medii proprius tendon. A review of the available literature is also presented.
A 22 year old male suffered an acute injury to the long finger of his dominant hand while playing volley-ball. The patient had persistent pain for approximately one-and-one-half years with undiagnosed ulnar extensor tendon subluxation. During operative reconstruction the patient was found to have an anomalous slip of extensor tendon to the long finger. The tear of the sagittal band was between the anomalous tendon and the extensor digitorum communis slip. The anomalous tendon was utilized as a radially-based sling to reconstruct the injured sagittal band with an excellent functional outcome.
Multidimensional Assessment of Chronic Neuropathic Pain
Institution where the work was prepared: Hand and Microsurgery Center of El Paso and UTEP, El Paso, TX, USA
Jose J. Monsivais, MD; Hand and Microsurgery Center of El Paso; Kris Robinson, PhD, FNP; University of Texas at El Paso; Diane B. Monsivais, PhD, RN; The University of Texas at El Paso
Introduction
Chronic pain affects 76.5 million people with an annual cost of $100 billion in health care, lost work productivity, and reduced income. Three out of four people with chronic pain are undertreated based on clinical practice guidelines. A frequent reason for this is the inadequate assessment of pain. Unidimensional pain (typically a scale of 0–10) assessment is the most common in most practices. This unidimensional measure does not reflect the psychosocial impact of pain or the impact on associated co-morbidities and function. Thus, the one time snapshot of assessment is notoriously inadequate and does not reflect the true impact of chronic pain.
Multidimensional assessment of pain: We suggest a three-part assessment. The first is a screening measure such as the Brief Pain Inventory (BPI) that is widely available to clinicians at no cost. Not only does the BPI assess the severity of pain, it assesses the impact on psychosocial function and activities of daily life. The BPI is a highly reliable and valid instrument. Second, is the assessment of anxiety and depression of which there are many non-proprietary tools that can be used without cost, such as the Zung depression scale. Last, is the identification of co morbidities, such as diabetes and other endocrinopathies, insomnia, deconditioning, etc., that influence and are influenced by chronic neuropathic pain.
Purpose
The purpose of this presentation is to demonstrate the use of a multidimensional assessment of pain that identifies areas amenable to treatment and enhance outcomes in terms of physical and psychosocial function, pain, and surgical results.
Methods
An exploratory, correlational research design guided the study. Through convenience sampling, we recruited 92 patients seeking pain management treatment for a neuropathic at a hand and microsurgery specialty clinic. Survey tools include the BPI, the SF-36vr2, a depression scale, and the unidimensional 1–10 pain scale. A statistician calculated descriptive statistics and conducted Pearson correlation coefficients. Post hoc analysis consisted of linear regression, ANOVA and MANOVA.
Results
The multidimensional assessment guided treatment that led to patient satisfaction and improved outcomes. We will present case studies emphasizing how the multidimensional assessment influenced treatment decisions and ultimately led to pain control and improved physical and psychosocial function.
Ganglion cysts in children: Experience at the Hospital for Sick Children
Institution where the work was prepared: Hospital for Sick Children, Toronto, ON, Canada
M. Amir Mrad, MBBS; Tatiana Cypel, MD; Ronald Zuker; University of Toronto
Purpose
Bumps and lumps are common among children. However, one bump that shouldn't be overlooked is called a ganglion cyst. A ganglion or a synovial cysts is a muscinous filled cyst which is usually found adjacent to joint capsule or tendon sheath. A common problem in adults, ganglion cysts are much less common in children. In this study, we aimed to detect the epidemiology, etiological factors, symptomatology, treatment and outcome of patients diagnosed with a ganglion cyst at The Hospital for Sick Children.
Methods
Records from the Pathology Department at The Hospital for Sick Children were searched for all cases of ganglion cyst operated between January 2000 and December 2007.
