
Abstract
A latissimus dorsi muscle flap was used to simultaneously resurface the dorsal index, middle, and ring fingers of a 10-year-old child who had sustained a severe abrasion burn from a go-kart injury. Rather than performing multiple individual flaps, or a single flap in which a secondary division procedure would have been needed, the flap was divided into three vascular territories, permitting a single-stage reconstruction. Use of this strategy minimized the need for prolonged rehabilitation, and the functional outcome was optimized.
Keywords
Case Report
A 10-year-old right-hand-dominant boy from an outlying region sustained a devastating abrasion injury to the right hand during a go-kart accident (Fig. 1). There was a loss of the dorsal half of the bones of the index and middle fingers from the metacarpophalangeal joint to the fingertips. The dorsal portions of the ring finger proximal interphalangeal joint and extensor tendon were also exposed. The dorsum of the hand sustained deep partial thickness abrasion injuries proximal to the metacarpophalangeal joints. The volar halves of the digits were sensate and well perfused. Debridements were carried out on the day of injury and on postinjury day 1. On postinjury day 2, the dorsal full thickness burn injury was debrided, resulting in a wound involving most of the dorsum of the hand, the index and middle fingers, and the dorsum of the ring finger proximal to the distal interphalangeal joint. DIP chondrodeses were performed on the index and middle fingers, preserving the physes. Fractures of the proximal phalanx and metacarpal bones of the thumb were pinned. The intrinsic tendons were dorsally sutured over the proximal phalanges. A serratus muscle flap was originally planned, with one slip of muscle intended for coverage of each of the three affected fingers. However, the vascular pedicles of the serratus muscle were inadequate (there was no serratus branch artery from the thoracodorsal system, and the lateral thoracic artery was of inadequate caliber). Therefore, a latissimus dorsi muscle flap was harvested and transferred to the hand. An end to end arterial anastomosis was performed with 10-0 nylon from the thoracodorsal artery to the dorsal branch of the radial artery. A venous anastomosis was performed from the thoracodorsal vein to a branch of the cephalic vein. The muscle was then trans-illuminated with the overhead operating room lights, allowing the vessels within the flap to be visualized and protected. The muscle was split into three “lobes” with curved Mayo scissors, protecting the vascular supply. A Doppler probe confirmed flow within the split distal parts of the flap during and after the splitting. The “trilobe” flap was then inset and extensively trimmed further to reduce its width and thickness. A meshed split thickness skin graft was placed (Fig. 2). He began a range of motion therapy on postoperative day 8. The muscle flap and skin graft healed uneventfully. Following rehabilitation, he was pain-free and his range of motion allowed him to perform self care activities without difficulty (Figs. 3 and 4; also see Supplementary Digital Content Video

Preoperative image demonstrating loss of the dorsal half of the bones of the index and middle fingers from the metacarpophalangeal joint to the fingertips. The dorsal portions of the ring finger proximal interphalangeal joint and extensor tendon were exposed. Written informed consent was obtained from the patient's family to publish all images and videos presented in this work.

Following completion of the ‘trilobe’ latissimus flap with a split thickness skin graft.

Six-month postoperative view of dorsum of hand demonstrating digital extension.

Six-month postoperative view demonstrating digital flexion.
Discussion
Potential alternatives could have included a fasciocutaneous flap [3], fascial flap, omental flap, or use of other flat skeletal muscles. Additionally, a “syndactylized” flap could have been used, with a second stage planned for division >and inset. In the case presented, a “trilobe” latissimus muscle flap was used to reconstruct the dorsal surfaces of three adjacent digits. A single-stage reconstruction helped optimize his outcome by streamlining his rehabilitation. Since travel was a major issue for this family, avoiding multiple surgical procedures was advantageous. A “bilobe” latissimus muscle flap has been previously reported [4]. Partial latissimus dorsi muscle flaps have been used for free tissue transfer based on either the medial or lateral branches of the thoracodorsal artery and vein (Fig. 5). Both the medial and lateral branches of the thoracodorsal vessels give rise to smaller longitudinal branches that may also be used for smaller subunits of these partial latissimus dorsi muscle flaps [1, 2]. To date, there have been no reports of a “trilobe” latissimus dorsi muscle flap for hand reconstruction. The approach in this case, therefore, represents a refinement of the principle behind the partial latissimus dorsi muscle flap.
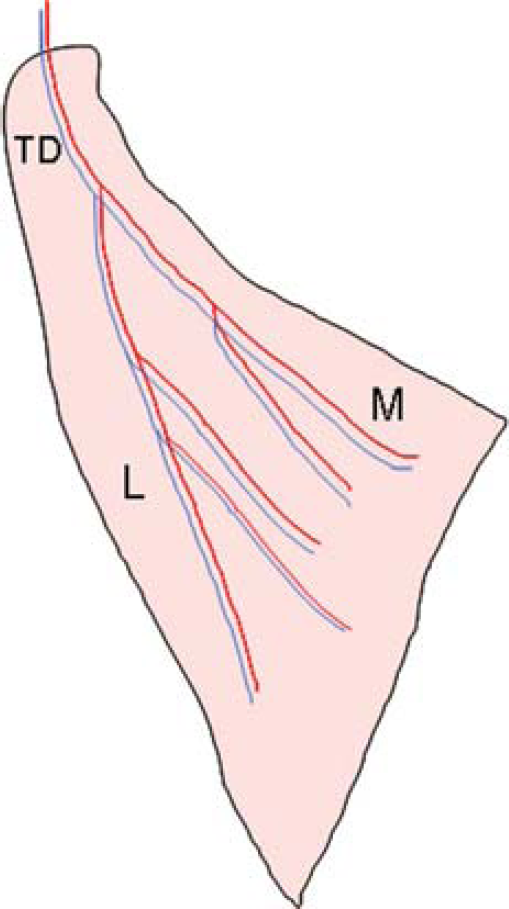
Diagram of vascular supply of the latissimus dorsi muscle free flap. The thoracodorsal artery and vein (TD) divide into medial (M) and lateral (L) branches, each of which give rise to smaller vessels that run parallel to the medial and lateral branches. Because the branches run parallel to the medial and lateral branches, the muscle can be split longitudinally into multiple subunits.
Footnotes
none.