
Abstract
Transection of the transverse carpal ligament (TCL) for carpal tunnel syndrome is commonly performed, yet actual knowledge of TCL morphology is rudimentary and the anatomical terminology is inconsistently used. The purpose of this study was to perform a morphological analysis of the TCL, to redefine the anatomical terminology concerning the TCL and surrounding structures, and to evaluate any correlation between external, measurable hand dimensions, and TCL dimensions. A silicone casting technique and digitization were employed to measure the morphology of the TCL in cadaveric specimens and to construct a three-dimensional TCL model. The TCL was the thickest distally at the midline and ulnar segments and the thickest proximally at the radial segment. External hand dimensions did not significantly correlate with TCL dimensions. The TCL thickness distribution is variable along the radioulnar axis. The thickness of the TCL was 2.1±0.8 mm, ranging from 1.3 to 3.0 mm.
Introduction
Carpal tunnel syndrome (CTS) is one of the most common entrapment neuropathies of the upper extremity, yet the exact anatomic definition of the transverse carpal ligament (TCL) and its associated anatomy remains inconsistently reported [1,2,4–7]. Knowledge of the TCL and its associated anatomy is necessary not only for the performance of a carpal tunnel release but also to facilitate further investigation into the etiology as well as alternative treatments. The terms flexor retinaculum (FR) and TCL have often been used interchangeably in the literature and have not always referred to the same structure or set of structures [4,6]. The FR is a large fascial plane on the volar aspect of the wrist, deep to the palmar fascia, that serves as the roof of the carpal tunnel [1]. It consists of three main portions: proximal, middle, and distal [1,2,5].
The proximal portion of the FR consists of the distal continuation of the antebrachial fascia [1] and can be distinguished from the middle portion of the FR based on fiber direction and thickness. The fibers of the antebrachial fascia are oriented longitudinally, and it is thinner than the TCL by a factor of 10 [2]. The antebrachial fascia has at times been considered the proximal portion of the TCL [3]. The middle portion of the FR consists of the TCL, which has at times been referred to as the FR in the literature [4,6]. It has four bony attachments—the ridge of the trapezium, the tubercle of the scaphoid, the pisiform, and the hook of the hamate [1,2,5,6]. Isogai et al. [3] performed an anatomical study of the TCL and observed specific variations in fiber orientation. The authors reported that the TCL consists of a superficial and deep layer and that its fibers are primarily arranged transversely, with some oblique components as well, although the specific arrangement can differ. The distal portion of the FR is an aponeurosis which courses transversely between the thenar and hypothenar musculature [1,2,5,6]. Cobb et al. [2] described this portion, as well as all portions, as being continuous. Tanabe and Okutsu [6] stated that the TCL and aponeurosis were separated by a layer of adipose tissue, used the term FR to refer to the TCL, and referred to the distal aponeurosis as the transverse fibers.
TCL morphology has been studied with varying techniques and outcomes. Cobb et al. [2] performed photographic measurements of both the TCL and distal aponeurosis together and reported that the thickness ranged from 0.8 to 2.5 mm. These authors also reported a mean length of the combined TCL and distal aponeurosis of 21.7 mm, ranging from 12 to 30 mm. Tanzer [7] identified thicknesses along the radioulnar midline of the TCL ranging from 1.5 to 2.5 mm along the proximal edge, 2.5 to 6.0 mm at the midpoint, and 2.5 to 6.0 mm at the distal edge.
While these studies provide information regarding the TCL dimensions, the TCL was not isolated from other portions of the FR and there was no information as to how the thickness changed in different regions of the TCL. A morphological analysis of TCL anatomy using advanced methodology is necessary to provide a more complete picture of its anatomical significance. In addition, no previous study has reported on the correlation between TCL dimensions and external hand morphology. If a readily measurable external hand parameter did correlate with TCL dimensions, then hand parameters may be used to correlate TCL thickness and its pathologic states.
The purpose of this study was to perform an advanced morphological analysis of the TCL through a novel silicone casting and digitization method. Additional purposes were to further clarify the anatomy of the flexor retinaculum and to identify correlations between hand and TCL dimensions.