Results
Thirty-four patients were diagnosed with ganglion cysts. The mean age was 15.7 years, ranging from 5 months to 17 year old. Male:female ratio was 1:1. Solid lump was the initial presentation of the ganglion in 36% of the cases. Pain was the most common symptom to indicate surgical removal. Only 11.4% of the patients reported previous trauma history. In 70% of the cases the diagnosis was done clinically and 61% of the patients were affected on the right side of the body. The most common sites of occurrence were volar wrist (25.7%), dorsal wrist (22.8%) and the volar aspect of the base of ring (17.1%). Surgical excision was the treatment of choice for 94.2% of patients with symptomatic lesions. Only one patient (2.8%) presented with recurrence in this series.
Conclusions
Ganglion cysts are not uncommon in children. Among all symptoms that ganglions can present with, pain was the most common symptom that indicated surgery. Surgical removal was the most effective treatment for symptomatic patients, with a very low rate of recurrence.
Operative Treatment Rates for Hand Pathologies based on Diagnostic Indications and Referral Patterns
Institution where the work was prepared: Harvard Medical School/Beth Israel Deaconess Medical Center, Boston, MA, USA
Melvin Chugh Makhni, BS1; Henry Horton1; Eric Makhni1; Christine Y. Ahn2; Charles Day1; (1)Harvard Medical School/Beth Israel Deaconness Medical Center, (2)Na
Background
This study looks at the distribution of hand and wrist pathologies as well as the referral patterns to orthopaedic surgeons to see how these factors correlate with likelihood of operative management.
Methods
We performed a retrospective chart review study of 1916 consecutive adult hand and wrist cases in the orthopaedic hand clinic at our academic tertiary care medical center, from January 2005 to January 2007. Over 300,000 data points were analyzed for the 1916 cases; each individual diagnosis pertaining to the hand or wrist was assigned as a unique case. Cases were designated as traumatic (trauma <21 days prior), acute non-traumatic (symptomatic <90 days), or chronic (>90 days).
Results
Traumatic pathologies represented 10% of cases, acute cases comprised 32%, and 58% were chronic. 41% of traumatic cases underwent surgical management as compared to 35% of chronic cases (p=.04); acute pathologies were treated with surgery 29% of the time, significantly less than chronic cases (p=.03). Traumatic cases underwent surgery immediately after first recommended significantly more commonly than acute or chronic cases (p=.006, p=.009). Overall, acute and chronic surgeries were performed when recommended at similar rates. However, 95% of acute strains and fractures were operated upon when recommended as compared to only 75% of chronic cases (p=.05), while a trend regarding neurological symptoms showed 89% of patients with chronic symptoms underwent surgery when recommended versus 76% of patients with acute symptoms (p=.08). −64% of the 1916 diagnoses were from females. Cases involving females resulted in surgery 32% of the time, as compared to 39% of male cases (p=.004). -Cases were referred by primary care physicians 68% of the time and from specialists 8% of the time. 13% came from the ER, while the rest were from other referral sources. Cases referred by specialists resulted in surgery 41% of the time, as compared to only 32% of cases from primary care physicians (p=.04). 96% of cases from the emergency room resulted in surgery immediately upon recommendation, as compared to 89% of cases referred from primary care physicians (p=.02).
Discussion
A better understanding of operative management rates will allow orthopaedic surgeons to convey to patients the likelihoods that cases will result in surgery. -Increased education of primary care physicians about musculoskeletal differentials and conservative treatment options may enhance the utility of orthopaedic surgeons to patients.
