
Abstract
Even though total absence of elbow flexion in obstetric brachial plexus palsy (OBPP) is rare, weakness is a frequent problem. Numerous procedures for elbow flexion restoration in late obstetric brachial plexus palsy have been described. In this study, children with OBPP who underwent secondary reconstruction for elbow flexion restoration were studied. A retrospective review of 15 patients (16 elbows) who underwent 16 pedicled and eight free-muscle transfers for elbow flexion restoration was conducted. The mean follow-up period was 8.4±2.9 years (range, 25 months to 12.2 years). The mean age at operation (elbow surgery) was 5.4±1.9 years. The total arc of elbow motion was the result of the active elbow flexion less the flexion contracture. There was significant improvement in biceps muscle power from an average grading of 2.49±0.80 preoperatively to 3.64±0.46 postoperatively (p<0.001). Thirteen of 16 elbows (81%) achieved good and excellent results (≥M3+); and three elbows (19%) fair results (M3- or M3). The average arc of motion was significantly improved from 36°±25° preoperatively to 94°± 26° postoperatively (p<0.001). The preoperative and postoperative average elbow flexion contracture was 10.9°±8.9° and 20°±12.2°, respectively. Pedicled and/or free-muscle transfers can significantly improve elbow flexion in late obstetric brachial plexus palsy. Choice of the procedure should be individualized and determined on the basis of the type of paralysis, availability of donor muscles, previous reconstruction, and experience of the surgeon.
Introduction
In children with obstetric brachial plexus palsy (OBPP), the ability to bring the hand to the mouth is imperative. Unless elbow flexion is restored, even hands that have been spared from injury are useless [1,2]. Mobility and stability of the elbow joint are of prime importance during recreational and daily activities [3], and patients with a loss or weakness of elbow function are severely disabled. Currently, the treatment of obstetric brachial plexus palsy is focused on early brachial plexus exploration and microsurgical reconstruction [4–7]. However, when the primary reconstruction does not yield satisfactory results and in cases of delayed presentation with long denervation, timely secondary procedures can augment specific functions and lessen deformity [8–10].
Various methods to restore elbow flexion have been described. These include the Steindler elbow flexorplasty [11,12], anterior transfer of the triceps tendon [10,13,14], transfer of the pectoralis major and/or pectoralis minor [13,15,16], and bipolar transfer of the latissimus dorsi [2,16–19]. Free-muscle transfers have also been employed when local muscles are not available [10,20,21].
The purpose of this article is to present the results of secondary reconstruction for elbow flexion restoration in late obstetric brachial plexus palsy. A retrospective review of 15 patients (16 elbows) with obstetric brachial plexus palsy who underwent 24 pedicled and free-muscle transfers for elbow flexion restoration is presented.
The current study was conducted under the guidelines and the approval of the Institutional Review Board committee of Eastern Virginia Medical School.
Patients and Methods
Patient Population
A retrospective review of 15 consecutive patients (16 elbows) who underwent secondary elbow flexion reconstruction for obstetrical brachial plexus palsy was conducted. These procedures were performed between October of 1984 and March of 2002. Evaluation of the results was carried out in all 16 reconstructed elbows. All patients had a minimum follow-up of 2 years after elbow flexion reconstruction. The mean follow-up period was 8.4±2.9 years (range, 25 months to 12.2 years).
The right upper extremity was involved in nine cases, and the left upper extremity was involved in seven cases. There were six male and nine female patients, for a total of 16 elbows. One female patient presented with bilateral palsy and underwent secondary reconstruction for elbow flexion in both extremities. All children used their uninjured limb as the dominant limb. Most of the patients had concomitant procedures to improve shoulder, forearm, and hand function. The mean age at operation (elbow surgery) was 5.4±1.9 years (range, 3 to 8.9 years). Characteristics of the patients are provided in Table 1.
Patients' demographics.