Materials and Methods
Ten fresh-frozen human cadaveric specimens disarticulated at the elbow, five male and five female, were utilized. Exclusion criteria for specimens were excessively small or large body mass index (BMI; <20 or >30 kg/m2); previous surgery or congenital deformity of the hand/wrist/forearm; or history of musculoskeletal, nervous, and connective tissue disorders, especially CTS.
Initially, measurements of wrist width (radial–ulnar), depth (anterior–posterior), and circumference were taken at the distal wrist crease using calipers; the widest or deepest point of the wrist at the distal wrist crease was used. Measurements of palm width (radial–ulnar), depth (anterior–posterior), and circumference were taken at the level of the metacarpal heads using calipers. Again, the widest or deepest point of the palm was recorded. Hand length was measured using the distance from the tip of the long finger to the distal wrist crease. Each of these hand measurements was taken three times and the mean was recorded. Finally, hand volume was measured using a standard hand volumeter (DBA Sammons Preston, Mount Joy, PA, USA) with the specimen inserted to a depth necessary to contact the bar in the volumeter between the long and ring fingers.
Dissection was then carried out with the aid of ×2.8 loupe magnification down to the FR and structural observations were recorded. Edges of the TCL were identified based primarily on fiber direction and thickness. Any insertions of the thenar or hypothenar musculature onto the TCL were dissected free and reflected away from the TCL. The volar carpal ligament and the contents of Guyon's canal were dissected free from the ulnar aspect of the TCL. Next, the tendons of the flexor digitorum superficialis and profundus, the tendon of the flexor pollicis longus, and the median nerve were identified proximally, transected, and pulled through the carpal tunnel distally. Finally, the carpal tunnel was inspected to ensure that it had been completely evacuated of its contents. Care was taken to preserve the proximal and distal extents of the FR.
The specimen was then placed in a custom-made thermoplast splint (Pro Splint II-M200, Mercer County Rehab, Mercer, PA, USA) with the wrist at an anatomically neutral position at 0° of flexion/extension and radial/ulnar deviation and the thumb at 0° of palmar abduction and 45° of radial abduction. The specimen was affixed to a wooden board using threaded pins directed through the distal radius and third metacarpal head. After vertical positioning of the specimen, an aluminum plate was positioned in the carpal tunnel and held in place with an adjustable boom. The plate contained three control points used to define a local coordinate system and was positioned so that it did not contact the walls of the carpal tunnel. The proximal extent of the antebrachial fascia was then occluded with gauze while keeping the carpal tunnel completely vacant (Fig. 1).