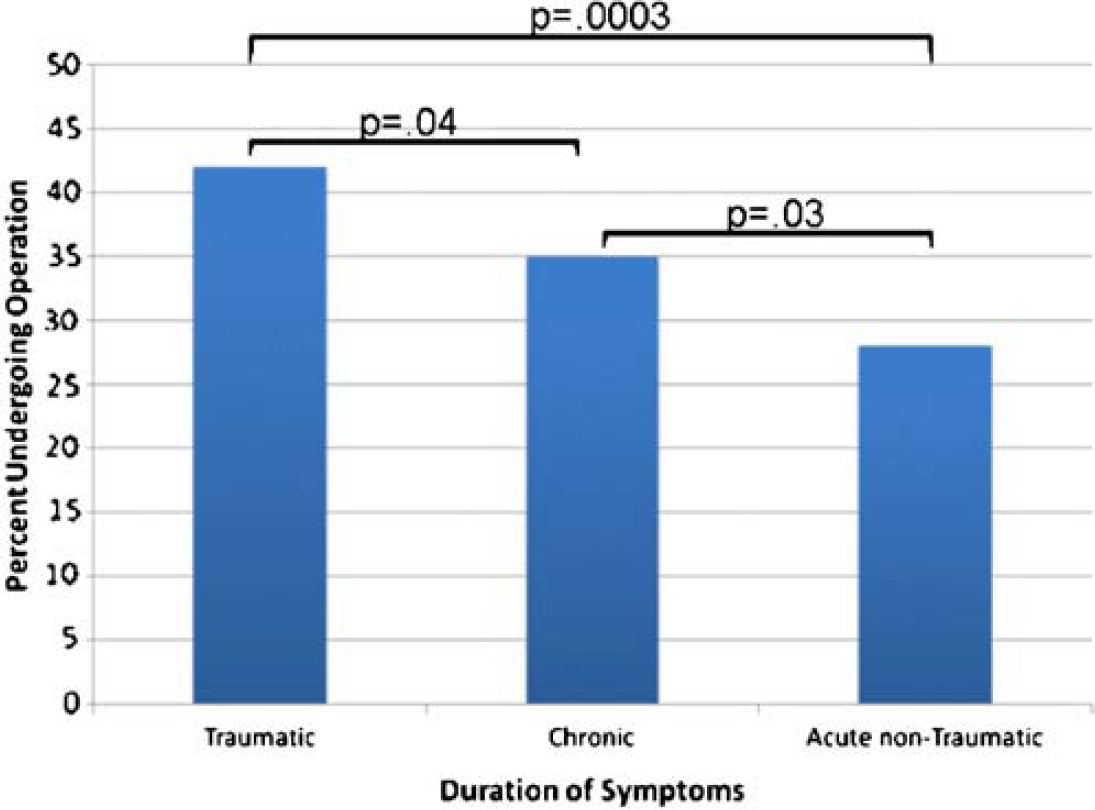
The Lateral Approach to PIPJ Ascension Arthroplasty
Institution where the work was prepared: University of Manitoba, Winnipeg MB, Canada
Ghazi Ayedh Althubaiti, MD; Kenneth Murray; Mehrdad Golian; University of Manitoba
Introduction
The dorsal approach is currently the most widely used approach for surface replacement arthroplasty of PIP joint. One of the major disadvantages of the dorsal approach is the need to divide or detach the central slip of the extensor tendon, which weakens extension and delays physiotherapy.
Purpose
Report our initial results of using the lateral approach as an alternative approach in 5 patients with 6 PIP arthroplasties.
Method
A retrospective chart review of all of our patients who had PIP joint Ascension arthroplasty who were operated on using lateral approach between 2004 and 2008.
Results
Among seven patients who underwent Ascension PIP aprthroplasties, five patients were operated on using the lateral approach. One patient had 2 adjacent joints simultaneously replaced. All of our patients were started on immediate ROM from first post-operative day. The average arc of motion was 49 degrees before surgery and 78 degrees after surgery with the average gain of 29 degrees to the arc of motion 6 weeks after surgery. Pain decreased in all patients after surgery. Two patients had joint subluxation, one of them had 2 adjacent fingers PIPJ arthroplasty that made physiotherapy and buddy taping difficult which affected the joint stability.
Conclusion
Although this is a small study, but it seems to show that lateral approach for PIPJ Ascension arthroplasty may offer the advantage of preserving the extensor tendon and starting early ROM that improves the final outcome. One of the learned lessons from this study is not to “arthroplasty” two adjacent digit hence it will affect the lateral stability of both joints and make physiotherapy and buddy taping difficult.
Learning Objectives
The audience will be introduced to the lateral approach PIPJ Ascension arthroplasty.
Never use this approach to simultaneously treat two adjacent digits.