In the total population (16 elbows), 6% of the cases were diagnosed with classic Erb palsy (C5 and C6); 25% with C5, C6, and C7 palsy; and 69% with global palsy (C5 to T1) (Table 2). Secondary reconstruction was performed in 11 elbows (group A) that had previously undergone primary plexus reconstruction and in five elbows (group B), that had no prior nerve surgery, as the only procedure for improvement of elbow flexion function. Mean age in group A was 4.9±1.8 years, while in group B was 6.6±1.5 years (Table 2). In short, previous nerve reconstruction in group A consisted of the following: the musculocutaneous nerve was reconstructed from intraplexus (four elbows), extraplexus donors (three elbows), or both intraplexus and extraplexus donors (two elbows); in two elbows, the upper trunk underwent neurolysis as there was conductivity across the neuroma-in-continuity. Extraplexus donors included motor donors of the cervical plexus, the spinal accessory nerve, and the contralateral C7. Poor prognostic factors in these cases were the long time interval between birth and primary nerve reconstruction (average, 23 months), length of the nerve graft, and type of paralysis (eight of 11 elbows had global palsy [C5–T1]).
Type of brachial plexus injury and type of reconstruction.
Patient Assessment
All patients were evaluated according to a standard preoperative and postoperative protocol. The British Medical Research Council grading system, further modified by Terzis et al. [22] with intermediate grades of (+) and (-), was used for the assessment of the motor power of the biceps muscle. The postoperative results were assessed as follows: a poor result was a grade of M0 to M2; M2+ to M3 was fair result; M3+ to M4- indicated a good result; and M4 to M5- was excellent result [23].