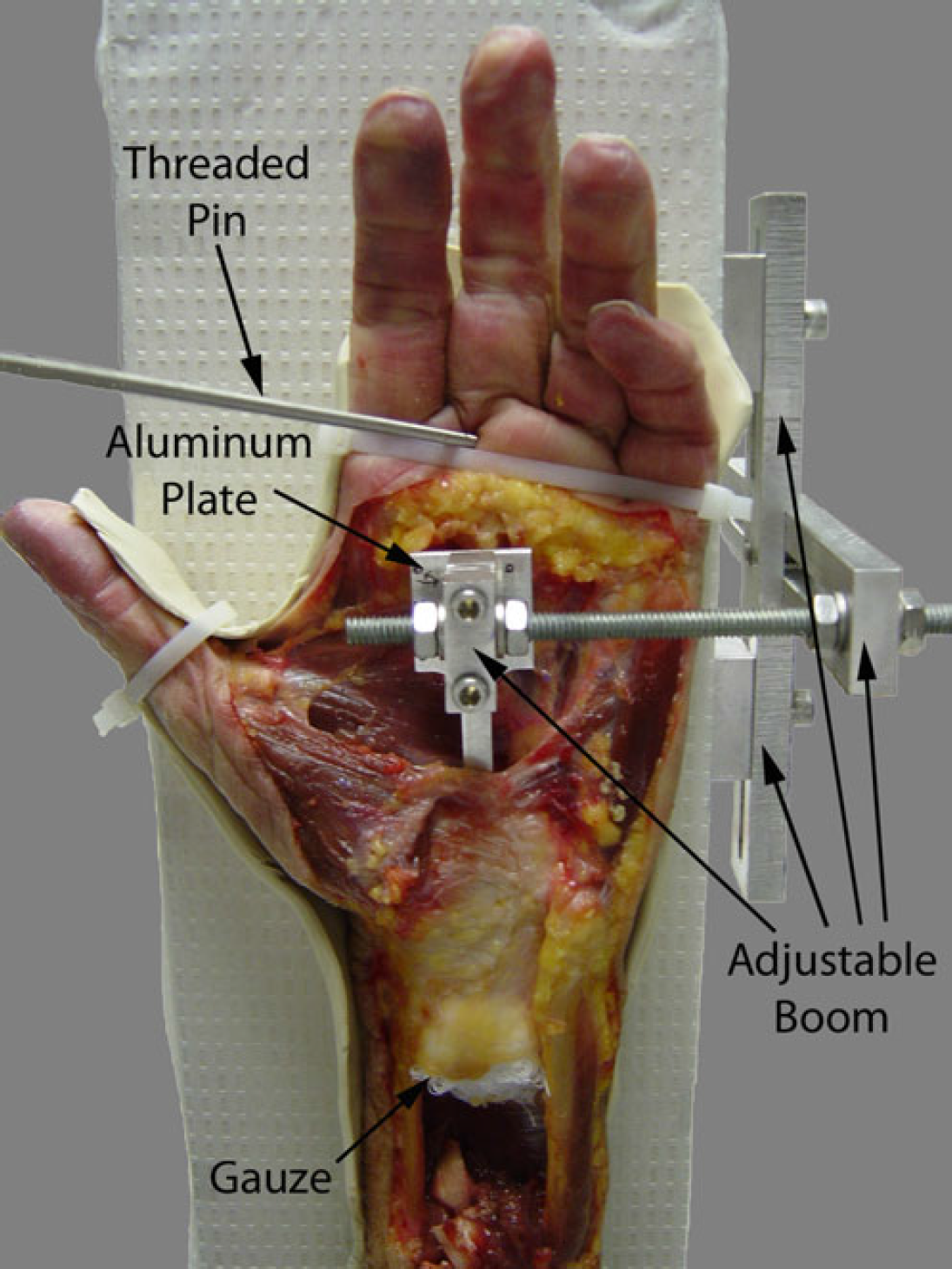
Proper positioning of the dissected specimen in the apparatus ready for pouring of the silicone cast is shown, with the aluminum plate in place and the boom tightened, the specimen securely attached to the splint and apparatus with a threaded pin, and the proximal extent of the antebrachial fascial occluded with gauze.
A platinum-catalyst silicone rubber (Body Double Standard Set, Smooth-On Inc, Easton, PA, USA) was prepared and poured into the carpal tunnel using a 60-cc catheter tipped syringe. This silicone was chosen because it is nonreactive and noncaustic to human tissue. The carpal tunnel was filled beginning with the central proximal aspect and the silicone slowly added to allow it to flow gently without incorporating air. Sufficient silicone was added to ensure that the entire carpal tunnel as well as the proximal and distal FR was filled. This produced a cast longer than the actual carpal tunnel, ensuring that the entire length of the TCL was included. The silicone was allowed to cure for 30 min per manufacturer recommendations.
Digitization using a three-dimensional digitizer (Microscribe GX2, Immersion Corp., San Jose, CA, USA) was then carried out. First, the control points on the aluminum plate were digitized to define the local coordinate system. Several anatomical landmarks were then digitized as reference points—the four bony insertions of the TCL (the ridge of the trapezium, the tubercle of the scaphoid, the pisiform, and the hook of the hamate) and the proximal and distal edges of the TCL. The proximal and distal edges of the TCL were determined through visual inspection using ×2.8 loupe magnification. By convention, the most central (toward the third digital ray) and proximal (regarding the trapezium and hamate) or distal (regarding the scaphoid and pisiform) point of the bony insertions was digitized. Next, the volar surface of the TCL was digitized in its entirety. The TCL was then excised en masse from its bony attachments. The volar surface of the carpal tunnel cast was then digitized as a representation of the dorsal surface of the TCL.
In addition, the accuracy and precision of the digitization protocol was validated prior to formal data acquisition. An aluminum rectangular plate (25.5×25.5×3.1 mm) and a silicone rectangular plate (25.5×25.5×3.6 mm) were manufactured to roughly approximate the overall size of the TCL. The top and bottom surfaces of the plates were digitized and then reconstructed digitally. The thicknesses at multiple points of each plate were then calculated. To test precision, the digitization and calculation were repeated five times. The accuracies of thickness measurement were better than 0.15 mm for the aluminum plate and 0.20 mm for the silicone plate. Regarding precision, the coefficient of variation from the repeated measurements was less than 2.6% for the aluminum plate and 2.3% for the silicone plate.