Carpal Tunnel Syndrome: Factors Influencing Permanent Nerve Damage
Institution where the work was prepared: The Hand Center, Houston, TX, USA
Michael Fitzmaurice, MD1; Michael Brown2; Randolph Lopez, MD2; Mark Khorsand2; Andrew Lee2; Douglas Harpe2; Nur Nurbhai2; P Stephen Mahoney1; (1)Brown Hand Center; (2)The Hand Center
12,171 patients with carpal tunnel syndrome (CTS) were studied over twelve-years to determine the treatment factors that contribute to permanent nerve damage (PND). The diagnosis was established electrodiagnostically and categorized into mild, moderate, severe or profound. Various treatment modalities were studied including the Brown procedure endoscopic carpal tunnel release only, as well as various non-operative interventions: Non-steroidal anti-inflammatory drugs (NSAIDS), NSAIDS and oral steroids, and injected steroids. The incidence of resultant permanent nerve damage was further categorized as to duration of CTS subsequent to definitive electrodiagnostic confirmation of CTS. Patients with more severe CTS as well as patients with a longer duration of CTS regardless of severity had a higher incidence of PND. Those patients who underwent non-operative treatment had longer durations of symptoms and higher rates of PND. Treatment with injectable steroids prior to definitive surgical treatment resulted in a significantly higher incidence of PND.
Quantifiying Upper Extremity Replant Patients Quality of Life Using Utility Theory
Institution where the work was prepared: University of Montreal & McGill University, Montreal, QC, Canada
Oren Tessler, MD, MBA1; Genevieve Landes, MD2; Jean-Paul Brutus, MD3; Patrick Harris, MD2; H. Bruce Williams, MD1; Andreas Nikolis2; (1)McGill University; (2)Université de Montréal, Hôpital Notre-Dame; (3)Centre Hospitalier de l Université de Montréal
Purpose
Improvements in microsurgical technique have dramatically increased replant survival rates to over 90% since the initial report of upper extremity replantation in 1964. Tissue survival however, does not always correlate with useful extremity function. Measuring functional outcomes has been historically difficult because of the heterogeneity of mechanisms involved in the injury, patient factors, and associated injuries. Research in this field has thus attempted to develop increasingly specific evidence-based surgical indications. Utility theory represents a group of economic game theory-derived Health Related Quality of life assessment tools designed to help quantify uncertainty in medicine. It has been used extensively in medical decision-making over the past 40 years and has proven to be valid, reliable, and responsive for a large number of clinical conditions. This study is a novel attempt to examine the validity of utility theory measures as it applies to upper extremity replant patients.
Methods
Patients treated by the Quebec Replant Center were evaluated at a point of one year or greater from their final reconstructive procedure. Using the EuroQol, Visual Analog Scale (VAS), Time Trade-Off (TTO), and Standard Gamble (SG) questionnaires, we compare scores to the previously validated hypothetical clinical marker states of monocular and binocular blindness and to traditional replant outcome measures, including objective (ROM, sensibility, etc.), subjective (satisfaction, pain, etc..), and DASH assessments.
Results
We report that utility theory can represent a highly reliable, valid, and responsive standardized tool that can be used universally in assessing replantation results.
Discussion
It is our belief that utility theory can be developed as a simple and unified score for the multitude of surrogate measures in use to evaluate replantation outcomes.
Learning Objectives
Participants will be able to identify patients who will likely benefit from surgical replantation. Participants will be able to communicate realistic outcome expectations with patients. Participants will be able to develop more specific treatment algorithms for upper extremity replant programs.
Lunotriquetral Instability: Treatment via Dorsal Capsulodesis
Institution where the work was prepared: University of California, Davis, Sacramento, CA, USA
Robert R. Slater, MD; University of California, Davis
Introduction
Instability of the lunotriquetral (LT) joint is one source of ulnar wrist pain, and symptoms can be disabling. Traditional treatment options have focused either on indirect management via ulnar shortening osteotomies in an effort to tighten all ulnar-sided soft tissue structures or on arthrodesis of the LT joint. Ideally, it would be better to treat the pathology directly while still preserving intercarpal motion. A new technique to achieve that goal is described herein.