The range of active elbow flexion was measured, with a goniometer, against gravity as well as the degree of elbow flexion contracture (extension deficit). The total arc of motion was the result of the active elbow flexion less the flexion contracture. The results are expressed as average ±SD. Preoperatively, all patients had plain radiographs of the affected elbow joint for possible joint deformities such as dislocation of the elbow joint.
Type of Secondary Reconstructions
The patients received a combination of pedicled muscle and/or free-muscle transfers for weak or absent elbow flexion. Sixteen pedicled muscle transfers and eight free-muscle transfers were performed, for a total of 24 muscle transfers (Table 3).
Type of secondary reconstructions performed in 15 patients (16 elbows).
Pedicled Muscle Transfers (n=16)
Pectoralis Major Transfer (n=3) The pectoralis major muscle, with (n=2) or without (n=1) the pectoralis minor, has been transferred as a pedicle muscle flap for elbow flexion restoration in three elbows. The lower part of the pectoralis major (sternocostal part) was transferred from its origin and raised with its nerve and blood supply intact. Careful dissection was performed, since the neurovascular pedicle of the muscle could be easily avulsed. Its humerus insertion was anchored to the distal clavicle, and the sternocostal origin was transferred to the biceps tendon using a strip of fascia lata as a tendon graft.
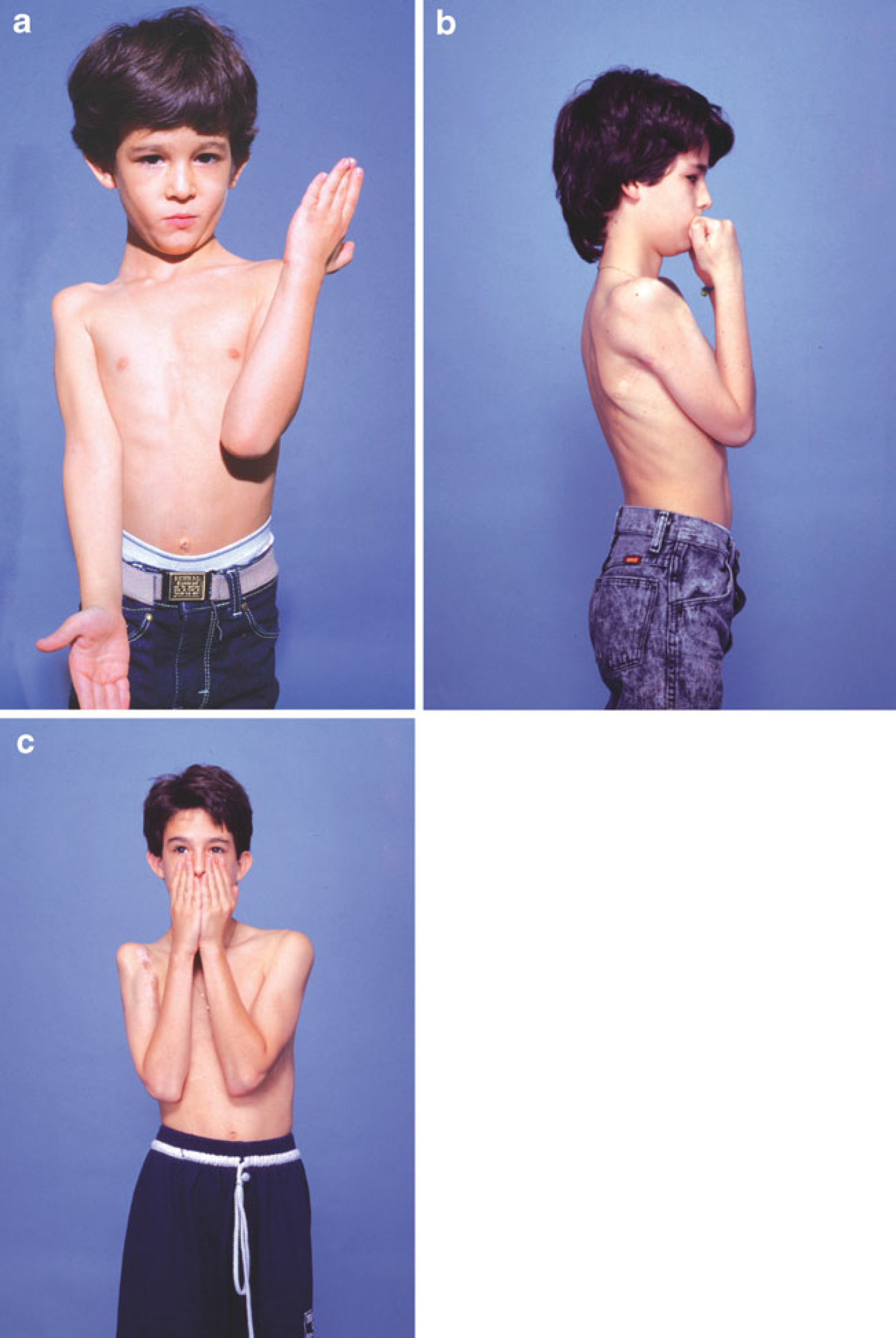
Pectoralis Minor Transfer (n=7) The pectoralis minor has been used to supplement elbow flexion in seven elbows. As mentioned, in two elbows it was transferred along with the pectoralis major. Monopolar transfer of the pectoralis minor was performed. The muscle origin was mobilized along with the fascia over the ribs to get extra length and then transferred laterally and anchored on the biceps (Fig. 1).
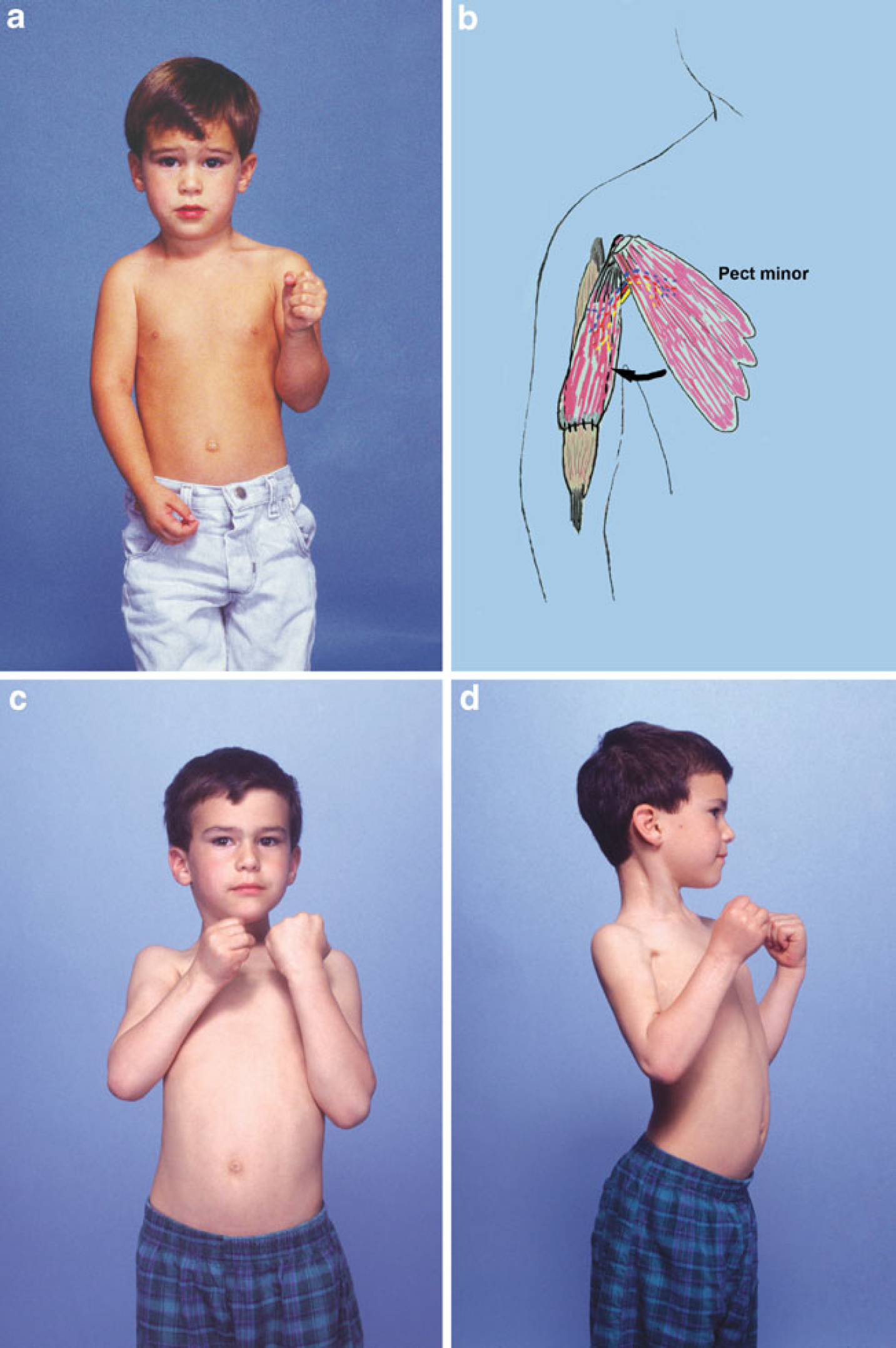
A boy with right global palsy underwent primary nerve reconstruction at 6 months of age. At 3.1 years of age, he presented limited elbow flexion (M3;
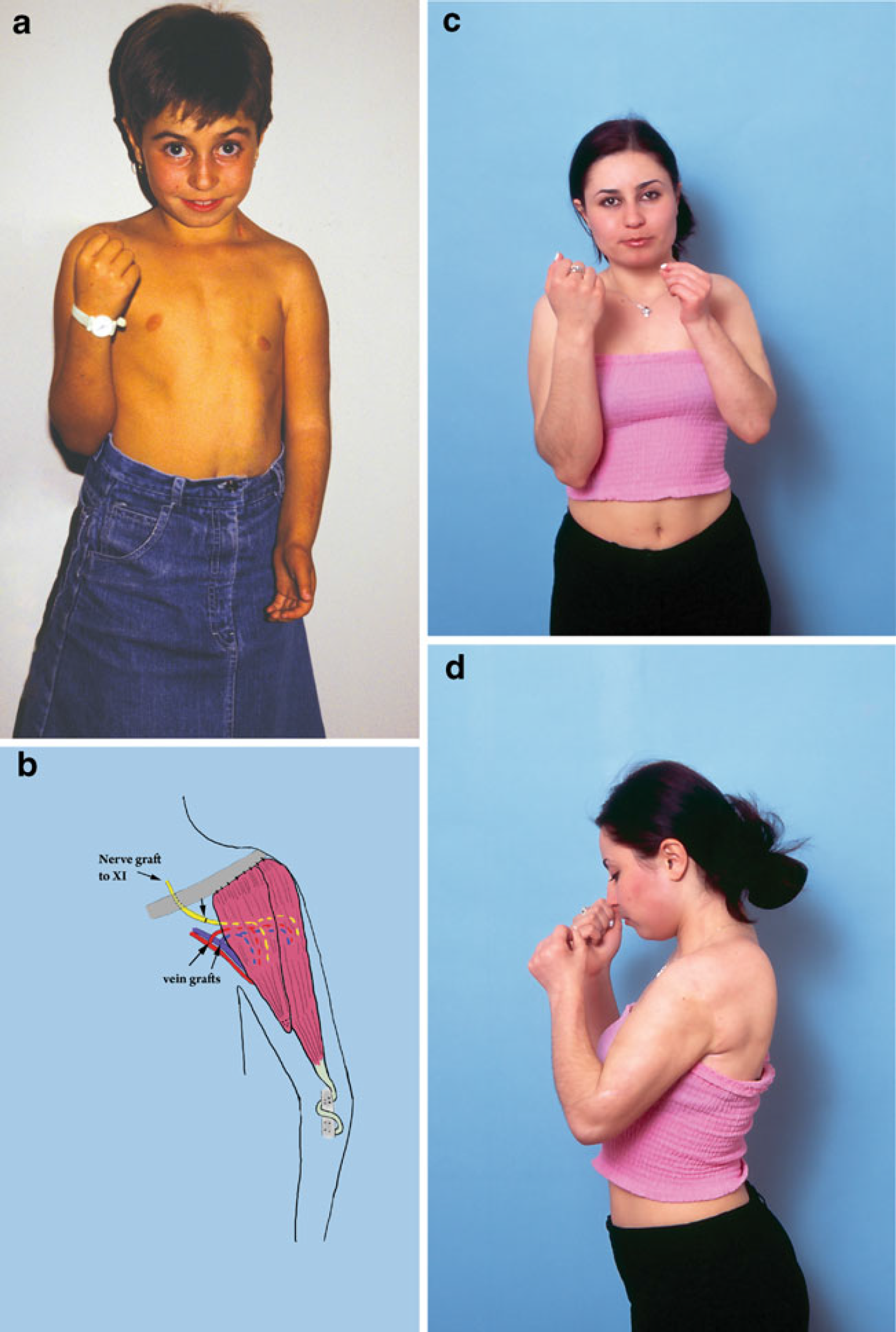
Latissimus Dorsi Transfer (n=4) The ipsilateral latissimus dorsi muscle was transferred as a myocutaneous pedicled flap in four elbows (Fig. 2). A large enough pocket was created to fit the muscle in the anteriomedial aspect of the arm, and then the muscle was harvested from its origin to its insertion, based on its neurovascular pedicle. The neurovascular bundle, readily identified entering the undersurface of the muscle in the proximal third, was carefully preserved. Once the entire muscle had been freed, the tendinous insertion to the humerus was anchored proximally to the lateral clavicle and coracoid process. The origin of the muscle was “wrapped” to form a “tube” with a strip of fascia lata and was anchored distally to the radial tuberosity with compression screws.