The digitized data for the TCL of each specimen was analyzed using custom software (MATLAB, MathWorks, Natick, MA, USA). The three-dimensional coordinate data of the volar and dorsal surfaces were converted to the local coordinate system defined by the aluminum plate. Best fit surfaces were constructed based on the TCL surface data points for both the volar and dorsal surfaces. These surfaces were then used in conjunction with the anatomical reference data to calculate the TCL dimensional data. In order to calculate these data, a definition of the TCL was necessary. Radial and ulnar borders of the TCL were defined by the line passing through the ridge of the trapezium and tubercle of the scaphoid and by the line passing through the hook of the hamate and the pisiform, respectively. The midpoints of these two bony lines were then connected with another line, which was defined as the transverse direction (x-axis). The longitudinal direction (y-axis) was then defined perpendicular to this line. The proximal and distal edges of TCL were defined using the digitized proximal and distal edges (Fig. 2a).
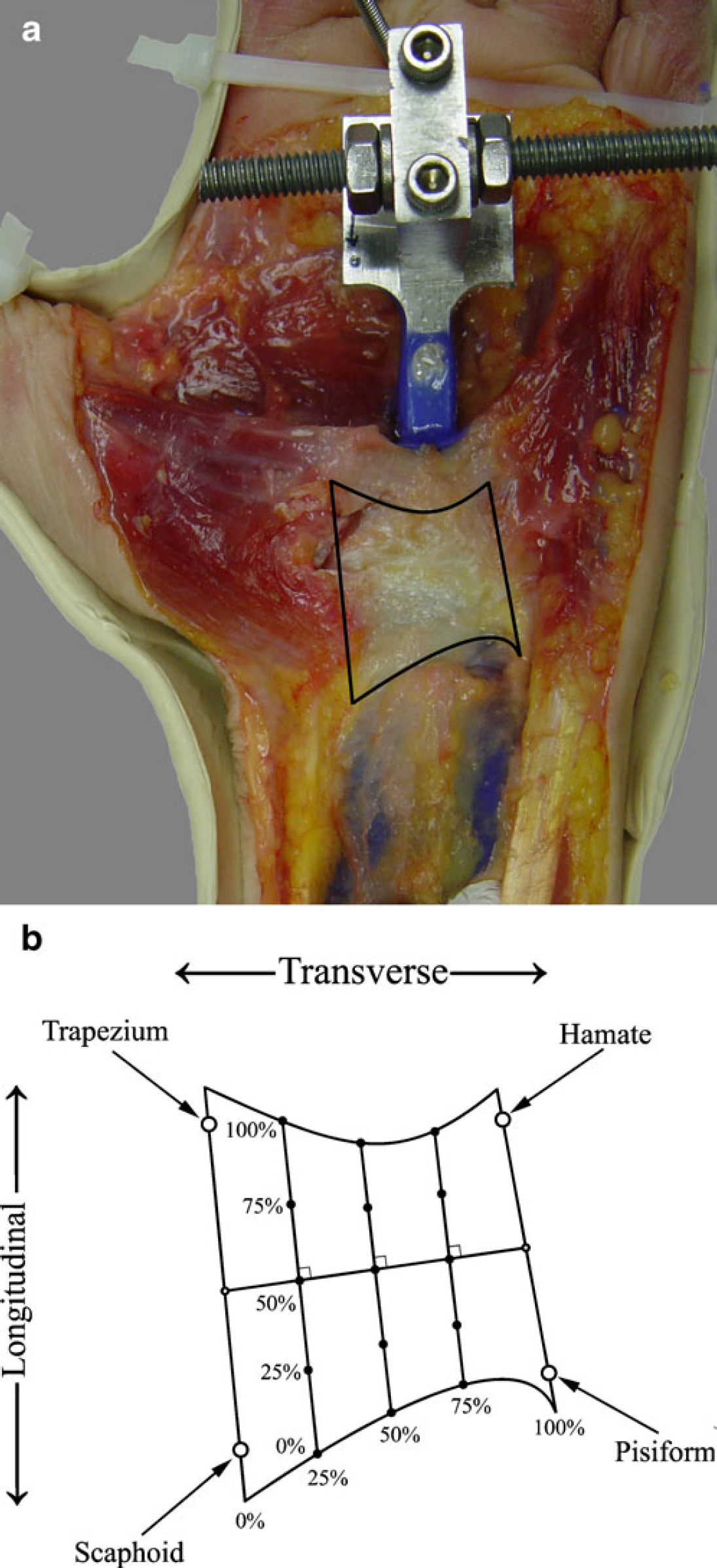
The definition of the TCL.