Methods
The wrist is approached dorsally and the dorsal intercarpal ligament (DICL) is dissected. A strip of the ligament is harvested from its distal, radial insertion, rotated on its origin off the dorsal triquetrum and then anchored to the lunate. Pin fixation maintains the intercarpal alignment post-operatively while the wrist is casted. Supervised hand therapy follows pin and cast removal.
Illustrative Case
A male custodian presented with post-traumatic ulnar-sided wrist pain. Clunking occurred as the injured wrist moved from radial to ulnar deviation. Grip strength was 75% and ROM was 90% vs. the opposite wrist. Fluoroscopy showed LT instability. At surgery, the LT disruption was confirmed arthroscopically. Open reconstruction was performed as described. The cast and K-wires were removed at 8 weeks. Outcome was excellent: return to full activities and labor without pain.
Results
Excellent results were obtained as evidenced by elimination of pain and return of grip strength to nearly match the uninjured side. ROM remained slightly decreased, particularly in flexion, but did not cause functional limitations.
Discussion
The treatment of flexible deformities of the wrist due to intercarpal ligament injuries remains controversial. Tenodeses and arthrodeses have been utilized in the past for LT instability but with problems due to stiffness and nonunion. Ulnar shortening has different complications and does not attack the pathology directly. The technique described here was developed in an effort to solve these challenging dilemmas. Favorable results suggest the technique is a valid option that warrants consideration and further investigation.
Plate Arthrodesis of the Proximal Interphalangeal Joint
Institution where the work was prepared: Medical College of Georgia, Augusta, GA, USA
Samuel Schroerlucke, MD; Simeon Marcus Fulcher, MD; Clay Spitler, MD; Medical College of Georgia
Hypothesis
Several fixation techniques have been described for proximal interphalangeal joint (PIP) arthrodesis. The literature is sparse with respect to plating and suggests that it has inferior fusion rates, is technically difficult, frequently requires hardware removal and should be reserved only for extensive PIP joint trauma. A review of all plate arthrodeses of the PIP joint at our institution reveal an excellent fusion rate, no need for future hardware removal, and a technically simple and reproducible surgical technique for all conditions requiring a PIP fusion.
Methods
Between November 2001 and June 2007, 21 patients, totaling 27 fingers, had PIP arthrodeses using plating techniques by a single surgeon. The indications were trauma with open fractures in 8 fingers, contractures of the PIP joint in 7 fingers, posttraumatic arthritis in 8 fingers, degenerative or inflammatory arthritis in 3 fingers, and salvage of a failed tension band wire arthrodesis in one patient. The technique was performed by the same surgeon (SMF) through a dorsal approach using mini-plates and screws (1.3, 1.5 or 2.0 mm). Patients were analyzed for preoperative diagnosis, age, time to fusion, need for subsequent procedures, and type and size of plate used.
Results
Twenty-six of twenty-seven (96%) PIP joints achieved fusion with an average time to union of fifty-six days. Average age of the patients was 47. The most common plate used was a 5 hole 2.0 mm plate, however, three 1.3 mm T-plates and four 6 hole 1.5 mm plates were used. The single nonunion was an acute open fracture which developed an infection requiring early hardware removal. No other finger required hardware removal.
Summary
The literature suggests that plating for PIP arthrodesis as compared to other methods has an inferior fusion rate, the necessity for frequent plate removal, and states that the procedure itself is technically demanding.
We present a 96% fusion rate (26/27) of proximal interphalangeal joints treated by plate arthrodesis. No patient required hardware removal for prominent hardware. Surgical technique is technically simple and reproducible.
Forearm Compartment Syndrome. A 5-Year Review
Institution where the work was prepared: University of Texas- Houston/Health Science Center, Houston, TX, USA
Erik Marques, MD; University of Texas- Houston
Background
Appropriate and timely treatment of upper extremity compartment syndrome is dependent on accurate diagnosis of the underlying process, including both common and infrequent etiologies. If treatment is delayed, compartment syndrome may result in tissue loss and permanent functional impairment.