A 5.3-year-old boy with right upper plexus palsy presented with weak elbow flexion (M3-;
Steindler Flexorplasty (n=2) A modified Steindler flexorplasty was performed in two elbows. Proximal advancement of the forearm flexor mass was performed. Both the ulnar and median nerves were identified and mobilized, taking care to preserve the motor branches to the flexor carpi ulnaris and pronator teres. The flexor mass was elevated with a small periosteal flap, mobilized, and anchored with compression screws on the distal third of the humerus (moved 5 to 7 cm proximally).
Free-Muscle Transfers (n=8)
When local muscle donors were unavailable, then free-muscle transfers were employed to augment elbow flexion restoration. The contralateral latissimus dorsi (n=2), the adductor longus (n=1), and the gracilis muscle (n=5) were transferred as free vascularized innervated muscle flaps to restore elbow flexion function (Fig. 3). The proximal end of the free-muscle transplant was anchored proximally to the anterolateral acromion, and the distal end was sutured to the distal biceps tendon or radial tuberosity. The free muscles were neurotized by either the ipsilateral intercostal nerves (n=4) or by banked nerve grafts from the distal spinal accessory nerve (n=4; Table 4). Arterial anastomoses and venous outflow were carried out in an end-to-side fashion to the brachial artery and vein, respectively, in all free transfers.
A girl presented at 8.9 years of age with a diagnosis of left global brachial plexus palsy. She exhibited inadequate elbow flexion (M3;
Preoperative and postoperative data.