Using the digitized data and the aforementioned definition of the TCL, several morphological dimensions were calculated. Thicknesses were calculated at five points along the longitudinal direction (y=0%, 25%, 50%, 75%, and 100%; proximal=0%) for each of three locations along the transverse direction (x=25%, 50%, and 75%; radial=25%), producing 15 thicknesses per specimen (Fig. 2b). TCL length and cross-sectional area along the longitudinal (y) direction were also calculated at the three locations along the transverse direction (x=25%, 50%, and 75%). The mean thickness of the central 25% of the TCL area (bounded by 25 and 75% in both the transverse [x] and longitudinal [y] directions) was calculated to provide a general representation of TCL thickness. Finally, the volume of the TCL was calculated using 100% of the longitudinal direction and 70% of the transverse direction (15% to 85% of the transverse direction). The exclusion of the extreme radial and ulnar portions of the TCL was necessary to ensure that the bony attachments of the TCL were not included in the calculation, as the radial and ulnar borders of TCL are slightly concave. Repeated measures analysis of variance (ANOVA) as well as post hoc Tukey's test were performed using SPSS (SPSS Inc., Chicago, IL, USA) to evaluate changes in thicknesses, cross-sectional areas, and lengths. In addition, correlation analyses were performed between external hand dimensions prior to dissection and TCL dimensions as outlined above.
Results
In all specimens, the proximal and distal edges of the TCL were clearly defined by identifying fiber direction and thickness under loupe magnification. The three portions of the FR were noted to be continuous in all specimens. The distal aponeurosis was easily identified based on the distal bony TCL insertion sites as well as fiber directions. Proximally, the division between the TCL and the antebrachial fascia was identified through the opposing fiber directions as well as the large difference in thickness. Distinction of these differences was apparent with the aid of loupe magnification.
With respect to fiber direction, the TCL contained transversely oriented fibers with occasional superficial oblique components in the direction of the pisiform to the trapezium. The distal aponeurosis consisted of obliquely oriented fibers radially along the thenar muscles and ulnarly along the hypothenar muscles, which gradually swept to a transverse orientation toward the midline. The antebrachial fascia had a longitudinal fiber arrangement, which was in clear distinction with the TCL.
A significant portion of the abductor pollicis brevis as well as a smaller portion of flexor pollicis brevis was noted to originate from the TCL. It was necessary to dissect these fibers free in order to produce a surface appropriate for digitization as well as for clear identification of the insertion of the TCL into the ridge of the trapezium. A smaller portion of flexor digiti minimi brevis originated from the ulnar side of the TCL.
An example of the reconstructed volar and dorsal surfaces of the TCL is shown in Fig. 3. The thickness of the TCL was the greatest distally in the midline (x=50%, p<0.05) and ulnar segments (x=75%, p<0.01). However, at the radial segment (x=25%), the thickness was the greatest at the proximal edge (p<0.01). These trends can be seen in Fig. 4. The overall mean thicknesses along the radial, midline, and ulnar portions of the TCL were 2.3±0.9, 1.9±0.6, and 2.0±0.8 mm, respectively, and are not significantly different (p=0.11). The thickness of the central 25% of the TCL was 2.0±0.4 mm. The mean thickness of all points measured in all specimens was 2.1±0.8 mm, ranging from 1.3 to 3.0 mm.