Methods
A retrospective chart review was conducted on all cases of forearm compartment syndrome (CS) managed by a single plastic surgeon over a 5-year period (12/2002 to 12/2007) at an academic medical center.
Results
Fourteen extremities in eleven patients (9 male, 2 female) were diagnosed with forearm CS preoperatively. Average age was 37.5 years (range 11 months to 57 years). The most common cause was direct trauma to the affected extremity (7/14; 5 penetrating, 2 crush injuries). In the remaining extremities, the etiologies included: advanced infection; avulsion amputation of index finger at PIP joint; infiltrated antecubital intravenous line during blood transfusion (Figure 1); radial artery punctures for arterial blood gas in an anti-coagulated patient (bilateral upper extremity); and after prolonged CPR in an obtunded, ventilated patient on pressor support (bilateral upper extremity). All affected extremities underwent emergent fasciotomy. Treatment was delayed (>6 hours) in 3 patients (4 extremities), of which 2 patients (3 extremities) were unconscious; both patients developed Volkman's contractures.
Discussion
This case series highlights several important points regarding forearm CS: (1) Although forearm compartment syndrome is frequently caused by direct trauma, less common etiologies must be considered. (2) Prompt diagnosis and timely treatment are required for salvage of limb function (3) A high index of suspicion is necessary when patients are anti-coagulated and/or unconscious (ie. sedated, obtunded, ventilated). (4) We must strive to educate our referring physicians about the diagnosis, treatment, and multiple potential etiologies of upper extremity compartment syndrome.

The Rise of Methicillin Resistant Staphylococcus Aureus in Surgically Treated Hand Infections
Friedrich JB; Division of Plastic Surgery, University of Washington, Seattle, WA; Imahara SD, Division of Plastic Surgery, University of Washington, Seattle, WA
Background
Hand surgeons are commonly asked to treat bacterial infections of the hand. Recently, an alarming increase in the incidence of community-acquired methicillin-resistant Staphylococcus aureus (ca-MRSA) infections has been observed among all soft-tissues, including the hand. In addition to the inherent morbidity of hand infections, this pathogen poses further treatment and prevention challenges. Prior studies of ca-MRSA infections of the hand, specifically regarding risk factors, are small in number. The purpose of this study is to determine the change in incidence of surgically-treated ca-MRSA hand infections, and to identify risk factors associated with this pathogen.
Methods
A retrospective review of a county hospital discharge database was performed to examine all surgically-treated hand infections over a 10-year time period (1997–2007). Examined data included demographic information, social factors, nature and location of infection, surgical management, and postoperative antibiotics. The yearly incidence of ca-MRSA was calculated. Independent variables associated with ca-MRSA were determined, and were then analyzed via logistic regression to determine risk factors for ca-MRSA hand infections.
Results
There were 159 surgically-treated hand infections during the study period. Forty-eight (30%) were culture-positive for ca-MRSA. Mean age was 40 years, mean inpatient length of stay was 4.9 days, and 72% of patients were male. The yearly incidence of ca-MRSA increased over the study period (p<0.001). Variables independently associated with ca-MRSA were IV drug use (p=0.002), and second admission for a separate hand infection (p=0.005). The following were not associated with ca-MRSA: age, gender, homelessness, incarceration, other co-morbidities including HIV and diabetes mellitus, and infection type/location. Binary logistic regression identified increasing year of infection (OR 1.39, 95% CI 1.18–1.63) and IV drug use (OR 3.91, 95% CI 1.67–9.13) as significant risk factors for ca-MRSA hand infections.
Conclusions
Like ca-MRSA infections of other soft tissues, the incidence of surgically treated ca-MRSA hand infections increased with time in the last decade. Additionally, more recent infection and injection drug use were associated with an increased likelihood of ca-MRSA. Factors previously thought to be associated with this pathogen, such as homelessness, incarceration, and other co-morbidities were not found to be risks in this study. Future prospective studies are needed to further define risk factors for, and optimal treatment of ca-MRSA hand infections.