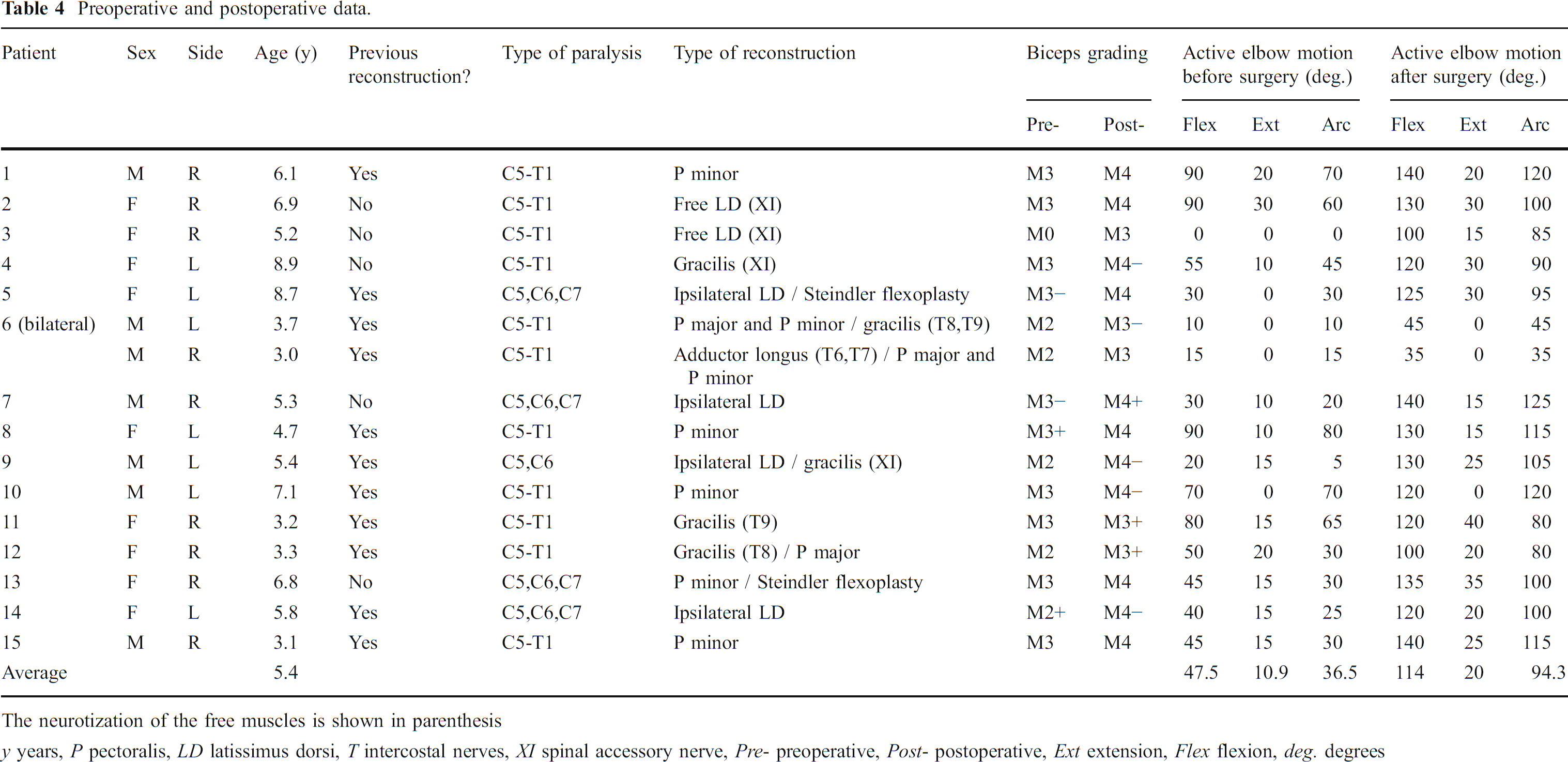
The neurotization of the free muscles is shown in parenthesis
y years, P pectoralis, LD latissimus dorsi, T intercostal nerves, XL spinal accessory nerve, Pre- preoperative, Post- postoperative, Ext extension, Flex flexion, deg. degrees
Postoperative Care
At the completion of surgery and before extubation, a custom-made brace is applied to the patient with the shoulder in 45° of anterior flexion and the elbow flexed to 90°. The upper extremity was immobilized in the brace for 6 weeks. After this period, the brace was removed, and physical therapy was directed. This involved ultrasound and gentle massage on the surgery sites and passive range of motion in all the joints of the upper extremity. Slow-pulse stimulation was initiated at 6 weeks with a portable device that the parents were instructed to use for approximately 6 h every day. The first follow-up visit was arranged at 6 weeks after surgery and then every 6 months. The parents were instructed to monitor any early contraction in cases of free-muscle transfer and to document specific dates of elbow flexion recovery. Instructions were given to the parents and patients to try to activate and produce successful contraction by replicating the function of the donor nerve. Written instructions were also given and were followed by direct communication with the physiotherapist that was involved with the postoperative rehabilitation of each patient.