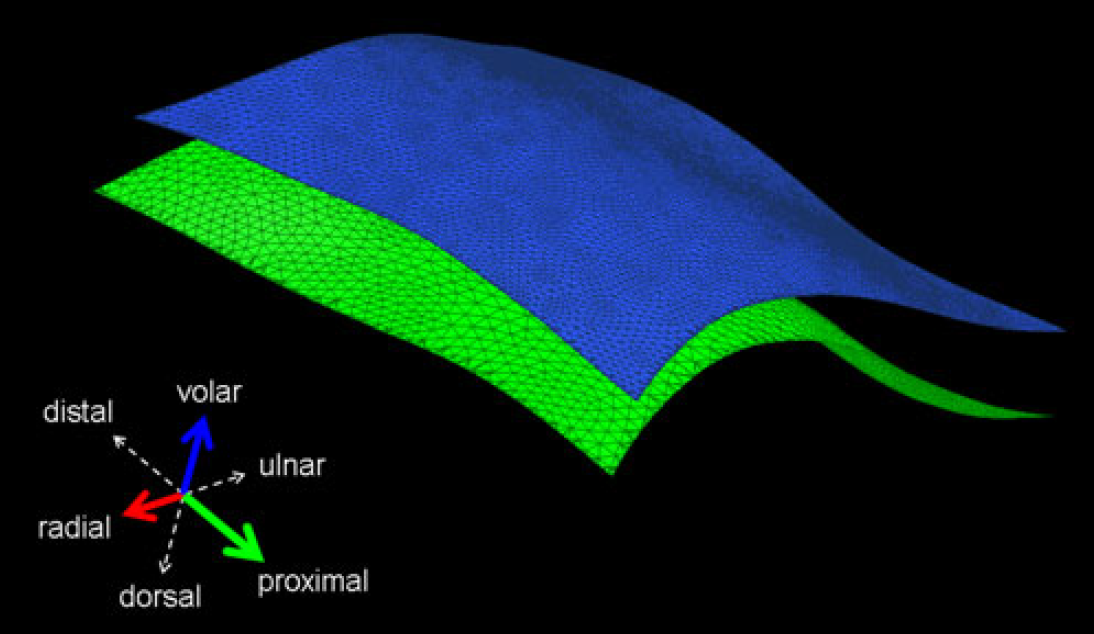
A reconstructed three-dimensional computer model of the TCL from a left hand is depicted. The legend coordinate system is shown in the lower left-hand corner. Solid arrows imply structures projecting out from the page toward the reader; dotted arrows imply structures projecting behind the page away from the reader.
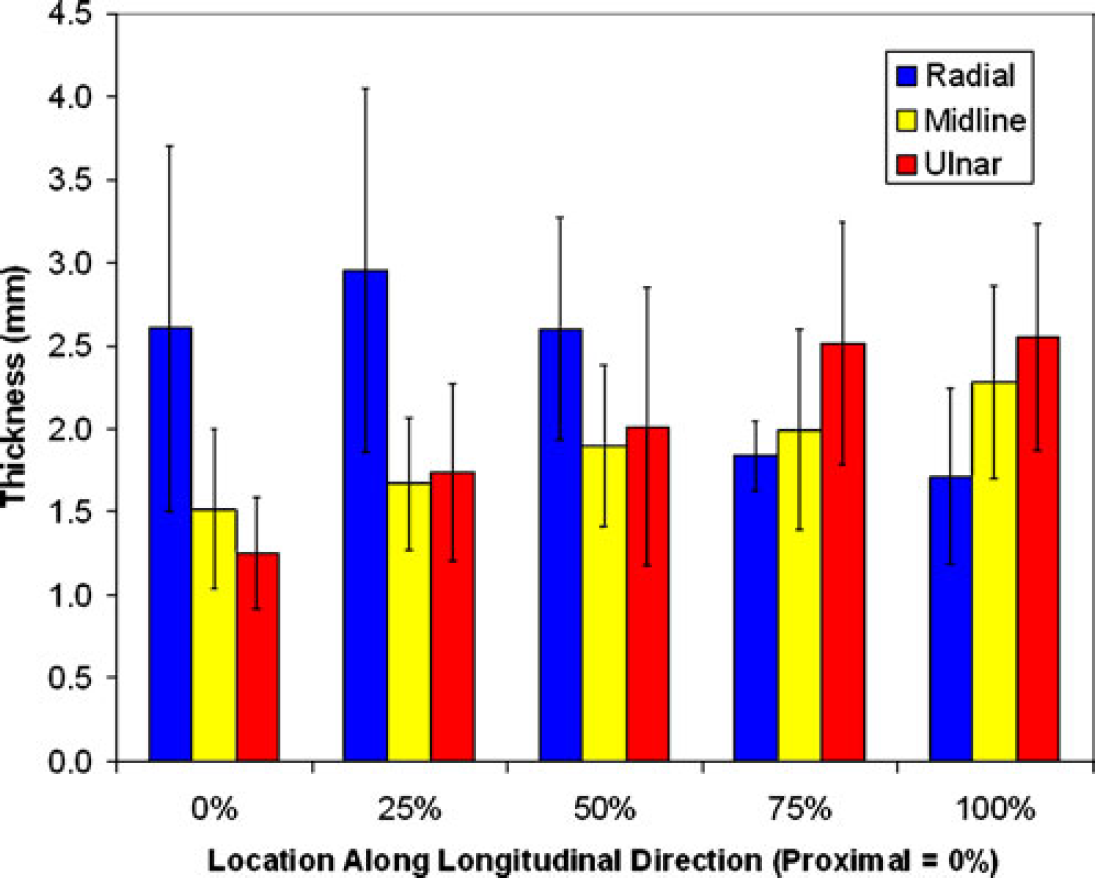
TCL thickness from proximal to distal along the radial, midline, and ulnar portions of the TCL.
The lengths along the radial, midline, and ulnar portions of the TCL were 16.5±2.0, 14.4±1.9, and 15.1±2.6 mm, respectively. These