Statistical Analysis
Comparisons between preoperative and postoperative values were carried out using Wilcoxon signed-rank test for the biceps muscle grading data and paired t test for the degrees of flexion data. The small sample size and the combination of pedicled and free-muscle transfers in some elbows limited the power of our study to detect differences among the various transfer groups. All the analysis was performed in SAS 9.1.3 (Cary, NC, USA). Two-tailed p values of <0.05 were considered to be significant.
Results
Overall, the 16 elbows had improvement in their elbow function following the various secondary procedures. There was significant improvement in biceps muscle power from an average grading of 2.49±0.80 preoperatively to 3.64±0.46 postoperatively (Wilcoxon signed-rank test, p<0.001). Seven elbows (44%) achieved excellent results (M4 or M4+), six elbows (38%) good results (M3+ or M4-), and three elbows (19%) fair results (M3- or M3).
The average arc of motion was significantly improved from 36°±25° preoperatively to 94°±26° postoperatively (paired t test, p<0.001). The preoperative and postoperative average elbow flexion contracture was 10.9°±8.9° and 20°±12.2°, respectively (p<0.001). Detailed preoperative and postoperative data for all patients are presented in Table 4.
An improvement was observed after palliative surgery, irrespective of prior nerve reconstruction (group A, n=11) or late presentation (group B, n=5). Average biceps muscle power was 3.57±0.45 in group A and 3.79±0.5 in group B, but the difference was not significant (Mann–Whitney U test, p=0.36).
All procedures were completed uneventfully. No complications were seen in this series. No infections, hematomas, or muscle failures were developed postoperatively.
Discussion
Elbow flexion is generally the result of the combined action of the primary elbow flexors, the biceps, and brachialis muscles. Although the elbow can be partially flexed by accessory elbow flexors (brachioradialis and extensor carpi radialis longus), weakness of the biceps power results in a significant functional impairment; the patient cannot bring the hand to the mouth for feeding, buttoning a shirt, or combing the hair [2]. Elbow flexion is frequently absent or diminished in obstetrical brachial plexus palsy involving the musculocutaneous nerve (C5 and C6 nerve roots). Children with typical C5–C6 palsies and children with global palsy without recovery of C5–C6 function develop weak elbow flexion and supination [13]. This is because they lack power in the biceps. In late cases, they may develop pronation–flexion contractures that may even dislocate their radial heads posteriorly [24]. The surgeons should perform radiologic studies that would alert them to the presence of joint deformities. In such cases, timely orthopedic consultation can be invaluable in planning a reconstructive strategy.
Fortunately, the majority of the patients with OBPP do regain adequate strong elbow flexion and range of motion [2,6,7,20]. Those with inadequate elbow flexion and the late cases are good candidates for muscle transfers. Secondary procedures are performed when patients have reached a plateau in their rehabilitative efforts, irrespective of any previous treatments [25].
The latissimus dorsi is widely used as a pedicled muscle flap for elbow flexion reconstruction [2,8,16–19]. Favorable results were obtained in most series. Botte and Wood [16] reported a mean antigravity elbow flexion of 87° in five cases, while Marshall et al. [17] reported an average range of 102° in six cases. Bennett and Allan [26] stated that, although transfer of the latissimus dorsi is technically demanding and requires precise knowledge of the anatomy of the muscle, the results are superior to that seen with other techniques. In our series, the four patients who underwent pedicled latissimus dorsi transfer achieved an average biceps grading of 3.91, an average active elbow flexion of 128°, and an average arc of motion of 106° (range, 95°–125°).