lengths were not significantly different (p=0.11). The TCL cross-sectional areas at the radial, midline, and ulnar segments were 37.8±9.8, 25.2±8.8, and 32.7±12.2 mm2, respectively. ANOVA and post hoc analysis showed that the cross-sectional area of the radial and ulnar segments were significantly greater than that of the midline segment (p<0.01). The volume of the TCL was 781.1±224.1 mm3.
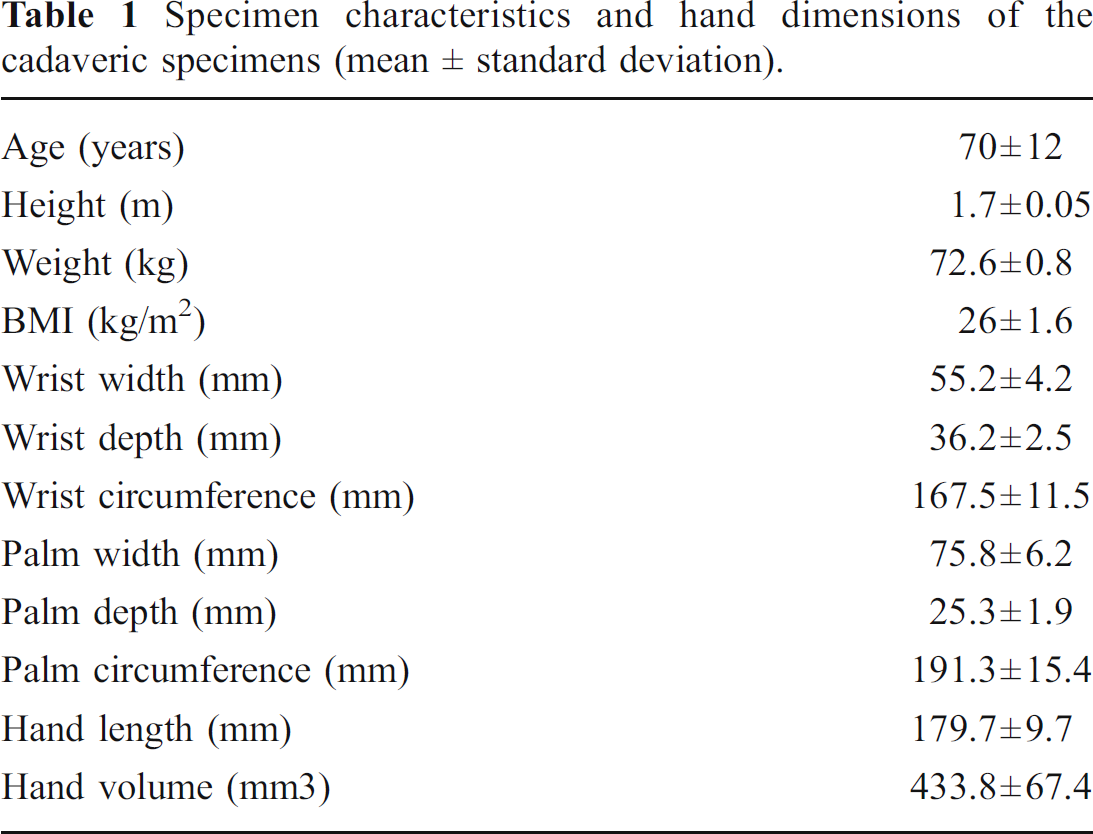
Table 1 lists the mean hand dimensions of the specimens. There was no statistically significant correlation between any TCL dimensions and hand dimensions (all p>0.05).