Other surgical options include the transfer of the pectoralis major and/or minor [13,15–17] and Steindler flexoplasty [11–13]. Pectoralis major transfers can be disappointing in adults [17], while it can give reliable results in children [15]. Atkins et al. [15] reported that a total pectoralis major transfer in children suffering from paralysis of elbow flexion due to arthrogryposis or to trauma has given good results in six out of seven patients. In arthrogrypotic children, the functional results were deteriorating due to a gradual increase in the flexion deformity in the operated elbow and a decrease in the effective arc of flexion [27]. In our series, transfers of pectoralis major and/or minor were performed in most cases in combination with free-muscle transfers (three elbows) because they were not strong enough to substitute for adequate biceps function. To produce desirable results, the sternocostal part of the pectoralis major muscle should have adequate strength and the elbow joint a full passive range of motion. The pectoralis minor muscle was not strong enough to substitute for the biceps in cases with total absence of elbow flexion.
Another procedure is the anterior transfer of the triceps tendon insertion [10,13,14], which provides better strength of elbow flexion than the Steindler transfer does but leaves the patient unable to actively extend the elbow which is necessary for a wide range of daily activities [2,26]. Chuang et al. [10] abandoned this procedure since their patients developed severe flexion contracture of the elbow with loss of elbow extension. Thus, the sacrifice of a functioning triceps, especially in late cases of obstetric paralysis, is rarely justified.
Functioning free-muscle transplantation has become a reconstructive option in cases of delayed patient presentation with long denervation time or in cases with multiple-root avulsions. Furthermore, this technique can be extremely useful when primary reconstruction of the biceps has not yielded satisfactory results. To be used as a biceps substitute, the muscle must have adequate strength and a suitable contractile force to flex the elbow. Free vascularized transfer of the contralateral latissimus dorsi and the gracilis muscles were used in our series. It is important to plan these procedures ahead of time by placing banked nerves at the distal arm. Reinnervation was performed by either the intercostal nerves or banked nerve grafts from the distal spinal accessory nerve. Of great importance is the training of the patient and physical therapy in all aspects of the new neurotizations [4]. If intercostal nerves have been used to reinnervate the free muscle, the patient needs to perform the Valsalva maneuver while attempting to flex the elbow to achieve stronger contraction. Following such neurotizations in children, central nervous system neurons exhibit extreme plasticity, and the patient quickly embraces the new nerve pathways [28].
In the current series, due to the greater power demands needed for elbow flexion, the free latissimus dorsi transfer was a more effective substitute than the free gracilis transfer. However, due to the small sample size and the combination of pedicled and free-muscle transfers in some elbows, no statistical analysis could be performed. Donor morbidity of the normal upper extremity and a big scar are the main drawbacks of the latissimus dorsi transfer in children. Gilbert et al. [29] reported that active elbow flexion has been achieved in nearly 60% of their cases treated with free gracilis transfer, while Chung et al. [30] showed that free-muscle transplantation for biceps replacement powered by intercostal nerves has been successful in achieving adequate elbow flexion in 78% of their patients.
However, using the spinal accessory nerve in four elbows, strength of only M2+ was achieved [30]. In our series, good results (M3+ or M4-) with free-muscle transfers (eight elbows) were seen in five (63%) patients. No significant difference was observed between intercostal nerves and the distal spinal accessory neurotizations.
Atraumatic operative technique and postoperative care are equally important factors in achieving success after muscle transfers [31]. Of great importance is the condition of the corresponding elbow joint; thus, before any muscle transfer, the elbow joint needs to be free of contracture, otherwise one could end up with a strong muscle unit but with limited joint excursion. In this series, a tendency for increased flexion contracture after various muscle transfers was observed; and the difference was statistically significant. However, in only two elbows, the flexion contracture was more than 35°, with an average contracture of 20°± 12.2° postoperatively in all elbows.
Conclusion
Numerous procedures for elbow flexion restoration in late obstetric brachial plexus palsy have been described. Elbow flexion weakness can be treated with local muscle transfers; when no local donors are available, free vascularized muscle transfers are indicated. Choice of the procedure should be individualized and determined on the basis of the type of paralysis, availability of donor muscles, previous reconstruction, and experience of the surgeon. Further comparative studies and expertise in this area are needed to identify the most successful treatment algorithm.