Specimen characteristics and hand dimensions of the cadaveric specimens (mean ± standard deviation).
Discussion
Utilizing our research findings and prior anatomical studies [1,2,5,6], we propose revised definitions of the FR and TCL. The FR exists as a fascial plane that is continuous with the flexor forearm fascia. It consists of three sections with the first being the distal fascia over the forearm musculature which is also termed the antebrachial fascia. This portion is quite thin and its fibers are readily identified through their longitudinal orientation. The second portion of the FR is the TCL. It has distinct proximal and distal edges which are continuous with the proximal and distal portions of the FR. The TCL is much thicker than the proximal portion of the FR. It consists primarily of fibers oriented in a transverse and oblique manner, as identified by Isogai et al. [3]. The third and most distal portion of the FR is the aponeurosis between the thenar and hypothenar musculature. Its gross thickness is similar to the TCL, and likewise, it has transversely oriented fibers in the midline. These fibers sweep gently to a more oblique direction along the same path as the muscular fibers. The aponeurosis can be distinguished from the TCL based on this fiber direction and location of the thenar and hypothenar musculature. These three portions of the FR may vary in their dimensions and configurations, but are always present.
The current knowledge of TCL morphology has limitations. In the past, only the central portion of the TCL thickness had been studied, and at times, the distal aponeurosis had been considered as part of the TCL [2,7]. The TCL has been previously considered to be thicker centrally and distally while becoming thinner proximally [7]. Our findings show that the midline and ulnar portions of the TCL are the thickest distally as stated in the literature. The radial portion of the TCL, however, is the thickest proximally. While the mean thicknesses of the TCL at the radial, midline, and ulnar portions are not significantly different, the variability in the thickness distribution at the radial portion as compared to the midline and ulnar portions was statistically significant. Thus, the TCL becomes thicker distally at the midline and ulnar portions, but becomes thinner distally at the radial portion. The etiology of this variation in TCL thickness is unknown, but is anatomically significant. The median nerve traverses the radial portion of the carpal tunnel, deep to this sudden change in typical TCL thickness distribution. This normal anatomic variation may be involved with the development of CTS, either by a third factor that affects both the TCL thickness and the median nerve or by this thickened portion of the TCL directly affecting the median nerve. Further research into the TCL anatomy of patients with CTS is necessary to evaluate if this change in thickness distribution is seen in these patients as well, if the thickness is greater, or if some other pattern is present. If the TCL could be imaged reliably and noninvasively in patients, such analysis would be possible.
Hand dimensions did not significantly correlate with any of the TCL dimensions identified. It is not possible to draw direct conclusions from this result, as this statistical result may be a reflection of inadequate sample size to detect a small correlation. It is possible that a correlation does exist but is simply too weak or the variance explained through too many factors to identify this correlation with any one specific variable.
This study has several limitations. First, the dimensional calculations of the TCL excluded 15% of ligament at the radial and ulnar borders. This procedure was justified for the quantification of TCL thickness, but resulted in underestimation of the TCL volume. Secondly, the sample size utilized in this study was relatively small. The relationship between hand size and TCL dimensions might be better established with a larger sample size.
Footnotes
Acknowledgments
The authors thank Jie Tang and Luke Xie for their technical help and Jay Irrgang, PhD, for his assistance with statistical analysis. The authors acknowledge the support from the National Institutes Health (NIH R03AR054510), and The Pittsburgh Foundation, Albert B. Ferguson, M.D., Orthopaedic Fund.